
 Control
Control{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Aug 3 |
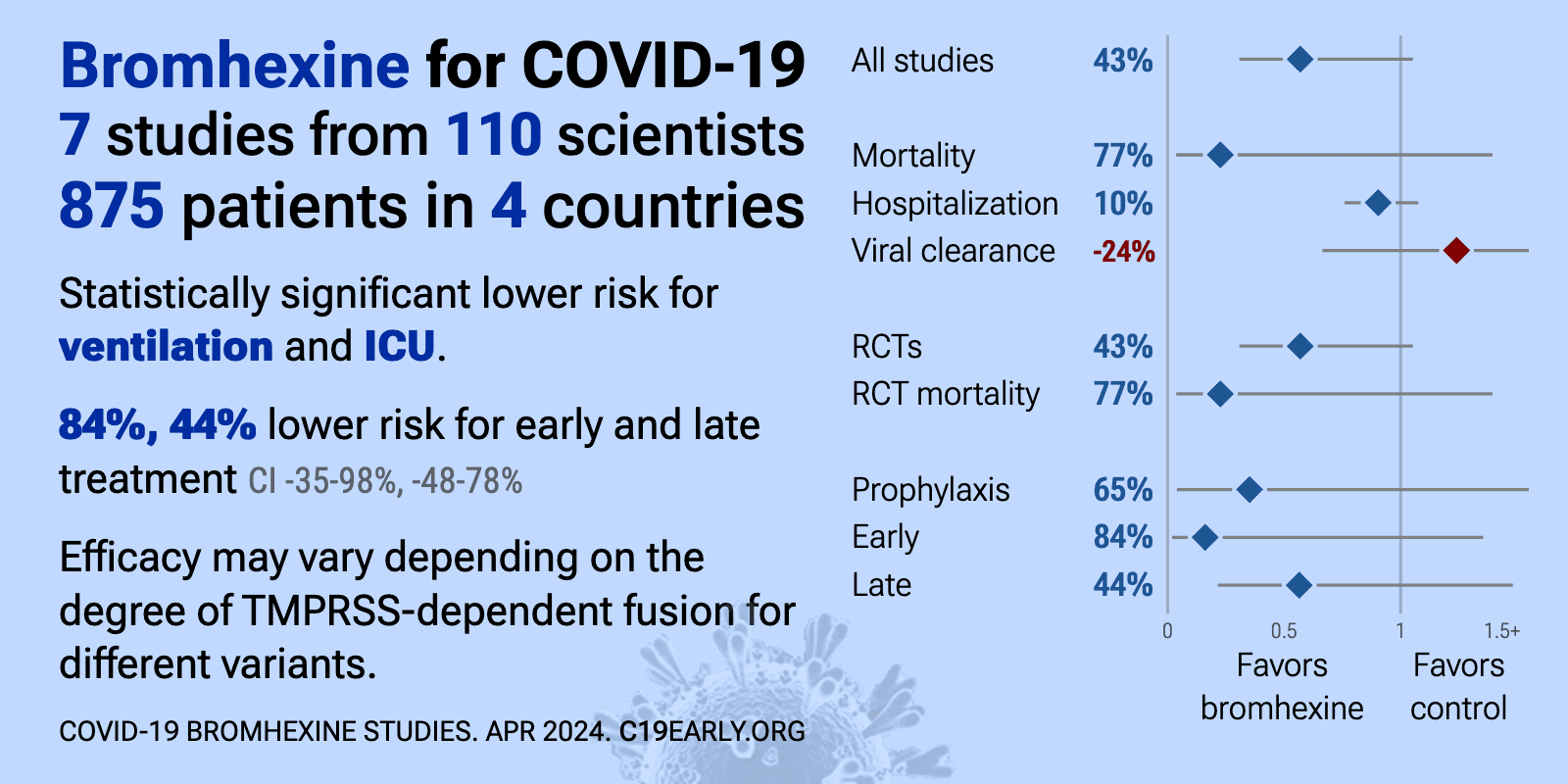
Bromhexine for COVID-19: real-time meta-analysis of 7 studies (Version 22) | |
| Significantly lower risk is seen for ventilation and ICU admission. 3 studies from 3 independent teams in 2 countries show significant benefit. Meta-analysis using the most serious outcome reported shows 43% [-5‑69%] lower risk.. | ||
Jan 12 |
et al., Frontiers in Pharmacology, doi:10.3389/fphar.2025.1745277 | Bromhexine inhibits SARS-CoV-2 Omicron and variant pseudovirus infection via ACE2-targeted mechanisms |
| In vitro study showing that bromhexine inhibits SARS-CoV-2 Omicron and variant pseudovirus infection via ACE2-targeted mechanisms. Authors found that the antiviral mechanism involves destabilization of the SARS-CoV-2 spike-ACE2 interface,.. | ||
Apr 15 2025 |
, V., MDPI AG, doi:10.20944/preprints202504.1220.v1 | Prevention and Treatment of COVID-19 and Influenza with Bromhexine and High Doses of Colchicine |
| Review of bromhexine and colchicine for COVID-19 and influenza prevention and treatment. | ||
Nov 21 2024 |
et al., Discover Molecules, doi:10.1007/s44345-024-00005-5 | Exploring potential therapeutic candidates against COVID-19: a molecular docking study |
| In silico study showing potential inhibition of SARS-CoV-2 proteins by various compounds including dactinomycin, itraconazole, ivermectin, vitamin D, quercetin, curcumin, montelukast, bromhexine, hesperidin, EGCG and raloxifene. Authors p.. | ||
Oct 25 2024 |
et al., Immunity, Inflammation and Disease, doi:10.1002/iid3.70438 | COVID‐19 Prophylactic Effect of Bromhexine Hydrochloride |
| Retrospective 125 outpatients showing reduced COVID-19 infection rates with prophylactic bromhexine hydrochloride (BRH) use during 2021-2022 COVID waves in Bulgaria. Prior to BRH prophylaxis, 62% of participants reported confirmed COVID-1.. | ||
Mar 14 2024 |
et al., eClinicalMedicine, 10.1016/j.eclinm.2024.102517 | Early treatment with fluvoxamine, bromhexine, cyproheptadine, and niclosamide to prevent clinical deterioration in patients with symptomatic COVID-19: a randomized clinical trial |
| 98% lower ventilation (p<0.0001), 100% lower need for oxygen therapy (p<0.0001), 98% lower hospitalization (p<0.0001), and 55% lower long COVID (p<0.0001). RCT 995 outpatients showing significantly lower progression with early treatment within 48 hours using fluvoxamine, fluvoxamine+bromhexine, fluvoxamine+cyproheptadine, and niclosamide+bromhexine. 70% of patients received treatment within .. | ||
Dec 14 2023 |
et al., Heliyon, doi:10.1016/j.heliyon.2023.e23662 | Association of genetic polymorphisms with COVID-19 infection and outcomes: An updated meta-analysis based on 62 studies |
| Meta-analysis of 62 studies with 19,600 COVID-19 cases showing certain genetic polymorphisms associated with COVID-19 infection risk, severity, and mortality. Specifically, the ACE I/D polymorphism was associated with lower COVID-19 infec.. | ||
Oct 20 2023 |
, V., Pharmacia, doi:10.3897/pharmacia.70.e112550 | Comparison of treatment of COVID-19 with inhaled bromhexine, higher doses of colchicine and hymecromone with WHO-recommended paxlovid, molnupiravir, remdesivir, anti-IL-6 receptor antibodies and baricitinib |
| Review of treatment of COVID-19 with inhaled bromhexine, higher doses of colchicine and hymecromone compared to WHO-recommended paxlovid, molnupiravir, remdesivir, anti-IL-6 receptor antibodies, and baricitinib. The author argues that the.. | ||
Jan 3 2023 |
et al., Research Square, doi:10.21203/rs.3.rs-2309373/v2 | Evaluation of the recovery rate and prevention of hospitalization among covid-19 outpatients: a randomized clinical trial comparing N-acetylcysteine with Bromhexine |
| 93% lower mortality (p=0.01), 88% lower hospitalization (p<0.0001), and 28% faster recovery (p<0.0001). RCT 225 outpatients in Iran showing lower mortality and hospitalization, and faster recovery with N-acetylcysteine and bromhexine. Baseline information per group is not provided, Figure 1 has the control group hospitalization status switc.. | ||
Dec 26 2022 |
et al., bioRxiv, doi:10.1101/2022.12.23.521817 | In Vitro Inhibition of SARS-CoV-2 Infection by Bromhexine hydrochloride |
| In vitro study showing that bromhexine inhibits SARS-CoV-2 infection and replication in vitro by blocking the host cell protease TMPRSS2. | ||
Dec 24 2022 |
et al., Journal of Clinical Medicine, doi:10.3390/jcm12010142 | Efficacy of Bromhexine versus Standard of Care in Reducing Viral Load in Patients with Mild-to-Moderate COVID-19 Disease Attended in Primary Care: A Randomized Open-Label Trial |
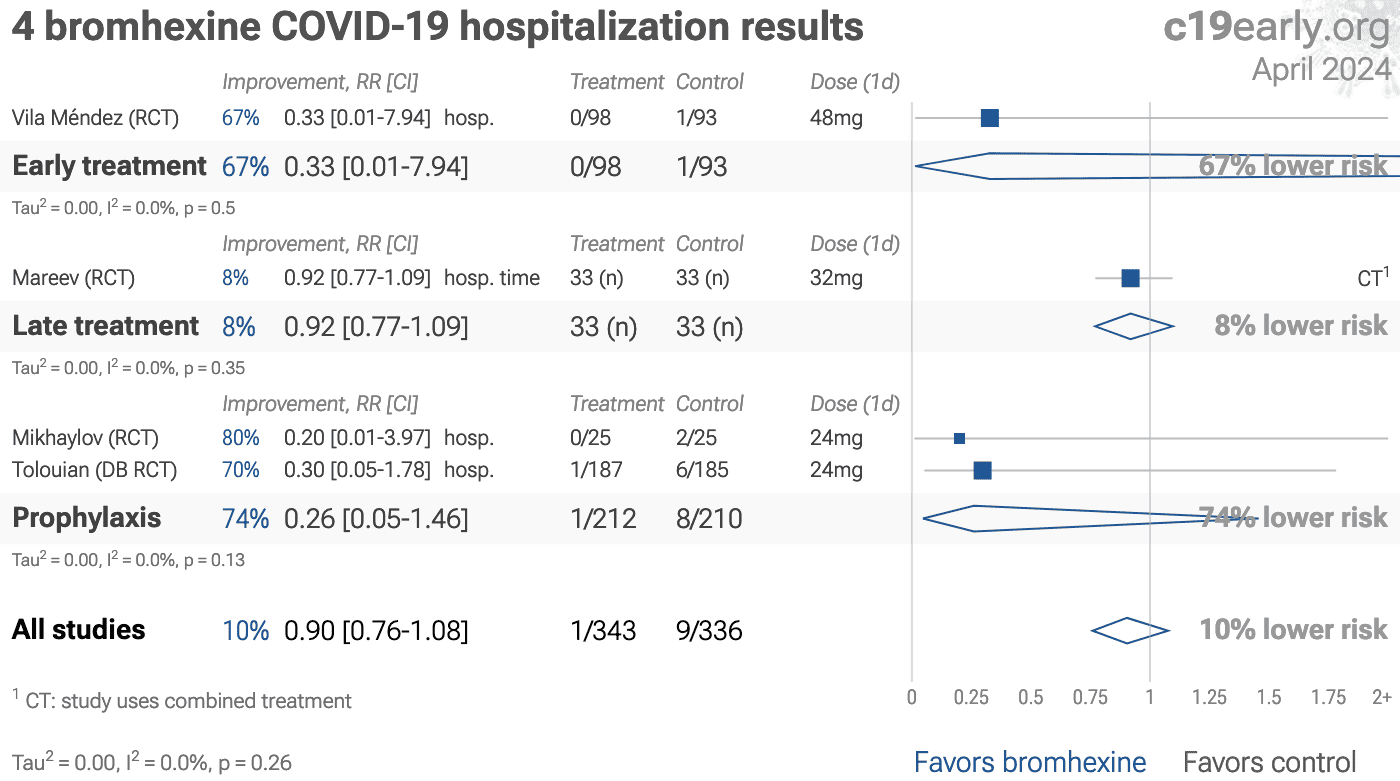
| 67% lower hospitalization (p=0.49) and 7% worse viral clearance (p=0.82). RCT 191 low risk (no mortality) outpatients in Spain, showing no significant differences with bromhexine. Authors note that "statistical differences between the study groups were observed in the percentage of patients treated with.. | ||
Oct 18 2022 |
et al., Journal of Clinical Medicine, doi:10.3390/jcm11206138 | Early Outpatient Treatment of COVID-19: A Retrospective Analysis of 392 Cases in Italy |
| Retrospective 392 outpatients in Italy showing 0.2% mortality with early treatment, compared with >3% in Italy at the time. Treatment varied for individual patients and included HCQ, vitamin D, vitamin C, vitamin A, zinc, quercetin, bromh.. | ||
Jan 3 2022 |
et al., bioRxiv, doi:10.1101/2021.12.31.474653 | The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry |
| In vitro study showing that omicron can efficiently enter cells via the endosomal route, independent of TMPRSS2. | ||
Jan 3 2022 |
et al., medRxiv, doi:10.1101/2022.01.03.21268111 | The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism |
| In vitro study showing that the entry process for omicron has moved towards TMPRSS2-independent fusion, indicating that TMPRSS2 inhibitors may be less effective for omicron. | ||
Dec 20 2021 |
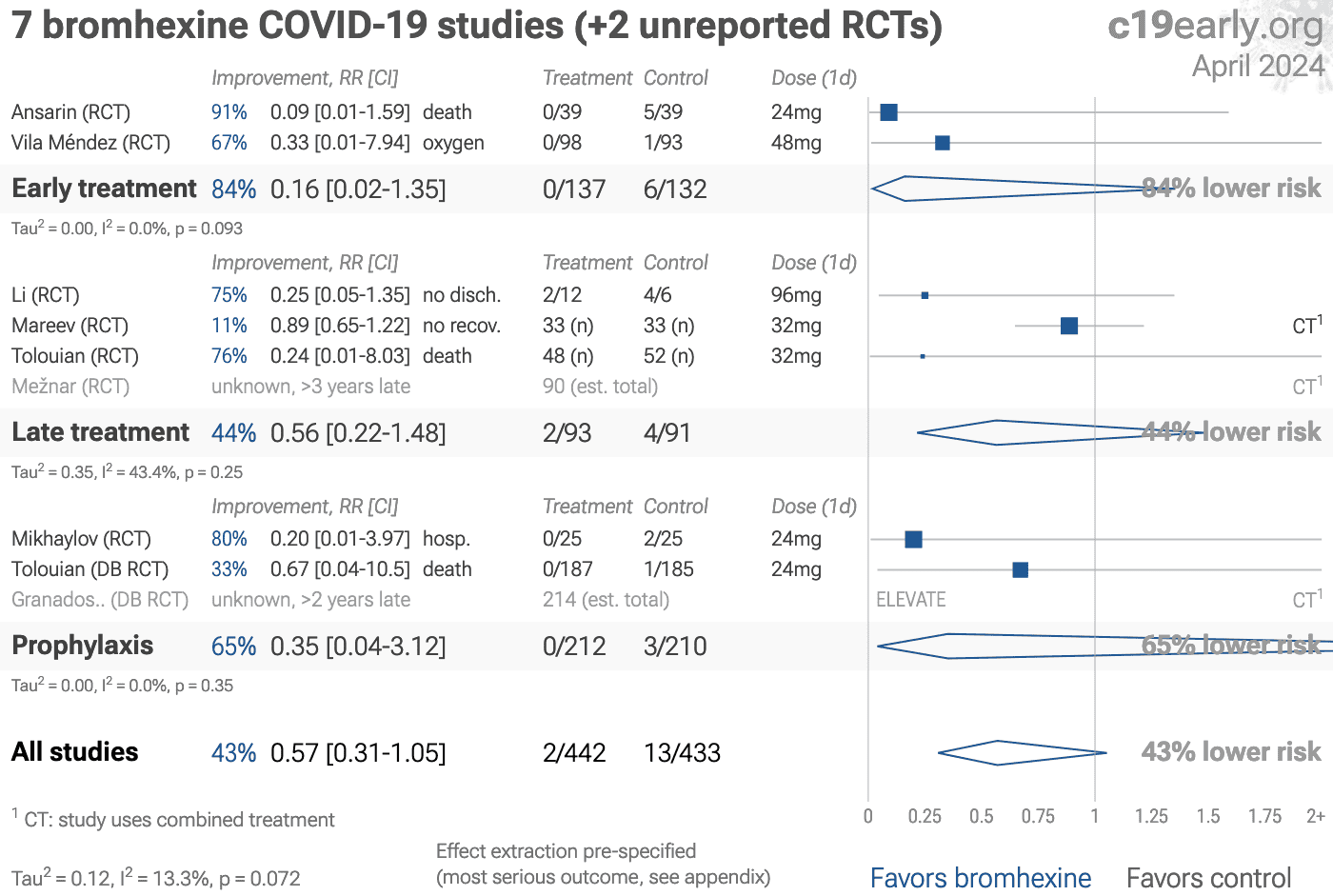
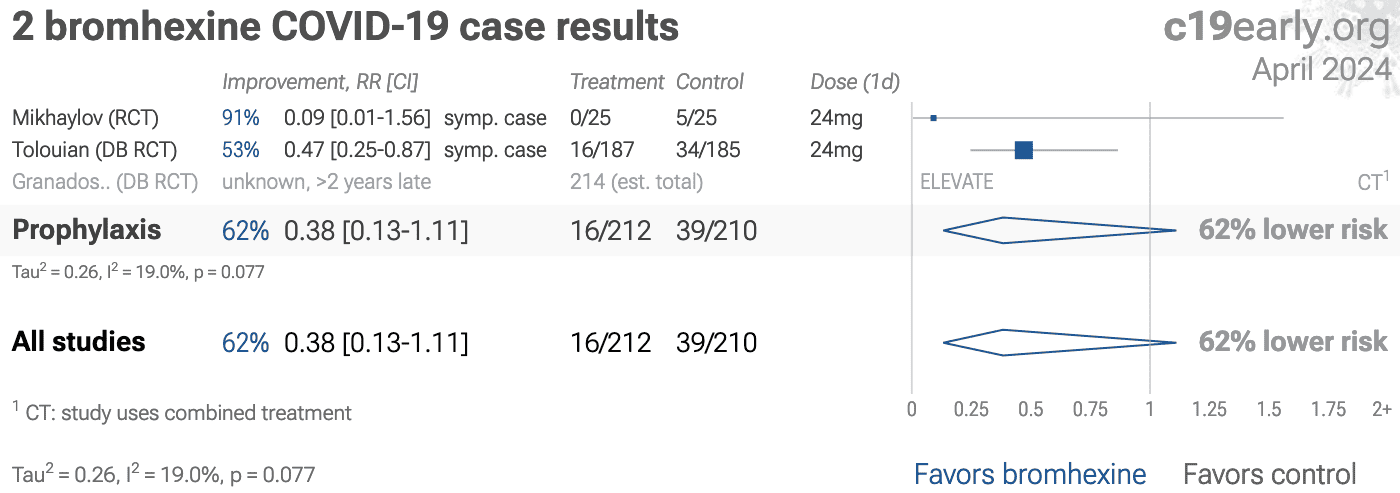
et al., SSRN, doi:10.2139/ssrn.3989 | Bromhexine, for Post Exposure COVID-19 Prophylaxis: A Randomized, Double-Blind, Placebo Control Trial |
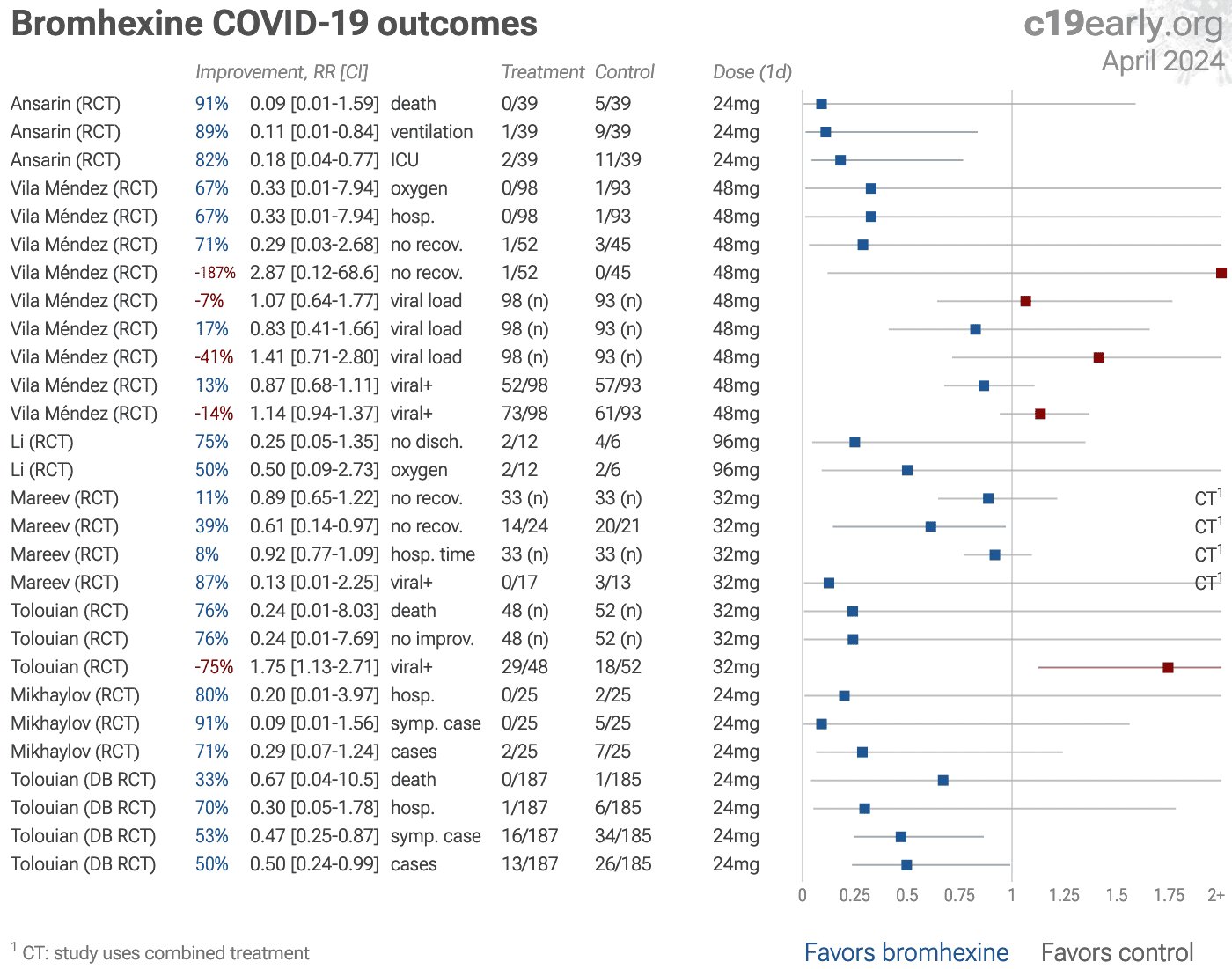
| 70% lower hospitalization (p=0.15), 53% fewer symptomatic cases (p=0.007), and 50% fewer cases (p=0.03). PEP RCT with 372 close contacts of COVID+ patients, 187 treated with bromhexine, showing significantly lower cases with treatment. IRCT20120703010178N22. | ||
Jun 30 2021 |
et al., BMJ Open, doi:10.1136/bmjopen-2020-045190 | New prophylaxis regimen for SARS-CoV-2 infection in health professionals with low doses of hydroxychloroquine and bromhexine: a randomised, double-blind placebo clinical trial (ELEVATE Trial) |
| Estimated 214 participant bromhexine + HCQ prophylaxis RCT with results not reported over 5 years after estimated completion. | ||
Apr 30 2021 |
et al., Frontiers in Molecular Biosciences, doi:10.3389/fmolb.2021.666626 | Computational Identification of a Putative Allosteric Binding Pocket in TMPRSS2 |
| In silico study of TMPRSS2 inhibition by camostat, nafamostat, and bromhexine, suggesting allosteric binding for bromhexine, compared to camostat and nafamostat which bind to the active site of TMPRSS2 forming covalent adducts. | ||
Mar 15 2021 |
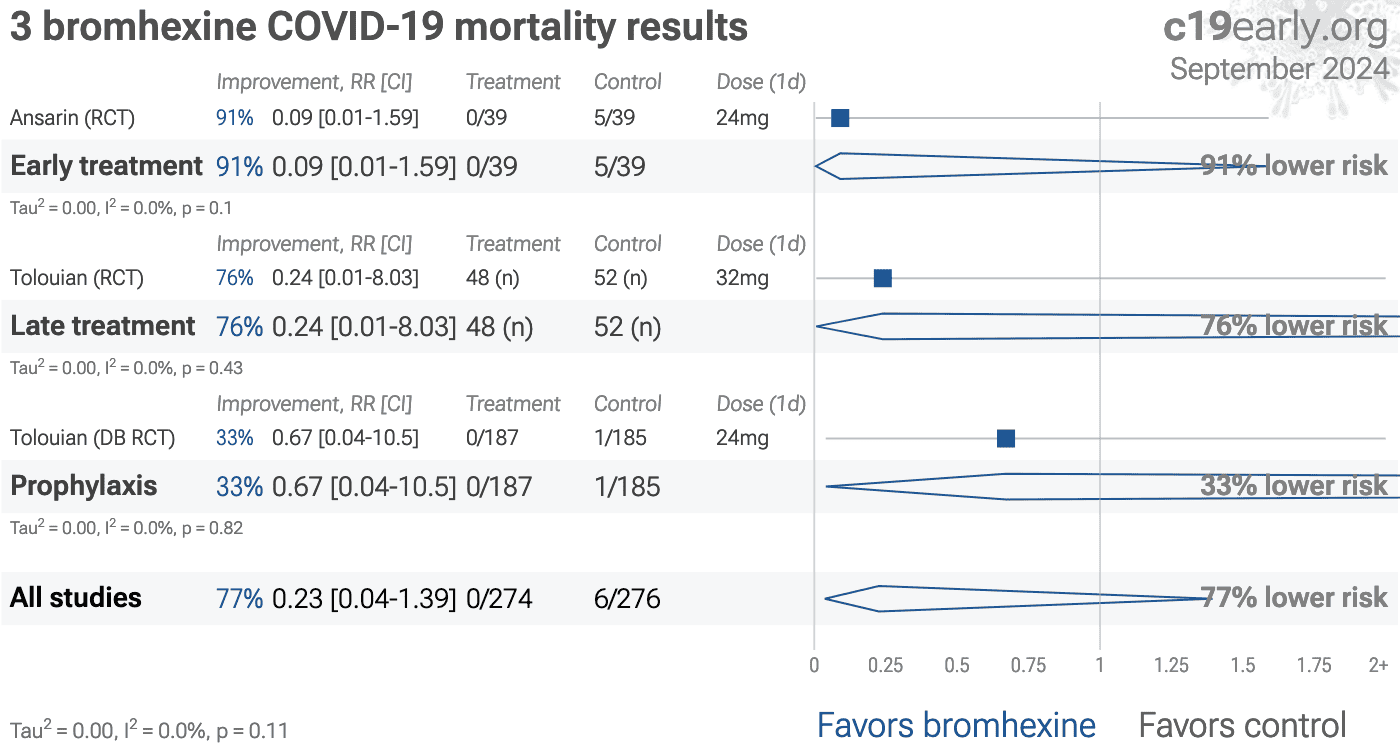
et al., J. Investig. Med., doi:10.1136/jim-2020-001747 | Effect of bromhexine in hospitalized patients with COVID-19 |
| 76% lower mortality (p=0.43), 76% greater improvement (p=0.43), and 75% worse viral clearance (p=0.02). Small RCT with 100 patients, 48 with bromhexine added to SOC, showing slower viral- conversion but lower mortality and greater clinical improvement with bromhexine (not statistically significant with few deaths and very high recovery). Th.. | ||
Mar 8 2021 |
et al., Interdisciplinary Perspectives on Infectious Diseases, doi:10.1155/2022/4693121 (date from preprint) | Bromhexine Hydrochloride Prophylaxis of COVID-19 for Medical Personnel: A Randomized Open-Label Study |
| 91% fewer symptomatic cases (p=0.05) and 71% fewer cases (p=0.14). Small prophylaxis RCT with 25 treatment and 25 control health care workers, showing lower PCR+, symptomatic cases, and hospitalization with treatment, although not statistically significant with the small sample size. | ||
Jan 31 2021 |
et al., Journal of Biological Chemistry, doi:10.1016/j.jbc.2021.100701 | Inhibition of acid sphingomyelinase by ambroxol prevents SARS-CoV-2 entry into epithelial cells |
| In vitro study showing that ambroxol (a metabolite of bromhexine) inhibits SARS-CoV-2 infection. | ||
Dec 31 2020 |
et al., Current Medical and Drug Research | The potential role of Bromhexine in the management of COVID-19: Decipher and a real game-changer |
| Review article noting that bromhexine is a TMPRSS2 inhibitor with greater effect in lung tissue and attenuates the entry and proliferation of SARS-CoV-2. | ||
Dec 3 2020 |
et al., Кардиология, doi:10.18087/cardio.2020.11.n1440 | Results of Open-Label non-Randomized Comparative Clinical Trial: “BromhexIne and Spironolactone for CoronаvirUs Infection requiring hospiTalization (BISCUIT) |
| 11% improved recovery (p=0.47), 8% shorter hospitalization (p=0.35), and 87% improved viral clearance (p=0.08). Prospective 103 PCR+ patients in Russia, 33 treated with bromexhine+spironolactone, showing lower PCR+ at day 10 or hospitalization >10 days with treatment. Bromhexine 8mg 4 times daily, spironolactone 25-50 mg/day for 10 days. | ||
Sep 3 2020 |
et al., Clinical and Translational Science, doi:10.1111/cts.12881 | Bromhexine Hydrochloride Tablets for the Treatment of Moderate COVID-19: An Open-Label Randomized Controlled Pilot Study |
| 75% higher hospital discharge (p=0.11) and 3% slower recovery. Tiny RCT with 12 bromhexine and 6 control patients showing non-statistically significant improvements in chest CT, need for oxygen therapy, and discharge rate within 20 days. Authors recommend a larger scale trial. | ||
Jul 31 2020 |
et al., NCT04355026 | Use of Bromhexine and Hydroxychloroquine for Treatment of COVID-19 Pneumonia |
| Estimated 90 patient bromhexine + HCQ late treatment RCT with results not reported over 6 years after estimated completion. | ||
Jul 19 2020 |
et al., Bioimpacts, doi:10.34172/bi.2020.27 | Effect of bromhexine on clinical outcomes and mortality in COVID-19 patients: A randomized clinical trial |
| 91% lower mortality (p=0.05), 89% lower ventilation (p=0.01), and 82% lower ICU admission (p=0.01). RCT with 39 bromhexine and 39 control patients showing lower mortality, intubation, and ICU admission with treatment. The treatment group received bromhexine hydrochloride 8 mg three times a day for two weeks. All patients received SOC in.. | ||
May 26 2020 |
et al., Internal and Emergency Medicine, doi:10.1007/s11739-020-02383-3 | Potential new treatment strategies for COVID-19: is there a role for bromhexine as add-on therapy? |
| Proposal to use bromhexine to inhibit TMPRSS2-specific viral entry for prophylaxis and treatment of COVID-19. | ||
Apr 30 2020 |
et al., Pharmacol. Res., doi:10.1016/j.phrs.2020.104853 | Possible use of the mucolytic drug, bromhexine hydrochloride, as a prophylactic agent against SARS-CoV-2 infection based on its action on the Transmembrane Serine Protease 2 |
| Note on the potential use of bromhexine hydrochloride for prophylaxis of SARS-CoV-2, based on the role of TMPRSS2 in SARS-CoV-2 infection, and the TMPRSS2 inhibition of bromhexine hydrochloride. | ||
Apr 22 2020 |
et al., Pharmacol Res., doi:10.1016/j.phrs.2020.104837 | Repurposing the mucolytic cough suppressant and TMPRSS2 protease inhibitor bromhexine for the prevention and management of SARS-CoV-2 infection |
| Proposal to use bromhexine for prophylaxis and treatment of COVID-19 based on TMPRSS2 inhibition, widespread clinical use, and supporting pharmacokinetic and safety data. | ||
Mar 5 2020 |
et al., Cell, doi:10.1016/j.cell.2020.02.052 | SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor |
| In vitro study showing that SARS-CoV-2 uses ACE2 for entry and TMPRSS2 for S protein priming, and that TMPRSS2 inhibitor camostat blocked entry and may be an effective treaetment. | ||
References