Vitamin D reduces COVID-19 risk: real-time meta-analysis of 370 studies (138 treatment studies and 232 sufficiency studies)
 Control
ControlAbstract
Significantly lower risk is seen for
mortality,
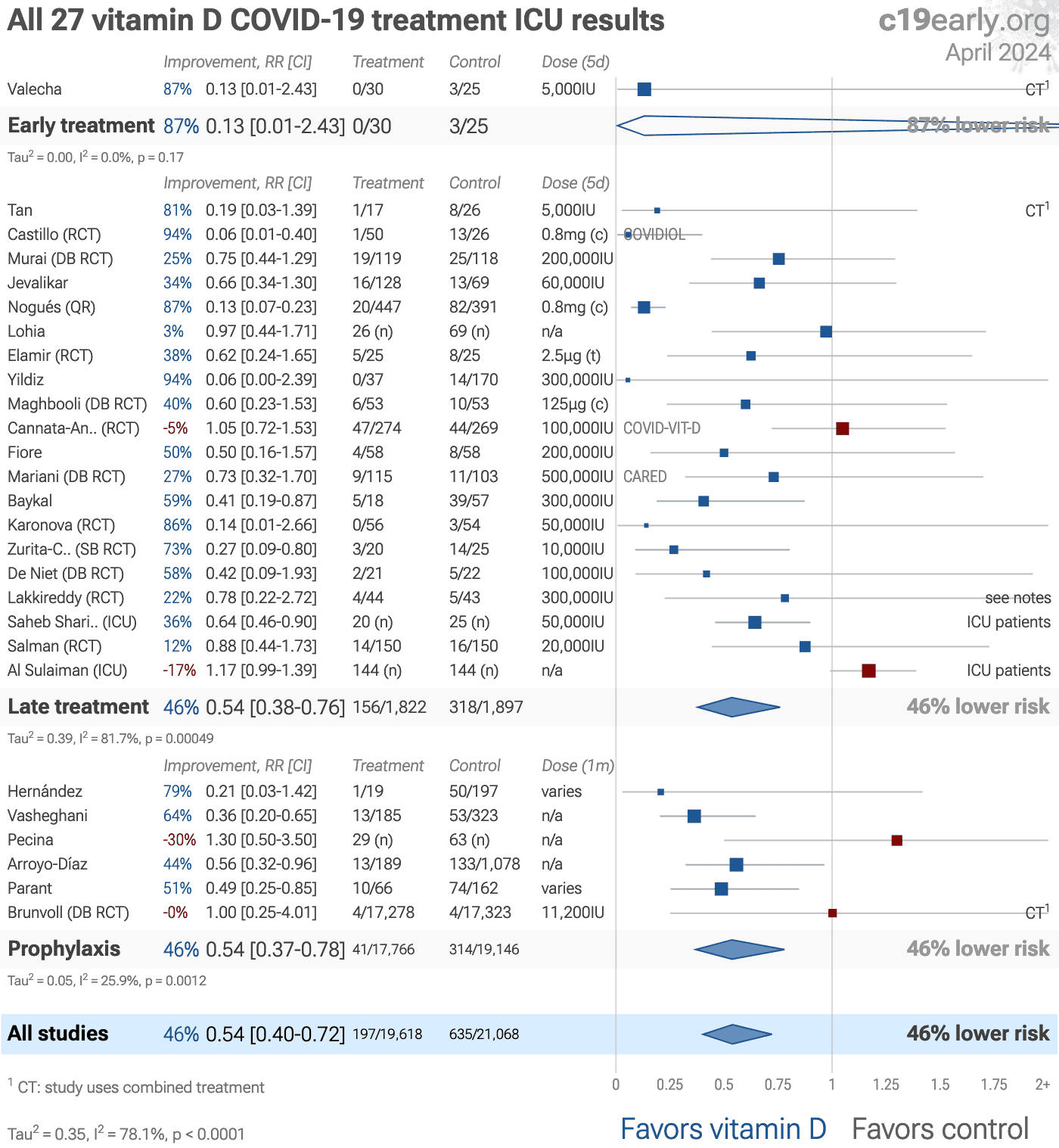
ICU admission,
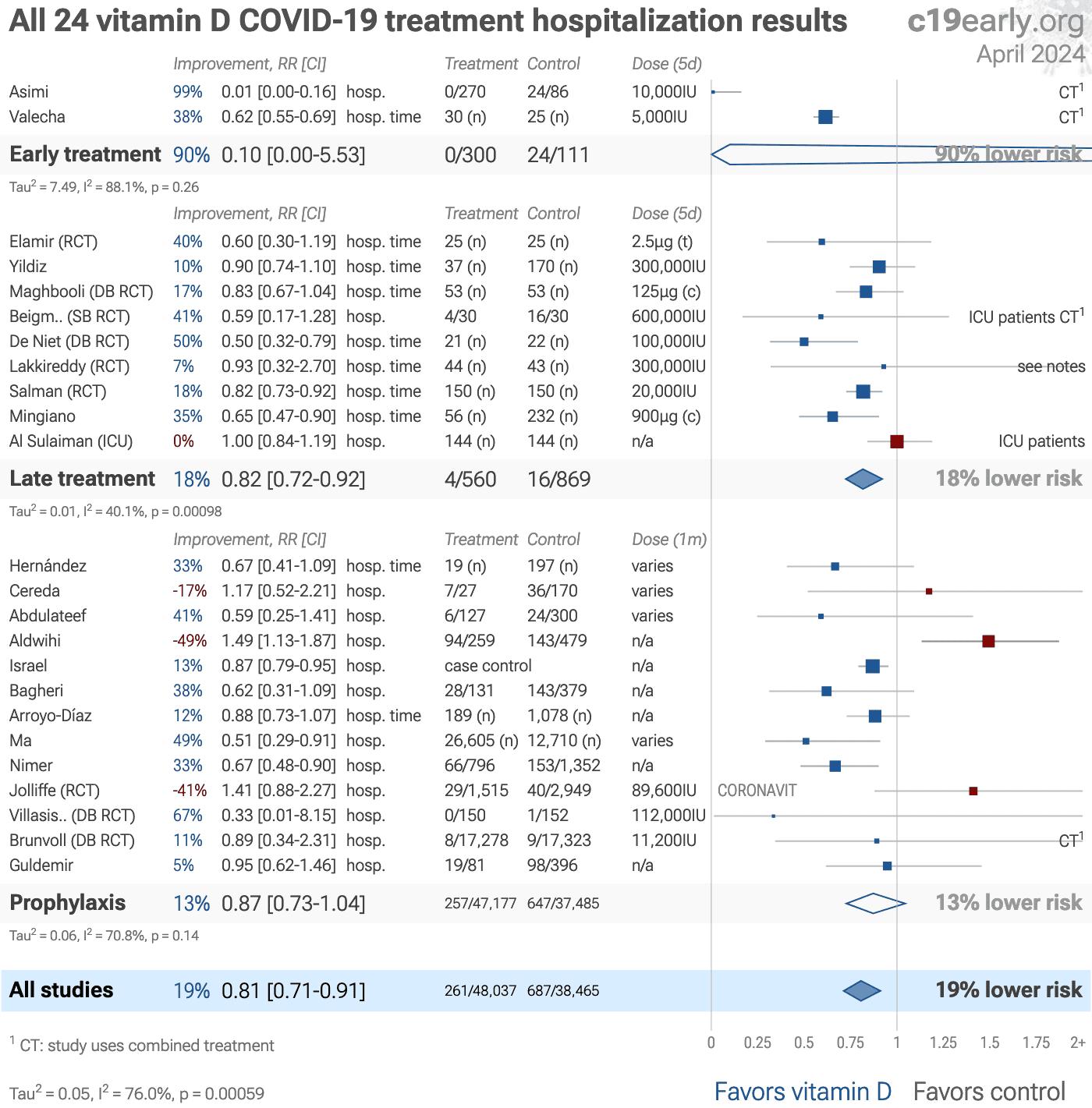
hospitalization, and
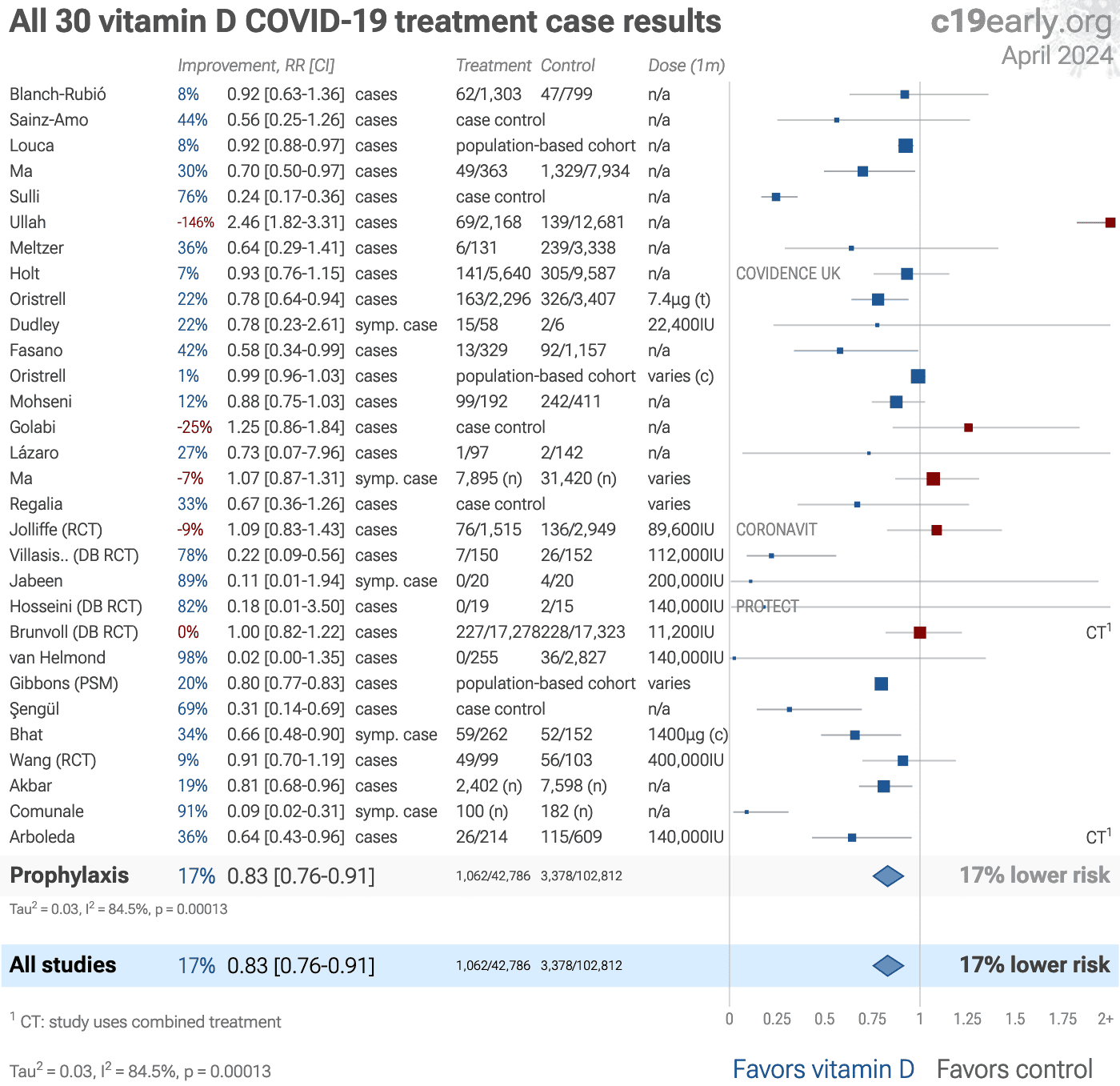
cases.
75 studies from 69 independent teams in 25 countries show significantly
lower risk.
Meta-analysis using the most serious
outcome reported shows 56% [37‑70%] and
38% [33‑43%] lower risk for early treatment
and for all studies.
Results are similar for higher quality studies,
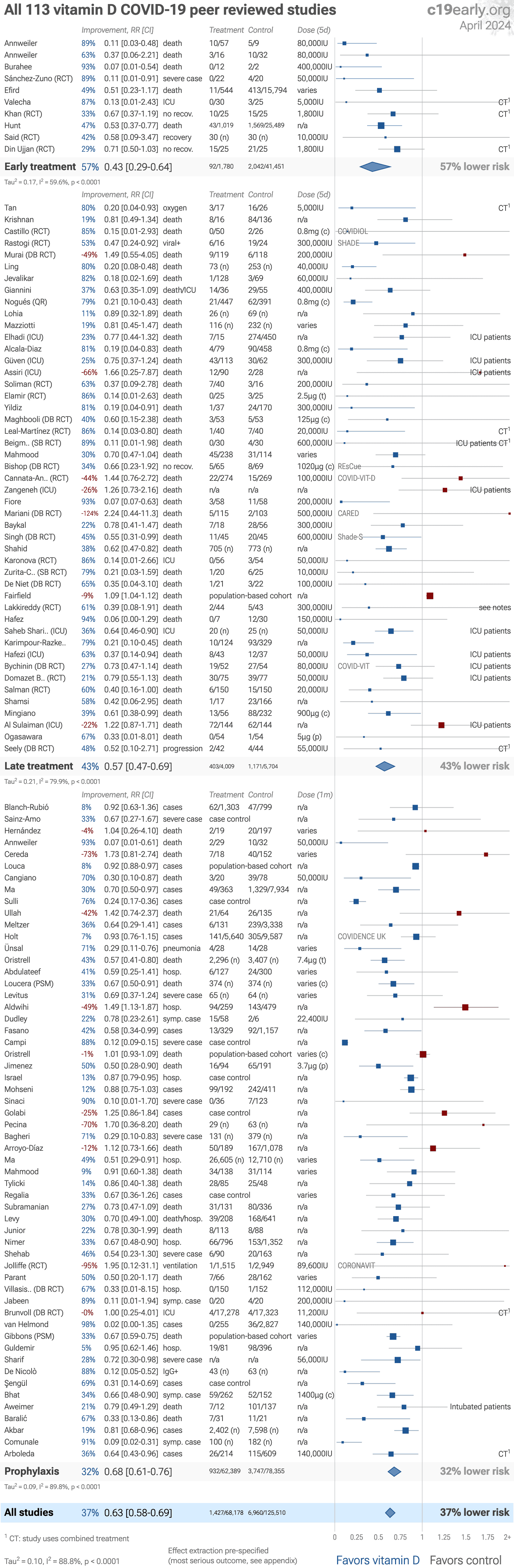
peer-reviewed studies, and mortality.
Late stage treatment with calcitriol/calcifediol
and analogs is more effective than cholecalciferol: 66% [47‑78%]
vs. 43% [32‑52%].
Ongoing treatment with multiple doses is more
effective than single bolus doses:
60% [50‑68%] vs. 22% [1‑38%]
Results are very robust—in worst case exclusion sensitivity analysis 91 of
138 studies must be excluded before statistical significance is lost.
Emergent results matching biological mechanisms confirm efficacy: efficacy gradient across outcomes (p = 0.031), calcitriol/calcifediol vs. cholecalciferol (p = 0.033), continuous vs. bolus treatment (p = 0.000035), and acute treatment vs. chronic prophylaxis (p = 0.0042).
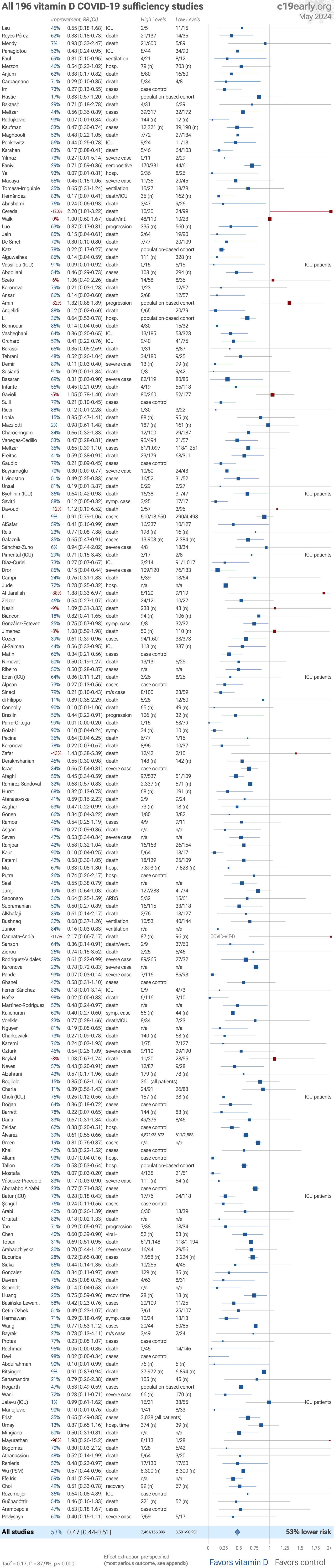
232 sufficiency studies
show a strong association between vitamin D sufficiency and outcomes, with
50% [47‑53%] lower risk for higher levels.
No treatment is 100%
effective. Protocols combine safe and effective options with individual
risk/benefit analysis and monitoring.
Other treatments are more effective.
Administration with fat increases the bioavailability of vitamin D, and may aid distribution to target tissues.
Sunlight or dietary sources may be preferred.
The quality of non-prescription supplements varies widely1-3.

Vitamin D for COVID-19 — Highlights
Vitamin D reduces risk with very high confidence for mortality, ICU admission, hospitalization, recovery, cases, viral clearance, and in pooled analysis, high confidence for progression, and low confidence for ventilation.
Ongoing treatment with multiple doses is more effective than single bolus doses.
Calcitriol/calcifediol and analogs are more effective than cholecalciferol.
Emergent results matching biological mechanisms confirm efficacy: efficacy gradient across outcomes (p = 0.031), calcitriol/calcifediol vs. cholecalciferol (p = 0.033), continuous vs. bolus treatment (p = 0.000035), and acute treatment vs. chronic prophylaxis (p = 0.0042).
Early treatment is more effective than late treatment.
8th treatment shown effective in October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
Real-time updates and corrections with a consistent protocol for 226 treatments. Outcome specific analysis and combined evidence from all studies including treatment delay, a primary confounding factor.
B
Loading..
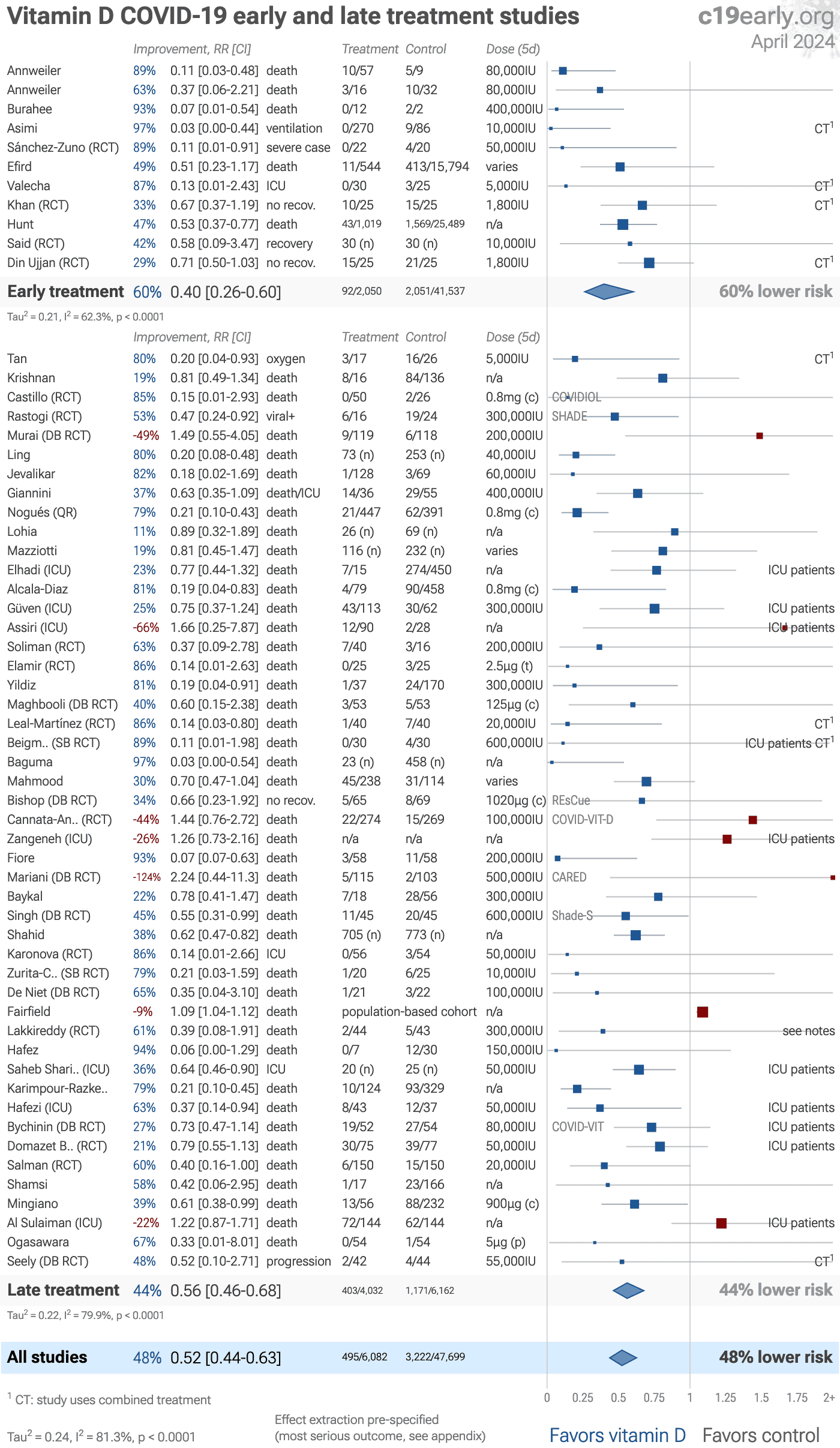
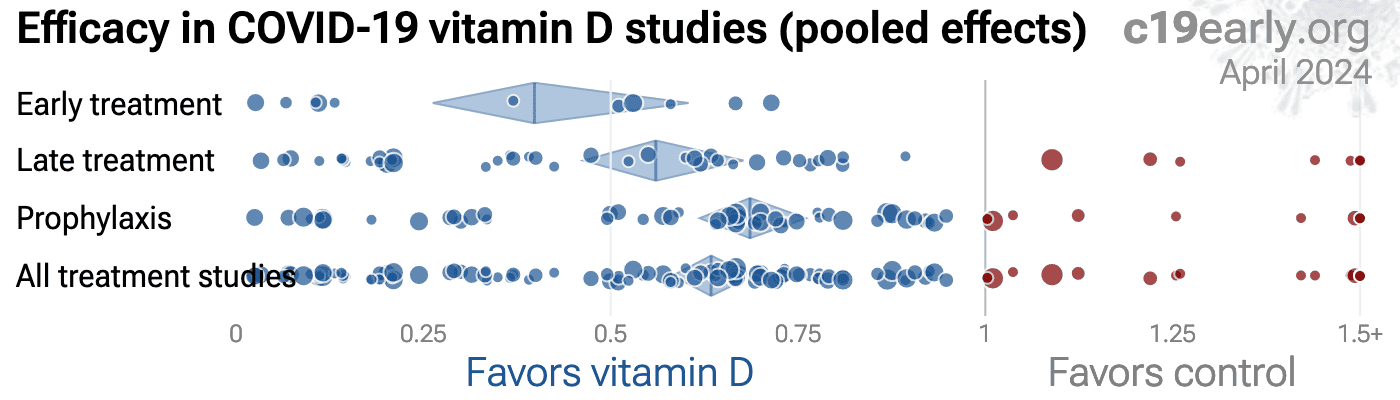
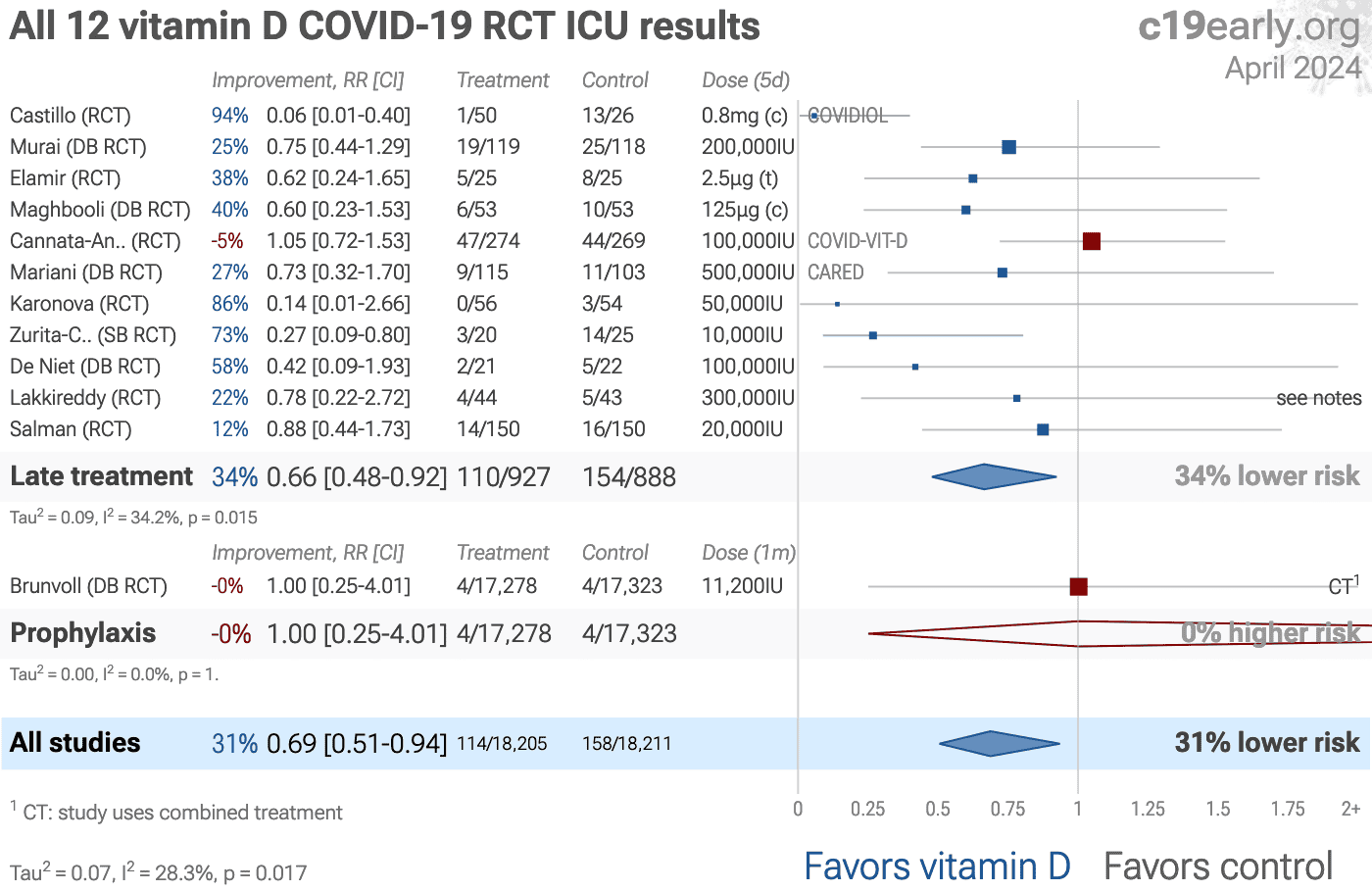
Fig. 1. A. Random-effects meta-analysis for early and late treatment studies. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
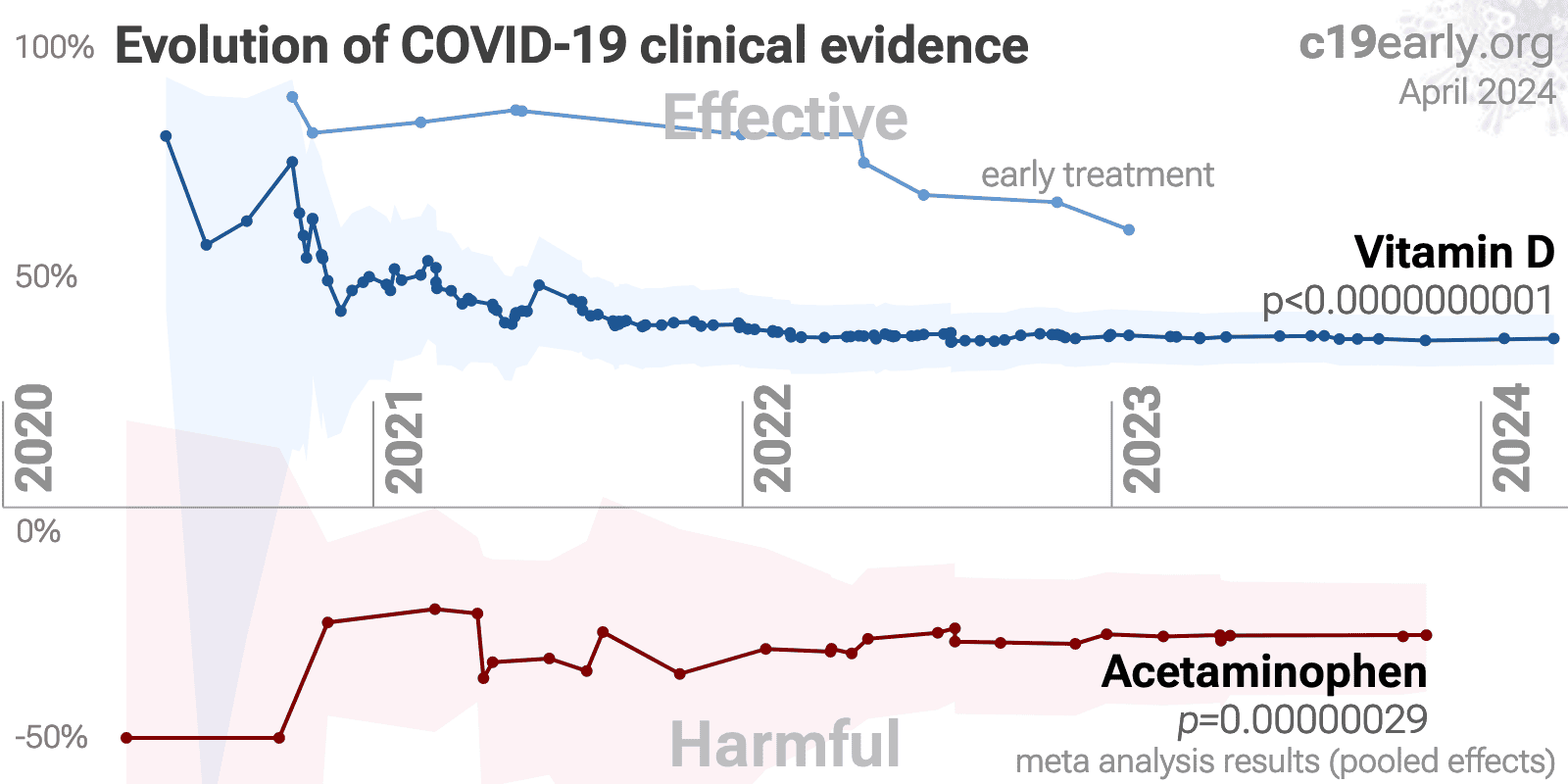
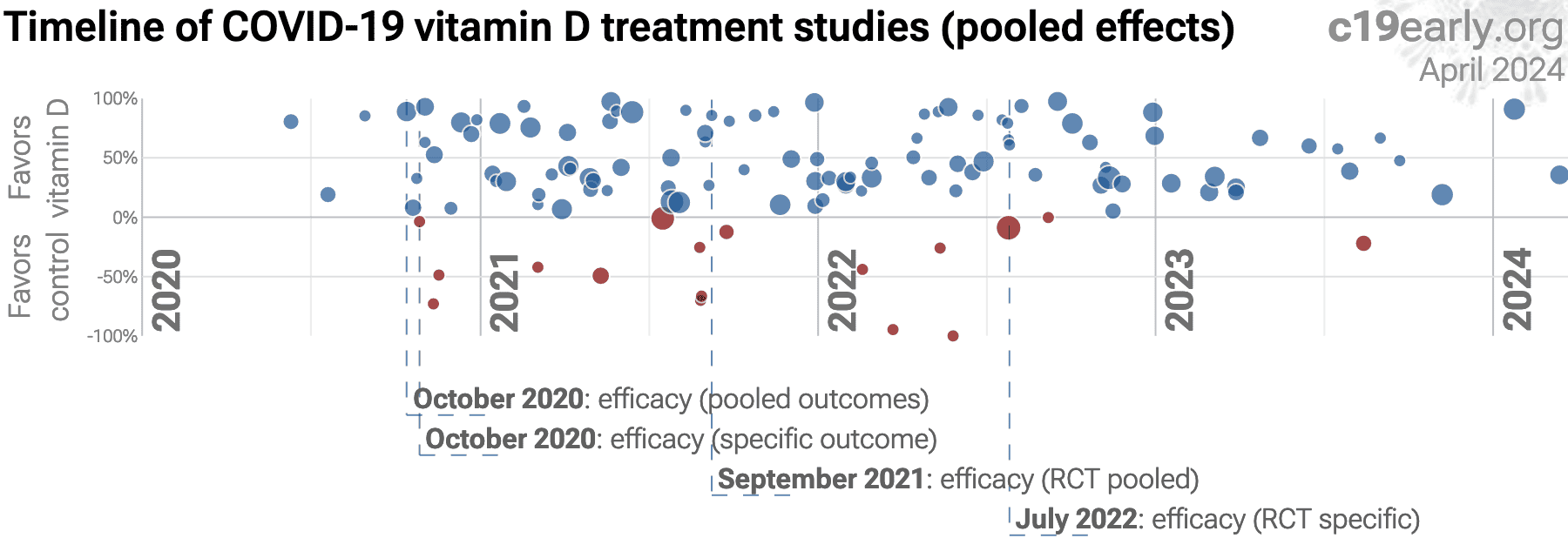
B. Timeline of results in vitamin D studies. The marked dates indicate the time when efficacy was known with a statistically significant improvement of ≥10% from ≥3 studies for pooled outcomes, one or more specific outcome, pooled outcomes in RCTs, and one or more specific outcome in RCTs. Efficacy based on RCTs only was delayed by 12.0 months, compared to using all studies. Efficacy based on specific outcomes in RCTs was delayed by 9.4 months, compared to using pooled outcomes in RCTs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
SARS-CoV-2 infection primarily begins in the upper respiratory
tract and may progress to the lower respiratory tract, other tissues, and the
nervous and cardiovascular systems, which may lead to cytokine storm,
pneumonia, ARDS, neurological injury27-43 and
cognitive deficits30,35, cardiovascular
complications44-50, DNA
damage51-54, organ failure, and death.
Even mild untreated infections may result in persistent cognitive
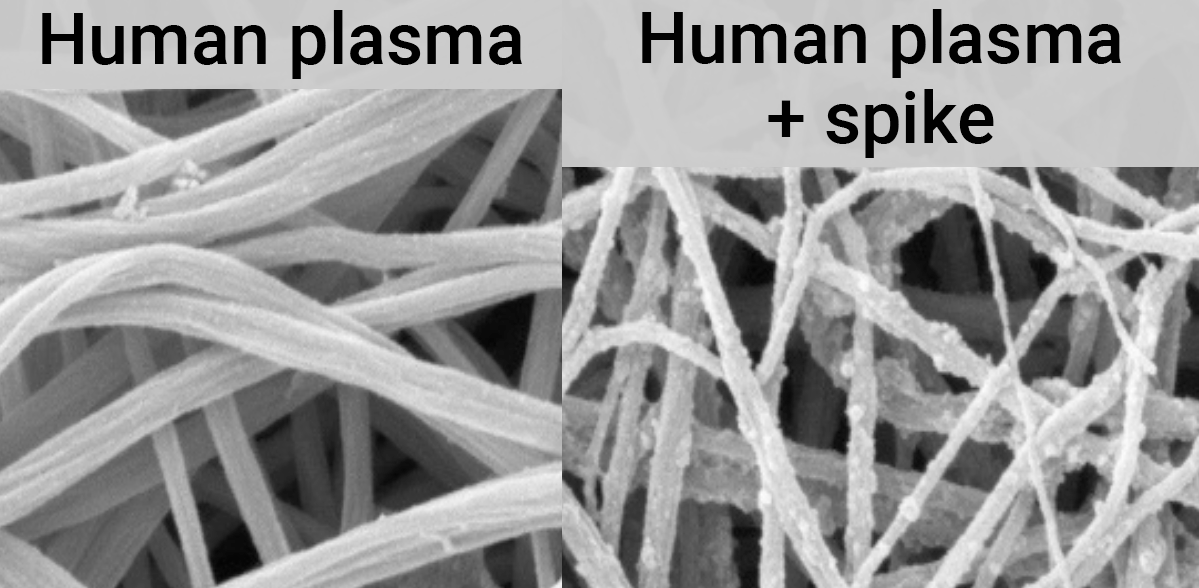
deficits55—the spike protein binds to fibrin leading to
fibrinolysis-resistant blood clots, thromboinflammation, and
neuropathology.
Minimizing replication as early as possible is recommended.
SARS-CoV-2 infection and replication involves the complex interplay of 500+
host and viral proteins and other factorsA,56-63 , providing many
therapeutic targets for which many existing compounds have known activity.
Scientists have predicted that over 11,000 compounds may
reduce COVID-19 risk64, either by
directly minimizing infection or replication, by supporting immune system
function, or by minimizing secondary complications.
We analyze all significant controlled studies of vitamin D for
COVID-19. Search methods, inclusion criteria, effect extraction criteria (more
serious outcomes have priority), all individual study data, PRISMA answers,
and statistical methods are detailed in Appendix 1.
We perform random-effects meta-analysis for all treatment studies, Randomized
Controlled Trials, peer-reviewed studies, studies using cholecalciferol vs.
calcifediol/calcitriol and analogs, studies using large bolus doses vs.
ongoing treatment, higher quality studies, and for specific outcomes:
mortality, mechanical ventilation, ICU admission, hospitalization, and case
results. Results are presented for prophylaxis, early treatment, and late
treatment.
Separately, we perform random-effects meta-analysis for studies that analyze
outcomes based on vitamin D sufficiency (non-treatment studies).
Vitamin D has been identified by the European Food Safety Authority (EFSA) as having sufficient evidence for a causal relationship between intake and optimal immune system function65-68.
Vitamin D inhibits SARS-CoV-2 replication in vitro69,70, mitigates lung inflammation, damage, and lethality in mice with an MHV-3 model for β-CoV respiratory infections69,70, reduces SARS-CoV-2 replication in nasal epithelial cells via increased type I interferon expression71, downregulates proinflammatory cytokines IL-1β and TNF-α in SARS-CoV-2 spike protein-stimulated cells72, attenuates nucleocapsid protein-induced hyperinflammation by inactivating the NLRP3 inflammasome through the VDR-BRCC3 signaling pathway73, may be neuroprotective by protecting the blood-brain barrier, reducing neuroinflammation, and via immunomodulatory effects74, may mitigate hyperinflammation and cytokine storm by upregulating TLR10 expression which downregulates proinflammatory cytokines75, downregulates ACE2 and TMPRSS2 in human trophoblasts and minimizes spike protein-induced inflammation76, may minimize cytokine storm by dampening excessive cytokine production77, may suppress viral entry and replication via LL-37 induction78,79, and minimizes platelet aggregation mediated by SARS-CoV-2 spike protein via inhibiting integrin αIIbβ3 outside-in signaling80.
Cholecalciferol and calcifediol directly bind two allosteric pockets on the SARS-CoV-2 Spike RBD, bias the trimer toward a closed state, weaken ACE2 engagement, and reduce viral entry in cell models81.
Calcitriol may destabilize the Spike protein architecture and inhibit IL-17R dimerization, blocking viral entry and mitigating hyperinflammatory cytokine storm82.
Vitamin D improves regulatory immune cell levels and control of proinflammatory cytokines in severe COVID-1983.
Calcifediol inhibits SARS-CoV-2 papain-like protease (PLpro), a critical enzyme for viral replication84.
Symptomatic COVID-19 is associated with a lower frequency of natural killer (NK) cells and vitamin D has been shown to improve NK cell activity85,86.
Vitamin D
is a steroid hormone that helps regulate the immune system by binding to
specific receptors and activating genes involved in immune defense. It
increases the production of antimicrobial proteins, like cathelicidin and
defensins, which fight a variety of pathogens, including bacteria, viruses,
and fungi. Vitamin D supports the immune system by boosting our natural
defenses and promoting healthy cell connections. It helps clear respiratory
pathogens through processes like apoptosis and autophagy and regulates
toll-like receptors, which play a key role in immunity. Vitamin D also aids in
immune cell maturation, balances inflammation, and reduces the production of
proinflammatory cytokines. Vitamin D has been shown to downregulate
angiotensin-converting enzyme-2 (ACE-2) receptors, which play a role in
COVID-19 infection. By suppressing the production of ACE-2 and related
molecules, vitamin D increases antioxidant and anti-inflammatory effects,
enhances antimicrobial defenses, reduces cytokine storms, and promotes a
protective immune response, all of which help decrease the severity of the
disease. Vitamin D was first identified in relation to bone health, but is now
known to have multiple functions, including an important role in the immune
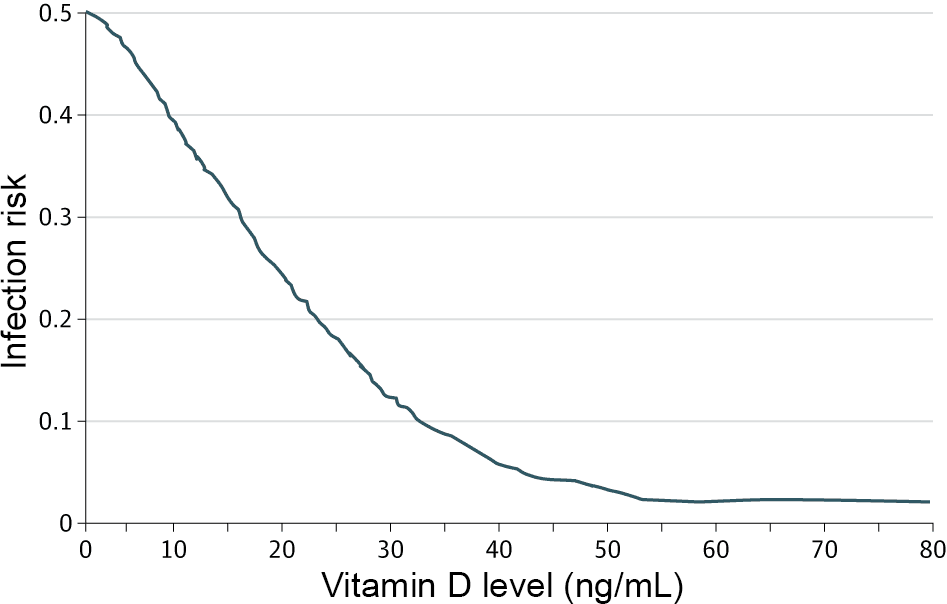
system91,92. For example, Quraishi et al. show a
strong association between pre-operative vitamin D levels and
hospital-acquired infections, as shown in Fig. 3.
{kind=link}
Fig. 3. Risk of hospital-acquired infections as a function of pre-operative vitamin D levels, from Quraishi et al.
{kind=link}
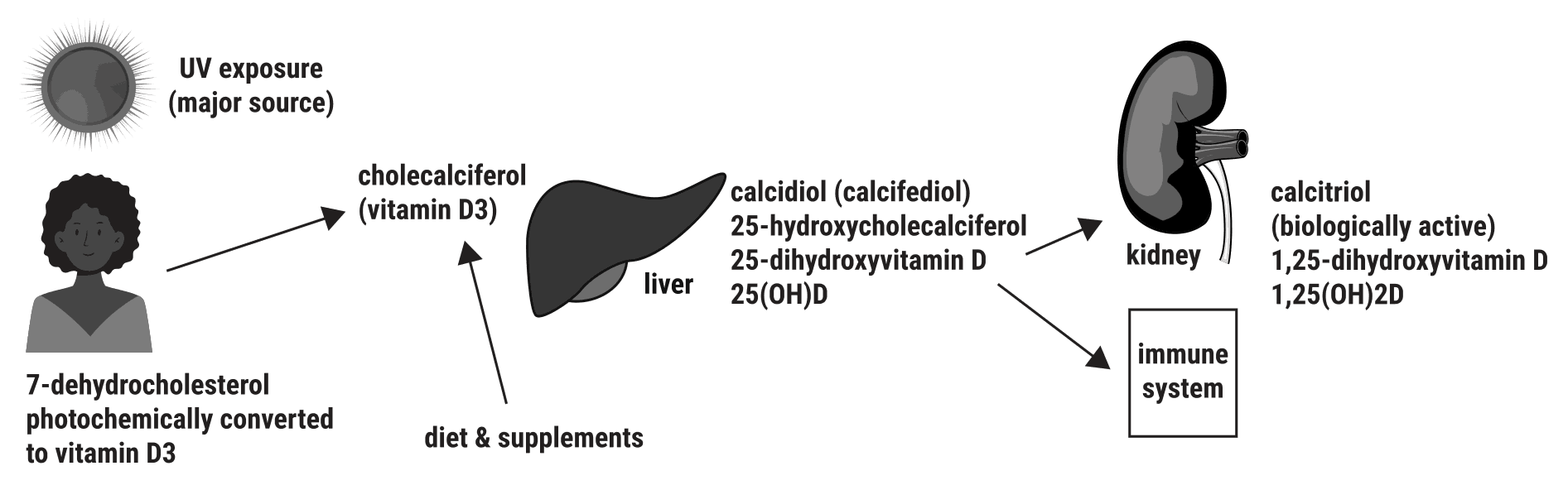
Fig. 4. Simplified view of vitamin D sources and conversion.
Vitamin D undergoes two conversion steps before reaching the biologically
active form as shown in Fig. 4. The first step is conversion to
calcidiol, or 25(OH)D, in the liver. The second is conversion to calcitriol,
or 1,25(OH)2D, which occurs in the kidneys, the immune system, and elsewhere.
Calcitriol is the active, steroid-hormone form of vitamin D, which binds with
vitamin D receptors found in most cells in the body. There is a significant
delay involved in the conversion from cholecalciferol, therefore calcifediol
(calcidiol) or calcitriol may be preferable for treatment.
Many vitamin D studies
analyze outcomes based on serum vitamin D levels which may be maintained via
sun exposure, diet, or supplementation. We refer to these studies as
sufficiency studies, as they typically present outcomes based on vitamin D
sufficiency. These studies do not establish a causal link between vitamin D
and outcomes. In general, low vitamin D levels are correlated with many other
factors that may influence COVID-19 susceptibility and severity. Therefore,
beneficial effects found in these studies may be due to factors other than
vitamin D. On the other hand, if vitamin D is causally linked to the observed
benefits, it is possible that adjustments for correlated factors could obscure
this relationship. COVID-19 disease may also affect vitamin D
levels94, suggesting additional caution in interpreting results
for studies where the vitamin D levels are measured during the disease. For
these reasons, we analyze sufficiency studies separately from treatment
studies. We include all sufficiency studies that provide a comparison between
two groups with low and high levels. Some studies only provide results as a
function of change in vitamin D levels95-97,
which may not be indicative of results for deficiency/insufficiency versus
sufficiency (increasing already sufficient levels may be less useful for
example).
Some studies only show the average vitamin D level for patients in different
groups98-140, most of which show lower D
levels for worse outcomes. Other studies analyze vitamin D status and outcomes
in geographic regions141-148, all finding
worse outcomes to be more likely with lower D levels.
Sufficiency studies vary widely in terms of when vitamin D
levels were measured, the cutoff level used, and the population analyzed (for
example studies with hospitalized patients exclude the effect of vitamin D on
the risk of hospitalization). We do not analyze sufficiency studies in more
detail because there are many controlled treatment studies that provide better
information on the use of vitamin D as a treatment for COVID-19. A more
detailed analysis of sufficiency studies can be found in Chiodini et al.
Mishra et al. present a systematic review and meta-analysis showing that
vitamin D levels are significantly associated with COVID-19 cases.
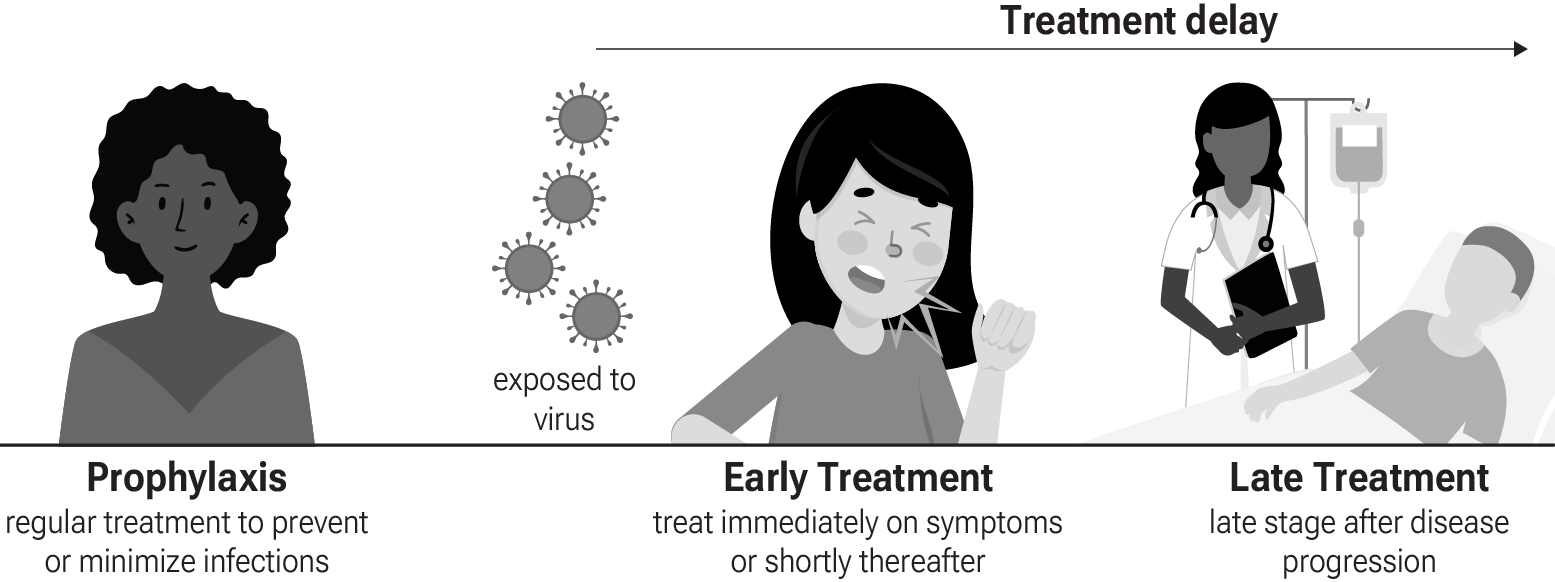
For studies regarding treatment with vitamin D, we distinguish
three stages as shown in Fig. 5. Prophylaxis refers to
regularly taking vitamin D before being infected in order to minimize the
severity of infection. Due to the mechanism of action, vitamin D is unlikely
to completely prevent infection, although it may prevent infection from
reaching a level detectable by PCR. Early treatment refers to treatment
immediately or soon after symptoms appear, while late treatment refers
to more delayed treatment.
{kind=link}
Fig. 5. Treatment stages.
Vitamin D inhibits SARS-CoV-2 replication in vitro69,70, mitigates lung inflammation, damage, and lethality in mice with an MHV-3 model for β-CoV respiratory infections69,70, reduces SARS-CoV-2 replication in nasal epithelial cells via increased type I interferon expression71, downregulates proinflammatory cytokines IL-1β and TNF-α in SARS-CoV-2 spike protein-stimulated cells72, attenuates nucleocapsid protein-induced hyperinflammation by inactivating the NLRP3 inflammasome through the VDR-BRCC3 signaling pathway73, may be neuroprotective by protecting the blood-brain barrier, reducing neuroinflammation, and via immunomodulatory effects74, may mitigate hyperinflammation and cytokine storm by upregulating TLR10 expression which downregulates proinflammatory cytokines75, downregulates ACE2 and TMPRSS2 in human trophoblasts and minimizes spike protein-induced inflammation76, may minimize cytokine storm by dampening excessive cytokine production77, may suppress viral entry and replication via LL-37 induction78,79, and minimizes platelet aggregation mediated by SARS-CoV-2 spike protein via inhibiting integrin αIIbβ3 outside-in signaling80.
Cholecalciferol and calcifediol directly bind two allosteric pockets on the SARS-CoV-2 Spike RBD, bias the trimer toward a closed state, weaken ACE2 engagement, and reduce viral entry in cell models81.
Calcitriol may destabilize the Spike protein architecture and inhibit IL-17R dimerization, blocking viral entry and mitigating hyperinflammatory cytokine storm82.
Preclinical research is an important part of the development of
treatments, however results may be very different in clinical trials.
Preclinical results are not used in this paper.
Table 1 summarizes the results for all stages combined, for Randomized Controlled Trials, for peer-reviewed studies, with different exclusions, for specific outcomes, and for sufficiency (non-treatment) studies.
Table 2 shows results by treatment stage.
Fig. 6 shows individual results by treatment stage.
Fig. 7, 8, 9, 10, 11, 12, 13, and 14
show forest plots for random-effects meta-analysis of
all treatment studies, treatment mortality, treatment ventilation, treatment ICU admission, treatment hospitalization, treatment cases, treatment peer-reviewed studies, and sufficiency studies.
| Relative Risk | Studies | Patients | |
|---|---|---|---|
| All studies | 0.62 [0.57‑0.67] p < 0.0001**** | 138 | 200K |
| Exc. late treatmentExc. late | 0.51 [0.43‑0.60] p < 0.0001**** | 73 | 50K |
| After exclusions | 0.58 [0.53‑0.64] p < 0.0001**** | 102 | 170K |
| Peer-reviewedPeer-reviewed | 0.61 [0.56‑0.67] p < 0.0001**** | 131 | 190K |
| RCTsRCTs | 0.65 [0.55‑0.77] p < 0.0001**** | 41 | 40K |
| RCTs after exclusionsRCTs w/exc. | 0.59 [0.48‑0.73] p < 0.0001**** | 32 | 40K |
| Cholecalciferol | 0.63 [0.58‑0.68] p < 0.0001**** | 123 | 190K |
| Calcifediol/calcitriolCalcifediol | 0.48 [0.35‑0.67] p < 0.0001**** | 15 | 9,569 |
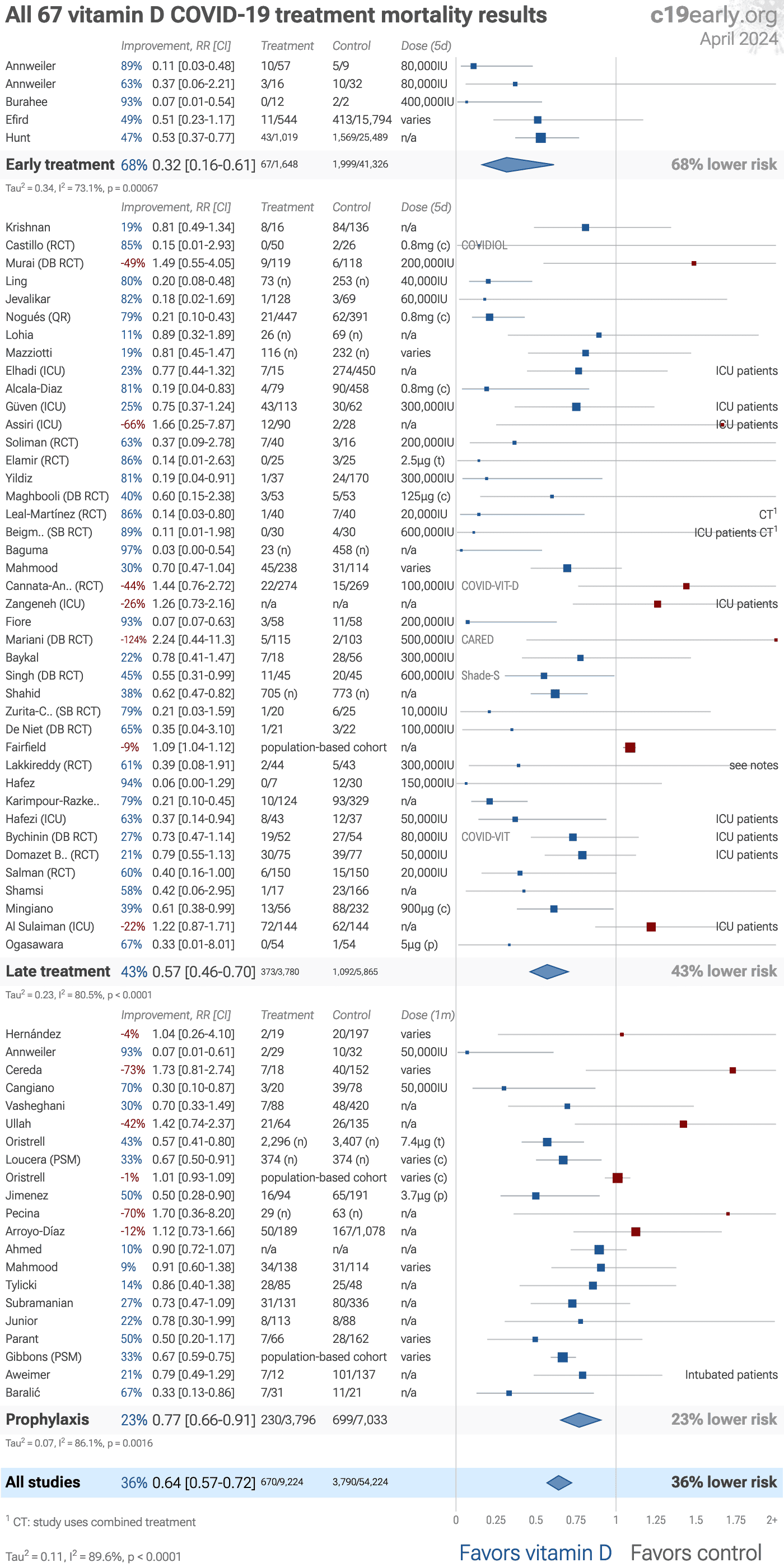
| Mortality | 0.61 [0.55‑0.68] p < 0.0001**** | 79 | 60K |
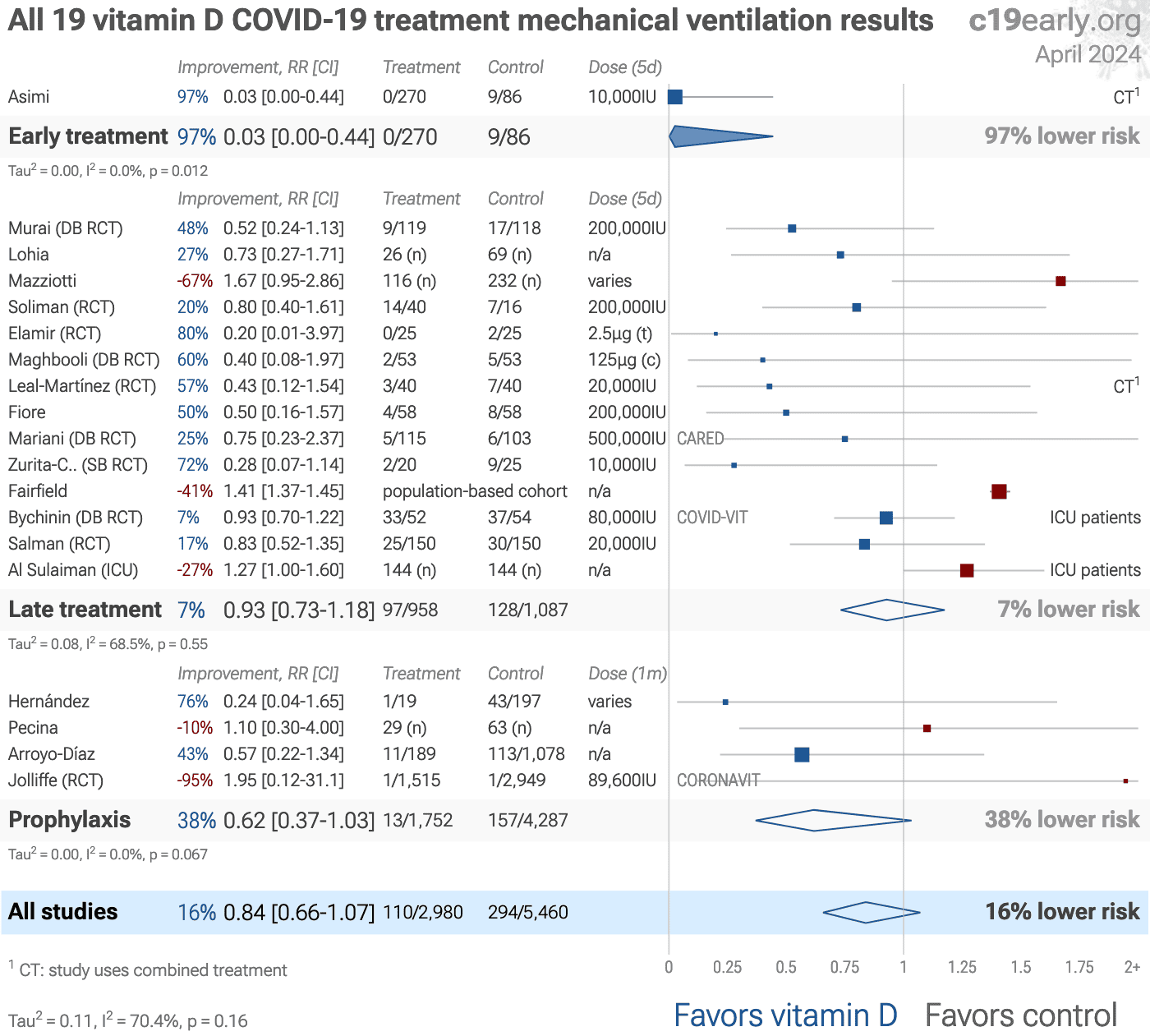
| VentilationVent. | 0.83 [0.65‑1.05] p = 0.12 | 22 | 8,720 |
| ICU admissionICU | 0.55 [0.43‑0.72] p < 0.0001**** | 33 | 40K |
| HospitalizationHosp. | 0.78 [0.70‑0.87] p < 0.0001**** | 27 | 80K |
| Recovery | 0.77 [0.69‑0.85] p < 0.0001**** | 15 | 1,359 |
| Cases | 0.82 [0.75‑0.90] p < 0.0001**** | 33 | 140K |
| Viral | 0.43 [0.27‑0.68] p = 0.00033*** | 6 | 510 |
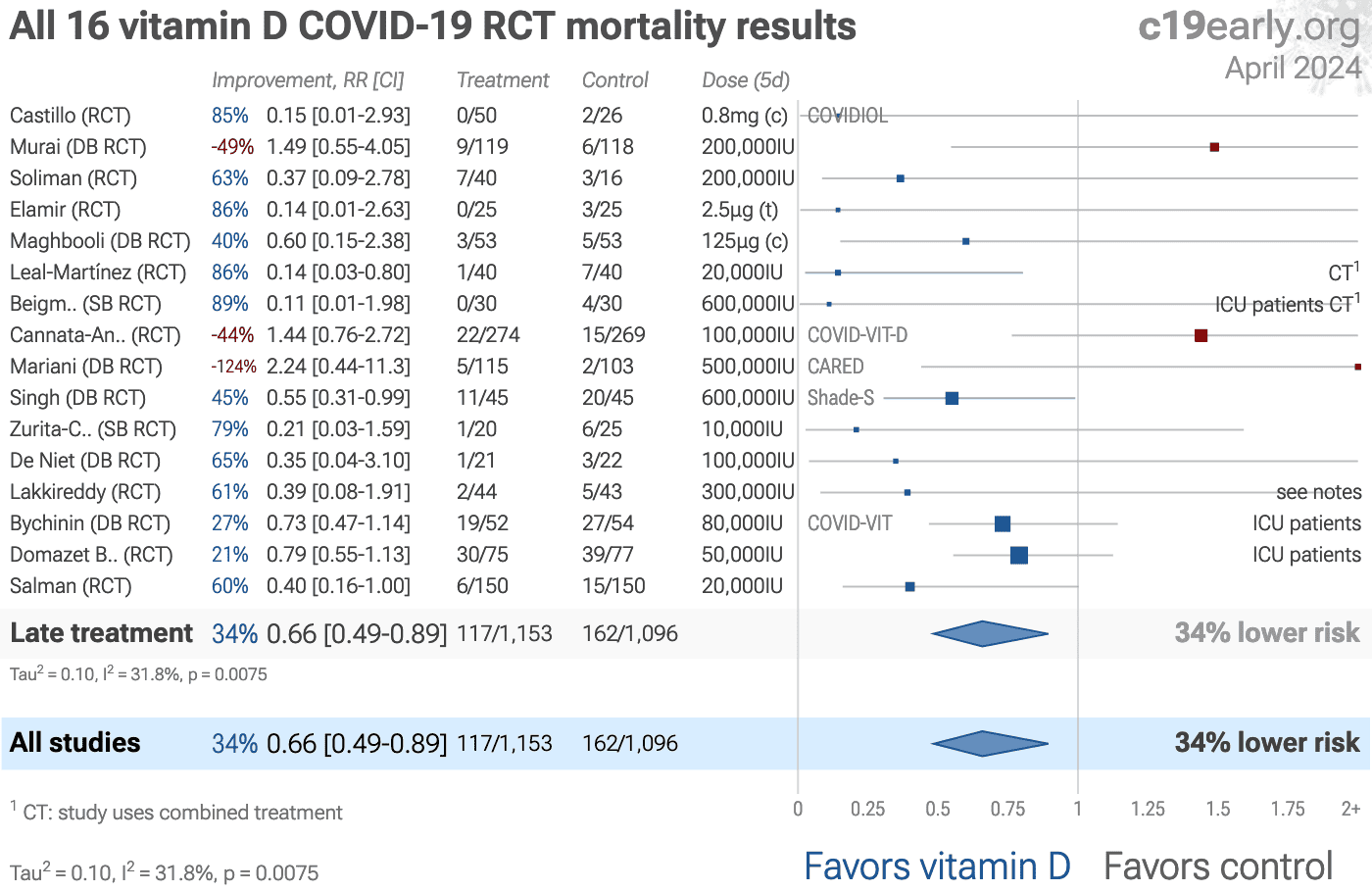
| RCT mortality | 0.62 [0.47‑0.81] p = 0.00041*** | 24 | 3,210 |
| RCT ventilationRCT vent. | 0.77 [0.60‑0.98] p = 0.031* | 12 | 5,762 |
| RCT ICU admissionRCT ICU | 0.69 [0.53‑0.90] p = 0.0055** | 17 | 30K |
| RCT hospitalizationRCT hosp. | 0.74 [0.64‑0.86] p < 0.0001**** | 12 | 40K |
| Sufficiency | 0.50 [0.47‑0.53] p < 0.0001**** | 232 | 410K |
| Early treatment | Late treatment | Prophylaxis | |
|---|---|---|---|
| All studies | 0.44 [0.30‑0.63]****0.44**** [0.30‑0.63] | 0.53 [0.45‑0.63]****0.53**** [0.45‑0.63] | 0.68 [0.61‑0.75]****0.68**** [0.61‑0.75] |
| Exc. late treatmentExc. late | 0.44 [0.30‑0.63]****0.44**** [0.30‑0.63] | 0.53 [0.45‑0.63]****0.53**** [0.45‑0.63] | |
| After exclusions | 0.37 [0.23‑0.60]****0.37**** [0.23‑0.60] | 0.40 [0.32‑0.50]****0.40**** [0.32‑0.50] | 0.70 [0.63‑0.77]****0.70**** [0.63‑0.77] |
| Peer-reviewedPeer-reviewed | 0.47 [0.33‑0.66]****0.47**** [0.33‑0.66] | 0.54 [0.45‑0.64]****0.54**** [0.45‑0.64] | 0.67 [0.60‑0.75]****0.67**** [0.60‑0.75] |
| RCTsRCTs | 0.69 [0.53‑0.90]**0.69** [0.53‑0.90] | 0.60 [0.47‑0.76]****0.60**** [0.47‑0.76] | 0.72 [0.56‑0.94]*0.72* [0.56‑0.94] |
| RCTs after exclusionsRCTs w/exc. | 0.65 [0.38‑1.10]0.65 [0.38‑1.10] | 0.51 [0.37‑0.70]****0.51**** [0.37‑0.70] | 0.72 [0.56‑0.94]*0.72* [0.56‑0.94] |
| Cholecalciferol | 0.44 [0.30‑0.63]****0.44**** [0.30‑0.63] | 0.57 [0.48‑0.68]****0.57**** [0.48‑0.68] | 0.68 [0.61‑0.76]****0.68**** [0.61‑0.76] |
| Calcifediol/calcitriolCalcifediol | 0.34 [0.22‑0.53]****0.34**** [0.22‑0.53] | 0.64 [0.46‑0.87]**0.64** [0.46‑0.87] |
|
| Mortality | 0.38 [0.23‑0.65]***0.38*** [0.23‑0.65] | 0.53 [0.44‑0.64]****0.53**** [0.44‑0.64] | 0.77 [0.66‑0.91]**0.77** [0.66‑0.91] |
| VentilationVent. | 0.03 [0.00‑0.44]*0.03* [0.00‑0.44] | 0.90 [0.71‑1.14]0.90 [0.71‑1.14] | 0.62 [0.37‑1.03]0.62 [0.37‑1.03] |
| ICU admissionICU | 0.13 [0.01‑2.43]0.13 [0.01‑2.43] | 0.56 [0.41‑0.75]***0.56*** [0.41‑0.75] | 0.54 [0.37‑0.78]**0.54** [0.37‑0.78] |
| HospitalizationHosp. | 0.10 [0.00‑5.53]0.10 [0.00‑5.53] | 0.75 [0.67‑0.85]****0.75**** [0.67‑0.85] | 0.87 [0.73‑1.04]0.87 [0.73‑1.04] |
| Recovery | 0.69 [0.51‑0.93]*0.69* [0.51‑0.93] | 0.76 [0.67‑0.87]****0.76**** [0.67‑0.87] | |
| Cases | 0.82 [0.75‑0.90]****0.82**** [0.75‑0.90] |
||
| Viral | 0.48 [0.30‑0.76]**0.48** [0.30‑0.76] | 0.42 [0.22‑0.82]*0.42* [0.22‑0.82] | |
| RCT mortality | 0.70 [0.36‑1.36]0.70 [0.36‑1.36] | 0.60 [0.45‑0.81]***0.60*** [0.45‑0.81] | |
| RCT ventilationRCT vent. | 0.75 [0.57‑0.97]*0.75* [0.57‑0.97] | 1.95 [0.12‑31.10]1.95 [0.12‑31.10] |
|
| RCT ICU admissionRCT ICU | 0.67 [0.51‑0.88]**0.67** [0.51‑0.88] | 1.00 [0.25‑4.01]1.00 [0.25‑4.01] |
|
| RCT hospitalizationRCT hosp. | 0.71 [0.62‑0.82]****0.71**** [0.62‑0.82] | 1.26 [0.83‑1.92]1.26 [0.83‑1.92] |
|
{kind=link}
Fig. 6. Results by treatment stage.
{kind=link}
Loading..
Loading..
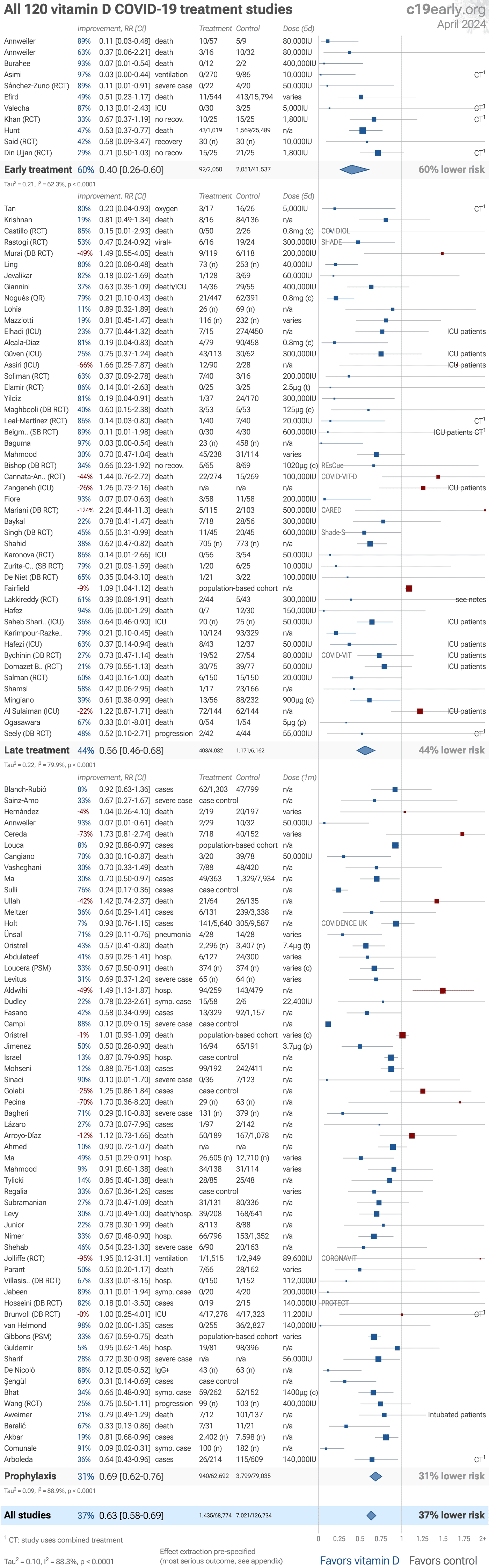
Fig. 7. Random-effects meta-analysis for all treatment studies.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Loading..
Fig. 13. Random-effects meta-analysis for treatment peer-reviewed studies.
Zeraatkar et al. analyze 356 COVID-19 trials, finding no significant
evidence that preprint results are inconsistent with peer-reviewed studies.
They also show extremely long peer-review delays, with a median of 6 months to
journal publication. A six month delay was equivalent to around 1.5 million
deaths during the first two years of the pandemic. Authors recommend using
preprint evidence, with appropriate checks for potential falsified data, which
provides higher certainty much earlier. Davidson et al. also showed no
important difference between meta-analysis results of preprints and
peer-reviewed publications for COVID-19, based on 37 meta-analyses including
114 trials.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
{kind=link}
Loading..
Fig. 14. Random-effects meta-analysis for sufficiency studies.
This plot pools studies with different effects, different vitamin D cutoff levels and measurement times, and studies may be within hospitalized patients, excluding the risk of hospitalization. However, the prevalence of positive effects is notable.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Fig. 15, 16, 17, 18, and 19
show forest plots for random-effects meta-analysis of
all Randomized Controlled Trials, RCTs after exclusions, RCT mortality results, RCT ICU results, and RCT hospitalization results.
{kind=link}
Loading..
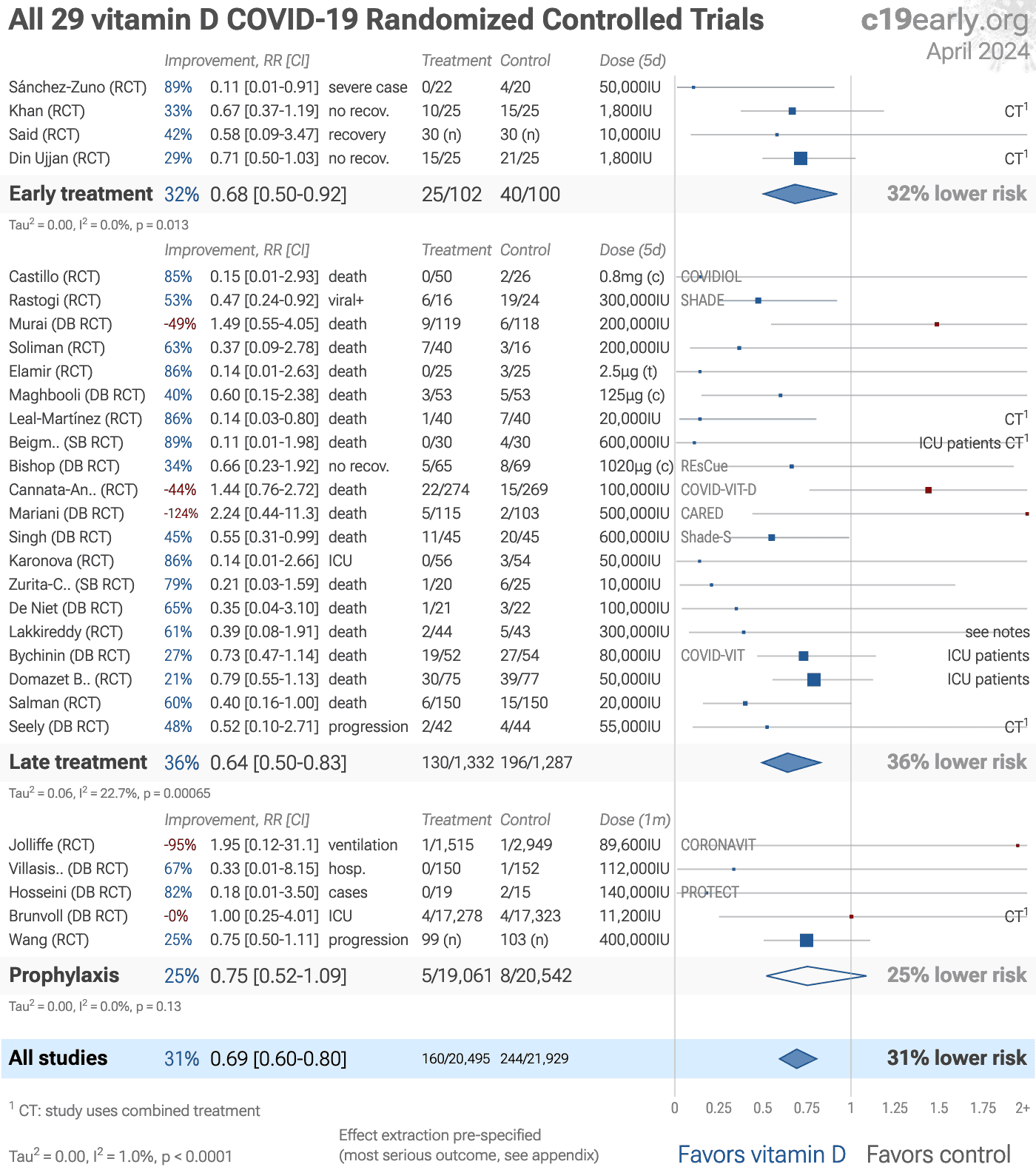
Fig. 15. Random-effects meta-analysis for all Randomized Controlled Trials.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
RCTs help to make study groups more similar and can provide a higher level of
evidence, however they are subject to many biases173, and
analysis of double-blind RCTs has identified extreme levels of bias174.
For COVID-19, the overhead may delay treatment, dramatically compromising
efficacy; they may encourage monotherapy for simplicity at the cost of
efficacy which may rely on combined or synergistic effects; the participants
that sign up may not reflect real world usage or the population that benefits
most in terms of age, comorbidities, severity of illness, or other factors;
standard of care may be compromised and unable to evolve quickly based on
emerging research for new diseases; errors may be made in randomization and
medication delivery; and investigators may have hidden agendas or vested
interests influencing design, operation, analysis, reporting, and the
potential for fraud. All of these biases have been observed with COVID-19
RCTs. There is no guarantee that a specific RCT provides a higher level of
evidence.
RCTs are expensive and many RCTs are funded
by pharmaceutical companies or other organizations with conflicts of interest, for example
governments that previously denied treatment with the study drug.
For COVID-19, this creates an incentive to show efficacy for
patented commercial products, and an incentive to show a lack of efficacy for
inexpensive treatments. The bias is expected to be significant, for example
Als-Nielsen et al. analyzed 370 RCTs from Cochrane reviews, showing that
trials funded by for-profit organizations were 5 times more likely to
recommend the experimental drug compared with those funded by nonprofit
organizations. Bekelman et al. and Lundh et al. show that
industry-sponsored studies are more likely to be favorable.
For COVID-19, some major philanthropic organizations are
largely funded by investments with extreme conflicts of interest for and
against specific COVID-19 interventions.
High quality RCTs for novel acute diseases are more challenging, with
increased ethical issues due to the urgency of treatment, increased risk due
to enrollment delays, and more difficult design with a rapidly evolving
evidence base. For COVID-19, the most common site of initial infection is the
upper respiratory tract. Immediate treatment is likely to be most successful
and may prevent or slow progression to other parts of the body. For a
non-prophylaxis RCT, it makes sense to provide treatment in advance and
instruct patients to use it immediately on symptoms, just as some governments
have done by providing medication kits in advance. Unfortunately, no RCTs have
been done in this way. Every treatment RCT to date involves delayed treatment.
Among the 226 treatments we have analyzed,
67% of RCTs involve very late treatment 5+ days after
onset. No non-prophylaxis COVID-19 RCTs match the potential real-world use of
early treatments. They may more accurately represent results for treatments
that require visiting a medical facility, e.g., those requiring intravenous
administration.
RCTs have a bias against finding an effect for interventions
that are widely available—patients that believe they need the
intervention are more likely to decline participation and take the
intervention. RCTs for vitamin D are more likely to enroll low-risk
participants that do not need treatment to recover, making the results less
applicable to clinical practice. This bias is likely to be greater for widely
known treatments, and may be greater when the risk of a serious outcome is
overstated. This bias does not apply to the typical pharmaceutical trial of a
new drug that is otherwise unavailable.
{kind=link}
Evidence shows that observational studies
can also provide reliable results. Concato et al. found that well-designed
observational studies do not systematically overestimate the magnitude of the
effects of treatment compared to RCTs. Anglemyer et al. analyzed reviews
comparing RCTs to observational studies and found little evidence for
significant differences in effect estimates.
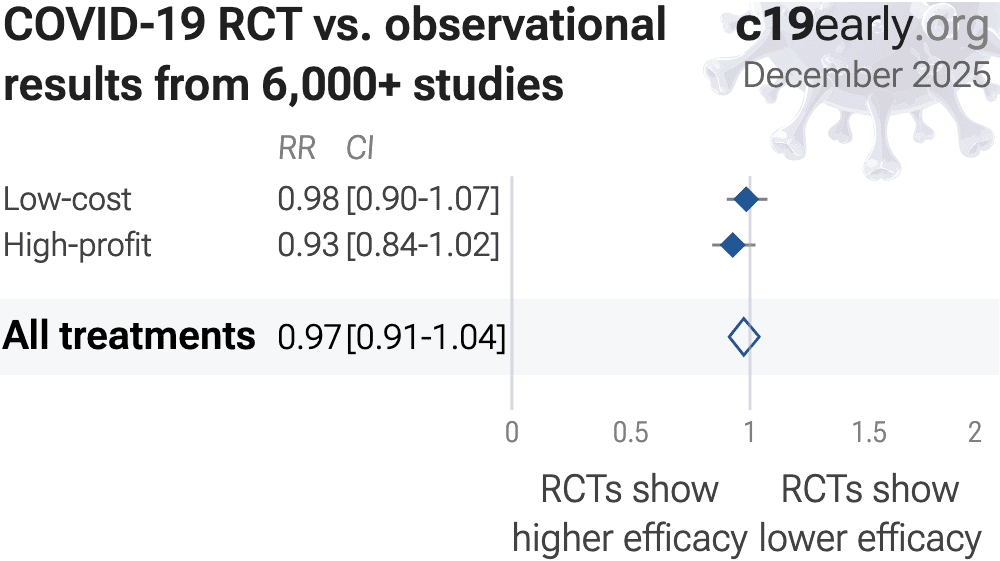
We performed a similar analysis across the 226 treatments
we cover, showing no significant difference in the results of RCTs compared to
observational studies, RR 0.97 [0.91‑1.03]155. Similar results are found for all low-cost treatments, RR
0.98 [0.90‑1.06]. High-cost treatments
show a non-significant trend towards RCTs showing greater efficacy,
RR 0.92 [0.84‑1.02].
Details can be found in the
supplementary data.
Lee et al. showed that only 14% of the guidelines of the Infectious
Diseases Society of America were based on RCTs. Evaluation of studies relies
on an understanding of the study and potential biases. Limitations in an RCT
can outweigh the benefits, for example excessive dosages, excessive treatment
delays, or remote survey bias may have a greater effect on results. Ethical
issues may also prevent running RCTs for known effective treatments. For more
on issues with RCTs see182,183.
Concato et al. report a paradoxical finding—RCT results had higher
variability, and only RCTs were found to sometimes report significant results the opposite
of the overall result. The same trend is seen for the most popular (most politicized)
COVID-19 treatments including vitamin D—considering all statistically significant results reported in
studies, RCTs are slightly more likely to report a result in the opposite direction. In
other words, for these COVID-19 treatments and for the topics covered by Concato et al., assuming causality from a single study is more likely to result in an incorrect conclusion for
RCTs.
Increased risk of inconsistent results for RCTs suggests higher prevalence of
bias, which may arise due to many issues including design bias, conflicts of interest,
treatment differences by physicians aware of allocation, attrition bias, ascertainment
bias, randomization failures, errors, or fraud.
Currently, 59 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. Of these, 54% have been confirmed in RCTs, with a mean delay of 7.8 months (62% with 8.7 months delay for low-cost treatments). The remaining treatments either have no RCTs, or the point estimate is consistent.
Neither observational studies nor RCTs prove causation—any study can be
flawed or fraudulent. We need much more, for example a combination of results from many
independent teams, detailed understanding of each study, knowledge of conflicts/team
reliability, dose-response relationships, delay-response relationships, logical results across outcomes, or details consistent with preclinical expectations.
All studies must be evaluated individually. RCTs for a
given medication and disease may be more reliable, however they may also be
less reliable. For off-patent medications, very high conflict of interest
trials may be more likely to be RCTs, and more likely to be large trials that
dominate meta-analyses.
NIH provides an analysis of vitamin D for
COVID-19184,
concluding that there is insufficient evidence to recommend for or against use.
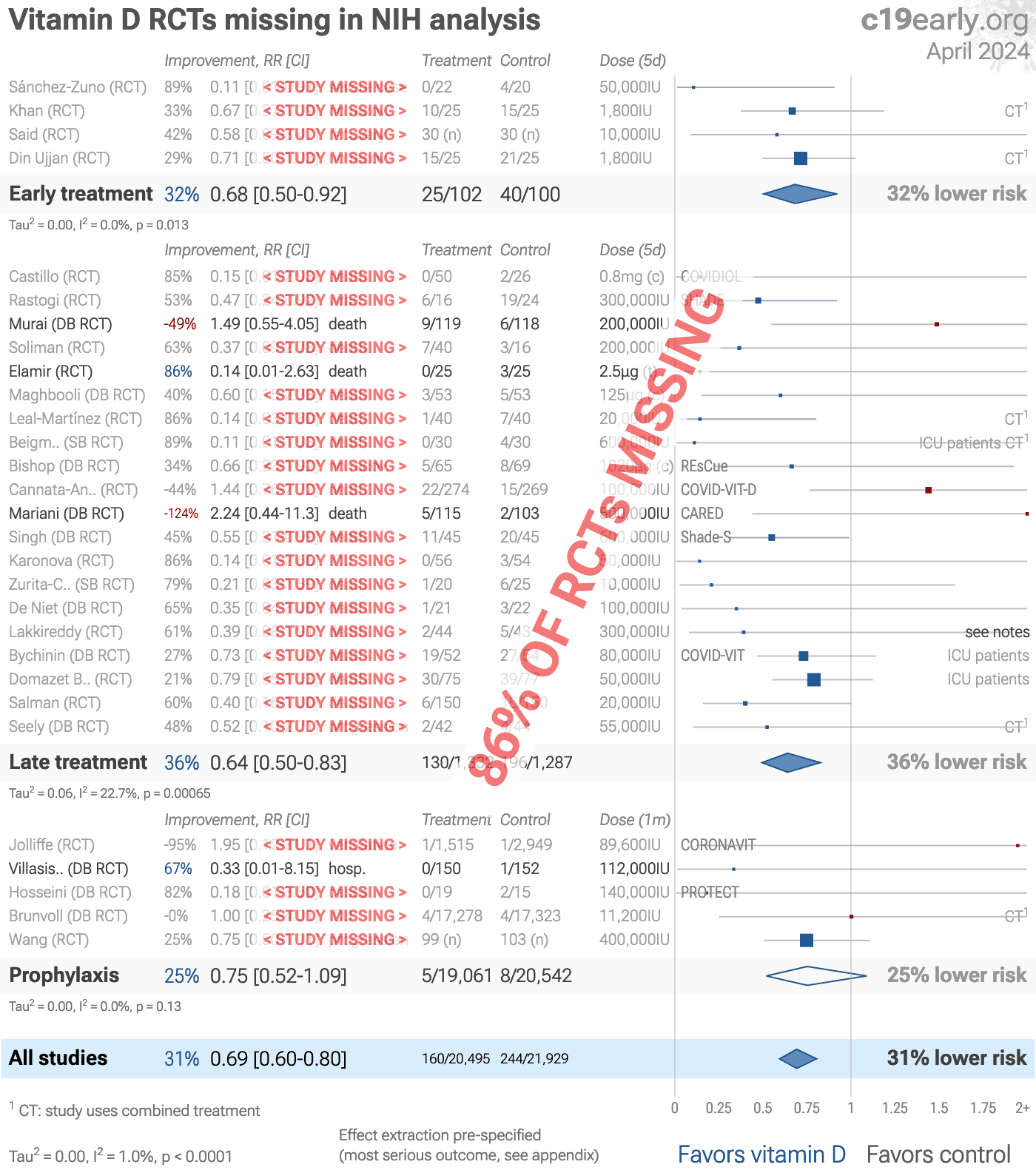
However, they appear to have not examined the majority of the evidence.
For example, considering RCTs providing clinical
results for COVID-19 and vitamin D, they reference only185-188, and appear not to know about 37 other RCTs189-225
as shown in Fig. 21.
Notably, the NIH selection does not correspond to the most relevant and
highest quality studies, for example including Murai et al., which studies
very late treatment (10 days from symptom onset, with 90% on oxygen at
baseline) using a bolus dose of cholecalciferol—a trifecta of poor design and low relevance compared to recommended use:
early treatment is better, continuous dosing is more effective than bolus doses, and calcifediol,
calcitriol, or analogs avoid very long delays in conversion.
They include none of the early treatment
RCTs.
Authors reference only one of the 97 observational studies.
For COVID-19, observational study results do not systematically
differ from RCTs, RR 0.97 [0.91‑1.03]
across 226 treatments178.
{kind=link}
Fig. 21. Analysis by NIH is missing 37 RCTs.
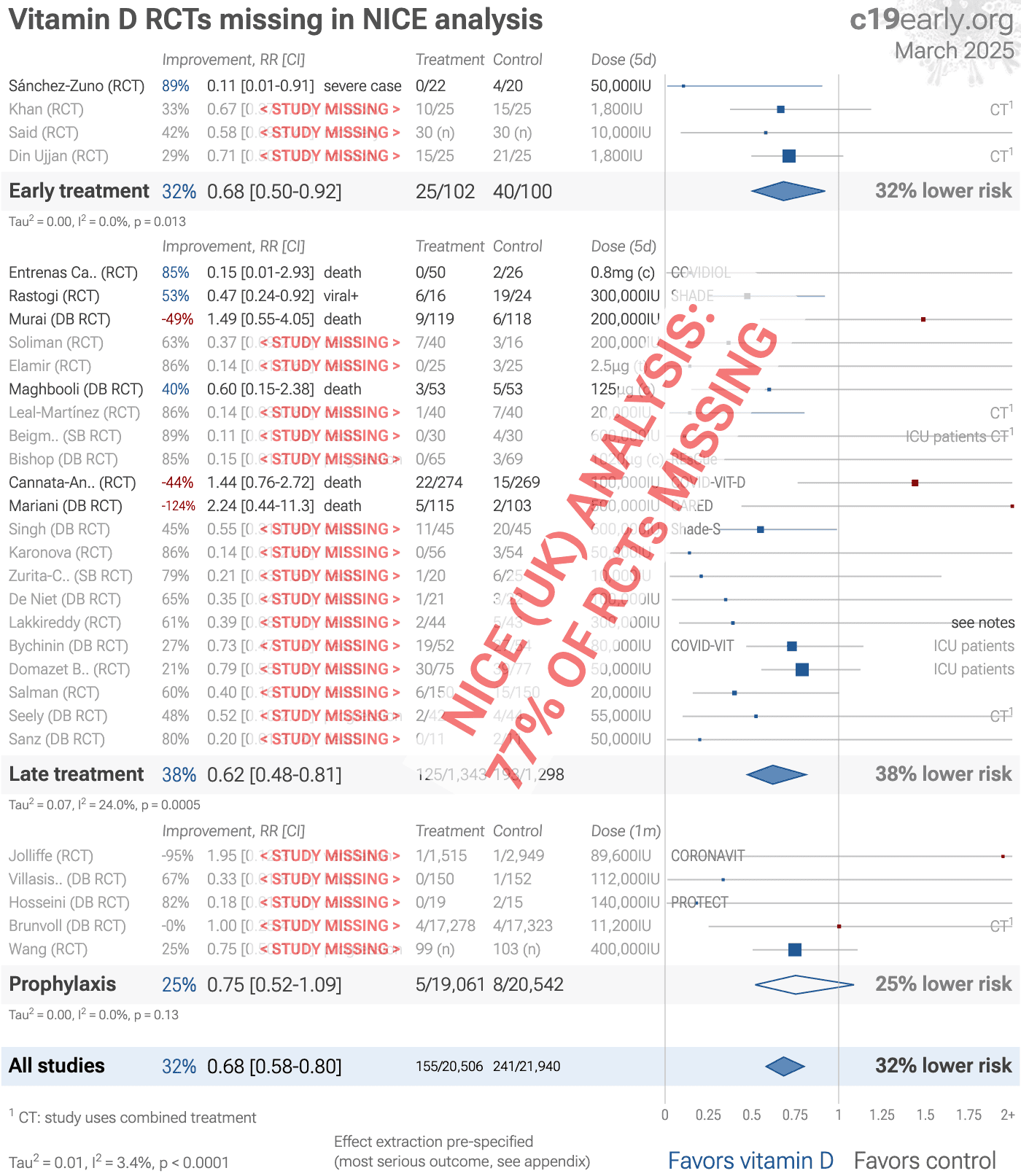
NICE (UK) provides an analysis of vitamin D for
COVID-19226,227,
recommending against use.
However, they appear to have not examined the majority of the evidence.
For example, considering RCTs providing clinical
results for COVID-19 and vitamin D, they reference only186,187,195,200,210,212,216 , and appear not to know about 34 other RCTs185,188-194,196-199,201-209,211,213-215,217-225
as shown in Fig. 22.
Authors do not reference any of the 97 observational studies.
For COVID-19, observational study results do not systematically
differ from RCTs, RR 0.97 [0.91‑1.03]
across 226 treatments178.
{kind=link}
Fig. 22. Analysis by NICE is missing 34 RCTs.
Fig. 23 shows the results for studies testing high vs. low doses.
Results are comparable to studies with a control group—there is no significant
difference in the main results when including or excluding these studies.
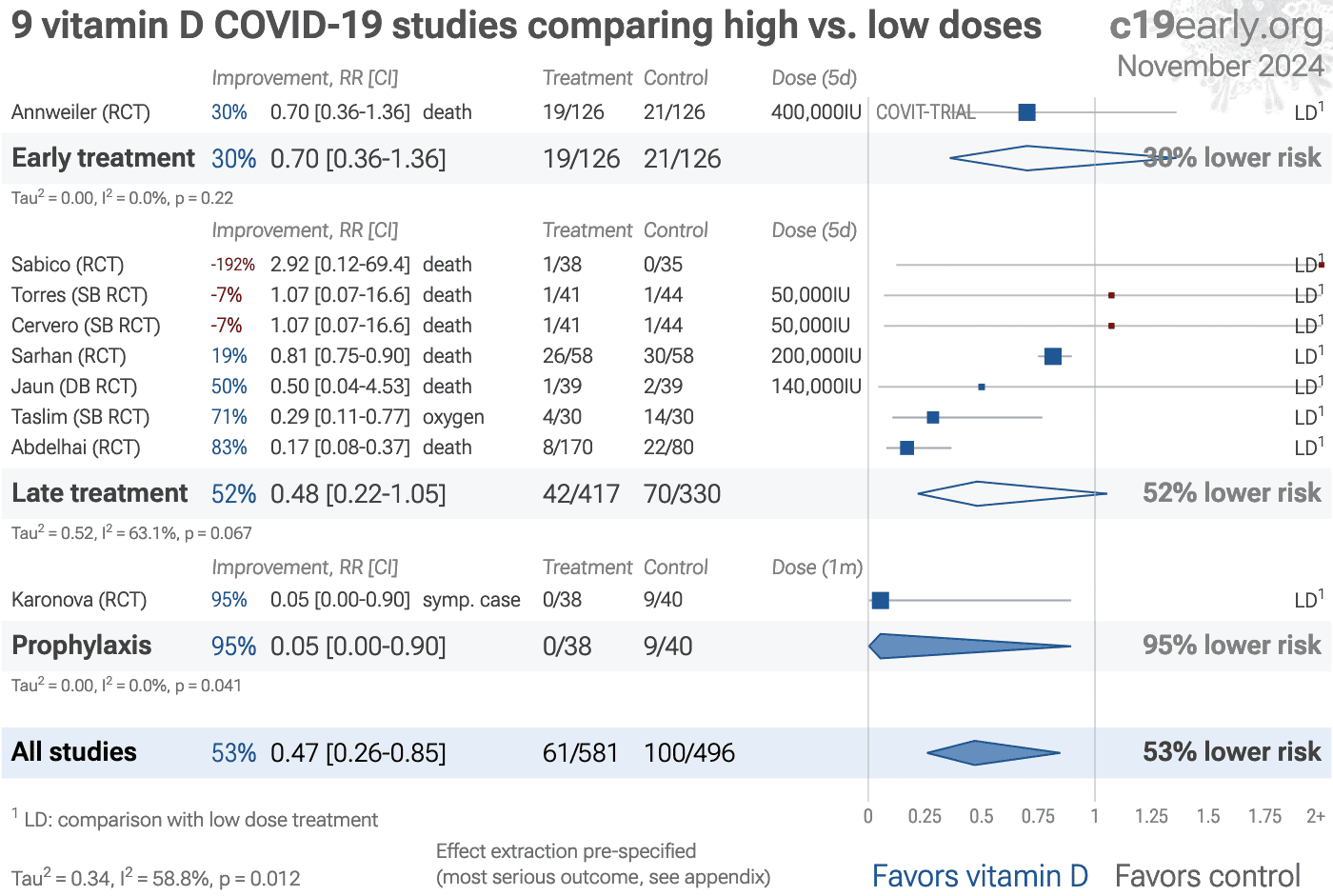{kind=link}
Loading..
Fig. 23. Random-effects meta-analysis for high vs. low-dose treatment studies (no control group), showing improved results with higher doses.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
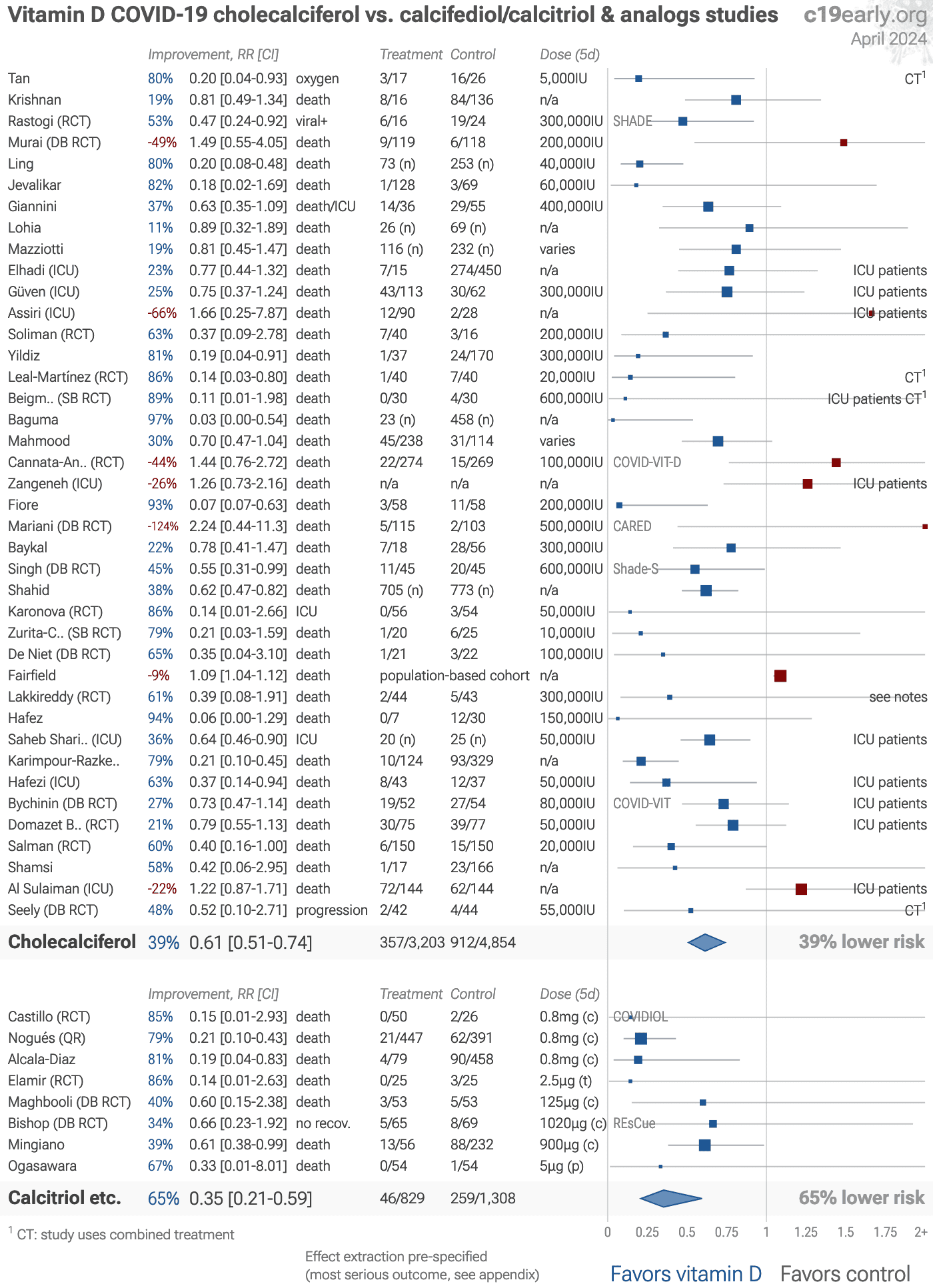
Fig. 24 shows the results for studies
using cholecalciferol and studies using calcifediol/calcitriol and analogs.
This shows late treatment studies as there are currently no early treatment
studies using calcifediol/calcitriol and analogs.
Calcifediol, calcitriol and analogs show significantly higher efficacy,
p = 0.033,
as expected given the long conversion delays with cholecalciferol. However they were rarely
used, despite wide availability.
{kind=link}
Loading..
Fig. 24. Random-effects meta-analysis for cholecalciferol vs. calcifediol/calcitriol and analogs, showing improved results with calcifediol/calcitriol and analogs.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
Pharmacokinetics and the potential side
effects of high bolus doses suggest that ongoing treatment spread over time is more
appropriate. One potential advantage of single dose treatment is patient compliance,
however this does not apply to COVID-19 trials with ongoing medical care.
Research has shown that lower dose regular treatment with
vitamin D is more effective than intermittent high-dose bolus treatment for
various conditions, including rickets and acute respiratory
infections89,228,229 . The biological mechanisms
supporting these
findings involve the induction of enzymes such as 24-hydroxylase and
fibroblast growth factor 23 (FGF23) by high-dose bolus treatments. These
enzymes play roles in inactivating vitamin D, which can paradoxically reduce
levels of activated vitamin D and suppress its activation for extended periods
post-dosage. Evidence indicates that 24-hydroxylase activity may remain
elevated for several weeks following a bolus dose, leading to reduced levels
of the activated form of vitamin D. Additionally, FGF23 levels can increase
for at least three months after a large bolus dose, which also contributes to
the suppression of vitamin D activation228.
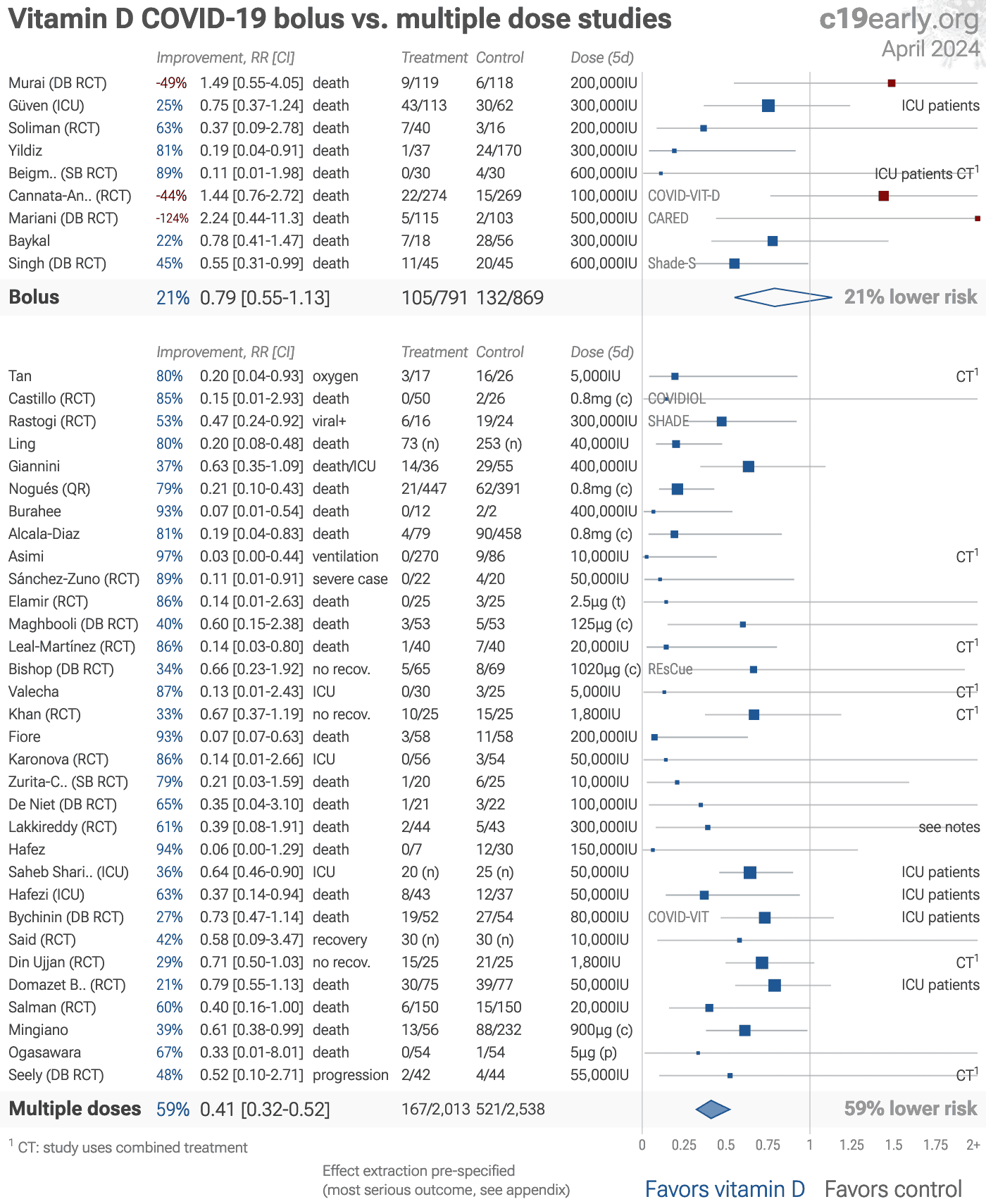
Fig. 25 shows the results for studies using a single bolus dose
≥100,000IU and for studies where treatment continues with multiple doses. Significantly
higher efficacy is seen with multiple doses, p = 0.000035. This analysis is a simplification - for both bolus doses and ongoing
treatment, individual trials may use doses that are significantly lower or higher than
optimal.
Yang (B) et al. also show improved results with multiple dose
treatment.
{kind=link}
Loading..
Fig. 25. Random-effects meta-analysis for bolus vs. multiple dose studies, showing improved results with multiple doses.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
To avoid bias in the selection of
studies, we include all studies in the main analysis, with the exception of
Espitia-Hernandez. This study uses a combined protocol with another medication
that shows high effectiveness when used alone. Authors report on viral clearance, showing
100% clearance with treatment and 0% for the control group. Based on the known mechanisms
of action, the combined medication is likely to contribute more to the improvement.
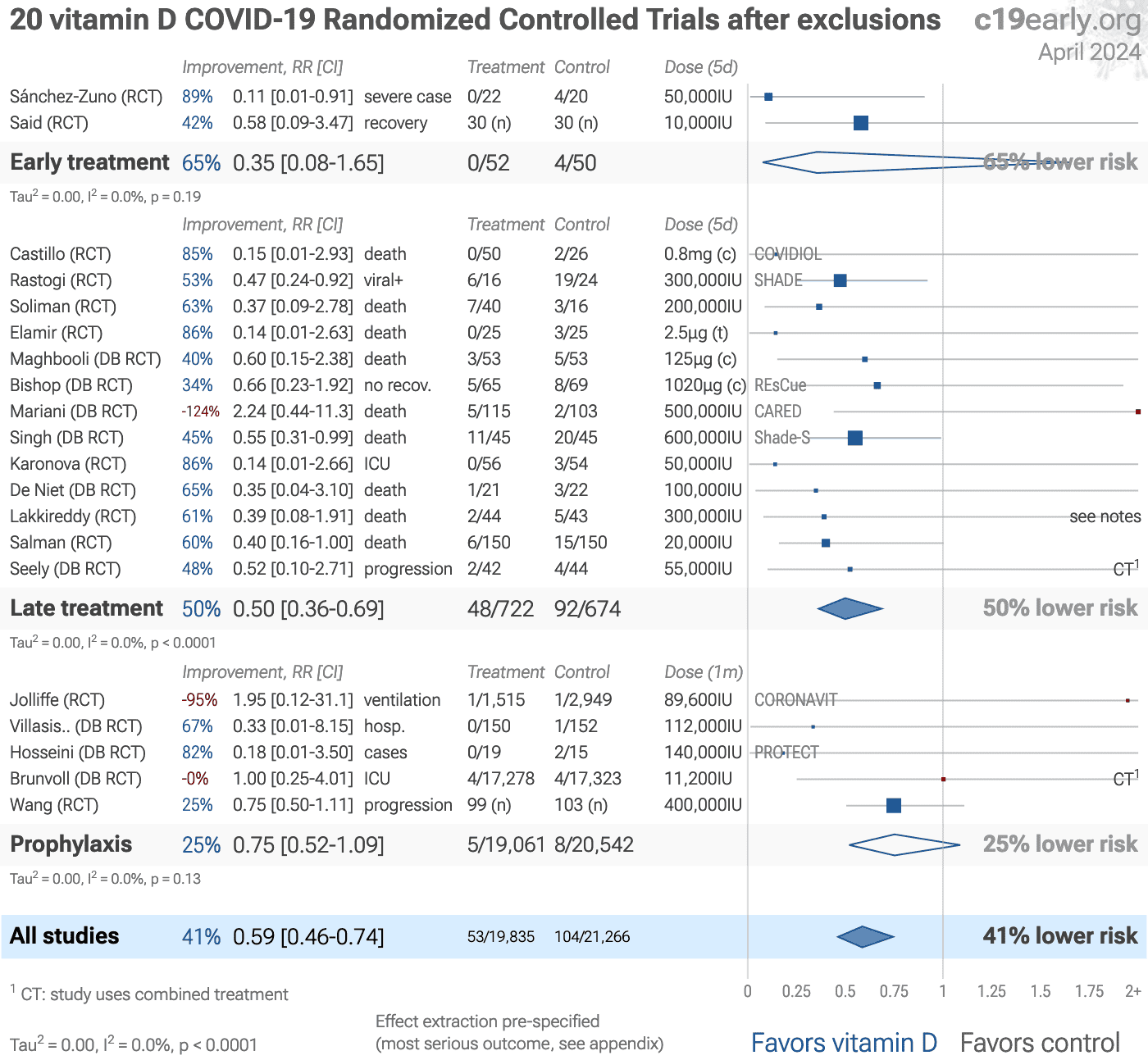
Here we show the results after excluding studies with critical
issues.
Murai is a very late stage study (mean 10 days from
symptom onset, with 90% on oxygen at baseline), with poorly matched arms in
terms of gender, ethnicity, hypertension, diabetes, and baseline ventilation,
all of which favor the control group. Further, this study uses
cholecalciferol, which may be especially poorly suited for such a late stage.
Mariani, Cannata-Andía are also very late stage studies using
cholecalciferol.
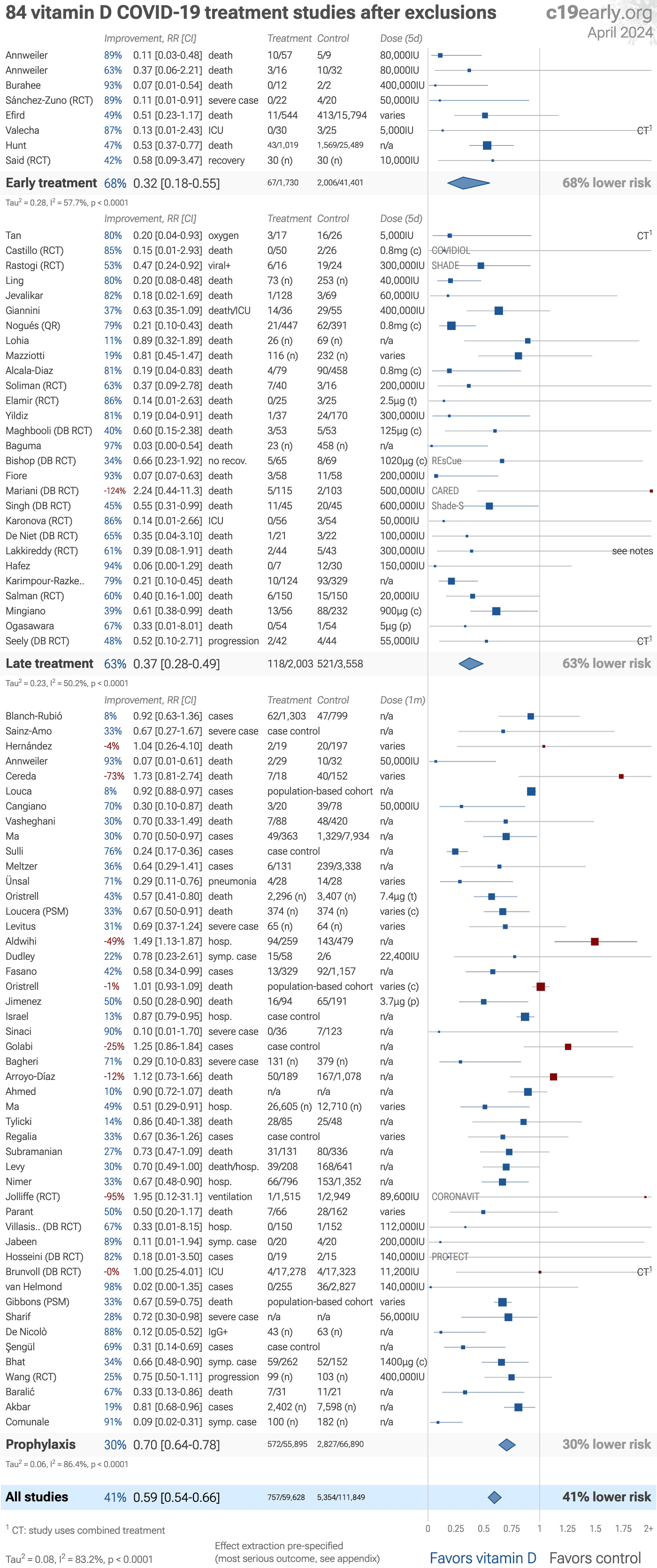
The studies excluded are as follows, and the resulting forest
plot is shown in Fig. 26.
Abdulateef, unadjusted results with no group details.
Al Sulaiman, very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Arboleda, unadjusted results with no group details.
Asimi, excessive unadjusted differences between groups.
Aweimer, unadjusted results with no group details.
Baykal, unadjusted results with no group details; significant confounding by time possible due to separation of groups in different time periods.
Beigmohammadi, very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Bychinin, very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Campi, significant unadjusted differences between groups.
Cannata-Andía, very late stage study using cholecalciferol instead of calcifediol or calcitriol.
di Filippo (B), potentially significant confounding by treatment propensity.
Din Ujjan, combined treatments may contribute significantly to the effect seen; unadjusted differences between groups.
Domazet Bugarin, very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Elhadi, unadjusted results with no group details.
Fairfield, substantial unadjusted confounding by indication likely.
Guldemir, unadjusted results with no group details.
Güven, very late stage, ICU patients.
Hafezi, very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Holt, significant unadjusted confounding possible.
Junior, unadjusted results with no group details.
Khan, based on dosages and previous research, combined treatments may contribute more to the effect seen.
Krishnan, unadjusted results with no group details.
Leal-Martínez, combined treatments may contribute more to the effect seen.
Lázaro, very few events; unadjusted results with no group details; minimal details provided.
Mahmood, unadjusted results with no group details; substantial unadjusted confounding by indication likely.
Mahmood, unadjusted results with no group details; substantial unadjusted confounding by indication likely.
Mohseni, unadjusted results with no group details.
Murai, very late stage, >50% on oxygen/ventilation at baseline; very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Pecina, unadjusted results with no group details.
Saheb Sharif-Askari (B), very late stage study using cholecalciferol instead of calcifediol or calcitriol.
Shahid, minimal details provided.
Shamsi, unadjusted results with no group details.
Shehab, unadjusted results with no group details.
Ullah, significant unadjusted confounding possible.
Zangeneh, data issues pending author response.
Zurita-Cruz, randomization resulted in significant baseline differences that were not adjusted for.
{kind=link}
Loading..
Fig. 26. Random-effects meta-analysis for treatment studies after exclusions.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first five days for treatment, and the monthly dose for prophylaxis.
Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p).
For details of effect extraction and full dosage information see the appendix.
Vitamin D may not have a direct antiviral effect;
rather, any benefits are hypothesized to stem from improving immune system function
(host-directed efficacy). For such immunomodulatory treatments, we may expect a gradient of efficacy across outcomes, with minimal impact on preventing
initial infection (PCR+ cases), but increasing efficacy as the disease progresses to more
severe stages.
For vitamin D, random-effects meta-regression shows a significant trend with
increasing efficacy for more severe outcomes. For every one-step increase in severity
(cases → hospitalization → critical outcomes: ICU, ventilation, and mortality),
meta-regression shows that the Risk Ratio decreases by a factor of
1.10 (slope β = -0.10
[-0.18 to -0.01]; p = 0.031). In other words, the protective effect becomes stronger as
the outcome becomes more critical.
The trend across outcomes is consistent with a host-directed
immunomodulatory mechanism rather than a direct antiviral effect.
This reinforces the reliability of the overall finding that vitamin D
reduces risk for COVID-19.
If the observed efficacy was due to a systematic bias increasing the efficacy of outcomes,
it would not be expected to create a trend across outcomes that matches the biological
mechanism.
With 138 studies for vitamin D, we can analyze interactions and trends across studies and groups. Significant
interactions that match the biological mechanisms provide further confirmation of
efficacy.
We find significant interactions for: efficacy gradient across outcomes (p = 0.031), calcitriol/calcifediol vs. cholecalciferol (p = 0.033), continuous vs. bolus treatment (p = 0.000035), and acute treatment vs. chronic prophylaxis (p = 0.0042).
This reinforces the reliability of the overall finding that vitamin D
reduces risk for COVID-19.
If the observed efficacy was due to a systematic bias increasing efficacy in results, we
would not expect analysis across studies to find these significant interactions
that match the biological mechanisms.
These results would not happen without a real treatment effect - it would require an
unrealistic conspiracy where many well-respected and independent teams in many countries
conspire to harm humanity and coordinate fraudulent results.
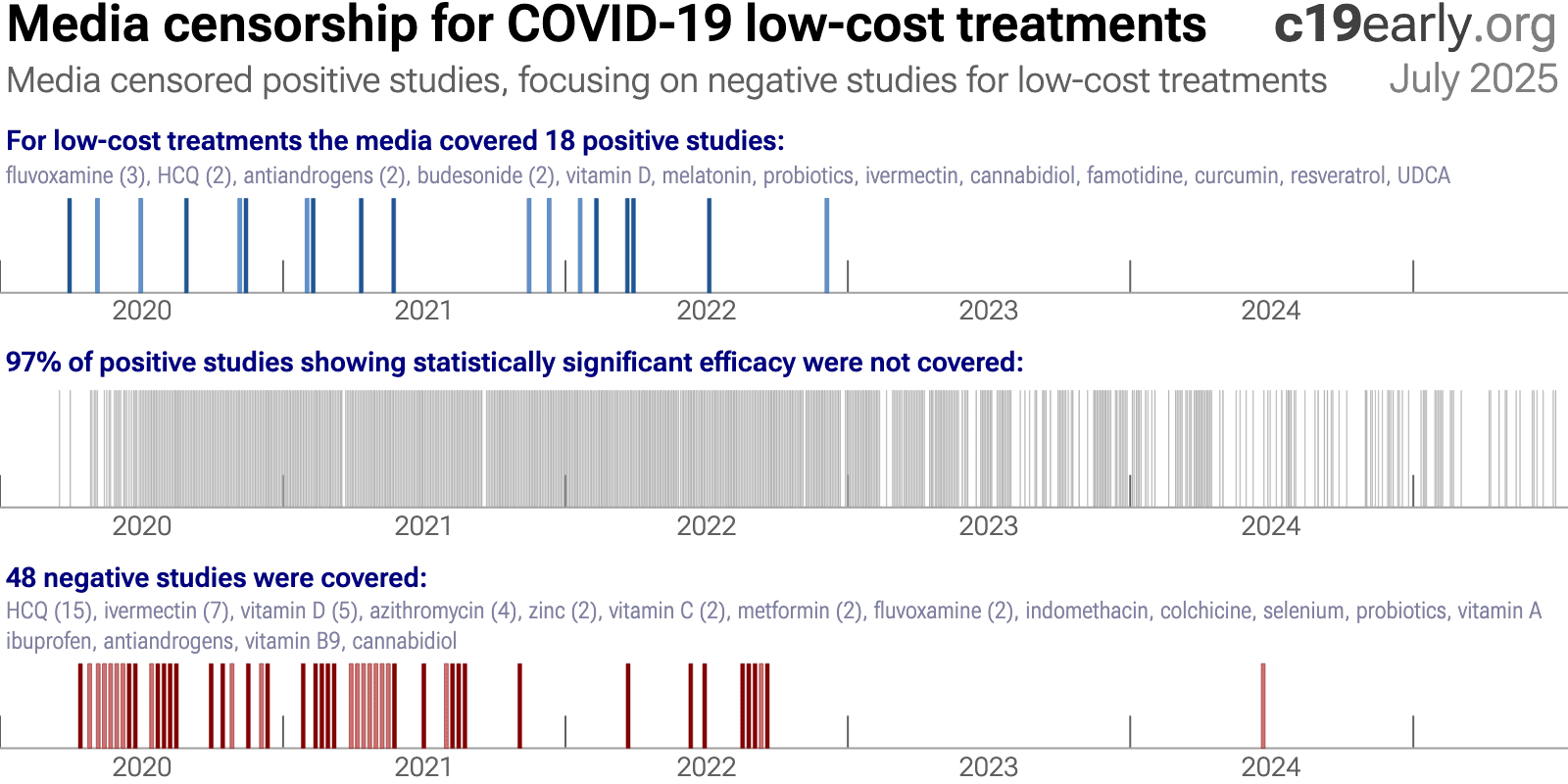
Low-cost treatments were subject to bias and censorship during the pandemic.
Scientific bias is seen in the design, analysis, presentation, and selective
reporting of studies, which often favored negative results. A similar bias is seen in the media
coverage for low-cost treatments.
While broadly seen, bias was particularly notable for ivermectin and hydroxychloroquine, e.g., Scott Alexander noted that "if you say anything in favor of ivermectin you will be cast out of civilization and thrown into the circle of social hell reserved for Klan members and 1/6 insurrectionists. All the health officials in the world will shout 'horse dewormer!' at you and compare you to Josef Mengele."151.
We analyze media coverage for the 226 treatments we cover using
Altmetric257, which reports the number of ~12,000 tracked news outlets that covered each study258. Studies are considered to have received significant media coverage if they were covered by at least 0.5% of the tracked news outlets.
Fig. 27 and 28 show the bias toward negative results for low-cost treatments, in contrast to the opposite bias for high-profit treatments.
Fig. 29 shows the bias toward coverage of negative results for vitamin D.
This may result in widespread incorrect perceptions on the relative efficacy of high-profit and low-cost treatments. The impact is significant—increased cost limits the use of high-profit
treatments and treatment equity, and high-profit treatments were also more difficult to access, especially for earlier treatment which improves efficacy and minimizes community transmission.
{kind=link}
Fig. 27. Mainstream media was biased against positive results for low-cost treatments.
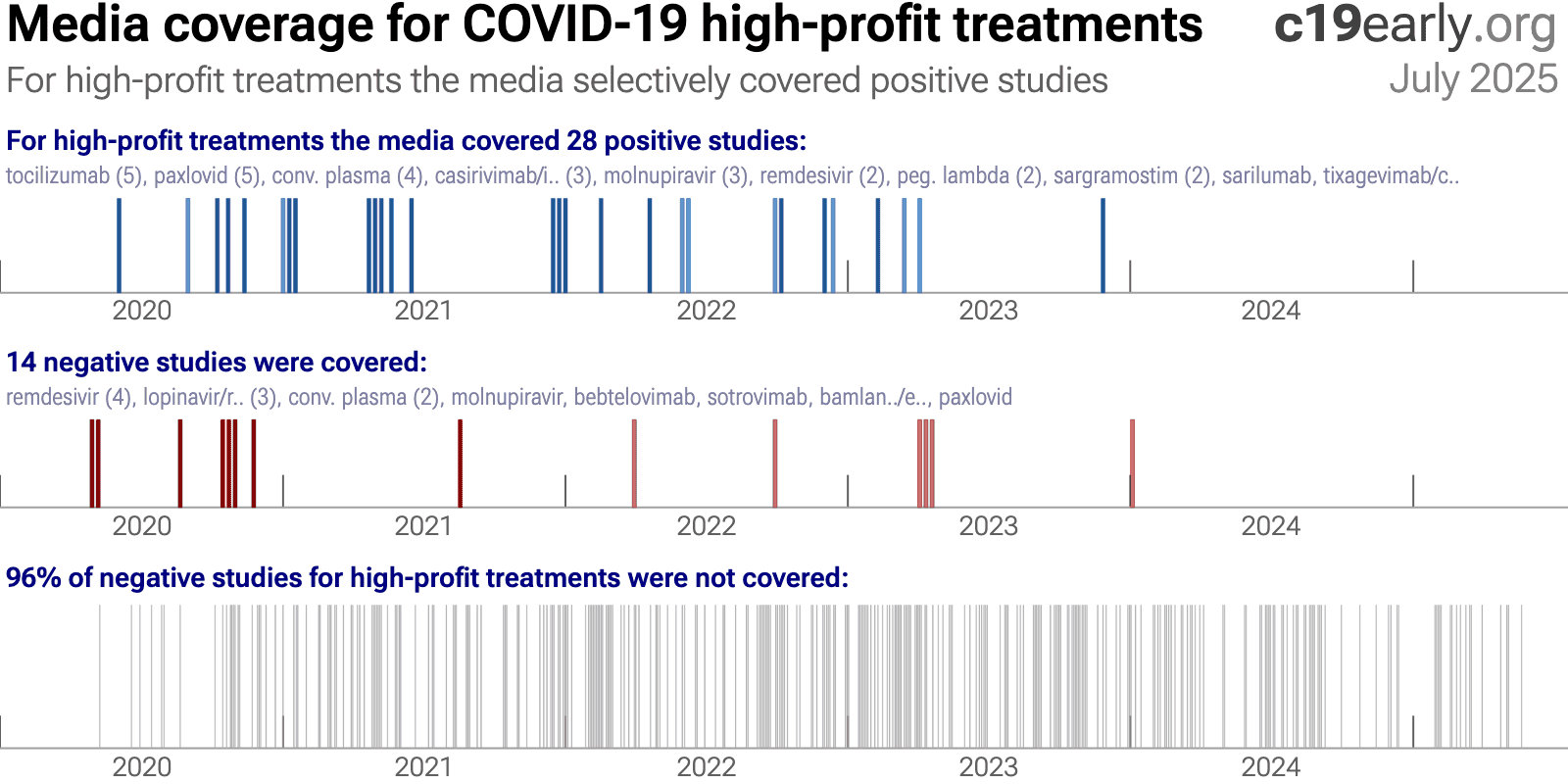{kind=link}
Fig. 28. In contrast to the results for low-cost treatments, mainstream media was biased towards positive results for high-cost treatments.
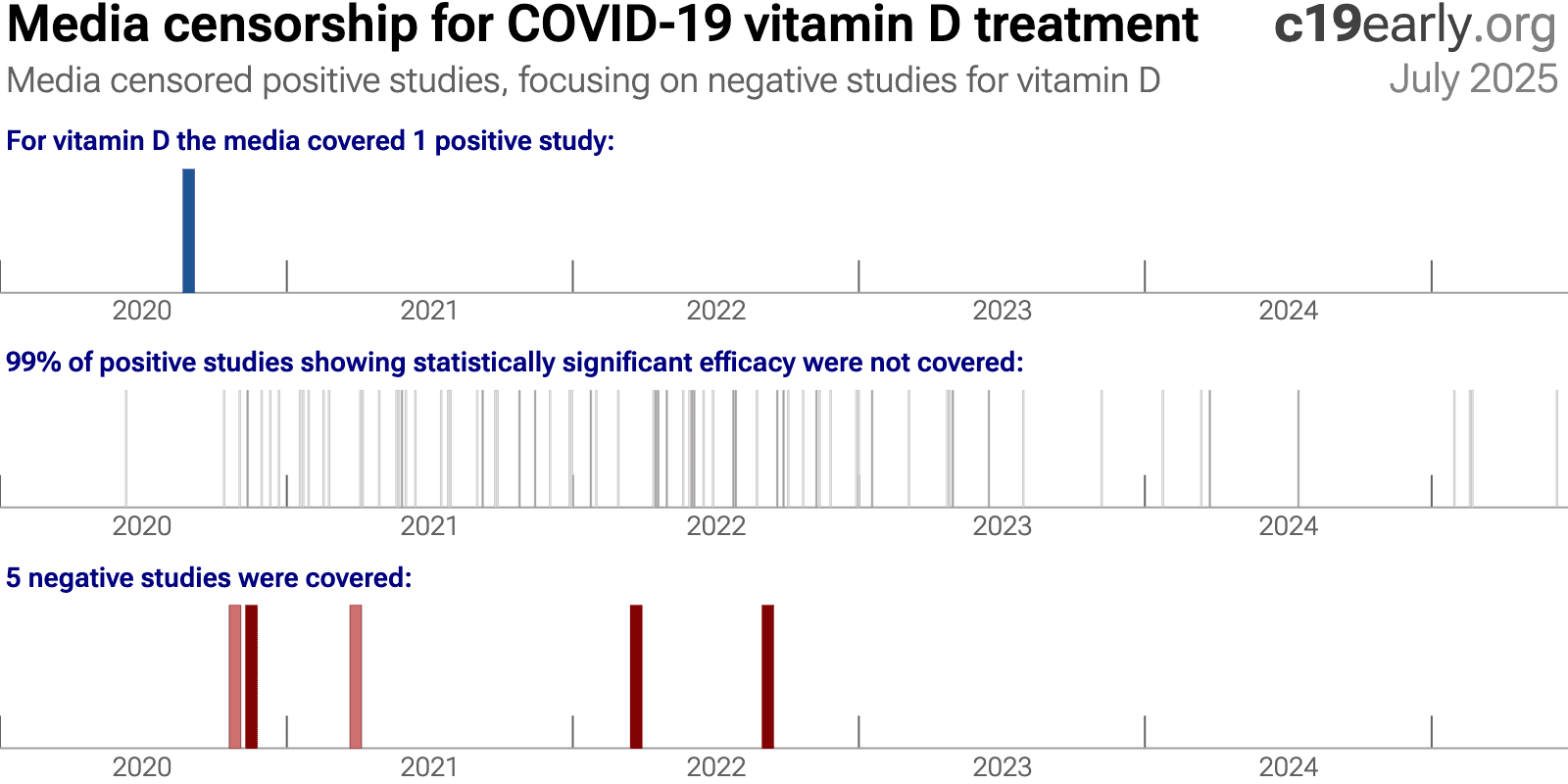{kind=link}
Fig. 29. Mainstream media was biased against positive results for vitamin D.
A combination of factors may have led to the media's suppression of low-cost treatments:
•
Politicization
led to a media environment where coverage was often framed to support a political
narrative rather than to provide objective scientific information. As Scott Alexander
said: "if you say anything in favor of ivermectin you will be cast out
of civilization and thrown into the circle of social hell reserved for Klan members and
1/6 insurrectionists. All the health officials in the world will shout 'horse dewormer!'
at you and compare you to Josef Mengele."
There was strong social pressure to
discredit low-cost treatments.•
Censorship
of
information conflicting with selected authorities. For example, individuals and
organizations presenting conflicting science were often banned on Twitter and
YouTube.•
FDA requires "no
adequate, approved, and available alternatives"
in order to grant an EUA for
novel high-profit interventions, creating a strong incentive for authorities to ignore or
downplay existing low-cost treatments.•
Regulatory
capture
biases authorities towards high-profit interventions.•
Authorities ignored
most evidence for low-cost treatments
, for example the NIH references only 2% of
studies in delayed, rarely-updated, biased commentaries with no quantitive analysis.•
Media coverage of
science is often not very accurate
, e.g., misunderstanding confounding issues. For
example the media widely considered the RECOVERY HCQ RCT to be conclusive on efficacy, but
very late treatment of late stage patients (mostly on oxygen already) with an excessive
toxic dose (shown dangerous in a dose comparison RCT) provides no information on the
recommended early/prophylactic treatment. With difficulting in understanding basic
confounders like treatment delay and dose, the media may favor deferring to authorities.
Many studies for low-cost treatments require greater expertise to analyze. Relatively few
journalists have a strong ability to analyze clinical trials and are outnumbered by the
rest.•
Substantial funding
from pharmaceutical advertising
biases editorial decisions towards high-profit
interventions.•
PR power
-
companies/teams with strong PR presence are favored in the media, which correlates with
high-profit and high conflict of interest studies.•
The media was very
negative in general
, inflating risk, fear, and anxieties. A negative bias may
improve ratings and revenue, increasing motivation to continue watching coverage. A
combination of low-cost treatments greatly reducing risk conflicts with the negative
narrative.25 low-cost treatments were approved in one
or more countries, yet many countries approved no low-cost treatments.
The countries that did adopt low-cost treatments analyzed the evidence early and made
timely approvals. With few exceptions, authorities did not change their initial views,
regardless of how much evidence accumulated showing either efficacy or harm. Why?
The harms of smoking here hidden for 25 yearsC. Authorities did not analyze the data in real-time, failing to act when
harm was known.
Widespread acknowledgement of harm came only after attempts by two new surgeon generals,
along with pressure from health advocates and a new president, and a review of 7,000 studies.
Similarly for COVID-19, most authorities and experts did not proactively
analyze data in real-time. This guarantees delayed recognition of efficacy or harm, by
which time moral, legal, career, and reputational liabilities strongly disincentivize any
admission of error. Claims of no efficacy (for effective treatments) or safety (for
harmful treatments) were often made prior to strong data being available. Correction
would require admitting to errors that increased mortality, which is unlikely with the
same generation of officials.
Analysis of potential treatments was rarely done, and when done these were
typically minimal efforts.
For example, NIH reviews were highly delayed, cover only a tiny fraction of treatments,
reference only 2% of studies for the treatments covered, and include no
quantitative analysis.
They appear as rarely updated side projects from
external panels implicitly tasked with justifying prior failures.
As with smoking, the thousands of studies could (and should)
have been analyzed and acted on in real-time.
A key structural improvement, applicable to all current and future
diseases, is for authorities to implement real-time proactive analysis of clinical
evidence. This does not remove all bias, but does make it possible to act on evidence,
whereas delayed action may be unlikely due to moral, legal, career, and reputational
liabilities.
c19early.org
Delayed public health acknowledgments
Official acknowledgment of efficacy or harm is often delayed—legal, career, and status risks disincentivize admission of error.
| Evidence | Official Acknowledgment | Approx. Delay | |
|---|---|---|---|
| Citrus Fruit (vitamin C) for Scurvy (effectiveness) | 1747: James Lind conducted one of the first-ever controlled clinical trials, proving that oranges and lemons cured scurvy in sailors. | 1795: The British Royal Navy finally made a daily ration of lemon juice a standard issue for all its sailors, effectively eliminating the disease. | 48 years |
| Handwashing (lower mortality) | 1847: Dr. Ignaz Semmelweis provided conclusive proof that having doctors wash their hands with a chlorine solution before delivering babies reduced maternal mortality rates from over 18% to around 1%. | ~1870s: Semmelweis's findings were rejected and he was ridiculed. His work was only validated decades later (after his death). | ~20+ years |
| Helicobacter pylori (bacteria causes ulcers) | 1982-1984: Marshall and Warren discovered that Helicobacter pylori bacteria causes ulcers, confirmed via direct exposure. Officials maintained that ulcers were caused by stress and spicy food. | 1994: The US NIH released a consensus statement officially recommending antibiotics as the standard treatment for peptic ulcers, overturning decades of acid-suppression therapy. | ~12 years |
| Asbestos (causes asbestosis & cancer) | 1924: The British Medical Journal published the first case study of a death from "asbestosis." By 1918, U.S. insurance companies had stopped selling life insurance to asbestos workers. | 1971 (US): The Occupational Safety and Health Administration (OSHA) was formed and began regulating asbestos as a carcinogen, setting the first federal workplace safety standards for it. | ~47 years |
| Leaded Gasoline (neurotoxicity) | ~1924: Dangers of low-level lead exposure were known. Experts like Alice Hamilton warned the U.S. Surgeon General that adding lead to gasoline would cause widespread public poisoning. | 1973 (US): The Environmental Protection Agency (EPA) ordered the first phasedown of lead in gasoline, following the Clean Air Act of 1970. A full ban for on-road vehicles took effect in 1996. | ~49 years |
| Harms of Smoking (causes lung cancer) | 1939: Franz Müller (Germany) published the first case-control epidemiological study strongly linking tobacco smoking to lung cancer. This was followed by major U.S. & U.K. studies in the 1950s. | 1964 (US): The U.S. Surgeon General's report, "Smoking and Health," was released. It was the first U.S. government report to definitively link smoking to lung cancer and heart disease. | 25 years |
Heterogeneity in COVID-19 studies arises from many factors including:
The time between infection or the onset of symptoms and
treatment may critically affect how well a treatment works. For example an
antiviral may be very effective when used early but may not be effective in
late stage disease, and may even be harmful. Oseltamivir, for example, is
generally only considered effective for influenza when used within 0-36 or
0-48 hours259,260. Baloxavir marboxil studies for influenza
also show that treatment delay is critical — Ikematsu et al. report
an 86% reduction in cases for post-exposure prophylaxis, Hayden et al.
show a 33 hour reduction in the time to alleviation of symptoms for treatment
within 24 hours and a reduction of 13 hours for treatment within 24-48 hours,
and Kumar (B) et al. report only 2.5 hours improvement for inpatient
treatment.
| Treatment delay | Result |
| Post-exposure prophylaxis | 86% fewer cases261 |
| <24 hours | -33 hours symptoms262 |
| 24-48 hours | -13 hours symptoms262 |
| Inpatients | -2.5 hours to improvement263 |
Fig. 30 shows a mixed-effects meta-regression for
efficacy as a function of treatment delay in COVID-19 studies from 226 treatments, showing that efficacy
declines rapidly with treatment delay. Early treatment is critical for COVID-19.
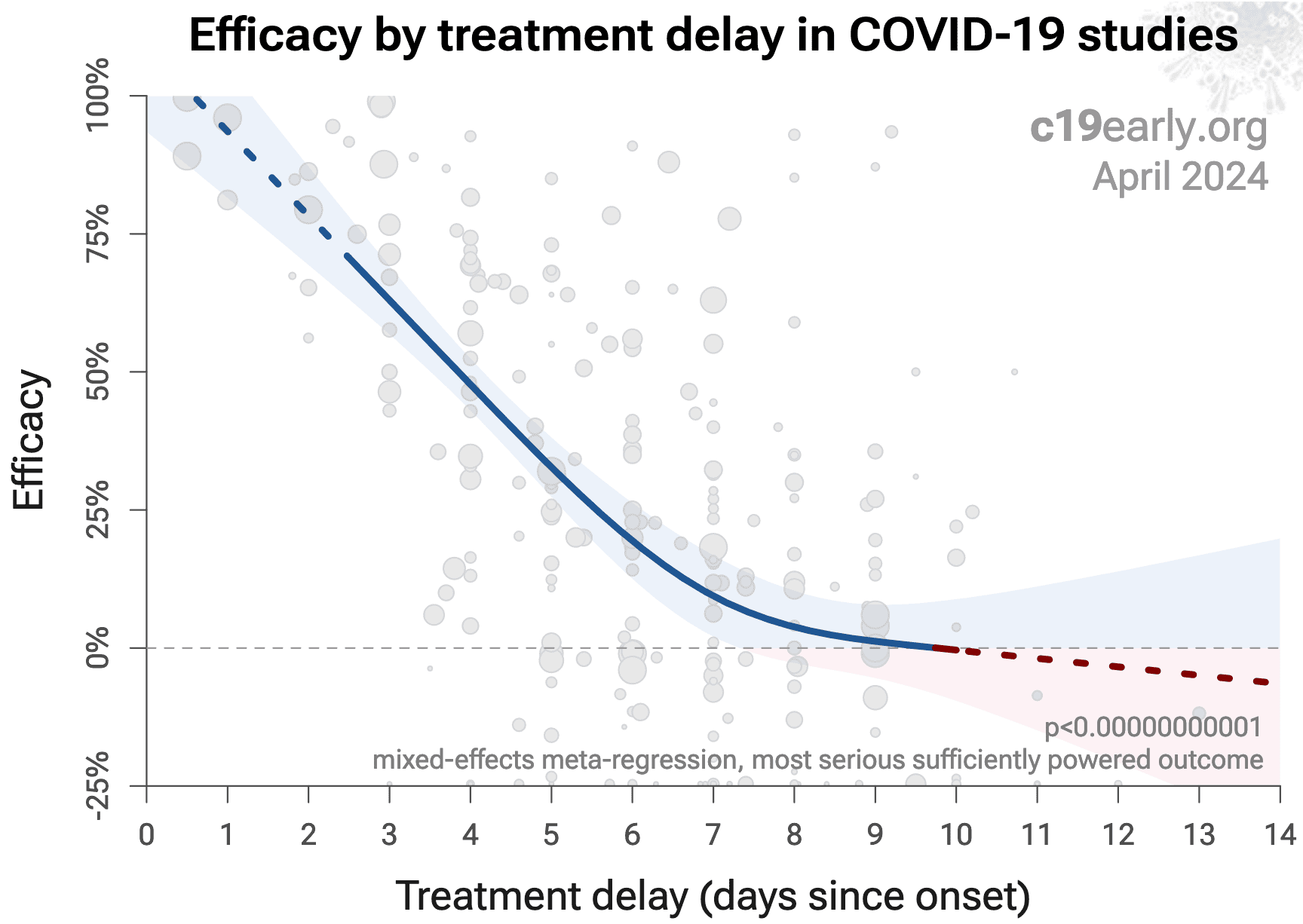{kind=link}
Fig. 30. Early treatment is more effective. Meta-regression showing efficacy as a function of treatment delay in COVID-19 studies from 226 treatments.
Details of the patient population including age and comorbidities may
critically affect how well a treatment works. For example, many COVID-19
studies with relatively young low-comorbidity patients show all patients
recovering quickly with or without treatment. In such cases, there is little
room for an effective treatment to improve results, for example as in
López-Medina et al.
Efficacy may depend critically on the distribution of
SARS-CoV-2 variants encountered by patients. Risk varies significantly across
variants265, for example the Gamma variant shows significantly
different characteristics266-269. Different
mechanisms of action may be more or less effective depending on variants, for
example the degree to which TMPRSS2 contributes to viral entry can differ
across variants270,271.
Effectiveness may depend strongly on the dosage, treatment regimen, and the
form of vitamin D used (cholecalciferol, calcifediol, or calcitriol).
The quality of medications may vary significantly between
manufacturers and production batches, which may significantly affect efficacy
and safety. Williams et al. analyze ivermectin from 11 different sources,
showing highly variable antiparasitic efficacy across different manufacturers.
Xu et al. analyze a treatment from two different manufacturers, showing 9
different impurities, with significantly different concentrations for each
manufacturer.
Non-prescription supplements may show very wide variations in quality1,2.
Across all
studies there is a strong association between different outcomes, for example
improved recovery is strongly associated with lower mortality. However,
efficacy may differ depending on the effect measured, for example a treatment
may be more effective against secondary complications and have minimal effect
on viral clearance.
The
distribution of studies will alter the outcome of a meta-analysis. Consider a
simplified example where everything is equal except for the treatment delay,
and effectiveness decreases to zero or below with increasing delay. If there
are many studies using very late treatment, the outcome may be negative, even
though early treatment is very effective.
All meta-analyses combine heterogeneous studies, varying in population,
variants, and potentially all factors above, and therefore may obscure
efficacy by including studies where treatment is less effective. Generally, we
expect the estimated effect size from meta-analysis to be less than that for
the optimal case.
Looking at all studies is valuable for providing an overview of all research,
important to avoid cherry-picking, and informative when a positive result is
found despite combining less-optimal situations. However, the resulting
estimate does not apply to specific cases such as
early treatment in high-risk populations with a specific form and dosage of vitamin D.
While we present results for all studies, we also present treatment time and
individual outcome analyses, which may be more informative for specific use
cases.
Vitamin D studies vary widely in all the factors above, which
makes the consistently positive results even more remarkable. A failure to
detect an association after combining heterogeneous studies does not mean the
treatment is not effective (it may only work in certain cases), however the
reverse is not true — an identified association is valid, although the
magnitude of the effect may be larger for more optimal cases, and lower for
less optimal cases. While we present results for all studies in this paper,
the individual outcome, form of vitamin D, and treatment time analyses are
more relevant for specific use cases.
This section validates the use of pooled effects for COVID-19, which enables
earlier detection of efficacy, however pooled effects are no longer required
for vitamin D as of October 2020. Efficacy is now known based on specific outcomes for all studies and when restricted to RCTs. Efficacy based on specific outcomes in RCTs was delayed by 9.4 months compared to using pooled outcomes in RCTs.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes" is not a good reason for
disregarding results.
Pooling the results of studies reporting different outcomes allows us to use
more of the available information. Logically we should, and do, use additional
information when evaluating treatments—for example dose-response and
treatment delay-response relationships provide additional evidence of efficacy
that is considered when reviewing the evidence for a treatment.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster and safer collection of evidence.
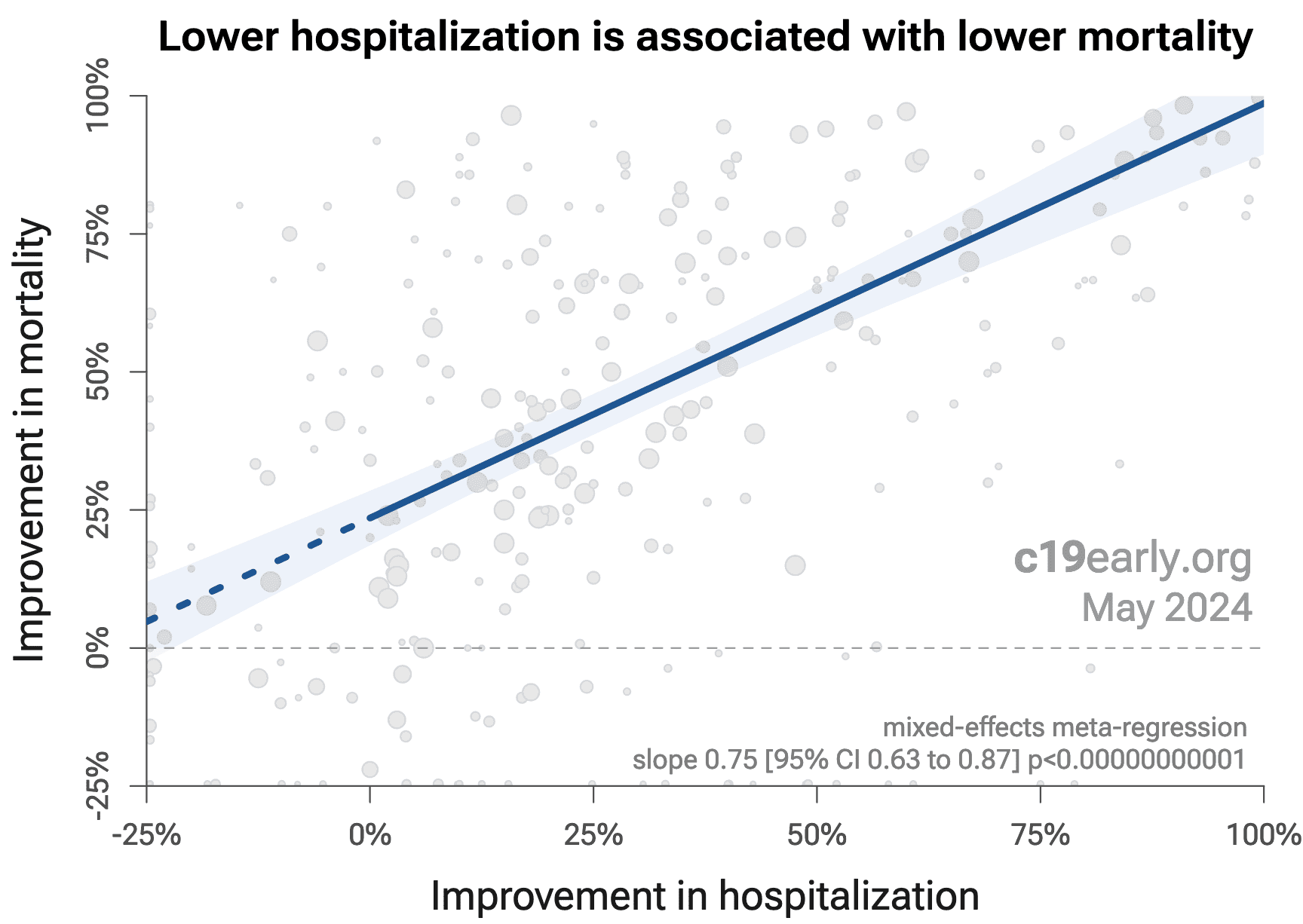
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 226
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
Fig. 31 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
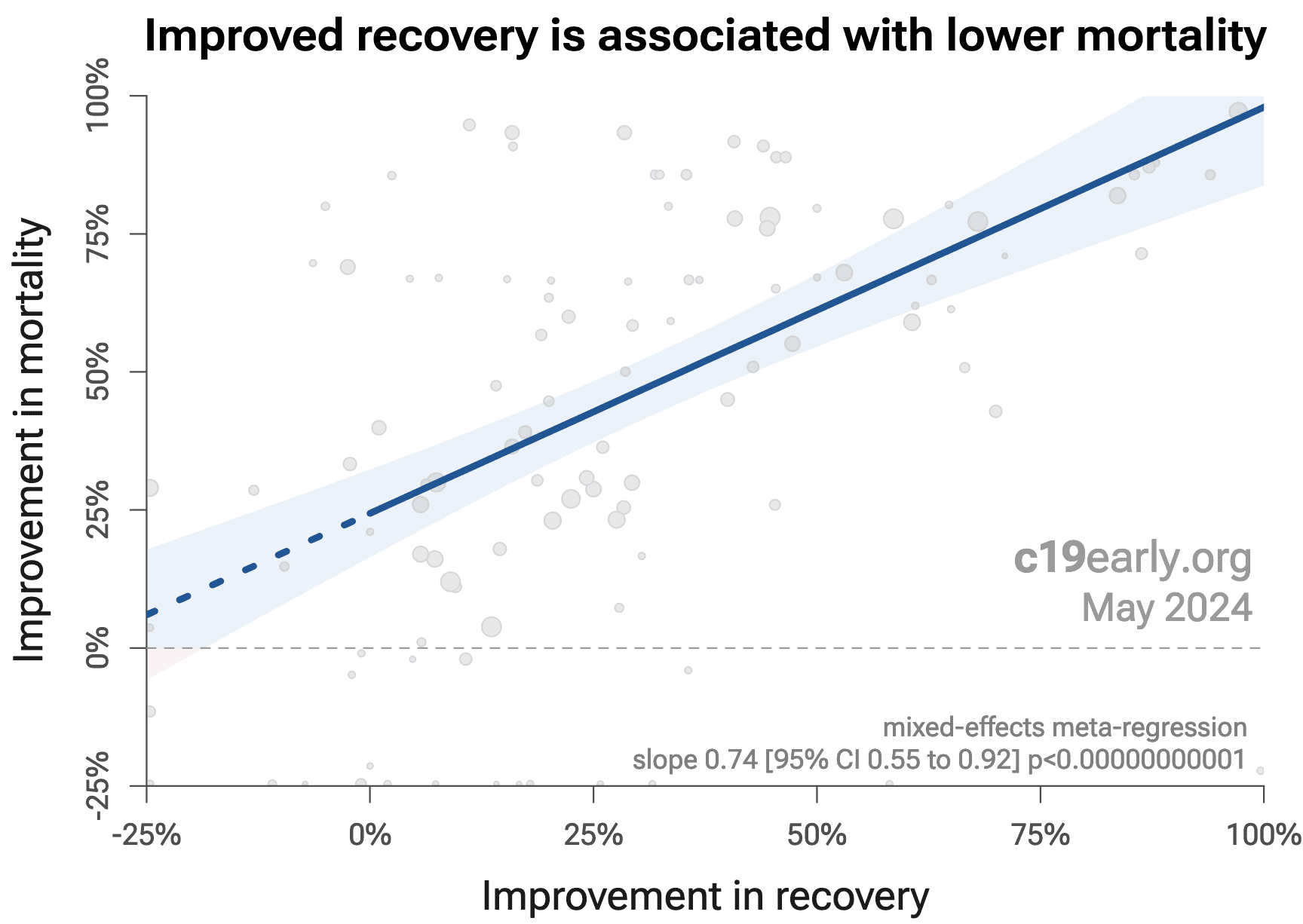
Similarly, Fig. 32 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
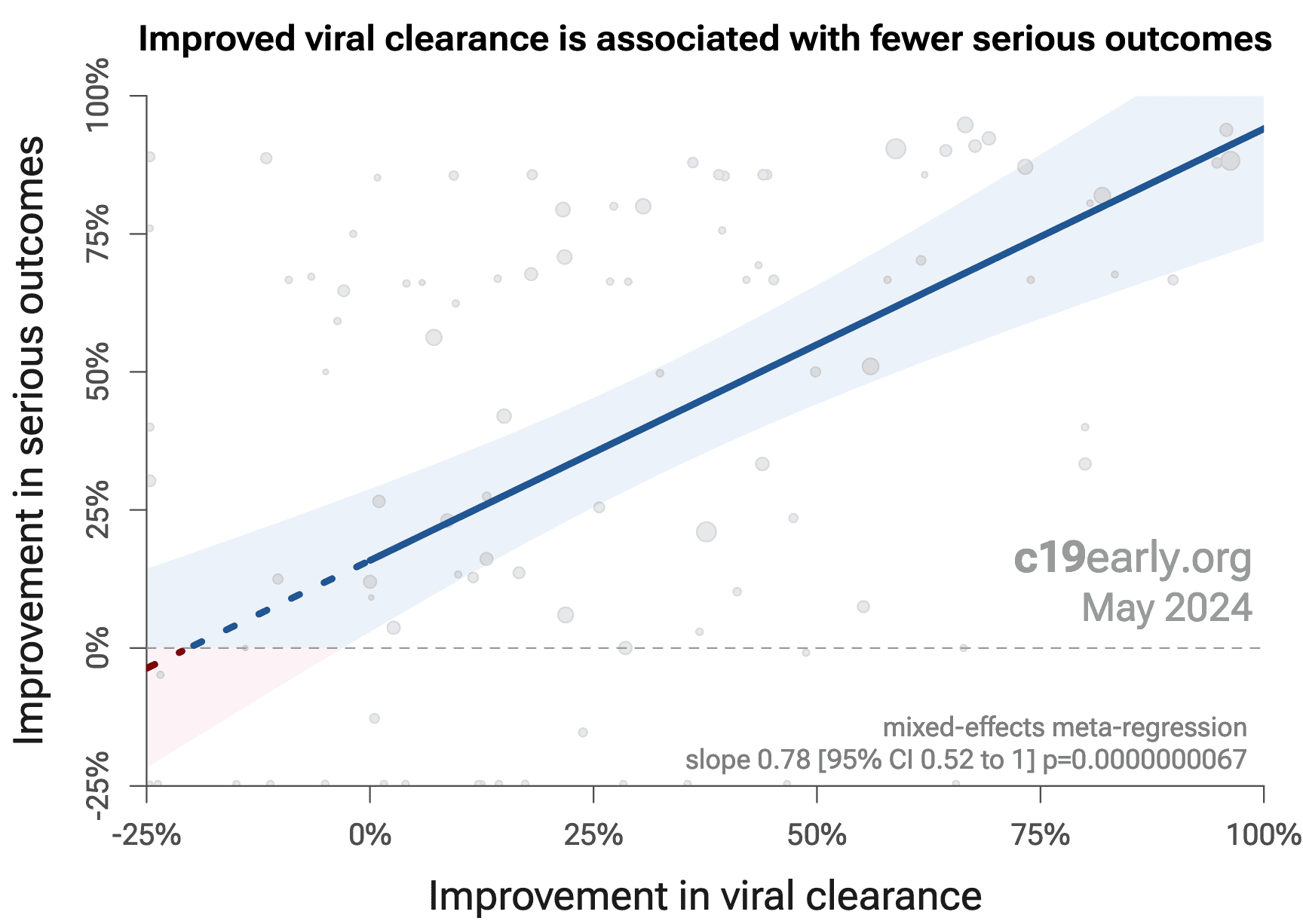
Considering the extremes, Singh (B) et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
Fig. 33 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh (B) et al., with higher confidence due to the larger number of
studies. As with Singh (B) et al., the confidence increases
when excluding the outlier treatment, from p = 0.000000011 to p = 0.00000000032.
{kind=link}
Fig. 31. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Fig. 32. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Fig. 31. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
Currently, 59 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 85% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.6 months. When restricting to RCTs only, 53% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 7.4 months.
Fig. 34 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
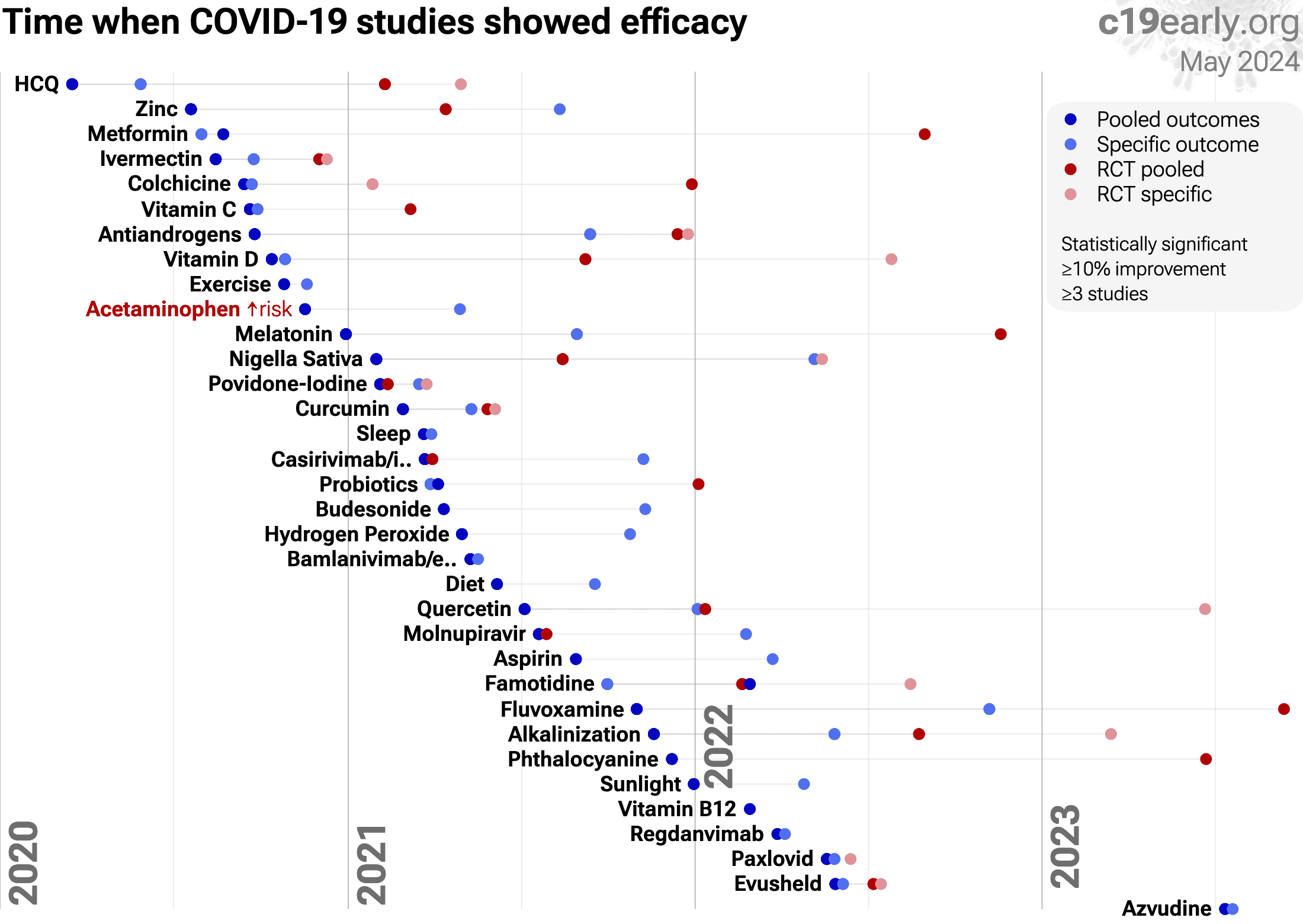{kind=link}
Fig. 34. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as differences in treatment delay are more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta-analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
For sufficiency
studies, different studies use different levels
as the threshold of sufficiency, vitamin D levels were measured at different
times, and some studies measure risk only within hospitalized patients, which
excludes the risk of a serious enough case to be hospitalized. However,
218 of 232 studies present positive effects.
Sufficiency studies show a strong correlation between low
vitamin D levels and worse COVID-19 outcomes, however they do not provide
information on vitamin D treatment. Studies with vitamin D levels measured
after admission may show lower levels because COVID-19 infection reduces
vitamin D levels. Studies with levels measured before infection also show
signficant benefit, however the cause could be one or more correlated factors.
For example, sunlight exposure increases vitamin D levels, but also increases
intracellular melatonin297, and melatonin shows significant
benefit for COVID-19298. Sun
exposure is also correlated with physical exercise, which also shows benefit
for COVID-19299.
119 of 138 treatment
studies report positive effects. Studies vary significantly in terms of
treatment delay, treatment regimen, patients characteristics, and (for the
pooled effects analysis) outcomes, as reflected in the high degree of
heterogeneity. However treatment consistently shows a significant benefit. The
treatment studies not showing positive effects are mostly prophylaxis studies
with unknown dosages. The only non-prophylaxis studies reporting negative
effects are a small unadjusted retrospective Assiri,
Zangeneh with no details of treatment, and
Murai, Mariani, Cannata-Andía which are very late stage studies using
cholecalciferol. For Murai, the result also has very low statistical
significance due to the small number of events, and the other reported
outcomes of ventilation and ICU admission, which have slightly more events and
higher confidence, show benefits for vitamin D. Calcifediol or calcitriol,
which avoids several days delay in conversion, may be more successful,
especially with very late stage usage.
Acute treatment shows greater efficacy than chronic prophylaxis
for mortality, p = 0.0042 (and also
in pooled analysis).
Chronic prophylaxis may have lower efficacy compared with acute treatment due to the
following:
•
CYP24A1 upregulation
-
chronic prophylaxis may upregulate CYP24A1, the enzyme that degrades active calcitriol.
The increased degradation rate can offset the availability of active calcitriol during the
high-demand acute phase. Specific forms and administration of vitamin D may
minimize upregulation of CYP24A1301.•
FGF23 elevation
- chronic
prophylaxis increases FGF23 which suppresses CYP27B1, the activating enzyme in the
kidney, and may also affect extrarenal activation in immune cells, though local
inflammatory signals can partially override this.•
Shifted immune baseline
-
chronic prophylaxis promotes a tolerogenic immune state (increased Tregs, tolerogenic
DCs). This may be beneficial for preventing autoimmunity and excessive inflammation, but
means the immune system is partially pre-regulated - potentially leaving less dynamic
range for vitamin D to modulate the acute inflammatory response.RCTs to date185,204 are consistent
with attenuating factors reducing the efficacy of prophylaxis, with
the shorter-term supplementation in Villasis-Keever et al. showing better
results compared to the longer-term high adherence supplementation in
Jolliffe et al. For acute respiratory infections, Wang (D) et al. also show
greater efficacy for prophylaxis trials with shorter durations.
Note that prophylaxis studies include case results, whereas we expect
vitamin D to be more effective against serious outcomes. Comparison of acute treatment
versus long-term supplementation should use the specific outcome analyses rather than the
pooled outcome analyses.
Other factors may be involved in the observed lower efficacy in prophylaxis studies. For
example, analysis of hospitalized patients is subject to selection bias because long-term
accurate-dosage supplementing individuals may be less likely to be hospitalized.
Publishing is often biased
towards positive results, however evidence suggests that there may be a negative bias for
inexpensive treatments for COVID-19. Both negative and positive results are
very important for COVID-19, media in many countries prioritizes negative
results for inexpensive treatments (inverting the typical incentive for
scientists that value media recognition), and there are many reports of
difficulty publishing positive results302-305.
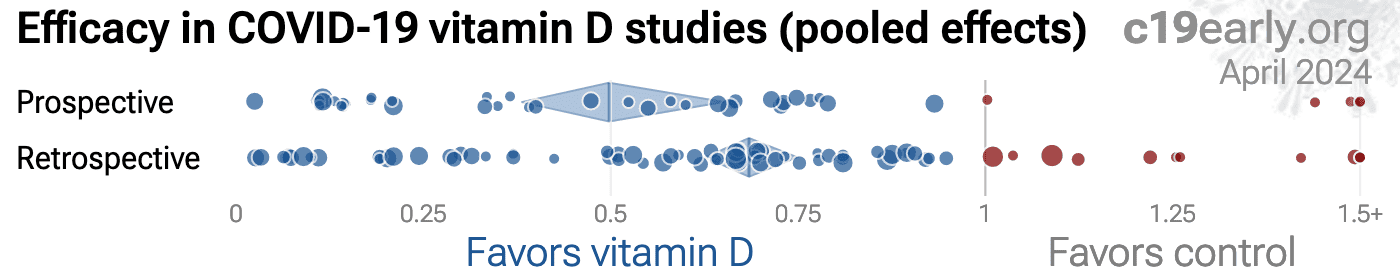
One method to evaluate bias is to compare prospective vs.
retrospective studies. Prospective studies are more likely to be published
regardless of the result, while retrospective studies are more likely to
exhibit bias. For example, researchers may perform preliminary analysis with
minimal effort and the results may influence their decision to continue.
Retrospective studies also provide more opportunities for the specifics of
data extraction and adjustments to influence results.
Fig. 35 shows a scatter plot of
results for prospective and retrospective treatment studies.
Prospective studies show 49% [36‑60%] improvement in meta-analysis,
compared to 34% [28‑40%] for retrospective
studies, suggesting possible negative publication bias, with a non-significant trend towards retrospective studies
reporting lower efficacy.
This gives us further confidence in the significant efficacy seen in all studies.
{kind=link}
Fig. 35. Prospective vs. retrospective studies.
The diamonds show the results of random-effects meta-analysis.
Funnel
plots have traditionally been used for analyzing publication bias. This is
invalid for COVID-19 acute treatment trials — the underlying assumptions
are invalid, which we can demonstrate with a simple example. Consider a set of
hypothetical perfect trials with no bias. Fig. 36 plot A
shows a funnel plot for a simulation of 80 perfect trials, with random group
sizes, and each patient's outcome randomly sampled (10% control event
probability, and a 30% effect size for treatment). Analysis shows no asymmetry
(p > 0.05). In plot B, we add a single typical variation in COVID-19 treatment
trials — treatment delay. Consider that efficacy varies from 90% for
treatment within 24 hours, reducing to 10% when treatment is delayed 3 days.
In plot B, each trial's treatment delay is randomly selected. Analysis now
shows highly significant asymmetry, p < 0.0001, with six variants of
Egger's test all showing p < 0.05306-313.
Note that these tests fail even though treatment delay is uniformly
distributed. In reality treatment delay is more complex — each trial has
a different distribution of delays across patients, and the distribution
across trials may be biased (e.g., late treatment trials may be more common).
Similarly, many other variations in trials may produce asymmetry, including
dose, administration, duration of treatment, differences in SOC,
comorbidities, age, variants, and bias in design, implementation, analysis,
and reporting.
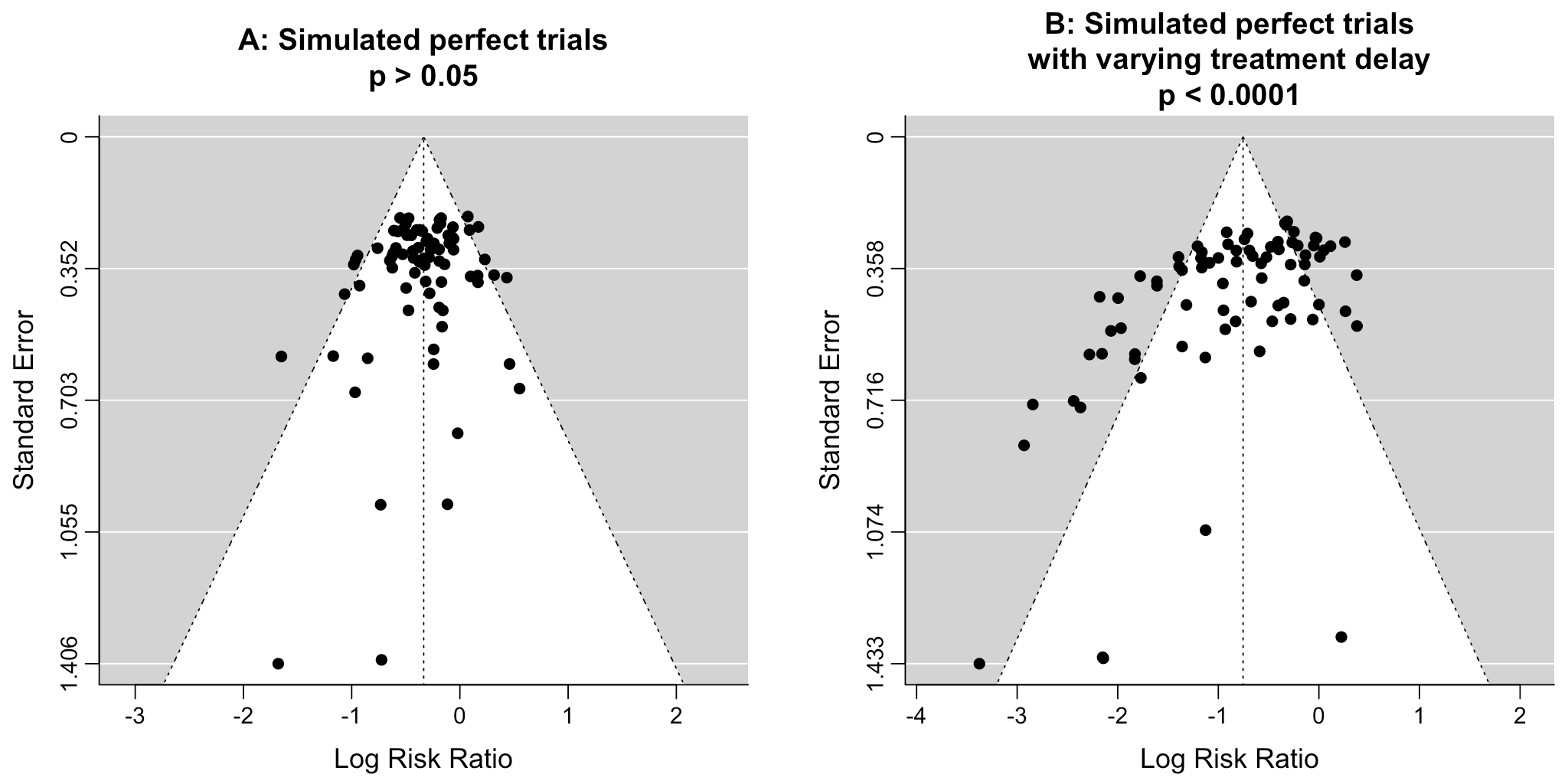{kind=link}
Fig. 36. Example funnel plot analysis for simulated perfect trials.
Pharmaceutical drug
trials often have conflicts of interest whereby sponsors or trial staff have a
financial interest in the outcome being positive. Vitamin D for COVID-19
lacks this because it is an inexpensive and widely available supplement.
In contrast, most COVID-19 vitamin D trials have been run by
physicians on the front lines with the primary goal of finding the best
methods to save human lives and minimize the collateral damage caused by
COVID-19. While pharmaceutical companies are careful to run trials under
optimal conditions (for example, restricting patients to those most likely to
benefit, only including patients that can be treated soon after onset when
necessary, and ensuring accurate dosing), not all vitamin D trials
represent the optimal conditions for efficacy.
The first version of
Lakkireddy was censored based on incorrect claims from an
anti-treatment researcher. For example, the author claims that the gender
difference between arms (7/44 vs. 15/43 female) indicates randomization
failure, however by simulation, using the group sizes and overall gender
ratio, the difference between the number of female patients in each arm is
expected to be ≥8 6.4% of the time (2.7% with ≥8 in the control arm, and 3.7%
with ≥8 in the treatment arm).
Author claims that the difference in CRP would only happen
about one in a billion times. This is incorrect. CRP is not normally
distributed, and the observed values could be due to a very small number of
outliers with very large CRP in one group.
A response from the study authors can be found at
c19early.org (I). The study was
republished.
Summary statistics from
meta-analysis necessarily lose information. As with all meta-analyses, studies
are heterogeneous, with differences
in treatment delay, treatment regimen, patient demographics, variants,
conflicts of interest, standard of care, and other factors. We provide analyses for specific
outcomes and by treatment delay, and we aim to identify key characteristics in
the forest plots and summaries. Results should be viewed in the context of
study characteristics.
Some analyses classify treatment based on early or late
administration, as done here, while others distinguish between mild, moderate,
and severe cases. Viral load does not indicate degree of symptoms — for
example patients may have a high viral load while being asymptomatic. With
regard to treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.
Details of treatment delay per patient is often not available.
For example, a study may treat 90% of patients relatively early, but the
events driving the outcome may come from 10% of patients treated very late.
Our 5 day cutoff for early treatment may be too conservative, 5 days may be too late in many cases.
Comparison across treatments is confounded by differences in
the studies performed, for example dose, variants, and conflicts of interest.
Trials with conflicts of interest may use designs better suited to the
preferred outcome.
In some cases, the most serious outcome has very few events,
resulting in lower confidence results being used in pooled analysis, however
the method is simpler and more transparent. This is less critical as the
number of studies increases. Restriction to outcomes with sufficient power may
be beneficial in pooled analysis and improve accuracy when there are few
studies, however we maintain our pre-specified method to avoid any
retrospective changes.
Studies show that combinations of treatments can be highly
synergistic and may result in many times greater efficacy than individual
treatments alone214,274-295 .
Therefore standard of care may be critical and benefits may diminish or
disappear if standard of care does not include certain treatments.
This real-time analysis is constantly updated based on
submissions. Accuracy benefits from widespread review and submission of
updates and corrections from reviewers. Less popular treatments may receive
fewer reviews.
No treatment or intervention is 100% available and
effective for all current and future variants. Efficacy may vary significantly
with different variants and within different populations. All treatments have
potential side effects. Propensity to experience side effects may be predicted
in advance by qualified physicians. We do not provide medical advice. Before
taking any medication, consult a qualified physician who can compare all
options, provide personalized advice, and provide details of risks and
benefits based on individual medical history and situations.
Treatments like vitamin C, D,
and zinc were often not recommended by health authorities in contradiction to
the clinical evidence. However use was common,
with increased prevalence for healthcare
professionals371-373 (and specifically those with more
experience374),
more highly educated
individuals352,372,375-381 ,
and with higher income374,376,379,380 .
Healthcare professionals also had lower risk than
expected for COVID-19382,383, consistent with greater use of effective
treatments.
Table 4 shows the reported results of physicians that used combined
early treatment protocols for COVID-19, compared to results for physicians following
guidelines focusing on late treatment (Dr. Uip reportedly prescribed early treatment for
himself, but not for patients384). The protocols vary, but include ivermectin,
HCQ, vitamin D, vitamin C, zinc, melatonin, quercetin, budesonide, and other treatments.
These results are subject to selection and ascertainment bias and more accurate analysis
requires details of the patient populations and follow-up, however results are consistently
better across many teams, and consistent with the extensive controlled trial evidence that
shows a significant reduction in risk with many early treatments, and improved results
with the use of multiple treatments in combination.
| LATE TREATMENT | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. David Uip (*) | Brazil | 2,200 | 38.6% (850) | 2.5% (54) |
| Dr. Jake Scott (**) | USA | 1,000 | 10.0% (100) | |
| Average | 38.6% | 6.2% | ||
| EARLY TREATMENT PROTOCOLS - 40 physicians/teams | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. Roberto Alfonso Accinelli 0/360 deaths for treatment within 3 days |
Peru | 1,265 | 0.6% (7) | |
| Dr. Mohammed Tarek Alam patients up to 84 years old |
Bangladesh | 100 | 0.0% (0) | |
| Dr. Oluwagbenga Alonge | Nigeria | 310 | 0.0% (0) | |
| Dr. Raja Bhattacharya up to 88yo, 81% comorbidities |
India | 148 | 1.4% (2) | |
| Dr. Flavio Cadegiani | Brazil | 3,450 | 0.1% (4) | 0.0% (0) |
| Dr. Alessandro Capucci | Italy | 350 | 4.6% (16) | |
| Dr. Shankara Chetty | South Africa | 8,000 | 0.0% (0) | |
| Dr. Deborah Chisholm | USA | 100 | 0.0% (0) | |
| Dr. Ryan Cole | USA | 400 | 0.0% (0) | 0.0% (0) |
| Dr. Marco Cosentino earlier treatment results were better |
Italy | 392 | 6.4% (25) | 0.3% (1) |
| Dr. Jeff Davis | USA | 6,000 | 0.0% (0) | |
| Dr. Dhanajay | India | 500 | 0.0% (0) | |
| Dr. Bryan Tyson & Dr. George Fareed | USA | 20,000 | 0.0% (6) | 0.0% (4) |
| Dr. Raphael Furtado | Brazil | 170 | 0.6% (1) | 0.0% (0) |
| Rabbi Yehoshua Gerzi | Israel | 860 | 0.1% (1) | 0.0% (0) |
| Dr. Heather Gessling | USA | 1,500 | 0.1% (1) | |
| Dr. Ellen Guimarães | Brazil | 500 | 1.6% (8) | 0.4% (2) |
| Dr. Syed Haider | USA | 4,000 | 0.1% (5) | 0.0% (0) |
| Dr. Mark Hancock | USA | 24 | 0.0% (0) | |
| Dr. Sabine Hazan | USA | 1,000 | 0.0% (0) | |
| Dr. Mollie James | USA | 3,500 | 1.1% (40) | 0.0% (1) |
| Dr. Roberta Lacerda | Brazil | 550 | 1.5% (8) | 0.4% (2) |
| Dr. Katarina Lindley | USA | 100 | 5.0% (5) | 0.0% (0) |
| Dr. Ben Marble | USA | 150,000 | 0.0% (4) | |
| Dr. Edimilson Migowski | Brazil | 2,000 | 0.3% (7) | 0.1% (2) |
| Dr. Abdulrahman Mohana | Saudi Arabia | 2,733 | 0.0% (0) | |
| Dr. Carlos Nigro | Brazil | 5,000 | 0.9% (45) | 0.5% (23) |
| Dr. Benoit Ochs | Luxembourg | 800 | 0.0% (0) | |
| Dr. Ortore | Italy | 240 | 1.2% (3) | 0.0% (0) |
| Dr. Valerio Pascua one patient already on oxygen died |
Honduras | 415 | 6.3% (26) | 0.2% (1) |
| Dr. Sebastian Pop | Romania | 300 | 0.0% (0) | |
| Dr. Brian Proctor | USA | 869 | 2.3% (20) | 0.2% (2) |
| Dr. Anastacio Queiroz | Brazil | 700 | 0.0% (0) | |
| Dr. Didier Raoult | France | 8,315 | 2.6% (214) | 0.1% (5) |
| Dr. Karin Ried up to 99yo, 73% comorbidities |
Turkey | 237 | 0.4% (1) | |
| Dr. Roman Rozencwaig patients up to 86 years old |
Canada | 80 | 0.0% (0) | |
| Dr. Vipul Shah | India | 8,000 | 0.1% (5) | |
| Dr. Silvestre Sobrinho | Brazil | 116 | 8.6% (10) | 0.0% (0) |
| Dr. Unknown | Brazil | 957 | 1.7% (16) | 0.2% (2) |
| Dr. Vladimir Zelenko | USA | 2,200 | 0.5% (12) | 0.1% (2) |
| Average | 2.2% | 0.1% | ||
SARS-CoV-2 infection and replication involves a complex
interplay of 500+ host and viral proteins and other
factors56-63, providing many therapeutic
targets.
Over 11,000 compounds have been predicted to reduce COVID-19
risk64, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
Fig. 37 shows an overview of the results for vitamin D
in the context of multiple COVID-19 treatments, and Fig. 38 shows a plot
of efficacy vs. cost for COVID-19 treatments.
{kind=link}
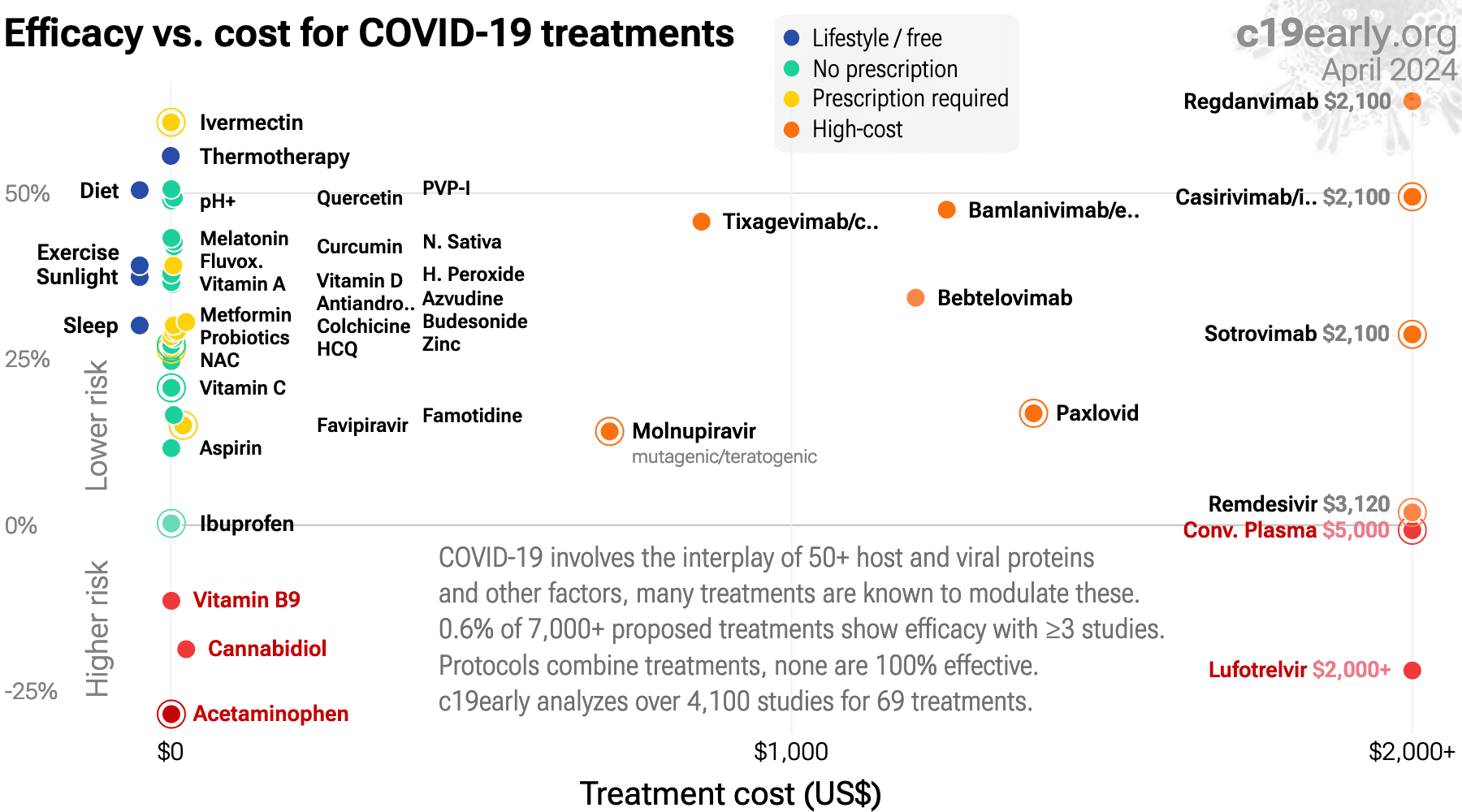{kind=link}
Fig. 38. Efficacy vs. cost for COVID-19 treatments.
Meta-analysis using the most serious
outcome reported shows 56% [37‑70%] and
38% [33‑43%] lower risk for early treatment
and for all studies.
Results are similar for higher quality studies,
peer-reviewed studies, and mortality.
Significantly lower risk is seen for
mortality,
ICU admission,
hospitalization, and
cases.
75 studies from 69 independent teams in 25 countries show significantly
lower risk.
Results are very robust—in worst case exclusion sensitivity analysis 91 of
138 studies must be excluded before statistical significance is lost.
Emergent results matching biological mechanisms confirm efficacy: efficacy gradient across outcomes (p = 0.031), calcitriol/calcifediol vs. cholecalciferol (p = 0.033), continuous vs. bolus treatment (p = 0.000035), and acute treatment vs. chronic prophylaxis (p = 0.0042).
Acute treatment (early 56% [37‑70%], late 47% [37‑55%]) shows greater efficacy than chronic
prophylaxis (32% [25‑39%]).
Late stage treatment with calcitriol/calcifediol
and analogs is more effective than cholecalciferol: 66% [47‑78%]
vs. 43% [32‑52%].
Ongoing treatment with multiple doses is more
effective than single bolus doses:
60% [50‑68%] vs. 22% [1‑38%]
22 other meta-analyses show significant improvements with vitamin D treatment for mortality4-18, mechanical ventilation4,8,9,14,19-21 , ICU admission4,6,8,9,12,14,16,18-24 , hospitalization14, severity5,7,8,13,25 , and cases10,23,25 .
Contact.
Contact us on X at @CovidAnalysis.
Funding.
We have received no funding or
compensation in any form, and do not accept donations. This is entirely volunteer work.
Conflicts of interest.
We have no conflicts of interest.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.AI.
We use AI models (Gemini, Grok, Claude, and
ChatGPT) tasked with functioning as additional peer-reviewers to check for errors, suggest
improvements, and review spelling and grammar. Any corrections are verified and applied
manually. Our preference for em dashes is independent of AI.Updates.
Our COVID-19 meta-analyses involve the extraction of over 226,000
datapoints from thousands of papers for 226 treatments. We thank the
thousands of scientists, physicians, and other contributors that have provided updates,
suggestions, feedback, and corrections. These are all welcome and can be submitted
at https://c19early.org/dmeta.html.
Dedication.
This work is dedicated to top
evidence-based physicians that worked tirelessly to analyze evidence and greatly reduce
mortality and morbidity during the pandemic. In alphabetical order:
Dr. Thomas J. Borody, Dr. Mary Talley Bowden, Dr. Flavio Cadegiani, Dr. Shankara Chetty,
Dr. Ryan Cole, Dr. George Fareed, Dr. Sabine Hazan, Dr. Pierre Kory, Dr. Tess Lawrie, Dr.
Robert Malone, Dr. Paul Marik, Dr. Peter McCullough, Dr. Didier Raoult, Dr. Harvey Risch,
Dr. Jackie Stone, Dr. Brian Tyson, Dr. Joseph Varon, and Dr. Vladimir (Zev) Zelenko.
Public domain.
This is a public domain work
distributed in accordance with the Creative Commons CC0 1.0 Universal license, which
dedicates the work to the public domain by waiving all rights worldwide under copyright law.
You can distribute, remix, adapt, and build upon this work in any medium or format,
including for commercial purposes, without asking permission. Referenced material and
third-party images retain any original copyrights or restrictions.
See: https://creativecommons.org/publicdomain/zero/1.0/.
c19early.org
Emergent results match biological mechanisms
While meta-analysis shows very strong confidence in efficacy, emergent results across studies that match biological mechanisms provides additional confirmation.
| Gradient across outcomes | Vitamin D may not have a direct antiviral effect; rather, any benefits are hypothesized to stem from improving immune system function. We may expect a gradient of efficacy across outcomes, with minimal impact on preventing initial infection (PCR+ cases), but increasing efficacy as the disease progresses to more severe stages. Meta-regression confirms this with p = 0.031. |
| Calcitriol etc. vs. cholecalciferol | We expect calcitriol, calcifediol and analogs to be more effective than cholecalciferol due to the added conversion delay with cholecalciferol. Studies specifying calcitriol etc. vs. cholecalciferol show 1.5 times greater efficacy, interaction p = 0.033. |
| Continuous dosing vs. bolus dosing | Pharmacokinetics and the potential side effects of high bolus doses suggest that ongoing treatment spread over time is more appropriate. Studies specifying continuous dosing vs. bolus dosing show 2.8 times greater efficacy, interaction p = 0.000035. |
| Acute vs. chronic treatment | We expect acute treatment to avoid issues with chronic prophylaxis (CYP24A1 upregulation, FGF23 elevation, and a shifted immune baseline providing less dynamic range during acute infection). Acute treatment vs. chronic prophylaxis shows 2.1 times greater efficacy, interaction p = 0.0042. |
This paper is data driven, all graphs and numbers are
dynamically generated. Please
submit updates and corrections at https://c19early.org/dmeta.html.
6/13/2026: We added di Filippo (C).
5/25/2026: Discussion updates.
5/17/2026: We added Almacioglu.
5/15/2026: We added Yang.
4/21/2026: We added Rizzi.
4/20/2026: We added Abbas.
3/24/2026: We added di Filippo (B).
3/21/2026: We added Dip.
3/12/2026: We added Ganmaa.
2/27/2026: We excluded Assiri due to data issues.
1/19/2026: Summary of emergent results matching biological mechanisms.
1/16/2026: Updated discussion of chronic prophylaxis vs. acute treatment.
1/13/2026: We added analysis of the efficacy gradient across outcomes.
1/2/2026: We added Doustmohammadian.
12/13/2025: Inclusion and discussion of low vs. high dose studies.
12/10/2025: We added Meltzer.
11/1/2025: Media coverage analysis and discussion updates.
10/5/2025: We added Nahhas.
7/24/2025: We added Monroy-Iglesias.
6/10/2025: We added Blázquez-Cabrera.
5/30/2025: We added Wagner.
5/9/2025: We added Ito.
5/2/2025: We added Tanriverdi.
4/4/2025: We added Hossain.
3/9/2025: We added Domènech-Montoliu.
2/22/2025: We added Mohamed.
2/19/2025: We added Vasconcelos.
2/4/2025: We added Najih.
1/30/2025: We added Sümegi.
1/23/2025: We updated the preclinical discussion.
12/23/2024: We added You.
12/10/2024: We added Chadda.
11/10/2024: We added Pashaei.
11/10/2024: We added Mirkarimi.
11/8/2024: We added Vargas-Castro.
10/23/2024: We added Chan.
10/22/2024: We added Hemdan.
10/14/2024: We added García-Zendejas.
9/28/2024: We added references to Wang (D) regarding
dosing and trial duration for prophylaxis of acute respiratory
infections.
9/22/2024: We updated Wang (C) to the journal
version.
9/18/2024: We added Rachman.
8/18/2024: We added Božić.
8/11/2024: We added Pietzner.
8/10/2024: We added Değirmenci.
7/12/2024: We added Węgrzynek-Gallina.
6/22/2024: We added Milan.
6/14/2024: We added Sanz.
6/12/2024: We added Cardoso.
6/10/2024: We added Singhsakul.
5/28/2024: We added Yang (B).
5/18/2024: We added Wang (B).
4/26/2024: Updated discussion of bolus treatment.
4/25/2024: We added Chen.
4/8/2024: We added Pavlyshyn.
3/27/2024: We added Arambepola, and updated discussion of pooled outcomes.
3/24/2024: We added Arboleda.
3/13/2024: We added Guðnadóttir.
3/11/2024: We added Devi.
2/28/2024: We added Sartini.
2/24/2024: We added Comunale.
2/23/2024: RCT discussion updates.
2/1/2024: We added Athanassiou.
1/31/2024: We updated Singh to the journal
version.
1/24/2024: We added Rozemeijer.
1/24/2024: We updated the introduction.
1/16/2024: We added Choi.
1/9/2024: We added Efe Iris.
12/20/2023: We added Wu (B).
12/15/2023: Updated discussion of preclinical results.
11/27/2023: We added Renieris.
11/9/2023: We added Akbar.
10/2/2023: We added Bogomaz.
9/24/2023: We added Seely (B).
9/8/2023: We added Ogasawara.
8/29/2023: We added Shamsi.
8/24/2023: We added Al Sulaiman.
8/21/2023: We added Mayurathan.
8/13/2023: We added Mingiano.
8/10/2023: We added Connolly.
8/5/2023: We added analysis for RCT ICU outcomes.
6/24/2023: We added Frish.
6/4/2023: We added Manojlovic.
6/4/2023: We added Jalavu.
6/4/2023: We added Wani.
5/8/2023: We added Hogarth.
5/6/2023: We added Ritsinger.
5/5/2023: We added Regalia.
5/2/2023: We added Sanamandra.
4/20/2023: We added Allami.
4/19/2023: We added Zafar, Cetin Ozbek.
4/16/2023: We added Rachman (B).
4/12/2023: We added Basińska-Lewandowska.
4/6/2023: We added Bayrak.
4/2/2023: We added Gonzalez.
4/1/2023: We added Arabadzhiyska.
3/28/2023: We added Schmidt.
3/23/2023: We added Davran.
3/15/2023: We added Bucurica.
3/15/2023: We added Topan.
3/14/2023: We added Domazet Bugarin, Siuka.
3/4/2023: We added Şengül.
3/4/2023: We added Chen (F).
3/2/2023: We added Tan.
2/18/2023: We added Ortatatli.
2/8/2023: We added Arabi.
1/28/2023: We added Batur.
1/20/2023: We added Mostafa.
1/19/2023: We added Din Ujjan.
1/17/2023: We added Valecha.
1/8/2023: We updated van Helmond to the journal
version.
1/7/2023: We updated discussion of acute treatment vs.
long-term supplementation.
12/31/2022: We added De Nicolò.
12/20/2022: We added Abdrabbo AlYafei.
12/20/2022: We updated the discussion of heterogeneity and
RCTs.
12/12/2022: We added Vásquez-Procopio.
12/3/2022: We added Tallon.
11/27/2022: We added Guldemir (B).
11/26/2022: We added Sharif.
11/13/2022: We added Gibbons.
11/8/2022: We added Said.
11/4/2022: We added Bychinin.
10/28/2022: We added Álvarez.
10/26/2022: We added Hafezi.
10/15/2022: We added Charla.
10/8/2022: We added Karimpour-Razkenari.
10/1/2022: We added Singh.
9/20/2022: We added Shahid.
9/19/2022: We added van Helmond.
9/15/2022: We added Brunvoll.
9/11/2022: We added Zeidan.
8/25/2022: We added Hafez (B).
8/24/2022: We added Saheb Sharif-Askari (B), Aldwihi.
8/23/2022: We added Doğan (B).
8/21/2022: We added Reyes Pérez.
8/19/2022: We added Kalichuran.
8/16/2022: We updated Lakkireddy to the new version (post
censorship of the previous version).
8/12/2022: We added Zurita-Cruz, Dana.
8/10/2022: We added Barrett.
8/5/2022: We added Bogliolo.
8/3/2022: We added Alzahrani (B).
7/27/2022: We added De Niet.
7/26/2022: We added Neves.
7/24/2022: We added Gholi.
7/19/2022: We added Baykal.
7/2/2022: We added Hunt.
6/24/2022: We added Karonova (B).
5/28/2022: We added Mariani.
5/24/2022: We added Ghanei.
5/23/2022: We added Fiore.
5/20/2022: We added Hosseini (C).
5/19/2022: We added Jabeen.
5/19/2022: We added Ozturk.
5/8/2022: We added Charkowick.
5/5/2022: We added Nguyen.
5/1/2022: We added Khan.
4/30/2022: We added Voelkle.
4/24/2022: We added Davoudi.
4/22/2022: We added discussion of Lakkireddy.
4/18/2022: We added Villasis-Keever.
4/17/2022: We added a section on preclinical research.
4/15/2022: We added Parant.
4/12/2022: We added Martínez-Rodríguez.
4/5/2022: We added preprint discussion based on
Zeraatkar.
4/2/2022: We added Ferrer-Sánchez.
3/31/2022: We added Ramos.
3/27/2022: We added Pande.
3/25/2022: We added Elhadi.
3/23/2022: We added Jolliffe.
3/20/2022: We added Bushnaq.
3/19/2022: We added Shehab.
3/7/2022: We added Rodríguez-Vidales.
3/5/2022: We added Reis.
3/4/2022: We added Nimer.
3/3/2022: We added Karonova (C).
2/24/2022: We added Zidrou.
2/20/2022: We added Sanson.
2/19/2022: We added Cannata-Andía.
2/18/2022: We added Junior, González-Estevez.
2/17/2022: We added Mahmood.
2/15/2022: We updated Vanegas-Cedillo to the journal version.
2/11/2022: We added Bychinin (B).
2/8/2022: We added Subramanian.
2/8/2022: We added Ranjbar.
2/6/2022: We added Bishop.
2/4/2022: We added Ahmed (B).
2/4/2022: We updated Dror to the journal version.
1/30/2022: We updated Leal-Martínez to the journal version.
1/29/2022: We added Ansari.
1/28/2022: We added Anjum.
1/25/2022: We added Saponaro.
1/23/2022: We added Smaha.
1/14/2022: We added Baguma.
1/13/2022: We updated Israel to the journal version.
1/8/2022: We added Seal.
1/5/2022: We added Pepkowitz.
1/3/2022: We added Efird.
12/26/2021: We added Abdulateef.
12/21/2021: We added Beigmohammadi, Sainz-Amo.
12/20/2021: We added Galaznik.
12/17/2021: We added Seven.
12/16/2021: We added Parra-Ortega.
12/14/2021: We added Putra.
12/9/2021: We added analysis of the number of independent research
groups reporting statistically significant positive results.
12/7/2021: We added Ma.
12/5/2021: We added Asgari.
12/3/2021: We updated Loucera to the journal version.
12/3/2021: We added Fatemi.
12/3/2021: We added Kaur.
11/22/2021: Added discussion related to sufficiency studies.
11/14/2021: We added Gönen.
11/12/2021: We added Asghar.
11/7/2021: We added Holt.
11/3/2021: We added Atanasovska.
11/1/2021: We updated Golabi to the journal version.
10/31/2021: We added Leal-Martínez, Assiri, Bianconi .
10/19/2021: We added Jimenez.
10/18/2021: We added Mohseni.
10/16/2021: We added a summary plot for all results.
10/15/2021: We added Ramirez-Sandoval.
10/15/2021: We added Maghbooli.
10/14/2021: We added Burahee, Arroyo-Díaz and analysis of treatment mechanical ventilation, ICU admission, and hospitalization results.
9/28/2021: We added Yildiz.
9/27/2021: We added Derakhshanian.
9/22/2021: We added Bagheri.
9/14/2021: We added Ribeiro.
9/14/2021: We updated Vasheghani to the journal version of the article.
9/14/2021: We added Elamir.
9/10/2021: We added Tomasa-Irriguible.
9/7/2021: We added Pecina, Karonova (D).
9/6/2021: We added Soliman.
9/1/2021: We added Golabi.
8/23/2021: We corrected Jain (B) to include the mortality outcome.
8/15/2021: We added Nimavat.
8/13/2021: We added di Filippo (D) and updated Louca to the journal version of the article.
8/12/2021: We added Alpcan.
8/10/2021: We added discussion of the immune system and vitamin
D.
8/2/2021: We added Matin.
8/1/2021: We added Pimental.
7/28/2021: We added Israel (B).
7/27/2021: We added Cozier.
7/26/2021: We added Güven.
7/25/2021: We added Asimi.
7/24/2021: We added Orchard.
7/21/2021: We added Savitri.
7/19/2021: We added Oristrell.
7/11/2021: We added Krishnan.
6/25/2021: We added Cereda.
6/19/2021: We added Jude.
6/16/2021: We added Campi.
6/12/2021: We added Levitus.
6/11/2021: We updated Oristrell (B) to the journal version.
6/9/2021: We added Fasano.
6/8/2021: We updated Nogués to the journal version.
6/7/2021: We added Dror, Diaz-Curiel.
5/29/2021: We added Sánchez-Zuno.
5/22/2021: We added analysis restricted to cholecalciferol
studies.
5/21/2021: We added Alcala-Diaz, Li (B).
5/20/2021: We updated Lakkireddy to the journal version.
5/19/2021: We added AlSafar.
5/10/2021: We added additional information in the abstract.
5/9/2021: We clarified terminology for prophylaxis and added
discussion of heterogeneity.
5/8/2021: We added analysis for treatment studies restricted to
peer-reviewed articles.
4/30/2021: We added Loucera.
4/29/2021: We corrected the treatment group counts for the early
treatment group in Annweiler (B) (there was no change in the relative
risk).
4/24/2021: We added analysis restricted to RCT studies and to
calcifediol/calcitriol studies. We have excluded Espitia-Hernandez
in the treatment analysis because they use a combined protocol with another
medication that shows high effectiveness when used alone.
4/14/2021: We added Blanch-Rubió.
4/13/2021: We added Oristrell (B), Lohia.
4/12/2021: We added Barassi.
4/10/2021: We added Szeto.
4/9/2021: We added Ünsal.
4/5/2021: We added Bayramoğlu, Livingston.
4/4/2021: We added event counts to the forest plots.
3/31/2021: We added Mendy.
3/30/2021: We added Macaya.
3/29/2021: We added Im.
3/28/2021: We added Freitas (B).
3/22/2021: We added Meltzer (B).
3/15/2021: We added Vanegas-Cedillo.
3/14/2021: We added Cereda (B).
3/12/2021: We added Charoenngam.
3/10/2021: We added Mazziotti.
3/6/2021: We added Ricci.
2/26/2021: We added Lakkireddy.
2/25/2021: We added Sulli.
2/20/2021: We added Gavioli.
2/20/2021: We added Infante.
2/18/2021: Murai was updated to the journal version of the
paper.
2/17/2021: We corrected an error in the effect extraction for
Angelidi, and we added treatment case and viral clearance forest
plots.
2/16/2021: We added Susianti.
2/10/2021: We added Nogués.
2/10/2021: We added Karonova (E).
2/9/2021: We added Karahan.
2/7/2021: We added Li (C).
2/5/2021: We added Yılmaz.
1/31/2021: We added Demir.
1/30/2021: We added Ma (B).
1/22/2021: We added Giannini.
1/21/2021: We added Bennouar.
1/19/2021: We added Amin.
1/18/2021: We added Vasheghani.
1/16/2021: We moved the analysis with exclusions to the main text,
and added additional commentary.
1/15/2021: We added the effect measured for each study in the forest
plots.
1/10/2021: We added Angelidi.
1/7/2021: We added direct links to the study details in the
chronological plots.
1/5/2021: We added direct links to the study details in the forest
plots.
1/2/2021: We added dosage information and we added the number of
patients to the forest plots.
12/31/2020: We added additional details about the studies in the
appendix.
12/28/2020: We added Jevalikar.
12/27/2020: We added the total number of authors and patients.
12/23/2020: We added Cangiano.
12/17/2020: Initial revision.
We perform ongoing searches of PubMed, medRxiv, Europe PMC, ClinicalTrials.gov, The Cochrane
Library, Google Scholar, Research Square, ScienceDirect, Oxford University Press, the
reference lists of other studies and meta-analyses, and submissions to the site c19early.org, which regularly receives notification of studies upon
publication.
Search terms are vitamin D, cholecalciferol, or calcitriol, and COVID-19 or SARS-CoV-2. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of vitamin D for COVID-19 that report a comparison with a
control group are included in the main treatment analysis, and all studies comparing COVID-19 outcomes in groups of patients with
low and high vitamin D levels are included in the sufficiency analysis. A few studies only
provide results as a function of change in vitamin D levels, which may not be indicative
of results for deficiency/insufficiency versus sufficiency (if levels are already
sufficient then further increase may be less beneficial).
Sensitivity analysis is performed, excluding studies with major issues, epidemiological
studies, and studies with minimal available information.
Studies with major unexplained data issues, for example major outcome data that is
impossible to be correct with no response from the authors, are excluded.
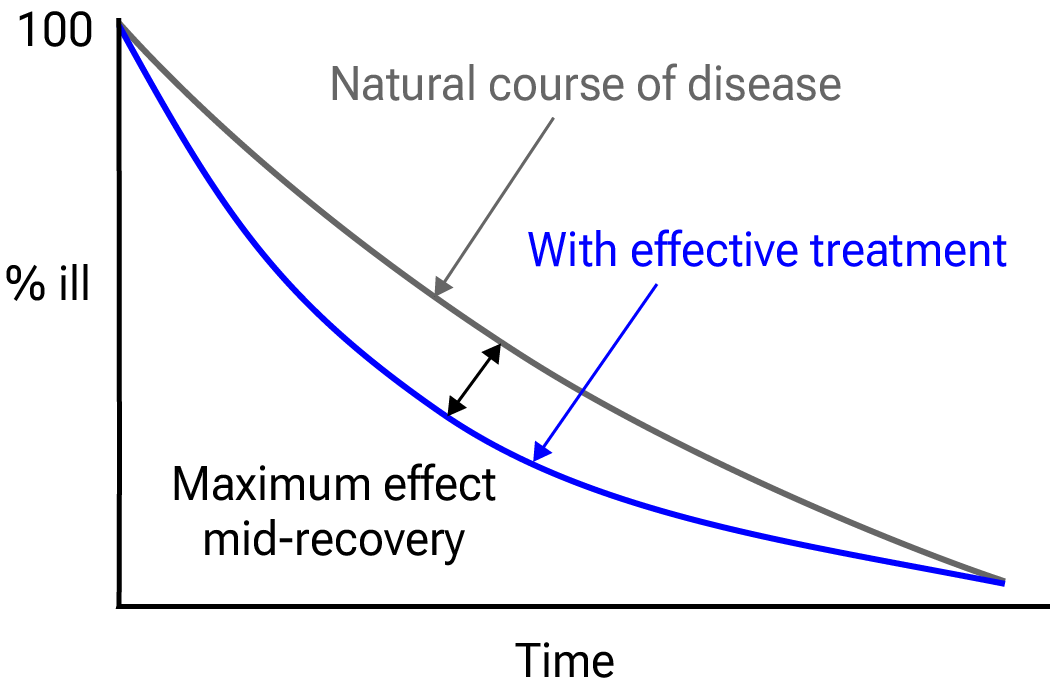{kind=link}

Fig. 39.
Mid-recovery results can more accurately reflect efficacy when almost all patients
recover. Mateja et al. confirm that intermediate viral load results more accurately
reflect hospitalization/death.
We extracted effect sizes and associated data from all studies. If studies report multiple
kinds of effects then the most serious outcome is used in pooled analysis, while
other outcomes are included in the outcome-specific analyses. For example, if effects for
mortality and cases are reported then they are both used in specific outcome analyses,
while mortality is used for pooled analysis.
If symptomatic results are reported at multiple times, we use the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28 days have
preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious outcome with
one or more events is used. For example, in low-risk populations with no mortality, a
reduction in mortality with treatment is not possible, however a reduction in
hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral outcomes.
When basically all patients recover in both treatment and control groups, preference for
viral clearance and recovery is given to results mid-recovery where available. After most
or all patients have recovered there is little or no room for an effective treatment to do
better, however faster recovery is valuable.
An IPD meta-analysis confirms that intermediate viral load reduction is more closely
associated with hospitalization/death than later viral load reduction630.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
Forest plots are computed using PythonMeta631 with the DerSimonian and
Laird random-effects model (the fixed effect assumption is not plausible in this case) and
inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
When results provide an odds ratio, we compute the relative risk when possible, or convert
to a relative risk according to Zhang (B) et al.
Reported confidence intervals and p-values are used when available, and adjusted
values are used when provided. If multiple types of adjustments are reported propensity
score matching and multivariable regression has preference over propensity score matching
or weighting, which has preference over multivariable regression. Adjusted results have
preference over unadjusted results for a more serious outcome when the adjustments
significantly alter results.
When needed, conversion between reported p-values and confidence intervals followed
Altman, Altman (B), and Fisher's exact test was used to calculate
p-values for event data. If continuity correction for zero values is required, we
use the reciprocal of the opposite arm with the sum of the correction factors equal to
1635.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of a negative
outcome when applicable (for example, the risk of death rather than the risk of survival).
If studies only report relative continuous values such as relative times, the ratio of the
time for the treatment group versus the time for the control group is used. Calculations
are done in Python (3.14.6) with
scipy (1.18.0), pythonmeta (1.26), numpy (2.5.1), statsmodels (0.14.6), and plotly (6.9.0).
Mixed-effects meta-regression results are computed with R (4.4.0) using the metafor
(4.6-0) and rms (6.8-0) packages, and using the most serious sufficiently powered outcome.
Forest plots show simplified dosages for comparison, these are the total dose in the first five days for treatment, and the monthly dose for prophylaxis. Calcifediol, calcitriol, and paricalcitol treatment are indicated with (c), (t), and (p). For full dosage details see below.
For all statistical tests, a p-value less than 0.05 was considered statistically
significant.
Grobid 0.8.2 is used to parse PDF documents.
For treatments that may improve immune system function but are not expected
to have a direct antiviral effect,
we may expect a gradient of efficacy across outcomes,
with minimal impact on preventing initial infection (PCR+ cases), but increasing efficacy
against more severe outcomes. To evaluate this hypothesis we performed meta-regression
with robust variance estimation. Clinical outcomes were categorized into an ordinal
severity scale with cases at severity 1, hospitalization at severity 2, and critical
outcomes at severity 3 (ICU admission, ventilation, and mortality).
The dependent variable was the natural logarithm of the Risk Ratio (ln(RR)) for each
outcome, and the independent variable was the ordinal severity score.
We used the DerSimonian and Laird (DL) method-of-moments estimator to estimate residual
heterogeneity (τ2) around the meta-regression line, with weights assigned
using the inverse-variance method (wi = 1 / (vi +
τ2)).
To account for the non-independence of multiple outcomes reported within the same study
(e.g., mortality and hospitalization data derived from the same patient population), we
used cluster-robust standard errors clustered by study ID.
The meta-regression slope (β) represents the change in ln(RR) per unit
increase in severity. A negative slope indicates improving efficacy (lower Risk
Ratio) for more severe outcomes.
When evaluating potential effect modification across groups, we use an
interaction test as described by Altman (C) et al. We compared the log-transformed
relative risks using a z-test, deriving the standard error of the difference from
the 95% confidence intervals. A two-sided interaction p-value of < 0.05 was
considered a statistically significant difference in treatment effect between the
groups.
Cochrane RoB 2/ROBINS-I are often used to evaluate studies, and have the advantage of
providing standardized rules that can be applied with minimal understanding of the domain
and study. However, the rules do not account for many real-world issues, often
overemphasize or underemphasize others, and studies show low inter-rater
reliability643.
Certain domains are more applicable for these tools, however the time-sensitive nature of
a pandemic, with significant mortality for every day of delay in evidence assessment, and
the characteristics of COVID-19 make them inappropriate for this domain.
This can be demonstrated with examples where expert RoB 2/ROBINS-I ratings do not match
reality for COVID-19. Popp et al. use RoB 2 to classify Reis (B) et al. as low
risk of bias, however this is the opposite of reality—the trial not only has very
high risk of bias, but has very high actual known bias, refusing to release data despite
pledging to, reporting multiple impossible numbers, having blinding and randomization
failure, and many other issues645.
Axfors et al. use RoB 2 to classify Horby et al. as low risk of bias, however
this is the opposite of reality—the very late treatment and excessive dosage used
produces results with no relevance to recommended usage.
HCQ shows poor results with
late treatment and excessive dosage, and the combination shows harmD.
Hempenius et al. use ROBINS-I to classify 33 studies for HCQ. The two rated as having
the lowest risk of bias641,642 are far from the most informative. Both
involve very late treatment, providing no information on recommended usage, and ROBINS-I
does a very poor job of accounting for the impact of confounding factorsE.
Our quality evaluation focuses on known issues and bias, and the potential
impact on outcomes, rather than just the risk of bias.
The estimated potential impact of each confounding factor, and the direction of the impact
is considered. For example, consider a study that shows significantly lower risk, the
value of the study varies significantly if confounding points to an underestimate or an
overestimate of efficacy. In one case, the real effect may be null, while the other case
provides stronger evidence of efficacy (which may be greater than the study shows).
Analysis focusing on the risk of bias, while simpler, may penalize studies for theoretical
or technical issues that have no or minimal impact on outcomes. Analysis also depends on
the outcome, for example certain issues are less relevant for objective outcomes such as
mortality.
Inaccurate penalization, and inaccurate high-quality evaluation in the face of known major
issues affecting outcomes, increases in significance during a pandemic when immediate
recognition of new evidence is critical, and when considering all global studies, as
required during a pandemic. Investigators in other countries may have different customs
for design, analysis, and reporting, and different English language skills, however they
may not be less diligent or have greater bias.
Investigators in lower-pharmaceutical-profit countries may have lower bias towards
profitable interventions.
We have classified studies as
early treatment if most patients are not already at a severe stage at the time of
treatment (for example based on oxygen status or lung involvement), and treatment started
within 5 days of the onset of symptoms. If studies contain a mix of early treatment and
late treatment patients, we consider the treatment time of patients contributing most to
the events (for example, consider a study where most patients are treated early but late
treatment patients are included, and all mortality events were observed with late
treatment patients).
This is a living analysis and is updated regularly.
We received no funding, this research is done in our spare time.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/dmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Abbas, 4/15/2026, retrospective, Pakistan, peer-reviewed, mean age 44.7, 11 authors, study period February 2023 - August 2024. | risk of long COVID, 26.0% lower, RR 0.74, p = 0.11, all groups combined. |
| risk of long COVID, 31.0% lower, OR 0.69, p = 0.003, cutoff 20 ng/mL, inverted to make OR<1 favor high D levels (≥20 ng/mL), neuropsychiatric, RR approximated with OR. | |
| risk of long COVID, 56.5% lower, OR 0.43, p = 0.001, cutoff 20 ng/mL, inverted to make OR<1 favor high D levels (≥20 ng/mL), musculoskeletal, RR approximated with OR. | |
| risk of long COVID, 2.0% lower, OR 0.98, p = 0.04, cutoff 20 ng/mL, inverted to make OR<1 favor high D levels (≥20 ng/mL), other, RR approximated with OR. | |
| Abdollahi, 12/12/2020, retrospective, Iran, peer-reviewed, 7 authors. | risk of case, 53.9% lower, RR 0.46, p = 0.001, high D levels 108, low D levels 294, >30ng/ml. |
| Abdrabbo AlYafei, 12/5/2022, retrospective, Qatar, peer-reviewed, mean age 19.0, 5 authors. | risk of case, 23.2% lower, OR 0.77, p < 0.001, cutoff 10ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥10ng/mL), case control OR, severe deficiency vs. optimal, multivariable. |
| risk of case, 21.5% lower, OR 0.78, p < 0.001, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), case control OR, mild/moderate deficiency vs. optimal, multivariable. | |
| Abdulrahman, 4/17/2023, retrospective, United Kingdom, peer-reviewed, mean age 69.0, 7 authors, study period April 2020 - May 2021. | risk of death, 90.1% lower, OR 0.10, p = 0.048, high D levels (≥25nmol/L) 76, low D levels (<25nmol/L) 5, adjusted per study, inverted to make OR<1 favor high D levels (≥25nmol/L), multivariable, RR approximated with OR. |
| risk of progression, 82.5% lower, OR 0.18, p = 0.09, high D levels (≥25nmol/L) 76, low D levels (<25nmol/L) 5, adjusted per study, inverted to make OR<1 favor high D levels (≥25nmol/L), hospitalization, ICU, or death, multivariable, RR approximated with OR. | |
| Abrishami, 10/30/2020, retrospective, Iran, peer-reviewed, mean age 55.2, 7 authors. | risk of death, 75.9% lower, RR 0.24, p = 0.04, high D levels (≥25ng/mL) 3 of 47 (6.4%), low D levels (<25ng/mL) 9 of 26 (34.6%), NNT 3.5, adjusted per study, inverted to make RR<1 favor high D levels (≥25ng/mL), Cox model 2. |
| Afaghi, 10/12/2021, retrospective, Iran, peer-reviewed, 7 authors. | risk of death, 55.0% lower, RR 0.45, p = 0.002, high D levels 97 of 537 (18.1%), low D levels 51 of 109 (46.8%), NNT 3.5, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL, multivariate. |
| risk of mechanical ventilation, 55.9% lower, RR 0.44, p < 0.001, high D levels 89 of 537 (16.6%), low D levels 41 of 109 (37.6%), NNT 4.8, >20ng/mL, unadjusted. | |
| risk of ICU admission, 34.1% lower, RR 0.66, p < 0.001, high D levels 211 of 537 (39.3%), low D levels 65 of 109 (59.6%), NNT 4.9, >20ng/mL, unadjusted. | |
| Al-Jarallah, 6/20/2021, retrospective, Kuwait, peer-reviewed, 20 authors. | risk of death, 88.3% higher, RR 1.88, p = 0.45, high D levels 8 of 120 (6.7%), low D levels 9 of 119 (7.6%), odds ratio converted to relative risk. |
| Al-Salman, 7/29/2021, retrospective, Bahrain, peer-reviewed, 5 authors. | risk of ICU admission, 44.4% lower, OR 0.56, p = 0.03, high D levels (≥50nmol/L) 113, low D levels (<50nmol/L) 337, inverted to make OR<1 favor high D levels (≥50nmol/L), multinomial regression, RR approximated with OR. |
| Alguwaihes, 12/5/2020, retrospective, Saudi Arabia, peer-reviewed, 10 authors. | risk of death, 85.7% lower, RR 0.14, p = 0.007, high D levels 111, low D levels 328, inverted to make RR<1 favor high D levels, >12.5 nmol/L. |
| AlKhafaji, 1/31/2022, retrospective, Saudi Arabia, peer-reviewed, mean age 56.8, 16 authors, study period January 2021 - August 2021. | risk of death, 38.6% lower, RR 0.61, p = 0.50, high D levels (≥20ng/mL) 2 of 76 (2.6%), low D levels (<20ng/mL) 13 of 127 (10.2%), inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk. |
| risk of mechanical ventilation, 31.0% lower, RR 0.69, p = 0.51, high D levels (≥20ng/mL) 2 of 76 (2.6%), low D levels (<20ng/mL) 13 of 127 (10.2%), inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk. | |
| risk of ICU admission, 41.8% lower, RR 0.58, p = 0.20, high D levels (≥20ng/mL) 2 of 76 (2.6%), low D levels (<20ng/mL) 13 of 127 (10.2%), inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk. | |
| Allami, 11/8/2022, retrospective, Iraq, peer-reviewed, 6 authors. | risk of hospitalization, 92.5% lower, OR 0.07, p < 0.001, high D levels (≥10ng/mL) 91, low D levels (<10ng/mL) 80, adjusted per study, inverted to make OR<1 favor high D levels (≥10ng/mL), case control OR, multivariable. |
| Almacioglu, 5/13/2026, retrospective, Turkey, peer-reviewed, 3 authors. | risk of case, 52.9% lower, RR 0.47, p < 0.001, high D levels (≥20 ng/mL) 14 of 39 (35.9%), low D levels (<12 ng/mL) 32 of 42 (76.2%), NNT 2.5. |
| Alpcan, 8/10/2021, retrospective, Turkey, peer-reviewed, 3 authors. | risk of case, 73.0% lower, OR 0.27, p < 0.001, high D levels 42 of 75 (56.0%) cases, 66 of 80 (82.5%) controls, NNT 3.2, case control OR, >20ng/mL. |
| AlSafar, 5/19/2021, retrospective, United Arab Emirates, peer-reviewed, 8 authors. | risk of death, 59.3% lower, RR 0.41, p = 0.048, high D levels 16 of 337 (4.7%), low D levels 10 of 127 (7.9%), adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, ≥12ng/mL. |
| risk of severe case, 33.2% lower, RR 0.67, p = 0.005, high D levels 337, low D levels 127, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, ≥12ng/mL. | |
| Alzahrani (B), 6/23/2022, retrospective, Saudi Arabia, peer-reviewed, mean age 54.3, 9 authors, study period March 2020 - July 2021. | risk of death, 42.5% lower, OR 0.57, p = 0.46, high D levels (≥25ng/mL) 179, low D levels (<25ng/mL) 78, adjusted per study, inverted to make OR<1 favor high D levels (≥25ng/mL), multivariable, RR approximated with OR. |
| risk of ICU admission, 7.4% lower, OR 0.93, p = 0.80, high D levels (≥25ng/mL) 179, low D levels (<25ng/mL) 78, adjusted per study, inverted to make OR<1 favor high D levels (≥25ng/mL), multivariable, RR approximated with OR. | |
| Amin, 1/7/2021, retrospective, population-based cohort, United Kingdom, peer-reviewed, 2 authors. | COVID-19 severity, 32.3% higher, RR 1.32, p = 0.20, high D levels 140,898, low D levels 35,079, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, ≥50nmol/L vs. <25nmol/L, MR Egger, baseline risk approximated with overall risk. |
| risk of case, 7.6% higher, RR 1.08, p = 0.14, high D levels 140,898, low D levels 35,079, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, ≥50nmol/L vs. <25nmol/L, MR Egger, baseline risk approximated with overall risk. | |
| Angelidi, 1/9/2021, retrospective, USA, peer-reviewed, 8 authors. | risk of death, 88.0% lower, RR 0.12, p = 0.01, high D levels 6 of 65 (9.2%), low D levels 20 of 79 (25.3%), NNT 6.2, adjusted per study, >30ng/mL, supplementary table 2, multivariable logistic regression model 5. |
| Anjum, 7/31/2020, prospective, Pakistan, peer-reviewed, 6 authors, study period March 2020 - June 2020, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 62.5% lower, RR 0.38, p = 0.02, high D levels (≥25nmol/L) 8 of 80 (10.0%), low D levels (<25nmol/L) 16 of 60 (26.7%), NNT 6.0. |
| Ansari, 12/31/2020, prospective, Pakistan, peer-reviewed, 6 authors, study period 1 March, 2020 - 31 August, 2020, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 86.0% lower, RR 0.14, p = 0.02, high D levels (≥25nmol/L) 2 of 68 (2.9%), low D levels (<25nmol/L) 12 of 57 (21.1%), NNT 5.5. |
| Arabadzhiyska, 2/28/2023, retrospective, Bulgaria, peer-reviewed, mean age 53.7, 2 authors, study period October 2021 - December 2021. | risk of severe case, 29.8% lower, RR 0.70, p = 0.16, high D levels (≥20ng/ml) 16 of 44 (36.4%), low D levels (<20ng/ml) 29 of 56 (51.8%), NNT 6.5. |
| Arabi, 1/22/2023, retrospective, Iran, peer-reviewed, 7 authors. | risk of death, 40.0% lower, RR 0.60, p = 0.28, high D levels (≥20ng/mL) 6 of 30 (20.0%), low D levels (<20ng/mL) 13 of 39 (33.3%), NNT 7.5. |
| risk of ICU admission, 39.3% lower, RR 0.61, p = 0.20, high D levels (≥20ng/mL) 7 of 30 (23.3%), low D levels (<20ng/mL) 15 of 39 (38.5%), NNT 6.6. | |
| risk of AKI, 42.2% lower, RR 0.58, p = 0.13, high D levels (≥20ng/mL) 8 of 30 (26.7%), low D levels (<20ng/mL) 18 of 39 (46.2%), NNT 5.1. | |
| Arambepola, 3/28/2024, retrospective, India, preprint, 6 authors. | risk of case, 47.4% lower, OR 0.53, p = 0.27, high D levels (≥50nmol/L) 17 of 104 (16.3%) cases, 30 of 104 (28.8%) controls, NNT 5.6, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), case control OR. |
| Asgari, 11/21/2021, retrospective, Iran, peer-reviewed, 6 authors, study period 21 May, 2020 - 4 September, 2020. | risk of death, 72.5% lower, OR 0.27, p = 0.03, cutoff 25ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥25ng/mL), RR approximated with OR. |
| risk of progression, 65.6% lower, OR 0.34, p = 0.02, cutoff 25ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥25ng/mL), RR approximated with OR. | |
| Asghar, 11/10/2021, retrospective, Pakistan, peer-reviewed, 8 authors. | risk of death, 53.1% lower, HR 0.47, p = 0.046, high D levels (≥10ng/mL) 73, low D levels (<10ng/mL) 18, inverted to make HR<1 favor high D levels (≥10ng/mL), multivariate Cox regression. |
| risk of mechanical ventilation, 19.4% lower, HR 0.81, p = 0.32, high D levels (≥10ng/mL) 5 of 73 (6.8%), low D levels (<10ng/mL) 6 of 18 (33.3%), NNT 3.8, adjusted per study, inverted to make HR<1 favor high D levels (≥10ng/mL), multivariate Cox regression. | |
| risk of ICU admission, 32.9% lower, HR 0.67, p = 0.54, high D levels (≥10ng/mL) 73, low D levels (<10ng/mL) 18, inverted to make HR<1 favor high D levels (≥10ng/mL), multivariate Cox regression. | |
| Atanasovska, 11/2/2021, retrospective, North Macedonia, peer-reviewed, 8 authors. | risk of death, 40.7% lower, RR 0.59, p = 0.68, high D levels (≥30ng/mL) 2 of 9 (22.2%), low D levels (<30ng/mL) 9 of 24 (37.5%), NNT 6.5. |
| risk of severe case, 59.0% lower, RR 0.41, p = 0.13, high D levels (≥30ng/mL) 2 of 9 (22.2%), low D levels (<30ng/mL) 13 of 24 (54.2%), NNT 3.1. | |
| Athanassiou, 9/15/2023, prospective, Greece, peer-reviewed, 9 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 47.9% lower, RR 0.52, p = 0.39, high D levels (≥10ng/mL) 5 of 64 (7.8%), low D levels (<10ng/mL) 3 of 20 (15.0%), NNT 14. |
| risk of death, 43.0% lower, RR 0.57, p = 0.70, high D levels (≥20ng/mL) 2 of 31 (6.5%), low D levels (<20ng/mL) 6 of 53 (11.3%), NNT 21. | |
| Baktash, 8/27/2020, prospective, United Kingdom, peer-reviewed, 8 authors. | risk of death, 28.6% lower, RR 0.71, p = 0.50, high D levels 4 of 31 (12.9%), low D levels 6 of 39 (15.4%), adjusted per study, inverted to make RR<1 favor high D levels, >30nmol/L. |
| Barassi, 1/25/2021, retrospective, Italy, peer-reviewed, 8 authors. | risk of death, 64.9% lower, RR 0.35, p = 0.44, high D levels 1 of 31 (3.2%), low D levels 8 of 87 (9.2%), NNT 17, >20ng/mL. |
| risk of mechanical ventilation, 64.9% lower, RR 0.35, p = 0.15, high D levels 2 of 31 (6.5%), low D levels 16 of 87 (18.4%), NNT 8.4, >20ng/mL. | |
| Barrett, 8/9/2022, prospective, Ireland, peer-reviewed, mean age 56.0, 19 authors, study period March 2020 - April 2021. | risk of death, 78.4% lower, OR 0.22, p = 0.006, high D levels (≥30nmol/L) 144, low D levels (<30nmol/L) 88, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/L), multivariable, RR approximated with OR. |
| risk of ICU admission, 15.3% lower, OR 0.85, p = 0.63, high D levels (≥30nmol/L) 144, low D levels (<30nmol/L) 88, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/L), multivariable, RR approximated with OR. | |
| risk of progression, 52.6% lower, OR 0.47, p = 0.12, high D levels (≥30nmol/L) 144, low D levels (<30nmol/L) 88, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/L), extended oxygen requirement, multivariable, RR approximated with OR. | |
| Basaran, 2/12/2021, retrospective, Turkey, peer-reviewed, 6 authors. | risk of severe case, 68.6% lower, RR 0.31, p = 0.005, high D levels 82 of 119 (68.9%), low D levels 80 of 85 (94.1%), NNT 4.0, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >10μg/L, per standard deviation increase in levels. |
| Basińska-Lewandowska, 3/24/2023, retrospective, Poland, peer-reviewed, 5 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of case, 58.3% lower, RR 0.42, p = 0.02, high D levels (≥12ng/mL) 20 of 109 (18.3%), low D levels (<12ng/mL) 11 of 25 (44.0%), NNT 3.9. |
| Batur, 12/26/2022, retrospective, Turkey, peer-reviewed, 2 authors, study period March 2020 - June 2021, excluded in exclusion analyses: unadjusted differences between groups. | risk of death, 71.9% lower, RR 0.28, p < 0.001, high D levels (≥20ng/mL) 17 of 76 (22.4%), low D levels (<20ng/mL) 94 of 118 (79.7%), NNT 1.7. |
| secondary infection, 23.3% lower, RR 0.77, p = 0.03, high D levels (≥20ng/mL) 40 of 76 (52.6%), low D levels (<20ng/mL) 81 of 118 (68.6%), NNT 6.2, growth in culture. | |
| Baykal, 5/30/2022, retrospective, Turkey, peer-reviewed, 2 authors, study period 1 April, 2020 - 1 March, 2021, dosage 300,000IU single dose. | risk of death, 8.0% higher, RR 1.08, p = 0.80, high D levels (≥20ng/mL) 11 of 20 (55.0%), low D levels (<20ng/mL) 28 of 55 (50.9%), outcome based on serum levels. |
| risk of ICU admission, 4.8% lower, RR 0.95, p = 1.00, high D levels (≥20ng/mL) 9 of 20 (45.0%), low D levels (<20ng/mL) 26 of 55 (47.3%), NNT 44, outcome based on serum levels. | |
| risk of progression, 6.1% lower, RR 0.94, p = 0.77, high D levels (≥20ng/mL) 14 of 20 (70.0%), low D levels (<20ng/mL) 41 of 55 (74.5%), NNT 22, severe/critical, outcome based on serum levels. | |
| Bayrak, 4/5/2023, retrospective, Turkey, peer-reviewed, mean age 19.0, 8 authors, study period November 2020 - January 2021. | risk of moderate/severe case, 26.5% lower, RR 0.73, p = 1.00, high D levels (≥20ng/mL) 3 of 49 (6.1%), low D levels (<20ng/mL) 2 of 24 (8.3%), NNT 45. |
| risk of case, 33.4% lower, OR 0.67, p = 0.23, high D levels (≥20ng/mL) 41 of 73 (56.2%) cases, 50 of 76 (65.8%) controls, NNT 9.9, case control OR. | |
| Bayramoğlu, 3/31/2021, retrospective, Turkey, peer-reviewed, 7 authors. | risk of moderate/severe case, 69.5% lower, RR 0.30, p = 0.03, high D levels 10 of 60 (16.7%), low D levels 24 of 43 (55.8%), NNT 2.6, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >12 ng/mL, multivariate logistic regression. |
| Begum (B), 9/29/2025, retrospective, Saudi Arabia, peer-reviewed, 5 authors. | risk of long COVID, 59.2% lower, OR 0.41, p = 0.01, high D levels 176, low D levels 248, RR approximated with OR. |
| Bennouar, 1/12/2021, prospective, Algeria, peer-reviewed, 5 authors. | risk of death, 85.5% lower, RR 0.14, p = 0.002, high D levels 4 of 30 (13.3%), low D levels 15 of 32 (46.9%), NNT 3.0, adjusted per study, inverted to make RR<1 favor high D levels, >30μg/l vs. <10μg/l, proportional Cox regression. |
| risk of death, 63.0% lower, RR 0.37, p = 0.10, high D levels 4 of 30 (13.3%), low D levels 14 of 35 (40.0%), NNT 3.7, adjusted per study, inverted to make RR<1 favor high D levels, >30μg/l vs. 10-19μg/l, proportional Cox regression. | |
| risk of death, 23.1% lower, RR 0.77, p = 0.73, high D levels 4 of 30 (13.3%), low D levels 4 of 23 (17.4%), NNT 25, adjusted per study, inverted to make RR<1 favor high D levels, >30μg/l vs. 20-29μg/l, proportional Cox regression. | |
| Bianconi, 7/1/2021, prospective, Italy, peer-reviewed, 12 authors. | risk of death, 17.5% lower, HR 0.82, p = 0.58, high D levels (≥12ng/ml) 94, low D levels (<12ng/ml) 106, model 3, Table S2, Cox proportional hazards. |
| risk of death, 13.9% lower, HR 0.86, p = 0.73, high D levels (≥20ng/ml) 40, low D levels (<20ng/ml) 160, model 3, Table S2, Cox proportional hazards. | |
| risk of death/ICU, 15.9% lower, HR 0.84, p = 0.53, high D levels (≥12ng/ml) 94, low D levels (<12ng/ml) 106, model 3, Cox proportional hazards. | |
| risk of death/ICU, 10.9% lower, HR 0.89, p = 0.73, high D levels (≥20ng/ml) 40, low D levels (<20ng/ml) 160, model 3, Cox proportional hazards. | |
| Bogliolo, 7/5/2022, prospective, Italy, peer-reviewed, median age 73.0, 16 authors, study period March 2020 - August 2020. | risk of death, 15.3% lower, HR 0.85, p = 0.29, cutoff 20ng/mL, inverted to make HR<1 favor high D levels (≥20ng/mL). |
| Bogomaz, 8/24/2023, retrospective, Ukraine, peer-reviewed, median age 62.0, 2 authors. | risk of death, 70.0% lower, RR 0.30, p = 0.24, high D levels (≥30ng/ml) 1 of 28 (3.6%), low D levels (<30ng/ml) 5 of 42 (11.9%), NNT 12, inverted to make RR<1 favor high D levels (≥30ng/ml), odds ratio converted to relative risk. |
| risk of mechanical ventilation, 75.0% lower, RR 0.25, p = 0.23, high D levels (≥30ng/ml) 1 of 28 (3.6%), low D levels (<30ng/ml) 6 of 42 (14.3%), NNT 9.3. | |
| risk of progression, 62.5% lower, RR 0.38, p = 0.30, high D levels (≥30ng/ml) 2 of 28 (7.1%), low D levels (<30ng/ml) 8 of 42 (19.0%), NNT 8.4, critical case. | |
| risk of oxygen therapy, 27.0% lower, RR 0.73, p = 0.24, high D levels (≥30ng/ml) 10 of 28 (35.7%), low D levels (<30ng/ml) 28 of 42 (66.7%), NNT 3.2, adjusted per study, inverted to make RR<1 favor high D levels (≥30ng/ml), odds ratio converted to relative risk, multivariable. | |
| Božić, 6/20/2024, prospective, Serbia, peer-reviewed, median age 69.0, 4 authors, study period October 2021 - December 2021. | risk of death, 53.3% lower, OR 0.47, p = 0.007, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. |
| risk of ICU admission, 30.5% lower, OR 0.70, p = 0.21, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. | |
| Breslin, 8/17/2021, retrospective, Ireland, peer-reviewed, 4 authors. | risk of progression, 55.6% lower, OR 0.44, p = 0.03, high D levels (≥30nmol/l) 106, low D levels (<30nmol/l) 32, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/l), infiltrates on chest X-ray, multivariable, RR approximated with OR. |
| Bucurica, 3/6/2023, retrospective, Romania, peer-reviewed, mean age 55.2, 9 authors, study period 1 June, 2020 - 31 May, 2022. | risk of case, 27.6% lower, OR 0.72, p < 0.001, high D levels (≥20ng/mL) 7,958, low D levels (<20ng/mL) 3,224, inverted to make OR<1 favor high D levels (≥20ng/mL), RR approximated with OR. |
| risk of case, 7.4% higher, OR 1.07, p = 0.19, high D levels (≥30ng/mL) 4,367, low D levels (<30ng/mL) 6,815, inverted to make OR<1 favor high D levels (≥30ng/mL), RR approximated with OR. | |
| Bushnaq, 2/8/2022, retrospective, Saudi Arabia, peer-reviewed, 7 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of mechanical ventilation, 32.1% lower, RR 0.68, p = 0.27, high D levels (≥20ng/mL) 10 of 53 (18.9%), low D levels (<20ng/mL) 40 of 144 (27.8%), NNT 11, unadjusted. |
| risk of ICU admission, 3.9% lower, RR 0.96, p = 0.87, high D levels (≥20ng/mL) 23 of 53 (43.4%), low D levels (<20ng/mL) 65 of 144 (45.1%), NNT 57, unadjusted. | |
| Bychinin (B), 5/7/2021, retrospective, Russia, peer-reviewed, 5 authors, excluded in exclusion analyses: excessive unadjusted differences between groups. | risk of death, 36.2% lower, RR 0.64, p = 0.03, high D levels (≥10ng/mL) 16 of 38 (42.1%), low D levels (<10ng/mL) 31 of 47 (66.0%), NNT 4.2. |
| Campi, 6/14/2021, prospective, Italy, peer-reviewed, 21 authors, dosage not specified. | risk of death for severe patients, 24.3% lower, RR 0.76, p = 0.53, high D levels (≥20ng/ml) 6 of 39 (15.4%), low D levels (<20ng/ml) 13 of 64 (20.3%), NNT 20, hospitalized patients, outcome based on serum levels. |
| risk of ICU for severe patients, 53.1% lower, RR 0.47, p < 0.001, high D levels (≥20ng/ml) 12 of 39 (30.8%), low D levels (<20ng/ml) 42 of 64 (65.6%), NNT 2.9, hospitalized patients, outcome based on serum levels. | |
| Cannata-Andía, 2/18/2022, prospective, multiple countries, peer-reviewed, median age 59.0, 22 authors, study period 4 April, 2020 - 22 April, 2021, dosage 100,000IU single dose, trial NCT04552951 (history) (COVID-VIT-D), excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 117.0% higher, RR 2.17, p = 0.20, high D levels 87, low D levels 96, >25 vs. ≤10 ng/mL, adjusted by demographics, comorbidities, and laboratory parameters, outcome based on serum levels. |
| risk of ICU admission, 65.0% lower, RR 0.35, p = 0.04, high D levels 87, low D levels 96, >25 vs. ≤10 ng/mL, adjusted by demographics, comorbidities, and laboratory parameters, outcome based on serum levels. | |
| risk of progression, 79.0% lower, RR 0.21, p = 0.003, high D levels 87, low D levels 96, pulmonary involvment at admission, >25 vs. ≤10 ng/mL, adjusted by demographics, comorbidities, and laboratory parameters, outcome based on serum levels. | |
| Cardoso, 6/11/2024, prospective, Brazil, preprint, 7 authors, study period April 2020 - February 2022. | severe pneumonia, 66.7% lower, OR 0.33, p < 0.001, high D levels (≥30ng/ml) 83 of 145 (57.2%) cases, 147 of 175 (84.0%) controls, NNT 3.0, adjusted per study, inverted to make OR<1 favor high D levels (≥30ng/ml), case control OR, deficient vs. sufficient, multivariable. |
| severe pneumonia, 50.0% lower, OR 0.50, p < 0.001, high D levels (≥30ng/mL) 83 of 245 (33.9%) cases, 147 of 279 (52.7%) controls, NNT 5.3, adjusted per study, inverted to make OR<1 favor high D levels (≥30ng/mL), case control OR, insufficient vs. sufficient, multivariable. | |
| Carpagnano, 8/9/2020, retrospective, Italy, peer-reviewed, 10 authors. | risk of death at day 26, 70.6% lower, RR 0.29, p = 0.0499, high D levels 5 of 34 (14.7%), low D levels 4 of 8 (50.0%), NNT 2.8, >30 ng/mL. |
| risk of death at day 10, 90.0% lower, RR 0.10, p = 0.02, high D levels 2 of 34 (5.9%), low D levels 4 of 8 (50.0%), NNT 2.3, adjusted per study, >30 ng/mL. | |
| Cereda (B), 11/1/2020, prospective, Italy, peer-reviewed, 13 authors. | risk of death, 120.0% higher, RR 2.20, p = 0.04, high D levels 10 of 30 (33.3%), low D levels 24 of 99 (24.2%), inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL. |
| risk of ICU admission, 86.7% lower, RR 0.13, p = 0.59, high D levels 0 of 30 (0.0%), low D levels 5 of 99 (5.1%), NNT 20, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| Cetin Ozbek, 3/24/2023, retrospective, Turkey, peer-reviewed, mean age 63.4, 6 authors, study period 1 August, 2021 - 31 October, 2021. | risk of death, 50.9% lower, RR 0.49, p = 0.07, high D levels (≥20ng/mL) 7 of 61 (11.5%), low D levels (<20ng/mL) 25 of 107 (23.4%), NNT 8.4. |
| risk of death, 3.0% lower, OR 0.97, p = 0.32, adjusted per study, continuous values, multivariable, RR approximated with OR. | |
| Chadda, 11/25/2024, retrospective, United Kingdom, peer-reviewed, 13 authors, study period 12 May, 2020 - 22 May, 2020. | recovery time, 7.1% lower, relative time 0.93, p = 0.49, high D levels (≥30 nmol/l) median 13.0 IQR 14.0 n=331, low D levels (<30 nmol/l) median 14.0 IQR 14.5 n=61, all symptoms. |
| risk of no recovery, 67.4% lower, OR 0.33, p = 0.002, high D levels (≥30 nmol/l) 331, low D levels (<30 nmol/l) 61, adjusted per study, inverted to make OR<1 favor high D levels (≥30 nmol/l), multivariable, body ache, RR approximated with OR. | |
| risk of no recovery, 52.1% lower, OR 0.48, p = 0.03, high D levels (≥30 nmol/l) 331, low D levels (<30 nmol/l) 61, adjusted per study, inverted to make OR<1 favor high D levels (≥30 nmol/l), multivariable, fatigue, RR approximated with OR. | |
| risk of progression, 27.2% lower, RR 0.73, p = 0.01, high D levels (≥30 nmol/l) 158 of 331 (47.7%), low D levels (<30 nmol/l) 40 of 61 (65.6%), NNT 5.6, >4 symptoms. | |
| Chan, 10/20/2024, retrospective, multiple countries, peer-reviewed, 3 authors, study period January 2022 - September 2024. | risk of death, 5.7% lower, HR 0.94, p = 0.42, high D levels (≥20ng/mL) 365 of 34,407 (1.1%), low D levels (<20ng/mL) 382 of 34,407 (1.1%), NNT 2024, inverted to make HR<1 favor high D levels (≥20ng/mL), Cox proportional hazards. |
| risk of progression, 4.8% lower, HR 0.95, p = 0.02, high D levels (≥20ng/mL) 4,181 of 34,407 (12.2%), low D levels (<20ng/mL) 4,345 of 34,407 (12.6%), NNT 210, inverted to make HR<1 favor high D levels (≥20ng/mL), death, hospitalization, critical care, Cox proportional hazards. | |
| risk of progression, 21.9% lower, HR 0.78, p < 0.001, high D levels (≥20ng/mL) 702 of 34,407 (2.0%), low D levels (<20ng/mL) 885 of 34,407 (2.6%), NNT 188, inverted to make HR<1 favor high D levels (≥20ng/mL), critical care, Cox proportional hazards. | |
| risk of hospitalization, 1.0% lower, HR 0.99, p = 0.80, high D levels (≥20ng/mL) 3,812 of 34,407 (11.1%), low D levels (<20ng/mL) 3,803 of 34,407 (11.1%), inverted to make HR<1 favor high D levels (≥20ng/mL), Cox proportional hazards. | |
| Chang, 7/4/2020, retrospective, USA, preprint, 13 authors, study period 9 March, 2020 - 14 June, 2020. | risk of case, 43.2% lower, OR 0.57, p < 0.001, cutoff 20ng/mL, inverted to make OR<1 favor high D levels (≥20ng/mL), Table S4, RR approximated with OR. |
| Charkowick, 5/5/2022, retrospective, USA, peer-reviewed, 10 authors, study period 1 January, 2020 - 5 February, 2021. | risk of death, 73.4% lower, OR 0.27, p = 0.02, high D levels 140, low D levels 68, adjusted per study, inverted to make OR<1 favor high D levels, multivariable, RR approximated with OR. |
| risk of ICU admission, 67.2% lower, OR 0.33, p = 0.001, high D levels 140, low D levels 68, adjusted per study, inverted to make OR<1 favor high D levels, multivariable, RR approximated with OR. | |
| Charla, 7/13/2022, retrospective, India, preprint, 8 authors, study period 1 April, 2020 - 30 April, 2021, excluded in exclusion analyses: excessive unadjusted differences between groups. | risk of death, 10.7% lower, RR 0.89, p = 0.74, high D levels (≥20ng/ml) 24 of 91 (26.4%), low D levels (<20ng/ml) 26 of 88 (29.5%), NNT 32. |
| Charoenngam, 3/8/2021, retrospective, USA, peer-reviewed, 6 authors. | risk of death, 34.1% lower, RR 0.66, p = 0.26, high D levels 12 of 100 (12.0%), low D levels 29 of 187 (15.5%), adjusted per study, odds ratio converted to relative risk, ≥30ng/mL. |
| risk of mechanical ventilation, 37.2% lower, RR 0.63, p = 0.17, high D levels 14 of 100 (14.0%), low D levels 34 of 187 (18.2%), adjusted per study, odds ratio converted to relative risk, ≥30ng/mL. | |
| risk of ICU admission, 23.1% lower, RR 0.77, p = 0.28, high D levels 25 of 100 (25.0%), low D levels 56 of 187 (29.9%), NNT 20, adjusted per study, odds ratio converted to relative risk, ≥30ng/mL. | |
| risk of death, 58.1% lower, RR 0.42, p = 0.05, high D levels 7 of 57 (12.3%), low D levels 25 of 79 (31.6%), NNT 5.2, adjusted per study, odds ratio converted to relative risk, >65 years old, ≥30ng/mL. | |
| Chen (E), 6/18/2025, retrospective, multiple countries, peer-reviewed, mean age 51.3, 6 authors, study period June 2022 - December 2023. | risk of death, 61.3% lower, RR 0.39, p = 0.007, high D levels 45,276, low D levels 45,276, both periods combined. |
| risk of death, 72.8% lower, OR 0.27, p < 0.001, high D levels 22,638, low D levels 22,638, inverted to make OR<1 favor high D levels, pre-Omicron, propensity score matching, RR approximated with OR. | |
| risk of death, 45.1% lower, OR 0.55, p < 0.001, high D levels 22,638, low D levels 22,638, inverted to make OR<1 favor high D levels, post-Omicron, propensity score matching, RR approximated with OR. | |
| Chen (F), 2/28/2023, retrospective, China, peer-reviewed, 9 authors, study period 1 June, 2022 - 5 July, 2022. | viral clearance, 40.0% improved, HR 0.60, p = 0.01, high D levels (≥41.07ng/mL) 52, low D levels (<27.5ng/mL) 53, adjusted per study, tertile 3 vs. tertile 1, multivariable, Cox proportional hazards. |
| Choi, 1/2/2024, retrospective, South Korea, peer-reviewed, mean age 55.7, 6 authors, study period April 2022 - December 2022. | risk of no recovery, 48.9% lower, HR 0.51, p = 0.002, high D levels (≥20ng/mL) 99, low D levels (<20ng/mL) 67, adjusted per study, multivariable. |
| risk of long COVID, 68.4% lower, HR 0.32, p = 0.001, high D levels (≥20ng/mL) 99, low D levels (<20ng/mL) 67, adjusted per study, inverted to make HR<1 favor high D levels (≥20ng/mL), multivariable. | |
| risk of hospitalization, 25.6% lower, RR 0.74, p = 0.48, high D levels (≥20ng/mL) 11 of 99 (11.1%), low D levels (<20ng/mL) 10 of 67 (14.9%), NNT 26, unadjusted. | |
| Connolly, 8/17/2021, retrospective, Ireland, peer-reviewed, 8 authors, study period March 2020 - May 2020. | risk of death, 90.4% lower, OR 0.10, p = 0.06, high D levels (≥30nmol/l) 65, low D levels (<30nmol/l) 49, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/l), multivariable, RR approximated with OR. |
| risk of oxygen therapy, 73.3% lower, OR 0.27, p = 0.048, high D levels (≥30nmol/l) 65, low D levels (<30nmol/l) 49, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/l), multivariable, RR approximated with OR. | |
| Cozier, 7/27/2021, prospective, USA, peer-reviewed, 6 authors. | risk of case, 38.6% lower, RR 0.61, p = 0.04, high D levels 94 of 1,601 (5.9%), low D levels 33 of 373 (8.8%), NNT 34, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL, multivariable. |
| Dana, 8/11/2022, retrospective, Iran, peer-reviewed, 16 authors, study period March 2020 - November 2020. | risk of death, 33.1% lower, RR 0.67, p = 0.29, high D levels (≥10ng/mL) 49 of 376 (13.0%), low D levels (<10ng/mL) 8 of 46 (17.4%), NNT 23, adjusted per study, inverted to make RR<1 favor high D levels (≥10ng/mL), odds ratio converted to relative risk, sufficiency vs. severe deficiency, multivariable. |
| risk of death, 15.7% lower, RR 0.84, p = 0.44, high D levels (≥20ng/mL) 49 of 376 (13.0%), low D levels (<20ng/mL) 30 of 197 (15.2%), NNT 46, adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, sufficiency vs. deficiency, multivariable. | |
| risk of severe case, no change, RR 1.00, p = 1.00, high D levels (≥10ng/mL) 59 of 376 (15.7%), low D levels (<10ng/mL) 7 of 46 (15.2%), adjusted per study, inverted to make RR<1 favor high D levels (≥10ng/mL), odds ratio converted to relative risk, sufficiency vs. severe deficiency, multivariable. | |
| risk of severe case, 11.6% lower, RR 0.88, p = 0.45, high D levels (≥20ng/mL) 59 of 376 (15.7%), low D levels (<20ng/mL) 35 of 197 (17.8%), NNT 48, adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, sufficiency vs. deficiency, multivariable. | |
| Davoudi, 5/18/2021, retrospective, Iran, peer-reviewed, 11 authors, study period February 2020 - March 2020, excluded in exclusion analyses: excessive unadjusted differences between groups. | risk of death, 12.3% higher, RR 1.12, p = 1.00, high D levels (≥30ng/mL) 2 of 57 (3.5%), low D levels (<30ng/mL) 3 of 96 (3.1%). |
| risk of mechanical ventilation, 15.8% lower, RR 0.84, p = 1.00, high D levels (≥30ng/mL) 1 of 57 (1.8%), low D levels (<30ng/mL) 2 of 96 (2.1%), NNT 304. | |
| risk of ICU admission, 27.8% lower, RR 0.72, p = 0.74, high D levels (≥30ng/mL) 3 of 57 (5.3%), low D levels (<30ng/mL) 7 of 96 (7.3%), NNT 49. | |
| risk of severe case, 68.4% higher, RR 1.68, p = 0.30, high D levels (≥30ng/mL) 9 of 57 (15.8%), low D levels (<30ng/mL) 9 of 96 (9.4%). | |
| Davran, 3/15/2023, retrospective, Turkey, peer-reviewed, mean age 53.6, 9 authors. | risk of death, 75.4% lower, RR 0.25, p = 0.02, high D levels (≥10ng/ml) 4 of 63 (6.3%), low D levels (<10ng/ml) 8 of 31 (25.8%), NNT 5.1. |
| De Smet, 11/25/2020, retrospective, Belgium, peer-reviewed, 5 authors. | risk of death, 70.1% lower, RR 0.30, p = 0.02, high D levels 7 of 77 (9.1%), low D levels 20 of 109 (18.3%), adjusted per study, odds ratio converted to relative risk, >20ng/mL. |
| Demir, 1/29/2021, retrospective, Turkey, peer-reviewed, 3 authors. | risk of severe case, 89.3% lower, RR 0.11, p < 0.001, high D levels 13, low D levels 99, ratio of the mean number of affected lung segments, >30ng/ml vs. ≤10ng/mL. |
| hospitalization time, 87.1% lower, relative time 0.13, p < 0.001, high D levels 13, low D levels 99, >30ng/ml vs. ≤10ng/mL. | |
| risk of case, 24.2% lower, RR 0.76, p = 0.18, high D levels 13 of 31 (41.9%), low D levels 99 of 179 (55.3%), NNT 7.5, >30ng/ml vs. ≤10ng/mL. | |
| Derakhshanian, 9/19/2021, retrospective, Iran, peer-reviewed, 11 authors. | risk of death, 44.8% lower, RR 0.55, p = 0.046, high D levels 148, low D levels 142, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, control prevalance approximated with overall prevalence. |
| risk of mechanical ventilation, 41.7% lower, RR 0.58, p = 0.09, high D levels 148, low D levels 142, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, control prevalance approximated with overall prevalence. | |
| risk of ICU admission, 37.3% lower, RR 0.63, p = 0.04, high D levels 148, low D levels 142, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, control prevalance approximated with overall prevalence. | |
| Devi, 4/15/2023, retrospective, India, peer-reviewed, mean age 47.0, 4 authors, study period August 2020 - August 2022. | risk of case, 98.0% lower, OR 0.02, p = 0.007, high D levels (≥10ng/mL) 69 of 88 (78.4%) cases, 88 of 88 (100.0%) controls, NNT 1.8, case control OR. |
| risk of case, 88.4% lower, OR 0.12, p < 0.001, high D levels (≥20ng/mL) 54 of 88 (61.4%) cases, 82 of 88 (93.2%) controls, NNT 2.2, case control OR. | |
| Değirmenci, 7/30/2024, retrospective, Turkey, peer-reviewed, mean age 29.3, 7 authors, study period March 2020 - January 2021. | risk of ICU admission, 50.6% lower, RR 0.49, p = 0.27, high D levels (≥20ng/ml) 3 of 36 (8.3%), low D levels (<20ng/ml) 15 of 89 (16.9%), NNT 12. |
| severe CT finding, 36.0% lower, RR 0.64, p = 0.53, high D levels (≥20ng/ml) 3 of 16 (18.8%), low D levels (<20ng/ml) 17 of 58 (29.3%), NNT 9.5. | |
| moderate/severe CT finding, 25.6% lower, RR 0.74, p = 0.25, high D levels (≥20ng/ml) 8 of 16 (50.0%), low D levels (<20ng/ml) 39 of 58 (67.2%), NNT 5.8. | |
| hospitalization time, 16.7% lower, relative time 0.83, p = 0.48, high D levels (≥20ng/ml) 36, low D levels (<20ng/ml) 89. | |
| di Filippo (D), 8/12/2021, retrospective, Italy, peer-reviewed, 8 authors. | risk of death, 10.7% lower, RR 0.89, p = 1.00, high D levels 5 of 28 (17.9%), low D levels 12 of 60 (20.0%), NNT 47, >20ng/mL. |
| risk of ICU admission, 41.6% lower, RR 0.58, p = 0.22, high D levels 6 of 28 (21.4%), low D levels 22 of 60 (36.7%), NNT 6.6, >20ng/mL. | |
| risk of severe case, 39.6% lower, RR 0.60, p = 0.04, high D levels 11 of 28 (39.3%), low D levels 39 of 60 (65.0%), NNT 3.9, >20ng/mL. | |
| Diaz-Curiel, 6/6/2021, retrospective, Spain, peer-reviewed, 8 authors. | risk of ICU admission, 73.2% lower, RR 0.27, p = 0.02, high D levels 3 of 214 (1.4%), low D levels 91 of 1,017 (8.9%), odds ratio converted to relative risk, >30ng/mL vs. <20ng/mL. |
| Dip, 6/25/2024, retrospective, Bangladesh, peer-reviewed, 9 authors, study period January 2021 - December 2021. | risk of severe case, 88.4% lower, OR 0.12, p = 0.003, high D levels (≥20 ng/ml) 46, low D levels (<20 ng/ml) 57, adjusted per study, inverted to make OR<1 favor high D levels (≥20 ng/ml), multivariable, RR approximated with OR. |
| Domènech-Montoliu, 3/5/2025, prospective, Spain, peer-reviewed, mean age 38.8, 17 authors, study period January 2020 - August 2023. | risk of case, 37.9% lower, HR 0.62, p = 0.02, high D levels (≥30 ng/ml) 169, low D levels (<30 ng/ml) 208, inverted to make HR<1 favor high D levels (≥30 ng/ml). |
| Doğan (B), 8/4/2022, prospective, Turkey, peer-reviewed, 5 authors, study period 1 July, 2021 - 30 October, 2021. | risk of case, 63.7% lower, OR 0.36, p = 0.003, high D levels (≥10ng/ml) 53 of 88 (60.2%) cases, 71 of 88 (80.7%) controls, NNT 4.1, case control OR. |
| Eden, 8/5/2021, retrospective, United Kingdom, peer-reviewed, 5 authors. | risk of death, 63.9% lower, RR 0.36, p = 0.10, high D levels (≥25nmol/L) 3 of 26 (11.5%), low D levels (<25nmol/L) 8 of 25 (32.0%), NNT 4.9. |
| risk of death, 92.9% lower, RR 0.07, p = 0.18, high D levels (≥50nmol/L) 0 of 8 (0.0%), low D levels (<50nmol/L) 11 of 43 (25.6%), NNT 3.9, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| Efe Iris, 12/30/2023, retrospective, Turkey, peer-reviewed, mean age 46.9, 8 authors. | risk of case, 59.2% lower, OR 0.41, p < 0.001, cutoff 18.4ng/mL, inverted to make OR<1 favor high D levels (≥18.4ng/mL), RR approximated with OR. |
| Faniyi, 10/6/2020, prospective, United Kingdom, preprint, 10 authors. | risk of seropositive, 28.8% lower, RR 0.71, p = 0.003, high D levels 170 of 331 (51.4%), low D levels 44 of 61 (72.1%), NNT 4.8, >30nmol/L. |
| Fatemi, 11/30/2021, prospective, Iran, peer-reviewed, 5 authors, study period 1 October, 2020 - 31 May, 2021. | risk of death, 42.0% lower, RR 0.58, p = 0.07, high D levels 18 of 139 (12.9%), low D levels 25 of 109 (22.9%), NNT 10, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, vitamin D measured prior to COVID-19, multivariate. |
| risk of death, 51.1% lower, RR 0.49, p = 0.02, high D levels 13 of 115 (11.3%), low D levels 30 of 133 (22.6%), NNT 8.9, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, vitamin D measured on admission, multivariate. | |
| risk of severe case, 37.9% lower, RR 0.62, p = 0.007, high D levels 38 of 139 (27.3%), low D levels 48 of 109 (44.0%), NNT 6.0, vitamin D measured prior to COVID-19. | |
| risk of severe case, 34.8% lower, RR 0.65, p = 0.02, high D levels 31 of 115 (27.0%), low D levels 55 of 133 (41.4%), NNT 6.9, vitamin D measured on admission. | |
| Faul, 6/30/2020, retrospective, Ireland, peer-reviewed, 9 authors. | risk of mechanical ventilation, 69.0% lower, RR 0.31, p = 0.03, high D levels 4 of 21 (19.0%), low D levels 8 of 12 (66.7%), NNT 2.1, adjusted per study, >30nmol/L. |
| Ferrer-Sánchez, 3/26/2022, retrospective, Spain, peer-reviewed, 7 authors. | risk of ICU admission, 81.8% lower, RR 0.18, p = 1.00, high D levels (≥20ng/mL) 0 of 9 (0.0%), low D levels (<20ng/mL) 4 of 73 (5.5%), NNT 18, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), excluded in exclusion analyses: unadjusted results with no group details. |
| risk of moderate/severe case, 88.7% lower, RR 0.11, p = 1.00, high D levels (≥20ng/mL) 0 of 9 (0.0%), low D levels (<20ng/mL) 7 of 73 (9.6%), NNT 10, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), excluded in exclusion analyses: unadjusted results with no group details. | |
| risk of case, 62.7% lower, OR 0.37, p = 0.01, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. | |
| Freitas (B), 3/27/2021, retrospective, Portugal, preprint, 36 authors. | risk of death, 41.2% lower, RR 0.59, p = 0.02, high D levels 23 of 179 (12.8%), low D levels 68 of 311 (21.9%), NNT 11, >20ng/mL. |
| Frish, 6/15/2023, retrospective, Israel, peer-reviewed, 7 authors, study period 1 February, 2020 - 31 December, 2020. | risk of case, 35.5% lower, OR 0.65, p = 0.001, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. |
| Galaznik, 5/28/2021, retrospective, USA, preprint, 6 authors. | risk of case, 35.1% lower, OR 0.65, p = 0.01, high D levels 13,903, low D levels 2,384, adjusted per study, inverted to make OR<1 favor high D levels, breast cancer patients, logistic regression, RR approximated with OR. |
| risk of case, 32.4% lower, OR 0.68, p = 0.045, high D levels 13,601, low D levels 1,318, adjusted per study, inverted to make OR<1 favor high D levels, prostate cancer patients, logistic regression, RR approximated with OR. | |
| García-Zendejas, 9/16/2024, retrospective, Mexico, peer-reviewed, mean age 53.4, 3 authors. | risk of death, 65.2% lower, OR 0.35, p = 0.18, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. |
| risk of ICU admission, 64.2% lower, OR 0.36, p = 0.15, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. | |
| risk of hospitalization, 83.7% lower, OR 0.16, p = 0.02, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. | |
| risk of case, 57.6% lower, OR 0.42, p = 0.26, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. | |
| Gaudio, 3/27/2021, retrospective, Italy, peer-reviewed, 6 authors. | risk of case, 79.3% lower, OR 0.21, p < 0.001, high D levels 27 of 50 (54.0%) cases, 85 of 100 (85.0%) controls, NNT 2.7, case control OR. |
| Gavioli, 2/19/2021, retrospective, USA, peer-reviewed, 4 authors. | risk of death, 4.7% higher, RR 1.05, p = 0.83, high D levels 80 of 260 (30.8%), low D levels 52 of 177 (29.4%), >20ng/ml. |
| risk of death, 44.8% lower, RR 0.55, p < 0.001, high D levels 102 of 376 (27.1%), low D levels 30 of 61 (49.2%), NNT 4.5, >10ng/ml. | |
| risk of oxygen therapy, 55.2% lower, RR 0.45, p < 0.001, high D levels 127 of 260 (48.8%), low D levels 116 of 177 (65.5%), NNT 6.0, adjusted per study, inverted to make RR<1 favor high D levels, >20ng/ml, multivariate. | |
| risk of hospitalization, 3.6% lower, RR 0.96, p = 0.41, high D levels 218 of 260 (83.8%), low D levels 154 of 177 (87.0%), NNT 32, >20ng/ml. | |
| Ghanei, 3/23/2022, prospective, Iran, peer-reviewed, 6 authors, study period 20 March, 2020 - 20 January, 2021. | risk of case, 42.1% lower, OR 0.58, p = 0.09, high D levels (≥20ng/ml) 58 of 90 (64.4%) cases, 72 of 95 (75.8%) controls, NNT 7.4, case control OR. |
| Gholi, 7/19/2022, prospective, Iran, peer-reviewed, 4 authors. | risk of death, 74.7% lower, HR 0.25, p < 0.001, high D levels 157, low D levels 38, inverted to make HR<1 favor high D levels, >30ng/mL vs. <20ng/mL, model 2, day 45. |
| risk of death, 39.8% lower, HR 0.60, p = 0.05, high D levels 157, low D levels 38, inverted to make HR<1 favor high D levels, >30ng/mL vs. <20ng/mL, ICU mortality, model 2. | |
| risk of mechanical ventilation, 44.9% higher, HR 1.45, p = 0.27, high D levels 157, low D levels 38, inverted to make HR<1 favor high D levels, >30ng/mL vs. <20ng/mL, model 2, day 45. | |
| Golabi, 8/26/2021, retrospective, Iran, peer-reviewed, 10 authors. | odds of symptoms, 90.0% lower, OR 0.10, p < 0.001, high D levels 34, low D levels 10, >30ng/mL vs. <20ng/mL, GEE regression, RR approximated with OR. |
| odds of symptoms, 81.0% lower, OR 0.19, p = 0.006, high D levels 34, low D levels 9, 20-30ng/mL vs. <20ng/mL, GEE regression, RR approximated with OR. | |
| risk of case, 71.7% lower, OR 0.28, p = 0.07, high D levels 34 of 44 (77.3%) cases, 36 of 39 (92.3%) controls, NNT 3.5, case control OR, >30ng/mL vs. <20ng/mL. | |
| Gonzalez, 3/13/2023, retrospective, Argentina, peer-reviewed, 10 authors. | risk of death, 66.1% lower, OR 0.34, p = 0.046, high D levels (≥12ng/ml) 129, low D levels (<12ng/ml) 35, adjusted per study, inverted to make OR<1 favor high D levels (≥12ng/ml), multivariable, RR approximated with OR. |
| González-Estevez, 7/7/2021, retrospective, Mexico, peer-reviewed, 6 authors. | risk of symptomatic case, 25.0% lower, RR 0.75, p = 0.04, high D levels (≥30ng/mL) 6 of 8 (75.0%), low D levels (<30ng/mL) 32 of 32 (100.0%), NNT 4.0. |
| Green, 11/7/2022, retrospective, Israel, peer-reviewed, 9 authors, study period 1 February, 2020 - 31 December, 2020. | risk of case, 18.7% lower, OR 0.81, p < 0.001, cutoff 30ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥30ng/mL), multivariable, RR approximated with OR. |
| Guðnadóttir, 3/4/2024, retrospective, Iceland, peer-reviewed, 4 authors, study period February 2020 - March 2021. | risk of death, 54.3% lower, OR 0.46, p = 0.15, high D levels (≥50nmol/L) 221, low D levels (<50nmol/L) 52, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), multivariable, RR approximated with OR. |
| risk of mechanical ventilation, 8.3% lower, OR 0.92, p = 0.86, high D levels (≥50nmol/L) 221, low D levels (<50nmol/L) 52, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), multivariable, RR approximated with OR. | |
| risk of ICU admission, 28.1% lower, OR 0.72, p = 0.43, high D levels (≥50nmol/L) 221, low D levels (<50nmol/L) 52, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), multivariable, RR approximated with OR. | |
| Gönen, 11/12/2021, retrospective, Turkey, peer-reviewed, 20 authors, dosage varies. | risk of death, 65.8% lower, RR 0.34, p = 0.62, high D levels (≥12ng/mL) 1 of 80 (1.2%), low D levels (<12ng/mL) 3 of 82 (3.7%), NNT 42, retrospective study. |
| risk of ICU admission, 16.9% lower, RR 0.83, p = 1.00, high D levels (≥12ng/mL) 4 of 77 (5.2%), low D levels (<12ng/mL) 5 of 80 (6.2%), NNT 95, retrospective study. | |
| hospital stay >8 days, 21.1% lower, RR 0.79, p = 0.11, high D levels (≥12ng/mL) 40 of 78 (51.3%), low D levels (<12ng/mL) 52 of 80 (65.0%), NNT 7.3, retrospective study. | |
| Hafez, 3/29/2022, retrospective, United Arab Emirates, peer-reviewed, mean age 43.0, 11 authors. | risk of death, 97.7% lower, RR 0.02, p = 0.02, high D levels (≥12ng/mL) 6 of 116 (5.2%), low D levels (<12ng/mL) 3 of 10 (30.0%), NNT 4.0, adjusted per study, inverted to make RR<1 favor high D levels (≥12ng/mL), odds ratio converted to relative risk, multivariable, model 2. |
| risk of death, 96.3% lower, RR 0.04, p = 0.04, high D levels (≥20ng/mL) 4 of 64 (6.2%), low D levels (<20ng/mL) 5 of 62 (8.1%), adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable, model 3. | |
| Hammam, 8/16/2024, retrospective, Egypt, peer-reviewed, 7 authors, study period December 2021 - April 2022. | risk of severe case, 51.6% lower, RR 0.48, p = 0.02, high D levels (≥25ng/mL) 11 of 49 (22.4%), low D levels (<25ng/mL) 19 of 41 (46.3%), NNT 4.2, excluded in exclusion analyses: unadjusted results with no group details. |
| risk of case, 95.5% lower, OR 0.04, p < 0.001, cutoff 14.8ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥14.8ng/mL), multivariable, RR approximated with OR. | |
| Hastie, 8/26/2020, retrospective, population-based cohort, database analysis, United Kingdom, peer-reviewed, 14 authors. | risk of death, 17.4% lower, RR 0.83, p = 0.31, cutoff 25nmol/L, adjusted per study, inverted to make RR<1 favor high D levels (≥25nmol/L), multivariable Cox. |
| risk of hospitalization, 9.1% lower, RR 0.91, p = 0.40, cutoff 25nmol/L, adjusted per study, inverted to make RR<1 favor high D levels (≥25nmol/L), multivariable Cox. | |
| Hemdan, 3/1/2022, retrospective, Saudi Arabia, peer-reviewed, 1 author, study period March 2020 - February 2021. | risk of death, 30.7% lower, RR 0.69, p = 0.02, high D levels 36 of 92 (39.1%), low D levels 57 of 101 (56.4%), NNT 5.8. |
| Hermawan, 3/28/2023, retrospective, Indonesia, peer-reviewed, survey, 5 authors, study period March 2022 - July 2022. | risk of symptomatic case, 70.6% lower, RR 0.29, p < 0.001, high D levels (≥10ng/ml) 10 of 34 (29.4%), low D levels (<10ng/ml) 13 of 13 (100.0%), NNT 1.4. |
| risk of symptomatic case, 45.6% lower, RR 0.54, p = 0.42, high D levels (≥20ng/ml) 2 of 7 (28.6%), low D levels (<20ng/ml) 21 of 40 (52.5%), NNT 4.2. | |
| Hernández, 10/27/2020, retrospective, Spain, peer-reviewed, mean age 60.9, 12 authors. | risk of combined death/ICU/ventilation, 83.0% lower, RR 0.17, p < 0.001, high D levels 35, low D levels 162, ≥20ng/mL risk of hospitalization * risk of death/ICU/ventilation | hospitalization. |
| risk of combined death/ICU/ventilation if hospitalized, 12.0% lower, RR 0.88, p = 0.86, high D levels 35, low D levels 162, ≥20ng/mL risk of death/ICU/ventilation | hospitalization. | |
| risk of hospitalization, 80.6% lower, RR 0.19, p < 0.001, ≥20ng/mL. | |
| Hogarth, 5/3/2023, retrospective, USA, peer-reviewed, median age 56.0, 9 authors, study period 1 January, 2021 - 8 November, 2021. | risk of case, 46.5% lower, OR 0.53, p < 0.001, high D levels (≥20ng/mL) 96,894, low D levels (<20ng/mL) 13,486, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), breakthrough case, multivariable, RR approximated with OR. |
| Hossain, 4/1/2025, retrospective, India, peer-reviewed, mean age 51.7, 5 authors, study period January 2021 - January 2022. | risk of severe case, 58.4% lower, RR 0.42, p = 0.002, high D levels (≥20 ng/ml) 8 of 33 (24.2%), low D levels (<20 ng/ml) 39 of 67 (58.2%), NNT 2.9. |
| Huang, 3/24/2023, retrospective, China, peer-reviewed, 5 authors, study period 14 June, 2021 - 1 April, 2022. | recovery time, 25.0% lower, relative time 0.75, p = 0.02, high D levels (≥20ng/ml) 28, low D levels (<20ng/ml) 18, relative time until resolution of pneumonia. |
| Hurst, 10/22/2021, prospective, United Kingdom, peer-reviewed, 23 authors. | risk of death, 68.4% lower, RR 0.32, p = 0.005, high D levels 68, low D levels 191, odds ratio converted to relative risk, >50nmol/l, multivariable, Supplementary Table 2, control prevalance approximated with overall prevalence. |
| risk of mechanical ventilation, 66.0% lower, RR 0.34, p = 0.004, high D levels 6 of 68 (8.8%), low D levels 61 of 191 (31.9%), NNT 4.3, odds ratio converted to relative risk, >50nmol/l, multivariable, Supplementary Table 2. | |
| Im, 8/11/2020, retrospective, South Korea, peer-reviewed, 6 authors. | risk of case, 73.1% lower, OR 0.27, p < 0.001, high D levels 13 of 50 (26.0%) cases, 85 of 150 (56.7%) controls, NNT 4.3, case control OR. |
| Infante, 2/18/2021, retrospective, Italy, peer-reviewed, 11 authors. | risk of death, 54.8% lower, RR 0.45, p = 0.046, high D levels 4 of 19 (21.1%), low D levels 55 of 118 (46.6%), NNT 3.9, >20ng/mL. |
| Israel, 9/20/2021, retrospective, population-based cohort, Israel, peer-reviewed, 9 authors, study period 1 March, 2020 - 31 October, 2020. | risk of severe case, 33.9% lower, OR 0.66, p < 0.001, high D levels 423 of 1,036 (40.8%) cases, 509 of 934 (54.5%) controls, NNT 7.3, adjusted per study, inverted to make OR<1 favor high D levels, case control OR, >75 nmol/L vs. <30 nmol/L, multivariable. |
| risk of case, 19.7% lower, OR 0.80, p < 0.001, high D levels 6,152 of 15,892 (38.7%) cases, 73,810 of 159,193 (46.4%) controls, NNT 39, adjusted per study, inverted to make OR<1 favor high D levels, case control OR, >75 nmol/L vs. <30 nmol/L, among COVID+ cases, multivariable. | |
| Ito, 5/6/2025, retrospective, Japan, peer-reviewed, 12 authors. | risk of case, 5.3% higher, HR 1.05, p = 0.89, cutoff <12 ng/mL and ≥20 ng/mL, inverted to make HR<1 favor high D levels (≥20 ng/mL). |
| Jain (B), 11/19/2020, prospective, India, peer-reviewed, 6 authors. | risk of death, 85.2% lower, RR 0.15, p = 0.001, high D levels 2 of 64 (3.1%), low D levels 19 of 90 (21.1%), NNT 5.6, >20ng/mL. |
| risk of ICU admission, 95.4% lower, RR 0.05, p < 0.001, high D levels 2 of 64 (3.1%), low D levels 61 of 90 (67.8%), NNT 1.5, >20ng/mL. | |
| Jalavu, 6/1/2023, prospective, South Africa, peer-reviewed, 16 authors, study period 29 October, 2020 - 10 February, 2021. | risk of death, 1.0% lower, HR 0.99, p = 0.97, high D levels (≥50nmol/L) 16 of 31 (51.6%), low D levels (<50nmol/L) 38 of 55 (69.1%), NNT 5.7, Kaplan-Meier. |
| Jazar, 12/25/2025, retrospective, Qatar, peer-reviewed, mean age 46.6, 7 authors. | risk of death, 20.6% lower, RR 0.79, p = 0.78, high D levels (≥20 ng/mL) 4 of 93 (4.3%), low D levels (<20 ng/mL) 11 of 203 (5.4%), NNT 89. |
| ICU time, 42.6% lower, relative time 0.57, p = 0.04, high D levels (≥20 ng/mL) mean 11.3 (±11.0) n=93, low D levels (<20 ng/mL) mean 19.7 (±22.6) n=203. | |
| hospitalization time, 20.0% lower, relative time 0.80, p = 0.23, high D levels (≥20 ng/mL) mean 14.8 (±8.8) n=93, low D levels (<20 ng/mL) mean 18.5 (±16.8) n=203. | |
| Jimenez, 7/26/2021, retrospective, Spain, peer-reviewed, 21 authors, study period 12 March, 2020 - 21 May, 2020, dosage paricalcitol 0.9μg weekly, excluded in exclusion analyses: many patients received vitamin D treatment. | risk of death, 7.7% higher, OR 1.08, p = 0.81, high D levels 50, low D levels 110, >30 vs. <20ng/ml, RR approximated with OR, outcome based on serum levels. |
| risk of mechanical ventilation, 47.5% lower, OR 0.53, p = 0.56, high D levels 50, low D levels 110, >30 vs. <20ng/ml, RR approximated with OR, outcome based on serum levels. | |
| risk of ICU admission, 12.2% lower, OR 0.88, p = 0.87, high D levels 50, low D levels 110, >30 vs. <20ng/ml, RR approximated with OR, outcome based on serum levels. | |
| risk of hospitalization, 0.8% lower, OR 0.99, p = 0.98, high D levels 50, low D levels 110, >30 vs. <20ng/ml, RR approximated with OR, outcome based on serum levels. | |
| Jude, 6/17/2021, retrospective, United Kingdom, peer-reviewed, 5 authors. | risk of hospitalization, 71.6% lower, RR 0.28, p < 0.001, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >25 nmol/L, control prevalence approximated with overall prevalence. |
| risk of hospitalization, 57.9% lower, RR 0.42, p < 0.001, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >50 nmol/L, control prevalence approximated with overall prevalence. | |
| Junior, 2/17/2022, prospective, Brazil, peer-reviewed, 6 authors, dosage not specified. | risk of mechanical ventilation, 84.4% lower, OR 0.16, p = 0.03, cutoff 40ng/dl, inverted to make OR<1 favor high D levels (≥40ng/dl), risk of mechanical ventilation for vitamin D levels >40ng/ml, RR approximated with OR, outcome based on serum levels. |
| Kalichuran, 4/26/2022, prospective, South Africa, peer-reviewed, survey, 4 authors, study period September 2020 - February 2021. | risk of symptomatic case, 60.0% lower, RR 0.40, p < 0.001, high D levels (≥20ng/mL) 56, low D levels (<20ng/mL) 44, inverted to make RR<1 favor high D levels (≥20ng/mL). |
| risk of symptomatic case, 58.2% lower, RR 0.42, p = 0.004, inverted to make RR<1 favor high D levels, higher sunlight exposure vs. lower sunlight exposure. | |
| Karahan, 10/5/2020, retrospective, Turkey, peer-reviewed, 2 authors. | risk of death, 82.5% lower, RR 0.17, p < 0.001, high D levels 5 of 46 (10.9%), low D levels 64 of 103 (62.1%), NNT 2.0, >20nmol/L. |
| Karonova (C), 3/2/2022, retrospective, Russia, peer-reviewed, 11 authors, study period 30 November, 2020 - 20 March, 2021. | risk of severe case, 22.5% lower, OR 0.78, p = 0.01, cutoff 11.4ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥11.4ng/mL), multivariable, RR approximated with OR. |
| Karonova (D), 8/29/2021, retrospective, Russia, peer-reviewed, 8 authors, study period April 2020 - December 2020. | risk of death, 77.8% lower, RR 0.22, p = 0.006, high D levels 8 of 96 (8.3%), low D levels 10 of 37 (27.0%), NNT 5.3, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >10ng/mL, logistic regression model 2. |
| risk of death, 84.8% lower, RR 0.15, p = 0.06, high D levels 1 of 43 (2.3%), low D levels 17 of 90 (18.9%), NNT 6.0, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL, logistic regression model 2. | |
| risk of severe case, 67.3% lower, RR 0.33, p = 0.005, high D levels 12 of 96 (12.5%), low D levels 13 of 37 (35.1%), NNT 4.4, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >10ng/mL, logistic regression model 2. | |
| risk of severe case, 53.2% lower, RR 0.47, p = 0.13, high D levels 4 of 43 (9.3%), low D levels 21 of 90 (23.3%), NNT 7.1, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL, logistic regression model 2. | |
| Karonova (E), 12/31/2020, retrospective, Russia, peer-reviewed, 3 authors. | risk of death, 79.4% lower, RR 0.21, p = 0.11, high D levels 1 of 23 (4.3%), low D levels 12 of 57 (21.1%), NNT 6.0, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/ml. |
| risk of severe case, 71.1% lower, RR 0.29, p = 0.05, high D levels 3 of 23 (13.0%), low D levels 22 of 57 (38.6%), NNT 3.9, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/ml. | |
| Katz, 12/4/2020, retrospective, population-based cohort, USA, peer-reviewed, 3 authors. | risk of case, 78.4% lower, RR 0.22, p < 0.001, high D levels 85 of 101,175 (0.1%), low D levels 87 of 31,950 (0.3%), NNT 531, adjusted per study, inverted to make RR<1 favor high D levels. |
| Kaufman, 9/17/2020, retrospective, population-based cohort, USA, peer-reviewed, median age 54.0, 5 authors. | risk of case, 53.0% lower, RR 0.47, p < 0.001, high D levels 12,321, low D levels 39,190, >55 ng/mL vs. <20 ng/mL. |
| Kaur, 11/30/2021, prospective, India, peer-reviewed, 5 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 89.8% lower, RR 0.10, p < 0.001, high D levels (≥10ng/mL) 5 of 64 (7.8%), low D levels (<10ng/mL) 13 of 17 (76.5%), NNT 1.5. |
| risk of mechanical ventilation, 90.3% lower, RR 0.10, p < 0.001, high D levels (≥10ng/mL) 4 of 64 (6.2%), low D levels (<10ng/mL) 11 of 17 (64.7%), NNT 1.7. | |
| Kazemi, 5/7/2022, retrospective, Iran, peer-reviewed, mean age 56.0, 4 authors. | risk of death, 75.8% lower, RR 0.24, p = 0.26, high D levels (≥30ng/mL) 1 of 75 (1.3%), low D levels (<30ng/mL) 7 of 127 (5.5%), NNT 24. |
| risk of severe case, 4.8% higher, RR 1.05, p = 1.00, high D levels (≥30ng/mL) 13 of 75 (17.3%), low D levels (<30ng/mL) 21 of 127 (16.5%). | |
| Khalil, 11/8/2022, retrospective, Iraq, peer-reviewed, 3 authors. | risk of case, 41.6% lower, OR 0.58, p = 0.27, high D levels (≥10ng/ml) 30 of 52 (57.7%) cases, 21 of 30 (70.0%) controls, NNT 8.2, case control OR. |
| Lau, 4/28/2020, retrospective, USA, preprint, 7 authors. | risk of ICU admission, 45.0% lower, RR 0.55, p = 0.29, high D levels 2 of 5 (40.0%), low D levels 11 of 15 (73.3%), NNT 3.0, >30ng/mL. |
| Li, 6/24/2025, prospective, China, peer-reviewed, 7 authors, study period 1 April, 2023 - 20 September, 2023. | risk of case, 5.9% lower, OR 0.94, p = 0.31, high D levels (≥20 ng/mL) 23, low D levels (<20 ng/mL) 39, adjusted per study, inverted to make OR<1 favor high D levels (≥20 ng/mL), case control OR, multivariable. |
| Li (B), 5/19/2021, retrospective, USA, peer-reviewed, 4 authors. | risk of case, 8.6% lower, RR 0.91, p = 0.24, high D levels 610 of 13,650 (4.5%), low D levels 290 of 4,498 (6.4%), adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL, Figure 2. |
| risk of case, 12.4% lower, RR 0.88, p = 0.07, high D levels 289 of 7,272 (4.0%), low D levels 611 of 10,876 (5.6%), adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >30ng/mL, Figure 2. | |
| Li (C), 1/11/2021, retrospective, population-based cohort, United Kingdom, peer-reviewed, 6 authors. | risk of hospitalization, 36.2% lower, RR 0.64, p < 0.001, NNT 932, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >25nmol/L. |
| risk of case, 29.5% lower, RR 0.71, p < 0.001, NNT 823, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >25nmol/L. | |
| Livingston, 4/2/2021, retrospective, United Kingdom, peer-reviewed, 7 authors. | risk of case, 50.9% lower, RR 0.49, p = 0.02, high D levels 16 of 52 (30.8%), low D levels 31 of 52 (59.6%), NNT 3.5, odds ratio converted to relative risk, >34.4nmol/L. |
| Lohia, 3/4/2021, retrospective, USA, peer-reviewed, 4 authors. | risk of death, 14.7% lower, RR 0.85, p = 0.56, high D levels 88, low D levels 95, odds ratio converted to relative risk, control prevalence approximated with overall prevalence, >30 ng/mL vs. <20 ng/mL, >30 ng/mL group size approximated. |
| risk of mechanical ventilation, 18.9% lower, RR 0.81, p = 0.48, high D levels 88, low D levels 95, odds ratio converted to relative risk, control prevalence approximated with overall prevalence, >30 ng/mL vs. <20 ng/mL, >30 ng/mL group size approximated. | |
| risk of ICU admission, 28.5% lower, RR 0.72, p = 0.17, high D levels 88, low D levels 95, odds ratio converted to relative risk, control prevalence approximated with overall prevalence, >30 ng/mL vs. <20 ng/mL, >30 ng/mL group size approximated. | |
| Luo, 11/13/2020, retrospective, China, peer-reviewed, median age 56.0, 5 authors. | risk of progression, 63.0% lower, RR 0.37, p = 0.01, high D levels 335, low D levels 560, >30nmol/L. |
| Ma, 12/3/2021, retrospective, USA, peer-reviewed, 16 authors, study period May 2020 - March 2021, dosage varies. | risk of hospitalization, 67.0% lower, OR 0.33, p = 0.15, high D levels 7,893, low D levels 7,823, adjusted per study, highest quintile vs. lowest quintile predicted vitamin D levels, model 3, supplemental table 3, multivariable, RR approximated with OR, outcome based on serum levels. |
| risk of symptomatic case, 9.0% lower, OR 0.91, p = 0.52, high D levels 7,893, low D levels 7,823, adjusted per study, highest quintile vs. lowest quintile predicted vitamin D levels, model 3, supplemental table 3, multivariable, RR approximated with OR, outcome based on serum levels. | |
| risk of case, 52.0% lower, OR 0.48, p = 0.01, high D levels 7,893, low D levels 7,823, adjusted per study, highest quintile vs. lowest quintile predicted vitamin D levels, model 3, supplemental table 3, multivariable, RR approximated with OR, outcome based on serum levels. | |
| Macaya, 10/21/2020, retrospective, Spain, peer-reviewed, 8 authors. | risk of severe case, 55.0% lower, RR 0.45, p = 0.07, high D levels 11 of 35 (31.4%), low D levels 20 of 45 (44.4%), NNT 7.7, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >20ng/mL. |
| Madar, 6/27/2025, retrospective, Lebanon, peer-reviewed, mean age 38.8, 4 authors, study period 23 November, 2021 - 30 April, 2022. | risk of case, 33.8% lower, OR 0.66, p = 0.15, high D levels (≥50 ng/mL) 143, low D levels (<30 ng/mL) 114, adjusted per study, inverted to make OR<1 favor high D levels (≥50 ng/mL), RR approximated with OR. |
| Manojlovic, 6/15/2023, retrospective, Serbia, peer-reviewed, mean age 57.6, 11 authors, excluded in exclusion analyses: unadjusted differences between groups. | risk of death, 89.9% lower, RR 0.10, p = 0.009, high D levels (≥30nmol/l) 1 of 41 (2.4%), low D levels (<30nmol/l) 8 of 33 (24.2%), NNT 4.6. |
| Martínez-Rodríguez, 3/31/2022, retrospective, Mexico, peer-reviewed, 5 authors. | risk of death, 52.2% lower, OR 0.48, p = 0.04, cutoff 20ng/mL, adjusted per study, multivariable, RR approximated with OR. |
| Matangkha, 9/18/2025, retrospective, Thailand, peer-reviewed, mean age 45.9, 4 authors. | risk of long COVID, 82.8% lower, OR 0.17, p < 0.001, high D levels (≥30 ng/mL) 48, low D levels (<20 ng/mL) 52, adjusted per study, inverted to make OR<1 favor high D levels (≥30 ng/mL), multivariable, RR approximated with OR. |
| Matin, 7/30/2021, retrospective, case control, Iran, peer-reviewed, 8 authors. | risk of case, 66.1% lower, OR 0.34, p < 0.001, inverted to make OR<1 favor high D levels, case control OR, >20ng/mL. |
| Mayurathan, 8/8/2023, retrospective, Sri Lanka, peer-reviewed, 11 authors. | risk of death, 98.2% higher, RR 1.98, p = 0.69, high D levels (≥20ng/mL) 8 of 113 (7.1%), low D levels (<20ng/mL) 1 of 28 (3.6%). |
| risk of severe case, 67.3% higher, RR 1.67, p = 0.32, high D levels (≥20ng/mL) 27 of 113 (23.9%), low D levels (<20ng/mL) 4 of 28 (14.3%). | |
| Mazziotti, 3/5/2021, retrospective, Italy, peer-reviewed, 11 authors, dosage varies. | risk of death, 2.4% lower, RR 0.98, p = 0.91, high D levels 187, low D levels 161, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >12ng/mL, control prevalance approximated with overall prevalence, outcome based on serum levels. |
| risk of acute hypoxemic respiratory failure, 37.0% lower, RR 0.63, p = 0.006, high D levels 72 of 187 (38.5%), low D levels 97 of 161 (60.2%), NNT 4.6, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >12ng/mL, outcome based on serum levels. | |
| Meltzer (B), 3/19/2021, retrospective, database analysis, USA, peer-reviewed, 6 authors. | risk of case, 34.6% lower, RR 0.65, p = 0.11, high D levels 61 of 1,097 (5.6%), low D levels 118 of 1,251 (9.4%), NNT 26, adjusted per study, inverted to make RR<1 favor high D levels, >40ng/mL vs. <20ng/mL, Table 2, Model 2. |
| Meltzer (C), 9/3/2020, retrospective, USA, peer-reviewed, 6 authors. | risk of case, 43.5% lower, RR 0.56, p = 0.02, high D levels 39 of 317 (12.3%), low D levels 32 of 172 (18.6%), NNT 16, adjusted per study, inverted to make RR<1 favor high D levels, >20ng/mL. |
| Mendy, 6/27/2020, retrospective, USA, preprint, 4 authors. | risk of death, 7.0% lower, RR 0.93, p = 0.89, high D levels 21 of 600 (3.5%), low D levels 5 of 89 (5.6%), inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. |
| risk of death/ICU, 16.7% lower, RR 0.83, p < 0.001, high D levels 68 of 600 (11.3%), low D levels 23 of 89 (25.8%), NNT 6.9, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. | |
| risk of ICU admission, 55.3% lower, RR 0.45, p = 0.008, high D levels 47 of 600 (7.8%), low D levels 18 of 89 (20.2%), NNT 8.1, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. | |
| risk of hospitalization, 15.1% lower, RR 0.85, p < 0.001, high D levels 171 of 600 (28.5%), low D levels 45 of 89 (50.6%), NNT 4.5, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. | |
| Merzon, 7/23/2020, retrospective, Israel, peer-reviewed, 7 authors. | risk of hospitalization, 46.4% lower, RR 0.54, p = 0.06, high D levels 79, low D levels 703, odds ratio converted to relative risk, >30ng/mL. |
| risk of case, 28.4% lower, RR 0.72, p < 0.001, high D levels 1,139, low D levels 6,668, odds ratio converted to relative risk, >30ng/mL. | |
| Mingiano, 7/30/2023, retrospective, Italy, peer-reviewed, 11 authors, study period November 2020 - February 2021, dosage calcifediol 450μg days 1-2, patients with deficiency only. | risk of death, 49.8% lower, RR 0.50, p = 0.005, cutoff 10ng/mL, outcome based on serum levels. |
| risk of death, 35.9% lower, RR 0.64, p = 0.04, cutoff 20ng/mL, outcome based on serum levels. | |
| Mirkarimi, 11/6/2024, retrospective, Iran, peer-reviewed, 7 authors, study period May 2022 - May 2023. | risk of moderate/severe case, 62.9% lower, RR 0.37, p < 0.001, high D levels (≥20 ng/mL) 117 of 345 (33.9%), low D levels (<20 ng/mL) 233 of 255 (91.4%), NNT 1.7, moderate/severe vs. mild. |
| Mohamed, 12/31/2024, retrospective, Egypt, peer-reviewed, mean age 5.5, 2 authors, study period 1 June, 2023 - 31 May, 2024. | risk of death, 44.7% lower, RR 0.55, p = 0.19, high D levels (≥10 ng/mL) 14 of 47 (29.8%), low D levels (<10 ng/mL) 7 of 13 (53.8%), NNT 4.2. |
| risk of death, 67.3% lower, RR 0.33, p = 0.003, high D levels (≥20 ng/mL) 6 of 33 (18.2%), low D levels (<20 ng/mL) 15 of 27 (55.6%), NNT 2.7. | |
| Monroy-Iglesias, 7/18/2025, retrospective, United Kingdom, peer-reviewed, mean age 56.0, 8 authors, study period March 2020 - October 2020. | risk of hospitalization, 26.5% lower, OR 0.74, p < 0.001, high D levels (≥50nmol/L) 69,746, low D levels (<25nmol/L) 19,358, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), deficiency, model B, multivariable, RR approximated with OR. |
| risk of hospitalization, 16.0% lower, OR 0.84, p < 0.001, high D levels (≥50nmol/L) 69,746, low D levels (<50nmol/L) 81,797, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), deficiency, model B, multivariable, RR approximated with OR. | |
| risk of case, 5.3% higher, OR 1.05, p = 0.03, high D levels (≥50nmol/L) 69,746, low D levels (<25nmol/L) 19,358, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), deficiency, model B, multivariable, RR approximated with OR. | |
| risk of case, 3.1% higher, OR 1.03, p = 0.05, high D levels (≥50nmol/L) 69,746, low D levels (<50nmol/L) 81,797, adjusted per study, inverted to make OR<1 favor high D levels (≥50nmol/L), deficiency, model B, multivariable, RR approximated with OR. | |
| Mostafa, 11/30/2022, retrospective, Egypt, peer-reviewed, 10 authors, study period November 2020 - December 2021, excluded in exclusion analyses: categorical results are unadjusted with significant differences between groups. | risk of death, 92.8% lower, RR 0.07, p < 0.001, high D levels (≥20ng/mL) 4 of 135 (3.0%), low D levels (<20ng/mL) 21 of 51 (41.2%), NNT 2.6, unadjusted, normal vs. deficiency. |
| risk of mechanical ventilation, 95.0% lower, RR 0.05, p < 0.001, high D levels (≥20ng/mL) 4 of 135 (3.0%), low D levels (<20ng/mL) 30 of 51 (58.8%), NNT 1.8, unadjusted, normal vs. deficiency. | |
| risk of ICU admission, 90.6% lower, RR 0.09, p < 0.001, high D levels (≥20ng/mL) 9 of 135 (6.7%), low D levels (<20ng/mL) 36 of 51 (70.6%), NNT 1.6, unadjusted, normal vs. deficiency. | |
| Nahhas, 10/1/2025, retrospective, Saudi Arabia, peer-reviewed, mean age 42.0, 5 authors. | risk of hospitalization, 51.2% lower, RR 0.49, p = 0.29, high D levels (≥50 nmol/l) 4 of 129 (3.1%), low D levels (<30 nmol/l) 11 of 173 (6.4%), NNT 31. |
| Najih, 1/31/2025, retrospective, Morocco, peer-reviewed, 7 authors, study period January 2021 - January 2022. | risk of symptomatic case, 53.1% lower, RR 0.47, p = 0.002, high D levels (≥20 ng/mL) 20 of 67 (29.9%), low D levels (<20 ng/mL) 21 of 33 (63.6%), NNT 3.0, symptomatic vs. mildly symptomatic/asymptomatic. |
| Nasiri, 6/30/2021, retrospective, Iran, peer-reviewed, 3 authors. | risk of death, 8.9% higher, OR 1.09, p = 0.89, high D levels (≥30ng/mL) 238, low D levels (<20ng/mL) 43, inverted to make OR<1 favor high D levels (≥30ng/mL), RR approximated with OR. |
| Neves, 6/14/2022, retrospective, Brazil, peer-reviewed, mean age 62.1, 7 authors, study period July 2020 - December 2020, excluded in exclusion analyses: excessive unadjusted differences between groups. | risk of death, 57.1% lower, RR 0.43, p = 0.046, high D levels (≥50nmol/L) 12 of 87 (13.8%), low D levels (<50nmol/L) 9 of 28 (32.1%), NNT 5.4. |
| risk of ICU admission, 19.5% higher, RR 1.20, p = 0.81, high D levels (≥50nmol/L) 26 of 87 (29.9%), low D levels (<50nmol/L) 7 of 28 (25.0%). | |
| Nguyen, 5/3/2022, retrospective, USA, peer-reviewed, 11 authors, study period 15 July, 2020 - 15 October, 2020. | risk of death, 81.1% lower, OR 0.19, p = 0.008, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), 25-OH-D3, multivariable, RR approximated with OR. |
| risk of mechanical ventilation, 52.8% lower, OR 0.47, p = 0.13, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), 25-OH-D3, multivariable, RR approximated with OR. | |
| risk of no hospital discharge, 74.0% lower, HR 0.26, p < 0.001, cutoff 20ng/mL, 25-OH-D3, Cox proportional hazards. | |
| Nimavat, 8/5/2021, retrospective, India, peer-reviewed, 5 authors. | risk of death, 50.4% lower, RR 0.50, p = 0.17, high D levels 13 of 131 (9.9%), low D levels 5 of 25 (20.0%), NNT 9.9, >10ng/mL, within cases. |
| risk of severe case, 67.6% lower, RR 0.32, p = 0.003, high D levels 17 of 131 (13.0%), low D levels 10 of 25 (40.0%), NNT 3.7, >10ng/mL, within cases. | |
| Orchard, 1/19/2021, retrospective, United Kingdom, peer-reviewed, 7 authors. | risk of ICU admission, 58.8% lower, RR 0.41, p = 0.001, high D levels 9 of 40 (22.5%), low D levels 41 of 75 (54.7%), NNT 3.1, all hospitalized patients, >50 nmol/L. |
| risk of death, 24.1% lower, RR 0.76, p = 1.00, high D levels 1 of 9 (11.1%), low D levels 6 of 41 (14.6%), NNT 28, ICU patients only, >50 nmol/L. | |
| risk of mechanical ventilation, 8.9% lower, RR 0.91, p = 0.70, high D levels 6 of 9 (66.7%), low D levels 30 of 41 (73.2%), NNT 15, ICU patients only, >50 nmol/L. | |
| Ortatatli, 2/14/2023, prospective, Turkey, peer-reviewed, 9 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 82.1% lower, RR 0.18, p = 0.09, cutoff 20ng/mL, inverted to make RR<1 favor high D levels (≥20ng/mL), 25(OH)D. |
| risk of death, 73.7% lower, RR 0.26, p = 0.04, cutoff 1ng/mL, inverted to make RR<1 favor high D levels (≥1ng/mL), 1,25(OH)2D. | |
| Ozturk, 5/16/2022, retrospective, Turkey, peer-reviewed, 6 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of severe case, 46.4% lower, RR 0.54, p = 0.10, high D levels (≥20ng/mL) 9 of 110 (8.2%), low D levels (<20ng/mL) 29 of 190 (15.3%), NNT 14. |
| Panagiotou, 6/30/2020, retrospective, United Kingdom, preprint, 12 authors. | risk of ICU admission, 52.0% lower, RR 0.48, p = 0.02, high D levels 8 of 44 (18.2%), low D levels 34 of 90 (37.8%), NNT 5.1, >50nmol/L. |
| Pande, 3/16/2022, retrospective, India, peer-reviewed, 7 authors, study period October 2020 - October 2021, excluded in exclusion analyses: unadjusted results with no group details. | risk of severe case, 93.4% lower, RR 0.07, p < 0.001, high D levels (≥20ng/ml) 7 of 116 (6.0%), low D levels (<20ng/ml) 85 of 93 (91.4%), NNT 1.2. |
| Parra-Ortega, 8/24/2021, prospective, Mexico, peer-reviewed, 9 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 98.7% lower, RR 0.01, p < 0.001, high D levels (≥20ng/dL) 0 of 15 (0.0%), low D levels (<20ng/dL) 63 of 79 (79.7%), NNT 1.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), unadjusted. |
| Pashaei, 11/18/2024, retrospective, Iran, peer-reviewed, 7 authors. | risk of severe case, 12.5% lower, RR 0.88, p = 0.76, high D levels (≥31 ng/mL) 19 of 38 (50.0%), low D levels (<31 ng/mL) 8 of 14 (57.1%), NNT 14. |
| Pavlyshyn, 4/5/2024, retrospective, Ukraine, peer-reviewed, 3 authors. | risk of severe case, 59.7% lower, RR 0.40, p = 0.13, high D levels (≥20ng/ml) 7 of 59 (11.9%), low D levels (<20ng/ml) 5 of 17 (29.4%), NNT 5.7, deficiency vs. other. |
| risk of case, 89.0% lower, OR 0.11, p = 0.13, high D levels (≥20ng/ml) 59 of 76 (77.6%) cases, 15 of 15 (100.0%) controls, NNT 4.9, case control OR. | |
| Pecina, 8/27/2021, retrospective, USA, peer-reviewed, 4 authors, dosage not specified. | risk of death, 35.9% lower, RR 0.64, p = 0.74, high D levels (≥20ng/mL) 6 of 77 (7.8%), low D levels (<20ng/mL) 1 of 15 (6.7%), inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable logistic regression, outcome based on serum levels. |
| risk of mechanical ventilation, 56.9% lower, RR 0.43, p = 0.22, high D levels (≥20ng/mL) 8 of 15 (53.3%), low D levels (<20ng/mL) 4 of 15 (26.7%), inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable logistic regression, outcome based on serum levels. | |
| risk of ICU admission, 13.1% higher, RR 1.13, p = 0.57, high D levels (≥20ng/mL) 54 of 77 (70.1%), low D levels (<20ng/mL) 9 of 15 (60.0%), inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable logistic regression, outcome based on serum levels. | |
| Pepkowitz, 9/29/2020, retrospective, USA, preprint, 7 authors. | risk of ICU admission, 55.8% lower, RR 0.44, p = 0.01, high D levels (≥20ng/mL) 9 of 24 (37.5%), low D levels (<20ng/mL) 11 of 13 (84.6%), NNT 2.1, inverted to make RR<1 favor high D levels (≥20ng/mL). |
| Perestiuk, 2/14/2025, prospective, Ukraine, peer-reviewed, 5 authors, study period September 2022 - March 2024. | risk of long COVID, 54.3% lower, OR 0.46, p = 0.03, high D levels 108, low D levels 54, inverted to make OR<1 favor high D levels, RR approximated with OR. |
| Pietzner, 7/8/2024, retrospective, United Kingdom, peer-reviewed, 9 authors. | risk of death, 55.4% lower, HR 0.45, p < 0.001, cutoff 25nmol/L, inverted to make HR<1 favor high D levels (≥25nmol/L), Cox proportional hazards. |
| risk of hospitalization, 52.6% lower, HR 0.47, p < 0.001, cutoff 25nmol/L, inverted to make HR<1 favor high D levels (≥25nmol/L), Cox proportional hazards. | |
| severe respiratory failure, 24.8% lower, HR 0.75, p = 0.05, cutoff 25nmol/L, inverted to make HR<1 favor high D levels (≥25nmol/L), Cox proportional hazards. | |
| risk of long COVID, 56.1% lower, HR 0.44, p < 0.001, cutoff 25nmol/L, inverted to make HR<1 favor high D levels (≥25nmol/L), Cox proportional hazards. | |
| Pimental, 5/31/2021, retrospective, Brazil, peer-reviewed, 3 authors. | risk of death, 29.4% lower, RR 0.71, p = 1.00, high D levels 3 of 17 (17.6%), low D levels 2 of 8 (25.0%), NNT 14, >20ng/mL. |
| Protas, 4/6/2023, retrospective, Kazakhstan, peer-reviewed, survey, 6 authors, study period October 2022 - November 2022. | risk of case, 76.6% lower, OR 0.23, p = 0.06, high D levels (≥10ng/ml) 68 of 88 (77.3%) cases, 29 of 31 (93.5%) controls, NNT 4.8, case control OR. |
| risk of case, 46.2% lower, OR 0.54, p = 0.17, high D levels (≥20ng/ml) 50 of 88 (56.8%) cases, 22 of 31 (71.0%) controls, NNT 8.8, case control OR. | |
| Putra, 12/10/2021, retrospective, Indonesia, peer-reviewed, 3 authors, study period February 2020 - September 2020. | risk of hospitalization, 25.6% lower, OR 0.74, p = 0.59, high D levels 9 of 31 (29.0%) cases, 11 of 31 (35.5%) controls, NNT 14, case control OR. |
| Rachman, 9/13/2024, retrospective, Indonesia, peer-reviewed, mean age 42.8, 5 authors, study period October 2021 - January 2022. | risk of severe case, 51.5% lower, RR 0.48, p = 0.37, high D levels (≥20ng/mL) 2 of 28 (7.1%), low D levels (<20ng/mL) 19 of 129 (14.7%), NNT 13. |
| Rachman (B), 4/13/2023, prospective, Indonesia, peer-reviewed, 4 authors, study period October 2021 - February 2022. | risk of death, 94.8% lower, RR 0.05, p = 0.04, high D levels (≥20ng/mL) 0 of 45 (0.0%), low D levels (<20ng/mL) 14 of 146 (9.6%), NNT 10, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of severe case, 77.6% lower, RR 0.22, p = 0.01, high D levels (≥20ng/mL) 2 of 45 (4.4%), low D levels (<20ng/mL) 29 of 146 (19.9%), NNT 6.5. | |
| Radujkovic, 9/10/2020, prospective, Germany, peer-reviewed, 6 authors. | risk of death, 93.2% lower, HR 0.07, p = 0.001, high D levels 144, low D levels 12, >30nmol/L. |
| risk of death/intubation, 84.0% lower, HR 0.16, p < 0.001, high D levels 144, low D levels 12, >30nmol/L. | |
| Ramirez-Sandoval, 10/15/2021, retrospective, Mexico, peer-reviewed, 7 authors. | risk of death, 31.5% lower, HR 0.68, p < 0.001, high D levels 2,337, low D levels 571, adjusted per study, inverted to make HR<1 favor high D levels, >12.5ng/mL, 30 day in-hospital mortality. |
| hospitalization time, 22.2% lower, relative time 0.78, p < 0.001, high D levels 2,337, low D levels 571. | |
| Ramos, 11/15/2021, retrospective, Brazil, peer-reviewed, 11 authors. | risk of case, 45.7% lower, RR 0.54, p = 0.16, high D levels (≥20ng/mL) 4 of 9 (44.4%), low D levels (<20ng/mL) 9 of 11 (81.8%), NNT 2.7. |
| Ranjbar, 11/29/2021, retrospective, Iran, peer-reviewed, 27 authors, study period 16 February, 2020 - 21 March, 2020. | risk of death, 41.9% lower, RR 0.58, p = 0.07, high D levels (≥20ng/mL) 16 of 163 (9.8%), low D levels (<20ng/mL) 26 of 154 (16.9%), NNT 14. |
| Reis, 5/21/2021, prospective, Brazil, peer-reviewed, 19 authors. | risk of death, 23.0% lower, HR 0.77, p = 0.82, high D levels (≥10ng/mL) 198, low D levels (<10ng/mL) 16, model 2, Cox proportional hazards. |
| risk of mechanical ventilation, 45.0% higher, HR 1.45, p = 0.77, high D levels (≥10ng/mL) 198, low D levels (<10ng/mL) 16, adjusted per study, model 2, multivariable, Cox proportional hazards. | |
| risk of no hospital discharge, 33.3% lower, HR 0.67, p = 0.18, high D levels (≥10ng/mL) 198, low D levels (<10ng/mL) 16, adjusted per study, inverted to make HR<1 favor high D levels (≥10ng/mL), model 2, multivariable, Cox proportional hazards. | |
| hospitalization time, 22.2% lower, relative time 0.78, p = 0.06, high D levels (≥10ng/mL) 191, low D levels (<10ng/mL) 15, model 2. | |
| Renieris, 11/26/2023, retrospective, Greece, peer-reviewed, 10 authors, trial NCT04357366 (history). | risk of death, 52.4% lower, HR 0.48, p = 0.04, high D levels (≥20ng/mL) 17 of 130 (13.1%), low D levels (<20ng/mL) 17 of 60 (28.3%), NNT 6.6, inverted to make HR<1 favor high D levels (≥20ng/mL). |
| Reyes Pérez, 4/30/2020, retrospective, Mexico, peer-reviewed, 5 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 61.7% lower, RR 0.38, p = 0.006, high D levels (≥8ng/mL) 21 of 137 (15.3%), low D levels (<8ng/mL) 14 of 35 (40.0%), NNT 4.1, inverted to make RR<1 favor high D levels (≥8ng/mL), odds ratio converted to relative risk. |
| Ribeiro, 8/5/2021, retrospective, Brazil, peer-reviewed, 8 authors. | risk of case, 50.5% lower, OR 0.50, p = 0.01, inverted to make OR<1 favor high D levels, >30ng/mL, multivariate, RR approximated with OR. |
| Ricci, 3/3/2021, retrospective, Italy, peer-reviewed, 15 authors. | risk of death, 87.6% lower, RR 0.12, p = 0.07, high D levels 0 of 30 (0.0%), low D levels 3 of 22 (13.6%), NNT 7.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), >10 ng/mL. |
| Ritsinger, 4/28/2023, retrospective, Sweden, peer-reviewed, mean age 79.8, 8 authors, study period 1 January, 2020 - 9 September, 2021. | risk of death, 9.1% lower, HR 0.91, p < 0.001, high D levels (≥50nmol/L) 37,972, low D levels (<50nmol/L) 6,894, inverted to make HR<1 favor high D levels (≥50nmol/L). |
| Rizzi, 4/16/2026, prospective, Italy, peer-reviewed, 21 authors, study period January 2021 - May 2021. | risk of no recovery, 59.2% lower, OR 0.41, p = 0.04, high D levels (≥11 ng/mL) 93, low D levels (<11 ng/mL) 46, adjusted per study, inverted to make OR<1 favor high D levels (≥11 ng/mL), risk of no discharge alive and/or NEWS2 ≤ 2 for at least 24 h within 14 days, multivariable, Table 6, RR approximated with OR. |
| Rodríguez-Vidales, 2/24/2022, retrospective, Mexico, peer-reviewed, 8 authors, study period March 2020 - September 2020. | risk of severe case, 38.9% lower, RR 0.61, p = 0.05, high D levels (≥10ng/mL) 89 of 265 (33.6%), low D levels (<10ng/mL) 27 of 32 (84.4%), NNT 2.0, adjusted per study, inverted to make RR<1 favor high D levels (≥10ng/mL), odds ratio converted to relative risk, multivariable. |
| Rozemeijer, 1/29/2024, prospective, Netherlands, peer-reviewed, 9 authors. | risk of ICU admission, 35.7% lower, OR 0.64, p = 0.67, high D levels (≥50nmol/L) 6 of 20 (30.0%) cases, 2 of 5 (40.0%) controls, NNT 14, case control OR. |
| Sanamandra, 4/30/2023, prospective, India, peer-reviewed, 6 authors, study period August 2020 - March 2021. | risk of death, 20.9% lower, OR 0.79, p = 0.67, high D levels (≥10ng/mL) 155, low D levels (<10ng/mL) 45, inverted to make OR<1 favor high D levels (≥10ng/mL), RR approximated with OR. |
| risk of mechanical ventilation, 15.3% lower, OR 0.85, p = 0.73, high D levels (≥10ng/mL) 155, low D levels (<10ng/mL) 45, inverted to make OR<1 favor high D levels (≥10ng/mL), RR approximated with OR. | |
| risk of severe case, 434.8% higher, OR 5.35, p = 0.12, high D levels (≥10ng/mL) 155, low D levels (<10ng/mL) 45, inverted to make OR<1 favor high D levels (≥10ng/mL), RR approximated with OR. | |
| Sanson, 2/19/2022, prospective, Italy, peer-reviewed, 13 authors, study period March 2020 - September 2020, excluded in exclusion analyses: unadjusted results with no group details. | NIV/IMV/death, 64.0% lower, RR 0.36, p = 0.03, high D levels (≥30ng/mL) 2 of 9 (22.2%), low D levels (<30ng/mL) 37 of 60 (61.7%), NNT 2.5. |
| Saponaro, 1/24/2022, retrospective, Italy, peer-reviewed, 13 authors, study period March 2020 - May 2020. | risk of ARDS, 36.5% lower, RR 0.64, p = 0.43, high D levels (≥20ng/ml) 5 of 32 (15.6%), low D levels (<20ng/ml) 15 of 61 (24.6%), NNT 11, severe ARDS. |
| Savitri, 5/8/2021, retrospective, Indonesia, peer-reviewed, 5 authors. | risk of symptomatic case, 88.0% lower, RR 0.12, p < 0.001, high D levels 3 of 25 (12.0%), low D levels 17 of 17 (100.0%), NNT 1.1, >20ng/ml. |
| Schmidt, 3/22/2023, prospective, Poland, peer-reviewed, 4 authors, study period 4 February, 2021 - 31 December, 2021. | risk of death, 85.5% lower, OR 0.14, p = 0.003, cutoff 27ng/mL, inverted to make OR<1 favor high D levels (≥27ng/mL), RR approximated with OR. |
| Seal, 1/1/2022, retrospective, USA, peer-reviewed, 6 authors. | risk of death, 45.1% lower, RR 0.55, p = 0.001, adjusted per study, inverted to make RR<1 favor high D levels, 60ng/mL vs. 15 ng/mL. |
| risk of death, 40.5% lower, RR 0.60, p = 0.001, adjusted per study, inverted to make RR<1 favor high D levels, 50ng/mL vs. 15 ng/mL. | |
| risk of death, 34.6% lower, RR 0.65, p = 0.001, adjusted per study, inverted to make RR<1 favor high D levels, 40ng/mL vs. 15 ng/mL. | |
| risk of death, 25.9% lower, RR 0.74, p = 0.001, adjusted per study, inverted to make RR<1 favor high D levels, 30ng/mL vs. 15 ng/mL. | |
| risk of death, 20.0% lower, RR 0.80, p = 0.001, adjusted per study, inverted to make RR<1 favor high D levels, 25ng/mL vs. 15 ng/mL. | |
| risk of death, 11.5% lower, RR 0.88, p = 0.001, adjusted per study, inverted to make RR<1 favor high D levels, 20ng/mL vs. 15 ng/mL. | |
| risk of hospitalization, 22.5% lower, RR 0.78, p = 0.01, adjusted per study, inverted to make RR<1 favor high D levels, 60ng/mL vs. 15 ng/mL. | |
| risk of hospitalization, 20.0% lower, RR 0.80, p = 0.009, adjusted per study, inverted to make RR<1 favor high D levels, 50ng/mL vs. 15 ng/mL. | |
| risk of hospitalization, 16.7% lower, RR 0.83, p = 0.007, adjusted per study, inverted to make RR<1 favor high D levels, 40ng/mL vs. 15 ng/mL. | |
| risk of hospitalization, 12.3% lower, RR 0.88, p = 0.008, adjusted per study, inverted to make RR<1 favor high D levels, 30ng/mL vs. 15 ng/mL. | |
| risk of hospitalization, 9.1% lower, RR 0.91, p = 0.01, adjusted per study, inverted to make RR<1 favor high D levels, 25ng/mL vs. 15 ng/mL. | |
| risk of hospitalization, 4.8% lower, RR 0.95, p = 0.02, adjusted per study, inverted to make RR<1 favor high D levels, 20ng/mL vs. 15 ng/mL. | |
| Seven, 11/23/2021, prospective, Turkey, peer-reviewed, 6 authors, study period September 2020 - November 2020. | risk of severe disease or poor prognostic factor, 46.5% lower, RR 0.53, p = 0.006, cutoff 14.5ng/ml, inverted to make RR<1 favor high D levels (≥14.5ng/ml). |
| Sheng, 9/12/2025, retrospective, Taiwan, peer-reviewed, mean age 58.2, 6 authors. | risk of death, 90.6% lower, OR 0.09, p = 0.04, high D levels (≥30 ng/mL) 22, low D levels (<20 ng/mL) 45, adjusted per study, inverted to make OR<1 favor high D levels (≥30 ng/mL), multivariable, RR approximated with OR. |
| Sinaci, 8/11/2021, retrospective, Turkey, peer-reviewed, 10 authors, dosage not specified. | risk of moderate/severe case, 79.5% lower, RR 0.21, p < 0.001, high D levels (≥10ng/mL) 8 of 100 (8.0%), low D levels (<10ng/mL) 23 of 59 (39.0%), NNT 3.2, outcome based on serum levels. |
| risk of case, 59.9% lower, RR 0.40, p < 0.001, high D levels (≥10ng/mL) 100 of 397 (25.2%), low D levels (<10ng/mL) 59 of 94 (62.8%), NNT 2.7, outcome based on serum levels. | |
| Singhsakul, 6/9/2024, retrospective, Thailand, peer-reviewed, mean age 50.8, 6 authors, study period 1 September, 2021 - 30 November, 2021. | risk of severe case, 51.2% lower, RR 0.49, p = 0.02, high D levels (≥20ng/mL) 16 of 52 (30.8%), low D levels (<20ng/mL) 28 of 45 (62.2%), NNT 3.2, adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable. |
| moderate case, 67.3% lower, RR 0.33, p = 0.34, high D levels (≥20ng/mL) 2 of 52 (3.8%), low D levels (<20ng/mL) 2 of 45 (4.4%), adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable. | |
| Siuka, 3/9/2023, prospective, Slovenia, peer-reviewed, 7 authors, study period December 2020 - December 2021. | risk of death, 55.9% lower, RR 0.44, p = 0.24, high D levels (≥30nmol/L) 10 of 255 (3.9%), low D levels (<30nmol/L) 4 of 45 (8.9%), NNT 20. |
| risk of ICU admission, 58.8% higher, RR 1.59, p = 0.59, high D levels (≥30nmol/L) 27 of 255 (10.6%), low D levels (<30nmol/L) 3 of 45 (6.7%). | |
| risk of severe case, 61.0% higher, RR 1.61, p = 0.009, high D levels (≥30nmol/L) 146 of 255 (57.3%), low D levels (<30nmol/L) 16 of 45 (35.6%). | |
| Smaha, 1/22/2022, retrospective, Slovakia, peer-reviewed, 13 authors, study period 1 November, 2020 - 30 April, 2021. | risk of death, 19.0% lower, RR 0.81, p = 0.05, high D levels (≥12ng/mL) 127 of 283 (44.9%), low D levels (<12ng/mL) 41 of 74 (55.4%), NNT 9.5. |
| Subramanian, 1/31/2022, prospective, United Kingdom, peer-reviewed, 16 authors, dosage not specified. | risk of death, 49.7% lower, RR 0.50, p = 0.02, high D levels 16 of 115 (13.9%), low D levels 33 of 118 (28.0%), NNT 7.1, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, 50-74 nmol/L vs. <25nmol/L, multivariable, outcome based on serum levels. |
| risk of death, 39.7% lower, RR 0.60, p = 0.07, high D levels 16 of 115 (13.9%), low D levels 38 of 157 (24.2%), NNT 9.7, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, 50-74 nmol/L vs. 25-49nmol/L, multivariable, outcome based on serum levels. | |
| Sulli (B), 2/24/2021, retrospective, Italy, peer-reviewed, 10 authors, dosage not specified. | risk of case, 79.2% lower, OR 0.21, p < 0.001, high D levels 28 of 65 (43.1%) cases, 51 of 65 (78.5%) controls, NNT 2.7, case control OR, >10ng/mL. |
| Susianti, 2/12/2021, retrospective, Indonesia, peer-reviewed, 8 authors. | risk of death, 91.5% lower, RR 0.09, p = 0.32, high D levels 0 of 8 (0.0%), low D levels 9 of 42 (21.4%), NNT 4.7, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), >49.92 nmol/L. |
| risk of ICU admission, 90.5% lower, RR 0.10, p = 0.32, high D levels 0 of 8 (0.0%), low D levels 8 of 42 (19.0%), NNT 5.2, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), >49.92 nmol/L. | |
| risk of progression, 81.5% lower, OR 0.19, p = 0.04, high D levels 8, low D levels 42, inverted to make OR<1 favor high D levels, ISTH DIC≥5, >49.92 nmol/L, bivariate, RR approximated with OR. | |
| risk of progression, 44.4% lower, OR 0.56, p = 0.03, high D levels 8, low D levels 42, inverted to make OR<1 favor high D levels, increased D-dimer >2 mg/L, >49.92 nmol/L, multivariate, RR approximated with OR. | |
| Szeto, 12/30/2020, retrospective, USA, peer-reviewed, 7 authors. | risk of death, 5.6% higher, RR 1.06, p = 1.00, high D levels 14 of 58 (24.1%), low D levels 8 of 35 (22.9%). |
| risk of mechanical ventilation, 39.7% lower, RR 0.60, p = 0.21, high D levels 10 of 58 (17.2%), low D levels 10 of 35 (28.6%), NNT 8.8. | |
| risk of no hospital discharge, 26.7% higher, RR 1.27, p = 0.50, high D levels 21 of 58 (36.2%), low D levels 10 of 35 (28.6%). | |
| Sánchez-Zuno (B), 5/28/2021, prospective, Mexico, peer-reviewed, 12 authors, dosage 10,000IU days 1-14. | risk of severe case, 5.6% lower, RR 0.94, p = 1.00, high D levels 4 of 8 (50.0%), low D levels 18 of 34 (52.9%), NNT 34, >30ng/mL, >4 symptoms. |
| Tallon, 11/15/2022, retrospective, USA, peer-reviewed, 17 authors. | risk of hospitalization, 41.5% lower, OR 0.58, p < 0.001, high D levels (≥30ng/mL) 113,143, low D levels (<30ng/mL) 3,227, adjusted per study, inverted to make OR<1 favor high D levels (≥30ng/mL), RR approximated with OR. |
| Tan, 2/27/2023, retrospective, Philippines, peer-reviewed, 3 authors. | risk of progression, 71.5% lower, RR 0.29, p = 0.04, high D levels (≥30ng/mL) 7 of 38 (18.4%), low D levels (<20ng/mL) 18 of 34 (52.9%), NNT 2.9, adjusted per study, inverted to make RR<1 favor high D levels (≥30ng/mL), odds ratio converted to relative risk, combined mortality and morbidity, multivariable. |
| risk of death, 91.1% lower, RR 0.09, p = 0.002, high D levels (≥30ng/mL) 1 of 38 (2.6%), low D levels (<20ng/mL) 10 of 34 (29.4%), NNT 3.7, unadjusted. | |
| risk of ICU admission, 82.1% lower, RR 0.18, p = 0.010, high D levels (≥30ng/mL) 2 of 38 (5.3%), low D levels (<20ng/mL) 10 of 34 (29.4%), NNT 4.1, unadjusted. | |
| Tanriverdi, 4/30/2025, retrospective, Turkey, peer-reviewed, mean age 64.0, 1 author, study period 1 June, 2020 - 31 December, 2022, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 59.6% lower, RR 0.40, p = 0.07, high D levels (≥30 ng/mL) 4 of 52 (7.7%), low D levels (<30 ng/mL) 24 of 126 (19.0%), NNT 8.8. |
| Tehrani, 1/25/2021, retrospective, Iran, peer-reviewed, 5 authors. | risk of death, 47.5% lower, RR 0.52, p = 0.07, high D levels 34 of 180 (18.9%), low D levels 9 of 25 (36.0%), NNT 5.8, >10ng/ml. |
| Tomasa-Irriguible, 10/26/2020, retrospective, Spain, peer-reviewed, 7 authors, study period March 2020 - May 2020. | risk of mechanical ventilation, 35.0% lower, RR 0.65, p = 0.21, high D levels 15 of 27 (55.6%), low D levels 18 of 78 (23.1%), adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, ≥20 ng/mL, bivariate logistic regression. |
| risk of ICU admission, 16.9% lower, RR 0.83, p = 0.58, high D levels 11 of 27 (40.7%), low D levels 17 of 78 (21.8%), adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, ≥20 ng/mL, bivariate logistic regression. | |
| Topan, 2/28/2023, retrospective, Romania, peer-reviewed, survey, 6 authors, study period April 2020 - May 2022. | risk of death, 30.6% lower, RR 0.69, p = 0.02, high D levels (≥20ng/mL) 61 of 1,148 (5.3%), low D levels (<20ng/mL) 118 of 1,194 (9.9%), adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, multivariable. |
| risk of severe case, 10.9% lower, RR 0.89, p = 0.02, high D levels (≥20ng/mL) 432 of 1,148 (37.6%), low D levels (<20ng/mL) 560 of 1,194 (46.9%), NNT 11, adjusted per study, inverted to make RR<1 favor high D levels (≥20ng/mL), odds ratio converted to relative risk, severe/critical case, multivariable. | |
| Umay, 7/26/2023, retrospective, Turkey, peer-reviewed, 4 authors, study period 1 March, 2020 - 31 January, 2021. | hospitalization time, 13.5% lower, relative time 0.87, p = 0.33, high D levels 374, low D levels 39. |
| Vanegas-Cedillo, 3/14/2021, retrospective, Mexico, peer-reviewed, 15 authors. | risk of death, 52.6% lower, RR 0.47, p = 0.006, high D levels (≥12ng/mL) 95 of 494 (19.2%), low D levels (<12ng/mL) 21 of 57 (36.8%), NNT 5.7, adjusted per study, inverted to make RR<1 favor high D levels (≥12ng/mL). |
| Vasheghani (B), 1/18/2021, retrospective, Iran, preprint, 6 authors, dosage not specified. | risk of ICU admission, 63.8% lower, RR 0.36, p = 0.009, high D levels 13 of 185 (7.0%), low D levels 53 of 323 (16.4%), NNT 11, adjusted per study, inverted to make RR<1 favor high D levels, vitamin D levels >30ng/mL. |
| Vassiliou (B), 12/9/2020, prospective, Greece, peer-reviewed, 6 authors. | risk of death, 90.9% lower, RR 0.09, p = 0.04, high D levels 0 of 15 (0.0%), low D levels 5 of 15 (33.3%), NNT 3.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), >15.2ng/mL. |
| Voelkle, 4/30/2022, prospective, Switzerland, peer-reviewed, median age 67.0, 9 authors, study period 17 March, 2020 - 30 April, 2020. | risk of death/ICU, 23.4% lower, RR 0.77, p = 0.55, high D levels 8 of 34 (23.5%), low D levels 7 of 23 (30.4%), NNT 14, adjusted per study, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. |
| Vásquez-Procopio, 12/2/2022, retrospective, Mexico, peer-reviewed, 12 authors. | risk of severe case, 82.8% lower, OR 0.17, p = 0.04, high D levels (≥20ng/mL) 111, low D levels (<20ng/mL) 54, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), multivariable, RR approximated with OR. |
| Wagner, 5/31/2025, prospective, USA, peer-reviewed, mean age 64.3, 12 authors, study period July 2020 - December 2021, trial NCT04482673 (history). | risk of case, 74.1% lower, RR 0.26, p = 0.01, high D levels 22 of 106 (20.8%), low D levels 22 of 25 (88.0%), NNT 1.5, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. |
| Walk, 11/9/2020, retrospective, Netherlands, preprint, 5 authors. | risk of death/intubation, 0.4% higher, RR 1.00, p = 1.00, high D levels 48 of 110 (43.6%), low D levels 10 of 23 (43.5%), >25nmol/L. |
| Wang (C), 3/29/2023, prospective, China, peer-reviewed, median age 36.5, 23 authors, study period 18 December, 2022 - 20 February, 2023, dosage 200,000IU days 1, 14, trial NCT05673980 (history). | risk of case, 22.7% lower, RR 0.77, p = 0.19, high D levels (≥30ng/ml) 20 of 44 (45.5%), low D levels (<20ng/ml) 50 of 85 (58.8%), NNT 7.5, outcome based on serum levels. |
| Wani, 6/1/2023, retrospective, India, peer-reviewed, 5 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of severe case, 72.2% lower, OR 0.28, p = 0.007, high D levels (≥28ng/mL) 66, low D levels (<28ng/mL) 170, inverted to make OR<1 favor high D levels (≥28ng/mL), RR approximated with OR. |
| Wu (B), 12/19/2023, retrospective, multiple countries, peer-reviewed, 9 authors, study period 1 January, 2022 - 30 November, 2022. | risk of death, 42.8% lower, HR 0.57, p = 0.005, high D levels (≥20 ng/mL) 8,300, low D levels (<20 ng/mL) 8,300, inverted to make HR<1 favor high D levels (≥20 ng/mL), propensity score matching. |
| risk of hospitalization, 18.7% lower, HR 0.81, p < 0.001, high D levels (≥20 ng/mL) 8,300, low D levels (<20 ng/mL) 8,300, inverted to make HR<1 favor high D levels (≥20 ng/mL), propensity score matching. | |
| ER visit, 10.2% lower, HR 0.90, p = 0.03, high D levels (≥20 ng/mL) 8,300, low D levels (<20 ng/mL) 8,300, inverted to make HR<1 favor high D levels (≥20 ng/mL), propensity score matching. | |
| risk of long COVID, 2.0% higher, HR 1.02, p = 0.93, high D levels (≥20 ng/mL) 8,300, low D levels (<20 ng/mL) 8,300, inverted to make HR<1 favor high D levels (≥20 ng/mL), propensity score matching. | |
| Węgrzynek-Gallina, 1/31/2024, retrospective, Poland, peer-reviewed, mean age 66.5, 6 authors, study period November 2020 - June 2021. | hospitalization time, 33.3% lower, relative time 0.67, p < 0.001, high D levels (≥50nmol/L) 169, low D levels (<50nmol/L) 63. |
| Ye, 10/13/2020, retrospective, China, peer-reviewed, 18 authors. | risk of severe/critical COVID-19, 93.4% lower, RR 0.07, p = 0.03, high D levels 2 of 36 (5.6%), low D levels 8 of 26 (30.8%), NNT 4.0, adjusted per study, inverted to make RR<1 favor high D levels, >50nmol/L. |
| You, 12/22/2024, retrospective, China, peer-reviewed, 5 authors. | risk of death, 81.9% lower, OR 0.18, p = 0.15, high D levels 96, low D levels 73, adjusted per study, inverted to make OR<1 favor high D levels, multivariable, RR approximated with OR. |
| risk of severe case, 95.6% lower, OR 0.04, p = 0.01, high D levels 96, low D levels 73, adjusted per study, inverted to make OR<1 favor high D levels, multivariable, RR approximated with OR. | |
| Yılmaz, 10/5/2020, retrospective, Turkey, peer-reviewed, 2 authors. | risk of severe case, 73.4% lower, RR 0.27, p = 1.00, high D levels 0 of 11 (0.0%), low D levels 2 of 29 (6.9%), NNT 14, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), >20ng/ml. |
| risk of moderate or severe case, 41.4% lower, RR 0.59, p = 0.69, high D levels 2 of 11 (18.2%), low D levels 9 of 29 (31.0%), NNT 7.8, >20ng/ml. | |
| Zafar, 9/6/2021, retrospective, United Kingdom, peer-reviewed, median age 68.0, 37 authors. | risk of death, 42.9% higher, RR 1.43, p = 0.71, high D levels (≥25nmol/L) 12 of 42 (28.6%), low D levels (<25nmol/L) 2 of 10 (20.0%), COVID+ patients. |
| risk of death, 6.0% lower, OR 0.94, p = 0.68, high D levels 42, low D levels 10, COVID+ patients, RR approximated with OR. | |
| Zeidan, 9/9/2022, prospective, Egypt, peer-reviewed, median age 11.4, 38 authors. | risk of hospitalization, 61.5% lower, OR 0.38, p = 0.002, cutoff 20ng/mL, adjusted per study, inverted to make OR<1 favor high D levels (≥20ng/mL), case control OR, multivariable. |
| Zelzer, 6/22/2021, retrospective, Austria, peer-reviewed, 7 authors. | risk of death, 46.4% lower, RR 0.54, p = 0.08, high D levels 24 of 121 (19.8%), low D levels 10 of 27 (37.0%), NNT 5.8, >30nmol/L. |
| Zendehdel, 1/12/2026, retrospective, Iran, preprint, 7 authors, study period 21 March, 2020 - 11 September, 2020. | risk of death, 65.9% lower, OR 0.34, p = 0.04, high D levels (≥30 ng/mL) 91, low D levels (<12 ng/mL) 65, adjusted per study, inverted to make OR<1 favor high D levels (≥30 ng/mL), multivariable, RR approximated with OR. |
| risk of mechanical ventilation, 25.9% lower, OR 0.74, p = 0.67, high D levels (≥30 ng/mL) 91, low D levels (<12 ng/mL) 65, adjusted per study, inverted to make OR<1 favor high D levels (≥30 ng/mL), multivariable, RR approximated with OR. | |
| risk of ICU admission, 47.9% lower, OR 0.52, p = 0.16, high D levels (≥30 ng/mL) 91, low D levels (<12 ng/mL) 65, adjusted per study, inverted to make OR<1 favor high D levels (≥30 ng/mL), multivariable, RR approximated with OR. | |
| risk of death, 41.2% lower, OR 0.59, p = 0.13, high D levels (≥20 ng/mL) 145, low D levels (<20 ng/mL) 131, adjusted per study, inverted to make OR<1 favor high D levels (≥20 ng/mL), multivariable, RR approximated with OR. | |
| risk of mechanical ventilation, 34.2% lower, OR 0.66, p = 0.36, high D levels (≥20 ng/mL) 145, low D levels (<20 ng/mL) 131, adjusted per study, inverted to make OR<1 favor high D levels (≥20 ng/mL), multivariable, RR approximated with OR. | |
| risk of ICU admission, 13.0% lower, OR 0.87, p = 0.68, high D levels (≥20 ng/mL) 145, low D levels (<20 ng/mL) 131, adjusted per study, inverted to make OR<1 favor high D levels (≥20 ng/mL), multivariable, RR approximated with OR. | |
| Zidrou, 2/19/2022, retrospective, Greece, peer-reviewed, 6 authors, study period August 2020 - October 2020. | risk of death, 26.4% lower, RR 0.74, p = 1.00, high D levels (≥20ng/ml) 2 of 25 (8.0%), low D levels (<20ng/ml) 5 of 46 (10.9%), NNT 35. |
| radiographic changes, 18.2% lower, RR 0.82, p = 0.26, high D levels (≥20ng/ml) 16 of 25 (64.0%), low D levels (<20ng/ml) 36 of 46 (78.3%), NNT 7.0. | |
| hospitalization time, 37.7% lower, relative time 0.62, p = 0.16, high D levels (≥20ng/ml) 25, low D levels (<20ng/ml) 46. | |
| Álvarez, 10/28/2022, retrospective, Spain, preprint, 1 author, study period March 2020 - March 2021, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 38.8% lower, RR 0.61, p < 0.001, high D levels 4,871 of 33,673 (14.5%), low D levels 611 of 2,588 (23.6%), NNT 11, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. |
| risk of ICU admission, 54.7% lower, RR 0.45, p < 0.001, high D levels 289 of 33,673 (0.9%), low D levels 49 of 2,588 (1.9%), NNT 97, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. | |
| risk of hospitalization, 43.0% lower, RR 0.57, p < 0.001, high D levels 8,905 of 33,673 (26.4%), low D levels 1,202 of 2,588 (46.4%), NNT 5.0, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk. | |
| Ünsal, 4/5/2021, retrospective, Turkey, peer-reviewed, 10 authors. | risk of death, 80.6% lower, RR 0.19, p = 0.23, high D levels 0 of 29 (0.0%), low D levels 2 of 27 (7.4%), NNT 14, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), ≥20ng/mL. |
| risk of oxygen therapy, 73.4% lower, RR 0.27, p = 0.07, high D levels 2 of 29 (6.9%), low D levels 7 of 27 (25.9%), NNT 5.3, ≥20ng/mL. | |
| Şengül, 12/31/2022, retrospective, Turkey, peer-reviewed, 4 authors, study period March 2020 - December 2021, dosage not specified. | risk of case, 75.6% lower, OR 0.24, p < 0.001, high D levels (≥20ng/mL) 7 of 54 (13.0%) cases, 100 of 264 (37.9%) controls, NNT 6.4, case control OR, outcome based on serum levels. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Annweiler, 5/31/2022, Randomized Controlled Trial, France, peer-reviewed, 17 authors, study period 15 April, 2020 - 17 December, 2020, dosage 400,000IU single dose, trial NCT04344041 (history) (COVIT-TRIAL). | risk of death, 30.0% lower, HR 0.70, p = 0.29, treatment 19 of 126 (15.1%), control 21 of 126 (16.7%), Cox proportional hazards, day 28, intention-to-treat. |
| risk of death, 38.0% lower, HR 0.62, p = 0.17, treatment 17 of 121 (14.0%), control 21 of 121 (17.4%), Cox proportional hazards, day 28, per-protocol. | |
| risk of death, 61.0% lower, HR 0.39, p = 0.049, treatment 8 of 127 (6.3%), control 14 of 127 (11.0%), Cox proportional hazards, day 14, intention-to-treat. | |
| risk of death, 65.0% lower, HR 0.35, p = 0.03, treatment 7 of 122 (5.7%), control 14 of 122 (11.5%), Cox proportional hazards, day 14, per-protocol. | |
| Annweiler (B), 11/2/2020, retrospective, France, peer-reviewed, 7 authors, dosage 80,000IU single dose. | risk of death, 63.0% lower, RR 0.37, p = 0.28, treatment 3 of 16 (18.8%), control 10 of 32 (31.2%), NNT 8.0, adjusted per study, supplementation after diagnosis. |
| Annweiler (C), 10/13/2020, retrospective, France, peer-reviewed, mean age 87.7, 6 authors, dosage 80,000IU single dose, 80,000IU either in the week following the suspicion or diagnosis of COVID-19, or during the previous month. | risk of death, 89.0% lower, RR 0.11, p = 0.002, treatment 10 of 57 (17.5%), control 5 of 9 (55.6%), NNT 2.6, adjusted per study. |
| Asimi, 5/22/2021, retrospective, Bosnia and Herzegovina, preprint, 3 authors, dosage 2,000IU daily, this trial uses multiple treatments in the treatment arm (combined with zinc and selenium) - results of individual treatments may vary, excluded in exclusion analyses: excessive unadjusted differences between groups. | risk of mechanical ventilation, 97.4% lower, RR 0.03, p < 0.001, treatment 0 of 270 (0.0%), control 9 of 86 (10.5%), NNT 9.6, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), unadjusted. |
| risk of hospitalization, 99.0% lower, RR 0.010, p < 0.001, treatment 0 of 270 (0.0%), control 24 of 86 (27.9%), NNT 3.6, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), unadjusted. | |
| risk of severe case, 99.5% lower, RR 0.005, p < 0.001, treatment 0 of 270 (0.0%), control 51 of 86 (59.3%), NNT 1.7, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), unadjusted. | Boukef, 2/28/2023, Double Blind Randomized Controlled Trial, placebo-controlled, Tunisia, trial NCT05670444 (history). | 150 patient RCT with results unknown and over 3 years late. |
| Burahee, 2/17/2021, retrospective, United Kingdom, peer-reviewed, 4 authors, dosage 100,000IU days 1-4, additional 200000IU over four weeks if serum level insufficient. | risk of death, 93.3% lower, RR 0.07, p = 0.01, treatment 0 of 12 (0.0%), control 2 of 2 (100.0%), NNT 1.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Din Ujjan, 1/18/2023, Randomized Controlled Trial, Pakistan, peer-reviewed, 6 authors, study period 21 September, 2021 - 21 January, 2022, dosage 360IU days 1-14, this trial uses multiple treatments in the treatment arm (combined with curcumin and quercetin) - results of individual treatments may vary, trial NCT04603690 (history), excluded in exclusion analyses: combined treatments may contribute significantly to the effect seen; unadjusted differences between groups. | risk of no recovery, 28.6% lower, RR 0.71, p = 0.11, treatment 15 of 25 (60.0%), control 21 of 25 (84.0%), NNT 4.2, no symptoms, day 7. |
| risk of no recovery, 71.4% lower, RR 0.29, p < 0.001, treatment 6 of 25 (24.0%), control 21 of 25 (84.0%), NNT 1.7, ≤1 symptom, day 7. | |
| risk of no recovery, 76.9% lower, RR 0.23, p = 0.005, treatment 3 of 25 (12.0%), control 13 of 25 (52.0%), NNT 2.5, ≤2 symptoms, day 7. | |
| risk of no recovery, 85.7% lower, RR 0.14, p = 0.23, treatment 0 of 25 (0.0%), control 3 of 25 (12.0%), NNT 8.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), ≤3 symptoms, day 7. | |
| risk of no viral clearance, 90.9% lower, RR 0.09, p = 0.05, treatment 0 of 25 (0.0%), control 5 of 25 (20.0%), NNT 5.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 14. | |
| risk of no viral clearance, 73.7% lower, RR 0.26, p < 0.001, treatment 5 of 25 (20.0%), control 19 of 25 (76.0%), NNT 1.8, day 7. | |
| Efird, 12/31/2021, retrospective, USA, peer-reviewed, 10 authors, study period 1 March, 2020 - 10 September, 2020, dosage varies. | risk of death, 48.9% lower, RR 0.51, p = 0.10, treatment 11 of 544 (2.0%), control 413 of 15,794 (2.6%), adjusted per study, non-hospitalized patients, vitamin D + no corticosteroids vs. no vitamin D + no corticosteroids. |
| risk of death, 54.5% lower, RR 0.45, p = 0.02, treatment 11 of 192 (5.7%), control 553 of 4,340 (12.7%), NNT 14, adjusted per study, hospitalized patients, vitamin D + no corticosteroids vs. no vitamin D + no corticosteroids. | |
| Hunt, 6/29/2022, retrospective, USA, peer-reviewed, 8 authors, study period 1 March, 2020 - 10 September, 2020, dosage not specified. | risk of death, 47.0% lower, RR 0.53, p < 0.001, treatment 43 of 1,019 (4.2%), control 1,569 of 25,489 (6.2%), adjusted per study, day 30. |
| Khan, 5/1/2022, Randomized Controlled Trial, Pakistan, peer-reviewed, 7 authors, study period 2 September, 2021 - 28 November, 2021, dosage 360IU days 1-14, this trial uses multiple treatments in the treatment arm (combined with curcumin and quercetin) - results of individual treatments may vary, trial NCT05130671 (history), excluded in exclusion analyses: based on dosages and previous research, combined treatments may contribute more to the effect seen. | risk of no recovery, 33.3% lower, RR 0.67, p = 0.15, treatment 10 of 25 (40.0%), control 15 of 25 (60.0%), NNT 5.0. |
| relative CRP reduction, 39.1% better, RR 0.61, p = 0.006, treatment 25, control 25. | |
| risk of no viral clearance, 50.0% lower, RR 0.50, p = 0.009, treatment 10 of 25 (40.0%), control 20 of 25 (80.0%), NNT 2.5. | |
| Said, 11/8/2022, Randomized Controlled Trial, Egypt, peer-reviewed, 5 authors, study period 21 July, 2021 - 30 December, 2021, dosage 2,000IU daily, trial NCT04981743 (history). | risk of no recovery, 42.0% lower, OR 0.58, p = 0.57, treatment 30, control 30, adjusted per study, multivariable, dyspnea, RR approximated with OR. |
| risk of no recovery, 89.0% lower, OR 0.11, p = 0.01, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, dyspnea, RR approximated with OR. | |
| risk of no recovery, 52.0% lower, OR 0.48, p = 0.16, treatment 30, control 30, adjusted per study, multivariable, cough, RR approximated with OR. | |
| risk of no recovery, 77.0% lower, OR 0.23, p = 0.01, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, cough, RR approximated with OR. | |
| risk of no recovery, 56.0% lower, OR 0.44, p = 0.20, treatment 30, control 30, adjusted per study, multivariable, fatigue, RR approximated with OR. | |
| risk of no recovery, 90.0% lower, OR 0.10, p < 0.001, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, fatigue, RR approximated with OR. | |
| risk of no recovery, 33.0% lower, OR 0.67, p = 0.67, treatment 30, control 30, adjusted per study, multivariable, smell, RR approximated with OR. | |
| risk of no recovery, 67.0% lower, OR 0.33, p = 0.23, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, smell, RR approximated with OR. | |
| risk of no recovery, 25.0% higher, OR 1.25, p = 0.79, treatment 30, control 30, adjusted per study, multivariable, taste, RR approximated with OR. | |
| risk of no recovery, 58.0% lower, OR 0.42, p = 0.28, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, taste, RR approximated with OR. | |
| risk of no recovery, 56.0% lower, OR 0.44, p = 0.36, treatment 30, control 30, adjusted per study, multivariable, sore throat, RR approximated with OR. | |
| risk of no recovery, 86.0% lower, OR 0.14, p = 0.03, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, sore throat, RR approximated with OR. | |
| risk of no recovery, 175.0% higher, OR 2.75, p = 0.13, treatment 30, control 30, adjusted per study, multivariable, headache, RR approximated with OR. | |
| risk of no recovery, 56.0% lower, OR 0.44, p = 0.21, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, headache, RR approximated with OR. | |
| risk of no recovery, 87.0% lower, OR 0.13, p = 0.05, treatment 30, control 30, adjusted per study, multivariable, diarrhea, RR approximated with OR. | |
| risk of no recovery, 90.0% lower, OR 0.10, p = 0.03, treatment 30, control 30, adjusted per study, vitamin D and nigella sativa, multivariable, diarrhea, RR approximated with OR. | |
| risk of no viral clearance, 49.0% lower, OR 0.51, p = 0.20, treatment 30, control 30, day 14, RR approximated with OR. | |
| risk of no viral clearance, 23.0% lower, OR 0.77, p = 0.74, treatment 30, control 30, day 7, RR approximated with OR. | |
| risk of no viral clearance, 91.0% lower, OR 0.09, p < 0.001, treatment 30, control 30, vitamin D and nigella sativa, day 14, RR approximated with OR. | |
| risk of no viral clearance, 87.0% lower, OR 0.13, p = 0.003, treatment 30, control 30, vitamin D and nigella sativa, day 7, RR approximated with OR. | |
| Sánchez-Zuno, 5/28/2021, Randomized Controlled Trial, Mexico, peer-reviewed, 12 authors, dosage 10,000IU days 1-14. | risk of severe case, 89.4% lower, RR 0.11, p = 0.04, treatment 0 of 22 (0.0%), control 4 of 20 (20.0%), NNT 5.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), risk of >3 symptoms at day 14. |
| risk of no recovery, 80.8% lower, RR 0.19, p = 0.22, treatment 0 of 22 (0.0%), control 2 of 20 (10.0%), NNT 10.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), risk of fever at day 14, Table S1. | |
| Valecha, 4/26/2022, prospective, India, peer-reviewed, 1 author, average treatment delay 3.7 days, dosage 1,000IU daily, this trial uses multiple treatments in the treatment arm (combined with magnesium and vitamin B12) - results of individual treatments may vary. | risk of ICU admission, 86.8% lower, RR 0.13, p = 0.09, treatment 0 of 30 (0.0%), control 3 of 25 (12.0%), NNT 8.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| hospitalization time, 38.5% lower, relative time 0.62, p < 0.001, treatment mean 11.2 (±2.8) n=30, control mean 18.2 (±1.21) n=25. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Abdelhai, 7/15/2024, Randomized Controlled Trial, Egypt, peer-reviewed, 5 authors. | risk of death, 82.9% lower, RR 0.17, p < 0.001, treatment 8 of 170 (4.7%), control 22 of 80 (27.5%), NNT 4.4. |
| hospitalization time, 44.9% lower, relative time 0.55, p < 0.001, treatment mean 8.81 (±2.98) n=170, control mean 16.0 (±5.42) n=80. | |
| risk of no viral clearance, 74.3% lower, RR 0.26, p < 0.001, treatment 35 of 170 (20.6%), control 64 of 80 (80.0%), NNT 1.7. | |
| Al Sulaiman, 8/14/2023, retrospective, Saudi Arabia, peer-reviewed, 25 authors, study period March 2020 - July 2021, dosage not specified, excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 22.0% higher, HR 1.22, p = 0.25, treatment 72 of 144 (50.0%), control 62 of 144 (43.1%). |
| risk of mechanical ventilation, 27.0% higher, OR 1.27, p = 0.046, treatment 144, control 144, RR approximated with OR. | |
| risk of ICU admission, 17.0% higher, OR 1.17, p = 0.07, treatment 144, control 144, RR approximated with OR. | |
| risk of hospitalization, no change, OR 1.00, p = 1.00, treatment 144, control 144, RR approximated with OR. | |
| Alcala-Diaz, 5/21/2021, retrospective, Spain, peer-reviewed, 17 authors, dosage calcifediol 0.5mg day 1, 0.27mg day 3, 0.27mg day 7, 0.27mg day 14, 0.27mg day 21, 0.27mg day 28. | risk of death, 80.8% lower, RR 0.19, p = 0.04, treatment 4 of 79 (5.1%), control 90 of 458 (19.7%), NNT 6.9, adjusted per study, odds ratio converted to relative risk, day 30, multivariate logistic regression. |
| Baguma (B), 12/28/2021, retrospective, Uganda, preprint, 16 authors, study period March 2020 - October 2021, dosage not specified. | risk of death, 96.7% lower, RR 0.03, p = 0.02, treatment 23, control 458, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, multivariable, control prevalance approximated with overall prevalence. |
| Baykal, 5/30/2022, retrospective, Turkey, peer-reviewed, 2 authors, study period 1 April, 2020 - 1 March, 2021, dosage 300,000IU single dose, excluded in exclusion analyses: unadjusted results with no group details; significant confounding by time possible due to separation of groups in different time periods. | risk of death, 22.2% lower, RR 0.78, p = 0.43, treatment 7 of 18 (38.9%), control 28 of 56 (50.0%), NNT 9.0. |
| risk of ICU admission, 59.4% lower, RR 0.41, p = 0.005, treatment 5 of 18 (27.8%), control 39 of 57 (68.4%), NNT 2.5. | |
| Beigmohammadi, 11/14/2021, Single Blind Randomized Controlled Trial, Iran, peer-reviewed, 6 authors, study period April 2020 - July 2020, dosage 600,000IU single dose, this trial uses multiple treatments in the treatment arm (combined with vitamins A, B, C, E) - results of individual treatments may vary, trial IRCT20200319046819N1, excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 88.9% lower, RR 0.11, p = 0.11, treatment 0 of 30 (0.0%), control 4 of 30 (13.3%), NNT 7.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of hospitalization >7 days, 41.0% lower, RR 0.59, p = 0.25, treatment 4 of 30 (13.3%), control 16 of 30 (53.3%), NNT 2.5, adjusted per study, odds ratio converted to relative risk. | |
| relative SOFA score @day 7, 45.5% better, RR 0.55, p < 0.001, treatment 30, control 30. | |
| Bishop, 2/5/2022, Double Blind Randomized Controlled Trial, placebo-controlled, USA, peer-reviewed, survey, 11 authors, study period 2 November, 2020 - 8 October, 2021, dosage calcifediol 300μg days 1-3, 60μg days 4-27, trial NCT04551911 (history) (REsCue). | ER/urgent care visits, 85.4% lower, RR 0.15, p = 0.25, treatment 0 of 65 (0.0%), control 3 of 69 (4.3%), NNT 23, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of no recovery, 33.7% lower, RR 0.66, p = 0.56, treatment 5 of 65 (7.7%), control 8 of 69 (11.6%), NNT 26, day 21, mid-trial. | |
| risk of no recovery, 73.5% lower, RR 0.27, p = 0.37, treatment 1 of 65 (1.5%), control 4 of 69 (5.8%), NNT 23, day 35. | |
| risk of no recovery, 57.5% lower, RR 0.42, p = 0.44, treatment 2 of 65 (3.1%), control 5 of 69 (7.2%), NNT 24, day 28. | |
| risk of no recovery, 6.2% higher, RR 1.06, p = 0.85, treatment 17 of 65 (26.2%), control 17 of 69 (24.6%), day 14. | |
| risk of no recovery, 3.0% higher, RR 1.03, p = 1.00, treatment 33 of 65 (50.8%), control 34 of 69 (49.3%), day 7. | |
| resolution of 5 aggregated symptoms, 9.3% lower, relative time 0.91, p = 0.52, treatment mean 9.8 (±8.15) n=65, control mean 10.8 (±9.54) n=69. | |
| Blázquez-Cabrera, 6/10/2025, retrospective, Spain, peer-reviewed, mean age 73.0, 6 authors, study period 24 January, 2021 - 8 March, 2021, dosage varies (calcitriol), trial NCT05819918 (history) (ALBACOVIDIOL). | risk of death, 52.4% lower, OR 0.48, p = 0.05, treatment 119, control 111, adjusted per study, all patients, multivariable, RR approximated with OR. |
| risk of death, 95.4% lower, OR 0.05, p = 0.004, treatment 16, control 18, severely deficient patients, RR approximated with OR. | |
| risk of death, 38.5% lower, RR 0.62, p = 0.19, treatment 8 of 65 (12.3%), control 33 of 165 (20.0%), NNT 13, previous vitamin D treatment. | |
| Bychinin, 11/3/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Russia, peer-reviewed, 7 authors, study period 1 May, 2020 - 31 January, 2022, average treatment delay 9.0 days, dosage 60,000IU day 1, 5,000IU days 2-7, 8, 5,000IU days 9-14, 15, 5,000IU days 16-21, 22, 5,000IU days 23-28, trial NCT05092698 (history) (COVID-VIT), excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 26.9% lower, RR 0.73, p = 0.18, treatment 19 of 52 (36.5%), control 27 of 54 (50.0%), NNT 7.4. |
| risk of mechanical ventilation, 7.4% lower, RR 0.93, p = 0.68, treatment 33 of 52 (63.5%), control 37 of 54 (68.5%), NNT 20. | |
| Cannata-Andía, 2/18/2022, Randomized Controlled Trial, multiple countries, peer-reviewed, median age 59.0, 22 authors, study period 4 April, 2020 - 22 April, 2021, dosage 100,000IU single dose, trial NCT04552951 (history) (COVID-VIT-D), excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 44.0% higher, RR 1.44, p = 0.31, treatment 22 of 274 (8.0%), control 15 of 269 (5.6%). |
| risk of ICU admission, 4.9% higher, RR 1.05, p = 0.82, treatment 47 of 274 (17.2%), control 44 of 269 (16.4%). | |
| Cervero, 7/4/2022, Single Blind Randomized Controlled Trial, placebo-controlled, Spain, peer-reviewed, median age 65.0, 10 authors, study period June 2020 - March 2021, average treatment delay 7.0 days, dosage 10,000IU days 1-14. | risk of death, 7.3% higher, RR 1.07, p = 1.00, treatment 1 of 41 (2.4%), control 1 of 44 (2.3%). |
| risk of ICU admission, 78.5% lower, RR 0.21, p = 0.20, treatment 1 of 41 (2.4%), control 5 of 44 (11.4%), NNT 11. | |
| risk of ARDS, 28.5% lower, RR 0.72, p = 0.74, treatment 4 of 41 (9.8%), control 6 of 44 (13.6%), NNT 26. | |
| De Niet, 7/26/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Belgium, peer-reviewed, 16 authors, study period August 2020 - August 2021, dosage 25,000IU days 1-4, 11, 18, 25, trial NCT04636086 (history). | risk of death, 65.1% lower, RR 0.35, p = 0.61, treatment 1 of 21 (4.8%), control 3 of 22 (13.6%), NNT 11, COVID-19 mortality. |
| risk of death, 39.7% higher, RR 1.40, p = 0.70, treatment 4 of 21 (19.0%), control 3 of 22 (13.6%), all cause including after discharge and non-COVID-19. | |
| risk of ICU admission, 58.1% lower, RR 0.42, p = 0.41, treatment 2 of 21 (9.5%), control 5 of 22 (22.7%), NNT 7.6. | |
| ICU time, 67.7% lower, relative time 0.32, p = 0.47, treatment 21, control 22. | |
| risk of no hospital discharge, 79.6% lower, RR 0.20, p = 0.49, treatment 0 of 21 (0.0%), control 2 of 22 (9.1%), NNT 11, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 36. | |
| risk of no hospital discharge, 85.4% lower, RR 0.15, p = 0.23, treatment 0 of 21 (0.0%), control 3 of 22 (13.6%), NNT 7.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 28. | |
| risk of no hospital discharge, 85.4% lower, RR 0.15, p = 0.23, treatment 0 of 21 (0.0%), control 3 of 22 (13.6%), NNT 7.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 21. | |
| risk of no hospital discharge, 65.1% lower, RR 0.35, p = 0.61, treatment 1 of 21 (4.8%), control 3 of 22 (13.6%), NNT 11, day 14. | |
| risk of no hospital discharge, 65.1% lower, RR 0.35, p = 0.03, treatment 4 of 21 (19.0%), control 12 of 22 (54.5%), NNT 2.8, day 7. | |
| recovery time, 45.4% lower, relative time 0.55, p = 0.06, treatment 21, control 22, fever. | |
| hospitalization time, 50.0% lower, relative time 0.50, p = 0.003, treatment 21, control 22. | |
| Dinoi, 2/20/2025, retrospective, Italy, peer-reviewed, 11 authors, study period 17 March, 2020 - 15 June, 2021, dosage not specified. | risk of death, 48.4% lower, OR 0.52, p < 0.001, treatment 69 of 247 (27.9%) cases, 106 of 247 (42.9%) controls, NNT 6.1, case control OR. |
| Domazet Bugarin, 2/28/2023, Randomized Controlled Trial, Croatia, peer-reviewed, 9 authors, study period November 2021 - May 2022, dosage 10,000IU days 1-14, trial NCT05384574 (history), excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 21.0% lower, RR 0.79, p = 0.20, treatment 30 of 75 (40.0%), control 39 of 77 (50.6%), NNT 9.4, day 60. |
| risk of death, 12.5% lower, RR 0.87, p = 0.61, treatment 23 of 75 (30.7%), control 27 of 77 (35.1%), NNT 23, day 28. | |
| risk of death, 28.9% lower, RR 0.71, p = 0.49, treatment 9 of 75 (12.0%), control 13 of 77 (16.9%), NNT 20, day 14. | |
| Elamir, 9/8/2021, Randomized Controlled Trial, USA, peer-reviewed, 9 authors, study period September 2020 - December 2020, dosage calcitriol 0.5μg days 1-14. | risk of death, 85.7% lower, RR 0.14, p = 0.23, treatment 0 of 25 (0.0%), control 3 of 25 (12.0%), NNT 8.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of mechanical ventilation, 80.0% lower, RR 0.20, p = 0.48, treatment 0 of 25 (0.0%), control 2 of 25 (8.0%), NNT 12, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| risk of ICU admission, 37.5% lower, RR 0.62, p = 0.33, treatment 5 of 25 (20.0%), control 8 of 25 (32.0%), NNT 8.3. | |
| hospitalization time, 40.5% lower, relative time 0.60, p = 0.14, treatment 25, control 25. | |
| relative Δ SaO2/FiO2, RR 0.14, p = 0.03, treatment 25, control 25, primary outcome. | |
| Elhadi, 4/30/2021, prospective, Libya, peer-reviewed, 21 authors, study period 29 May, 2020 - 30 December, 2020, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 23.4% lower, RR 0.77, p = 0.29, treatment 7 of 15 (46.7%), control 274 of 450 (60.9%), NNT 7.0. |
| Entrenas Castillo, 8/29/2020, Randomized Controlled Trial, Spain, peer-reviewed, 7 authors, study period May 2020 - June 2020, dosage calcifediol 0.5mg day 1, 0.27mg day 3, 0.27mg day 7, and then weekly until discharge or ICU admission, trial NCT04366908 (history) (COVIDIOL). | risk of death, 85.4% lower, RR 0.15, p = 0.11, treatment 0 of 50 (0.0%), control 2 of 26 (7.7%), NNT 13, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of ICU admission, 94.2% lower, RR 0.06, p = 0.008, treatment 1 of 50 (2.0%), control 13 of 26 (50.0%), NNT 2.1, odds ratio converted to relative risk. | |
| Fairfield, 7/26/2022, retrospective, USA, peer-reviewed, 10 authors, study period 1 January, 2020 - 31 July, 2021, dosage not specified, excluded in exclusion analyses: substantial unadjusted confounding by indication likely. | risk of death, 8.9% higher, RR 1.09, p < 0.001, treatment 3,653 of 28,993 (12.6%), control 13,185 of 129,842 (10.2%), odds ratio converted to relative risk. |
| risk of mechanical ventilation, 40.8% higher, RR 1.41, p < 0.001, treatment 4,897 of 28,993 (16.9%), control 15,520 of 129,842 (12.0%), odds ratio converted to relative risk. | |
| Fiore, 5/22/2022, retrospective, matched cohort, Italy, peer-reviewed, mean age 62.5, 10 authors, dosage 100,000IU days 1-2. | risk of death, 92.7% lower, RR 0.07, p = 0.01, treatment 3 of 58 (5.2%), control 11 of 58 (19.0%), NNT 7.2, adjusted per study, odds ratio converted to relative risk, multivariable. |
| risk of mechanical ventilation, 50.0% lower, RR 0.50, p = 0.36, treatment 4 of 58 (6.9%), control 8 of 58 (13.8%), NNT 14. | |
| risk of ICU admission, 50.0% lower, RR 0.50, p = 0.36, treatment 4 of 58 (6.9%), control 8 of 58 (13.8%), NNT 14. | |
| NIV, 47.8% lower, RR 0.52, p = 0.04, treatment 12 of 58 (20.7%), control 23 of 58 (39.7%), NNT 5.3. | |
| Ganmaa, 3/12/2026, Double Blind Randomized Controlled Trial, placebo-controlled, multiple countries, peer-reviewed, 27 authors, study period 29 December, 2020 - 1 July, 2022, trial NCT04536298 (history) (VIVID). | HCU, 4.0% lower, OR 0.96, p = 0.76, treatment 863, control 884, COVID-19 related HCU, RR approximated with OR. |
| HCU, 3.0% lower, OR 0.97, p = 0.79, treatment 863, control 884, all-cause HCU, RR approximated with OR. | |
| risk of long COVID, 17.0% lower, OR 0.83, p = 0.24, treatment 863, control 884, RR approximated with OR. | |
| risk of transmission, 71.0% higher, OR 1.71, p = 0.21, treatment 139, control 138, RR approximated with OR. | |
| Giannini, 1/14/2021, retrospective, Italy, peer-reviewed, 21 authors, dosage 200,000IU days 1-2. | risk of death/ICU, 36.6% lower, RR 0.63, p = 0.13, treatment 14 of 36 (38.9%), control 29 of 55 (52.7%), NNT 7.2, odds ratio converted to relative risk. |
| Güven, 7/23/2021, retrospective, Turkey, peer-reviewed, 2 authors, dosage 300,000IU single dose, excluded in exclusion analyses: very late stage, ICU patients. | risk of death, 24.8% lower, RR 0.75, p = 0.32, treatment 43 of 113 (38.1%), control 30 of 62 (48.4%), NNT 9.7, odds ratio converted to relative risk. |
| Hafez (B), 8/9/2022, retrospective, Egypt, peer-reviewed, 2 authors, study period April 2020 - June 2020, dosage 50,000IU days 1, 3, 5, 7, 9, 11, 13, 50,000IU every other day for two weeks or one intramuscular shot of 300,000IU. | risk of death, 93.7% lower, RR 0.06, p = 0.07, treatment 0 of 7 (0.0%), control 12 of 30 (40.0%), NNT 2.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), high dose, 50,000IU every other day for two weeks or one intramuscular shot of 300,000IU. |
| risk of death, 58.3% lower, RR 0.42, p = 0.28, treatment 2 of 12 (16.7%), control 12 of 30 (40.0%), NNT 4.3, low dose, ≤10,000IU/day. | |
| Hafezi, 10/22/2022, retrospective, United Arab Emirates, peer-reviewed, 8 authors, study period September 2020 - January 2021, dosage 50,000IU days 1, 8, 15, excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 63.0% lower, HR 0.37, p = 0.04, treatment 8 of 43 (18.6%), control 12 of 37 (32.4%), NNT 7.2, Cox proportional hazards, day 29. |
| Jaun, 4/25/2023, Double Blind Randomized Controlled Trial, placebo-controlled, Switzerland, peer-reviewed, 14 authors, study period December 2020 - August 2021, average treatment delay 8.0 days, dosage 140,000IU single dose. | risk of death, 50.0% lower, RR 0.50, p = 0.56, treatment 1 of 39 (2.6%), control 2 of 39 (5.1%), NNT 39, odds ratio converted to relative risk. |
| risk of mechanical ventilation, 300.0% higher, RR 4.00, p = 0.20, treatment 4 of 39 (10.3%), control 1 of 39 (2.6%), odds ratio converted to relative risk. | |
| risk of ICU admission, 32.1% higher, RR 1.32, p = 0.69, treatment 4 of 39 (10.3%), control 4 of 39 (10.3%), odds ratio converted to relative risk. | |
| Jevalikar, 12/28/2020, prospective, India, peer-reviewed, 8 authors, dosage 60,000IU single dose, median total dose. | risk of death, 82.0% lower, RR 0.18, p = 0.12, treatment 1 of 128 (0.8%), control 3 of 69 (4.3%), NNT 28. |
| risk of ICU admission, 33.7% lower, RR 0.66, p = 0.29, treatment 16 of 128 (12.5%), control 13 of 69 (18.8%), NNT 16. | |
| risk of oxygen therapy, 31.7% lower, RR 0.68, p = 0.06, treatment 38 of 128 (29.7%), control 30 of 69 (43.5%), NNT 7.3. | |
| Karimpour-Razkenari, 10/3/2022, retrospective, Iran, peer-reviewed, median age 58.5, 9 authors, study period 23 February, 2020 - 23 May, 2020, dosage not specified. | risk of death, 79.0% lower, RR 0.21, p < 0.001, treatment 10 of 124 (8.1%), control 93 of 329 (28.3%), NNT 4.9, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, multivariable. |
| Karonova (B), 6/23/2022, Randomized Controlled Trial, Russia, peer-reviewed, 12 authors, study period 30 November, 2020 - 20 March, 2021, dosage 50,000IU days 1, 8, trial NCT05166005 (history). | risk of ICU admission, 85.9% lower, RR 0.14, p = 0.11, treatment 0 of 56 (0.0%), control 3 of 54 (5.6%), NNT 18, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 9. |
| risk of oxygen therapy, 7.0% lower, RR 0.93, p = 0.85, treatment 27 of 56 (48.2%), control 28 of 54 (51.9%), NNT 27, baseline oxygen supplementation was higher in the treatment group, 38 vs. 32, day 9. | |
| Krishnan, 7/20/2020, retrospective, USA, peer-reviewed, 13 authors, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 19.0% lower, RR 0.81, p = 0.42, treatment 8 of 16 (50.0%), control 84 of 136 (61.8%), NNT 8.5. |
| Lakkireddy, 7/27/2022, Randomized Controlled Trial, India, peer-reviewed, mean age 45.5, 9 authors, dosage 60,000IU days 1-8, 8 or 10 days depending on BMI. | risk of death, 60.9% lower, RR 0.39, p = 0.27, treatment 2 of 44 (4.5%), control 5 of 43 (11.6%), NNT 14. |
| risk of ICU admission, 21.8% lower, RR 0.78, p = 0.74, treatment 4 of 44 (9.1%), control 5 of 43 (11.6%), NNT 39. | |
| hospitalization time, 7.1% lower, relative time 0.93, p = 0.90, treatment 44, control 43. | |
| Leal-Martínez, 10/25/2021, Randomized Controlled Trial, Mexico, peer-reviewed, 7 authors, study period 1 September, 2020 - 28 February, 2021, dosage 4,000IU days 1-21, this trial uses multiple treatments in the treatment arm (combined with comprehensive nutritional support) - results of individual treatments may vary, trial NCT04507867 (history), excluded in exclusion analyses: combined treatments may contribute more to the effect seen. | risk of death, 85.7% lower, RR 0.14, p = 0.03, treatment 1 of 40 (2.5%), control 7 of 40 (17.5%), NNT 6.7. |
| risk of mechanical ventilation, 57.1% lower, RR 0.43, p = 0.31, treatment 3 of 40 (7.5%), control 7 of 40 (17.5%), NNT 10.0. | |
| Ling, 12/11/2020, retrospective, United Kingdom, peer-reviewed, 7 authors, dosage 40,000IU weekly, regimen varied with 77% receiving a total of 40,000IU/week. | risk of death, 79.8% lower, RR 0.20, p < 0.001, treatment 73, control 253, odds ratio converted to relative risk, primary cohort. |
| risk of death, 55.5% lower, RR 0.44, p = 0.02, treatment 80, control 443, odds ratio converted to relative risk, validation cohort. | |
| Lohia (B), 3/4/2021, retrospective, USA, peer-reviewed, 4 authors, dosage not specified. | risk of death, 10.7% lower, RR 0.89, p = 0.80, treatment 26, control 69, odds ratio converted to relative risk, <20 ng/mL, control prevalence approximated with overall prevalence. |
| risk of mechanical ventilation, 26.9% lower, RR 0.73, p = 0.51, treatment 26, control 69, odds ratio converted to relative risk, <20 ng/mL, control prevalence approximated with overall prevalence. | |
| risk of ICU admission, 2.7% lower, RR 0.97, p = 0.93, treatment 26, control 69, odds ratio converted to relative risk, <20 ng/mL, control prevalence approximated with overall prevalence. | |
| Maghbooli, 10/13/2021, Double Blind Randomized Controlled Trial, Iran, peer-reviewed, 12 authors, dosage calcifediol 25μg daily, mean daily dose. | risk of death, 40.0% lower, RR 0.60, p = 0.72, treatment 3 of 53 (5.7%), control 5 of 53 (9.4%), NNT 26. |
| risk of mechanical ventilation, 60.0% lower, RR 0.40, p = 0.44, treatment 2 of 53 (3.8%), control 5 of 53 (9.4%), NNT 18. | |
| risk of ICU admission, 40.0% lower, RR 0.60, p = 0.42, treatment 6 of 53 (11.3%), control 10 of 53 (18.9%), NNT 13. | |
| ICU time, 36.4% lower, relative time 0.64, p = 0.20, treatment 53, control 53. | |
| hospitalization time, 16.7% lower, relative time 0.83, p = 0.10, treatment 53, control 53. | |
| Mahmood, 12/29/2021, retrospective, United Kingdom, peer-reviewed, 4 authors, study period 23 March, 2020 - 31 December, 2020, dosage varies, excluded in exclusion analyses: unadjusted results with no group details; substantial unadjusted confounding by indication likely. | risk of death, 30.5% lower, RR 0.70, p = 0.10, treatment 45 of 238 (18.9%), control 31 of 114 (27.2%), NNT 12, started after admission, late treatment result. |
| Mariani, 5/27/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Argentina, peer-reviewed, mean age 59.1, 33 authors, study period 14 August, 2020 - 22 June, 2021, average treatment delay 7.0 days, dosage 500,000IU single dose, trial NCT04411446 (history) (CARED). | risk of death, 124.0% higher, RR 2.24, p = 0.45, treatment 5 of 115 (4.3%), control 2 of 103 (1.9%). |
| risk of mechanical ventilation, 25.0% lower, RR 0.75, p = 0.85, treatment 5 of 115 (4.3%), control 6 of 103 (5.8%), NNT 68. | |
| risk of ICU admission, 27.0% lower, RR 0.73, p = 0.62, treatment 9 of 115 (7.8%), control 11 of 103 (10.7%), NNT 35. | |
| risk of progression, 3.0% lower, OR 0.97, p = 0.82, treatment 115, control 103, Wilcoxon-Mann-Whitney, primary outcome, RR approximated with OR. | |
| risk of progression, 32.8% lower, RR 0.67, p = 0.71, treatment 3 of 115 (2.6%), control 4 of 103 (3.9%), NNT 78, Δ rSOFA 4. | |
| risk of progression, 79.1% higher, RR 1.79, p = 0.30, treatment 10 of 115 (8.7%), control 5 of 103 (4.9%), Δ rSOFA 3. | |
| risk of progression, 25.4% lower, RR 0.75, p = 0.76, treatment 5 of 115 (4.3%), control 6 of 103 (5.8%), NNT 68, Δ rSOFA 2. | |
| risk of progression, 16.0% lower, RR 0.84, p = 0.70, treatment 15 of 115 (13.0%), control 16 of 103 (15.5%), NNT 40, Δ rSOFA 1. | |
| Mazziotti, 3/5/2021, retrospective, Italy, peer-reviewed, 11 authors, dosage varies. | risk of death, 19.0% lower, OR 0.81, p = 0.49, treatment 116, control 232, supplementation, RR approximated with OR. |
| risk of mechanical ventilation, 67.0% higher, OR 1.67, p = 0.08, treatment 116, control 232, supplementation, RR approximated with OR. | |
| Milan, 4/30/2024, retrospective, Philippines, peer-reviewed, median age 11.0, 5 authors, study period 1 April, 2020 - 31 August, 2021. | risk of death, 46.5% lower, RR 0.53, p = 0.18, treatment 9 of 122 (7.4%), control 8 of 58 (13.8%), NNT 16, day 45. |
| risk of mechanical ventilation, 20.8% lower, RR 0.79, p = 0.53, treatment 20 of 122 (16.4%), control 12 of 58 (20.7%), NNT 23, day 45. | |
| risk of ICU admission, 15.9% lower, RR 0.84, p = 0.69, treatment 23 of 122 (18.9%), control 13 of 58 (22.4%), NNT 28, day 45. | |
| Mingiano, 7/30/2023, retrospective, Italy, peer-reviewed, 11 authors, study period November 2020 - February 2021, dosage calcifediol 450μg days 1-2, patients with deficiency only. | risk of death, 38.8% lower, RR 0.61, p = 0.04, treatment 13 of 56 (23.2%), control 88 of 232 (37.9%), NNT 6.8. |
| risk of oxygen therapy, 23.1% lower, RR 0.77, p = 0.22, treatment 18 of 56 (32.1%), control 97 of 232 (41.8%), NNT 10. | |
| hospitalization time, 34.6% lower, relative time 0.65, p = 0.01, treatment 56, control 232. | |
| Murai, 11/17/2020, Double Blind Randomized Controlled Trial, Brazil, peer-reviewed, 17 authors, study period 2 June, 2020 - 27 August, 2020, average treatment delay 10.2 days, dosage 200,000IU single dose, trial NCT04449718 (history), excluded in exclusion analyses: very late stage, >50% on oxygen/ventilation at baseline; very late stage study using cholecalciferol instead of calcifediol or calcitriol. | risk of death, 48.7% higher, RR 1.49, p = 0.43, treatment 9 of 119 (7.6%), control 6 of 118 (5.1%). |
| risk of mechanical ventilation, 47.5% lower, RR 0.52, p = 0.09, treatment 9 of 119 (7.6%), control 17 of 118 (14.4%), NNT 15. | |
| risk of ICU admission, 24.6% lower, RR 0.75, p = 0.30, treatment 19 of 119 (16.0%), control 25 of 118 (21.2%), NNT 19. | |
| risk of no hospital discharge, 6.5% lower, HR 0.93, p = 0.63, treatment 119, control 118, inverted to make HR<1 favor treatment. | |
| Nogués, 1/22/2021, prospective quasi-randomized (ward), Spain, peer-reviewed, 16 authors, dosage calcifediol 0.5mg day 1, 0.27mg day 3, 0.27mg day 7, 0.27mg day 15, 0.27mg day 30. | risk of death, 79.0% lower, RR 0.21, p = 0.001, treatment 21 of 447 (4.7%), control 62 of 391 (15.9%), NNT 9.0, adjusted per study, ITT. |
| risk of death, 48.0% lower, RR 0.52, p = 0.001, treatment 500, control 338, adjusted per study, including patients treated later. | |
| risk of ICU admission, 87.0% lower, RR 0.13, p < 0.001, treatment 20 of 447 (4.5%), control 82 of 391 (21.0%), NNT 6.1, adjusted per study, ITT. | |
| Ogasawara, 9/1/2023, retrospective, Japan, peer-reviewed, 10 authors, study period April 2021 - September 2022, dosage alfacalcidol 1μg days 1-8, median duration, alfacalcidol and eldecalcitol used. | risk of death, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 54 (0.0%), control 1 of 54 (1.9%), NNT 54, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of progression, 77.8% lower, RR 0.22, p = 0.05, treatment 2 of 54 (3.7%), control 9 of 54 (16.7%), NNT 7.7, high-flow oxygen, mechanical ventilation, or mortality, primary outcome. | |
| risk of oxygen therapy, 75.0% lower, RR 0.25, p = 0.09, treatment 2 of 54 (3.7%), control 8 of 54 (14.8%), NNT 9.0. | |
| Rastogi, 11/12/2020, Randomized Controlled Trial, India, peer-reviewed, 8 authors, dosage 60,000IU days 1-7, trial NCT04459247 (history) (SHADE). | risk of no viral clearance, 52.6% lower, RR 0.47, p = 0.02, treatment 6 of 16 (37.5%), control 19 of 24 (79.2%), NNT 2.4. |
| Sabico, 6/24/2021, Randomized Controlled Trial, Saudi Arabia, peer-reviewed, 12 authors, study period 29 July, 2020 - 22 November, 2020. | risk of death, 192.1% higher, RR 2.92, p = 1.00, treatment 1 of 38 (2.6%), control 0 of 35 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm). |
| risk of ICU admission, 38.9% lower, RR 0.61, p = 0.66, treatment 2 of 36 (5.6%), control 3 of 33 (9.1%), NNT 28. | |
| time to discharge, 14.3% lower, relative time 0.86, p = 0.14, treatment 36, control 33. | |
| recovery time, 14.1% lower, relative time 0.86, p = 0.97, treatment 36, control 33, fever. | |
| recovery time, 20.5% lower, relative time 0.79, p = 0.24, treatment 36, control 33, dyspnea. | |
| Saheb Sharif-Askari (B), 8/24/2022, retrospective, USA, peer-reviewed, 10 authors, dosage 50,000IU days 1, 8, 15, excluded in exclusion analyses: very late stage study using cholecalciferol instead of calcifediol or calcitriol. | ICU time, 35.7% lower, relative time 0.64, p = 0.01, treatment 20, control 25. |
| Salman, 6/16/2023, Randomized Controlled Trial, Pakistan, peer-reviewed, 6 authors, study period January 2021 - May 2021, dosage 4,000IU days 1-14. | risk of death, 60.0% lower, RR 0.40, p = 0.07, treatment 6 of 150 (4.0%), control 15 of 150 (10.0%), NNT 17. |
| risk of mechanical ventilation, 16.7% lower, RR 0.83, p = 0.55, treatment 25 of 150 (16.7%), control 30 of 150 (20.0%), NNT 30. | |
| risk of ICU admission, 12.5% lower, RR 0.88, p = 0.85, treatment 14 of 150 (9.3%), control 16 of 150 (10.7%), NNT 75. | |
| hospitalization time, 18.2% lower, relative time 0.82, p = 0.001, treatment 150, control 150. | |
| recovery time, 22.2% lower, relative time 0.78, p = 0.001, treatment 150, control 150. | |
| Sanz, 6/12/2024, Double Blind Randomized Controlled Trial, placebo-controlled, Argentina, peer-reviewed, mean age 59.0, 7 authors, study period August 2021 - June 2022, dosage 10,000IU days 1-10. | risk of death, 80.0% lower, RR 0.20, p = 0.48, treatment 0 of 11 (0.0%), control 2 of 11 (18.2%), NNT 5.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of mechanical ventilation, 83.3% lower, RR 0.17, p = 0.06, treatment 1 of 11 (9.1%), control 6 of 11 (54.5%), NNT 2.2. | |
| risk of ICU admission, 60.0% lower, RR 0.40, p = 0.36, treatment 2 of 11 (18.2%), control 5 of 11 (45.5%), NNT 3.7. | |
| Sarhan, 9/27/2022, Randomized Controlled Trial, Egypt, peer-reviewed, 9 authors, study period December 2020 - June 2021, dosage 200,000IU single dose, trial NCT04738760 (history). | risk of death, 18.5% lower, RR 0.81, p = 0.003, treatment 26 of 58 (44.8%), control 30 of 58 (51.7%), NNT 14, adjusted per study, odds ratio converted to relative risk, multivariable. |
| improvement, 74.4% better, OR 0.26, p = 0.03, treatment 58, control 58, adjusted per study, inverted to make OR<1 favor treatment, multivariable, RR approximated with OR. | |
| time to improvement, 28.8% lower, relative time 0.71, p = 0.002, treatment 58, control 58. | |
| hospitalization time, 31.5% lower, relative time 0.69, p = 0.04, treatment 58, control 58. | |
| Seely, 9/22/2023, Double Blind Randomized Controlled Trial, placebo-controlled, Canada, peer-reviewed, mean age 39.9, 10 authors, study period September 2021 - April 2022, dosage 51,000IU day 1, 1,000IU days 2-21, this trial uses multiple treatments in the treatment arm (combined with vitamin C, D, K2, and zinc) - results of individual treatments may vary, trial NCT04780061 (history). | ER visit, 47.6% lower, RR 0.52, p = 0.68, treatment 2 of 42 (4.8%), control 4 of 44 (9.1%), NNT 23. |
| relative mean cumulative symptom score, 13.8% better, RR 0.86, p = 0.41, treatment mean 166.3 (±92.3) n=34, control mean 192.9 (±153.6) n=24. | |
| EQ-VAS average score <80, 29.4% lower, RR 0.71, p = 0.54, treatment 7 of 34 (20.6%), control 7 of 24 (29.2%), NNT 12, average daily EQ-VAS score <80. | |
| relative EQ5D improvement, 28.6% better, RR 0.71, p = 0.44, treatment 32, control 31, relative improvement in EQ5D, week 1. | |
| relative EQ5D improvement, 14.3% better, RR 0.86, p = 0.73, treatment 33, control 30, relative improvement in EQ5D, week 2. | |
| relative EQ5D improvement, 50.0% better, RR 0.50, p = 0.17, treatment 32, control 33, relative improvement in EQ5D, week 3. | |
| relative EQ5D improvement, 12.5% worse, RR 1.12, p = 0.47, treatment 30, control 25, relative improvement in EQ5D, week 4. | |
| recovery time, 4.0% higher, relative time 1.04, p = 0.81, treatment 34, control 24. | |
| risk of long COVID, 12.1% lower, RR 0.88, p = 1.00, treatment 3 of 33 (9.1%), control 3 of 29 (10.3%), NNT 80, 12 weeks. | |
| risk of long COVID, 35.7% lower, RR 0.64, p = 0.69, treatment 3 of 35 (8.6%), control 4 of 30 (13.3%), NNT 21, 8 weeks. | |
| risk of long COVID, 0.6% lower, RR 0.99, p = 1.00, treatment 6 of 35 (17.1%), control 5 of 29 (17.2%), NNT 1015, 4 weeks. | |
| Shahid, 6/17/2022, retrospective, USA, peer-reviewed, 2 authors, dosage not specified, excluded in exclusion analyses: minimal details provided. | risk of death, 38.0% lower, RR 0.62, p < 0.001, treatment 705, control 773. |
| Shamsi, 7/17/2023, retrospective, Iran, peer-reviewed, 4 authors, study period 1 March, 2020 - 1 August, 2021, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 57.5% lower, RR 0.42, p = 0.70, treatment 1 of 17 (5.9%), control 23 of 166 (13.9%), NNT 13. |
| Singh, 6/1/2022, Double Blind Randomized Controlled Trial, placebo-controlled, India, peer-reviewed, 15 authors, study period 1 August, 2021 - 10 December, 2021, dosage 600,000IU single dose, trial NCT04952857 (history) (Shade-S). | risk of death, 45.0% lower, RR 0.55, p = 0.046, treatment 11 of 45 (24.4%), control 20 of 45 (44.4%), NNT 5.0. |
| risk of no recovery, 40.0% lower, RR 0.60, p = 0.01, treatment 45, control 45. | |
| Soliman, 9/1/2021, Randomized Controlled Trial, placebo-controlled, Egypt, peer-reviewed, 3 authors, dosage 200,000IU single dose. | risk of death, 63.4% lower, RR 0.37, p = 0.21, treatment 7 of 40 (17.5%), control 3 of 16 (18.8%), adjusted per study, odds ratio converted to relative risk, logistic regression. |
| risk of mechanical ventilation, 20.0% lower, RR 0.80, p = 0.56, treatment 14 of 40 (35.0%), control 7 of 16 (43.8%), NNT 11, unadjusted. | |
| risk of no recovery, 20.0% lower, RR 0.80, p = 0.56, treatment 14 of 40 (35.0%), control 7 of 16 (43.8%), NNT 11, unadjusted. | |
| Sümegi, 1/30/2025, retrospective, Hungary, peer-reviewed, mean age 67.5, 8 authors, study period December 2022 - April 2023, dosage 30,000IU days 1-3, 3,000IU days 4-28, 30,000IU for 3 days or 12,000IU for 7 days, followed by 3,000IU daily. | risk of death, 67.3% lower, RR 0.33, p < 0.001, treatment 10 of 76 (13.2%), control 29 of 72 (40.3%), NNT 3.7. |
| Tan (B), 6/10/2020, retrospective, Singapore, peer-reviewed, 14 authors, dosage 1,000IU daily, this trial uses multiple treatments in the treatment arm (combined with magnesium and vitamin B12) - results of individual treatments may vary. | risk of oxygen therapy, 80.5% lower, RR 0.20, p = 0.04, treatment 3 of 17 (17.6%), control 16 of 26 (61.5%), NNT 2.3, adjusted per study, multivariate. |
| risk of ICU admission, 80.9% lower, RR 0.19, p = 0.07, treatment 1 of 17 (5.9%), control 8 of 26 (30.8%), NNT 4.0, no adjusted result available. | |
| Taslim, 5/1/2023, Single Blind Randomized Controlled Trial, Indonesia, peer-reviewed, 10 authors, study period 1 April, 2021 - 30 September, 2021, trial NCT05126602 (history). | risk of oxygen therapy, 71.4% lower, RR 0.29, p = 0.01, treatment 4 of 30 (13.3%), control 14 of 30 (46.7%), NNT 3.0. |
| risk of oxygen therapy, 66.7% lower, RR 0.33, p = 0.61, treatment 1 of 30 (3.3%), control 3 of 30 (10.0%), NNT 15, mask. | |
| risk of oxygen therapy, 72.7% lower, RR 0.27, p = 0.03, treatment 3 of 30 (10.0%), control 11 of 30 (36.7%), NNT 3.8, nasal cannula. | |
| risk of no recovery, 60.0% lower, RR 0.40, p = 0.42, treatment 2 of 30 (6.7%), control 5 of 30 (16.7%), NNT 10.0, fever. | |
| hospitalization time, 21.0% lower, relative time 0.79, p < 0.001, treatment mean 11.63 (±2.5) n=30, control mean 14.73 (±3.45) n=30. | |
| time to viral-, 37.6% lower, relative time 0.62, p < 0.001, treatment mean 6.53 (±1.17) n=30, control mean 10.47 (±2.56) n=30, primary outcome. | |
| Torres, 4/14/2022, Single Blind Randomized Controlled Trial, Spain, peer-reviewed, median age 65.0, 51 authors, study period June 2020 - March 2021, average treatment delay 7.0 days, dosage 10,000IU days 1-14. | risk of death, 7.3% higher, RR 1.07, p = 1.00, treatment 1 of 41 (2.4%), control 1 of 44 (2.3%). |
| risk of ICU admission, 57.1% lower, RR 0.43, p = 0.44, treatment 2 of 41 (4.9%), control 5 of 44 (11.4%), NNT 15. | |
| risk of ARDS, 28.5% lower, RR 0.72, p = 0.74, treatment 4 of 41 (9.8%), control 6 of 44 (13.6%), NNT 26. | |
| Vasconcelos, 2/19/2025, retrospective, Portugal, peer-reviewed, 3 authors, study period 14 April, 2020 - 31 October, 2020, dosage 125,000IU days 1-2. | risk of death, 73.2% lower, RR 0.27, p = 0.02, treatment 9 of 72 (12.5%), control 18 of 54 (33.3%), NNT 4.8, adjusted per study, odds ratio converted to relative risk, 60 days after discharge, multivariable. |
| risk of death, 66.7% lower, RR 0.33, p = 0.04, treatment 9 of 72 (12.5%), control 16 of 54 (29.6%), NNT 5.8, adjusted per study, odds ratio converted to relative risk, in hospital, multivariable. | |
| risk of death, 86.9% lower, RR 0.13, p = 0.006, treatment 3 of 72 (4.2%), control 13 of 54 (24.1%), NNT 5.0, adjusted per study, odds ratio converted to relative risk, in ICU, multivariable. | |
| Yildiz, 9/27/2021, retrospective, Turkey, peer-reviewed, 5 authors, dosage 300,000IU single dose. | risk of death, 80.9% lower, RR 0.19, p = 0.04, treatment 1 of 37 (2.7%), control 24 of 170 (14.1%), NNT 8.8. |
| risk of ICU admission, 94.5% lower, RR 0.06, p = 0.13, treatment 0 of 37 (0.0%), control 14 of 170 (8.2%), NNT 12, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| hospitalization time, 9.6% lower, relative time 0.90, p = 0.32, treatment 37, control 170. | |
| Zangeneh, 5/13/2022, retrospective, Iran, peer-reviewed, 3 authors, dosage not specified, excluded in exclusion analyses: data issues pending author response. | risk of death, 26.0% higher, HR 1.26, p = 0.40, Cox proportional hazards. |
| Zurita-Cruz, 7/25/2022, Single Blind Randomized Controlled Trial, Mexico, peer-reviewed, median age 12.0, 7 authors, study period 24 March, 2020 - 31 March, 2021, dosage 2,000IU daily, daily, 1,000IU for children <1 year, trial NCT04502667 (history), excluded in exclusion analyses: randomization resulted in significant baseline differences that were not adjusted for. | risk of death, 79.2% lower, RR 0.21, p = 0.11, treatment 1 of 20 (5.0%), control 6 of 25 (24.0%), NNT 5.3. |
| risk of mechanical ventilation, 72.2% lower, RR 0.28, p = 0.08, treatment 2 of 20 (10.0%), control 9 of 25 (36.0%), NNT 3.8. | |
| risk of ICU admission, 73.2% lower, RR 0.27, p = 0.006, treatment 3 of 20 (15.0%), control 14 of 25 (56.0%), NNT 2.4. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Abdulateef, 4/8/2021, retrospective, Iraq, peer-reviewed, 7 authors, study period July 2020 - August 2020, dosage varies, excluded in exclusion analyses: unadjusted results with no group details. | risk of hospitalization, 40.9% lower, RR 0.59, p = 0.30, treatment 6 of 127 (4.7%), control 24 of 300 (8.0%), NNT 31, unadjusted. |
| Ahmed (B), 11/21/2021, retrospective, USA, preprint, 5 authors, dosage not specified. | risk of death, 10.5% lower, RR 0.90, p = 0.28. |
| Akbar, 11/7/2023, retrospective, Qatar, peer-reviewed, mean age 40.3, 9 authors, study period March 2020 - September 2020, dosage not specified. | risk of case, 19.0% lower, OR 0.81, p = 0.02, treatment 2,402, control 7,598, adjusted per study, multivariable, model 2, RR approximated with OR. |
| Aldwihi, 5/11/2021, retrospective, Saudi Arabia, peer-reviewed, survey, mean age 36.5, 8 authors, study period August 2020 - October 2020, dosage not specified. | risk of hospitalization, 49.3% higher, RR 1.49, p = 0.002, treatment 94 of 259 (36.3%), control 143 of 479 (29.9%), adjusted per study, odds ratio converted to relative risk, multivariable. |
| Annweiler (D), 11/2/2020, retrospective, France, peer-reviewed, mean age 88.0, 7 authors, dosage 50,000IU monthly, dose varies - 50,000 IU/month, or 80,000IU/100,000IU every 2-3 months. | risk of death, 93.0% lower, RR 0.07, p = 0.02, treatment 2 of 29 (6.9%), control 10 of 32 (31.2%), NNT 4.1, adjusted per study, regular bolus supplementation. |
| Arboleda, 3/13/2024, prospective, Colombia, peer-reviewed, 4 authors, dosage 5,000IU daily, this trial uses multiple treatments in the treatment arm (combined with vitamin C) - results of individual treatments may vary, excluded in exclusion analyses: unadjusted results with no group details. | risk of case, 35.7% lower, RR 0.64, p = 0.03, treatment 26 of 214 (12.1%), control 115 of 609 (18.9%), NNT 15. |
| Arroyo-Díaz, 9/24/2021, retrospective, Spain, peer-reviewed, 11 authors, dosage not specified. | risk of death, 12.4% higher, RR 1.12, p = 0.59, treatment 50 of 189 (26.5%), control 167 of 1,078 (15.5%), adjusted per study, odds ratio converted to relative risk. |
| risk of mechanical ventilation, 43.3% lower, RR 0.57, p = 0.22, treatment 11 of 189 (5.8%), control 113 of 1,078 (10.5%), NNT 21, adjusted per study, odds ratio converted to relative risk. | |
| risk of ICU admission, 44.2% lower, RR 0.56, p = 0.03, treatment 13 of 189 (6.9%), control 133 of 1,078 (12.3%), NNT 18, unadjusted. | |
| hospitalization time, 11.8% lower, relative time 0.88, p = 0.20, treatment 189, control 1,078, unadjusted. | |
| Aweimer, 3/29/2023, retrospective, Germany, peer-reviewed, median age 67.0, 19 authors, study period 1 March, 2020 - 31 August, 2021, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 20.9% lower, RR 0.79, p = 0.31, treatment 7 of 12 (58.3%), control 101 of 137 (73.7%), NNT 6.5. |
| Bagheri, 9/1/2021, retrospective, Iran, peer-reviewed, 6 authors, dosage not specified. | risk of severe case, 70.9% lower, OR 0.29, p = 0.02, treatment 131, control 379, adjusted per study, multinomial logistic regression, RR approximated with OR. |
| risk of hospitalization, 37.9% lower, RR 0.62, p = 0.11, treatment 28 of 131 (21.4%), control 143 of 379 (37.7%), NNT 6.1, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, binary logistic regression. | |
| Baralić, 4/24/2023, prospective, France, peer-reviewed, 15 authors, study period March 2020 - September 2022, dosage not specified. | risk of death, 66.8% lower, HR 0.33, p = 0.02, treatment 7 of 31 (22.6%), control 11 of 21 (52.4%), NNT 3.4, Cox proportional hazards. |
| Bhat, 3/6/2023, prospective, placebo-controlled, India, peer-reviewed, 13 authors, dosage calcifediol 50μg days 1-180, trial CTRI/2021/08/035709. | risk of symptomatic case, 34.2% lower, RR 0.66, p = 0.01, treatment 59 of 262 (22.5%), control 52 of 152 (34.2%), NNT 8.6. |
| Blanch-Rubió, 10/20/2020, retrospective, Spain, peer-reviewed, mean age 66.4, 11 authors, dosage not specified. | risk of case, 8.0% lower, RR 0.92, p = 0.68, treatment 62 of 1,303 (4.8%), control 47 of 799 (5.9%), adjusted per study. |
| Brunvoll, 9/7/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Norway, peer-reviewed, mean age 44.9, 15 authors, study period 10 November, 2020 - 2 June, 2021, dosage 400IU daily, this trial uses multiple treatments in the treatment arm (combined with cod liver oil) - results of individual treatments may vary, trial NCT04609423 (history). | risk of ICU admission, 0.3% higher, RR 1.00, p = 1.00, treatment 4 of 17,278 (0.0%), control 4 of 17,323 (0.0%). |
| risk of hospitalization, 10.9% lower, RR 0.89, p = 1.00, treatment 8 of 17,278 (0.0%), control 9 of 17,323 (0.1%), NNT 17692. | |
| risk of severe case, 20.0% higher, RR 1.20, p = 0.17, treatment 121 of 17,278 (0.7%), control 101 of 17,323 (0.6%). | |
| risk of case, no change, RR 1.00, p = 0.98, treatment 227 of 17,278 (1.3%), control 228 of 17,323 (1.3%), NNT 42377. | |
| Campi, 6/14/2021, prospective, Italy, peer-reviewed, 21 authors, dosage not specified, excluded in exclusion analyses: significant unadjusted differences between groups. | risk of severe case, 88.4% lower, OR 0.12, p < 0.001, treatment 31 of 103 (30.1%) cases, 41 of 52 (78.8%) controls, NNT 2.3, case control OR, vitamin D supplementation, hospitalized patients vs. controls. |
| Cangiano, 12/22/2020, retrospective, Italy, peer-reviewed, 14 authors, dosage 25,000IU 2x per month. | risk of death, 70.0% lower, RR 0.30, p = 0.04, treatment 3 of 20 (15.0%), control 39 of 78 (50.0%), NNT 2.9. |
| Cereda, 11/11/2020, retrospective, Italy, peer-reviewed, mean age 68.8, 7 authors, dosage varies. | risk of death, 73.0% higher, RR 1.73, p = 0.14, treatment 7 of 18 (38.9%), control 40 of 152 (26.3%), odds ratio converted to relative risk, ≥25,000IU/month for at least 3 months. |
| risk of hospitalization, 17.3% higher, RR 1.17, p = 0.68, treatment 7 of 27 (25.9%), control 36 of 170 (21.2%), odds ratio converted to relative risk. | |
| Comunale, 1/24/2024, retrospective, USA, peer-reviewed, 6 authors, study period November 2020 - May 2021, dosage not specified, trial NCT04639375 (history). | risk of symptomatic case, 91.0% lower, OR 0.09, p < 0.001, treatment 100, control 182, adjusted per study, multivariable, RR approximated with OR. |
| risk of case, 88.0% lower, OR 0.12, p = 0.001, treatment 100, control 182, adjusted per study, multivariable, RR approximated with OR. | |
| De Nicolò, 12/29/2022, prospective, Italy, peer-reviewed, 11 authors, study period January 2021 - April 2021, dosage not specified. | risk of IgG positive, 88.4% lower, OR 0.12, p = 0.002, treatment 43, control 63, adjusted per study, multivariable, RR approximated with OR. |
| di Filippo (C), 6/10/2026, retrospective, Italy, peer-reviewed, 5 authors, study period January 2021 - December 2021, trial NCT06452082 (history). | risk of symptomatic case, 50.0% lower, RR 0.50, p = 0.12, treatment 7 of 39 (17.9%), control 14 of 39 (35.9%), NNT 5.6, matched population. |
| risk of symptomatic case, 49.7% lower, RR 0.50, p = 0.04, treatment 12 of 70 (17.1%), control 15 of 44 (34.1%), NNT 5.9, all patients. | |
| di Filippo (B), 3/23/2026, retrospective, Italy, peer-reviewed, 9 authors, study period March 2020 - May 2021, trial NCT06452082 (history), excluded in exclusion analyses: potentially significant confounding by treatment propensity. | risk of long COVID, 78.0% lower, OR 0.22, p = 0.02, treatment 43, control 43, adjusted per study, Table 6, RR approximated with OR. |
| Dudley, 5/18/2021, retrospective, United Kingdom, peer-reviewed, 5 authors, dosage 800IU daily. | risk of symptomatic case, 22.4% lower, RR 0.78, p = 0.65, treatment 15 of 58 (25.9%), control 2 of 6 (33.3%), NNT 13, positive test. |
| Fasano, 6/2/2021, retrospective, Italy, peer-reviewed, 7 authors, dosage not specified. | risk of case, 42.0% lower, RR 0.58, p = 0.048, treatment 13 of 329 (4.0%), control 92 of 1,157 (8.0%), NNT 25, odds ratio converted to relative risk. |
| Gibbons, 11/12/2022, retrospective, USA, peer-reviewed, 7 authors, dosage varies. | risk of death, 33.3% lower, HR 0.67, p < 0.001, treatment 5,315 of 199,498 (2.7%), control 6,591 of 199,498 (3.3%), D3, propensity score matching, Cox proportional hazards. |
| risk of death, 23.5% lower, HR 0.77, p = 0.10, treatment 716 of 33,216 (2.2%), control 987 of 33,216 (3.0%), NNT 123, D2, propensity score matching, Cox proportional hazards. | |
| risk of case, 20.3% lower, HR 0.80, p < 0.001, treatment 462 of 199,498 (0.2%), control 689 of 199,498 (0.3%), D3, propensity score matching, Cox proportional hazards. | |
| risk of case, 28.0% lower, HR 0.72, p < 0.001, treatment 65 of 33,216 (0.2%), control 86 of 33,216 (0.3%), NNT 1582, D2, propensity score matching, Cox proportional hazards. | |
| Golabi (B), 8/26/2021, retrospective, Iran, peer-reviewed, 10 authors, dosage not specified. | risk of case, 25.4% higher, OR 1.25, p = 0.56, treatment 28 of 53 (52.8%) cases, 25 of 53 (47.2%) controls, case control OR. |
| Guldemir, 11/16/2022, retrospective, Turkey, peer-reviewed, 3 authors, study period 30 March, 2020 - 23 September, 2020, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of hospitalization, 5.2% lower, RR 0.95, p = 0.89 (Fisher's exact test), treatment 19 of 81 (23.5%), control 98 of 396 (24.7%), NNT 77. |
| Hernández (B), 10/27/2020, retrospective, Spain, peer-reviewed, mean age 60.9, 12 authors, dosage varies. | risk of death, 3.7% higher, RR 1.04, p = 1.00, treatment 2 of 19 (10.5%), control 20 of 197 (10.2%). |
| risk of mechanical ventilation, 75.9% lower, RR 0.24, p = 0.13, treatment 1 of 19 (5.3%), control 43 of 197 (21.8%), NNT 6.0. | |
| risk of ICU admission, 79.3% lower, RR 0.21, p = 0.05, treatment 1 of 19 (5.3%), control 50 of 197 (25.4%), NNT 5.0. | |
| hospitalization time, 33.3% lower, relative time 0.67, p = 0.11, treatment 19, control 197. | |
| Holt, 3/30/2021, prospective, United Kingdom, peer-reviewed, 34 authors, study period 1 May, 2020 - 5 February, 2021, dosage not specified, trial NCT04330599 (history) (COVIDENCE UK), excluded in exclusion analyses: significant unadjusted confounding possible. | risk of case, 6.8% lower, RR 0.93, p = 0.53, treatment 141 of 5,640 (2.5%), control 305 of 9,587 (3.2%), adjusted per study, odds ratio converted to relative risk, fully adjusted, group sizes approximated. |
| Hosseini (C), 7/19/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Canada, preprint, mean age 39.5, 9 authors, study period 8 February, 2021 - 4 May, 2021, dosage 100,000IU day 1, 10,000IU day 7, 10,000IU day 14, 10,000IU day 21, 10,000IU day 28, 100,000IU cholecalciferol at baseline, 10,000IU weekly for 16 weeks, trial NCT04483635 (history) (PROTECT). | risk of case, 81.9% lower, RR 0.18, p = 0.19, treatment 0 of 19 (0.0%), control 2 of 15 (13.3%), NNT 7.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Israel (B), 7/27/2021, retrospective, Israel, peer-reviewed, 10 authors, dosage not specified. | risk of hospitalization, 13.1% lower, OR 0.87, p = 0.003, treatment 737 of 6,953 (10.6%) cases, 1,669 of 13,906 (12.0%) controls, NNT 33, case control OR, PCR+, cohort 2. |
| Jabeen, 5/11/2022, prospective, Pakistan, peer-reviewed, 7 authors, dosage 200,000IU single dose. | risk of symptomatic case, 88.9% lower, RR 0.11, p = 0.11, treatment 0 of 20 (0.0%), control 4 of 20 (20.0%), NNT 5.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Jimenez, 7/26/2021, retrospective, Spain, peer-reviewed, 21 authors, study period 12 March, 2020 - 21 May, 2020, dosage paricalcitol 0.9μg weekly. | risk of death, 50.1% lower, HR 0.50, p = 0.02, treatment 16 of 94 (17.0%), control 65 of 191 (34.0%), NNT 5.9, adjusted per study, paricalcitol treatment, multivariate Cox regression. |
| risk of death, 50.7% lower, HR 0.49, p = 0.003, all vitamin D derivatives, univariate. | |
| Jolliffe, 3/23/2022, Randomized Controlled Trial, United Kingdom, peer-reviewed, median age 60.2, 25 authors, study period December 2020 - June 2021, dosage 3,200IU daily, daily, trial NCT04579640 (history) (CORONAVIT). | risk of mechanical ventilation, 94.7% higher, RR 1.95, p = 1.00, treatment 1 of 1,515 (0.1%), control 1 of 2,949 (0.0%), 3200IU/day. |
| risk of mechanical ventilation, 94.7% higher, RR 1.95, p = 1.00, treatment 1 of 1,515 (0.1%), control 1 of 2,949 (0.0%), 800IU/day. | |
| risk of hospitalization, 41.1% higher, RR 1.41, p = 0.16, treatment 29 of 1,515 (1.9%), control 40 of 2,949 (1.4%), 3200IU/day. | |
| risk of hospitalization, 16.8% higher, RR 1.17, p = 0.60, treatment 24 of 1,515 (1.6%), control 40 of 2,949 (1.4%), 800IU/day. | |
| risk of case, 8.8% higher, RR 1.09, p = 0.55, treatment 76 of 1,515 (5.0%), control 136 of 2,949 (4.6%), 3200IU/day. | |
| risk of case, 24.5% higher, RR 1.25, p = 0.11, treatment 87 of 1,515 (5.7%), control 136 of 2,949 (4.6%), 800IU/day. | |
| risk of case, 12.3% higher, RR 1.12, p = 0.56, treatment 45 of 1,515 (3.0%), control 78 of 2,949 (2.6%), confirmed, 3200IU/day. | |
| risk of case, 37.3% higher, RR 1.37, p = 0.08, treatment 55 of 1,515 (3.6%), control 78 of 2,949 (2.6%), confirmed, 800IU/day. | |
| Junior, 2/17/2022, prospective, Brazil, peer-reviewed, 6 authors, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 22.1% lower, RR 0.78, p = 0.61, treatment 8 of 113 (7.1%), control 8 of 88 (9.1%), NNT 50. |
| risk of progression, 30.8% lower, RR 0.69, p = 0.26, treatment 16 of 113 (14.2%), control 18 of 88 (20.5%), NNT 16, respiratory failure. | |
| Karonova, 1/24/2022, Randomized Controlled Trial, Russia, peer-reviewed, 8 authors, study period 30 October, 2020 - 28 February, 2021. | risk of symptomatic case, 94.6% lower, RR 0.05, p = 0.002, treatment 0 of 38 (0.0%), control 9 of 40 (22.5%), NNT 4.4, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of case, 41.5% lower, RR 0.58, p = 0.10, treatment 10 of 38 (26.3%), control 18 of 40 (45.0%), NNT 5.4. | |
| Levitus, 5/3/2021, retrospective, USA, peer-reviewed, 9 authors, dosage varies. | risk of severe case, 30.8% lower, RR 0.69, p = 0.25, treatment 65, control 64, odds ratio converted to relative risk, ≥1,000IU, control prevalence approximated with overall prevalence. |
| risk of severe case, 40.0% lower, RR 0.60, p = 0.15, treatment 65, control 64, odds ratio converted to relative risk, ≥5,000IU, control prevalence approximated with overall prevalence. | |
| risk of severe case, no change, RR 1.00, p = 0.92, treatment 65, control 64, odds ratio converted to relative risk, ≥50,000IU, control prevalence approximated with overall prevalence. | |
| Levy, 1/31/2022, retrospective, Israel, peer-reviewed, 10 authors, dosage not specified. | risk of death/hospitalization, 30.0% lower, HR 0.70, p = 0.05, treatment 39 of 208 (18.8%), control 168 of 641 (26.2%), NNT 13, adjusted per study, multivariable, Cox proportional hazards, day 40. |
| Louca, 11/30/2020, retrospective, population-based cohort, United Kingdom, peer-reviewed, mean age 49.6, 26 authors, dosage not specified. | risk of case, 7.5% lower, RR 0.92, p < 0.001, odds ratio converted to relative risk, United Kingdom, all adjustment model. |
| Loucera, 4/29/2021, retrospective, propensity score matching, Spain, peer-reviewed, 11 authors, dosage varies (calcifediol). | risk of death, 33.0% lower, HR 0.67, p = 0.009, treatment 374, control 374, calcifediol, <15 days before hospitalization, Cox model with inverse propensity weighting. |
| risk of death, 27.0% lower, HR 0.73, p = 0.02, treatment 439, control 439, calcifediol, <30 days before hospitalization, Cox model with inverse propensity weighting. | |
| risk of death, 25.0% lower, HR 0.75, p = 0.005, treatment 570, control 570, cholecalciferol, <15 days before hospitalization, Cox model with inverse propensity weighting. | |
| risk of death, 12.0% lower, HR 0.88, p = 0.11, treatment 802, control 802, cholecalciferol, <30 days before hospitalization, Cox model with inverse propensity weighting. | |
| Lázaro, 9/5/2021, retrospective, Spain, preprint, 9 authors, dosage not specified, excluded in exclusion analyses: very few events; unadjusted results with no group details; minimal details provided. | risk of case, 26.8% lower, RR 0.73, p = 1.00, treatment 1 of 97 (1.0%), control 2 of 142 (1.4%), NNT 265. |
| Ma, 12/3/2021, retrospective, USA, peer-reviewed, 16 authors, study period May 2020 - March 2021, dosage varies. | risk of hospitalization, 49.0% lower, OR 0.51, p = 0.04, treatment 26,605, control 12,710, adjusted per study, supplementation ≥400 IU/day, model 3, supplemental table 3, multivariable, RR approximated with OR. |
| risk of symptomatic case, 7.0% higher, OR 1.07, p = 0.25, treatment 7,895, control 31,420, adjusted per study, supplementation ≥2000 IU/day vs. <400 IU/day, model 3, supplemental table 3, multivariable, RR approximated with OR. | |
| risk of case, 17.0% lower, OR 0.83, p = 0.07, treatment 7,895, control 31,420, adjusted per study, supplementation ≥2000 IU/day vs. <400 IU/day, model 3, supplemental table 3, multivariable, RR approximated with OR. | |
| Ma (B), 1/29/2021, retrospective, United Kingdom, peer-reviewed, 4 authors, dosage not specified. | risk of case, 30.0% lower, RR 0.70, p = 0.03, treatment 49 of 363 (13.5%), control 1,329 of 7,934 (16.8%), adjusted per study, odds ratio converted to relative risk. |
| Mahmood, 12/29/2021, retrospective, United Kingdom, peer-reviewed, 4 authors, study period 23 March, 2020 - 31 December, 2020, dosage varies, excluded in exclusion analyses: unadjusted results with no group details; substantial unadjusted confounding by indication likely. | risk of death, 9.4% lower, RR 0.91, p = 0.67, treatment 34 of 138 (24.6%), control 31 of 114 (27.2%), NNT 39, prescribed by GP. |
| Meltzer, 12/10/2025, Double Blind Randomized Controlled Trial, USA, preprint, 1 author, dosage 4,000IU daily, trial NCT04868903 (history). | risk of case, 27.0% lower, HR 0.73, p = 0.09, treatment 461, control 462, adjusted per study, 4,000 IU and 10,000 IU vs. 400 IU, multivariable, Cox proportional hazards. |
| risk of case, 38.0% lower, HR 0.62, p = 0.04, treatment 299, control 300, adjusted per study, 4,000 IU vs. 400 IU, multivariable, Cox proportional hazards. | |
| risk of case, 1.0% lower, HR 0.99, p = 0.98, treatment 162, control 162, adjusted per study, 10,000 IU vs. 400 IU, multivariable, Cox proportional hazards. | |
| risk of case, 38.0% lower, OR 0.62, p = 0.26, treatment 299, control 462, adjusted per study, 4,000 IU vs. 400 IU, multivariable, RR approximated with OR. | |
| risk of case, 62.0% lower, OR 0.38, p = 0.07, treatment 299, control 300, adjusted per study, 4,000 IU vs. 400 IU, multivariable, RR approximated with OR. | |
| risk of case, 67.0% higher, OR 1.67, p = 0.48, treatment 162, control 162, adjusted per study, 10,000 IU vs. 400 IU, multivariable, RR approximated with OR. | |
| Meltzer (D), 3/19/2021, retrospective, database analysis, USA, peer-reviewed, 6 authors, dosage not specified. | risk of case, 36.0% lower, RR 0.64, p = 0.38, treatment 6 of 131 (4.6%), control 239 of 3,338 (7.2%), NNT 39, ≥2,000IU/d. |
| risk of case, 31.1% lower, RR 0.69, p = 0.16, treatment 15 of 304 (4.9%), control 239 of 3,338 (7.2%), NNT 45, ≥1,001IU/d. | |
| risk of case, 8.9% lower, RR 0.91, p = 0.56, treatment 60 of 920 (6.5%), control 239 of 3,338 (7.2%), NNT 157, ≥1IU/d. | |
| Mohseni, 8/4/2021, retrospective, Iran, peer-reviewed, 4 authors, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of case, 12.4% lower, RR 0.88, p = 0.09, treatment 99 of 192 (51.6%), control 242 of 411 (58.9%), NNT 14. |
| Nimer, 2/28/2022, retrospective, Jordan, peer-reviewed, survey, 4 authors, study period March 2021 - July 2021, dosage not specified. | risk of hospitalization, 33.3% lower, RR 0.67, p = 0.001, treatment 66 of 796 (8.3%), control 153 of 1,352 (11.3%), NNT 33, adjusted per study, odds ratio converted to relative risk, multivariable. |
| risk of severe case, 29.0% lower, RR 0.71, p = 0.01, treatment 81 of 796 (10.2%), control 179 of 1,352 (13.2%), NNT 33, adjusted per study, odds ratio converted to relative risk, multivariable. | |
| Oristrell, 7/17/2021, retrospective, population-based cohort, Spain, peer-reviewed, 8 authors, dosage varies (calcifediol). | risk of death, 1.0% higher, RR 1.01, p = 0.91, calcifediol, univariate. |
| risk of death, 4.0% lower, RR 0.96, p = 0.37, cholecalciferol, univariate. | |
| risk of case, 1.0% lower, RR 0.99, p = 0.65, NNT 3499, calcifediol, univariate. | |
| risk of case, 5.0% lower, RR 0.95, p = 0.004, cholecalciferol, multivariate. | |
| Oristrell (B), 4/6/2021, retrospective, Spain, peer-reviewed, 10 authors, dosage calcitriol 0.3μg daily, mean daily dose. | risk of death, 43.0% lower, HR 0.57, p = 0.001, treatment 2,296, control 3,407, multivariate, patients with CKD stages 4-5. |
| risk of severe case, 43.0% lower, HR 0.57, p < 0.001, treatment 2,296, control 3,407, multivariate, patients with CKD stages 4-5. | |
| risk of case, 22.0% lower, HR 0.78, p = 0.01, treatment 163 of 2,296 (7.1%), control 326 of 3,407 (9.6%), NNT 40, multivariate, patients with CKD stages 4-5. | |
| Parant, 4/14/2022, retrospective, France, peer-reviewed, median age 78.0, 12 authors, study period 1 March, 2020 - 30 June, 2020, dosage varies, trial NCT04877509 (history). | risk of death, 50.5% lower, RR 0.50, p = 0.11, treatment 7 of 66 (10.6%), control 28 of 162 (17.3%), adjusted per study, odds ratio converted to relative risk, multivariable. |
| risk of ICU admission, 51.2% lower, RR 0.49, p = 0.008, treatment 10 of 66 (15.2%), control 74 of 162 (45.7%), NNT 3.3, adjusted per study, odds ratio converted to relative risk, multivariable. | |
| risk of severe case, 38.7% lower, RR 0.61, p = 0.01, treatment 19 of 66 (28.8%), control 86 of 162 (53.1%), NNT 4.1, adjusted per study, odds ratio converted to relative risk, multivariable. | |
| Pecina, 8/27/2021, retrospective, USA, peer-reviewed, 4 authors, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 70.0% higher, OR 1.70, p = 0.52, treatment 29, control 63, supplementation, unadjusted, RR approximated with OR. |
| risk of mechanical ventilation, 10.0% higher, OR 1.10, p = 0.89, treatment 29, control 63, supplementation, unadjusted, RR approximated with OR. | |
| risk of ICU admission, 30.0% higher, OR 1.30, p = 0.61, treatment 29, control 63, supplementation, unadjusted, RR approximated with OR. | |
| Regalia, 1/13/2022, retrospective, Italy, peer-reviewed, 10 authors, dosage varies. | risk of case, 33.0% lower, OR 0.67, p = 0.21, treatment 32 of 60 (53.3%) cases, 75 of 119 (63.0%) controls, NNT 11, case control OR, vitamin D supplementation for ≥3 months in the last year. |
| Sainz-Amo, 10/24/2020, retrospective, Spain, peer-reviewed, mean age 74.5, 13 authors, dosage not specified. | risk of severe case, 32.7% lower, OR 0.67, p = 0.45, treatment 5 of 29 (17.2%) cases, 43 of 182 (23.6%) controls, NNT 23, case control OR. |
| risk of case, 43.7% lower, OR 0.56, p = 0.23, treatment 6 of 39 (15.4%) cases, 42 of 172 (24.4%) controls, NNT 13, case control OR. | |
| Sharif, 11/26/2022, retrospective, Bangladesh, peer-reviewed, 14 authors, study period 13 December, 2020 - 4 February, 2021, dosage 2,000IU daily. | risk of severe case, 28.0% lower, OR 0.72, p = 0.001, adjusted per study, multivariable, RR approximated with OR. |
| Shehab, 2/28/2022, retrospective, multiple countries, peer-reviewed, survey, 7 authors, study period September 2020 - March 2021, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of severe case, 45.7% lower, RR 0.54, p = 0.20, treatment 6 of 90 (6.7%), control 20 of 163 (12.3%), NNT 18, unadjusted, severe vs. mild cases. |
| Sinaci, 8/11/2021, retrospective, Turkey, peer-reviewed, 10 authors, dosage not specified. | risk of severe case, 90.0% lower, RR 0.10, p = 0.35, treatment 0 of 36 (0.0%), control 7 of 123 (5.7%), NNT 18, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), supplementation. |
| risk of moderate/severe case, 18.8% higher, RR 1.19, p = 0.64, treatment 8 of 36 (22.2%), control 23 of 123 (18.7%), supplementation. | |
| Subramanian, 1/31/2022, prospective, United Kingdom, peer-reviewed, 16 authors, dosage not specified. | risk of death, 27.3% lower, RR 0.73, p = 0.12, treatment 31 of 131 (23.7%), control 80 of 336 (23.8%), adjusted per study, odds ratio converted to relative risk, prescribed supplement use, multivariable. |
| Sulli, 2/24/2021, retrospective, Italy, peer-reviewed, 10 authors, dosage not specified. | risk of case, 75.6% lower, OR 0.24, p < 0.001, treatment 22 of 65 (33.8%) cases, 44 of 65 (67.7%) controls, NNT 3.0, case control OR, vitamin D supplementation. |
| Tylicki, 1/6/2022, retrospective, Poland, peer-reviewed, 10 authors, study period 6 October, 2020 - 28 February, 2021, dosage not specified. | risk of death, 14.4% lower, RR 0.86, p = 0.61, treatment 28 of 85 (32.9%), control 25 of 48 (52.1%), NNT 5.2, adjusted per study, odds ratio converted to relative risk, multivariable. |
| Ullah, 3/4/2021, retrospective, United Kingdom, peer-reviewed, 3 authors, dosage not specified, excluded in exclusion analyses: significant unadjusted confounding possible. | risk of death, 42.1% higher, RR 1.42, p = 0.34, treatment 21 of 64 (32.8%), control 26 of 135 (19.3%), adjusted per study, odds ratio converted to relative risk. |
| risk of case, 146.0% higher, RR 2.46, p < 0.001, treatment 69 of 2,168 (3.2%), control 139 of 12,681 (1.1%), adjusted per study, odds ratio converted to relative risk. | |
| van Helmond, 9/17/2022, prospective, USA, peer-reviewed, 14 authors, study period 27 October, 2020 - 31 January, 2021, dosage 5,000IU daily, trial NCT04596657 (history). | risk of case, 97.5% lower, RR 0.02, p = 0.07, treatment 0 of 255 (0.0%), control 36 of 2,827 (1.3%), NNT 79, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Vasheghani, 1/18/2021, retrospective, Iran, preprint, 6 authors, dosage not specified. | risk of death, 30.4% lower, RR 0.70, p = 0.45, treatment 7 of 88 (8.0%), control 48 of 420 (11.4%), NNT 29, vitamin D supplementation. |
| risk of ICU admission, 63.8% lower, RR 0.36, p = 0.009, treatment 13 of 185 (7.0%), control 53 of 323 (16.4%), NNT 11, adjusted per study, inverted to make RR<1 favor treatment, vitamin D levels >30ng/mL. | |
| Villasis-Keever, 4/18/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Mexico, peer-reviewed, 16 authors, study period 15 July, 2020 - 30 December, 2020, dosage 4,000IU daily. | risk of hospitalization, 66.5% lower, RR 0.33, p = 1.00, treatment 0 of 150 (0.0%), control 1 of 152 (0.7%), NNT 152, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), ITT. |
| risk of case, 78.0% lower, RR 0.22, p = 0.001, treatment 7 of 150 (4.7%), control 26 of 152 (17.1%), NNT 8.0, adjusted per study, multivariable, Table 3. | |
| Wang (C), 3/29/2023, Randomized Controlled Trial, China, peer-reviewed, median age 36.5, 23 authors, study period 18 December, 2022 - 20 February, 2023, dosage 200,000IU days 1, 14, trial NCT05673980 (history). | risk of progression, 25.2% lower, RR 0.75, p = 0.15, treatment 99, control 103, combined symptoms. |
| risk of progression, 4.0% higher, RR 1.04, p = 1.00, treatment 5 of 99 (5.1%), control 5 of 103 (4.9%), risk of severe case, fever. | |
| risk of progression, 7.5% lower, RR 0.92, p = 1.00, treatment 8 of 99 (8.1%), control 9 of 103 (8.7%), NNT 152, risk of severe case, sore throat. | |
| risk of progression, 42.2% lower, RR 0.58, p = 0.41, treatment 5 of 99 (5.1%), control 9 of 103 (8.7%), NNT 27, risk of severe case, rhinorrhea or congestion. | |
| risk of progression, 66.2% lower, RR 0.34, p = 1.00, treatment 0 of 99 (0.0%), control 1 of 103 (1.0%), NNT 103, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), risk of severe case, diarrhea. | |
| risk of progression, 66.2% lower, RR 0.34, p = 1.00, treatment 0 of 99 (0.0%), control 1 of 103 (1.0%), NNT 103, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), risk of severe case, vomiting. | |
| risk of progression, 13.3% lower, RR 0.87, p = 0.82, treatment 10 of 99 (10.1%), control 12 of 103 (11.7%), NNT 65, risk of severe case, cough. | |
| risk of progression, 48.0% lower, RR 0.52, p = 0.13, treatment 8 of 99 (8.1%), control 16 of 103 (15.5%), NNT 13, risk of severe case, muscle/joint aches. | |
| risk of progression, 56.1% higher, RR 1.56, p = 0.68, treatment 3 of 99 (3.0%), control 2 of 103 (1.9%), risk of severe case, taste/smell. | |
| risk of case, 3.7% lower, RR 0.96, p = 0.89, treatment 50 of 99 (50.5%), control 54 of 103 (52.4%), NNT 52. | |
| risk of case, 15.0% higher, RR 1.15, p = 0.47, treatment 42 of 99 (42.4%), control 38 of 103 (36.9%), first two weeks. | |
| risk of case, 48.0% lower, RR 0.52, p = 0.13, treatment 8 of 99 (8.1%), control 16 of 103 (15.5%), NNT 13, last two weeks. | |
| Ünsal (B), 4/5/2021, retrospective, Turkey, peer-reviewed, 10 authors, dosage varies. | risk of pneumonia, 71.4% lower, RR 0.29, p = 0.009, treatment 4 of 28 (14.3%), control 14 of 28 (50.0%), NNT 2.8, average 800-1000IU/day cholecalciferol. |
| Şengül, 12/31/2022, retrospective, Turkey, peer-reviewed, 4 authors, study period March 2020 - December 2021, dosage not specified. | risk of case, 68.5% lower, OR 0.31, p = 0.004, treatment 8 of 54 (14.8%) cases, 94 of 264 (35.6%) controls, NNT 7.4, case control OR. |
Viral infection and replication involves attachment, entry, uncoating and release, genome replication and transcription, translation and protein processing, assembly and budding, and release. Each step can be disrupted by therapeutics.
Monoclonal antibodies were
previously included. Other treatments such as dexamethasone, tocilizumab, and baricitinib
were recommended for late stage hospitalized patients.
Smoking was
known to cause lung cancer since at least 1939, but this was not widely recognized in the
US until 1964, 25 years later. Surgeon general Leroy Burney tried publicizing the danger
starting in 1957, with limited success. Surgeon general Luther Terry, appointed in 1961,
prompted by President Kennedy in 1962 amid pressure from health advocates, finally got
recognition in 1964. The 1964 report reviewed 7,000+ studies, but these could (and should)
have been reviewed and acted upon in real-time as they were published.
Historians attribute the 25 year delay to an industry campaign to manufacture doubt and
controversy, through tactics like funding biased and fraudulent research from
"independent" organizations, attacking scientists, and political lobbying.
The success of the industry campaign is only possible because officials did not analyze
the research in detail. Fraudulent industry research supported prior failures, but would
have been called out as fraudulent by officials that analyzed and understood the research
in real-time.
When administered late in infection, HCQ may enhance viral egress by further increasing
lysosomal pH beyond the effect of ORF3a's water channel activity, thereby promoting
lysosomal exocytosis, inactivating degradative enzymes, and facilitating the release of
SARS-CoV-2 particles into the extracellular environment637,638.
Research also suggests potential cardioprotective effects at lower doses, but
cardiotoxicity with excessive dosage639. Bobrowski et al. also
indicate negative effects if HCQ and remdesivir are combined.
Peters (B) et al. is subject to confounding by calendar-time (SOC evolved rapidly early in
the pandemic, the linear covariate does not reflect non-linear SOC changes and hospital
specific effects), hospital type (non-treatment hospitals were tertiary university
centers), confounding by indication (4/7 hospitals initiated treatment on deterioration),
immortal-time bias for as-treated (exposure assigned after baseline), significant
differences for other experimental treatments, potential overadjustment from collider bias
(steroid use and indication bias), limited baseline severity information, differences in
hospice referral propensity across hospitals, unadjusted difference in time from onset to
admission, difference in PCR positivity, and other factors.
Mahévas et al. is subject to confounding by hospital (treatment highly dependent on
the hospital, different SOC/ICU transfer practices, not included in PS), immortal time
(only partly addressed in sensitivity analysis), co-treatment differences, calendar-time
(SOC evolved rapidly early in the pandemic), binary coding for age (age ≥65 despite steep
age-risk gradient), residual imbalance (variables dropped from PS), a composite outcome
dependent on hospital triage/capacity, and other factors.
Crawford et al., Analysis of Select Dietary Supplement Products Marketed to Support or Boost the Immune System, JAMA Network Open, doi:10.1001/jamanetworkopen.2022.26040.
Crighton et al., Toxicological screening and DNA sequencing detects contamination and adulteration in regulated herbal medicines and supplements for diet, weight loss and cardiovascular health, Journal of Pharmaceutical and Biomedical Analysis, doi:10.1016/j.jpba.2019.112834.
Chanyandura et al., Evaluation of The Pharmaceutical Quality of the Most Commonly Purchased Vitamin C (Ascorbic Acid) Formulations in COVID-19 Infection in South Africa, J. Basic Appl. Pharm. Sci., doi:10.33790/jbaps1100105.
Shah et al., Does vitamin D supplementation reduce COVID-19 severity? - a systematic review, QJM: An International Journal of Medicine, doi:10.1093/qjmed/hcac040.
Nikniaz et al., The impact of vitamin D supplementation on mortality rate and clinical outcomes of COVID-19 patients: A systematic review and meta-analysis, Pharmaceutical Sciences, doi:10.34172/PS.2021.13.
Hosseini et al., Effects of Vitamin D Supplementation on COVID-19 Related Outcomes: A Systematic Review and Meta-Analysis, Nutrients, doi:10.3390/nu14102134.
D’Ecclesiis et al., Vitamin D and SARS-CoV2 infection, severity and mortality: A systematic review and meta-analysis, PLOS ONE, doi:10.1371/journal.pone.0268396.
Xie et al., Micronutrient perspective on COVID-19: Umbrella review and reanalysis of meta-analyses, Critical Reviews in Food Science and Nutrition, doi:10.1080/10408398.2023.2174948.
Hariyanto et al., Vitamin D supplementation and Covid‐19 outcomes: A systematic review, meta‐analysis and meta‐regression, Reviews in Medical Virology, doi:10.1002/rmv.2269.
Begum et al., The Role of Vitamin D in COVID-19 Survival and Prevention: A Meta-analysis, Sudan Journal of Medical Sciences, doi:10.18502/sjms.v19i1.15776.
Jamilian et al., The role of vitamin D in outcomes of critical care in COVID-19 patients: Evidence from an umbrella meta-analysis of interventional and observational studies, Public Health Nutrition, doi:10.1017/S1368980024000934.
Sobczak et al., Effect of Vitamin D3 Supplementation on Severe COVID-19: A Meta-Analysis of Randomized Clinical Trials, Nutrients, doi:10.3390/nu16101402.
Petrelli et al., Therapeutic and prognostic role of vitamin D for COVID-19 infection: A systematic review and meta-analysis of 43 observational studies, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2021.105883.
Asla et al., Vitamin D on COVID-19 Patients During the Pandemic, 2022. A Systematic Review and Meta-Analysis, Current Research in Nutrition and Food Science Journal, doi:10.12944/CRNFSJ.11.1.3.
Kow et al., The impact of vitamin D administration on mortality in COVID-19 patients: a systematic review and meta-analysis of randomized controlled trials, Inflammopharmacology, doi:10.1007/s10787-024-01564-2.
Zhang et al., The impact of supplementing vitamin D through different methods on the prognosis of COVID-19 patients: a systematic review and meta-analysis, Frontiers in Nutrition, doi:10.3389/fnut.2024.1441847.
Doustmohammadian et al., Impact of vitamin D supplementation on COVID-19 mortality: A systematic review and meta-analysis, Nutrition Clinique et Métabolisme, doi:10.1016/j.nupar.2025.12.001.
Yang et al., Vitamin D supplementation benefits COVID-19: A systematic review and meta-analysis, Heliyon, doi:10.1016/j.heliyon.2026.e44988.
Meng et al., The role of vitamin D in the prevention and treatment of SARS-CoV-2 infection: A meta-analysis of randomized controlled trials, Clinical Nutrition, doi:10.1016/j.clnu.2023.09.008.
Yang (B) et al., Therapeutic effects of vitamin D supplementation on COVID-19 aggravation: a systematic review and meta-analysis of randomized controlled trials, Frontiers in Pharmacology, doi:10.3389/fphar.2024.1367686.
Szarpak et al., Vitamin D supplementation to treat SARS-CoV-2 positive patients. Evidence from meta-analysis, Cardiology Journal, doi:10.5603/CJ.a2021.0122.
Tentolouris et al., The effect of vitamin D supplementation on mortality and intensive care unit admission of COVID-19 patients. A systematic review, meta-analysis and meta-regression, Diabetes/Metabolism Research and Reviews, doi:10.1002/dmrr.3517.
Sartini et al., Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis, Nutrients, doi:10.3390/nu16050679.
Zaazouee et al., Hospital and laboratory outcomes of patients with COVID-19 who received vitamin D supplementation: a systematic review and meta-analysis of randomized controlled trials, Naunyn-Schmiedeberg's Archives of Pharmacology, doi:10.1007/s00210-022-02360-x.
Varikasuvu et al., COVID-19 and Vitamin D (Co-VIVID Study): a systematic review and meta-analysis of randomized controlled trials, Expert Review of Anti-infective Therapy, doi:10.1080/14787210.2022.2035217.
Ryu et al., Fibrin drives thromboinflammation and neuropathology in COVID-19, Nature, doi:10.1038/s41586-024-07873-4.
Rong et al., Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19, Cell Host & Microbe, doi:10.1016/j.chom.2024.11.007.
Yang (C) et al., SARS-CoV-2 infection causes dopaminergic neuron senescence, Cell Stem Cell, doi:10.1016/j.stem.2023.12.012.
Scardua-Silva et al., Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19, Scientific Reports, doi:10.1038/s41598-024-52005-7.
Hampshire et al., Cognition and Memory after Covid-19 in a Large Community Sample, New England Journal of Medicine, doi:10.1056/NEJMoa2311330.
Duloquin et al., Is COVID-19 Infection a Multiorganic Disease? Focus on Extrapulmonary Involvement of SARS-CoV-2, Journal of Clinical Medicine, doi:10.3390/jcm13051397.
Sodagar et al., Pathological Features and Neuroinflammatory Mechanisms of SARS-CoV-2 in the Brain and Potential Therapeutic Approaches, Biomolecules, doi:10.3390/biom12070971.
Sagar et al., COVID-19-associated cerebral microbleeds in the general population, Brain Communications, doi:10.1093/braincomms/fcae127.
Verma et al., Persistent Neurological Deficits in Mouse PASC Reveal Antiviral Drug Limitations, bioRxiv, doi:10.1101/2024.06.02.596989.
Panagea et al., Neurocognitive Impairment in Long COVID: A Systematic Review, Archives of Clinical Neuropsychology, doi:10.1093/arclin/acae042.
Ariza et al., COVID-19: Unveiling the Neuropsychiatric Maze—From Acute to Long-Term Manifestations, Biomedicines, doi:10.3390/biomedicines12061147.
Vashisht et al., Neurological Complications of COVID-19: Unraveling the Pathophysiological Underpinnings and Therapeutic Implications, Viruses, doi:10.3390/v16081183.
Ahmad et al., Neurological Complications and Outcomes in Critically Ill Patients With COVID-19: Results From International Neurological Study Group From the COVID-19 Critical Care Consortium, The Neurohospitalist, doi:10.1177/19418744241292487.
Wang et al., SARS-CoV-2 membrane protein induces neurodegeneration via affecting Golgi-mitochondria interaction, Translational Neurodegeneration, doi:10.1186/s40035-024-00458-1.
Freitas et al., Central nervous system and systemic inflammatory networks associated with acute neurological outcomes in COVID-19, Scientific Reports, doi:10.1038/s41598-025-08632-9.
Lu et al., Risk of neuropsychiatric and related conditions associated with SARS-CoV-2 infection: a difference-in-differences analysis, Nature Communications, doi:10.1038/s41467-025-61961-1.
Jachman-Kapułka et al., Cross-Section of Neurological Manifestations Among SARS-CoV-2 Omicron Subvariants—Single-Center Study, Brain Sciences, doi:10.3390/brainsci14111161.
Beckman et al., SARS-CoV-2 infects neurons and induces neuroinflammation in a non-human primate model of COVID-19, Cell Reports, doi:10.1016/j.celrep.2022.111573.
Eberhardt et al., SARS-CoV-2 infection triggers pro-atherogenic inflammatory responses in human coronary vessels, Nature Cardiovascular Research, doi:10.1038/s44161-023-00336-5.
Van Tin et al., Spike Protein of SARS-CoV-2 Activates Cardiac Fibrogenesis through NLRP3 Inflammasomes and NF-κB Signaling, Cells, doi:10.3390/cells13161331.
Borka Balas et al., COVID-19 and Cardiac Implications—Still a Mystery in Clinical Practice, Reviews in Cardiovascular Medicine, doi:10.31083/j.rcm2405125.
AlTaweel et al., An In-Depth Insight into Clinical, Cellular and Molecular Factors in COVID19-Associated Cardiovascular Ailments for Identifying Novel Disease Biomarkers, Drug Targets and Clinical Management Strategies, Archives of Microbiology & Immunology, doi:10.26502/ami.936500177.
Saha et al., COVID-19 beyond the lungs: Unraveling its vascular impact and cardiovascular complications—mechanisms and therapeutic implications, Science Progress, doi:10.1177/00368504251322069.
Yin et al., COVID-19: a vascular nightmare unfolding, Frontiers in Immunology, doi:10.3389/fimmu.2025.1593885.
Bruno et al., Accelerated vascular ageing after COVID-19 infection: the CARTESIAN study, European Heart Journal, doi:10.1093/eurheartj/ehaf430.
Abiri et al., The silent legacy of COVID-19: exploring genomic instability in long-term COVID-19 survivors, BMC Infectious Diseases, doi:10.1186/s12879-025-11419-y.
Gioia et al., SARS-CoV-2 infection induces DNA damage, through CHK1 degradation and impaired 53BP1 recruitment, and cellular senescence, Nature Cell Biology, doi:10.1038/s41556-023-01096-x.
Doğan et al., Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients, Current Issues in Molecular Biology, doi:10.3390/cimb45020062.
Rueda-Torres et al., Longitudinal Assessment of DNA Damage in PBMCs From Hospitalized COVID‐19 Patients via Alkaline Comet Assay, Environmental and Molecular Mutagenesis, doi:10.1002/em.70055.
Trender et al., Changes in memory and cognition during the SARS-CoV-2 human challenge study, eClinicalMedicine, doi:10.1016/j.eclinm.2024.102842.
Dugied et al., Multimodal SARS-CoV-2 interactome sketches the virus-host spatial organization, Communications Biology, doi:10.1038/s42003-025-07933-z.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Katiyar et al., SARS-CoV-2 Assembly: Gaining Infectivity and Beyond, Viruses, doi:10.3390/v16111648.
Wu et al., Decoding the genome of SARS-CoV-2: a pathway to drug development through translation inhibition, RNA Biology, doi:10.1080/15476286.2024.2433830.
Galmés et al., Suboptimal Consumption of Relevant Immune System Micronutrients Is Associated with a Worse Impact of COVID-19 in Spanish Populations, Nutrients, doi:10.3390/nu14112254.
Galmés (B) et al., Current State of Evidence: Influence of Nutritional and Nutrigenetic Factors on Immunity in the COVID-19 Pandemic Framework, Nutrients, doi:10.3390/nu12092738.
EFSA, Scientific Opinion on the substantiation of a health claim related to vitamin D and contribution to the normal function of the immune system pursuant to Article 14 of Regulation (EC) No 1924/2006, EFSA Journal, doi:10.2903/j.efsa.2015.4096.
EFSA (B), Scientific Opinion on the substantiation of health claims related to vitamin D and normal function of the immune system and inflammatory response (ID 154, 159), maintenance of normal muscle function (ID 155) and maintenance of normal cardiovascular function (ID 159) pursuant to Article 13(1) of Regulation (E, EFSA Journal, doi:10.2903/j.efsa.2010.1468.
Pickard et al., Discovery of re-purposed drugs that slow SARS-CoV-2 replication in human cells, PLOS Pathogens, doi:10.1371/journal.ppat.1009840.
Campolina-Silva et al., Dietary Vitamin D Mitigates Coronavirus-Induced Lung Inflammation and Damage in Mice, Viruses, doi:10.3390/v15122434.
Sposito et al., Age differential CD13 and interferon expression in airway epithelia affect SARS-CoV-2 infection - effects of vitamin D, Mucosal Immunology, doi:10.1016/j.mucimm.2023.08.002.
Alcalá-Santiago et al., Disentangling the Immunomodulatory Effects of Vitamin D on the SARS-CoV-2 Virus by In Vitro Approaches, The 14th European Nutrition Conference FENS 2023, doi:10.3390/proceedings2023091415.
Chen et al., Vitamin D3 attenuates SARS‐CoV‐2 nucleocapsid protein‐caused hyperinflammation by inactivating the NLRP3 inflammasome through the VDR‐BRCC3 signaling pathway in vitro and in vivo, MedComm, doi:10.1002/mco2.318.
Gotelli et al., Understanding the immune-endocrine effects of vitamin D in SARS-CoV-2 infection: a role in protecting against neurodamage?, Neuroimmunomodulation, doi:10.1159/000533286.
Knez et al., TLR10 overexpression modulates immune response in A549 lung epithelial cells challenged with SARS-CoV-2 S and N proteins, Frontiers in Immunology, doi:10.3389/fimmu.2024.1490478.
Vargas-Castro et al., Calcitriol prevents SARS-CoV spike-induced inflammation in human trophoblasts through downregulating ACE2 and TMPRSS2 expression, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2024.106625.
Alzahrani, A., A new investigation into the molecular mechanism of cholecalciferol towards reducing cytokines storm, Octahedron Drug Research, doi:10.21608/odr.2024.308273.1043.
Roth et al., Vitamin D-inducible antimicrobial peptide LL-37 binds SARS-CoV-2 Spike and accessory proteins ORF7a and ORF8, Frontiers in Cellular and Infection Microbiology, doi:10.3389/fcimb.2025.1671738.
Vercellino et al., Influence of Sex and 1,25α Dihydroxyvitamin D3 on SARS-CoV-2 Infection and Viral Entry, Pathogens, doi:10.3390/pathogens14080765.
Wang (B) et al., 1,25‐Dihydroxyvitamin D3 attenuates platelet aggregation potentiated by SARS‐CoV‐2 spike protein via inhibiting integrin αIIbβ3 outside‐in signaling, Cell Biochemistry and Function, doi:10.1002/cbf.4039.
García-Marín et al., Exploring SARS-CoV-2 Spike RBD Pockets as Targets for Generic Drugs: A Combined Computational, Biophysical, and Biological Approach, ACS Omega, doi:10.1021/acsomega.5c05175.
Fadel et al., Targeting asparagine and cysteine in SARS-CoV-2 variants and human pro-inflammatory mediators to alleviate COVID-19 severity; a cross-section and in-silico study, Scientific Reports, doi:10.1038/s41598-025-19359-y.
Saheb Sharif-Askari et al., Increased blood immune regulatory cells in severe COVID-19 with autoantibodies to type I interferons, Scientific Reports, doi:10.1038/s41598-023-43675-w.
Chen (B) et al., In Vitro Characterization of Inhibition Function of Calcifediol to the Protease Activity of SARS-COV-2 PLpro, Journal of Medical Virology, doi:10.1002/jmv.70085.
Graydon et al., High baseline frequencies of natural killer cells are associated with asymptomatic SARS-CoV-2 infection, Current Research in Immunology, doi:10.1016/j.crimmu.2023.100064.
Oh et al., Vitamin D and Exercise Are Major Determinants of Natural Killer Cell Activity, Which Is Age- and Gender-Specific, Frontiers in Immunology, doi:10.3389/fimmu.2021.594356.
Grant, W., Vitamin D and viral infections: Infectious diseases, autoimmune diseases, and cancers, Advances in Food and Nutrition Research, doi:10.1016/bs.afnr.2023.12.007.
Abioye et al., Effect of micronutrient supplements on influenza and other respiratory tract infections among adults: a systematic review and meta-analysis, BMJ Global Health, doi:10.1136/bmjgh-2020-003176.
Martineau et al., Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data, BMJ 2017, 356, doi:10.1136/bmj.i6583.
Ginde et al., High‐Dose Monthly Vitamin D for Prevention of Acute Respiratory Infection in Older Long‐Term Care Residents: A Randomized Clinical Trial, Journal of the American Geriatrics Society, doi:10.1111/jgs.14679.
Carlberg et al., In vivo response of the human epigenome to vitamin D: A Proof-of-principle study, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2018.01.002.
Quraishi et al., Association Between Preoperative 25-Hydroxyvitamin D Level and Hospital-Acquired Infections Following Roux-en-Y Gastric Bypass Surgery, JAMA Surgery, doi:10.1001/jamasurg.2013.3176.
Silva et al., Does serum 25-hydroxyvitamin D decrease during acute-phase response? A systematic review, Nutrition Research, doi:10.1016/j.nutres.2014.12.008.
Gupta et al., Temporal Association of Reduced Serum Vitamin D with COVID-19 Infection: Two Single-Institution Case–Control Studies, Nutrients, doi:10.3390/nu14132757.
Butler-Laporte et al., Vitamin D and COVID-19 susceptibility and severity in the COVID-19 Host Genetics Initiative: A Mendelian randomization study, PLOS Medicine, doi:10.1371/journal.pmed.1003605.
Raisi-Estabragh et al., Greater risk of severe COVID-19 in Black, Asian and Minority Ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: study of 1326 cases from the UK Biobank, J. Public Health, doi:10.1093/pubmed/fdaa095.
Khajebishak et al., Nutritional and inflammatory biomarkers for COVID-19 susceptibility: a focus on vitamin D, potassium, and hematological indices, BMC Infectious Diseases, doi:10.1186/s12879-025-12297-0.
Seifi Skishahr et al., Evaluation of Glutathione Redox Status and Inflammatory Markers in ICU Patients with Acute Respiratory Syndrome due to COVID-19, Jentashapir Journal of Cellular and Molecular Biology, doi:10.5812/jjcmb-159606.
Korkmaz et al., A New Biomarker Copeptin in Determining Disease Severity in COVID-19, Infectious Diseases and Clinical Microbiology, doi:10.36519/idcm.2024.324.
Secerlı et al., Effects of Immunotoxicity biomarkers, essential elements and vitamin D levels on the severity levels of COVID-19 disease in Turkey, Toxicology Research, doi:10.1093/toxres/tfae177.
AlKhuzaie et al., Electrolytes, Zinc and Vitamin D3 in COVID-19 Patients with Cardiovascular Complications, Problems of Virology, doi:10.36233/0507-4088-236.
Noraldinvand et al., Determination of Serum Vitamin D Levels in Patients with COVID-19, Journal of Medical Bacteriology, doi:10.18502/jmb.v12i2.15620.
Dong et al., Vitamin D level in COVID-19 patients has positive correlations with autophagy and negative correlations with disease severity, Frontiers in Pharmacology, doi:10.3389/fphar.2024.1388348.
Abdulameer et al., The vitamin D binding protein gene polymorphism association with Covid-19-infected Iraqi patients, Cellular and Molecular Biology, doi:10.14715/cmb/2023.69.5.5.
Aci et al., Effect of vitamin D receptor gene BsmI polymorphism on hospitalization of SARS-CoV-2 positive patients, Nucleosides, Nucleotides & Nucleic Acids, doi:10.1080/15257770.2023.2253281.
Jain et al., Demographical Profile and Clinical Outcomes of Covid-19 Patients at a Tertiary Care Centre, Journal of Cardiovascular Disease Research, doi:10.31838/jcdr.2023.14.05.215.
Saeed et al., Vitamin D Deficiency and Clinical Outcomes in Patients with COVID-19, University of Thi-Qar Journal of Medicine, 25:1, www.jmed.utq.edu.iq/index.php/main/article/view/380.
Pop-Kostova et al., Vitamin D status in patients with COVID-19 – sex differences associated with severity of the disease, Medical Journal MEDICUS, 28:1, eprints.ugd.edu.mk/31736/.
Beheshti et al., Correlation of vitamin D levels with serum parameters in Covid-19 patients, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2023.04.012.
di Filippo et al., Low vitamin D levels are associated with Long COVID syndrome in COVID-19 survivors, The Journal of Clinical Endocrinology & Metabolism, doi:10.1210/clinem/dgad207.
Rathod et al., Association of vitamin D with the severity of disease and mortality in COVID-19: Prospective study in central India, Annals of African Medicine, doi:10.4103/aam.aam_21_22.
Qu et al., Decreased serum vitamin D level as a prognostic marker in patients with COVID-19, arXiv, doi:10.48550/arXiv.2301.02660.
Morad et al., Serum vitamin D level in COVID-19 patients and its correlation with disease severity, Egyptian Rheumatology and Rehabilitation, doi:10.1186/s43166-022-00155-9.
Ahmeid et al., Evaluating the level of vitamin D in Iraqi COVID-19 patients besides the study of its association with biochemical parameters, Eurasian Chemical Communications, doi:10.22034/ecc.2023.158071.
Mansour et al., Association of serum zinc level and clinical outcome in Egyptian COVID-19 patients, The Egyptian Journal of Internal Medicine, doi:10.1186/s43162-022-00159-z.
Sinnberg et al., Vitamin C Deficiency in Blood Samples of COVID-19 Patients, Antioxidants, doi:10.3390/antiox11081580.
Shannak et al., Evaluation of the level of vitamin D3 in the blood serum of patients infected with COVID-19 in Al-Amiriya city, Technium BioChemMed, doi:10.47577/biochemmed.v3i2.7179.
Alarslan et al., Vitamin D levels and disease severity in COVID-19, Medical Journal of İzmir Hospital, 26:3, bozyakaeah.saglik.gov.tr/Eklenti/306811/0/tip-2022---3--91-98pdf.pdf.
Borzouei et al., Assessment of Vitamin D, Vitamin B12, Retinol-binding Protein (RBP), Zinc, Selenium, Copper and Magnesium in Iranian COVID-19 Patients and Their Relationships with the Disease Linked Death, Nutrition and Food Sciences Research, 9:2, nfsr.sbmu.ac.ir/article-1-559-fa.html.
Nicolescu et al., The evaluation of vitamin D deficiency as a risk factor in the case of patients with moderate COVID-19, Farmacia, doi:10.31925/farmacia.2022.3.17.
Takase et al., Association between 25-hydroxyvitamin D levels and COVID-19 severity, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2022.04.003.
Latifi-Pupovci et al., Relationship of anti-SARS-CoV-2 IgG antibodies with Vitamin D and inflammatory markers in COVID-19 patients, Scientific Reports, doi:10.1038/s41598-022-09785-7.
Saeed (B) et al., Cholecalciferol level and its impact on COVID-19 patients, The Egyptian Journal of Internal Medicine, doi:10.1186/s43162-022-00116-w.
Schmitt et al., Oxidative stress status and vitamin D levels of asymptomatic to mild symptomatic COVID-19 infections during the third trimester of pregnancy: A retrospective study in Metz, France, Journal of Medical Virology, doi:10.1002/jmv.27606.
Soltani-Zangbar et al., Serum levels of vitamin D and immune system function in patients with COVID-19 admitted to intensive care unit, Gene Reports, doi:10.1016/j.genrep.2022.101509.
Jabbar et al., Vitamin D Serum Levels and Its Association With COVID 19 Infection In Babylon Governorate, Iraq, Natural Volatiles & Essential Oils, 8:4, www.nveo.org/index.php/journal/article/view/1046.
Ranjbar et al., Serum level of Vitamin D is associated with COVID-19 mortality rate in hospitalized patients, Journal of Research in Medical Sciences, doi:10.4103/jrms.JRMS_1151_20.
Hosseini (B) et al., Comparing Serum Levels of Vitamin D and Zinc in Novel Coronavirus–Infected Patients and Healthy Individuals in Northeastern Iran, 2020, Infectious Diseases in Clinical Practice, doi:10.1097/IPC.0000000000001051.
Desai et al., Vitamin K & D Deficiencies Are Independently Associated With COVID-19 Disease Severity, Open Forum Infectious Diseases, doi:10.1093/ofid/ofab408.
Kumar et al., Association of vitamin D status with severity of COVID-19, Journal of Cardiovascular Disease Research, 12:6, jcdronline.org/admin/Uploads/Files/6249729ba2acf0.47779591.pdf.
Azadeh et al., Serum Vitamin D Concentrations in CoVID19 Patients, J. Mazandaran Univ. Med. Sci. 31:195, jmums.mazums.ac.ir/article-1-16104-en.html.
Al-Daghri et al., Vitamin D status of Arab Gulf residents screened for SARS-CoV-2 and its association with COVID-19 infection: a multi-centre case–control study, Journal of Translational Medicine, doi:10.1186/s12967-021-02838-x.
Ersöz et al., The association between micronutrient and hemogram values and prognostic factors in COVID-19 patients: A single-center experience from Turkey, International Journal of Clinical Practice, doi:10.1111/ijcp.14078.
Söbü et al., Vitamin D Levels of COVID-19 Positive Sypmtomatic Pediatric Cases, The Journal of Current Pediatrics, doi:10.4274/jcp.2021.0002.
Vassiliou et al., Vitamin D deficiency correlates with a reduced number of natural killer cells in intensive care unit (ICU) and non-ICU patients with COVID-19 pneumonia, Hellenic Journal of Cardiology, doi:10.1016/j.hjc.2020.11.011.
Kerget et al., Evaluation of the relationship of serum vitamin D levels in COVID-19 patients with clinical course and prognosis, Tuberk Toraks, doi:10.5578/tt.70027.
Mardani et al., Association of vitamin D with the modulation of the disease severity in COVID-19, Virus Research, doi:10.1016/j.virusres.2020.198148.
Chodick et al., Angiotensin-converting enzyme inhibitors and angiotensin-receptor blockers are not associated with increased risk of SARS-CoV-2 infection, Journal of Travel Medicine, doi:10.1093/jtm/taaa069.
D'Avolio et al., 25-hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2, Nutrients, 12:5, 1–7, doi:10.3390/nu12051359.
Sooriyaarachchi et al., Impact of vitamin D deficiency on COVID-19, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2021.05.011.
Papadimitriou et al., Association between population vitamin D status and SARS-CoV-2 related serious-critical illness and deaths: An ecological integrative approach, World J. Virology, doi:10.5501/wjv.v10.i3.111].
Jayawardena et al., Impact of the vitamin D deficiency on COVID-19 infection and mortality in Asian countries, Diabetes & Metabolic Syndrome: Clinical Research & Reviews, doi:10.1016/j.dsx.2021.03.006.
Yadav et al., Association of Vitamin D Status with COVID-19 Infection and Mortality in the Asia Pacific region: A Cross-Sectional Study, Indian Journal of Clinical Biochemistry, doi:10.1007/s12291-020-00950-1.
Bakaloudi et al., A critical update on the role of mild and serious vitamin D deficiency prevalence and the COVID-19 epidemic in Europe, Nutrition, doi:10.1016/j.nut.2021.111441.
Walrand, S., Autumn COVID-19 surge dates in Europe correlated to latitudes, not to temperature-humidity, pointing to vitamin D as contributing factor, Nature, doi:10.1038/s41598-021-81419-w.
Rhodes et al., COVID-19 mortality increases with northerly latitude after adjustment for age suggesting a link with ultraviolet and vitamin D, BMJ Nutr. Prev. Health, doi:10.1136/bmjnph-2020-000110.
Marik et al., Does vitamin D status impact mortality from SARS-CoV-2 infection?, Med Drug Discov., doi:10.1016/j.medidd.2020.100041.
Chiodini et al., Vitamin D Status and SARS-CoV-2 Infection and COVID-19 Clinical Outcomes, Frontiers in Public Health, doi:10.3389/fpubh.2021.736665.
Mishra et al., Vitamin D Deficiency and Comorbidities as Risk Factors of COVID-19 Infection: A Systematic Review and Meta-analysis, Journal of Preventive Medicine and Public Health, doi:10.3961/jpmph.21.640.
web.archive.org, web.archive.org/web/20211117052139/https://astralcodexten.substack.com/p/ivermectin-much-more-than-you-wanted.
Hayward et al., Ivermectin for COVID-19 in adults in the community (PRINCIPLE): an open, randomised, controlled, adaptive platform trial of short- and longer-term outcomes, Journal of Infection, doi:10.1016/j.jinf.2024.106130.
Haque et al., Exploring potential therapeutic candidates against COVID-19: a molecular docking study, Discover Molecules, doi:10.1007/s44345-024-00005-5.
Morales-Bayuelo et al., New findings on ligand series used as SARS-CoV-2 virus inhibitors within the frameworks of molecular docking, molecular quantum similarity and chemical reactivity indices, F1000Research, doi:10.12688/f1000research.123550.3.
Chellasamy et al., Docking and molecular dynamics studies of human ezrin protein with a modelled SARS-CoV-2 endodomain and their interaction with potential invasion inhibitors, Journal of King Saud University - Science, doi:10.1016/j.jksus.2022.102277.
Pandya et al., Unravelling Vitamin B12 as a potential inhibitor against SARS-CoV-2: A computational approach, Informatics in Medicine Unlocked, doi:10.1016/j.imu.2022.100951.
Mansouri et al., The impact of calcitriol and estradiol on the SARS-CoV-2 biological activity: a molecular modeling approach, Scientific Reports, doi:10.1038/s41598-022-04778-y.
Song et al., Vitamin D3 and its hydroxyderivatives as promising drugs against COVID-19: a computational study, Journal of Biomolecular Structure and Dynamics, doi:10.1080/07391102.2021.1964601.
Qayyum et al., Vitamin D and lumisterol novel metabolites can inhibit SARS-CoV-2 replication machinery enzymes, Endocrinology and Metabolism, doi:10.1152/ajpendo.00174.2021.
Al-Mazaideh et al., Vitamin D is a New Promising Inhibitor to the Main Protease (Mpro) of COVID-19 by Molecular Docking, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2021/v33i29B31603.
Moatasim et al., Potent Antiviral Activity of Vitamin B12 against Severe Acute Respiratory Syndrome Coronavirus 2, Middle East Respiratory Syndrome Coronavirus, and Human Coronavirus 229E, Microorganisms, doi:10.3390/microorganisms11112777.
Rybakovsky et al., Calcitriol modifies tight junctions, improves barrier function, and reduces TNF‐α‐induced barrier leak in the human lung‐derived epithelial cell culture model, 16HBE 14o‐, Physiological Reports, doi:10.14814/phy2.15592.
DiGuilio et al., The multiphasic TNF-α-induced compromise of Calu-3 airway epithelial barrier function, Experimental Lung Research, doi:10.1080/01902148.2023.2193637.
Mok et al., Calcitriol, the active form of vitamin D, is a promising candidate for COVID-19 prophylaxis, bioRxiv, doi:10.1101/2020.06.21.162396.
Fernandes de Souza et al., Lung Inflammation Induced by Inactivated SARS-CoV-2 in C57BL/6 Female Mice Is Controlled by Intranasal Instillation of Vitamin D, Cells, doi:10.3390/cells12071092.
Zeraatkar et al., Consistency of covid-19 trial preprints with published reports and impact for decision making: retrospective review, BMJ Medicine, doi:10.1136/bmjmed-2022-0003091.
Davidson et al., No evidence of important difference in summary treatment effects between COVID-19 preprints and peer-reviewed publications: a meta-epidemiological study, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2023.08.011.
Jadad et al., Randomized Controlled Trials: Questions, Answers, and Musings, Second Edition, doi:10.1002/9780470691922.
Gøtzsche, P., Bias in double-blind trials, Doctoral Thesis, University of Copenhagen, www.scientificfreedom.dk/2023/05/16/bias-in-double-blind-trials-doctoral-thesis/.
Als-Nielsen et al., Association of Funding and Conclusions in Randomized Drug Trials, JAMA, doi:10.1001/jama.290.7.921.
Bekelman et al., Scope and Impact of Financial Conflicts of Interest in Biomedical Research, JAMA, doi:10.1001/jama.289.4.454.
Lundh et al., Industry sponsorship and research outcome, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.MR000033.pub3.
Concato et al., Randomized, Controlled Trials, Observational Studies, and the Hierarchy of Research Designs, New England Journal of Medicine, doi:10.1056/NEJM200006223422507.
Anglemyer et al., Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.MR000034.pub2.
Lee et al., Analysis of Overall Level of Evidence Behind Infectious Diseases Society of America Practice Guidelines, Arch Intern Med., 2011, 171:1, 18-22, doi:10.1001/archinternmed.2010.482.
Deaton et al., Understanding and misunderstanding randomized controlled trials, Social Science & Medicine, 210, doi:10.1016/j.socscimed.2017.12.005.
Nichol et al., Challenging issues in randomised controlled trials, Injury, 2010, doi: 10.1016/j.injury.2010.03.033, www.injuryjournal.com/article/S0020-1383(10)00233-0/fulltext.
Villasis-Keever et al., Efficacy and Safety of Vitamin D Supplementation to Prevent COVID-19 in Frontline Healthcare Workers. A Randomized Clinical Trial, Archives of Medical Research, doi:10.1016/j.arcmed.2022.04.003.
Murai et al., Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients With Moderate to Severe COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2020.26848.
Mariani et al., High-dose vitamin D versus placebo to prevent complications in COVID-19 patients: Multicentre randomized controlled clinical trial, PLOS ONE, doi:10.1371/journal.pone.0267918.
Elamir et al., A Randomized Pilot Study Using Calcitriol in Hospitalized Patients, Bone, doi:10.1016/j.bone.2021.116175.
Abdelhai et al., Impact of Rapid Correction of Vitamin D Deficiency on Patients with COVID-19 Disease: A Randomized-Controlled Trial, The Egyptian Journal of Hospital Medicine, doi:10.21608/EJHM.2024.368093.
Annweiler et al., High-dose versus standard-dose vitamin D supplementation in older adults with COVID-19 (COVIT-TRIAL): A multicenter, open-label, randomized controlled superiority trial, PLoS Medicine, doi:10.1371/journal.pmed.1003999.
Beigmohammadi et al., The effect of supplementation with vitamins A, B, C, D, and E on disease severity and inflammatory responses in patients with COVID-19: a randomized clinical trial, Trials, doi:10.1186/s13063-021-05795-4.
Bishop et al., REsCue Trial: Randomized Controlled Clinical Trial with Extended-Release Calcifediol in Symptomatic COVID-19 Outpatients, Nutrition, doi:10.1016/j.nut.2022.111899.
Brunvoll et al., Prevention of covid-19 and other acute respiratory infections with cod liver oil supplementation, a low dose vitamin D supplement: quadruple blinded, randomised placebo controlled trial, BMJ, doi:10.1136/bmj-2022-071245.
Bychinin et al., Effect of vitamin D3 supplementation on cellular immunity and inflammatory markers in COVID-19 patients admitted to the ICU, Scientific Reports, doi:10.1038/s41598-022-22045-y.
Cannata-Andía et al., A single-oral bolus of 100,000 IU of cholecalciferol at hospital admission did not improve outcomes in the COVID-19 disease: the COVID-VIT-D — a randomised multicentre international clinical trial, BMC Medicine, doi:10.1186/s12916-022-02290-8.
Cervero et al., Beneficial Effect of Short-Term Supplementation of High Dose of Vitamin D3 in Hospitalized Patients With COVID-19: A Multicenter, Single-Blinded, Prospective Randomized Pilot Clinical Trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.863587.
De Niet et al., Positive Effects of Vitamin D Supplementation in Patients Hospitalized for COVID-19: A Randomized, Double-Blind, Placebo-Controlled Trial, Nutrients, doi:10.3390/nu14153048.
Din Ujjan et al., The possible therapeutic role of curcumin and quercetin in the early-stage of COVID-19—Results from a pragmatic randomized clinical trial, Frontiers in Nutrition, doi:10.3389/fnut.2022.1023997.
Domazet Bugarin et al., Vitamin D Supplementation and Clinical Outcomes in Severe COVID-19 Patients—Randomized Controlled Trial, Nutrients, doi:10.3390/nu15051234.
Entrenas Castillo et al., Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study, Journal of Steroid Biochemistry and Molecular Biology, 203, October 2020, doi:10.1016/j.jsbmb.2020.105751.
Ganmaa et al., A Randomized Trial of Vitamin D Supplementation and COVID-19 Clinical Outcomes and Long COVID: The Vitamin D for COVID-19 Trial, The Journal of Nutrition, doi:10.1016/j.tjnut.2026.101398.
Hosseini (C) et al., PRevention of COVID-19 with Oral Vitamin D supplemental Therapy in Essential healthCare Teams (PROTECT): Ancillary study of a randomised controlled trial, Research Square, doi:10.21203/rs.3.rs-1588325/v1.
Jaun et al., Effect of Single High Dose Vitamin D Substitution in Hospitalized COVID-19 Patients with Vitamin D Deficiency on Length of Hospital Stay, Biomedicines, doi:10.3390/biomedicines11051277.
Jolliffe et al., Effect of a test-and-treat approach to vitamin D supplementation on risk of all cause acute respiratory tract infection and covid-19: phase 3 randomised controlled trial (CORONAVIT), BMJ, doi:10.1136/bmj-2022-071230.
Karonova et al., Vitamin D Intake May Reduce SARS-CoV-2 Infection Morbidity in Health Care Workers, Nutrients, doi:10.3390/nu14030505.
Karonova (B) et al., Effect of Cholecalciferol Supplementation on the Clinical Features and Inflammatory Markers in Hospitalized COVID-19 Patients: A Randomized, Open-Label, Single-Center Study, Nutrients, doi:10.3390/nu14132602.
Khan et al., Oral Co-Supplementation of Curcumin, Quercetin, and Vitamin D3 as an Adjuvant Therapy for Mild to Moderate Symptoms of COVID-19—Results From a Pilot Open-Label, Randomized Controlled Trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.898062.
Lakkireddy et al., Effect of Short Term High Dose Oral Vitamin D Therapy on the Inflammatory Markers in Patients with COVID 19 Disease, Archives of Clinical and Biomedical Research, doi:10.26502/acbr.50170273.
Leal-Martínez et al., Effect of a Nutritional Support System to Increase Survival and Reduce Mortality in Patients with COVID-19 in Stage III and Comorbidities: A Blinded Randomized Controlled Clinical Trial, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph19031172.
Maghbooli et al., Treatment with 25-hydroxyvitamin D3 (calcifediol) is associated with a reduction in the blood neutrophil-to-lymphocyte ratio marker of disease severity in patients hospitalized with COVID-19: a pilot, multicenter, randomized, placebo-controlled double blind clinical trial, Endocrine Practice, doi:10.1016/j.eprac.2021.09.016.
Meltzer et al., Low vs. Moderate to High Dose Vitamin D for Prevention of COVID-19, NCT04868903, clinicaltrials.gov/study/NCT04868903.
Rastogi et al., Short term, high-dose vitamin D supplementation for COVID-19 disease: a randomised, placebo-controlled, study (SHADE study), Postgraduate Medical Journal, doi:10.1136/postgradmedj-2020-139065.
Sabico et al., Effects of a 2-Week 5000 IU versus 1000 IU Vitamin D3 Supplementation on Recovery of Symptoms in Patients with Mild to Moderate Covid-19: A Randomized Clinical Trial, Nutrients, doi:10.3390/nu13072170.
Said et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1011522.
Salman et al., Role of vitamin-D supplementation in COVID-19 patients, Biological and Clinical Sciences Research Journal, doi:10.54112/bcsrj.v2023i1.322.
Sánchez-Zuno, Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation, Journal of Clinical Medicine, doi:10.3390/jcm10112378.
Sanz et al., Vitamin D3 supplementation in COVID-19 patients with cardiovascular disease and gut dysbiosis, Hipertensión y Riesgo Vascular, doi:10.1016/j.hipert.2024.04.002.
Sarhan et al., Evidence for the Efficacy of a High Dose of Vitamin D on the Hyperinflammation State in Moderate-to-Severe COVID-19 Patients: A Randomized Clinical Trial, Medicina, doi:10.3390/medicina58101358.
Seely et al., Dietary supplements to reduce symptom severity and duration in people with SARS-CoV-2: a double-blind randomised controlled trial, BMJ Open, doi:10.1136/bmjopen-2023-073761.
Singh et al., Therapeutic high-dose vitamin D for vitamin D-deficient severe COVID-19 disease: randomized, double-blind, placebo-controlled study (SHADE-S), Journal of Public Health, doi:10.1093/pubmed/fdae007.
Soliman et al., Impact of Vitamin D Therapy on the Progress COVID-19: Six Weeks Follow-Up Study of Vitamin D Deficient Elderly Diabetes Patients, Proceedings of Singapore Healthcare, doi:10.1177/20101058211041405.
Taslim et al., The Effects of 10,000 IU Vitamin D Supplementation on Improvement of Clinical Outcomes, Inflammatory and Coagulation Markers in Moderate COVID-19 Patients: A Randomized-Controlled Trial, Nutr. clín. diet. hosp., doi:10.12873/432taslim.
Torres et al., Changes in the immune response against SARS-CoV-2 in individuals with severe COVID-19 treated with high dose of vitamin D, Biomedicine & Pharmacotherapy, doi:10.1016/j.biopha.2022.112965.
Wang (C) et al., Randomized trial of influence of vitamin D on the prevention and improvement of symptomatic COVID-19, Scientific Reports, doi:10.1038/s41598-024-66267-8.
Zurita-Cruz et al., Efficacy and safety of vitamin D supplementation in hospitalized COVID-19 pediatric patients: A randomized controlled trial, Frontiers in Pediatrics, doi:10.3389/fped.2022.943529.
nice.org.uk (B), www.nice.org.uk/guidance/ng191/resources/covid19-rapid-guideline-managing-covid19-pdf-66142077109189.
Griffin et al., Perspective: Vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: implications for COVID-19, Clinical Medicine, doi:10.7861/clinmed.2021-0035.
Wang (D) et al., Optimal methods of vitamin D supplementation to prevent acute respiratory infections: a systematic review, dose–response and pairwise meta-analysis of randomized controlled trials, Nutrition Journal, doi:10.1186/s12937-024-00990-w.
Espitia-Hernandez et al., Effects of Ivermectin-azithromycin-cholecalciferol combined therapy on COVID-19 infected patients: A proof of concept study, Biomedical Research, 31:5, www.biomedres.info/biomedical-research/effects-of-ivermectinazithromycincholecalciferol-combined-therapy-on-covid19-infected-patients-a-proof-of-concept-study-14435.html.
Abdulateef et al., COVID-19 severity in relation to sociodemographics and vitamin D use, Open Medicine, doi:10.1515/med-2021-0273.
Al Sulaiman et al., Survival implications vs. complications: unraveling the impact of vitamin D adjunctive use in critically ill patients with COVID-19—A multicenter cohort study, Frontiers in Medicine, doi:10.3389/fmed.2023.1237903.
Arboleda et al., EAST framework to promote adherence to nutritional supplementation: a strategy to mitigate COVID-19 within health workers, Behavioural Public Policy, doi:10.1017/bpp.2024.11.
Asimi et al., Selenium, zinc, and vitamin D supplementation affect the clinical course of COVID-19 infection in Hashimoto’s thyroiditis, Endocrine Abstracts, doi:10.1530/endoabs.73.PEP14.2.
Aweimer et al., Mortality rates of severe COVID-19-related respiratory failure with and without extracorporeal membrane oxygenation in the Middle Ruhr Region of Germany, Scientific Reports, doi:10.1038/s41598-023-31944-7.
Baykal et al., Correlation of vitamin D level with the clinical-radiological severity of COVID-19 in geriatric patients, Journal of Health Sciences and Medicine, doi:10.32322/jhsm.1063405.
Campi et al., Vitamin D and COVID-19 severity and related mortality: a prospective study in Italy, BMC Infectious Diseases, doi:10.1186/s12879-021-06281-7.
di Filippo (B) et al., Chronic cholecalciferol supplementation and adequate vitamin D status are associated with reduced risk of Long COVID, Journal of Endocrinological Investigation, doi:10.1007/s40618-026-02858-8.
Elhadi et al., Epidemiology, outcomes, and utilization of intensive care unit resources for critically ill COVID-19 patients in Libya: A prospective multi-center cohort study, PLOS ONE, doi:10.1371/journal.pone.0251085.
Fairfield et al., Association of Vitamin D Prescribing and Clinical Outcomes in Adults Hospitalized with COVID-19, Nutrients, doi:10.3390/nu14153073.
Guldemir et al., Clinical characteristics of bus drivers and field officers infected with COVID-19: A cross-sectional study from Istanbul, Work, doi:10.3233/wor-220292.
Güven et al., The effect of high-dose parenteral vitamin D3 on COVID-19-related inhospital mortality in critical COVID-19 patients during intensive care unit admission: an observational cohort study, European Journal of Clinical Nutrition, doi:10.1038/s41430-021-00984-5.
Hafezi et al., Vitamin D enhances type I IFN signaling in COVID-19 patients, Scientific Reports, doi:10.1038/s41598-022-22307-9.
Holt et al., Risk factors for developing COVID-19: a population-based longitudinal study (COVIDENCE UK), Thorax, doi:10.1136/thoraxjnl-2021-217487.
Junior et al., Chronic diseases, chest computed tomography, and laboratory tests as predictors of severe respiratory failure and death in elderly Brazilian patients hospitalized with COVID-19: a prospective cohort study, BMC Geriatrics, doi:10.1186/s12877-022-02776-3.
Krishnan et al., Clinical comorbidities, characteristics, and outcomes of mechanically ventilated patients in the State of Michigan with SARS-CoV-2 pneumonia, Journal of Clinical Anesthesia, doi:10.1016/j.jclinane.2020.110005.
Lázaro et al., Vitamin D deficit in type 2 diabetes patients during COVID-19 lockdown with and without supplementation, Endocrine Abstracts, doi:10.1530/endoabs.70.EP552.
Mahmood et al., Coronavirus in HIP Fractures CHIP 2: Is Vitamin D Deficiency Associated with Increased Mortality from COVID-19 Infections in A Hip Fracture Population?, European Journal of Medical and Health Sciences, doi:10.24018/ejmed.2021.3.6.1159.
Mohseni et al., Do body mass index (BMI) and history of nutritional supplementation play a role in the severity of COVID-19? A retrospective study, Nutrition & Food Science, doi:10.1108/NFS-11-2020-0421.
Pecina et al., Vitamin D Status and Severe COVID-19 Disease Outcomes in Hospitalized Patients, Journal of Primary Care & Community Health
, doi:10.1177/21501327211041206.
Saheb Sharif-Askari (B) et al., Vitamin D modulates systemic inflammation in patients with severe COVID-19, Life Sciences, doi:10.1016/j.lfs.2022.120909.
Shahid et al., The effects of vitamin D therapy on outcomes for hispanic patients hospitalized for COVID-19, Abstracts from the 2022 Annual Meeting of the Society of General Internal Medicine, Journal of General Internal Medicine, doi:10.1007/s11606-022-07653-8.
Shamsi et al., Survival and Mortality in Hospitalized Children with COVID-19: A Referral Center Experience in Yazd, Iran, Canadian Journal of Infectious Diseases and Medical Microbiology, doi:10.1155/2023/5205188.
Shehab et al., Immune-boosting effect of natural remedies and supplements on progress of, and recovery from COVID-19 infection, Tropical Journal of Pharmaceutical Research, doi:10.4314/tjpr.v21i2.13.
Ullah et al., COVID-19 in patients with hepatobiliary and pancreatic diseases in East London: a single-centre cohort study, Pancreatology, doi:10.1016/j.pan.2020.10.005.
Zangeneh et al., Survival analysis based on body mass index in patients with Covid-19 admitted to the intensive care unit of Amir Al-Momenin Hospital in Arak – 2021, Obesity Medicine, doi:10.1016/j.obmed.2022.100420.
help.altmetric.com, help.altmetric.com/support/solutions/articles/6000235983-attention-sources-tracked-by-altmetric.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Ikematsu et al., Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts, New England Journal of Medicine, doi:10.1056/NEJMoa1915341.
Hayden et al., Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents, New England Journal of Medicine, doi:10.1056/NEJMoa1716197.
Kumar (B) et al., Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(21)00469-2.
López-Medina et al., Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2021.3071.
Korves et al., SARS-CoV-2 Genetic Variants and Patient Factors Associated with Hospitalization Risk, medRxiv, doi:10.1101/2024.03.08.24303818.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
Karita et al., Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection, medRxiv, doi:10.1101/2021.08.27.21262754.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
Willett et al., The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism, medRxiv, doi:10.1101/2022.01.03.21268111.
Peacock et al., The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry, bioRxiv, doi:10.1101/2021.12.31.474653.
Williams, T., Not All Ivermectin Is Created Equal: Comparing The Quality of 11 Different Ivermectin Sources, Do Your Own Research, doyourownresearch.substack.com/p/not-all-ivermectin-is-created-equal.
Xu et al., A study of impurities in the repurposed COVID-19 drug hydroxychloroquine sulfate by UHPLC-Q/TOF-MS and LC-SPE-NMR, Rapid Communications in Mass Spectrometry, doi:10.1002/rcm.9358.
Jitobaom et al., Favipiravir and Ivermectin Showed in Vitro Synergistic Antiviral Activity against SARS-CoV-2, Research Square, doi:10.21203/rs.3.rs-941811/v1.
Jitobaom (B) et al., Synergistic anti-SARS-CoV-2 activity of repurposed anti-parasitic drug combinations, BMC Pharmacology and Toxicology, doi:10.1186/s40360-022-00580-8.
Jeffreys et al., Remdesivir-ivermectin combination displays synergistic interaction with improved in vitro activity against SARS-CoV-2, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2022.106542.
Ostrov et al., Highly Specific Sigma Receptor Ligands Exhibit Anti-Viral Properties in SARS-CoV-2 Infected Cells, Pathogens, doi:10.3390/pathogens10111514.
Alsaidi et al., Griffithsin and Carrageenan Combination Results in Antiviral Synergy against SARS-CoV-1 and 2 in a Pseudoviral Model, Marine Drugs, doi:10.3390/md19080418.
Andreani et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microbial Pathogenesis, doi:10.1016/j.micpath.2020.104228.
De Forni et al., Synergistic drug combinations designed to fully suppress SARS-CoV-2 in the lung of COVID-19 patients, PLoS ONE, doi:10.1371/journal.pone.0276751.
Wan et al., Synergistic inhibition effects of andrographolide and baicalin on coronavirus mechanisms by downregulation of ACE2 protein level, Scientific Reports, doi:10.1038/s41598-024-54722-5.
Fiaschi et al., In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants, Viruses, doi:10.3390/v16020168.
Xing et al., Published anti-SARS-CoV-2 in vitro hits share common mechanisms of action that synergize with antivirals, Briefings in Bioinformatics, doi:10.1093/bib/bbab249.
Chen (C) et al., Synergistic Inhibition of SARS-CoV-2 Replication Using Disulfiram/Ebselen and Remdesivir, ACS Pharmacology & Translational Science, doi:10.1021/acsptsci.1c00022.
Hempel et al., Synergistic inhibition of SARS-CoV-2 cell entry by otamixaban and covalent protease inhibitors: pre-clinical assessment of pharmacological and molecular properties, Chemical Science, doi:10.1039/D1SC01494C.
Schultz et al., Pyrimidine inhibitors synergize with nucleoside analogues to block SARS-CoV-2, Nature, doi:10.1038/s41586-022-04482-x.
Ohashi et al., Potential anti-COVID-19 agents, cepharanthine and nelfinavir, and their usage for combination treatment, iScience, doi:10.1016/j.isci.2021.102367.
Al Krad et al., The protease inhibitor Nirmatrelvir synergizes with inhibitors of GRP78 to suppress SARS-CoV-2 replication, bioRxiv, doi:10.1101/2025.03.09.642200.
Abd Elsalam et al., Anti-COVID-19 activity and simple HPLC method for concurrent detection of repurposed drugs in novel binary mixtures, AMB Express, doi:10.1186/s13568-026-02030-8.
Rana et al., Ivermectin and Doxycycline combination as a promising anti-viral drug candidate: an in-silico and DFT study, In Silico Pharmacology, doi:10.1007/s40203-026-00576-w.
Setz et al., Synergistic Virus Neutralizing Activities of European Black Elderberry Fruit Extract and Iota-Carrageenan Against SARS-CoV-2, Influenza A Virus and Respiratory Syncytial Virus, Nutrients, doi:10.3390/nu18081205.
Ali et al., Preclinical Screening Platform Identifies Azatadine‐Dimaleate as a Potent Repurposed Therapeutic Against SARS‐CoV‐2 Infection, Journal of Medical Virology, doi:10.1002/jmv.70713.
Lew et al., Combination of Remdesivir and Ivermectin Exerts Highly Potent and Synergistic Antiviral Activity Against Murine Coronavirus and SARS-CoV-2 Infections, Cells, doi:10.3390/cells15131146.
Khatun et al., An All-Oral Antiviral Combination Strategy against COVID-19 Enabled by the Synergistic Mechanism of Action of Auranofin and Remdesivir, Elsevier BV, doi:10.2139/ssrn.6942990.
Thairu et al., A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2022/v34i44A36328.
Singh (B) et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Zimmerman et al., Melatonin and the Optics of the Human Body, Melatonin Research, doi:10.32794/mr11250016.
Assiri et al., COVID-19 related treatment and outcomes among COVID-19 ICU patients: A retrospective cohort study, Journal of Infection and Public Health, doi:10.1016/j.jiph.2021.08.030.
Petkovich et al., Modified-release oral calcifediol corrects vitamin D insufficiency with minimal CYP24A1 upregulation, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2014.11.022.
Boulware, D., Comments regarding paper rejection, twitter.com/boulware_dr/status/1311331372884205570.
Rothstein, H., Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments, www.wiley.com/en-ae/Publication+Bias+in+Meta+Analysis:+Prevention,+Assessment+and+Adjustments-p-9780470870143.
Stanley et al., Meta-regression approximations to reduce publication selection bias, Research Synthesis Methods, doi:10.1002/jrsm.1095.
Rücker et al., Arcsine test for publication bias in meta-analyses with binary outcomes, Statistics in Medicine, doi:10.1002/sim.2971.
Peters, J., Comparison of Two Methods to Detect Publication Bias in Meta-analysis, JAMA, doi:10.1001/jama.295.6.676.
Moreno et al., Assessment of regression-based methods to adjust for publication bias through a comprehensive simulation study, BMC Medical Research Methodology, doi:10.1186/1471-2288-9-2.
Macaskill et al., A comparison of methods to detect publication bias in meta-analysis, Statistics in Medicine, doi:10.1002/sim.698.
Egger et al., Bias in meta-analysis detected by a simple, graphical test, BMJ, doi:10.1136/bmj.315.7109.629.
Harbord et al., A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints, Statistics in Medicine, doi:10.1002/sim.2380.
Ren et al., Association of genetic polymorphisms with COVID-19 infection and outcomes: An updated meta-analysis based on 62 studies, Heliyon, doi:10.1016/j.heliyon.2023.e23662.
Al-Gharrawi et al., Association of ApaI rs7975232 and BsmI rs1544410 in clinical outcomes of COVID-19 patients according to different SARS-CoV-2 variants, Scientific Reports, doi:10.1038/s41598-023-30859-7.
Zeidan et al., Vitamin D deficiency and vitamin D receptor FokI polymorphism as risk factors for COVID-19, Pediatric Research, doi:10.1038/s41390-022-02275-6.
Mamurova et al., A strong association between the VDR gene markers and SARS-CoV-2 variants, Research Square, doi:10.21203/rs.3.rs-1806260/v1.
Al-Anouti et al., Associations between Genetic Variants in the Vitamin D Metabolism Pathway and Severity of COVID-19 among UAE Residents, Nutrients, doi:10.3390/nu13113680.
Abdollahzadeh et al., Association of Vitamin D receptor gene polymorphisms and clinical/severe outcomes of COVID-19 patients, Infection, Genetics and Evolution, doi:10.1016/j.meegid.2021.105098.
Kotur et al., Association of Vitamin D, Zinc and Selenium Related Genetic Variants With COVID-19 Disease Severity, Frontiers in Nutrition, doi:10.3389/fnut.2021.689419.
Shawi Shawi et al., Role of FokI rs.2228570 and Tru9I rs.757343 Polymorphisms in the Mortality of Patients Infected with Different Variants of SARS-CoV-2, Archives of Medical Research, doi:10.1016/j.arcmed.2023.03.006.
Protas et al., Plasma 25-Hydroxyvitamin D Level and VDR Gene Single Nucleotide Polymorphism rs2228570 Influence on COVID-19 Susceptibility among the Kazakh Ethnic Group—A Pilot Study, Nutrients, doi:10.3390/nu15071781.
Alhammadin et al., Exploring the Influence of VDR Genetic Variants TaqI, ApaI, and FokI on COVID-19 Severity and Long-COVID-19 Symptoms, Journal of Personalized Medicine, doi:10.3390/jpm13121663.
Regina da Silva Correa da Ronda et al., Single-Nucleotide Polymorphisms Related to Vitamin D Metabolism and Severity or Mortality of COVID-19: A Systematic Review and Meta-analysis, Gene, doi:10.1016/j.gene.2024.148236.
Tentolouris (B) et al., The Association of Vitamin D Receptor Polymorphisms with COVID-19 Severity, Nutrients, doi:10.3390/nu16050727.
Ochoa-Ramírez et al., Vitamin D receptor gene polymorphisms role in COVID‐19 severity: Results of a Mexican patients’ cohort, International Journal of Immunogenetics, doi:10.1111/iji.12674.
Mohammadifard et al., Comparing vitamin D receptor gene polymorphisms in rs11568820, rs7970314, rs4334089 between COVID-19 patients with mild and severe symptoms: a case control study, Scientific Reports, doi:10.1038/s41598-024-57424-0.
Karcıoğlu Batur et al., Investigation of the Relationship between Vitamin D Deficiency and Vitamin D-Binding Protein Polymorphisms in Severe COVID-19 Patients, Diagnostics, doi:10.3390/diagnostics14171941.
Chen (D) et al., Vitamin D blood levels and vitamin D receptor polymorphisms contribute to post-acute sequelae of severe acute respiratory syndrome coronavirus 2 severity in the pediatric patients, Research Square, doi:10.21203/rs.3.rs-7146347/v1.
Jaurrieta-Largo et al., A Machine Learning Approach to Understanding the Genetic Role in COVID-19 Prognosis: The Influence of Gene Polymorphisms Related to Inflammation, Vitamin D, and ACE2, International Journal of Molecular Sciences, doi:10.3390/ijms26167975.
Awla et al., Vitamin D pathway as a multi-level predictor of COVID-19 severity and mortality: Integrating serum levels, FokI (rs2228570) VDR polymorphism, and lung tissue expression, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2025.106879.
Younes, S., The influence of micronutrients on olfactory dysfunction associated with COVID-19 and long COVID, Next Research, doi:10.1016/j.nexres.2026.101727.
Al-Khrasani et al., Do vitamins halt the COVID-19-evoked pro-inflammatory cytokines involved in the development of neuropathic pain?, Biomedicine & Pharmacotherapy, doi:10.1016/j.biopha.2025.118346.
Kow (B) et al., Vitamin D and COVID‐19: How much more evidence do we need?, Nutrition in Clinical Practice, doi:10.1002/ncp.11349.
Bigman et al., A Comprehensive Scoping Review on Diet and Nutrition in Relation to Long COVID-19 Symptoms and Recovery, Nutrients, doi:10.3390/nu17111802.
Hewison, M., COVID-19 and our understanding of vitamin D and immune function, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2025.106710.
Wimalawansa, S., Vitamin D Deficiency Meets Hill’s Criteria for Causation in SARS-CoV-2 Susceptibility, Complications, and Mortality: A Systematic Review, Nutrients, doi:10.3390/nu17030599.
Sanduzzi Zamparelli et al., Immune-Boosting and Antiviral Effects of Antioxidants in COVID-19 Pneumonia: A Therapeutic Perspective, Life, doi:10.3390/life15010113.
Fazli et al., Possible Link between Gut Microbiota, Diet, and COVID-19 Infection, Journal of Medical Bacteriology, 12:4, jmb.tums.ac.ir/index.php/jmb/article/view/525.
Wojciulik et al., The impact of genetic polymorphism on course and severity of the SARS-CoV-2 infection and COVID-19 disease, Przeglad Epidemiologiczny, doi:10.32394/pe/194862.
Wimalawansa (B), S., Unveiling the Interplay—Vitamin D and ACE-2 Molecular Interactions in Mitigating Complications and Deaths from SARS-CoV-2, Biology, doi:10.3390/biology13100831.
Santa et al., Comparative analysis of COVID-19 responses in Japan and Africa: diet, phytochemicals, vitamin D, and gut microbiota in reducing mortality—A systematic review and meta-analysis, Frontiers in Nutrition, doi:10.3389/fnut.2024.1465324.
Kaushal, A., Nutraceuticals and pharmacological to balance the transitional microbiome to extend immunity during COVID-19 and other viral infections, Journal of Translational Medicine, doi:10.1186/s12967-024-05587-9.
Mu et al., Anti-inflammatory and Nutritional Interventions Against SARS-CoV-2: A Comprehensive Review, Journal of Agriculture and Food Research, doi:10.1016/j.jafr.2024.101422.
Wimalawansa (C), S., Unlocking Insights: Navigating COVID-19 Challenges and Emulating Future Pandemic Resilience Strategies with Strengthening Natural Immunity, Heliyon, doi:10.1016/j.heliyon.2024.e34691.
Imran et al., Therapeutic Role of Vitamin D in COVID-19 Patients, Clinical Nutrition Open Science, doi:10.1016/j.nutos.2024.07.004.
Polonowita et al., Molecular Quantum and Logic Process of Consciousness—Vitamin D Big-Data in COVID-19—A Case for Incorporating Machine Learning In Medicine, European Journal of Biomedical and Pharmaceutical sciences, doi:10.5281/zenodo.10435649.
Gomaa et al., Pharmacological evaluation of vitamin D in COVID-19 and long COVID-19: recent studies confirm clinical validation and highlight metformin to improve VDR sensitivity and efficacy, Inflammopharmacology, doi:10.1007/s10787-023-01383-x.
Cutolo et al., Involvement of the secosteroid vitamin D in autoimmune rheumatic diseases and COVID-19, Nature Reviews Rheumatology, doi:10.1038/s41584-023-00944-2.
Schloss et al., Nutritional deficiencies that may predispose to long COVID, Inflammopharmacology, doi:10.1007/s10787-023-01183-3.
Arora et al., Global Dietary and Herbal Supplement Use during COVID-19—A Scoping Review, Nutrients, doi:10.3390/nu15030771.
Nicoll et al., COVID-19 Prevention: Vitamin D Is Still a Valid Remedy, Journal of Clinical Medicine, doi:10.3390/jcm11226818.
Foshati et al., Antioxidants and clinical outcomes of patients with coronavirus disease 2019: A systematic review of observational and interventional studies, Food Science & Nutrition, doi:10.1002/fsn3.3034.
Quesada-Gomez et al., Vitamin D Endocrine System and COVID-19: Treatment with Calcifediol, Nutrients, doi:10.3390/nu14132716.
DiGuilio (B) et al., Micronutrient Improvement of Epithelial Barrier Function in Various Disease States: A Case for Adjuvant Therapy, International Journal of Molecular Sciences, doi:10.3390/ijms23062995.
Grant (B) et al., A Narrative Review of the Evidence for Variations in Serum 25-Hydroxyvitamin D Concentration Thresholds for Optimal Health, Nutrients, doi:10.3390/nu14030639.
Shaw Stewart et al., Temperature dependent viral tropism: understanding viral seasonality and pathogenicity as applied to the avoidance and treatment of endemic viral respiratory illnesses, Reviews in Medical Virology, doi:10.1002/rmv.2241.
Shah Alam et al., The role of vitamin D in reducing SARS-CoV-2 infection: An update, International Immunopharmacology, doi:10.1016/j.intimp.2021.107686.
Kohlmeier et al., When Mendelian randomisation fails, BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000265.
Brenner, H., Vitamin D Supplementation to Prevent COVID-19 Infections and Deaths—Accumulating Evidence from Epidemiological and Intervention Studies Calls for Immediate Action, Nutrients, doi:10.3390/nu13020411.
Mercola et al., Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity, Nutrients 2020, 12:11, 3361, doi:10.3390/nu12113361.
Basha et al., Is the shielding effect of cholecalciferol in SARS CoV-2 infection dependable? An evidence based unraveling, Clinical Epidemiology and Global Health, doi:10.1016/j.cegh.2020.10.005.
Xu (B) et al., The importance of vitamin d metabolism as a potential prophylactic, immunoregulatory and neuroprotective treatment for COVID-19, Journal of Translational Medicine, doi:10.1186/s12967-020-02488-5.
Alexander et al., Early Nutritional Interventions with Zinc, Selenium and Vitamin D for Raising Anti-Viral Resistance Against Progressive COVID-19, Nutrients, doi:10.3390/nu12082358.
Andrade et al., Vitamin A and D deficiencies in the prognosis of respiratory tract infections: A systematic review with perspectives for COVID-19 and a critical analysis on supplementation, SciELO preprints, doi:10.1590/SciELOPreprints.839.
Grant (C) et al., Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths, Nutrients, 12:4, 988, doi:10.3390/nu12040988.
McCullough et al., Daily oral dosing of vitamin D3 using 5000 TO 50,000 international units a day in long-term hospitalized patients: Insights from a seven year experience, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2018.12.010.
Palacios et al., Is vitamin D deficiency a major global public health problem?, J Steroid Biochem Mol Biol., 2014, 144PA, 138–145, doi:10.1016/j.jsbmb.2013.11.003.
Cannell et al., Epidemic influenza and vitamin D, Epidemiol Infect., 2006, 134:6. 1129-40, doi:10.1017/S0950268806007175.
Elayeh et al., Prevalence and predictors of self‐medication drugs to prevent or treat COVID‐19: Experience from a Middle Eastern country, International Journal of Clinical Practice, doi:10.1111/ijcp.14860.
Sadio et al., Assessment of self-medication practices in the context of the COVID-19 outbreak in Togo, BMC Public Health, doi:10.1186/s12889-020-10145-1.
Dantas et al., Automedicação no contexto de COVID-19, os perigos da prática e fatores associados, Research, Society and Development, doi:10.33448/rsd-v12i6.42039.
Okoye et al., Self medication practices and its determinants in health care professionals during the coronavirus disease-2019 pandemic: cross-sectional study, International Journal of Clinical Pharmacy, doi:10.1007/s11096-021-01374-4.
Ahmed et al., Behavioral preventive measures and the use of medicines and herbal products among the public in response to Covid-19 in Bangladesh: A cross-sectional study, PLOS ONE, doi:10.1371/journal.pone.0243706.
Lam et al., A public survey of traditional, complementary and integrative medicine use during the COVID-19 outbreak in Hong Kong, PLOS ONE, doi:10.1371/journal.pone.0253890.
Chellappan et al., Self-medication for prevention of COVID-19: a cross-sectional online survey among the general public in South India, INDIAN JOURNAL OF APPLIED RESEARCH, doi:10.36106/ijar/9209352.
Mulder et al., Prevalence and predictive factors of complementary medicine use during the first wave of the COVID-19 pandemic of 2020 in the Netherlands, BMC Complementary Medicine and Therapies, doi:10.1186/s12906-022-03528-x.
Wegbom et al., Self-Medication Practices and Associated Factors in the Prevention and/or Treatment of COVID-19 Virus: A Population-Based Survey in Nigeria, Frontiers in Public Health, doi:10.3389/fpubh.2021.606801.
Aitafo et al., Self-Medication among Health Workers during the COVID-19 Pandemic in Southern Nigeria: Knowledge, Patterns, Practice and Associated Factors, International Journal of Health Sciences and Research, doi:10.52403/ijhsr.20220223.
Grosman-Dziewiszek et al., Patterns of Dietary Supplement Use during the COVID-19 Pandemic in Poland: Focus on Vitamin D and Magnesium, Nutrients, doi:10.3390/nu16193225.
Kaplan, R., Physician deaths from COVID-19 have been lower than expected, Occupational Medicine, doi:10.1093/occmed/kqaa210.
Kiang et al., Excess Mortality Among US Physicians During the COVID-19 Pandemic, JAMA Internal Medicine, doi:10.1001/jamainternmed.2022.6308.
medicospelavidacovid19.com.br, medicospelavidacovid19.com.br/editoriais/folha-de-s-paulo-revela-numeros-de-david-uip-veja-a-comparacao-com-medicos-que-fazem-tratamento-precoce/.
di Filippo (C) et al., Impact of chronic cholecalciferol supplementation and vitamin D status on risk of post-vaccination SARS-CoV-2 breakthrough infection, Endocrine, doi:10.1007/s12020-026-04677-6.
Almacioglu et al., Association of Serum Vitamin D and Hematological Parameters with SARS-CoV-2 PCR Positivity: A Combined Biomarker Approach in Asymptomatic Children, International Journal of Molecular Sciences, doi:10.3390/ijms27104393.
Rizzi et al., Higher 25(OH)D Levels at Admission Predict a Favorable Disease Evolution in Moderate-to-Severe COVID-19 Patients, International Journal of Molecular Sciences, doi:10.3390/ijms27083541.
Abbas et al., Acute SARS-CoV-2 viral load and systemic inflammation are associated with neuropsychiatric and musculoskeletal symptoms in long COVID, PLOS One, doi:10.1371/journal.pone.0346978.
Dip et al., Vitamin D status and its association with the severity of COVID-19 among hospitalized patients, International Journal of Advances in Medicine, doi:10.18203/2349-3933.ijam20241623.
Jazar et al., Role of Vitamin D Levels in COVID-19 Disease Severity: A Multicenter Retrospective Study from Qatar, Pakistan Journal of Biological Sciences, doi:10.3923/pjbs.2025.640.648.
Zendehdel et al., Investigation of the prevalence of vitamin D deficiency in hospitalized COVID-19 patients and its association with disease severity, outcome, and mortality, Research Square, doi:10.21203/rs.3.rs-8254002/v1.
Nahhas et al., Investigating the relationship between vitamin D levels and COVID-19 severity among patients at MNGHA in Saudi Arabia, International Journal of Medicine in Developing Countries, doi:10.24911/IJMDC.51-1747240075.
Monroy-Iglesias et al., Effects of vitamin D on COVID-19 risk and hospitalisation in the UK biobank, PLoS One, doi:10.1371/journal.pone.0328232.
Li et al., Association Between Vitamin A and D Status and the Risk of COVID-19 in the Elderly Population: A Single-Center Experience, Journal of Inflammation Research, doi:10.2147/JIR.S522566.
Madar et al., Vitamin D Status and SARS-CoV-2 Positivity in Lebanon Among Adults: A Cross-Sectional Study in South Lebanon, COVID, doi:10.3390/covid5070097.
Chen (E) et al., Association between vitamin D deficiency and clinical outcome in patients with COVID-19 in the post-Omicron phase, Frontiers in Nutrition, doi:10.3389/fnut.2025.1583276.
Blázquez-Cabrera et al., ALBACOVIDIOL Study: Effect of Calcifediol Treatment on Mortality in Patients Hospitalized for COVID-19: A Retrospective Analysis, Nutrients, doi:10.3390/nu17121968.
Wagner et al., Exploring the association between vitamin D status and Corona Virus-19 infection in a cohort of adults aged 50 years and older, Clinical Nutrition Open Science, doi:10.1016/j.nutos.2025.05.007.
Ito et al., Serum Vitamin D and the Risk of SARS-CoV-2 and Seasonal Influenza Infection During the Twindemic Period, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2025.05.007.
Tanriverdi et al., COVİD-19 Pnömonisi Gelişen Hastalarda Vitamin D Düzeylerinin Hastane Yatış Süresi ve Mortalite ile İlişkisinin Değerlendirilmesi: Retrospektif Analiz, International Journal of Tokat Medical Sciences, 17:18-25, dergipark.org.tr/tr/pub/ijtms/issue/91643/1537150.
Hossain et al., A Study on Serum Vitamin D3 Level in Patients with Covid-19: A Cross-Sectional Study in Kolkata, National Journal of Medical Research, doi:10.55489/njmr.150220251070.
Domènech-Montoliu et al., Vitamin D Status and Incidence of SARS-CoV-2 Reinfections in the Borriana COVID-19 Cohort: A Population-Based Prospective Cohort Study, Tropical Medicine and Infectious Disease, doi:10.3390/tropicalmed10040098.
Mohamed et al., Nutritional Assessment of Critically Ill Children with COVID-19 Admitted to PICU, The Medical Journal of Cairo University, doi:10.21608/mjcu.2024.411836.
Perestiuk et al., Vitamin D status in children with COVID-19: does it affect the development of long COVID and its symptoms?, Frontiers in Pediatrics, doi:10.3389/fped.2025.1507169.
Dinoi et al., Retrospective Clinical Investigation into the Association Between Abnormal Blood Clotting, Oral Anticoagulant Therapy, and Medium-Term Mortality in a Cohort of COVID-19 Patients, Biomedicines, doi:10.3390/biomedicines13030535.
Vasconcelos et al., High-dose vitamin D supplementation in patients with severe acute respiratory syndrome coronavirus 2 pneumonia hospitalized in a polyvalent intensive care unit: A retrospective cohort study, Nutrition in Clinical Practice, doi:10.1002/ncp.11277.
Najih et al., Impact of Vitamin D Levels on Clinical Outcomes in SARS-CoV-2 Infections, Cureus, doi:10.7759/cureus.78291.
Sümegi et al., Effect of Moderately High-Dose Vitamin D3 Supplementation on Mortality in Patients Hospitalized for COVID-19 Infection, Nutrients, doi:10.3390/nu17030507.
You et al., Associations of vitamin D levels and clinical parameters with COVID‐19 infection, severity and mortality in hemodialysis patients: A cohort study, Hemodialysis International, doi:10.1111/hdi.13194.
Chadda et al., Vitamin D deficiency and duration of COVID-19 symptoms in UK healthcare workers, Frontiers in Medicine, doi:10.3389/fmed.2024.1494129.
Pashaei et al., The Association Between COVID-19 Infection Severity and Micronutrient Deficiencies in Children, Journal of Comprehensive Pediatrics, doi:10.5812/jcp-149127.
Mirkarimi et al., Clinical and Epidemiological Features of Pediatric COVID‐19: A Retrospective Study, Health Science Reports, doi:10.1002/hsr2.70181.
Chan et al., Short-Term Outcomes in Patients With Coexistence of COVID-19 Infection and Vitamin D Deficiency: A Large Cohort Study, Cureus, doi:10.7759/cureus.71952.
Hemdan, D., Level of vitamins and minerals for people with coronavirus (Covid-19) in Taif, Kingdom of Saudi Arabia, Materials Express, doi:10.1166/mex.2022.2168.
García-Zendejas et al., Asociación de los niveles de vitamina D y magnesio con la gravedad y la mortalidad en pacientes con COVID-19, Cirugía y Cirujanos, doi:10.24875/CIRU.23000514.
Hammam et al., Relation between vitamin D and COVID-19 in Egyptian patients, The Egyptian Journal of Internal Medicine, doi:10.1186/s43162-024-00351-3.
Rachman et al., Adequate serum 25-hydroxy-vitamin D levels are correlated with low anti-PF4 levels in mild COVID-19 Patients: An observational study, Medicine, doi:10.1097/MD.0000000000039252.
Božić et al., The role of serum vitamin D concentrations in predicting COVID-19 course and outcome, Acta Facultatis Medicae Naissensis, doi:10.5937/afmnai41-42961.
Pietzner et al., Complex patterns of multimorbidity associated with severe COVID-19 and long COVID, Communications Medicine, doi:10.1038/s43856-024-00506-x.
Değirmenci et al., Is vitamin D level important in pregnant women with COVID-19?, Journal of Controversies in Obstetrics & Gynecology and Pediatrics, doi:10.51271/JCOGP-0035.
Węgrzynek-Gallina et al., Profile of patients diagnosed with COVID-19 infection: a single-center retrospective study, Health Problems of Civilization, doi:10.5114/hpc.2023.133494.
Milan et al., Factors Associated with Adverse Outcomes among SARS-CoV-2 Positive Children in a Tertiary Government COVID-19 Referral Hospital in the Philippines, Acta Medica Philippina, doi:10.47895/amp.v58i7.8392.
Cardoso et al., Vitamin D levels and COVID-19 severe pneumonia: a prospective case-control study, medRxiv, doi:10.1101/2024.06.10.24308690.
Singhsakul et al., Association of vitamin D level and severity of COVID-19 disease, Journal of Southeast Asian Medical Research, doi:10.55374/jseamed.v8.202.
Pavlyshyn et al., Micronutrient status (vitamins A and D) and its effect on the severity of the course of COVID-19 in children, Неонатологія, хірургія та перинатальна медицина, doi:10.24061/2413-4260.XIV.1.51.2024.6.
Arambepola et al., The role of vitamin D as a preventive strategy in COVID-19 infections: evidence from South Asia, Research Square, doi:10.21203/rs.3.rs-3964082/v1.
Guðnadóttir et al., High risk of malnutrition among hospitalised coronavirus disease 2019 (COVID-19) patients is associated with mortality and other clinical outcomes, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2024.02.023.
Devi et al., Vitamin D in COVID-19, International Journal of Clinical Biochemistry and Research, doi:10.18231/j.ijcbr.2023.007.
Comunale et al., Vitamin D Supplementation and Prior Oral Poliovirus Vaccination Decrease Odds of COVID-19 Outcomes among Adults Recently Inoculated with Inactivated Poliovirus Vaccine, Vaccines, doi:10.3390/vaccines12020121.
Athanassiou et al., Vitamin D Levels as a Marker of Severe SARS-CoV-2 Infection, Life, doi:10.3390/life14020210.
Rozemeijer et al., Micronutrient Status of Critically Ill Patients with COVID-19 Pneumonia, Nutrients, doi:10.3390/nu16030385.
Choi et al., Prognostic Factors for Predicting Post-COVID-19 Condition in Patients With COVID-19 in an Outpatient Setting, Journal of Korean Medical Science, doi:10.3346/jkms.2024.39.e23.
Efe Iris et al., Vitamin D Deficiency and Receptor Polymorphisms as Risk Factors for COVID-19, Jundishapur Journal of Microbiology, doi:10.5812/jjm-140726.
Wu (B) et al., Association between vitamin D deficiency and post-acute outcomes of SARS-CoV-2 infection, European Journal of Nutrition, doi:10.1007/s00394-023-03298-3.
Renieris et al., Association of Vitamin D with severity and outcome of COVID-19: Clinical and Experimental Evidence, Journal of Innate Immunity, doi:10.1159/000535302.
Akbar et al., The Association between Lifestyle Factors and COVID-19: Findings from Qatar Biobank, Nutrients, doi:10.3390/nu16071037.
Bogomaz et al., Vitamin D as a predictor of negative outcomes in hospitalized COVID-19 patients: An observational study, Canadian Journal of Respiratory Therapy, doi:10.29390/001c.87408.
Seely (B) et al., Dietary supplements to reduce symptom severity and duration in people with SARS-CoV-2: a double-blind randomised controlled trial, BMJ Open, doi:10.1136/bmjopen-2023-073761.
Ogasawara et al., The effect of 1-hydroxy-vitamin D treatment in hospitalized patients with COVID-19: A retrospective study, Clinical Nutrition, doi:10.1016/j.clnu.2023.08.021.
Mayurathan et al., Association of vitamin D levels with severity and outcome of COVID-19 infection among inward patients at a tertiary care unit in Sri Lanka, Asian Journal of Internal Medicine, 2:2, ajim.sljol.info/articles/10.4038/ajim.v2i2.84.
Mingiano et al., Vitamin D Deficiency in COVID-19 Patients and Role of Calcifediol Supplementation, Nutrients, doi:10.3390/nu15153392.
Connolly et al., An observational study of the association of vitamin D status and other patient characteristics with COVID-19 severity and mortality, Proceedings of the Nutrition Society, doi:10.1017/S0029665121002482.
Frish et al., The Association of Weight Reduction and Other Variables after Bariatric Surgery with the Likelihood of SARS-CoV-2 Infection, Journal of Clinical Medicine, doi:10.3390/jcm12124054.
Manojlovic et al., Association between vitamin D hypovitaminosis and severe forms of COVID-19, European Review for Medical and Pharmacological Sciences, doi:10.26355/eurrev_202306_32651.
Jalavu et al., An investigation of the correlation of vitamin D status and management outcomes in patients with severe COVID-19 at a South African tertiary hospital, IJID Regions, doi:10.1016/j.ijregi.2023.05.007.
Wani et al., Impact of Age and Clinico-Biochemical Parameters on Clinical severity of SARS-CoV-2 Infection, Intervirology, doi:10.1159/000530906.
Hogarth et al., Clinical Characteristics and Comorbidities associated with SARS-CoV-2 breakthrough infection in the University of California Healthcare Systems, The American Journal of the Medical Sciences, doi:10.1016/j.amjms.2023.04.019.
Ritsinger et al., History of heart failure and chronic kidney disease and risk of all-cause death after COVID-19 during the first three waves of the pandemic in comparison with influenza outbreaks in Sweden: a registry-based, retrospective, case–control study, BMJ Open, doi:10.1136/bmjopen-2022-069037.
Regalia et al., Vitamin D Status and SARS-CoV-2 Infection in a Cohort of Kidney Transplanted Patients, Nutrients, doi:10.3390/nu14020317.
Sanamandra et al., Correlation between Serum Vitamin D3 levels and severity of COVID-19, experience from a COVID-19-dedicated tertiary care hospital from Western India, Indian Journal of Endocrinology and Metabolism, doi:10.4103/ijem.ijem_383_22.
AlKhafaji et al., The Impact of Vitamin D Level on the Severity and Outcome of Hospitalized Patients with COVID-19 Disease, International Journal of General Medicine, doi:10.2147/ijgm.s346169.
Baralić et al., Significance of 1,25-Dihydroxyvitamin D3 on Overall Mortality in Peritoneal Dialysis Patients with COVID-19, Nutrients, doi:10.3390/nu15092050.
Hafez et al., Vitamin D Status in Relation to the Clinical Outcome of Hospitalized COVID-19 Patients, Frontiers in Medicine, doi:10.3389/fmed.2022.843737.
Allami et al., The risk of up normal values of two parameters obesity and vitamin D in incidence of coronavirus disease-19 among Iraqi patients, 1st Samarra International Conference for Pure and Applied Sciences (SICPS2021), doi:10.1063/5.0121166.
Zafar et al., Vitamin D levels and mortality with SARS-COV-2 infection: a retrospective two-centre cohort study, Postgraduate Medical Journal, doi:10.1136/postgradmedj-2021-140564.
Cetin Ozbek et al., Does the Level of Vitamin D in COVID-19 Patients Affect the Survival and Duration of Hospital Stay?, Clinical Science of Nutrition, doi:10.5152/ClinSciNutr.2023.22059.
Rachman (B) et al., The association between vitamin D deficiency and the clinical outcomes of hospitalized COVID-19 patients, F1000Research, doi:10.12688/f1000research.132214.4.
Basińska-Lewandowska et al., Frequency of COVID-19 Infection as a Function of Vitamin D Levels, Nutrients, doi:10.3390/nu15071581.
Hermawan et al., Association between 25(OH)D3 Levels and the Presence of COVID-19 Symptoms, Molecular and Cellular Biomedical Sciences, doi:10.21705/mcbs.v7i1.306.
Bayrak et al., Association Between Vitamin D Levels and COVID-19 Infection in Children: A Case-Control Study, Turkish Archives of Pediatrics, doi:10.5152/turkarchpediatr.2023.22217.
Khalil et al., Evaluation of vitamin D in COVID-19 patients, 1st Samarra International Conference for Pure and Applied Sciences (SICPS2021), doi:10.1063/5.0122108.
Gonzalez et al., Vitamin D on admission and disease severity in patients with COVID-19 in the Intensive Care Unit, Revista de Nutrición Clínica y Metabolismo, doi:10.35454/rncm.v6n2.485.
Arabadzhiyska et al., Serum vitamin D levels and inflammatory status in COVID-19 patients, Bratislava Medical Journal, doi:10.4149/bll_2023_069.
Schmidt et al., Identification of Clinical Response Predictors of Tocilizumab Treatment in Patients with Severe COVID-19 Based on Single-Center Experience, Journal of Clinical Medicine, doi:10.3390/jcm12062429.
Huang et al., Effect of vitamin D status on adult COVID-19 pneumonia induced by Delta variant: A longitudinal, real-world cohort study, Frontiers in Medicine, doi:10.3389/fmed.2023.1121256.
Nasiri et al., Does vitamin D serum level affect prognosis of COVID-19 patients?, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.04.083.
Davran et al., Relationship between vitamin D level and clinical status in COVID-19 patients, Konuralp Tıp Dergisi, doi:10.18521/ktd.1134319.
Bucurica et al., Association of Vitamin D Deficiency and Insufficiency with Pathology in Hospitalized Patients, Diagnostics, doi:10.3390/diagnostics13050998.
Topan et al., 25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital, Nutrients, doi:10.3390/nu15051227.
Siuka et al., The effect of Vitamin D levels on the course of COVID-19 in hospitalized patients – a 1-year prospective cohort study, F1000Research, doi:10.12688/f1000research.131730.1.
Şengül et al., Serum Vitamin D Concentrations and Covid-19 In Pregnant Women, Does Vitamin D Supplementation Impact Results? A Comprehensive Study, Cukurova Anestezi ve Cerrahi Bilimler Dergisi, doi:10.36516/jocass.1185181.
Chen (F) et al., Plasma 25(OH)D Level is Associated with the Nucleic Acid Negative Conversion Time of COVID-19 Patients: An Exploratory Study, Infection and Drug Resistance, doi:10.2147/idr.s400561.
Tan et al., Association of Vitamin D levels on the Clinical Outcomes of Patients Hospitalized for COVID-19 in a Tertiary Hospital, Journal of the ASEAN Federation of Endocrine Societies, doi:10.15605/jafes.038.01.07.
Ortatatli et al., Potential Role of Vitamin D, ACE2 and the Proteases as TMPRSS2 and Furin on SARS-CoV-2 Pathogenesis and COVID-19 Severity, Archives of Medical Research, doi:10.1016/j.arcmed.2023.02.002.
Arabi et al., The association between vitamin D3 deficiency and acute kidney injury in COVID-19 patients, Journal of Renal Injury Prevention, doi:10.34172/jrip.2022.32126.
Batur et al., Association between Vitamin D Status and Secondary Infections in Patients with Severe COVID-19 Admitted in the Intensive Care Unit of a Tertiary-Level Hospital in Turkey, Diagnostics, doi:10.3390/diagnostics13010059.
Mostafa et al., Clinical and Prognostic Significance of Baseline Serum Vitamin D Levels in Hospitalized Egyptian Covid-19 Patients, International Journal of General Medicine, doi:10.2147/IJGM.S386815.
Valecha et al., The Effect of Vitamin B12, Magnesium and Vitamin D in COVID-19 among Geriatric Patients, International Journal of Pharmaceutical and Clinical Research, 14:5, impactfactor.org/PDF/IJPCR/14/IJPCR,Vol14,Issue5,Article113.pdf.
van Helmond et al., Vitamin D3 Supplementation at 5000 IU Daily for the Prevention of Influenza-like Illness in Healthcare Workers: A Pragmatic Randomized Clinical Trial, Nutrients, doi:10.3390/nu15010180.
De Nicolò et al., Possible Impact of Vitamin D Status and Supplementation on SARS-CoV-2 Infection Risk and COVID-19 Symptoms in a Cohort of Patients with Inflammatory Bowel Disease, Nutrients, doi:10.3390/nu15010169.
Abdrabbo AlYafei et al., Association of Serum Vitamin D level and COVID-19 infection: A Case-control Study, Qatar Medical Journal, doi:10.5339/qmj.2022.48.
Vásquez-Procopio et al., Association between 25-OH Vitamin D Deficiency and COVID-19 Severity in Pregnant Women, International Journal of Molecular Sciences, doi:10.3390/ijms232315188.
Tallon et al., Impact of diabetes status and related factors on COVID-19-associated hospitalization: A nationwide retrospective cohort study of 116,370 adults with SARS-CoV-2 infection, Diabetes Research and Clinical Practice, doi:10.1016/j.diabres.2022.110156.
Guldemir (B) et al., Clinical characteristics of bus drivers and field officers infected with COVID-19: A cross-sectional study from Istanbul, Work, doi:10.3233/wor-220292.
Sharif et al., Impact of Zinc, Vitamins C and D on Disease Prognosis among Patients with COVID-19 in Bangladesh: A Cross-Sectional Study, Nutrients, doi:10.3390/nu14235029.
Gibbons et al., Association between vitamin D supplementation and COVID-19 infection and mortality, Scientific Reports, doi:10.1038/s41598-022-24053-4.
Álvarez et al., Vitamin D deficiency and SARS-CoV-2 infection: Big-data analysis from March 2020 to March 2021. D-COVID study, bioRxiv, doi:10.1101/2022.10.27.514012.
Charla et al., Is suboptimal circulating level of vitamin D a risk factor for the poor prognosis of COVID-19? – A comparison of first and second waves in India, Research Square, doi:10.21203/rs.3.rs-1826271/v1.
Karimpour-Razkenari et al., Evaluating the Effects of Clinical Characteristics and Therapeutic Regimens on Mortality in Hospitalized Patients with Severe COVID-19, Journal of Pharmaceutical Care, doi:10.18502/jpc.v10i3.10790.
Hafez (B) et al., Factors Influencing Disease Stability and Response to Tocilizumab Therapy in Severe COVID-19: A Retrospective Cohort Study, Antibiotics, doi:10.3390/antibiotics11081078.
Aldwihi et al., Patients’ Behavior Regarding Dietary or Herbal Supplements before and during COVID-19 in Saudi Arabia, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph18105086.
Doğan (B) et al., The Clinical Significance of Vitamin D and Zinc Levels with Respect to Immune Response in COVID-19 Positive Children, Journal of Tropical Pediatrics, doi:10.1093/tropej/fmac072.
Reyes Pérez et al., Deficiency of vitamin D is a risk factor of mortality in patients with COVID-19, Revista de Sanidad Militar, doi:10.35366/93773.
Kalichuran et al., Vitamin D status and COVID-19 severity, Southern African Journal of Infectious Diseases, doi:10.4102/sajid.v37i1.359.
Dana et al., Vitamin D Level in Laboratory Confirmed COVID-19 and Disease Progression, The Eurasian Journal of Medicine, doi:10.5152/eurasianjmed.2022.21088.
Barrett et al., Vitamin D Status and Mortality from SARS CoV-2: A Prospective Study of Unvaccinated Caucasian Adults, Nutrients, doi:10.3390/nu14163252.
Bogliolo et al., Vitamin D 25OH Deficiency and Mortality in Moderate to Severe COVID-19: A Multi-Center Prospective Observational Study, Frontiers in Nutrition, doi:10.3389/fnut.2022.934258.
Alzahrani (B) et al., The Association Between Vitamin D Serum Level and COVID-19 Patients’ Outcomes in a Tertiary Center in Saudi Arabia: A Retrospective Cohort Study, Cureus, doi:10.7759/cureus.26266.
Neves et al., Vitamin D deficiency predicts 30-day hospital mortality of adults with COVID-19, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2022.05.027.
Gholi et al., Vitamin D deficiency is associated with increased risk of delirium and mortality among critically Ill, elderly covid-19 patients, Complementary Therapies in Medicine, doi:10.1016/j.ctim.2022.102855.
Hunt et al., Medications Associated with Lower Mortality in a SARS-CoV-2 Positive Cohort of 26,508 Veterans, Journal of General Internal Medicine, doi:10.1007/s11606-022-07701-3.
Kazemi et al., Comparison of the cardiovascular system, clinical condition, and laboratory results in COVID-19 patients with and without vitamin D insufficiency, BMC Infectious Diseases, doi:10.1186/s12879-022-07438-8.
Ghanei et al., Low serum levels of zinc and 25-hydroxyvitmain D as potential risk factors for COVID-19 susceptibility: a pilot case-control study, European Journal of Clinical Nutrition, doi:10.1038/s41430-022-01095-5.
Fiore et al., Effectiveness of Vitamin D Supplements among Patients Hospitalized for COVID-19: Results from a Monocentric Matched-Cohort Study, Healthcare, doi:10.3390/healthcare10050956.
Jabeen et al., Protective Effect of Vitamin-D Supplementation in Patients of Acute Coronary Syndrome During COVID-19 Pandemic, Pakistan Journal of Medical and Health Sciences, doi:10.53350/pjmhs221631053.
Ozturk et al., Is there a relationship between vitamin D levels, inflammatory parameters, and clinical severity of COVID-19 infection?, Bratislava Medical Journal, doi:10.4149/BLL_2022_065.
Charkowick et al., Vitamin D Deficiency and Thrombosis in Hospitalized SARS-CoV-2 Patients with Suspected Pulmonary Embolism, AJRCCM Conference, 205:A4571, www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2022.205.1_MeetingAbstracts.A4571.
Nguyen et al., 25-hydroxyvitamin D is a predictor of COVID-19 severity of hospitalized patients, PLOS ONE, doi:10.1371/journal.pone.0268038.
Voelkle et al., Prevalence of Micronutrient Deficiencies in Patients Hospitalized with COVID-19: An Observational Cohort Study, Nutrients, doi:10.3390/nu14091862.
Davoudi et al., Lack of association between vitamin D insufficiency and clinical outcomes of patients with COVID-19 infection, BMC Infectious Diseases, doi:10.1186/s12879-021-06168-7.
Parant et al., Vitamin D and COVID-19 Severity in Hospitalized Older Patients: Potential Benefit of Prehospital Vitamin D Supplementation, Nutrients, doi:10.3390/nu14081641.
Martínez-Rodríguez et al., Evaluation of the usefulness of vitamin D as a predictor of mortality in patients with COVID-19, Gaceta Médica de México, doi:10.24875/GMM.M22000637.
Ferrer-Sánchez et al., Serum 25(OH) Vitamin D Levels in Pregnant Women with Coronavirus Disease 2019 (COVID-19): A Case-Control Study, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph19073965.
Ramos et al., Vitamin D, Zinc and Iron in Adult Patients with Covid-19 and Their Action in the Immune Response as Biomarkers, Global Journal of Health Science, doi:10.5539/gjhs.v14n1p1.
Pande et al., Vitamin D Levels and its Association with Inflammatory Markers, Severity and Outcome in Hospitalised COVID-19 Patients - An Indian Perspective, Journal of Communicable Diseases, doi:10.24321/0019.5138.202227.
Bushnaq et al., The Impact of Vitamin D Status on COVID-19 Severity among Hospitalized Patients in the Western Region of Saudi Arabia: A Retrospective Cross-Sectional Study, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph19031901.
Rodríguez-Vidales et al., Severe COVID-19 patients have severe vitamin D deficiency in Northeast Mexico, Nutrición Hospitalaria, doi:10.20960/nh.03731.
Reis et al., Influence of vitamin D status on hospital length of stay and prognosis in hospitalized patients with moderate to severe COVID-19: a multicenter prospective cohort study, The American Journal of Clinical Nutrition, doi:10.1093/ajcn/nqab151.
Nimer et al., The impact of vitamin and mineral supplements usage prior to COVID-19 infection on disease severity and hospitalization, Bosnian Journal of Basic Medical Sciences, doi:10.17305/bjbms.2021.7009.
Karonova (C) et al., Vitamin D Status and Immune Response in Hospitalized Patients with Moderate and Severe COVID-19, Pharmaceuticals, doi:10.3390/ph15030305.
Zidrou et al., The Relationship Between Vitamin D Status and the Clinical Severity of COVID-19 Infection: A Retrospective Single-Center Analysis, Cureus, doi:10.7759/cureus.22385.
Sanson et al., A combined role for low vitamin D and low albumin circulating levels as strong predictors of worse outcome in COVID-19 patients, Irish Journal of Medical Science (1971 -), doi:10.1007/s11845-022-02952-9.
González-Estevez et al., Association of Food Intake Quality with Vitamin D in SARS-CoV-2 Positive Patients from Mexico: A Cross-Sectional Study, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph18147266.
Vanegas-Cedillo et al., Serum Vitamin D Levels Are Associated With Increased COVID-19 Severity and Mortality Independent of Whole-Body and Visceral Adiposity, medRxiv, doi:10.1101/2021.03.12.21253490.
Bychinin (B) et al., Prevalence of hypovitaminosis D in COVID-19 patients in the intensive care unit, Journal of Clinical Practice, doi:10.17816/clinpract64976.
Subramanian et al., Vitamin D, D-binding protein, free vitamin D and COVID-19 mortality in hospitalized patients, The American Journal of Clinical Nutrition, doi:10.1093/ajcn/nqac027.
Tylicki et al., Predictors of Mortality in Hemodialyzed Patients after SARS-CoV-2 Infection, Journal of Clinical Medicine, doi:10.3390/jcm11020285.
Ahmed (B) et al., Causal Inference and COVID-19 Nursing Home Patients: Identifying Factors That Reduced Mortality Risk, medRxiv, doi:10.1101/2021.11.18.21266489.
Dror et al., Pre-infection 25-hydroxyvitamin D3 levels and association with severity of COVID-19 illness, PLOS ONE, doi:10.1371/journal.pone.0263069.
Ansari et al., Frequency of Severe Vitamin D Deficiency and its Association with Mortality in Patients with Corona virus Disease, Pakistan J. Med. Heal. Sci., 14:4, pjmhsonline.com/2020/oct_dec/1206.pdf.
Anjum et al., Examine the association between severe vitamin D deficiency and mortality in patients with Covid-19, Pakistan J. Med. Heal. Sci., 14:3, pjmhsonline.com/2020/july-sep/1184.pdf.
Saponaro et al., Is There a Crucial Link Between Vitamin D Status and Inflammatory Response in Patients With COVID-19?, Frontiers in Immunology, doi:10.3389/fimmu.2021.745713.
Smaha et al., COVID-19 pneumonia patients with 25(OH)D levels lower than 12 ng/ml are at increased risk of death, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2022.01.044.
Baguma et al., Characteristics of the COVID-19 patients treated at Gulu Regional Referral Hospital, Northern Uganda: A cross-sectional study, Research Square, doi:10.21203/rs.3.rs-1193578/v1.
Israel et al., Vitamin D deficiency is associated with higher risks for SARS-CoV-2 infection and COVID-19 severity: a retrospective case–control study, Internal and Emergency Medicine, doi:10.1007/s11739-021-02902-w.
Seal et al., Association of Vitamin D Status and COVID-19-Related Hospitalization and Mortality, Journal of General Internal Medicine, doi:10.1007/s11606-021-07170-0.
Pepkowitz et al., Vitamin D Deficiency is Associated with Increased COVID-19 Severity: Prospective Screening of At-Risk Groups is Medically Indicated, Research Square, doi:10.21203/rs.3.rs-83262/v1.
Efird et al., The Interaction of Vitamin D and Corticosteroids: A Mortality Analysis of 26,508 Veterans Who Tested Positive for SARS-CoV-2, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph19010447.
Sainz-Amo et al., COVID-19 in Parkinson’s disease: what holds the key?, Journal of Neurology, doi:10.1007/s00415-020-10272-0.
Galaznik et al., Assessment of vitamin D deficiency and COVID-19 diagnosis in patients with breast or prostate cancer using electronic medical records, Journal of Clinical Oncology, doi:10.1200/JCO.2021.39.15_suppl.6589.
Seven et al., Correlation between 25-hydroxy vitamin D levels and COVID-19 severity in pregnant women: a cross-sectional study, The Journal of Maternal-Fetal & Neonatal Medicine, doi:10.1080/14767058.2021.2005564.
Parra-Ortega et al., 25-Hydroxyvitamin D level is associated with mortality in patients with critical COVID-19: a prospective observational study in Mexico City, Nutrition Research and Practice, doi:10.4162/nrp.2021.15.S1.S32.
Putra et al., Vitamin D Levels among Hospitalized and Non-Hospitalized COVID-19 Patients in Dr. M. Djamil General Hospital Padang, European Journal of Medical and Health Sciences, doi:10.24018/ejmed.2021.3.6.1131.
Ma et al., Associations between predicted vitamin D status, vitamin D intake, and risk of SARS-CoV-2 infection and Coronavirus Disease 2019 severity, The American Journal of Clinical Nutrition, doi:10.1093/ajcn/nqab389.
Asgari et al., Vitamin D Insufficiency in Disease Severity and Prognosis of the Patients With SARS Corona Virus-2 Infection, Acta Medica Iranica, doi:10.18502/acta.v59i11.7779.
Loucera et al., Real world evidence of calcifediol or vitamin D prescription and mortality rate of COVID-19 in a retrospective cohort of hospitalized Andalusian patients, Scientific Reports, doi:10.1038/s41598-021-02701-5.
Fatemi et al., Association of vitamin D deficiency with COVID-19 severity and mortality in Iranian people: a prospective observational study, Acute and Critical Care, doi:10.4266/acc.2021.00605.
Kaur et al., Correlation of Vitamin D Levels with COVID-19 Severity and Outcome, Indian Journal of Clinical Practice, 32:6, ijcp.in/Admin/CMS/PDF/7.%20ClinicalStudy_2IJCP_Nov2021.pdf.
Gönen et al., Rapid and Effective Vitamin D Supplementation May Present Better Clinical Outcomes in COVID-19 (SARS-CoV-2) Patients by Altering Serum INOS1, IL1B, IFNg, Cathelicidin-LL37, and ICAM1, Nutrients, doi:10.3390/nu13114047.
Asghar et al., Evaluation of Vitamin-D Status and Its Association with Clinical Outcomes Among COVID-19 Patients in Pakistan, Am. J. Trop. Med. Hyg., doi:10.4269/ajtmh.21-0577.
Atanasovska et al., Vitamin D levels and oxidative stress markers in patients hospitalized with COVID-19, Redox Report
, doi:10.1080/13510002.2021.1999126.
Eden et al., Nutritional parameters and outcomes in patients admitted to intensive care with COVID-19: a retrospective single-centre service evaluation, BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000270.
Al-Salman et al., In COVID-19 patients, low 25-hydroxyvitamin D level in serum is associated with longer viral clearance time and higher risk of intensive care unit admission, Nutrition & Food Science, doi:10.1108/NFS-05-2021-0143.
Golabi et al., The Association between Vitamin D and Zinc Status and the Progression of Clinical Symptoms among Outpatients Infected with SARS-CoV-2 and Potentially Non-Infected Participants: A Cross-Sectional Study, Nutrients, doi:10.3390/nu13103368.
Bianconi et al., Prevalence of vitamin D deficiency and its prognostic impact on patients hospitalized with COVID-19, Nutrition, doi:10.1016/j.nut.2021.111408.
Gaudio et al., Vitamin D Levels Are Reduced at the Time of Hospital Admission in Sicilian SARS-CoV-2-Positive Patients, International Journal of Environmental Research and Public Health, doi:10.3390/ijerph18073491.
Hurst et al., Vitamin D insufficiency in COVID-19 and influenza A, and critical illness survivors: a cross-sectional study, BMJ Open, doi:10.1136/bmjopen-2021-055435.
Jimenez et al., Mortality in Hemodialysis Patients with COVID-19, the Effect of Paricalcitol or Calcimimetics, Nutrients, doi:10.3390/nu13082559.
Zelzer et al., Vitamin D Metabolites and Clinical Outcome in Hospitalized COVID-19 Patients, Nutrients, doi:10.3390/nu13072129.
Sinaci et al., Impact of vitamin D on the course of COVID-19 during pregnancy: A case control study, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2021.105964.
Basaran et al., The relationship between vitamin D and the severity of COVID-19, Bratislava Medical Journal, doi:10.4149/bll_2021_034.
Dudley et al., Revisiting vitamin D status and supplementation for in-patients with intellectual and developmental disability in the North of England, UK, BJPsych Bulletin, doi:10.1192/bjb.2021.55.
Ramirez-Sandoval et al., Very Low Vitamin D Levels are a Strong Independent Predictor of Mortality in Hospitalized Patients with Severe COVID-19, Archives of Medical Research, doi:10.1016/j.arcmed.2021.09.006.
Burahee et al., Older patients with proximal femur fractures and SARS-CoV-2 infection – An observational study, SICOT-J, doi:10.1051/sicotj/2021001.
Arroyo-Díaz et al., Previous Vitamin D Supplementation and Morbidity and Mortality Outcomes in People Hospitalised for COVID19: A Cross-Sectional Study, Frontiers in Public Health, doi:10.3389/fpubh.2021.758347.
Yildiz et al., The prognostic significance of vitamin D deficiency in patients with COVID-19 pneumonia, Bratislava Medical Journal, doi:10.4149/BLL_2021_119.
Derakhshanian et al., The predictive power of serum vitamin D for poor outcomes in COVID-19 patients, Food Science & Nutrition, doi:10.1002/fsn3.2591.
Bagheri et al., Supplement Usage Pattern in a Group of COVID-19 Patients in Tehran, Journal of Family & Reproductive Health, doi:10.18502/jfrh.v14i3.4668.
Ribeiro et al., Previous vitamin D status and total cholesterol are associated with SARS-CoV-2 infection, Clinica Chimica Acta, doi:10.1016/j.cca.2021.08.003.
Vasheghani et al., The relationship between serum 25-hydroxyvitamin D levels and the severity of COVID-19 disease and its mortality, Scientific Reports, doi:10.1038/s41598-021-97017-9.
Tomasa-Irriguible et al., Low Levels of Few Micronutrients May Impact COVID-19 Disease Progression: An Observational Study on the First Wave, Metabolites, doi:10.3390/metabo11090565.
Karonova (D) et al., Low 25(OH)D Level Is Associated with Severe Course and Poor Prognosis in COVID-19, Nutrients, doi:10.3390/nu13093021.
Jain (B) et al., Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers, Nature, doi:10.1038/s41598-020-77093-z.
Nimavat et al., Vitamin D deficiency and COVID-19: A case-control study at a tertiary care hospital in India, Annals of Medicine and Surgery, doi:10.1016/j.amsu.2021.102661.
di Filippo (D) et al., Vitamin D levels associate with blood glucose and BMI in COVID-19 patients predicting disease severity, The Journal of Clinical Endocrinology & Metabolism, doi:10.1210/clinem/dgab599.
Louca et al., Modest effects of dietary supplements during the COVID-19 pandemic: insights from 445 850 users of the COVID-19 Symptom Study app, BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000250.
Alpcan et al., Vitamin D levels in children with COVID-19: a report from Turkey, Epidemiology & Infection, doi:10.1017/S0950268821001825.
Matin et al., The sufficient vitamin D and albumin level have a protective effect on COVID-19 infection, Archives of Microbiology, doi:10.1007/s00203-021-02482-5.
Pimental et al., Low vitamin D levels and increased neutrophil in patients admitted at ICU with COVID-19, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2021.05.021.
Israel (B) et al., Identification of drugs associated with reduced severity of COVID-19: A case-control study in a large population, Epidemiology and Global Health Microbiology and Infectious Disease, doi:10.7554/eLife.68165.
Cozier et al., Lower serum 25(OH)D levels associated with higher risk of COVID-19 infection in U.S. Black women, PLoS ONE, doi:10.1371/journal.pone.0255132.
Orchard et al., Vitamin-D levels and intensive care unit outcomes of a cohort of critically ill COVID-19 patients, Clin Chem Lab Med, doi:10.1515/cclm-2020-1567.
Savitri et al., Comparison between Vitamin D Level of Asymptomatic Confirmed Covid-19 Patients with Symptomatic Confirmed Covid-19 Patients in Makassar, Annals of the Romanian Society for Cell Biology, 25:6, www.annalsofrscb.ro/index.php/journal/article/view/9130.
Oristrell et al., Vitamin D supplementation and COVID-19 risk: a population-based, cohort study, Journal of Endocrinological Investigation, doi:10.1007/s40618-021-01639-9.
Cereda et al., Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy, Nutrition, doi:10.1016/j.nut.2020.111055.
Jude et al., Vitamin D deficiency is associated with higher hospitalisation risk from COVID-19: a retrospective case-control study, Journal of Clinical Endocrinology & Metabolism, doi:10.1210/clinem/dgab439.
Levitus et al., The Effect of Vitamin D Supplementation on Severe COVID-19 Outcomes in Patients With Vitamin D Insufficiency, Journal of the Endocrine Society, doi: 10.1210/jendso/bvab048.567, academic.oup.com/jes/article/5/Supplement_1/A279/6240740.
Oristrell (B) et al., Association of Calcitriol Supplementation with Reduced COVID-19 Mortality in Patients with Chronic Kidney Disease: A Population-based Study, Biomedicines, doi:10.3390/biomedicines9050509.
Fasano et al., COVID-19 in Parkinson’s Disease Patients Living in Lombardy, Italy, Movement Disorders, doi:10.1002/mds.28176.
Nogués et al., Calcifediol Treatment and COVID-19-Related Outcomes, The Journal of Clinical Endocrinology & Metabolism, doi:10.1210/clinem/dgab405.
Diaz-Curiel et al., The relationship between 25(OH) vitamin D levels and COVID-19 onset and disease course in Spanish patients, Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2021.105928.
Alcala-Diaz et al., Calcifediol Treatment and Hospital Mortality Due to COVID-19: A Cohort Study, Nutrients, doi:10.3390/nu13061760.
Li (B) et al., Assessment of the Association of Vitamin D Level With SARS-CoV-2 Seropositivity Among Working-Age Adults, JAMA Network Open, doi:10.1001/jamanetworkopen.2021.11634.
AlSafar et al., COVID-19 Disease Severity and Death in Relation to Vitamin D Status among SARS-CoV-2-Positive UAE Residents, Nutrients, doi:10.3390/nu13051714.
Annweiler (B) et al., Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study, Nutrients, doi:10.3390/nu12113377.
Blanch-Rubió et al., Influence of anti-osteoporosis treatments on the incidence of COVID-19 in patients with non-inflammatory rheumatic conditions, Aging, doi:10.18632/aging.104117.
Lohia et al., Exploring the link between vitamin D and clinical outcomes in COVID-19, American Journal of Physiology-Endocrinology and Metabolism, doi:10.1152/ajpendo.00517.2020.
Barassi et al., Vitamin D in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) patients with non-invasive ventilation support, Panminerva Med., doi:10.23736/S0031-0808.21.04277-4.
Szeto et al., Vitamin D Status and COVID-19 Clinical Outcomes in Hospitalized Patients, Endocrine Research, doi:10.1080/07435800.2020.1867162.
Ünsal et al., Retrospective analysis of vitamin D status on ınflammatory markers and course of the disease in patients with COVID-19 infection, Journal of Endocrinological Investigation, doi:10.1007/s40618-021-01566-9.
Bayramoğlu et al., The association between vitamin D levels and the clinical severity and inflammation markers in pediatric COVID-19 patients: single-center experience from a pandemic hospital, European Journal of Pediatrics, doi:10.1007/s00431-021-04030-1.
Livingston et al., Detectable respiratory SARS-CoV-2 RNA is associated with low vitamin D levels and high social deprivation, Int. J. Clinical Practive, doi:10.1111/ijcp.14166.
Mendy et al., Factors Associated with Hospitalization and Disease Severity in a Racially and Ethnically Diverse Population of COVID-19 Patients, medRxiv, doi:10.1101/2020.06.25.20137323.
Macaya et al., Interaction between age and vitamin D deficiency in severe COVID-19 infection, Nutr. Hosp., doi:10.20960/nh.03193.
Im et al., Nutritional status of patients with COVID-19, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2020.08.018.
Freitas (B) et al., Vitamin D-related polymorphisms and vitamin D levels as risk biomarkers of COVID-19 infection severity, medRxiv, doi:10.1101/2021.03.22.21254032.
Meltzer (B) et al., Association of Vitamin D Levels, Race/Ethnicity, and Clinical Characteristics With COVID-19 Test Results, JAMA Netw Open., doi:10.1001/jamanetworkopen.2021.4117.
Cereda (B) et al., Vitamin D 25OH deficiency in COVID-19 patients admitted to a tertiary referral hospital, Clinical Nutrition (Edinburgh, Scotland), doi:10.1016/j.clnu.2020.10.055.
Charoenngam et al., Association of vitamin D status with hospital morbidity and mortality in adult hospitalized COVID-19 patients, Endocrine Practice, doi:10.1016/j.eprac.2021.02.013.
Mazziotti et al., Vitamin D deficiency, secondary hyperparathyroidism and respiratory insufficiency in hospitalized patients with COVID-19, Journal of Endocrinological Investigation, doi:10.1007/s40618-021-01535-2.
Ricci et al., Circulating Vitamin D levels status and clinical prognostic indices in COVID-19 patients, Respiratory Research, doi:10.1186/s12931-021-01666-3.
Sulli et al., Vitamin D and Lung Outcomes in Elderly COVID-19 Patients, Nutrients, doi:10.3390/nu13030717.
Gavioli et al., An Evaluation of Serum 25-Hydroxy Vitamin D Levels in Patients with COVID-19 in New York City, Journal of the American College of Nutrition, doi:10.1080/07315724.2020.1869626.
Infante et al., Low Vitamin D Status at Admission as a Risk Factor for Poor Survival in Hospitalized Patients With COVID-19: An Italian Retrospective Study, Journal of the American College of Nutrition, doi:10.1080/07315724.2021.1877580.
Angelidi et al., Vitamin D Status is Associated With In-hospital Mortality and Mechanical Ventilation: A Cohort of COVID-19 Hospitalized Patients, Mayo Clinic Proceedings, doi:10.1016/j.mayocp.2021.01.001.
Susianti et al., Low levels of vitamin D were associated with coagulopathy among hospitalized coronavirus disease-19 (COVID-19) patients: A single-centered study in Indonesia, Journal of Medical Biochemistry, doi:10.5937/jomb0-30228.
Karonova (E) et al., Serum 25(oH)D level in patients with CoVID-19, Infectology, doi:10.22625/2072-6732-2020-12-3-21-27.
Karahan et al., Impact of Serum 25(OH) Vitamin D Level on Mortality in Patients with COVID-19 in Turkey, J. Nutr. Health Aging
, doi:10.1007/s12603-020-1479-0.
Li (C) et al., Metabolic Healthy Obesity, Vitamin D Status, and Risk of COVID-19, Aging and Disease, doi:10.14336/AD.2020.1108.
Yılmaz et al., Is vitamin D deficiency a risk factor for COVID-19 in children?, Pediatric Pulmonology, doi:10.1002/ppul.25106.
Demir et al., Vitamin D deficiency is associated with COVID-19 positivity and the severity of the disease, Journal of Medical Virology, doi:10.1002/jmv.26832.
Ma (B) et al., Habitual use of vitamin D supplements and risk of coronavirus disease 2019 (COVID-19) infection: a prospective study in UK Biobank, The American Journal of Clinical Nutrition, doi:10.1093/ajcn/nqaa381.
Giannini et al., Effectiveness of In-Hospital Cholecalciferol Use on Clinical Outcomes in Comorbid COVID-19 Patients: A Hypothesis-Generating Study, Nutrients
, doi:10.3390/nu13010219.
Bennouar et al., Vitamin D Deficiency and Low Serum Calcium as Predictors of Poor Prognosis in Patients with Severe COVID-19, Journal of the American College of Nutrition, doi:10.1080/07315724.2020.1856013.
Amin et al., No evidence that vitamin D is able to prevent or affect the severity of COVID-19 in individuals with European ancestry: a Mendelian randomisation study of open data, BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2020-000151.
Jevalikar et al., Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID-19, Scientific Reports, doi:10.1038/s41598-021-85809-y.
Cangiano et al., Mortality in an Italian nursing home during COVID-19 pandemic: correlation with gender, age, ADL, vitamin D supplementation, and limitations of the diagnostic tests, Aging, doi:10.18632/aging.202307.
Mateja et al., The choice of viral load endpoint in early phase trials of COVID-19 treatments aiming to reduce 28-day hospitalization and/or death, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf282.
Zhang (B) et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Sweeting et al., What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data, Statistics in Medicine, doi:10.1002/sim.1761.
Altman (C) et al., Interaction revisited: the difference between two estimates, BMJ, doi:10.1136/bmj.326.7382.219.
Michelucci et al., SARS-CoV-2 ORF3a accessory protein is a water-permeable channel that induces lysosome swelling, Communications Biology, doi:10.1038/s42003-024-07442-5.
Ghosh et al., β-Coronaviruses Use Lysosomes for Egress Instead of the Biosynthetic Secretory Pathway, Cell, doi:10.1016/j.cell.2020.10.039.
Kamga Kapchoup et al., In vitro effect of hydroxychloroquine on pluripotent stem cells and their cardiomyocytes derivatives, Frontiers in Pharmacology, doi:10.3389/fphar.2023.1128382.
Bobrowski et al., Synergistic and Antagonistic Drug Combinations against SARS-CoV-2, Molecular Therapy, doi:10.1016/j.ymthe.2020.12.016.
Peters (B) et al., Outcomes of Persons With COVID-19 in Hospitals With and Without Standard Treatment With (Hydroxy)chloroquine, Clinical Microbiology and Infection, doi:10.1016/j.cmi.2020.10.004.
Mahévas et al., Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data, BMJ 2020, doi:10.1136/bmj.m1844.
Minozzi et al., The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2020.06.015.
Popp et al., Ivermectin for preventing and treating COVID-19, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.CD015017.pub3.
Reis (B) et al., Effect of Early Treatment with Ivermectin among Patients with Covid-19, New England Journal of Medicine, doi:10.1056/NEJMoa2115869.
Axfors et al., Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative meta-analysis of randomized trials, Nature, doi:10.1038/s41467-021-22446-z.
Horby et al., Effect of Hydroxychloroquine in Hospitalized Patients with COVID-19: Preliminary results from a multi-centre, randomized, controlled trial, NEJM, doi:10.1056/NEJMoa2022926.
Hempenius et al., Bias in observational studies on the effectiveness of in hospital use of hydroxychloroquine in COVID-19, Pharmacoepidemiology and Drug Safety, doi:10.1002/pds.5632.
Abdollahi et al., The Association Between the Level of Serum 25(OH) Vitamin D, Obesity, and underlying Diseases with the risk of Developing COVID-19 Infection: A case-control study of hospitalized patients in Tehran, Iran, Journal of Medical Virology, doi:10.1002/jmv.26726.
Abdulrahman et al., Correlates of poor clinical outcomes related to COVID-19 among older people with psychiatric illness - a mixed methods study, The International Journal of Psychiatry in Medicine, doi:10.1177/00912174231171220.
Abrishami et al., Possible association of vitamin D status with lung involvement and outcome in patients with COVID-19: a retrospective study, European Journal of Nutrition, doi:10.1007/s00394-020-02411-0.
Afaghi et al., Prevalence and Clinical Outcomes of Vitamin D Deficiency in COVID-19 Hospitalized Patients: A Retrospective Single-Center Analysis, The Tohoku Journal of Experimental Medicine, doi:10.1620/tjem.255.127.
Al-Jarallah et al., In‐hospital mortality in SARS‐CoV‐2 stratified by serum 25‐hydroxy‐vitamin D levels: A retrospective study, Journal of Medical Virology, doi:10.1002/jmv.27133.
Alguwaihes et al., Diabetes and Covid-19 among hospitalized patients in Saudi Arabia: a single-centre retrospective study, Cardiovascular Diabetology, doi:10.1186/s12933-020-01184-4.
Baktash et al., Vitamin D status and outcomes for hospitalised older patients with COVID-19, Postgraduate Medical Journal, doi:10.1136/postgradmedj-2020-138712.
Begum (B) et al., Prevalence and risk factors for post-COVID-19 syndrome on medical students in Tabuk, Saudi Arabia-2023-2024, Journal of Family Medicine and Primary Care, doi:10.4103/jfmpc.jfmpc_2017_24.
Breslin et al., The relationship between vitamin D, biomarkers and clinical outcome in hospitalised Covid-19 patients, Proceedings of the Nutrition Society, doi:10.1017/S0029665121002214.
Carpagnano et al., Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19, J. Endocrinol. Invest., 2020, Aug 9, 1-7, doi:10.1007/s40618-020-01370-x.
Chang et al., Prior diagnoses and medications as risk factors for COVID-19 in a Los Angeles Health System, medRxiv, doi:10.1101/2020.07.03.20145581.
De Smet et al., Serum 25(OH)D Level on Hospital Admission Associated With COVID-19 Stage and Mortality, American Journal of Clinical Pathology, doi:10.1093/ajcp/aqaa252.
Faniyi et al., Vitamin D status and seroconversion for COVID-19 in UK healthcare workers who isolated for COVID-19 like symptoms during the 2020 pandemic, medRxiv, doi:10.1101/2020.10.05.20206706.
Faul et al., Vitamin D Deficiency and ARDS after SARS-CoV-2 Infection, Irish Medical Journal, 113:5, 84, imj.ie/vitamin-d-deficiency-and-ards-after-sars-cov-2-infection/.
Green et al., A higher frequency of physical activity is associated with reduced rates of SARS-CoV-2 infection, European Journal of General Practice, doi:10.1080/13814788.2022.2138855.
Hastie et al., Vitamin D concentrations and COVID-19 infection in UK Biobank, Diabetes and Metabolic Syndrome: Clinical Research and Reviews, 14:4, 561–565, doi:10.1016/j.dsx.2020.04.050.
Hernández et al., Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection, The Journal of Clinical Endocrinology & Metabolism, doi:10.1210/clinem/dgaa733.
Katz et al., Increased risk for Covid-19 in patients with Vitamin D deficiency, Nutrition, doi:10.1016/j.nut.2020.111106.
Kaufman et al., SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels, PLOS One, doi:10.1371/journal.pone.0239252.
Lau et al., Vitamin D Insufficiency is Prevalent in Severe COVID-19, medRxiv, doi:10.1101/2020.04.24.20075838.
Luo et al., Vitamin D Deficiency Is Associated with COVID-19 Incidence and Disease Severity in Chinese People, The Journal of Nutrition, doi:10.1093/jn/nxaa332.
Matangkha et al., Association Between Vitamin D Levels and Long COVID Signs and Symptoms, Medical Sciences, doi:10.3390/medsci13030199.
Meltzer (C) et al., Association of Vitamin D Status and Other Clinical Characteristics With COVID-19 Test Results, JAMA network open, 3:9, doi:10.1001/jamanetworkopen.2020.19722.
Merzon et al., Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: an Israeli population-based study, The FEBS Journal, doi:10.1111/febs.15495.
Panagiotou et al., Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalised with COVID-19 are associated with greater disease severity: results of a local audit of practice, medRxiv, doi:10.1101/2020.06.21.20136903.
Radujkovic et al., Vitamin D Deficiency and Outcome of COVID-19 Patients, Nutrients 2020, 12:9, 2757, doi:10.3390/nu12092757.
Sheng et al., Association between vitamin D and COVID-19 infection and mortality in Taiwanese patients, Journal of the Chinese Medical Association, doi:10.1097/JCMA.0000000000001294.
Sulli (B) et al., Vitamin D and Lung Outcomes in Elderly COVID-19 Patients, Nutrients, doi:10.3390/nu13030717.
Sánchez-Zuno (B), Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation, Journal of Clinical Medicine, doi:10.3390/jcm10112378.
Tehrani et al., Evaluation of vitamin D levels in COVID-19 patients referred to Labafinejad hospital in Tehran and its relationship with disease severity and mortality, Clinical Nutrition, doi:10.1016/j.clnesp.2021.01.014.
Umay et al., Comparison of Length of Hospital Stay and Routine Laboratory Parameters in Covid-19 Patients With and Without Serum Vitamin D Deficiency, Journal of Contemporary Medicine, doi:10.16899/jcm.1319088.
Vasheghani (B) et al., The relationship between serum 25-hydroxyvitamin D levels and the severity of COVID-19 disease and its mortality, Scientific Reports, doi:10.1038/s41598-021-97017-9.
Vassiliou (B) et al., Low 25-Hydroxyvitamin D Levels on Admission to the Intensive Care Unit May Predispose COVID-19 Pneumonia Patients to a Higher 28-Day Mortality Risk: A Pilot Study on a Greek ICU Cohort, Nutrients, doi:10.3390/nu12123773.
Walk et al., Vitamin D - contrary to vitamin K - does not associate with clinical outcome in hospitalized COVID-19 patients, medRxiv, doi:10.1101/2020.11.07.20227512.
Ye et al., Does Serum Vitamin D Level Affect COVID-19 Infection and Its Severity? A Case-Control Study, Journal of the American College of Nutrition, doi:10.1080/07315724.2020.182600.
Annweiler (C) et al., Vitamin D and survival in COVID-19 patients: A quasi-experimental study, The Journal of Steroid Biochemistry and Molecular Biology, doi:10.1016/j.jsbmb.2020.105771.
Boukef et al., Melatonin, Vitamins and Minerals Supplements for the Treatment of Covid-19 and Covid-like Illness: Results of a Prospective, Randomised, Double-blinded Multicentre Study, NCT05670444, clinicaltrials.gov/study/NCT05670444.
Baguma (B) et al., Characteristics of the COVID-19 patients treated at Gulu Regional Referral Hospital, Northern Uganda: A cross-sectional study, Research Square, doi:10.21203/rs.3.rs-1193578/v1.
Ling et al., High-Dose Cholecalciferol Booster Therapy is Associated with a Reduced Risk of Mortality in Patients with COVID-19: A Cross-Sectional Multi-Centre Observational Study, Nutrients, doi:10.3390/nu12123799.
Lohia (B) et al., Exploring the link between vitamin D and clinical outcomes in COVID-19, American Journal of Physiology-Endocrinology and Metabolism, doi:10.1152/ajpendo.00517.2020.
Tan (B) et al., Cohort study to evaluate the effect of combination Vitamin D, Magnesium and Vitamin B12 (DMB) on progression to severe outcome in older COVID-19 patients, Nutrition, doi:10.1016/j.nut.2020.111017.
Annweiler (D) et al., Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study, Nutrients, doi:10.3390/nu12113377.
Bhat et al., Effect of calcifediol supplementation as add-on therapy on the immune repertoire in recipients of the ChAdOx1 nCoV-19 vaccine: A prospective open-label, placebo-controlled, clinical trial, Journal of Infection, doi:10.1016/j.jinf.2023.03.004.
Golabi (B) et al., The Association between Vitamin D and Zinc Status and the Progression of Clinical Symptoms among Outpatients Infected with SARS-CoV-2 and Potentially Non-Infected Participants: A Cross-Sectional Study, Nutrients, doi:10.3390/nu13103368.
Hernández (B) et al., Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection, The Journal of Clinical Endocrinology & Metabolism, doi:10.1210/clinem/dgaa733.
Levy et al., Frail Older Adults with Presymptomatic SARS-CoV-2 Infection: Clinical Course and Prognosis, Gerontology, doi:10.1159/000521412.