Effect of Early Treatment with Ivermectin among Patients with Covid-19
et al., New England Journal of Medicine, doi:10.1056/NEJMoa2115869 (results released 8/6/2021), TOGETHER, NCT04727424, Aug 2021
{kind=link}
Extreme COI, impossible data, blinding broken, randomization/blinding failure, uncorrected errors, protocol violations, no response from authors, refusal to release data
See also
Many major issues including multiple impossible numbers,
randomization failure, blinding broken (even externally), protocol violations, refusal to
release the data, and many more serious issues as detailed below.
The metformin arm has been retracted due to impossible data and
compromised integrity1. The ivermectin arm has far more serious issues,
however neither the journal nor the authors respond.
Private comments:
"There is a clear signal that IVM works in COVID patients..
that would be significant if more patients were added..
you will hear me retract previous statements where I had been previously negative"
— Ed Mills, Together Trial co-principal investigator2.
Public comments:
“There was no indication that ivermectin is clinically useful”
—
Ed Mills, Together Trial co-principal investigator.
| Author responses | |
| 83. modified without explanation | |
| No response for all other items | |
CRITICALPatient counts for reported period impossible.
Authors claim the ivermectin and control patients were all from on or after March 23, 2021, however independent analyses of the enrollment graph (contained in this presentation31) require including patients prior to this date to reach the reported numbers20,32. The enrollment graph shows much higher enrollment to ivermectin near the start of the trial. The only way that the number of placebo patients can be the same as the number of treatment patients is if placebo patients were taken from an earlier period29,33, which creates a nonconcurrent control group34 and substantial confounding by time as below.
CRITICALPlacebo counts vs. fluvoxamine not possible.
The IVM placebo arm has 679 patients and the FLV arm has 756. The 679 should be shared between the arms, with 77 extra patients for FLV. For FLV, there were 34 placebo patients requiring mechanical ventilation, for IVM there was only 25, indicating that 9 of the extra 77 placebo patients for FLV had mechanical ventilation, a much higher percentage during a period that had lower deaths and CFR (and included vaccinated patients). Placebo all-cause hospitalization shows 95/679 for IVM and 99/756 for FLV, i.e., only 4 of the extra 77 patients were hospitalized, but the paper reports an additional 9 patients with mechanical ventilation.
CRITICALImpossible baseline data.
Analysis of baseline data by Marinos shows conflicting data and points to data being changed to hide randomization failure and incomparable groups. For details see35.
CRITICALMetformin arm retracted for incorrect data and compromised integrity.
The metformin arm has been retracted due to impossible data and compromised integrity1. The ivermectin arm has far more serious issues, however neither the journal nor the authors respond (the metformin arm was published in a different journal).
CRITICALRandomization violation, significant confounding by time.
Unequal randomization, significant confounding by time. The trial reports 1:1:1:1 randomization, however independent analysis shows much higher enrollment in the ivermectin treatment arm towards the start of the trial20,36. This introduces very significant confounding by time due to the major change in the distribution of variants. Zavascki show dramatically higher mortality for Gamma vs non-Gamma variants (28 day mortality from symptom onset aHR 4.73 [1.15-19.41]). Many more patients were randomized to ivermectin vs. placebo in the first few weeks, for example the first week shows 82 ivermectin vs. 28 placebo patients, 2.9x higher. The period of excess ivermectin enrollment coincides closely with a period of significantly higher deaths and CFR in Brazil.
CRITICALBlinding broken.
Leaked documents show that blinding was broken, with interim results available not only within the team, but shared externally with a group of 90+ people, many from other ivermectin trials, in meetings organized by Dr. Andrew Hill. Unreleased leaked emails also indicate sharing with higher-up individuals at the NIH. As below, protocol changes were made mid-trial to add additional bias against ivermectin37.
CRITICALBlinding failure.
Ivermectin/placebo blinding was done by assigning a letter to each group that was only known to the pharmacist. If a patient received a 3-dose treatment, investigators immediately know that the patient is more likely to be in the treatment group than the control group, because 3-dose placebo was relatively rare (~46% from PP). If a patient received non-3-day treatment, investigators immediately know that the patient is not an ivermectin treatment patient. Moreover, by observing the frequency of allocations, investigators can easily determine which letter corresponds to active ivermectin 3-day treatment, thereby removing all blinding. For example, consider 3-dose-ivermectin and 3-dose-placebo being identified by the letters G and K. If allocations to date have been G:11 and K:20, there is a very high probability that K is ivermectin. Note that this blinding failure is only obvious because the journal required the authors to restrict to the 3-day placebo group. Also note that it would have been trivial to avoid if desired, for example by using a unique identifier for all medication bottles. Note that there may be additional reasons for blinding failure, for example the paper specifies identically shaped bottles, but does not appear to specify identical appearance tablets38, and patients receiving a placebo injection.
CRITICALData pledge violation, unavailable over 1,700 days from protocol, over 1,500 days from publication.
The trial registration states that data was to be available at termination and upon request39, however authors have not responded to a request for the data. Even funders of the trial have been unable to access the data40. Requests can be sent to thetogethertrial@gmail.com, let us know the outcome. For a detailed timeline of requests and the denial to release data see41 (appendix A).
CRITICALDSMC not independent.
Reviewer 1 of the protocol notes that the DSMC is not independent42. Prof. Thorlund is Vice President of the contract research organisation (CRO, Cytel), professor at the sponsoring university, and an author of the protocol. Dr. Häggström is an employee of the CRO. doyourownresearch.substack.com (B), twitter.com (D) reveals many other conflicts. Prof. Thorlund has written >100 papers with Prof. Mills. Prof. Singh has written 29 papers with Prof. Mills. Prof. Orbinski has written 9 papers with Prof. Mills. The first version of the web site showed Prof. Mills and Prof. Thorlund as joint leads. Emails pointed to a company MTEK Sciences, founded by Prof. Mills and Prof. Thorlund (MTEK is hypothesized to stand for Mills, Thorlund, Edward, Kristian). MTEK received grants from the Gates Foundation. MTEK also employed Dr. Häggström. MTEK was acquired by Cytel in 2019. Dr. Häggström works for the Gates Foundation. Two members of the DSMC have published a paper with members of a well known anti-ivermectin research group44 and Dr. Hill, whose meta analysis has reports of external influence45-47. The trial protocol reports that "an independent DSMC will be established, composed of scientists of unrivalled reputation and expertise, without involvement with this research protocol."
CRITICALExtreme conflicts of interest.
Disclosed conflicts of interest include: Pfizer, Merck, Bill & Melinda Gates Foundation, Australian Government, Medicines Development for Global Health, Novaquest, Regeneron, Astrazeneca, Daichi Sankyo, Commonwealth Science and Research Organization, and Card Research. Many conflicts of interest appear unreported. For example, Unitaid is a sponsor48,49.
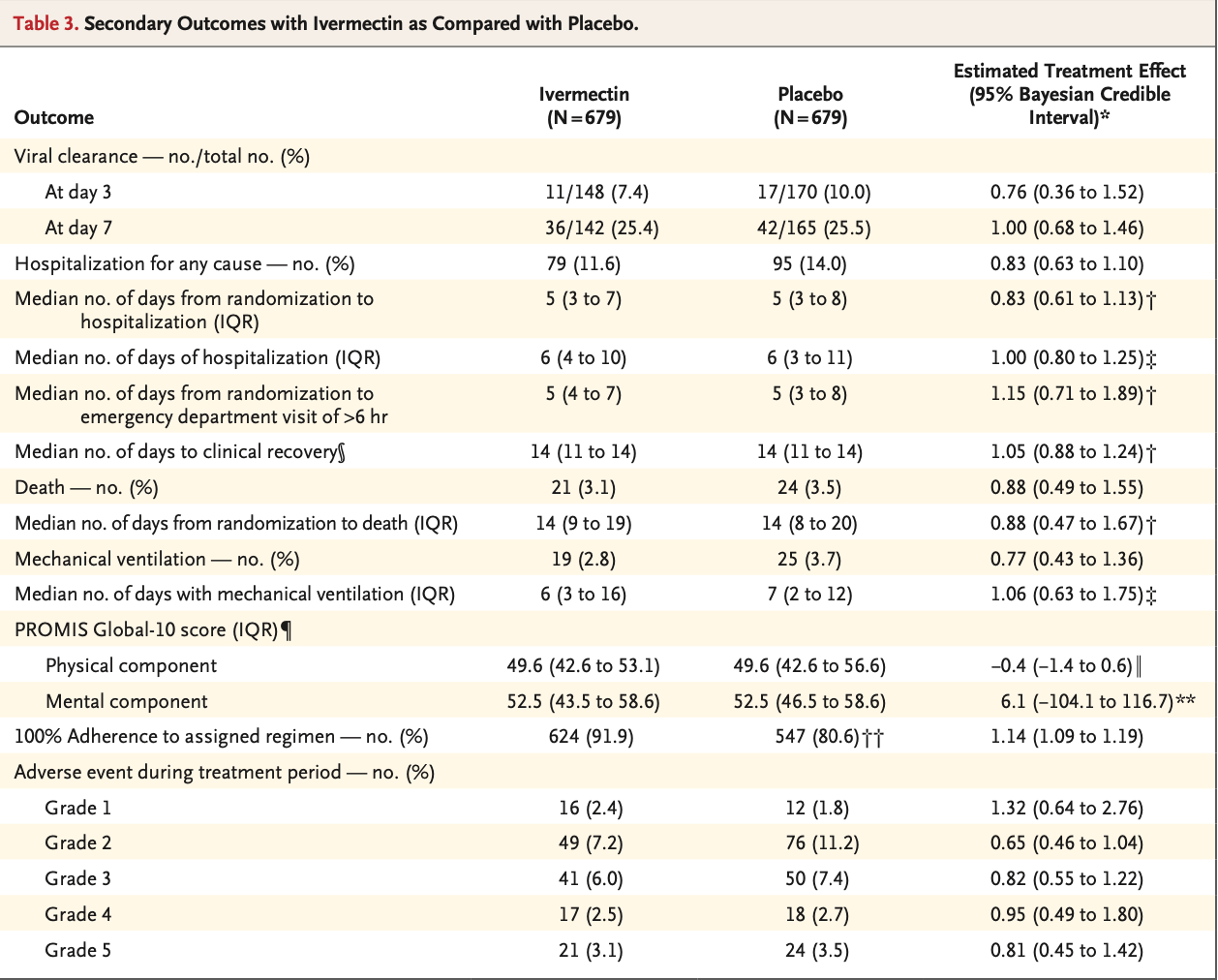
CRITICALThree conflicting death counts.
In the original paper, Table 3 shows 21 and 24 deaths, while Table S6 shows 20 and 2550. In Table 3, death and grade 5 events showed the same 21/24 numbers, but different effect sizes, with 0.81 being closer to the 20/25 counts and the previously reported number. This is consistent with one death being moved between arms after manuscript generation, but not updated in Table S6 or the Table 3 AE RR. This cannot be explained by the safety population excluding patients with zero doses because the AE control deaths are higher. In email, a co-principal investigator suggested that the discrepancy was due to one being COVID-19 deaths and the other being all-cause deaths2. That explanation does not fit the data because one arm increases while the other arm decreases. Both co-principal investigators report in the paper that "they had full access to all the trial data and vouch for the accuracy and completeness of the data and for the fidelity of the trial to the protocol." A third set of death counts, 20 and 24, with RR 0.84, was presented by a co-principal investigator on Mar 18, 202251. In total, 4 different death relative risks have been presented: Mar 18, 2022 presentation: 0.84, Mar 30 paper: 0.88 (T3), 0.81 (T3 AE), and 0.80 (TS6, presented as 20 and 25 only without group sizes). 6 days after publication, the paper was updated, with no information given on what was changed. In this version, a "respiratory, thoracic and mediastinal disorders" death was removed from the control arm and an "infections and infestations" death was added to the ivermectin arm. The paper still indicates RR 0.81 for death AE.
CRITICALPlacebo adverse event conflicts with fluvoxamine arm.
For FLV, there were 11 grade 1 AEs, for IVM there were 12, with 77 less patients. For FLV, there were 50 grade 3 AEs, for IVM there were also 50, meaning the 77 extra patients had 0% grade 3 AEs vs. an expected 7.4%. For FLV, there were 54 CKD patients according to Figure 3 and eTable1 (2 according to Table 1). For IVM there was 5.
CRITICALConflicting adverse event counts.
Table 3 and Table S6 adverse event counts do not match for any grade, e.g., grade 1/2 in Table S6 shows 82 for IVM, while Table 3 shows 6552. The Apr 5 update changed the grade 5 events without explanation, however the other grades remain conflicting.
CRITICAL3-day dosing patients before March 23 missing.
The co-principal investigator wrote on March 6 that 3-day dosing was being administered, and that the clinicaltrials entry was out of date at that time53. This earlier start of the 3-dose arm would resolve an oustanding major inconsistency. Analysis of the trial randomization shows that reaching the 3-day placebo count requires patients from March 454, and it would be logical for the 3-day placebo and 3-day active arms to have started on the same day. This reinforces existing concerns as to which patients were included in the analysis, and adds additional questions regarding what happened to the patients prior to March 23, and if patients were treated prior to ethics approval. Ethics approval for the dose change was received on March 21 according to the paper55, with the regulator document dated March 1556.
CRITICALMultiple false statements by investigators.
There has been multiple false statements by investigators raising questions about their ethics and the reliability of their work3.
CRITICALInvestigators not responding to concerns.
After details of major data errors and protocol violations became known, investigators appear to have stopped responding to all researchers regarding serious concerns with the trial3,57 (and have still not responded to us).
CRITICALICODA reports never having the data.
Investigators report that the data is available via ICODA: "The final trial dataset will be accessible by written request to the study principal investigators (G Reis or EJ Mills). There are no contractual agreements to limit access to final trial data. All data collected by the TOGETHER Trial will be shared with the International COVID-19 Data Alliance". Not only has there been no reports of successful access to the data, but an ICODA manager reports that they have never had the data58.
CRITICALIndications of ivermectin use in the placebo arm.
Recent ivermectin use was not in the exclusion criteria, however community use was widespread. Ivermectin was available OTC, was recommended by the government for COVID-19, and had nine times higher sales59. Authors claim they ensured patients did not use ivermectin via "extensive screening", but do not explain why this was not an exclusion criterion, or how this unwritten exclusion was ensured even though there is extensive missing data related to written exclusion criteria. Similar unwritten exclusions were not mentioned for other arms60, a primary investigator previously stated such an exclusion should not be an issue61, and it is not mentioned in the interview sheets62. After publication, a co-principal investigator reportedly wrote that "even if some patients did access IVM, the fact that it is blinded should still maintain balance", which is incorrect, placebo patients taking ivermectin are expected to improve, treatment patients that already have significant tissue distributions may have positive, neutral, or negative responses to additional treatment. Further, there are contradictory reports of how patients with prior ivermectin use were handled, and there is an indication that patients who had taken, or "were likely to take" ivermectin for COVID-19 were re-allocated to fluvoxamine or placebo63.
CRITICALConflicting and inconsistent PP/ITT groups.
Conflicting and inconsistent decreases in PP vs. ITT groups between different tables and between the treatment and control arms41.
CRITICALRefusal to release per-protocol mortality and hospitalization data.
Refusal to release per-protocol mortality and hospitalization results although they were reported for fluvoxamine and their importance was emphasized by coauthor Dr. Boulware41.
CRITICALConflicting descriptions of the placebo group.
There are multiple conflicting statements regarding the placebo group41.
CRITICALFailure of NEJM to publish letters reporting errors and issues.
NEJM has refused to publish any of the many letters submitted by scientists reporting errors and critical issues with the trial. For details see41.
CRITICALPlacebo tablets may not match treatment tablets.
Authors do not specify the appearance of the placebo tablets, suggesting that they may not match the treatment tablets, providing an additional reason for blinding failure. A Brazilian investigator reports that, at the time of the trial, there was only one likely placebo manufacturer, and they reportedly did not receive a request to produce identical placebo tablets38. They also report that compounded ivermectin in Brazil is considered unreliable.
CRITICAL162 control patients missing onset data vs. 1 for peginterferon lambda.
162 control patients are missing time from onset (Figure 2), however for peginterferon lambda (which overlaps with ivermectin in time) authors claim only one control patient is missing time from onset64 (page 25).
CRITICALContradictory inclusion/exclusion of vaccinated patients, changes, and confounding.
The trial changed from including vaccinated patients to excluding them on Mar 21, 202165,66, and on Jul 5 the exclusion was changed to specify >14 days. As discussed, meeting the reported placebo counts likely requires taking placebo patients from the earlier period, which has significant confounding due to variant changes. The vaccine inclusion change adds additional confounding, which also favors the placebo group. The original vaccine inclusion criterion is shown in both the protocol and the clinicaltrials.gov record67,68. Note that the paper, master protocol, Brazilian protocol, and trial registration report contradictory information on vaccine inclusion/exclusion and changes over time69.
CRITICALImpossible data in the metformin arm.
Data for the primary outcome in the metformin arm of this trial appears to be impossible70. For example, considering the metformin arm and the ITT population: 24 were hospitalized and 8 had an ER visit (tables S2/S3), therefore the number for combined ER or hospitalization must be between 24 and 32. However, authors report 34 events for ER/hospitalization.
CRITICALConflicting information on FTX funding.
There is conflicting information and statements regarding FTX funding of the trial71.
CRITICALMetformin/fluvoxamine conclusions opposite of COVID-OUT, but matching earlier studies on each team.
The Together trial and COVID-OUT both tested metformin and fluvoxamine. Notably, they came to opposite conclusions. In Together, authors found efficacy for fluvoxamine, but the metformin results were so negative that the trial was terminated early. In COVID-OUT it was the opposite, authors (although not the journal editor) found efficacy for metformin, while the fluvoxamine results were so negative that the trial was terminated early72. Note that the Together authors include researchers that found fluvoxamine effective in earlier studies, while the COVID-OUT authors include researchers that found metformin effective in earlier studies.
CRITICALAuthor claims results from 670 researchers should be censored for false information.
66 studies by 670 scientists report statistically significant positive results for ivermectin treatment of COVID-1973. One author claimed that a report of positive results is "disinformation" and distributed a request to report and censor the author74-76. While discussion is warranted for all studies, a call for censorship of results is extreme and raises questions. Author provides no basis for the results of the 670 scientists being wrong and warranting of censorship, and there is no indication that author has even read most of the studies. Author cherry-picked two of 106 studies, (COVID-OUT and ACTIV-677,78, both very high COI studies with an extensive list of issues and very delayed treatment) and claimed that "no benefit of ivermectin was observed"79. In addition to ignoring the 66 studies reporting statistically significant positive results, ACTIV-680 reported a posterior probability that ivermectin is effective of 99%, 98%, and 97% for mean time unwell, clinical progression @14 days, and clinical progression @7 days (even though none of the pre-specified primary outcomes were reported, and noting that these preprint results were changed without explanation), and COVID-OUT showed 61% lower hospitalization with ivermectin vs. placebo (not including metformin), although this was not reported.
CRITICALPaper silently modified without notification or explanation.
Apr 5: The paper was silently updated, with no indication or explanation of the changes. Changes include: age range, placebo description, per-protocol count, and death counts (as above). May 5: The paper was silently updated again. A new summary notes that authors attempted to screen for previous ivermectin use, contradicting both the discussion section, where authors claim they ensured no use for COVID-19, and the exclusion criteria and interview forms, which do not specify ivermectin use.
CRITICALTeam selected dose below what they believe is required.
Dr. Craig Rayner, a senior investigator on the trial, previously published research indicating that a higher dose is required81, raising the question of why the dose and fasting administration was chosen, for both the single day and 3 day dose regimens. Clinical equipoise82 raises ethical questions about running a trial where the invesigators do not believe the chosen dose is effective. Krolewiecki show an antiviral effect only with plasma concentrations above 160ng/mL. Figure S5 shows that the authors expected the mean concentration to be well below this level84. Dosage requirements are likely to vary significantly depending on many factors including the variant encountered, time of administration, mode of administration, patient genetics, concomitant medications, SOC, and the distribution of the infection in different tissues. However, the dose used is far below what is recommended by clinicians for post-infection treatment with the Gamma variant — about 2.5 - 6.5x lower, depending on the recommendation and which estimate of fasting/fed administration is used. The trial used fasting administration, however Merck's product information reports that "administration of 30mg ivermectin following a highfat meal resulted in an approximate 2.5-fold increase in bioavailability relative to administration of 30mg ivermectin in the fasted state."85.
CRITICALFDA concerns regarding trial conduct for peginterferon lambda.
The peginterferon lambda arm of this trial generated positive results, however the FDA denied a request for a pre-EUA meeting, citing concerns about the conduct of the trial89. Reportedly, the "FDA will not consider an EUA application based on results generated from the TOGETHER study"89. Details of the FDA's concerns were not provided.
CRITICALCo-principal investigator agrees with political need to demonstrate poor efficacy.
Frank Harrell commented that "..the question of whether this study was stopped too early in light of the political ramifications of needing to demonstrate that the efficacy is really unimpressive.. really could be raised..", and co-principal investigator Prof. Ed Mills responded "I totally agree with Frank"4.
CRITICALPrivate comments on efficacy contradict public comments.
Co-principal investigator Prof. Ed Mills said the following in private communication: "There is a clear signal that IVM works in COVID patients.. that would be significant if more patients were added.. you will hear me retract previous statements where I had been previously negative"2, while public comments are contradictory, e.g. “There was no indication that ivermectin is clinically useful”.
CRITICALMid-trial change adds patients showing lower efficacy.
Authors modified the inclusion criteria mid-trial to allow adding more low-risk patients <5090. Comparison with the metformin placebo arm shows many more patients <50 were included in the later part of the trial. Notably, the primary outcome shows much higher efficacy for patients ≥50, which would be statistically significant if there was about 50% more patients ≥50.
CRITICALFunding from Gates Foundation.
Analysis suggests funding of the ivermectin arm in part by the Gates Foundation by way of Certara and Prof. Rayner91, in addition to previously disclosed funding of the overall trial. Authors list only FastGrants and Rainwater in the ivermectin paper. The Gates Foundation was cited as a funder on the web site until Sep 13, 202192 (after completion of the trial). Correspondence regarding fluvoxamine and fluoxetine notes that Certara support for the TOGETHER study was funded by the Gates Foundation93.
CRITICALConflicting reports on trial end date.
There are conflicting reports on when enrollment into the ivermectin and fluvoxamine arms ended94, with the master protocol showing the end as July 26 and the web site confirming an end in July. However, the papers report August 5 and 6.
SERIOUSSide-effect prevalence consistent with treatment error.
The side effects (e.g., gastrointestinal side effects were lower in the ivermectin arm) suggest that many ivermectin patients may not have received authentic ivermectin, or that placebo patients may have taken ivermectin. For comparison, there was a 3.6 times greater incidence of diarrhea in the treatment arm in Lim.
SERIOUSScreening to treatment delay unknown.
Most Together Trial master protocols show an additional day delay in already late treatment for most patients. The Aug 5, 2021 protocol published with the metformin paper96, shows treatment administration one day after screening, baseline, and randomization (Table 2, schedule of study activities). This can also be found in the protocol dated Mar 11, 202197. The protocol attached to the ivermectin paper, dated Feb 15, 2021, shows a different schedule, stating that the treatment should be administered on the same day of randomization. There is no explanation of when this change was made, how the overlapping metformin and ivermectin arms could use different schedules, or how this change was implemented (there are many tasks in the screening and baseline visits). There is no reporting for how many patients received treatment on the same day. The form for the first treatment visit asks if there were clinical events including >6hr ER visits since the baseline visit, which would not be possible if this visit was immediately after randomization. Time of first treatment was recorded62, but no information has been reported. According to Forrest, WhatsApp messaging and video was used for recruitment, raising the question of how medication was delivered in cases where recruitment was done online. The Brazilian versions of the protocol do not match the master protocol, with all showing administration on the same day. The first Brazilian version of the protocol stated the drug "must be administered on the same day", however in March 2021 and later versions, this was changed to "should be administered on the same day".
SERIOUSUnknown onset patients show statistically significant efficacy.
For the known time since onset subgroups, both groups show worse results than the overall results99, with the missing 317 patients showing significant efficacy RR 0.51, p = 0.02 (compared to 1.00 and 1.14 for known patients).
SERIOUS317 unknown onset patients, onset required for inclusion.
Figure 2 shows that the time from onset was unknown for 317 patients, however time from onset is required for the inclusion criteria.
SERIOUSUnknown onset patients treated late.
After imputation, the percentage of patients in the late treatment subgroup went from 46% to 56%. 87% of the unknown patients were predicted to be in the late group. This is reasonable and expected — patients that do not recall when the onset was are more likely to have had onset further in the past. What is not clear is how these patients could be enrolled in the trial, how many of these patients had onset >7 days, how this very late 317 patient subgroup could show much greater efficacy as above, and why authors did not report this result, analyze this in greater detail, or recommend further research.
SERIOUSConflicting comorbidity counts.
The companion fluvoxamine arm ran from Jan 20 to Aug 5, 2021, while this trial ran from March 23 to Aug 6, 2021 — most control patients should be shared, with an additional 10% for fluvoxamine from the earlier start. The Aug 6 presentation, which has a date of 9:38am Aug 6 local trial time100, shows 678 placebo patients, indicating that either 0 or 1 placebo patients were randomized on Aug 6. Zero patients should have been randomized on Aug 6, because authors cannot add patients after unblinding. The fluvoxamine control arm shows 16/756 control patients with asthma. The ivermectin control arm has a subset of these patients (679), but shows a much higher prevalence of asthma (60 patients). This might be possible due to imputation if there was a very high percentage of missing data, however imputation does not appear to be a good explanation. For example, placebo CKD goes from 2 to 5 (FLV->IVM). First, it is not logical to impute CKD on patients based on the other variables. Second, the protocol specifies imputation only with up to 20% missing data, making it unlikely that imputation would add 150% of CKD patients. Third, the degree of change between FLV and IVM varies dramatically, with IVM reporting 666%, 275%, 150%, and 43% more patients for CPD, asthma, CKD, and CCD, without any clear explanation for similar differences in the percentage of missing data (all were collected on the same interview form).
SERIOUSUnexplained >6 month delay.
The paper was delayed over 6 months with no explanation. The companion fluvoxamine arm, completed at the same time, was published Aug 23, 2021. The very long delay, high profile of the topic, and other issues above raise questions. The paper was submitted to NEJM in Sep 2021101. COI forms suggest that additional authors were added after submission and the corresponding author changed from Prof. Mills to Dr. Rayner102, whose conflicts include Pfizer, Merck, the Gates Foundation, and the Australian Goverment.
SERIOUSPlacebo patients receiving an injection not blinded.
One-day placebo patients, which study documents repeatedly report as being included in the placebo group, would include those receiving a single injection, and are therefore not blinded41.
SERIOUSMajor imputation error.
In the paper authors use imputation in Table 1 but not in Figure 2. Authors also released a version of Figure 2 with imputation103, where the numbers for age and BMI now match the imputed numbers in Table 1. However, the time from onset numbers are very different, with the treatment arm showing 302 patients for 0-3 days, and the imputed version of Figure 2 showing 367104.
SERIOUSSingle dose results missing.
Results for the single dose ivermectin arm have not been reported.
SERIOUSIncorrect conclusion.
The conclusion states that ivermectin "did not result in a lower incidence of [hospitalization] or of [ER observation >6hr]". This is incorrect, hospitalization was 17% lower, which is not statistically significant with the sample size and typical statistical analysis. For the Bayesian analysis the authors use, the ITT probability of superiority for ivermectin was 79.4%, which is a positive result, the opposite of the conclusion.
SERIOUSMid-trial protocol changes.
There were several mid-trial protocol changes on July 5, 2021106. The number of patients for viral load analysis was reduced, only for the ivermectin arm. All-cause, cardiovascular, and respiratory death outcomes were deleted (all-cause was reported). Exclusions were modified to allow enrolling patients vaccinated within the last 14 days. Inclusion criteria were modified to allow enrolling healthy young people — the criterion "fever >38C at baseline" was added, allowing enrollment independent of increased risk.
SERIOUSCOI: designed by Cytel.
The trial was designed by Cytel, a company that helps pharmaceutical companies get approval and that works very closely with Pfizer107,108. Cytel's software and services are used by the top 30 pharmaceutical companies109.
SERIOUSCOI: co-principal investigator works for Cytel and the Gates Foundation.
A co-principal investigator works for Cytel and the Gates Foundation110: "The majority of the time I work for a company called Cytel, where I design clinical trials, predominantly for the Bill & Melinda Gates Foundation".
SERIOUSCOI: pharma funding and denial of independent investigator.
Reportedly, the first author's center is funded by pharmaceutical companies, and independent investigators tried to participate in the trial but were denied111.
SERIOUSCOI: Gates Foundation.
The Gates Foundation is a founding partner of GAVI, which took out Google ads telling people not to use ivermectin112, and a major funder of Unitaid, which may have modified the results of the Hill meta analysis in a way that prevented adoption45-47.
SERIOUSCOI: Certara.
One of the senior investigators was Dr. Craig Rayner, President of Integrated Drug Development at Certara - another company with a similar mission to MMS Holdings. They state on their website that: "Since 2014, our customers have received over 90% of new drug and biologic approvals by the FDA." One of their clients is Pfizer113.
SERIOUSCOI: MMS Holdings.
The trial is associated with MMS Holdings31, whose mission includes helping pharmaceutical companies get approval and designing scientific studies that help them get approval. One of their clients is Pfizer114.
SERIOUSCOI: analysis company works closely with Pfizer.
All analyses were done by Cytel. Cytel is a statistical modelling company that helps pharmaceutical companies get approval — they work very closely with Pfizer108. Cytel's software and services are used by the top 30 pharmaceutical companies109.
SERIOUSCOI: Fast Grants funding closely related to companies that censored scientific research.
Fast Grants funding is closely related to tech companies that censored ivermectin and other early treatment research. These companies have a strong conflict of interest in not admitting that their censorship was harmful115,116.
SERIOUSUnexpected differences in missing data.
Age is unknown for 98 patients, however according to Figure 2, BMI is missing for only 11 patients, smoking status is unknown for only 2 patients, lung disease is unknown for only one patient, and cardiovascular disease is known for all patients.
SERIOUSOut of funding claim contradicted by funder.
A co-principal investigator has reported that the trial was stopped because they ran out of funding, however this is contradicted by the Rainwater Foundation, which reported that they would have given more money to finish the trial if the investigators had asked117.
SERIOUSMisrepresentation of dosing recommendation.
Investigators have misrepresented an email from the FLCCC regarding recommended dosing117.
MAJORMean delay likely excluding unknown onset.
The reported mean number of days from symptoms to randomization probably only includes known onset patients and therefore is likely to significantly underestimate the actual average (in addition to not including the time between randomization and treatment).
MAJORPer-protocol placebo much more effective.
The 3-dose per-protocol placebo group shows greater efficacy29,118. This could be consistent with placebo patients accidently receiving treatment.
MAJORMultiple conflicting randomization protocols.
twitter.com (AE) reviewed the randomization protocol, finding three different algorithms, and conflicting versions in the papers.
MAJORDominated by Gamma variant with different characteristics, no discussion.
The trial took place in an area of Brazil and time when the Gamma variant was dominant. Brazilian clinicians report that this variant is much more virulent, and that significantly higher dosage and/or earlier treatment is required, as may be expected for variants where the peak viral load is significantly higher and/or reached earlier9,11.
MAJORIncorrect dose reporting, patients at higher risk due to BMI may have received lower per kg doses, and show lower efficacy.
The paper reports 400μg/kg for 3 days, however the protocol indicates that this was only up to 90kg, meaning that the dose received for higher-risk high BMI patients was even further reduced from dosage which is already far below clinician recommendations for the dominant variant120. 50% of patients had BMI ≥30. Much greater efficacy was seen in the low BMI subgroup (RR 0.77 vs 0.98).
MAJORConflicting target enrollment and reasons for termination.
There are conflicting target enrollment numbers. The protocol showed 800 patients per arm as of Mar 21, 2021 (after the trial started)121,122, the co-principal investigator reported 800 per arm in an interview published June 14, 2021123, and the protocol changed to 681 on June 22124. However, the trial record from Jan indicates 2724 (681*4) patients67, suggesting that the 800 goal was later, and was kept for fluvoxamine but reverted for ivermectin. The fluvoxamine arm which started two months earlier was terminated at the same time, and was terminated due to superiority125 after 741/756 patients. Note that Gamma was declining significantly around the termination point, which likely favors improved efficacy if the trial continued, given the late treatment and dosage used. The co-principal investigator reports three different reasons for stopping the trial126: a) because they ran out of money, b) because third parties were not supportive, and c) it was done by the DSMC and was out of their control.
MAJORPrimary outcome subject to bias, selected after single dose arm.
The subjective "emergency room visit for >6 hours" criterion shows higher risk (RR 1.16), while hospitalization is lower (RR 0.83 all-cause, RR 0.84 COVID-19). The primary outcome results were set on March 21, 2021, after the single dose ivermectin arm. Given the known public biases of some investigators, this may have been specifically chosen to reduce efficacy. Authors claim that the 6hr threshold did not include waiting time, however the emergency visit form has no mention of waiting time, only recording presentation and discharge times62.
MAJORReported terminated due to futility, but threshold not reached.
The trial was reportedly terminated due to futility127, however the futility thresholds were 20%, 40% and 60%, and all published probabilities are >60% (ITT 79.4%). Additionally, the fluvoxamine arm did not have the higher 60% threshold, only using 40%. Note the DSMC was not independent as below.
MAJORSubgroup analysis protocol violations.
The presented subgroup analysis is inconsistent with plans and with the fluvoxamine paper, including not presenting pre-specified subgroups, presenting subgroups that were not pre-specified, presenting different subgroups to the contemporary fluvoxamine paper, and modifying subgroup definitions128.
MAJORMany pre-specified outcomes missing.
Many outcomes specified in the protocol appear to be missing, including the co-primary outcome of COVID-19 mortality (only all-cause mortality is provided, specific AE details not provided), time to clinical failure, days with respiratory symptoms, mortality due to pulmonary complications, cardiovascular mortality, COVID-19 symptom scale assessment, WHO clinical worsening scale assessment, and 14 day mortality.
MAJORSingle-dose recruiting continued after change.
The trial had requested moving to 3-dose treatment by Feb 15/19, when only 19 patients had been recruited, however the trial continued recruiting an additional 59 patients to single dose treatment129.
MAJORFunding list incorrect, missing Gates Foundation and Unitaid.
The paper does not include the Bill and Melinda Gates Foundation or Unitaid as funders, however the protocol shows the Gates Foundation130 and the web site shows Unitaid48.
MAJORStatistical analysis plan dated after trial start.
The statistical analysis plan appears to be dated after the trial started131.
MAJORImputation protocol violation.
The protocol specifies multiple imputation with up to 20% of missing data, however imputation was done with time from symptom onset, which has >23% missing data132.
MAJORExpected analyses missing.
Authors do not provide time from onset analysis for either mortality or hospitalization, only the combined measure including the ER visits where anomalous results are seen. Authors do not provide per-protocol or mITT results for mortality or hospitalization. Per-protocol mortality results were provided for the companion fluvoxamine trial.
MAJORConflicting reasons for dose change.
Conflicting reasons have been given for the change from 1-day to 3-day dosing. In email from March 6, the co-principal investigator says the change was "based on emerging trials from Andrew Hill's synthesis"133. The paper says the change was made "on the basis of feedback from advocacy groups". Neither of these match the report that the dosing change was made at the request of one of the trial funders3.
MAJORDetails of placebo unspecified.
The placebo appears to be unspecified in the paper and protocol. The initial trial announcement indicated the placebo was vitamin C107, which would be an active treatment according to the results of 72 studies (mortality RR 0.81 [0.73-0.91]). The metformin arm reports using talc, however fluvoxamine and ivermectin do not appear to report details of the placebo, which could potentially be different, for example based on manufacturer limitations for matching active treatment tablets.
MAJORAntigen test requirement.
The protocol indicates that patients with a negative test may be included if they become positive a few days later, potentially resulting in a long unreported delay between randomization and treatment, depending on how investigators interpreted the protocol. The requirement for a positive antigen test excludes the possibility of early treatment in many cases - tests have very high false negative rates in the early stages of infection, and symptoms may appear before the test becomes positive.
MAJORTwo different per-protocol counts.
Figure 1 shows 228 per-protocol for the control arm, while Table 2 shows 288. This was modified in the Apr 5 update without explanation.
UNKNOWNSource of ivermectin unspecified (fluvoxamine source specified).
Authors do not specify the source of the ivermectin used in the trial, whereas they do specify the source for the fluvoxamine arm (Luvox, Abbott). Depending on the source, Ivermectin has been reported to be of unreliable quality in Brazil.
UNKNOWN100% adherence reported for 3-day placebo.
Reported numbers indicate that there was 100% adherence among 288 patients assigned to 3-day placebo, which is unexpected3,54.
UNKNOWNNo confirmation of placebo manufacturing.
A local Brazilian investigator reports that, at the time of the trial, there was only one likely placebo manufacturer, and they reportedly did not receive a request to produce identical placebo tablets38. They also report that compounded ivermectin in Brazil is considered unreliable. The protocol reports that "the study medication used will come from pharmaceutical plants that hold a commercial authorization for their production, already approved by ANVISA."
The following comments are prior to the publication and
may be out of date. We note that authors claim they have not included
patients prior to the time period for the 3 dose ivermectin patients, however
this conflicts with previously reported data as per the analyses above.
The trial randomization chart does not match the protocol,
suggesting major problems and indicating substantial confounding by time. For
example, trial week 43, the first week for 3 dose ivermectin, shows ~3x
patients assigned to ivermectin vs. placebo5.
Treatment efficacy can vary significantly over time, for example due to
overall improvement in protocols, changes in the distribution of variants, or
changes in public awareness and treatment delays.
Zavascki show dramatically higher mortality for Gamma vs non-Gamma
variants (28 day mortality from symptom onset aHR 4.73 [1.15-19.41]), and the
prevalence of the Gamma variant varied dramatically throughout the trial7.
This introduces confounding by time, which is common in COVID-19 retrospective
studies and has often obscured efficacy (many retrospectives have more
patients in the treatment group earlier in time when overall treatment
protocols were significantly worse).
According to this analysis5,
the total number of patients for the ivermectin and placebo groups do not
appear to match the totals in the presentation (the numbers for the
fluvoxamine arm match) — reaching the number reported for ivermectin
would require including some of the patients assigned to single dose
ivermectin. Reaching the placebo number requires including placebo patients
from the much earlier ivermectin single dose period, and from the early two
week period when zero ivermectin patients were assigned. If these earlier
participants were accidently included in the control group, this would
dramatically change the results in favor of the control group according to
the changes in Gamma variant prevalence.
An investigator from Brazil notes that the gamma variant became
prevailing in the state of Minas Gerais later than in the rest of the country,
with the time when gamma prevailed for the trial locations being more closely
aligned with the start of the ivermectin arm8.
Due to the substantial differences in disease course and risk between the
variants, authors need to consider only patients recruited during the same
time period.
Treatment delay is currently unknown, however the protocol
allows very late inclusion and a companion trial reported mostly late
treatment. Overall mortality is high for 18+ outpatients. Results may be
impacted by late treatment, poor SOC, and may be specific to local variants9-11.
Treatment was administered on an empty stomach, greatly reducing expected
tissue concentration12 and making the effective dose about
1/5th of current clinical practice. The trial was conducted in Minas Gerais,
Brazil which had substantial community use of ivermectin13,
and prior use of ivermectin is not listed in the exclusion criteria.
This trial uses a soft primary outcome, easily subject to bias
and event inflation in both arms (e.g., observe >6 hours independent of
indication). There is also an unusual inclusion criteria: "patients with
expected hospital stays of ≤5 days". This is similar to "patients less
likely to need treatment beyond SOC to recover", and would make it very easy
to reduce the effect seen. This is not in either of the published
protocols.
RCTs have a fundamental bias against finding an effect for
interventions that are widely available — patients that believe they
need treatment are more likely to decline participation and take the
intervention14, i.e. RCTs are more likely to enroll low-risk
participants that do not need treatment to recover (this does not apply to
the typical pharmaceutical trial of a new drug that is otherwise
unavailable). This trial was run in a community where ivermectin is widely
known and used.
The same trial's results for a previous treatment were
initially reported as RR 1.0 [0.45-2.21]15, while
the final paper reported something very different — HR 0.76 [0.30-1.88]16.
Trial design, analysis, and presentation, along with previous
public and private statements suggest investigator bias. Design: including
very late treatment, additional day before administration, operation in a
region with high community use, specifying administration on an empty
stomach, limiting treatment to 3 days, using soft inclusion criterion and a
soft primary outcome, easily subject to bias. Analysis: authors perform
analysis excluding events very shortly after randomization for fluvoxamine
but not ivermectin, and report viral load results for fluvoxamine but not
ivermectin. Presentation: falsely describing positive but not statistically
significant effects as "no effect, what so ever"17,18.
Prior statements: odysee.com.
The local Brazilian investigator also reports that nitazoxanide
was tested in the same location, however very few patients reportedly
experienced urine discoloration, while all are expected to experience this
side effect. They also suggest that 6-hour observation is a poor choice
because it is almost impossible to stay less than 6 hours in Brazil.
For additional issues see: stevekirsch.substack.com, cato.org, longhaulwiki.com, trialsitenews.com, covid19criticalcare.com, doyourownresearch.substack.com, twitter.com, web.archive.org, web.archive.org (B), twitter.com (B), Marinos, Marinos (B) .
Protocols, approvals, and statistical analysis plans can be found here
togethertrial.com.
Revisions: added the median number of days to clinical recovery outcome.
This is the 29th of 54 COVID-19 RCTs for ivermectin, which collectively show efficacy with p=0.00000004.
This is the 59th of 106 COVID-19 controlled studies for ivermectin, which collectively show efficacy with p<0.0000000001.
This study is excluded in the after exclusion results of meta-analysis:
multiple anomalies as per detailed analysis.
|
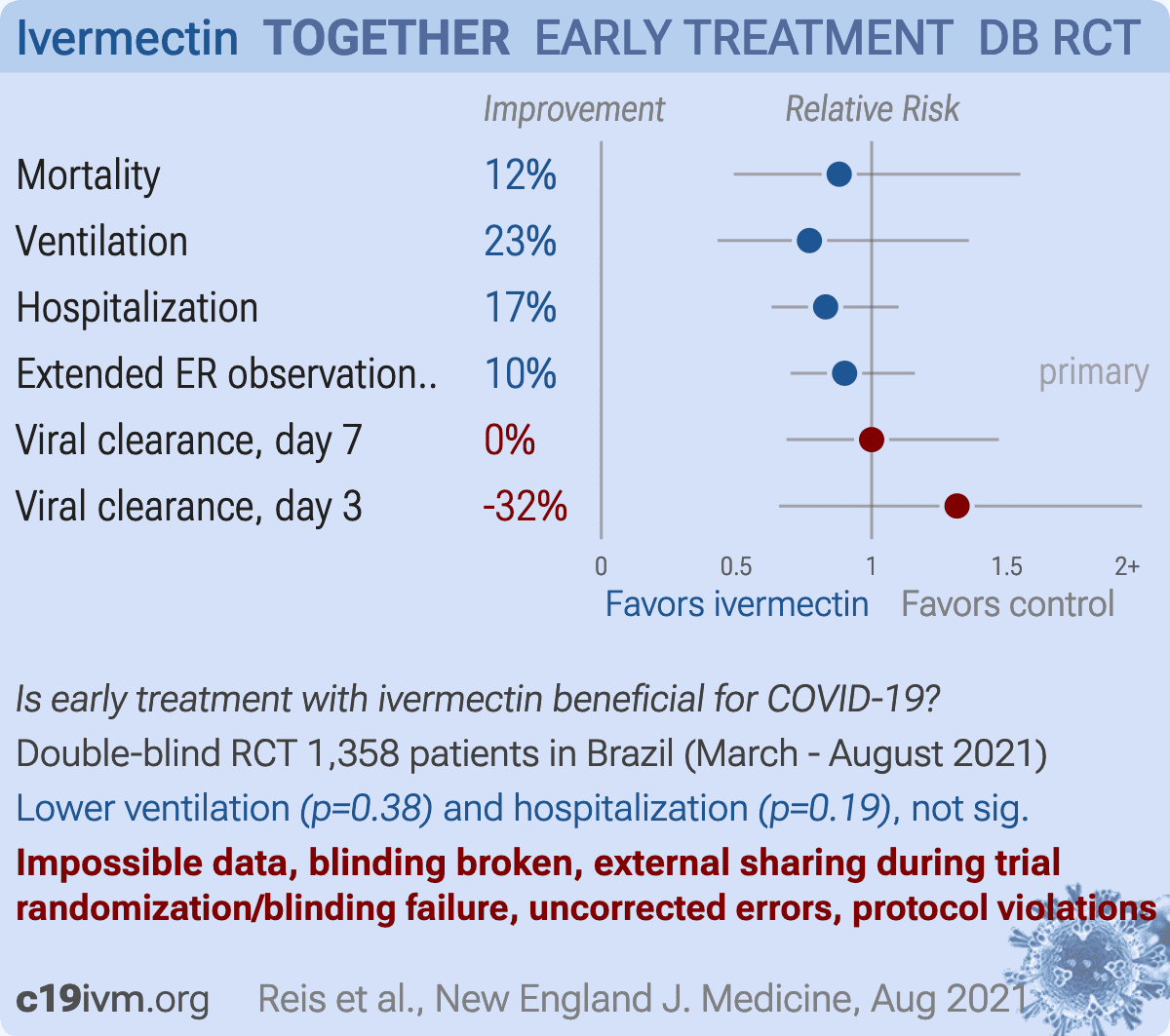
risk of death, 12.0% lower, RR 0.88, p = 0.68, treatment 21 of 679 (3.1%), control 24 of 679 (3.5%), NNT 226.
|
|
risk of mechanical ventilation, 23.0% lower, RR 0.77, p = 0.38, treatment 19 of 679 (2.8%), control 25 of 679 (3.7%), NNT 113.
|
|
risk of hospitalization, 17.0% lower, RR 0.83, p = 0.19, treatment 79 of 679 (11.6%), control 95 of 679 (14.0%), NNT 42.
|
|
extended ER observation or hospitalization, 10.0% lower, RR 0.90, p = 0.42, treatment 100 of 679 (14.7%), control 111 of 679 (16.3%), NNT 62, primary outcome.
|
|
risk of no recovery, 4.8% lower, HR 0.95, p = 0.59, treatment 679, control 679, inverted to make HR<1 favor treatment.
|
|
viral clearance, no change, RR 1.00, p = 1.00, treatment 106 of 142 (74.6%), control 123 of 165 (74.5%), day 7.
|
|
viral clearance, 31.6% higher, RR 1.32, p = 0.46, treatment 148, control 170, inverted to make RR<1 favor treatment, day 3.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
1.
Reis et al., RETRACTED: Effect of early treatment with metformin on risk of emergency care and hospitalization among patients with COVID-19: The TOGETHER randomized platform clinical trial, The Lancet Regional Health - Americas, doi:10.1016/j.lana.2021.100142.
5.
reddit.com, www.reddit.com/r/ivermectin/comments/p3vrrt/together_trial_was_not_randomized_possible/.
6.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
8.
ufmg.br, ufmg.br/comunicacao/noticias/minas-sao-muitas-distribuicao-de-variantes-do-sars-cov-2-pelo-estado-e-heterogenea.
9.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
10.
Sabino et al., Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence, Lancet, doi:10.1016/S0140-6736(21)00183-5.
11.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
12.
Guzzo et al., Safety, Tolerability, and Pharmacokinetics of Escalating High Doses of Ivermectin in Healthy Adult Subjects, J. Clinical Pharmacology, doi:10.1177/009127002237994.
13.
otempo.com.br, www.otempo.com.br/interessa/venda-de-ivermectina-aumenta-nove-vezes-em-minas-e-preocupa-por-risco-a-saude-1.2466432.
14.
Yeh et al., Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial, BMJ, doi:10.1136/bmj.k5094.
17.
Amrhein et al., Scientists rise up against statistical significance, Nature, 567:305-307, www.nature.com/articles/d41586-019-00857-9.
18.
odysee.com, odysee.com/@FrontlineCovid19CriticalCareAlliance:c/outpatients-defeating-the-delta-variant:a.
20.
longhaulwiki.com, longhaulwiki.com/resources/assets/Numerous%20issues%20with%20the%20TOGETHER%20trial.pdf.
21.
trialsitenews.com, trialsitenews.com/nejm-reported-3-30-that-ivermectin-in-the-together-trial-failed-to-show-significant-benefit-lets-take-a-closer-look/.
22.
covid19criticalcare.com, covid19criticalcare.com/wp-content/uploads/2022/03/Statement-on-Together-Trial-WSJ-Article-Mar-18-1.pdf.
23.
doyourownresearch.substack.com, doyourownresearch.substack.com/p/what-went-wrong-with-the-together.
25.
web.archive.org, web.archive.org/web/*/https://twitter.com/Covid19Crusher/status/1426612910579757059.
26.
web.archive.org (B), web.archive.org/web/*/https://twitter.com/Covid19Crusher/status/1427255119800848386.
28.
Marinos, A., The Problem With The TOGETHER Trial, Do Your Own Research, 4/13, doyourownresearch.substack.com/p/the-problem-with-the-together-trial.
29.
Marinos (B), A., TOGETHER Trial: Solving the 3-Day Placebo Subgroup Riddle, Do Your Own Research, 4/19, doyourownresearch.substack.com/p/together-trial-solving-the-3-day.
32.
doyourownresearch.substack.com (B), doyourownresearch.substack.com/p/together-trial-impossible-numbers.
33.
doyourownresearch.substack.com (C), doyourownresearch.substack.com/p/demonstrating-randomization-failure.
37.
doyourownresearch.substack.com (D), doyourownresearch.substack.com/p/the-together-files-1-the-andrew-hill.
38.
doyourownresearch.substack.com (E), doyourownresearch.substack.com/p/together-trial-solving-the-3-day/comment/6143361.
40.
odysee.com (B), odysee.com/@FrontlineCovid19CriticalCareAlliance:c/weekly_webinar_6April2022:c?t=2507.
41.
Scheim et al., When Characteristics of Clinical Trials Require Per-Protocol as Well as Intention-to-Treat Outcomes to Draw Reliable Conclusions: Three Examples, Journal of Clinical Medicine, doi:10.3390/jcm12113625.
44.
Thorlund et al., Making Statistical Sense of the Molnupiravir MOVe-OUT Clinical Trial, The American Journal of Tropical Medicine and Hygiene, doi:10.4269/ajtmh.21-1339.
49.
Harper, P., Professor tied to altered Andrew Hill paper also prepared 'Ivermectin Evidence' for World Health Organisation, philharper.substack.com/p/professor-tied-to-altered-andrew?s=r.
54.
doyourownresearch.substack.com (F), doyourownresearch.substack.com/p/together-trial-solving-the-3-day.
63.
doyourownresearch.substack.com (G), doyourownresearch.substack.com/p/did-the-placebo-group-in-the-together.
66.
clinicaltrials.gov (B), clinicaltrials.gov/ct2/history/NCT04727424?A=1&B=2&C=Side-by-Side#StudyPageTop.
68.
togethertrial.com (C), www.togethertrial.com/s/EN-Protocol_research_COVID19_AMB_02_Brazil_v10_17Dec2020.pdf.
70.
doyourownresearch.substack.com (H), doyourownresearch.substack.com/p/together-trial-and-the-negative-number.
71.
doyourownresearch.substack.com (I), doyourownresearch.substack.com/p/did-the-together-trial-lie-to-reuters.
77.
Bramante et al., Randomized Trial of Metformin, Ivermectin, and Fluvoxamine for Covid-19, NEJM, doi:10.1056/NEJMoa2201662.
78.
Naggie et al., Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2022.18590.
83.
Krolewiecki et al., Antiviral effect of high-dose ivermectin in adults with COVID-19: A proof-of-concept randomized trial, eClinicalMedicine, doi:10.1016/j.eclinm.2021.100959.
89.
ir.eigerbio.com, ir.eigerbio.com/news-releases/news-release-details/eiger-biopharmaceuticals-provides-update-plans-emergency-use.
91.
doyourownresearch.substack.com (J), doyourownresearch.substack.com/p/together-trial-on-ivermectin-did.
94.
doyourownresearch.substack.com (K), doyourownresearch.substack.com/p/when-did-the-ivermectin-and-fluvoxamine.
95.
Lim et al., Efficacy of Ivermectin Treatment on Disease Progression Among Adults With Mild to Moderate COVID-19 and Comorbidities: The I-TECH Randomized Clinical Trial, JAMA, doi:10.1001/jamainternmed.2022.0189.
98.
Forrest et al., Resilient Clinical Trial Infrastructure in Response to the COVID-19 Pandemic: Lessons Learned from the TOGETHER Randomized Platform Clinical Trial, The American Journal of Tropical Medicine and Hygiene, doi:10.4269/ajtmh.21-1202.
100.
doyourownresearch.substack.com (L), doyourownresearch.substack.com/p/was-the-data-in-the-together-trial/comment/6409395.
102.
doyourownresearch.substack.com (M), doyourownresearch.substack.com/p/the-problem-with-the-together-trial/comment/6043250.
104.
doyourownresearch.substack.com (N), doyourownresearch.substack.com/p/the-together-trial-cant-make-up-its?utm_source=twitter&sd=fs&s=r.
106.
clinicaltrials.gov (D), clinicaltrials.gov/ct2/history/NCT04727424?A=2&B=3&C=merged#StudyPageTop.
107.
cytel.com, www.cytel.com/blog/the-together-trial-cytel-designs-and-implements-novel-adaptive-platform-trial-for-covid-19-therapies.
109.
cytel.com (C), www.cytel.com/news/nordic-capital-and-astorg-invest-in-pharmaceutical-technology-and-advanced-analytics-company-cytel.
110.
empendium.com, empendium.com/mcmtextbook/interviews/perspective/236226%2Ccovid-19-to-treat-or-not-to-treat-platform-trials.
111.
odysee.com (C), odysee.com/@FrontlineCovid19CriticalCareAlliance:c/weekly_webinar_6April2022:c?t=612.
113.
certara.com, www.certara.com/pressrelease/pfizer-deploys-certaras-d360-for-scientific-data-access-and-analysis/.
114.
mmsholdings.com, www.mmsholdings.com/pfizer-selects-mms-as-preferred-provider-for-plain-language-summary-writing-support/.
117.
pierrekory.substack.com (B), pierrekory.substack.com/p/the-false-sinister-and-duplicitous?utm_source=twitter&sd=fs&s=r.
122.
static1.squarespace.com, static1.squarespace.com/static/6112a257d1c1153666ccb987/t/622282bf613a7d79403e7efe/1646428864052/Together_MP_V2.0_25Mar2021.pdf.
124.
static1.squarespace.com (B), static1.squarespace.com/static/6112a257d1c1153666ccb987/t/622283c2cf74fa66a07f6904/1646429124965/Together_MP_V3.0_22June2021.pdf.
Reis et al., 6 Aug 2021, Double Blind Randomized Controlled Trial, Brazil, peer-reviewed, 27 authors, study period 23 March, 2021 - 6 August, 2021, dosage 400μg/kg days 1-3, impossible data, see notes, trial NCT04727424 (history) (TOGETHER).
{kind=link}
Effect of Early Treatment with Ivermectin among Patients with Covid-19
New England Journal of Medicine, doi:10.1056/nejmoa2115869
BACKGROUND The efficacy of ivermectin in preventing hospitalization or extended observation in an emergency setting among outpatients with acutely symptomatic coronavirus disease 2019 (Covid-19), the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is unclear.
METHODS We conducted a double-blind, randomized, placebo-controlled, adaptive platform trial involving symptomatic SARS-CoV-2-positive adults recruited from 12 public health clinics in Brazil. Patients who had had symptoms of Covid-19 for up to 7 days and had at least one risk factor for disease progression were randomly assigned to receive ivermectin (400 μg per kilogram of body weight) once daily for 3 days or placebo. (The trial also involved other interventions that are not reported here.) The primary composite outcome was hospitalization due to Covid-19 within 28 days after randomization or an emergency department visit due to clinical worsening of Covid-19 (defined as the participant remaining under observation for >6 hours) within 28 days after randomization.
RESULTS A total of 3515 patients were randomly assigned to receive ivermectin (679 patients), placebo (679), or another intervention (2157). Overall, 100 patients (14.7%) in the ivermectin group had a primary-outcome event, as compared with 111 (16.3%) in the placebo group (relative risk, 0.90; 95% Bayesian credible interval, 0.70 to 1.16). Of the 211 primary-outcome events, 171 (81.0%) were hospital admissions. Findings were similar to the primary analysis in a modified intention-to-treat analysis that included only patients who received at least one dose of ivermectin or placebo (relative risk, 0.89; 95% Bayesian credible interval, 0.69 to 1.15) and in a per-protocol analysis that included only patients who reported 100% adherence to the assigned regimen (relative risk, 0.94; 95% Bayesian credible interval, 0.67 to 1.35). There were no significant effects of ivermectin use on secondary outcomes or adverse events.
CONCLUSIONS Treatment with ivermectin did not result in a lower incidence of medical admission to a hospital due to progression of Covid-19 or of prolonged emergency department observation among outpatients with an early diagnosis of Covid-19. (Funded by FastGrants and the Rainwater Charitable Foundation; TOGETHER ClinicalTrials.gov number, NCT04727424.
References
Azur, Stuart, Frangakis, Leaf, Multiple imputation by chained equations: what is it and how does it work?, Int J Methods Psychiatr Res
Bryant, Lawrie, Dowswell, Ivermectin for prevention and treatment of COVID-19 infection: a systematic review, meta-analysis, and trial sequential analysis to inform clinical guidelines, Am J Ther
Chua, Conti, Becker, US insurer spending on ivermectin prescriptions for COVID-19, JAMA
Forrester, Prichard, Beech, A glutamate-gated chloride channel subunit from Haemonchus contortus: expression in a mammalian cell line, ligand binding, and modulation of anthelmintic binding by glutamate, Biochem Pharmacol
Heidary, Gharebaghi, Ivermectin: a systematic review from antiviral effects to COVID-19 complementary regimen, J Antibiot
Hill, Mirchandani, Pilkington, Ivermectin for COVID-19: addressing potential bias and medical fraud, Open Forum Infect Dis
Kim, An, Kim, Hwang, Comparative efficacy and safety of pharmacological interventions for the treatment of COVID-19: A systematic review and network meta-analysis, PLoS Med
Kow, Merchant, Mustafa, Hasan, The association between the use of ivermectin and mortality in patients with COVID-19: a meta-analysis, Pharmacol Rep
Mahani, Sharabiani, Bayesian, and non-Bayesian, cause-specific competing-risk analysis for parametric and nonparametric survival functions: the R Package CFC, J Stat Softw
Montori, Permanyer-Miralda, Ferreira-González, Validity of composite end points in clinical trials, BMJ
Rayner, Dron, Park, Accelerating clinical evaluation of repurposed combination therapies for COVID-19
Reardon, Flawed ivermectin preprint highlights challenges of COVID drug studies, Nature
Reis, Eadsm, Silva, A multi-center, adaptive, randomized, platform trial to evaluate the effect of repurposed medicines in outpatients with early coronavirus disease 2019 (COVID-19) and high-risk for complications: the TOGETHER master trial protocol, Gates Open Research
Reis, Silva, Silva, Effect of early treatment with hydroxychloroquine or lopinavir and ritonavir on risk of hospitalization among patients with COVID-19: the TOGETHER randomized clinical trial, JAMA Netw Open
Schulz, Altman, Moher, Group, CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials, BMJ
Siemieniuk, Bartoszko, Ge, Drug treatments for covid-19: living systematic review and network metaanalysis, BMJ
Thorlund, Dron, Park, Hsu, Forrest et al., A real-time dashboard of clinical trials for COVID-19, Lancet Digit Health
Torres, Artaza, Profeta, Alonso, Kang, COVID-19 vaccination: returning to WHO's Health For All, Lancet Glob Health
Zein, Sulistiyana, Raffaelo, Pranata, Ivermectin and mortality in patients with COVID-19: a systematic review, meta-analysis, and meta-regression of randomized controlled trials
DOI record:
{
"DOI": "10.1056/nejmoa2115869",
"ISSN": [
"0028-4793",
"1533-4406"
],
"URL": "http://dx.doi.org/10.1056/nejmoa2115869",
"alternative-id": [
"10.1056/NEJMoa2115869"
],
"author": [
{
"ORCID": "http://orcid.org/0000-0002-4847-1034",
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"authenticated-orcid": false,
"family": "Reis",
"given": "Gilmar",
"sequence": "first"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Silva",
"given": "Eduardo A.S.M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Silva",
"given": "Daniela C.M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Thabane",
"given": "Lehana",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Milagres",
"given": "Aline C.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Ferreira",
"given": "Thiago S.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "dos Santos",
"given": "Castilho V.Q.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Campos",
"given": "Vitoria H.S.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Nogueira",
"given": "Ana M.R.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "de Almeida",
"given": "Ana P.F.G.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Callegari",
"given": "Eduardo D.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Neto",
"given": "Adhemar D.F.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Savassi",
"given": "Leonardo C.M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Simplicio",
"given": "Maria I.C.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Ribeiro",
"given": "Luciene B.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Oliveira",
"given": "Rosemary",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-2901-0558",
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"authenticated-orcid": false,
"family": "Harari",
"given": "Ofir",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Forrest",
"given": "Jamie I.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Ruton",
"given": "Hinda",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Sprague",
"given": "Sheila",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "McKay",
"given": "Paula",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Guo",
"given": "Christina M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Rowland-Yeo",
"given": "Karen",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Guyatt",
"given": "Gordon H.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-4715-0060",
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"authenticated-orcid": false,
"family": "Boulware",
"given": "David R.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Rayner",
"given": "Craig R.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "From the Research Division, Cardresearch–Cardiologia Assistencial e de Pesquisa (G.R., E.A.S.M.S., D.C.M.S., T.S.F., C.V.Q.S., V.H.S.C., M.I.C.S., L.B.R., R.O.), and the Department of Medicine, Pontifical Catholic University of Minas Gerais (G.R., E.A.S.M.S., D.C.M.S., C.V.Q.S., V.H.S.C.), Belo Horizonte, the Department of Public Health and Mental and Family Medicine, Ouro Preto Federal University, Ouro Preto (A.C.M., L.C.M.S.), the Public Health Care Division, Ibirité (A.C.M.), the Department of Public..."
}
],
"family": "Mills",
"given": "Edward J.",
"sequence": "additional"
}
],
"container-title": [
"New England Journal of Medicine"
],
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2022,
3,
30
]
],
"date-time": "2022-03-30T21:00:27Z",
"timestamp": 1648674027000
},
"deposited": {
"date-parts": [
[
2022,
3,
30
]
],
"date-time": "2022-03-30T21:00:31Z",
"timestamp": 1648674031000
},
"funder": [
{
"DOI": "10.13039/100016608",
"award": [
"NA"
],
"doi-asserted-by": "publisher",
"name": "The Rainwater Foundation"
},
{
"award": [
"NA"
],
"name": "FastGrants"
}
],
"indexed": {
"date-parts": [
[
2022,
3,
30
]
],
"date-time": "2022-03-30T21:41:59Z",
"timestamp": 1648676519806
},
"is-referenced-by-count": 0,
"issn-type": [
{
"type": "print",
"value": "0028-4793"
},
{
"type": "electronic",
"value": "1533-4406"
}
],
"issued": {
"date-parts": [
[
2022,
3,
30
]
]
},
"language": "en",
"license": [
{
"URL": "http://www.nejmgroup.org/legal/terms-of-use.htm",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2022,
3,
30
]
],
"date-time": "2022-03-30T00:00:00Z",
"timestamp": 1648598400000
}
}
],
"link": [
{
"URL": "http://www.nejm.org/doi/pdf/10.1056/NEJMoa2115869",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "150",
"original-title": [],
"prefix": "10.1056",
"published": {
"date-parts": [
[
2022,
3,
30
]
]
},
"published-online": {
"date-parts": [
[
2022,
3,
30
]
]
},
"publisher": "Massachusetts Medical Society",
"reference-count": 21,
"references-count": 21,
"relation": {},
"resource": {
"primary": {
"URL": "http://www.nejm.org/doi/10.1056/NEJMoa2115869"
}
},
"score": 1,
"short-container-title": [
"N Engl J Med"
],
"short-title": [],
"source": "Crossref",
"subject": [
"General Medicine"
],
"subtitle": [],
"title": [
"Effect of Early Treatment with Ivermectin among Patients with Covid-19"
],
"type": "journal-article"
}