COVID-19 treatment: real-time analysis of 6,688 studies
| Papantoniou | 1,939 patient sleep study: 29% lower long COVID (p=0.02) |
| Luxi | Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential.. |
| Du | Review of drug repurposing as a broad-spectrum antiviral strategy against coronaviruses, with a focus on SARS-CoV-2/COVID-19. Authors systematically.. |
{kind=link}

c19early.org
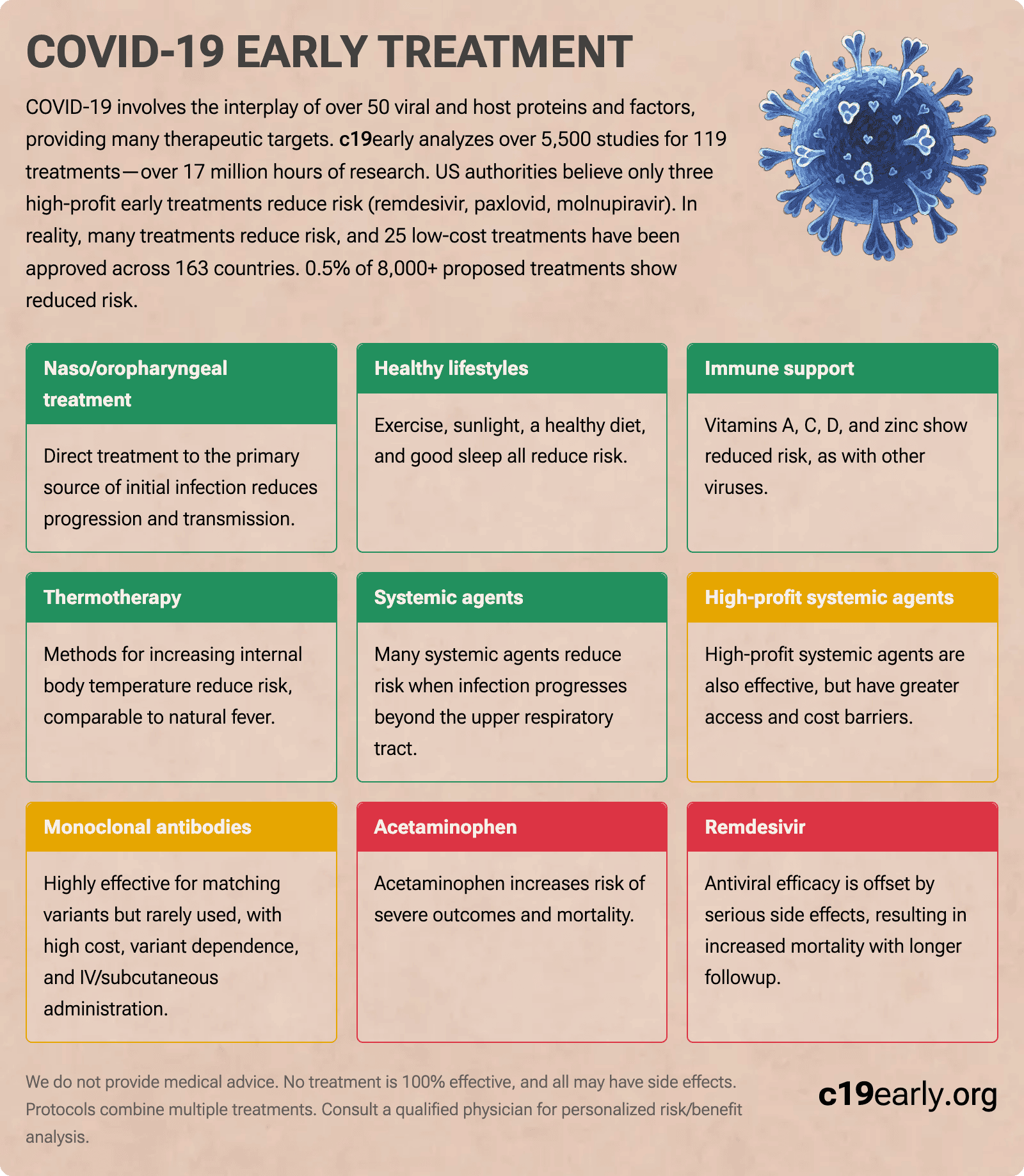
COVID-19 involves the interplay of 500+ viral and host proteins and factors, providing many therapeutic targets.
c19early analyzes 6,600+ studies for 226 treatments—over 17 million hours of research.
Only three high-profit early treatments are approved in the US.
In reality, many treatments reduce risk,
with 25 low-cost treatments approved across 163 countries.
-
Naso/
oropharyngeal treatment Effective Treatment directly to the primary source of initial infection. -
Healthy lifestyles Protective Exercise, sunlight, a healthy diet, and good sleep all reduce risk.
-
Immune support Effective Vitamins A, C, D, and zinc show reduced risk, as with other viruses.
-
Thermotherapy Effective Methods for increasing internal body temperature, enhancing immune system function.
-
Systemic agents Effective Many systemic agents reduce risk, and may be required when infection progresses.
-
High-profit systemic agents Conditional Effective, but with greater access and cost barriers.
-
Monoclonal antibodies Limited Utility Effective but rarely used—high cost, variant dependence, IV/SC admin.
-
Acetaminophen Harmful Increased risk of severe outcomes and mortality.
-
Remdesivir Harmful Increased mortality with longer followup. Increased kidney and liver injury, cardiac disorders.
{kind=link}
{kind=link}
{kind=link}
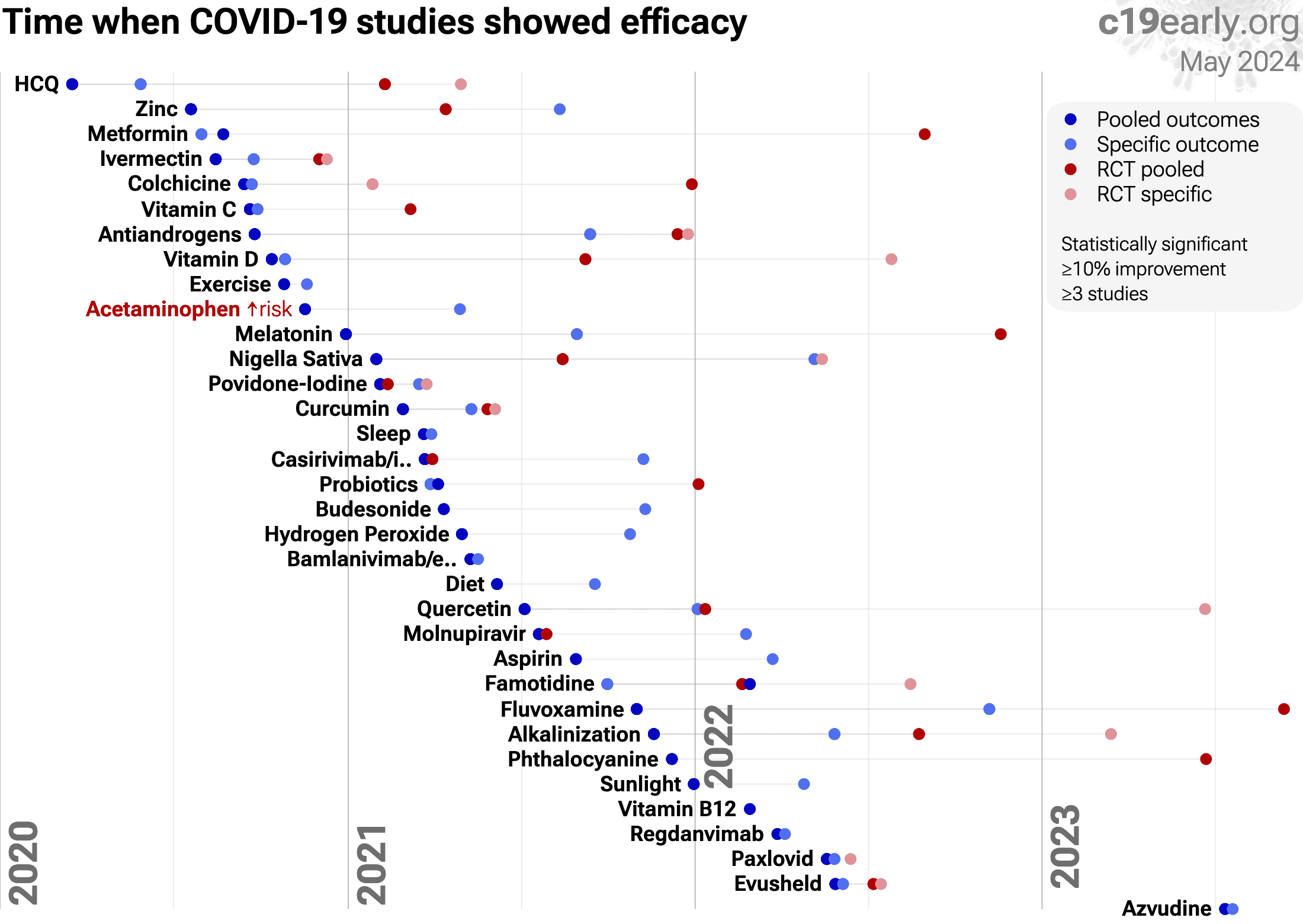
Timeline for when studies showed efficacy - details and limitations.
0.5% of treatments show efficacy.
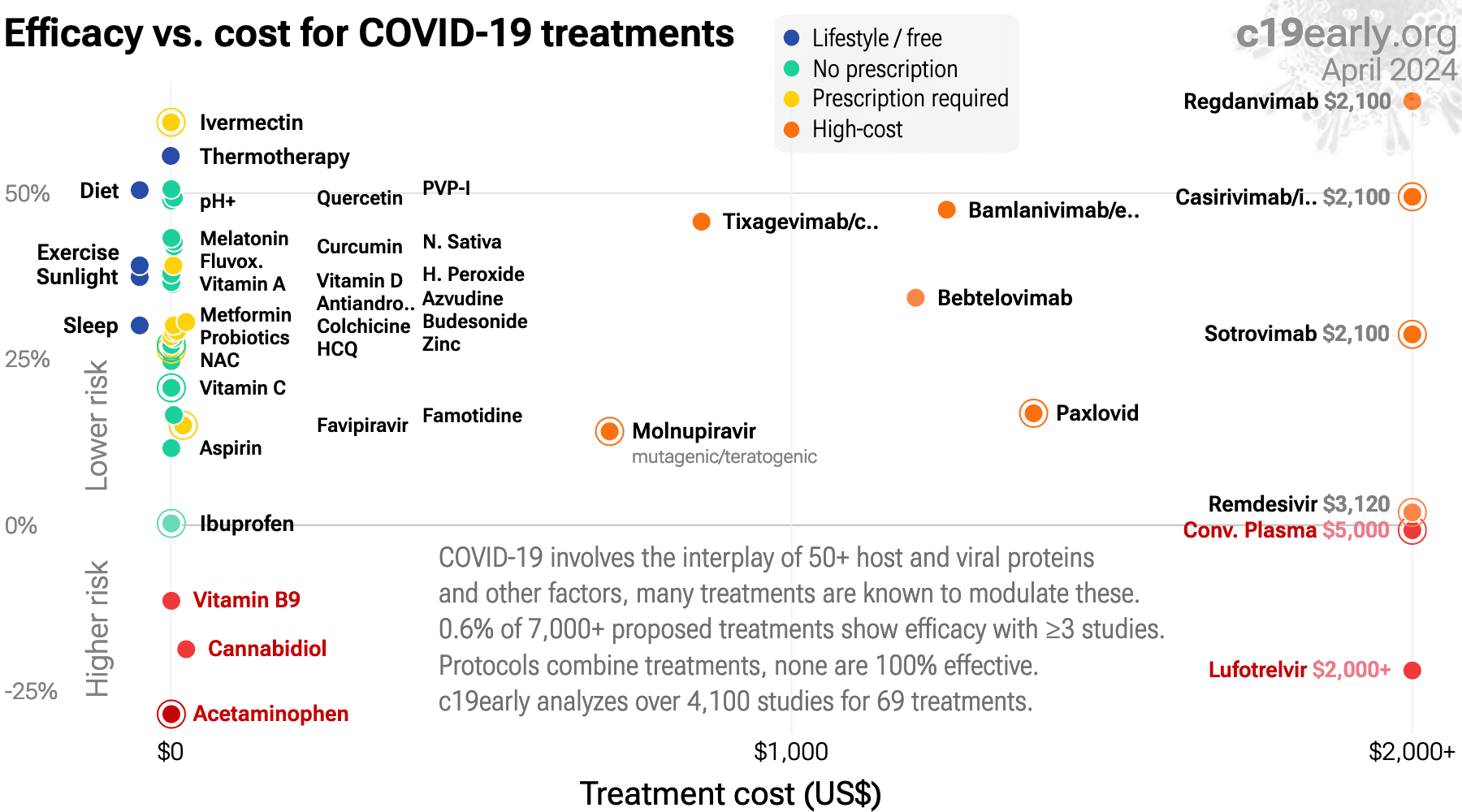
Treatment cost times median NNT - details and limitations.
0.5% of treatments show efficacy.
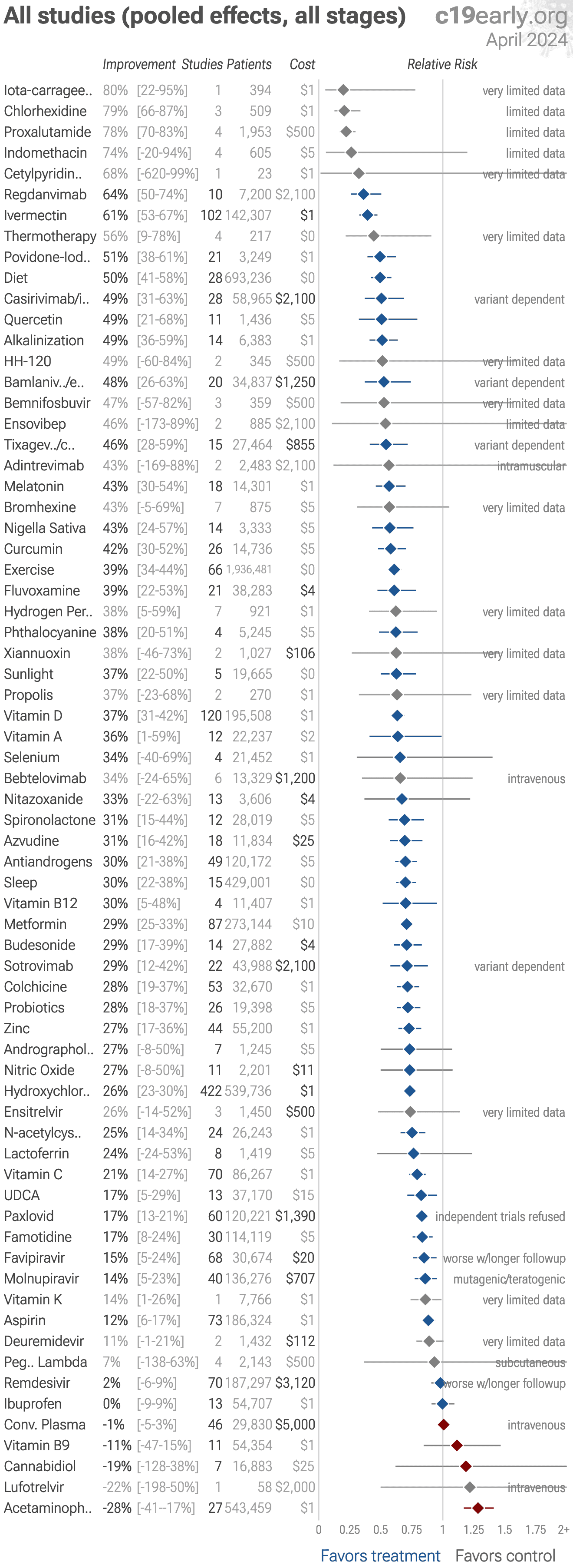
All clinical results for selected treatments. 0.5% of treatments show efficacy.
{kind=link}
{kind=link}
Top journals that accept positive studies for low cost treatments:
Nutrients,
Scientific Reports,
PLOS ONE,
International Journal of Infectious Diseases,
Frontiers in Medicine,
Cureus,
more...
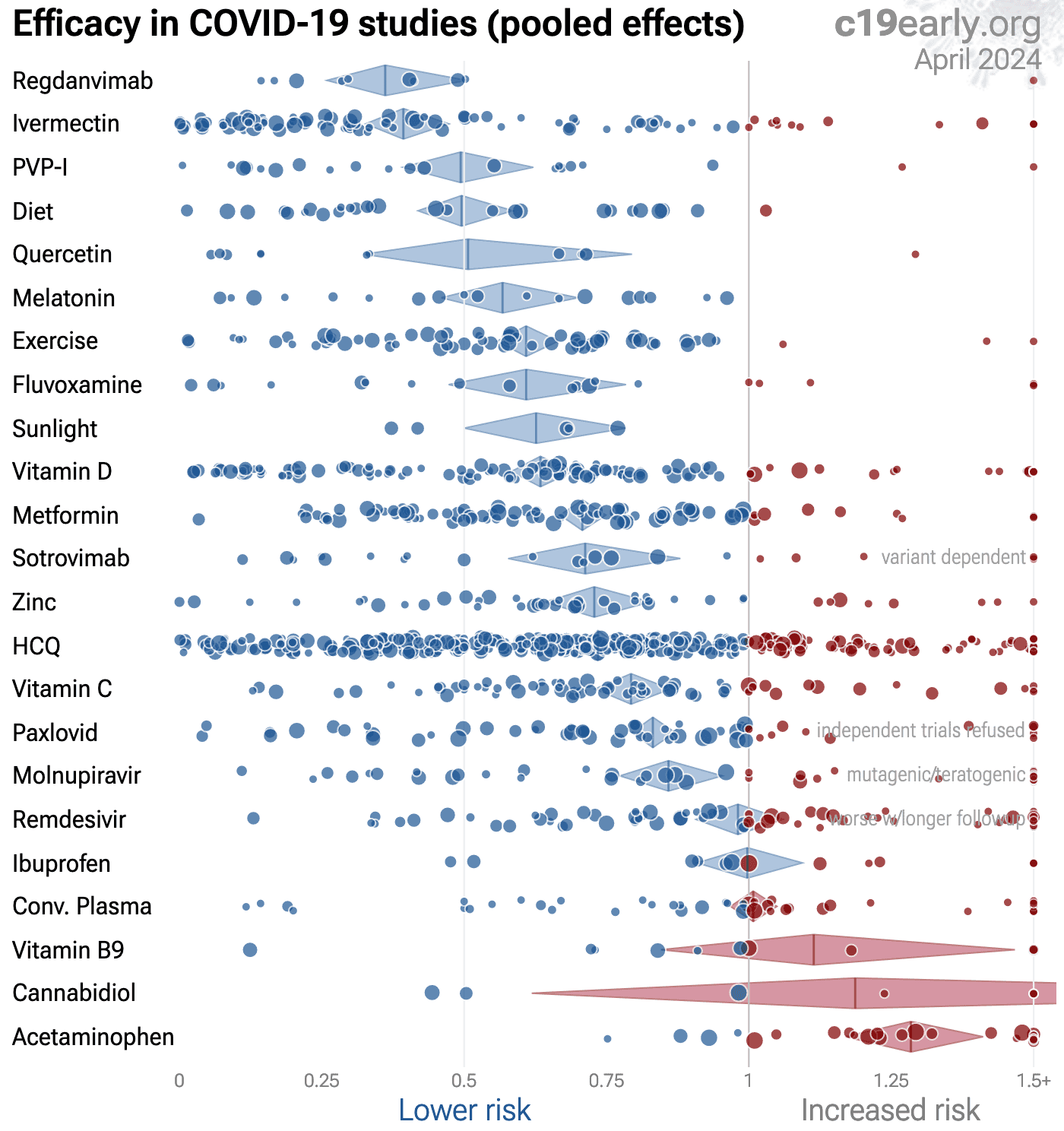
| Random-effects meta-analysis of all studies (pooled effects, all stages). Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all stages and outcomes depend on the distribution of stages and outcomes tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage and outcome analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
| Random-effects meta-analysis of early treatment studies (pooled effects). Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all outcomes are affected by the distribution of outcomes tested, please see detail pages for specific outcome analysis. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
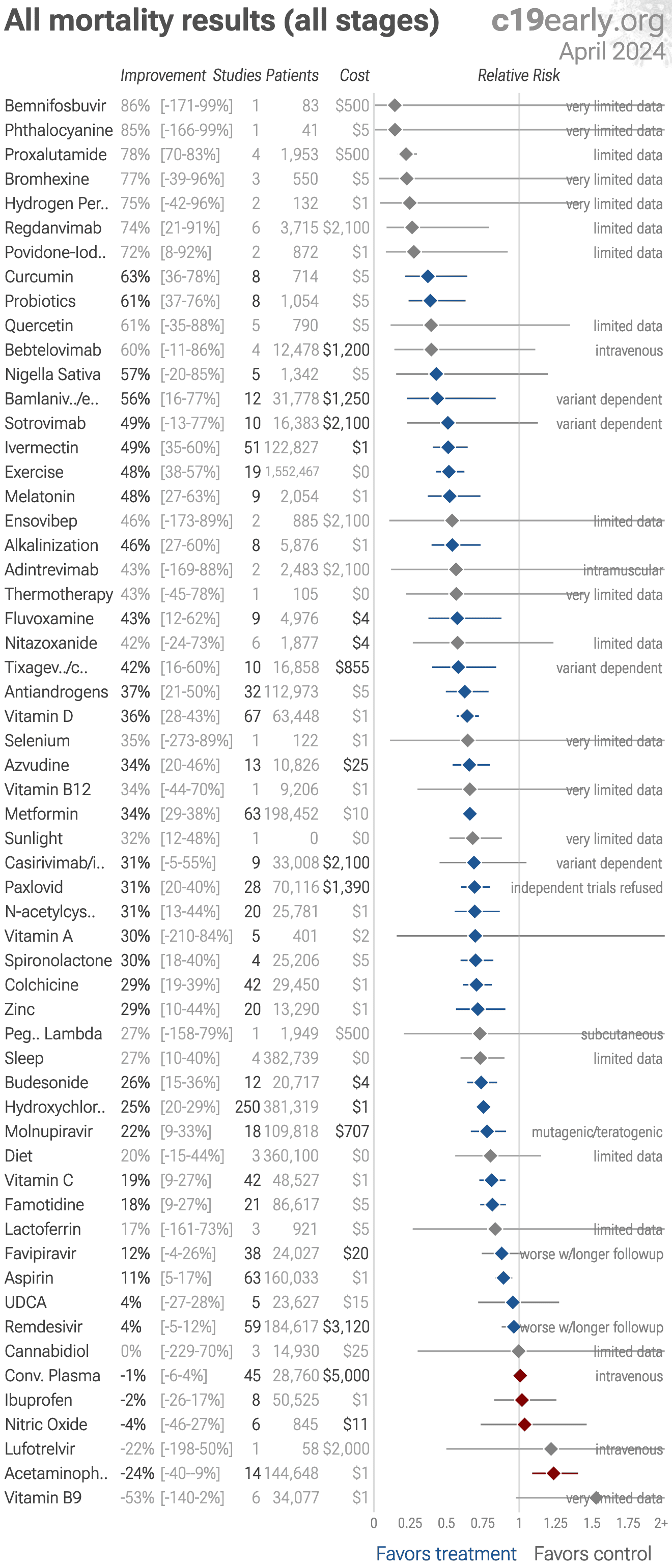
| Random-effects meta-analysis of all mortality results (all stages). Treatments with ≤3 studies with distinct authors or with <25 control events are shown in grey. Pooled results across all stages depend on the distribution of stages tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
| Random-effects meta-analysis of early treatment mortality results. Treatments with ≤3 studies with distinct authors or with <25 control events are shown in grey. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
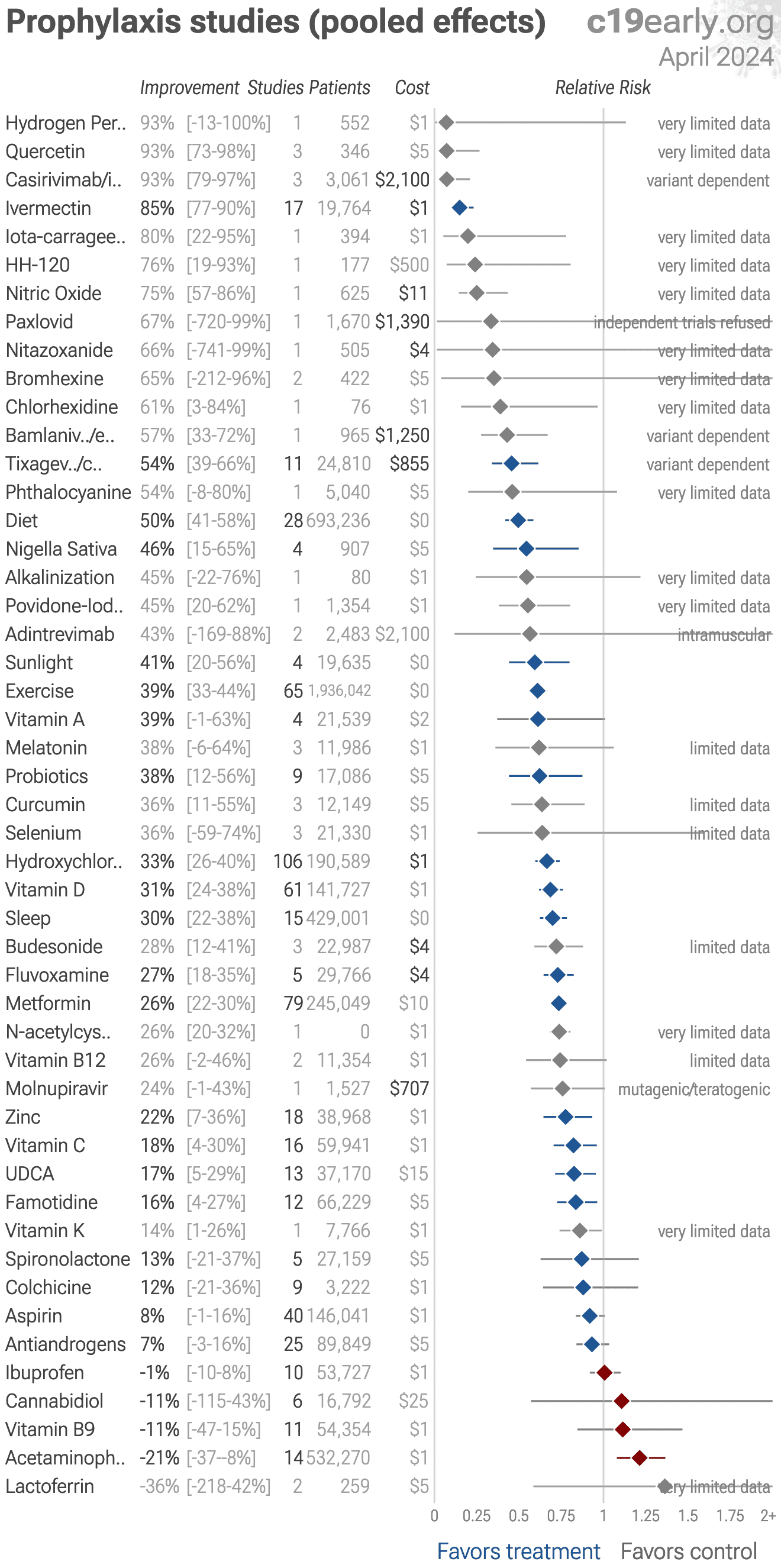
| Random-effects meta-analysis of prophylaxis studies (pooled effects). Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all outcomes are affected by the distribution of outcomes tested, please see detail pages for specific outcome analysis. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
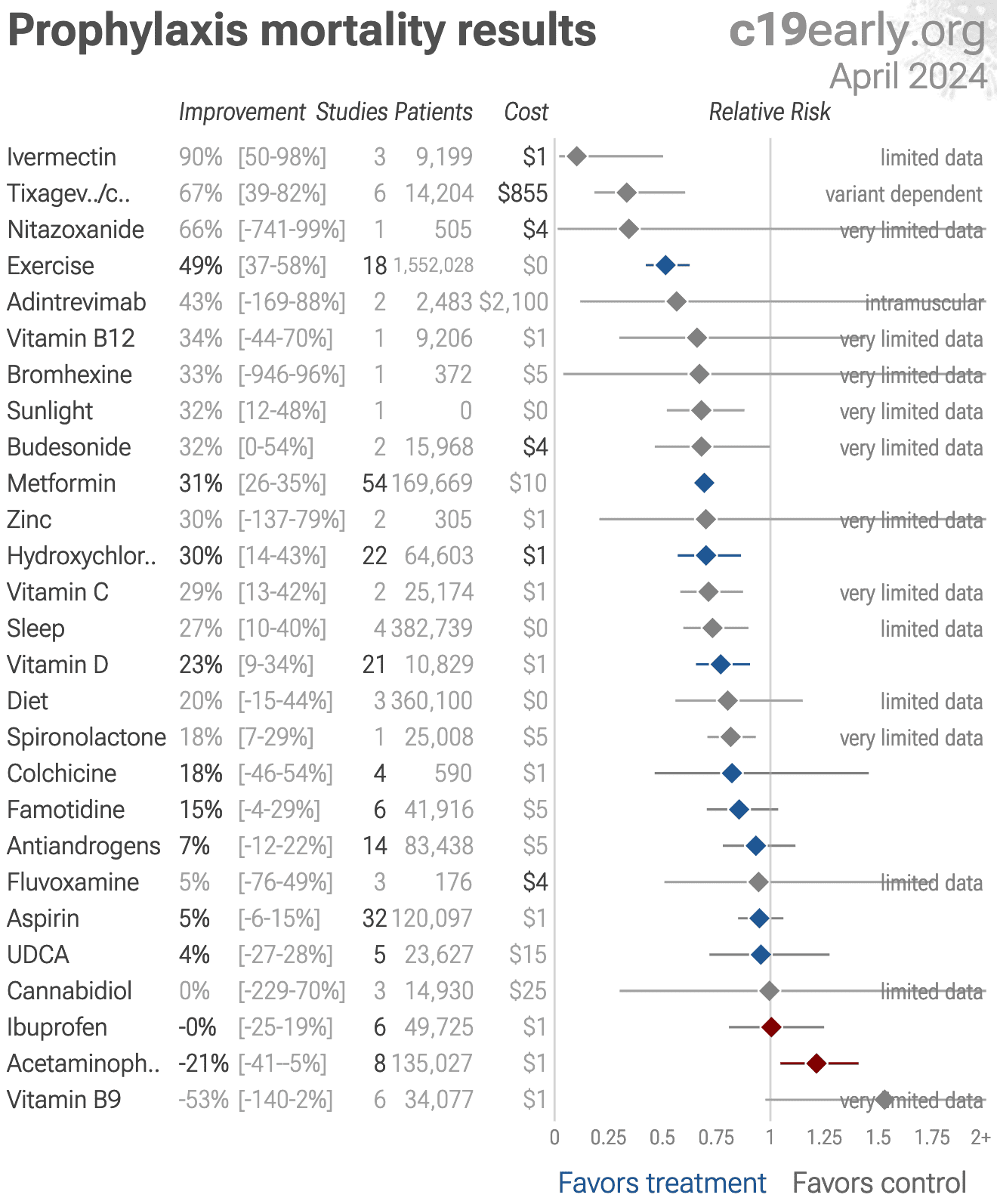
| Random-effects meta-analysis of prophylaxis mortality results. Treatments with ≤3 studies with distinct authors or with <25 control events are shown in grey. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
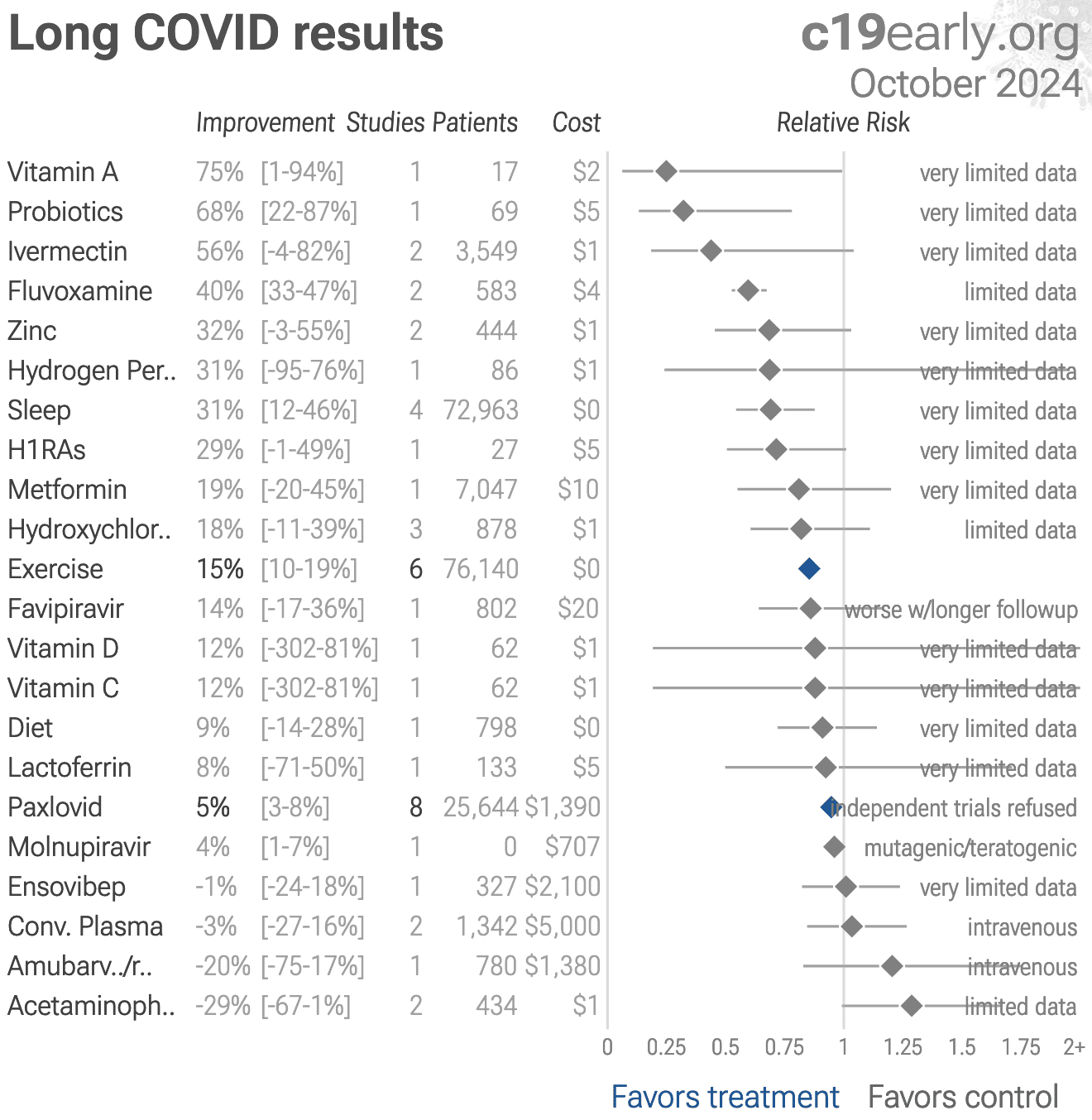
| Random-effects meta-analysis of long covid results. Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all stages and outcomes depend on the distribution of stages and outcomes tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage and outcome analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
| Random-effects meta-analysis of transmission results. Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all stages and outcomes depend on the distribution of stages and outcomes tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage and outcome analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LATE TREATMENT | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. David Uip (*) | Brazil | 2,200 | 38.6% (850) | 2.5% (54) |
| Dr. Jake Scott (**) | USA | 1,000 | 10.0% (100) | |
| Average | 38.6% | 6.2% | ||
| EARLY TREATMENT PROTOCOLS - 40 physicians/teams | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. Roberto Alfonso Accinelli 0/360 deaths for treatment within 3 days |
Peru | 1,265 | 0.6% (7) | |
| Dr. Mohammed Tarek Alam patients up to 84 years old |
Bangladesh | 100 | 0.0% (0) | |
| Dr. Oluwagbenga Alonge | Nigeria | 310 | 0.0% (0) | |
| Dr. Raja Bhattacharya up to 88yo, 81% comorbidities |
India | 148 | 1.4% (2) | |
| Dr. Flavio Cadegiani | Brazil | 3,450 | 0.1% (4) | 0.0% (0) |
| Dr. Alessandro Capucci | Italy | 350 | 4.6% (16) | |
| Dr. Shankara Chetty | South Africa | 8,000 | 0.0% (0) | |
| Dr. Deborah Chisholm | USA | 100 | 0.0% (0) | |
| Dr. Ryan Cole | USA | 400 | 0.0% (0) | 0.0% (0) |
| Dr. Marco Cosentino earlier treatment results were better |
Italy | 392 | 6.4% (25) | 0.3% (1) |
| Dr. Jeff Davis | USA | 6,000 | 0.0% (0) | |
| Dr. Dhanajay | India | 500 | 0.0% (0) | |
| Dr. Bryan Tyson & Dr. George Fareed | USA | 20,000 | 0.0% (6) | 0.0% (4) |
| Dr. Raphael Furtado | Brazil | 170 | 0.6% (1) | 0.0% (0) |
| Rabbi Yehoshua Gerzi | Israel | 860 | 0.1% (1) | 0.0% (0) |
| Dr. Heather Gessling | USA | 1,500 | 0.1% (1) | |
| Dr. Ellen Guimarães | Brazil | 500 | 1.6% (8) | 0.4% (2) |
| Dr. Syed Haider | USA | 4,000 | 0.1% (5) | 0.0% (0) |
| Dr. Mark Hancock | USA | 24 | 0.0% (0) | |
| Dr. Sabine Hazan | USA | 1,000 | 0.0% (0) | |
| Dr. Mollie James | USA | 3,500 | 1.1% (40) | 0.0% (1) |
| Dr. Roberta Lacerda | Brazil | 550 | 1.5% (8) | 0.4% (2) |
| Dr. Katarina Lindley | USA | 100 | 5.0% (5) | 0.0% (0) |
| Dr. Ben Marble | USA | 150,000 | 0.0% (4) | |
| Dr. Edimilson Migowski | Brazil | 2,000 | 0.3% (7) | 0.1% (2) |
| Dr. Abdulrahman Mohana | Saudi Arabia | 2,733 | 0.0% (0) | |
| Dr. Carlos Nigro | Brazil | 5,000 | 0.9% (45) | 0.5% (23) |
| Dr. Benoit Ochs | Luxembourg | 800 | 0.0% (0) | |
| Dr. Ortore | Italy | 240 | 1.2% (3) | 0.0% (0) |
| Dr. Valerio Pascua one patient already on oxygen died |
Honduras | 415 | 6.3% (26) | 0.2% (1) |
| Dr. Sebastian Pop | Romania | 300 | 0.0% (0) | |
| Dr. Brian Proctor | USA | 869 | 2.3% (20) | 0.2% (2) |
| Dr. Anastacio Queiroz | Brazil | 700 | 0.0% (0) | |
| Dr. Didier Raoult | France | 8,315 | 2.6% (214) | 0.1% (5) |
| Dr. Karin Ried up to 99yo, 73% comorbidities |
Turkey | 237 | 0.4% (1) | |
| Dr. Roman Rozencwaig patients up to 86 years old |
Canada | 80 | 0.0% (0) | |
| Dr. Vipul Shah | India | 8,000 | 0.1% (5) | |
| Dr. Silvestre Sobrinho | Brazil | 116 | 8.6% (10) | 0.0% (0) |
| Dr. Unknown | Brazil | 957 | 1.7% (16) | 0.2% (2) |
| Dr. Vladimir Zelenko | USA | 2,200 | 0.5% (12) | 0.1% (2) |
| Average | 2.2% | 0.1% | ||
Physicians using early combined treatment protocols had much lower
hospitalization and mortality rates compared with those following guidelines focusing on
late treatment.
Results are subject to selection and ascertainment bias and accurate analysis requires
details of the patient populations and followup, however the results are consistent across
many teams, and consistent with the extensive controlled clinical evidence showing a
significant reduction in risk with many early treatments, and complementary/synergistic
benefits with combined treatments.
(*) Dr. Uip reportedly prescribed early treatment for himself, but not for
patients1.
(**) Dr. Scott reports treating hundreds of patients and losing over a hundred,
but has not provided specific numbers2.
Dr. Scott reports following (and helping create) US guidelines.
| Papantoniou | 1,939 patients: 29% lower long COVID (p=0.02) |
| Luxi | Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential.. |
| Luxi | Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential.. |
| Luxi | Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential.. |
| Luxi | Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential.. |
| Luxi | Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential.. |
| Du | Review of drug repurposing as a broad-spectrum antiviral strategy against coronaviruses, with a focus on SARS-CoV-2/COVID-19. Authors systematically.. |
| Fang | Phase I RCT of 26 healthy adults (20 STSA-1002, 6 placebo) showing STSA-1002, a fully human anti-C5a monoclonal antibody, was safe and well.. |
| Ma | In silico study using network pharmacology, molecular docking, and molecular dynamics simulation to investigate the mechanisms of Xiangxue Decoction.. |
| Porta | Review of SARS-CoV-2 non-structural proteins as targets for direct-acting small-molecule antivirals. |
| Soto Albrecht | In vitro study showing that inhibition of mitochondrial oxidative phosphorylation (OXPHOS) enhances SARS-CoV-2 replication, while restoration of.. |
| Khatun | Preclinical study (in vitro and mouse model) demonstrating synergistic antiviral efficacy of auranofin and GS-621763 (an oral prodrug of remdesivir).. |
| Lew | In vitro study showing synergistic antiviral activity of ivermectin and remdesivir against murine coronavirus (MHV) and SARS-CoV-2. |
| Stevenson | Non-COVID-19 retrospective ecological study using a time-stratified case-crossover design examining daily sunlight exposure and excess influenza.. |
| Liu | Retrospective 1,219 hospitalized severe COVID-19 patients in China showing significantly lower 28-day mortality with paxlovid. This study has.. |
| Khoo | Phase I RCT of 24 outpatients (16 combination therapy, 8 standard of care) showing that molnupiravir (800 mg twice daily) combined with nirmatrelvir.. |
| Borriello | Phase 1 double-blind, placebo-controlled RCT of 51 healthy volunteers showing that GB-0669 - an AI-designed, half-life-extended monoclonal antibody.. |
| Sines | 429 patients late treatment: 8% lower mortality (p=0.56) |
| Butzin-Dozier | 53,332 patients prophylaxis: 39% lower mortality (p<0.0001) and 13% lower long COVID (p=0.0003) |
| Khoo | Phase I RCT of 24 outpatients (16 combination therapy, 8 standard of care) showing that molnupiravir (800 mg twice daily) combined with nirmatrelvir.. |
| Lew | In vitro study showing synergistic antiviral activity of ivermectin and remdesivir against murine coronavirus (MHV) and SARS-CoV-2. |
| Oliveira | Syrian golden hamster study showing benefits of vitamin B12 treatment for mitigating long COVID neurological sequelae. Authors propose that B12's.. |
| di Filippo | 114 patients prophylaxis: 50% fewer symptomatic cases (p=0.12) |
| Rahardjo | RCT 30 hospitalized COVID-19 patients in Indonesia showing significantly shorter length of hospital stay with convalescent plasma, however there are.. |
| Morikawa | Retrospective 283 hospitalized COVID-19 patients in Japan showing potential benefit with butyrate-producing Clostridium butyricum (CB)-containing.. |
Recent studies (see the individual treatment pages for all studies):
Jul 22 |
et al., Drug Safety, doi:10.1007/s40264-026-01705-2 | Challenges and Opportunities for Signal Detection During Public Health Emergencies: An Historical Re-evaluation of the Disproportionality Analysis of the ADR Reporting of Anti-COVID-19 Monoclonal Antibodies in Vigibase |
| Disproportionality analysis of 15,250 de-duplicated individual case safety reports from VigiBase (February 2020-December 2023) identifying potential cardiovascular and neurological safety signals for monoclonal antibodies (mAbs) used in e.. | ||
Jul 21 |
et al., Viruses, doi:10.3390/v18070804 | Drug Repurposing as a Broad-Spectrum Strategy Against Coronaviruses: Frontiers in Mechanisms and Clinical Translation |
| Review of drug repurposing as a broad-spectrum antiviral strategy against coronaviruses, with a focus on SARS-CoV-2/COVID-19. Authors systematically summarize repurposed drugs targeting key coronavirus proteins and host factors, organized.. | ||
Jul 14 |
et al., The Journal of Infectious Diseases, doi:10.1093/infdis/jiag349 | Randomized, Double-Blind, Placebo-Controlled First-in-Human Trial of a First-in-Class AI-Designed Monoclonal Antibody (GB-0669) Against the Conserved SARS-CoV-2 Spike S2 Stem Helix |
| Phase 1 double-blind, placebo-controlled RCT of 51 healthy volunteers showing that GB-0669 - an AI-designed, half-life-extended monoclonal antibody targeting the conserved SARS-CoV-2 spike S2 stem helix - was well-tolerated, with no dose-.. | ||
Jul 9 |
et al., medRxiv, doi:10.64898/2026.07.06.26357398 | Metformin and Severe Post-COVID-19 Outcomes Among Individuals with Diabetes Mellitus |
| 39% lower mortality (p<0.0001) and 13% lower long COVID (p=0.0003). Retrospective 53,332 adults with type 2 diabetes mellitus and COVID-19 in the U.S. National Clinical Cohort Collaborative (N3C), showing lower 12-month all-cause mortality and probable long COVID with metformin vs. DPP4 inhibitor (DPP4i) .. | ||
Jul 6 |
et al., International Journal of Population Data Science, doi:10.23889/ijpds.v11i5.3763 | Sunlight and Influenza Mortality in Scotland: Insights From the 1918 Influenza Pandemic and Later Flu Outbreaks |
| Non-COVID-19 retrospective ecological study using a time-stratified case-crossover design examining daily sunlight exposure and excess influenza mortality during the 1918 pandemic in Scotland, showing that a one standard deviation increas.. | ||
We aim to cover the most promising early treatments for
COVID-19. We use pre-specified effect extraction criteria that prioritizes
more serious outcomes, for details see methods. For specific
outcomes and different treatment stages see the individual pages.
References