Quercetin reduces COVID-19 risk: real-time meta-analysis of 9 studies
 Control
ControlAbstract
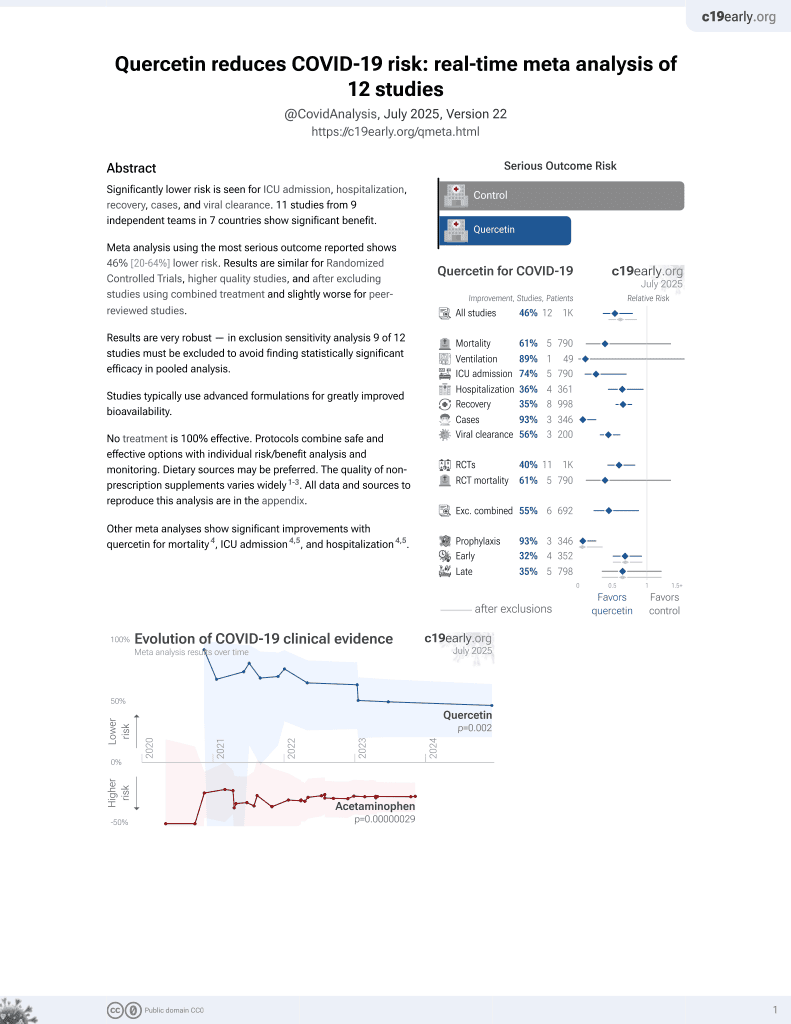
Significantly lower risk is seen for mortality, ICU admission, hospitalization, recovery, cases, and viral clearance. 9 studies from 7 independent teams in 5 countries show significant
benefit.
Meta-analysis using the most serious outcome reported shows
35% [15‑51%] lower risk. Results are similar for higher quality studies and better after excluding studies using combined treatment.
Currently all studies are RCTs.
Currently there is limited data, with only 841 patients in trials to date.
Studies typically use advanced formulations for greatly improved bioavailability.
No treatment is 100%
effective. Protocols combine safe and effective options with individual
risk/benefit analysis and monitoring.
Other treatments are more effective.
Dietary sources may be preferred. The quality of non-prescription supplements varies widely1-4.
A lipid-optimized formulation may be required for therapeutic concentrations of quercetin.
All data and sources to reproduce this analysis are in the appendix.
Quercetin for COVID-19 — Highlights
Quercetin reduces risk with very high confidence for recovery, viral clearance, and in pooled analysis, high confidence for mortality, ICU admission, and hospitalization, low confidence for cases, and very low confidence for ventilation.
Studies typically use advanced formulations for greatly improved bioavailability.
36th treatment shown effective in January 2022, now with p = 0.0018 from 9 studies.
Real-time updates and corrections with a consistent protocol for 226 treatments. Outcome specific analysis and combined evidence from all studies including treatment delay, a primary confounding factor.
B
Loading..
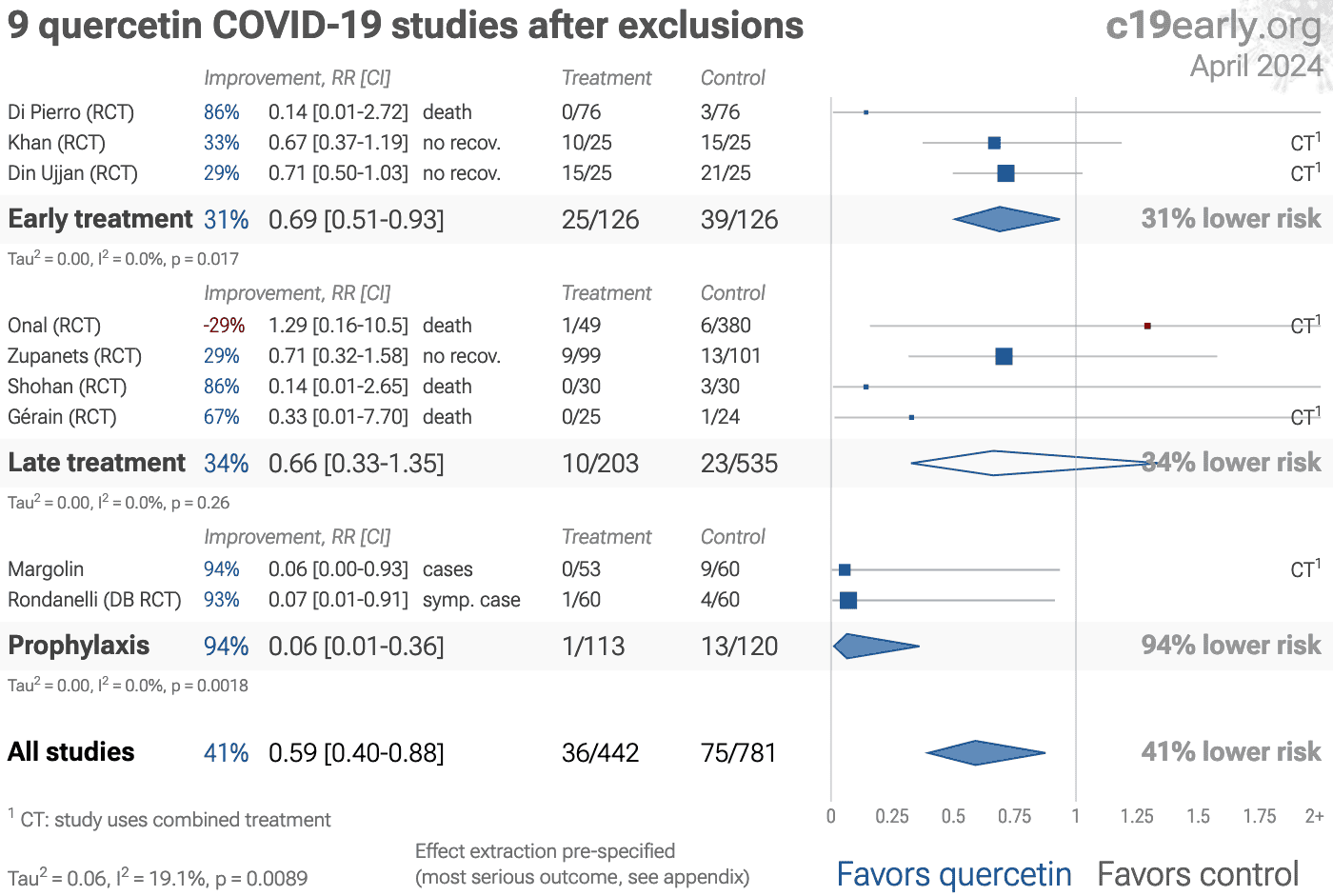
Fig. 1. A. Random-effects meta-analysis. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
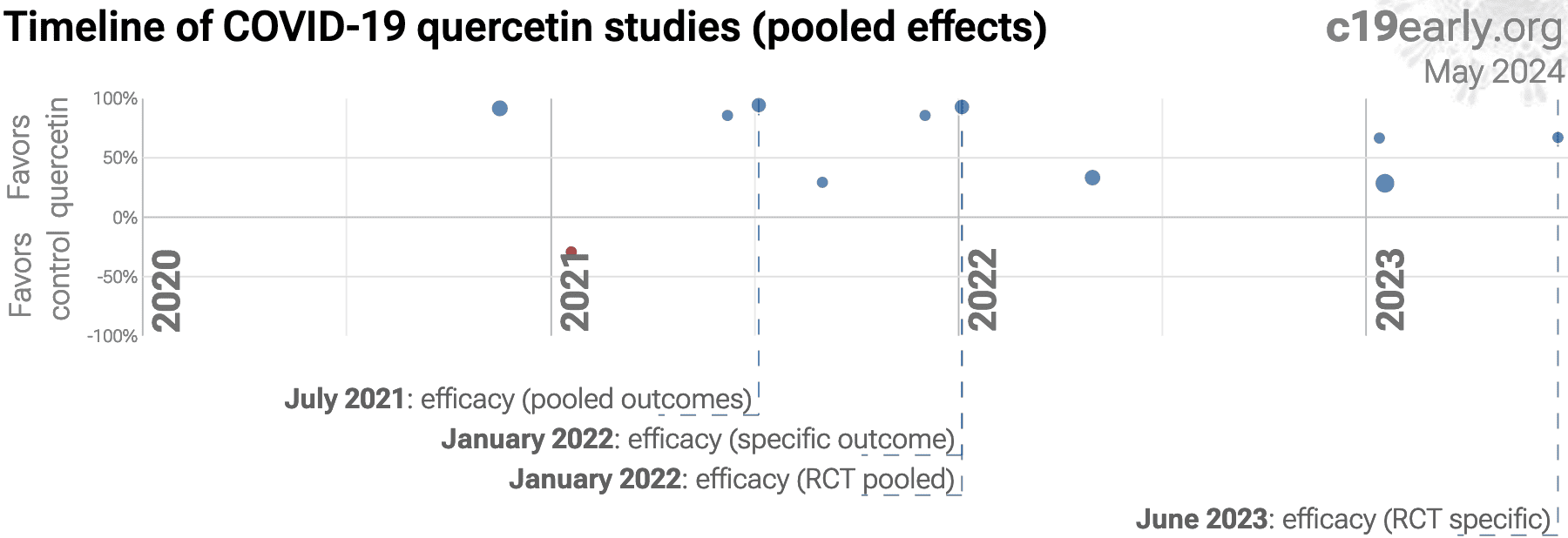
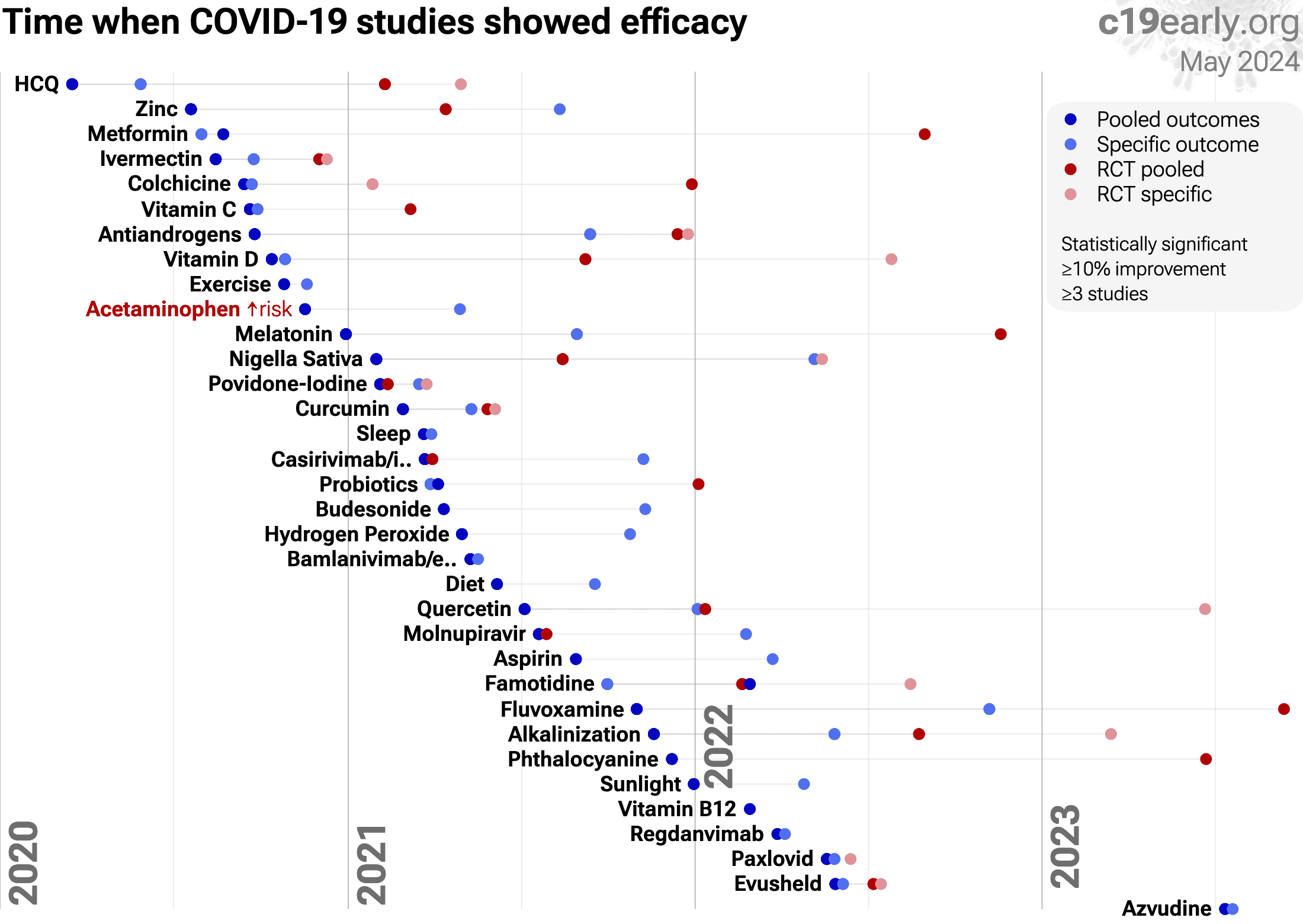
B. Timeline of results in quercetin studies. The marked dates indicate the time when efficacy was known with a statistically significant improvement of ≥10% from ≥3 studies for pooled outcomes, one or more specific outcome, pooled outcomes in RCTs, and one or more specific outcome in RCTs. Efficacy based on specific outcomes was delayed by 12.5 months, compared to using pooled outcomes. Efficacy based on specific outcomes in RCTs was delayed by 17.5 months, compared to using pooled outcomes in RCTs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
SARS-CoV-2 infection primarily begins in the upper respiratory
tract and may progress to the lower respiratory tract, other tissues, and the
nervous and cardiovascular systems, which may lead to cytokine storm,
pneumonia, ARDS, neurological injury8-24 and
cognitive deficits11,16, cardiovascular
complications25-31, DNA
damage32-35, organ failure, and death.
Even mild untreated infections may result in persistent cognitive
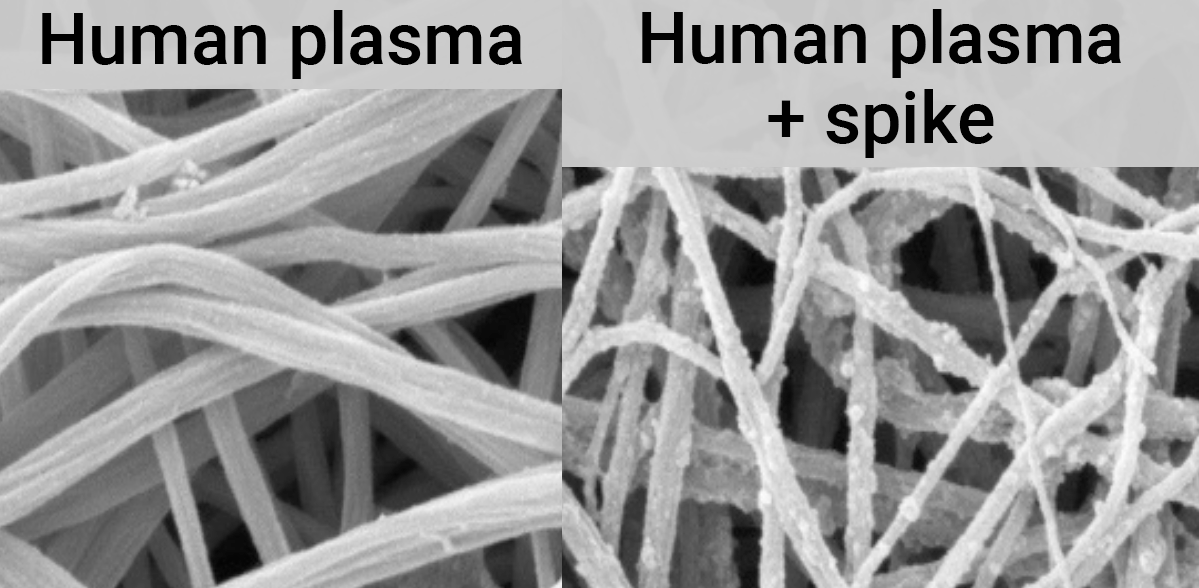
deficits36—the spike protein binds to fibrin leading to
fibrinolysis-resistant blood clots, thromboinflammation, and
neuropathology.
Minimizing replication as early as possible is recommended.
SARS-CoV-2 infection and replication involves the complex interplay of 500+
host and viral proteins and other factorsA,37-44 , providing many
therapeutic targets for which many existing compounds have known activity.
Scientists have predicted that over 11,000 compounds may
reduce COVID-19 risk45, either by
directly minimizing infection or replication, by supporting immune system
function, or by minimizing secondary complications.
In silico studies predict inhibition of SARS-CoV-2, or minimization of side effects, with quercetin or metabolites via binding to the spikeB,46-59 (and specifically the receptor binding domainC,60), MproD,49-52,54,55,58-76 , RNA-dependent RNA polymeraseE,55,58-60,77,78 , PLproF,58,63,69 , ACE2G,48,54,56,63,64,79,80 , TMPRSS2H,48, nucleocapsidI,58, helicaseJ,58,62,81 , endoribonucleaseK,46, NSP16/10L,82, cathepsin LM,83, Wnt-3N,48, FZDO,48, LRP6P,48, ezrinQ,84, ADRPR,52, NRP1S,56, EP300T,85, PTGS2U,64, HSP90AA1V,64,85 , matrix metalloproteinase 9W,86, IL-6X,87,88 , IL-10Y,87, VEGFAZ,88, and RELAAA,88 proteins, and inhibition of spike-ACE2 interactionAB,89.
In vitro studies demonstrate inhibition of the MproD,71,90-92 protein, and inhibition of spike-ACE2 interactionAB,93.
In vitro studies demonstrate efficacy in Calu-3AC,94, A549AD,87, HEK293-ACE2+AE,95, Huh-7AF,53, Caco-2AG,96, Vero E6AH,49,96,97 , mTECAI,98, RAW264.7AJ,98, and HLMECAK,89 cells.
Animal studies demonstrate efficacy in K18-hACE2 miceAL,99, db/db miceAM,98,100 , BALB/c miceAN,101, and rats97.
Quercetin reduced proinflammatory cytokines and protected lung and kidney tissue against LPS-induced damage in mice101, inhibits LPS-induced cytokine storm by modulating key inflammatory and antioxidant pathways in macrophages102, may block ACE2-spike interaction and NLRP3 inflammasome, limiting viral entry and inflammation103, upregulates the SIRT1/AMPK axis to inhibit oxidative injury and accelerate viral clearance104, inhibits SARS-CoV-2 ORF3a ion channel activity, which contributes to viral pathogenicity and cytotoxicity105, may alleviate COVID-19 ARDS via inhibition of EGFR and JAK2 inflammatory targets106, may destabilize the Spike protein, IL-6R, and integrins via conserved residues, blocking viral entry, hyperinflammation, and platelet aggregation107, and may reduce COVID-19 neuroinflammation and cognitive dysfunction through anti-inflammatory mechanisms and neuroprotective effects108.
We analyze all significant
controlled studies of
quercetin
for COVID-19.
Search methods, inclusion criteria, effect extraction criteria (more serious
outcomes have priority), all individual study data, PRISMA answers, and
statistical methods are detailed in Appendix 1. We present random-effects
meta-analysis results for all studies, studies within each treatment stage, individual outcomes, Randomized Controlled Trials (RCTs), and higher quality studies.
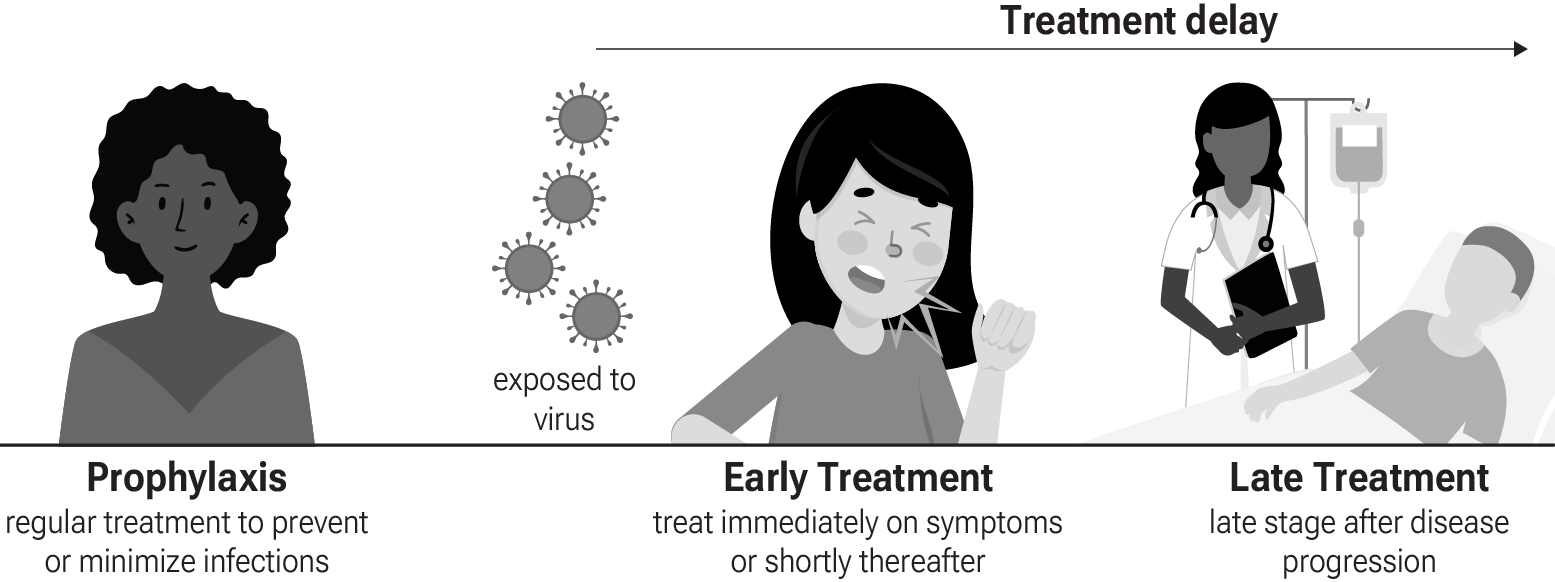
Fig. 3 shows stages of possible treatment for
COVID-19. Prophylaxis refers to regularly taking medication before
becoming sick, in order to prevent or minimize infection. Early
treatment refers to treatment immediately or soon after symptoms appear,
while late treatment refers to more delayed treatment.
{kind=link}
Fig. 3. Treatment stages.
In silico studies predict inhibition of SARS-CoV-2, or minimization of side effects, with quercetin or metabolites via binding to the spikeB,46-59 (and specifically the receptor binding domainC,60), MproD,49-52,54,55,58-76 , RNA-dependent RNA polymeraseE,55,58-60,77,78 , PLproF,58,63,69 , ACE2G,48,54,56,63,64,79,80 , TMPRSS2H,48, nucleocapsidI,58, helicaseJ,58,62,81 , endoribonucleaseK,46, NSP16/10L,82, cathepsin LM,83, Wnt-3N,48, FZDO,48, LRP6P,48, ezrinQ,84, ADRPR,52, NRP1S,56, EP300T,85, PTGS2U,64, HSP90AA1V,64,85 , matrix metalloproteinase 9W,86, IL-6X,87,88 , IL-10Y,87, VEGFAZ,88, and RELAAA,88 proteins, and inhibition of spike-ACE2 interactionAB,89.
In vitro studies demonstrate inhibition of the MproD,71,90-92 protein, and inhibition of spike-ACE2 interactionAB,93.
In vitro studies demonstrate efficacy in Calu-3AC,94, A549AD,87, HEK293-ACE2+AE,95, Huh-7AF,53, Caco-2AG,96, Vero E6AH,49,96,97 , mTECAI,98, RAW264.7AJ,98, and HLMECAK,89 cells.
Animal studies demonstrate efficacy in K18-hACE2 miceAL,99, db/db miceAM,98,100 , BALB/c miceAN,101, and rats97.
Quercetin reduced proinflammatory cytokines and protected lung and kidney tissue against LPS-induced damage in mice101, inhibits LPS-induced cytokine storm by modulating key inflammatory and antioxidant pathways in macrophages102, may block ACE2-spike interaction and NLRP3 inflammasome, limiting viral entry and inflammation103, upregulates the SIRT1/AMPK axis to inhibit oxidative injury and accelerate viral clearance104, inhibits SARS-CoV-2 ORF3a ion channel activity, which contributes to viral pathogenicity and cytotoxicity105, may alleviate COVID-19 ARDS via inhibition of EGFR and JAK2 inflammatory targets106, may destabilize the Spike protein, IL-6R, and integrins via conserved residues, blocking viral entry, hyperinflammation, and platelet aggregation107, and may reduce COVID-19 neuroinflammation and cognitive dysfunction through anti-inflammatory mechanisms and neuroprotective effects108.
31 in vitro studies support the efficacy of quercetin49,53,59,71,75,76,78,87,89-99,102,105,116,118-120,126-131 .
2 studies investigate novel formulations of quercetin that may be more
effective for COVID-19128,132.
Preclinical research is an important part of the development of
treatments, however results may be very different in clinical trials.
Preclinical results are not used in this paper.
SARS-CoV-2 infection and replication involves multiple steps as
shown in Table 1. Each step can be disrupted by therapeutics. The
timing of each step may vary significantly, and the cycle is continuous, with
released virions attaching to new host cells.
The efficacy of treatments depends on the delay from infection and the steps
targeted. Preclinical research suggests that quercetin is most likely to interfere with early steps in the viral lifecycle, suggesting greater benefit for prophylaxis and very early treatment.
| Step | Details | Approximate timing | Predicted benefit of quercetin |
|---|---|---|---|
| Viral attachment | Viral binding to specific receptors on host cell surface | Initial step | High: spike and ACE2 binding |
| Viral entry | Uptake of viral particle into host cell via mechanisms like endocytosis or membrane fusion | Within minutes to 1 hour | Moderate: spike binding |
| Viral uncoating and release | Disassembly of virion to release viral genome into host cell | 1-2 hours | - |
| Genome replication and transcription | Production of viral mRNAs from the genome template and genome copies | 2-4 hours | Moderate: RdRp binding |
| Translation and protein processing | Production of new viral proteins from the viral transcripts | 4-8 hours | Moderate: Mpro and PLpro binding |
| Viral assembly and budding | Self-assembly of viral components and encapsidation of viral genome to form new viral particles, often utilizing host cell membrane | 8-12 hours | - |
| Viral release | Escape of newly formed virions from the host cell to spread infection | 12-24 hours | - |
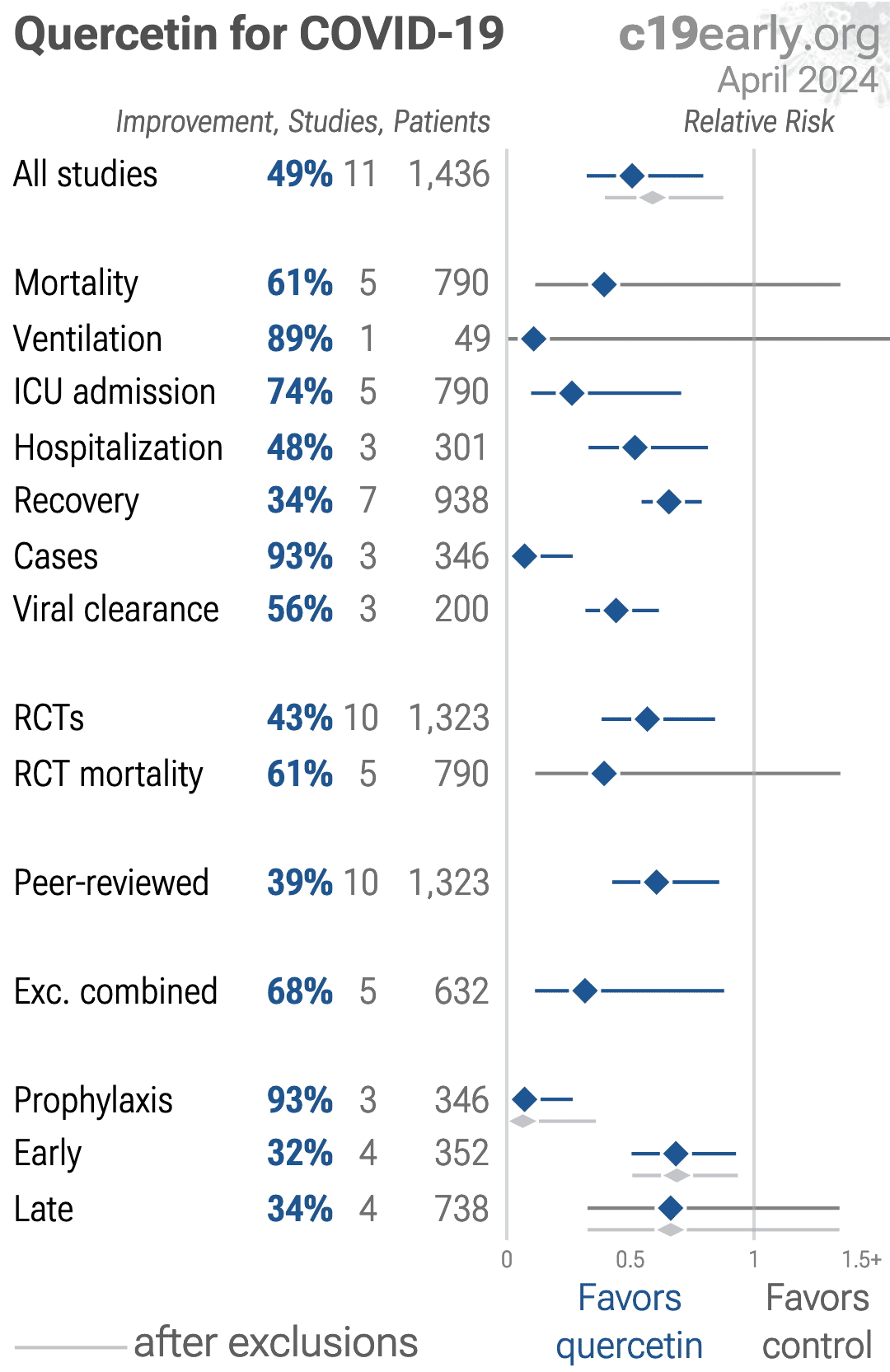
Table 2 summarizes the results for all stages combined, for Randomized Controlled Trials, with different exclusions, and for specific outcomes.
Table 3 shows results by treatment stage.
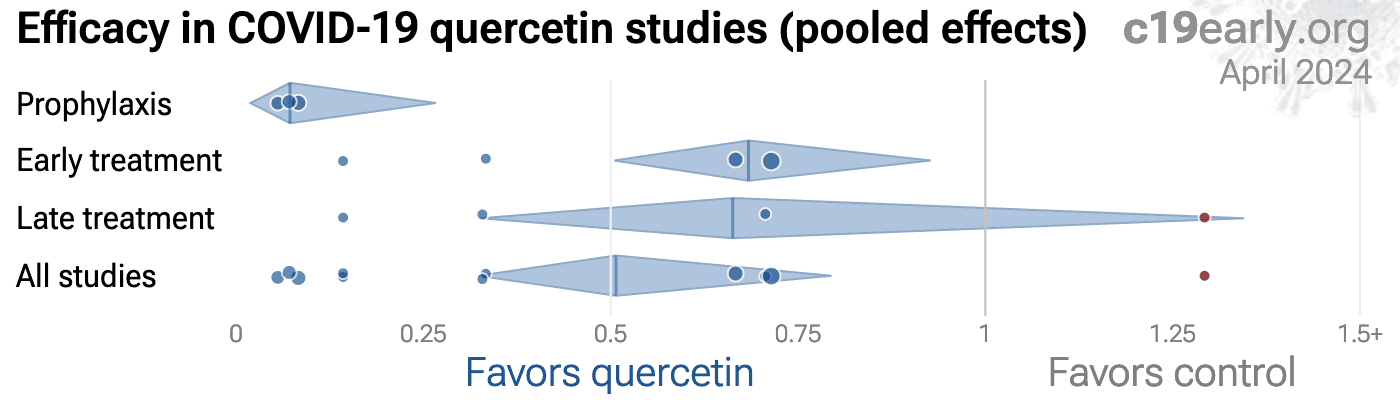
Fig. 4 plots individual results by treatment stage.
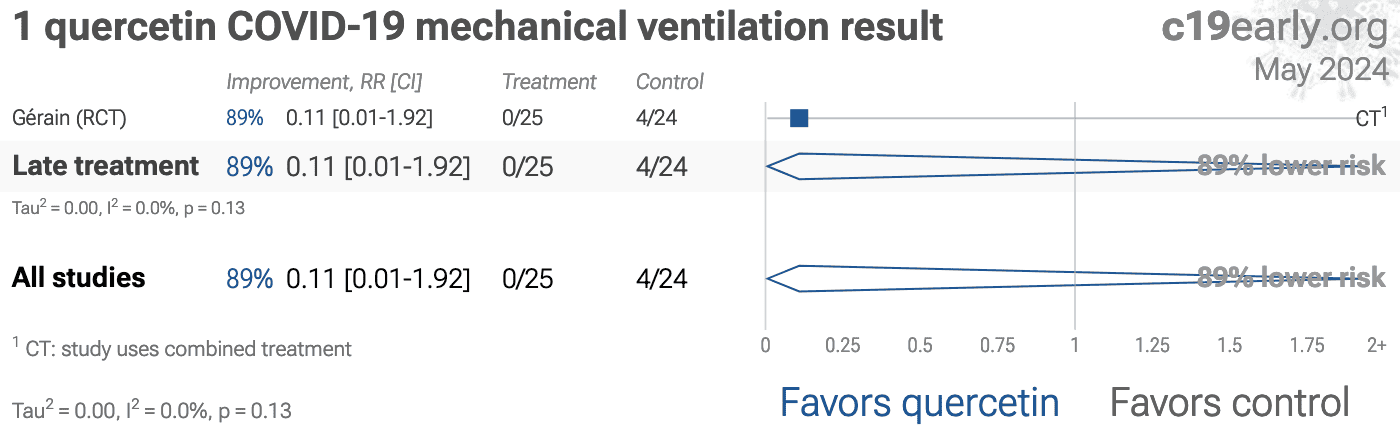
Fig. 5, 6, 7, 8, 9, 10, 11, 12, and 13
show forest plots for random-effects meta-analysis of
all studies with pooled effects, mortality results, ventilation, ICU admission, hospitalization, recovery, cases, viral clearance, and all studies excluding combined treatment studies.
| Relative Risk | Studies | Patients | |
|---|---|---|---|
| All studies | 0.65 [0.49‑0.85]** | 9 | 841 |
| After exclusions | 0.58 [0.38‑0.90]* | 6 | 539 |
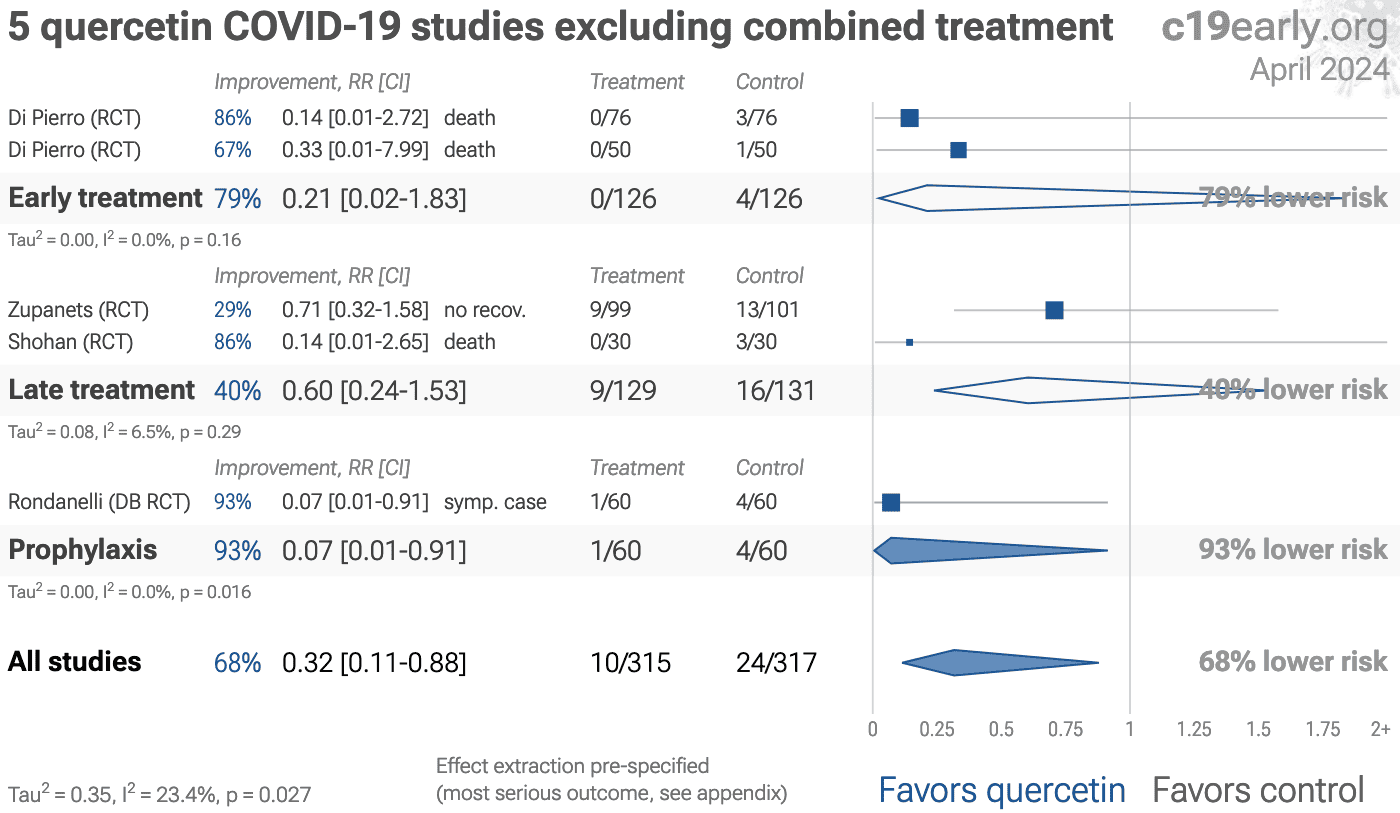
| Excluding combined treatmentExc. combined | 0.45 [0.23‑0.88]* | 6 | 692 |
| RCTsRCTs | 0.65 [0.49‑0.85]** | 9 | 841 |
| Mortality | 0.21 [0.05‑0.96]* | 4 | 361 |
| ICU admissionICU | 0.32 [0.11‑0.93]* | 4 | 361 |
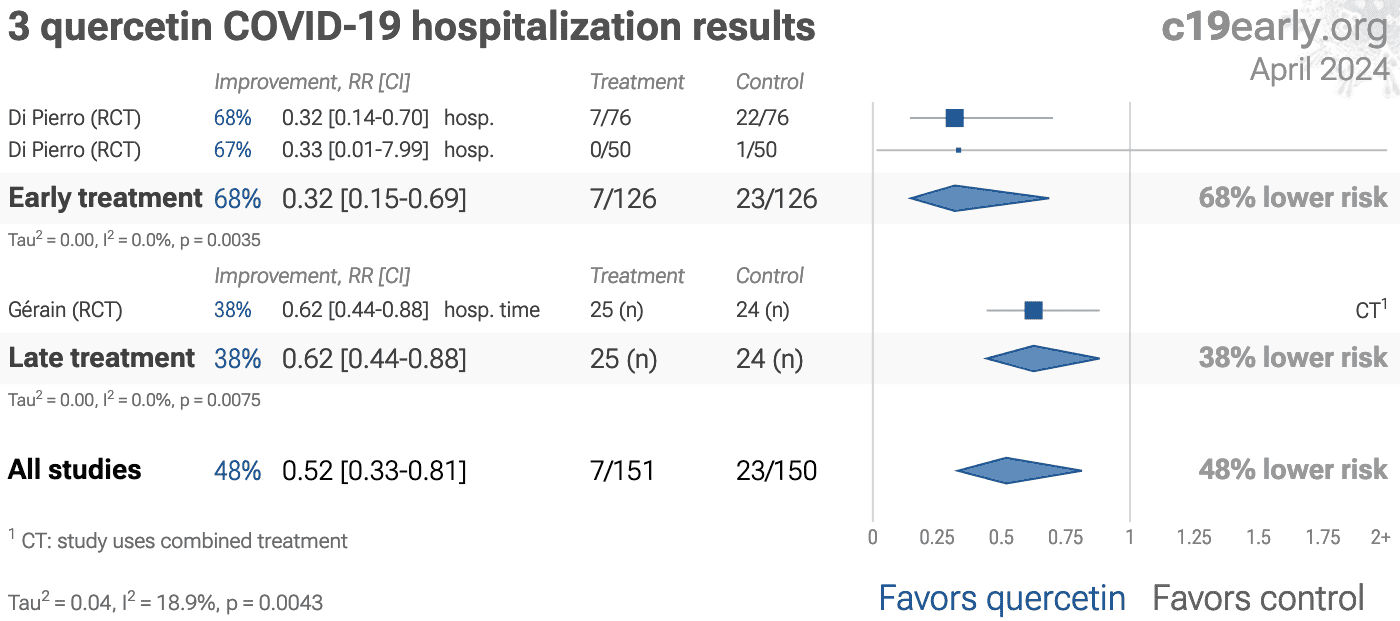
| HospitalizationHosp. | 0.64 [0.44‑0.95]* | 4 | 361 |
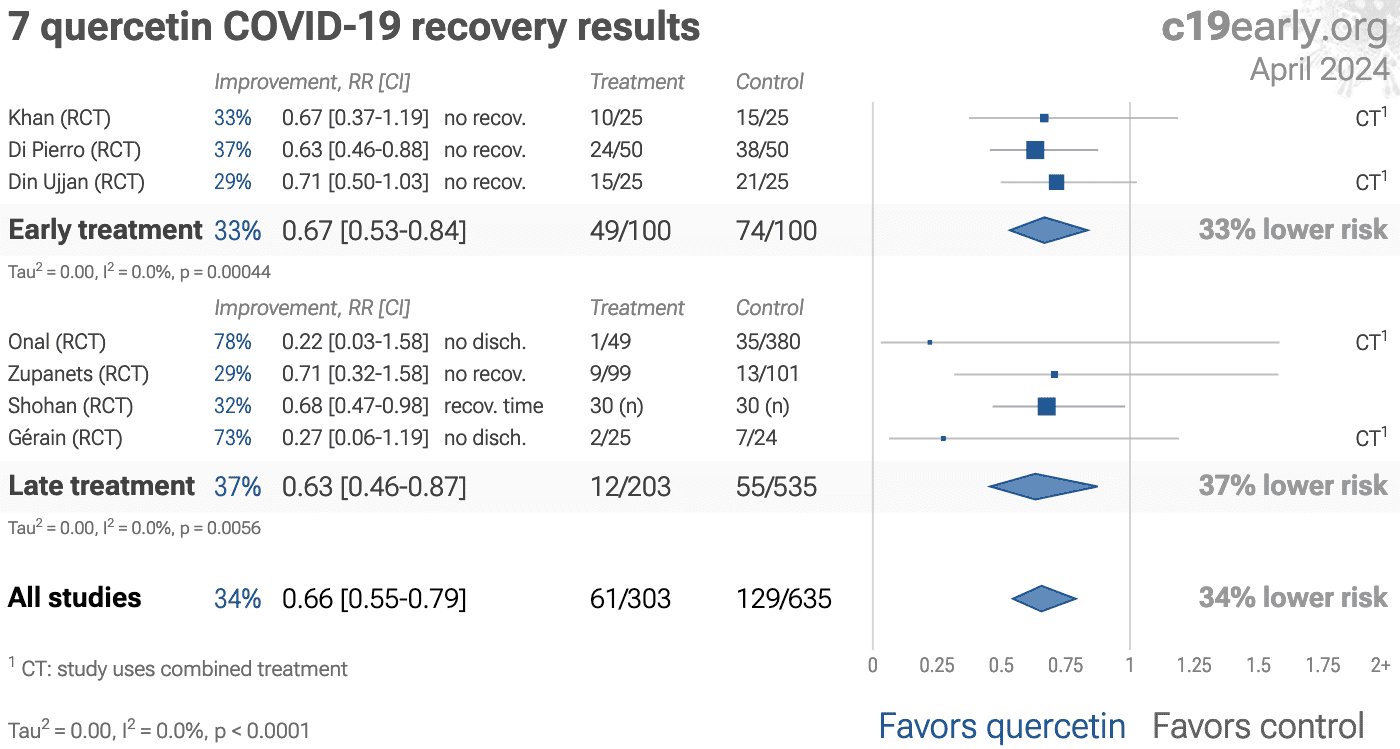
| Recovery | 0.66 [0.55‑0.79]**** | 7 | 569 |
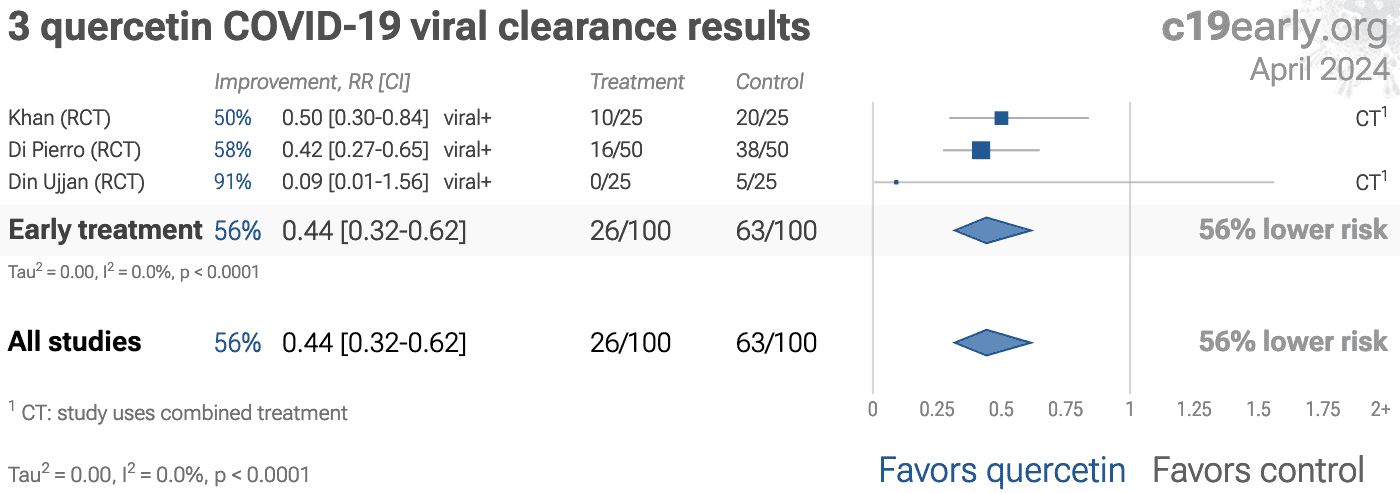
| Viral | 0.44 [0.32‑0.62]**** | 3 | 200 |
| RCT mortality | 0.21 [0.05‑0.96]* | 4 | 361 |
| RCT hospitalizationRCT hosp. | 0.64 [0.44‑0.95]* | 4 | 361 |
| Early treatment | Late treatment | Prophylaxis | |
|---|---|---|---|
| All studies | 0.68 [0.50‑0.93]*0.68* [0.50‑0.93] | 0.61 [0.31‑1.17]0.61 [0.31‑1.17] | 0.07 [0.01‑0.91]*0.07* [0.01‑0.91] |
| After exclusions | 0.67 [0.37‑1.19]0.67 [0.37‑1.19] | 0.61 [0.31‑1.17]0.61 [0.31‑1.17] | 0.07 [0.01‑0.91]*0.07* [0.01‑0.91] |
| Excluding combined treatmentExc. combined | 0.21 [0.02‑1.83]0.21 [0.02‑1.83] | 0.62 [0.32‑1.22]0.62 [0.32‑1.22] | 0.07 [0.01‑0.91]*0.07* [0.01‑0.91] |
| RCTsRCTs | 0.68 [0.50‑0.93]*0.68* [0.50‑0.93] | 0.61 [0.31‑1.17]0.61 [0.31‑1.17] | 0.07 [0.01‑0.91]*0.07* [0.01‑0.91] |
| Mortality | 0.21 [0.02‑1.83]0.21 [0.02‑1.83] | 0.21 [0.02‑1.79]0.21 [0.02‑1.79] | |
| ICU admissionICU | 0.13 [0.02‑1.05]0.13 [0.02‑1.05] | 0.42 [0.11‑1.64]0.42 [0.11‑1.64] | |
| HospitalizationHosp. | 0.32 [0.15‑0.69]**0.32** [0.15‑0.69] | 0.77 [0.57‑1.03]0.77 [0.57‑1.03] | |
| Recovery | 0.67 [0.53‑0.84]***0.67*** [0.53‑0.84] | 0.65 [0.47‑0.89]**0.65** [0.47‑0.89] | |
| Viral | 0.44 [0.32‑0.62]****0.44**** [0.32‑0.62] | ||
| RCT mortality | 0.21 [0.02‑1.83]0.21 [0.02‑1.83] | 0.21 [0.02‑1.79]0.21 [0.02‑1.79] | |
| RCT hospitalizationRCT hosp. | 0.32 [0.15‑0.69]**0.32** [0.15‑0.69] | 0.77 [0.57‑1.03]0.77 [0.57‑1.03] | |
{kind=link}
Fig. 4. Scatter plot showing the most serious outcome in all studies, and for studies within each stage. Diamonds shows the results of random-effects meta-analysis.
Loading..
Loading..
Fig. 5. Random-effects meta-analysis for all studies.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Currently all studies are RCTs.
To avoid bias in the selection of studies, we analyze all
non-retracted studies. Here we show the results after excluding
studies with major issues likely to alter results, non-standard studies, and
studies where very minimal detail is currently available. Our bias evaluation
is based on analysis of each study and identifying when there is a significant
chance that limitations will substantially change the outcome of the study. We
believe this can be more valuable than checklist-based approaches such as
Cochrane GRADE, which can be easily influenced by potential bias, may ignore
or underemphasize serious issues not captured in the checklists, and may
overemphasize issues unlikely to alter outcomes in specific cases (for example
certain specifics of randomization with a very large effect size and
well-matched baseline characteristics).
The studies excluded are as below.
Fig. 14 shows a forest plot for random-effects
meta-analysis of all studies after exclusions.
Di Pierro, randomization resulted in significant baseline differences that were not adjusted for.
Di Pierro (B), multiple data issues - pending author response.
Din Ujjan, combined treatments may contribute significantly to the effect seen; unadjusted differences between groups.
{kind=link}
Loading..
Fig. 14. Random-effects meta-analysis for all studies after exclusions.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
Low-cost treatments were subject to bias and censorship during the pandemic.
Scientific bias is seen in the design, analysis, presentation, and selective
reporting of studies, which often favored negative results. A similar bias is seen in the media
coverage for low-cost treatments.
While broadly seen, bias was particularly notable for ivermectin and hydroxychloroquine, e.g., Scott Alexander noted that "if you say anything in favor of ivermectin you will be cast out of civilization and thrown into the circle of social hell reserved for Klan members and 1/6 insurrectionists. All the health officials in the world will shout 'horse dewormer!' at you and compare you to Josef Mengele."109.
We analyze media coverage for the 226 treatments we cover using
Altmetric136, which reports the number of ~12,000 tracked news outlets that covered each study137. Studies are considered to have received significant media coverage if they were covered by at least 0.5% of the tracked news outlets.
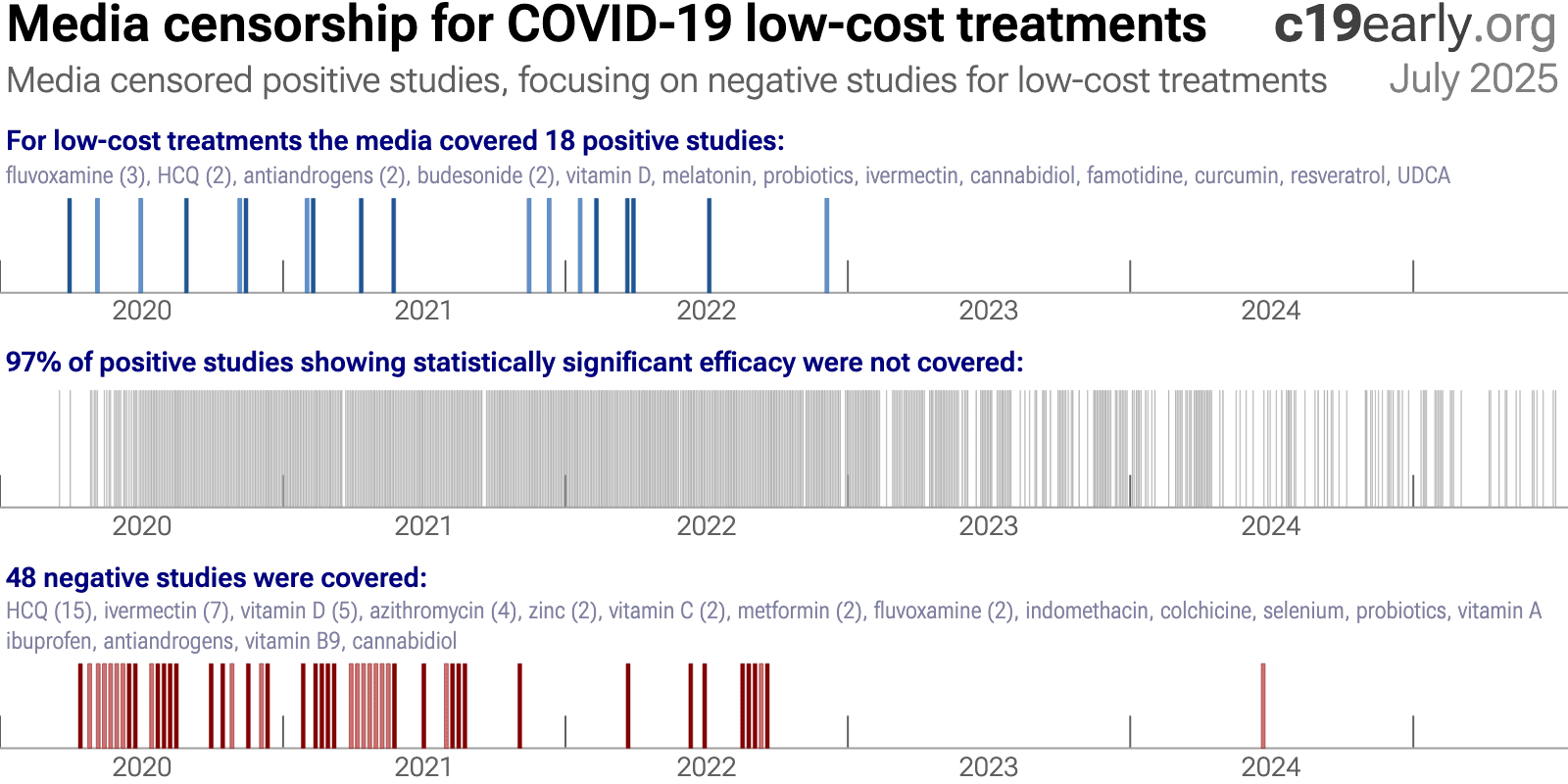
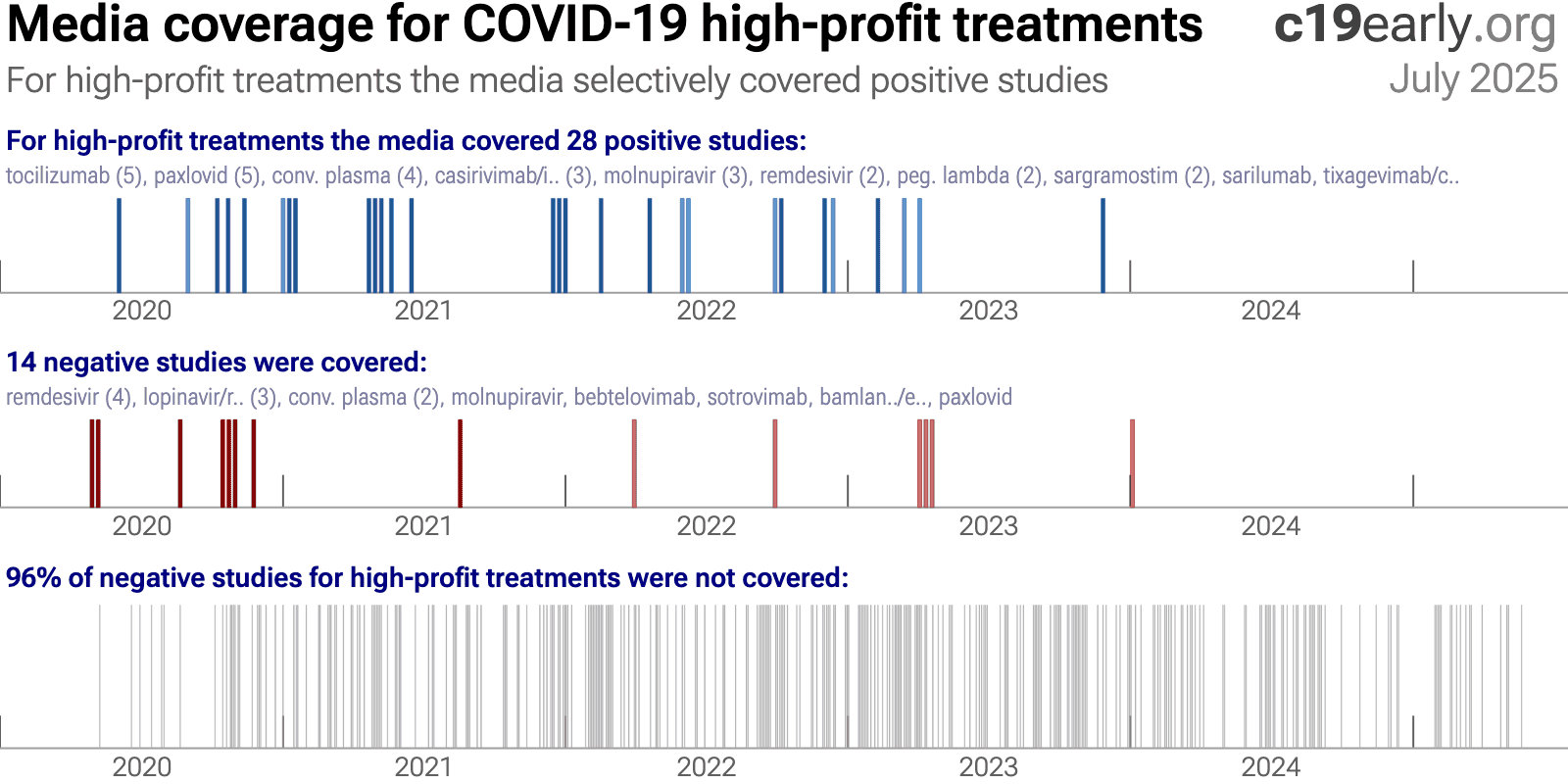
Fig. 15 and 16 show the bias toward negative results for low-cost treatments, in contrast to the opposite bias for high-profit treatments.
This may result in widespread incorrect perceptions on the relative efficacy of high-profit and low-cost treatments. The impact is significant—increased cost limits the use of high-profit
treatments and treatment equity, and high-profit treatments were also more difficult to access, especially for earlier treatment which improves efficacy and minimizes community transmission.
The mainstream media did not cover any of the positive studies for quercetin.
{kind=link}
Fig. 15. Mainstream media was biased against positive results for low-cost treatments.
{kind=link}
Fig. 16. In contrast to the results for low-cost treatments, mainstream media was biased towards positive results for high-cost treatments.
A combination of factors may have led to the media's suppression of low-cost treatments:
•
Politicization
led to a media environment where coverage was often framed to support a political
narrative rather than to provide objective scientific information. As Scott Alexander
said: "if you say anything in favor of ivermectin you will be cast out
of civilization and thrown into the circle of social hell reserved for Klan members and
1/6 insurrectionists. All the health officials in the world will shout 'horse dewormer!'
at you and compare you to Josef Mengele."
There was strong social pressure to
discredit low-cost treatments.•
Censorship
of
information conflicting with selected authorities. For example, individuals and
organizations presenting conflicting science were often banned on Twitter and
YouTube.•
FDA requires "no
adequate, approved, and available alternatives"
in order to grant an EUA for
novel high-profit interventions, creating a strong incentive for authorities to ignore or
downplay existing low-cost treatments.•
Regulatory
capture
biases authorities towards high-profit interventions.•
Authorities ignored
most evidence for low-cost treatments
, for example the NIH references only 2% of
studies in delayed, rarely-updated, biased commentaries with no quantitive analysis.•
Media coverage of
science is often not very accurate
, e.g., misunderstanding confounding issues. For
example the media widely considered the RECOVERY HCQ RCT to be conclusive on efficacy, but
very late treatment of late stage patients (mostly on oxygen already) with an excessive
toxic dose (shown dangerous in a dose comparison RCT) provides no information on the
recommended early/prophylactic treatment. With difficulting in understanding basic
confounders like treatment delay and dose, the media may favor deferring to authorities.
Many studies for low-cost treatments require greater expertise to analyze. Relatively few
journalists have a strong ability to analyze clinical trials and are outnumbered by the
rest.•
Substantial funding
from pharmaceutical advertising
biases editorial decisions towards high-profit
interventions.•
PR power
-
companies/teams with strong PR presence are favored in the media, which correlates with
high-profit and high conflict of interest studies.•
The media was very
negative in general
, inflating risk, fear, and anxieties. A negative bias may
improve ratings and revenue, increasing motivation to continue watching coverage. A
combination of low-cost treatments greatly reducing risk conflicts with the negative
narrative.25 low-cost treatments were approved in one
or more countries, yet many countries approved no low-cost treatments.
The countries that did adopt low-cost treatments analyzed the evidence early and made
timely approvals. With few exceptions, authorities did not change their initial views,
regardless of how much evidence accumulated showing either efficacy or harm. Why?
The harms of smoking here hidden for 25 yearsAP. Authorities did not analyze the data in real-time, failing to act when
harm was known.
Widespread acknowledgement of harm came only after attempts by two new surgeon generals,
along with pressure from health advocates and a new president, and a review of 7,000 studies.
Similarly for COVID-19, most authorities and experts did not proactively
analyze data in real-time. This guarantees delayed recognition of efficacy or harm, by
which time moral, legal, career, and reputational liabilities strongly disincentivize any
admission of error. Claims of no efficacy (for effective treatments) or safety (for
harmful treatments) were often made prior to strong data being available. Correction
would require admitting to errors that increased mortality, which is unlikely with the
same generation of officials.
Analysis of potential treatments was rarely done, and when done these were
typically minimal efforts.
For example, NIH reviews were highly delayed, cover only a tiny fraction of treatments,
reference only 2% of studies for the treatments covered, and include no
quantitative analysis.
They appear as rarely updated side projects from
external panels implicitly tasked with justifying prior failures.
As with smoking, the thousands of studies could (and should)
have been analyzed and acted on in real-time.
A key structural improvement, applicable to all current and future
diseases, is for authorities to implement real-time proactive analysis of clinical
evidence. This does not remove all bias, but does make it possible to act on evidence,
whereas delayed action may be unlikely due to moral, legal, career, and reputational
liabilities.
c19early.org
Delayed public health acknowledgments
Official acknowledgment of efficacy or harm is often delayed—legal, career, and status risks disincentivize admission of error.
| Evidence | Official Acknowledgment | Approx. Delay | |
|---|---|---|---|
| Citrus Fruit (vitamin C) for Scurvy (effectiveness) | 1747: James Lind conducted one of the first-ever controlled clinical trials, proving that oranges and lemons cured scurvy in sailors. | 1795: The British Royal Navy finally made a daily ration of lemon juice a standard issue for all its sailors, effectively eliminating the disease. | 48 years |
| Handwashing (lower mortality) | 1847: Dr. Ignaz Semmelweis provided conclusive proof that having doctors wash their hands with a chlorine solution before delivering babies reduced maternal mortality rates from over 18% to around 1%. | ~1870s: Semmelweis's findings were rejected and he was ridiculed. His work was only validated decades later (after his death). | ~20+ years |
| Helicobacter pylori (bacteria causes ulcers) | 1982-1984: Marshall and Warren discovered that Helicobacter pylori bacteria causes ulcers, confirmed via direct exposure. Officials maintained that ulcers were caused by stress and spicy food. | 1994: The US NIH released a consensus statement officially recommending antibiotics as the standard treatment for peptic ulcers, overturning decades of acid-suppression therapy. | ~12 years |
| Asbestos (causes asbestosis & cancer) | 1924: The British Medical Journal published the first case study of a death from "asbestosis." By 1918, U.S. insurance companies had stopped selling life insurance to asbestos workers. | 1971 (US): The Occupational Safety and Health Administration (OSHA) was formed and began regulating asbestos as a carcinogen, setting the first federal workplace safety standards for it. | ~47 years |
| Leaded Gasoline (neurotoxicity) | ~1924: Dangers of low-level lead exposure were known. Experts like Alice Hamilton warned the U.S. Surgeon General that adding lead to gasoline would cause widespread public poisoning. | 1973 (US): The Environmental Protection Agency (EPA) ordered the first phasedown of lead in gasoline, following the Clean Air Act of 1970. A full ban for on-road vehicles took effect in 1996. | ~49 years |
| Harms of Smoking (causes lung cancer) | 1939: Franz Müller (Germany) published the first case-control epidemiological study strongly linking tobacco smoking to lung cancer. This was followed by major U.S. & U.K. studies in the 1950s. | 1964 (US): The U.S. Surgeon General's report, "Smoking and Health," was released. It was the first U.S. government report to definitively link smoking to lung cancer and heart disease. | 25 years |
Heterogeneity in COVID-19 studies arises from many factors including:
The time between infection or the onset of symptoms and
treatment may critically affect how well a treatment works. For example an
antiviral may be very effective when used early but may not be effective in
late stage disease, and may even be harmful. Oseltamivir, for example, is
generally only considered effective for influenza when used within 0-36 or
0-48 hours138,139. Baloxavir marboxil studies for influenza
also show that treatment delay is critical — Ikematsu et al. report
an 86% reduction in cases for post-exposure prophylaxis, Hayden et al.
show a 33 hour reduction in the time to alleviation of symptoms for treatment
within 24 hours and a reduction of 13 hours for treatment within 24-48 hours,
and Kumar et al. report only 2.5 hours improvement for inpatient
treatment.
| Treatment delay | Result |
| Post-exposure prophylaxis | 86% fewer cases140 |
| <24 hours | -33 hours symptoms141 |
| 24-48 hours | -13 hours symptoms141 |
| Inpatients | -2.5 hours to improvement142 |
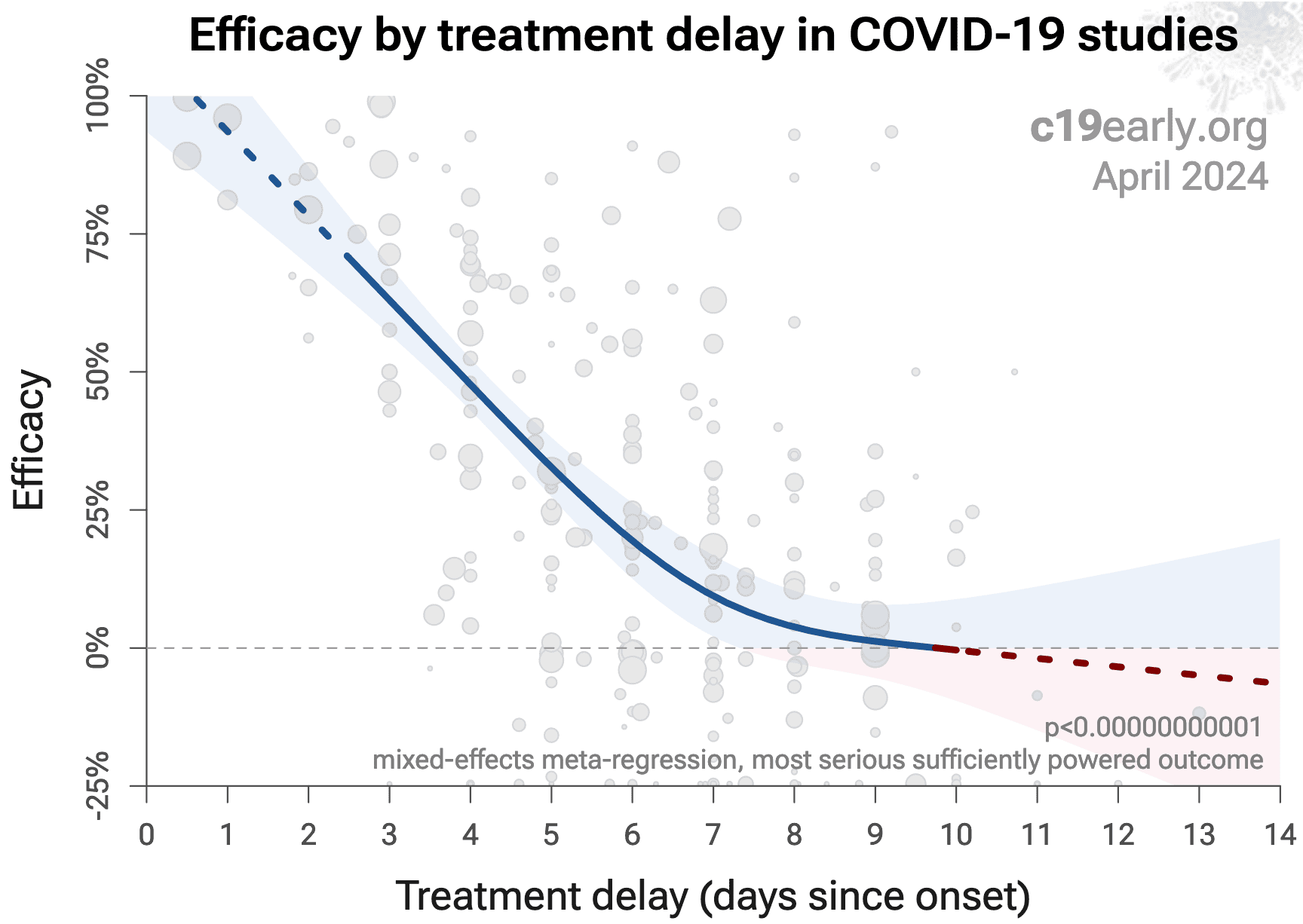
Fig. 17 shows a mixed-effects meta-regression for
efficacy as a function of treatment delay in COVID-19 studies from 226 treatments, showing that efficacy
declines rapidly with treatment delay. Early treatment is critical for COVID-19.
{kind=link}
Fig. 17. Early treatment is more effective. Meta-regression showing efficacy as a function of treatment delay in COVID-19 studies from 226 treatments.
Details of the patient population including age and comorbidities may
critically affect how well a treatment works. For example, many COVID-19
studies with relatively young low-comorbidity patients show all patients
recovering quickly with or without treatment. In such cases, there is little
room for an effective treatment to improve results, for example as in
López-Medina et al.
Efficacy may depend critically on the distribution of
SARS-CoV-2 variants encountered by patients. Risk varies significantly across
variants144, for example the Gamma variant shows significantly
different characteristics145-148. Different
mechanisms of action may be more or less effective depending on variants, for
example the degree to which TMPRSS2 contributes to viral entry can differ
across variants149,150.
Effectiveness may depend strongly on the dosage and treatment regimen.
The quality of medications may vary significantly between
manufacturers and production batches, which may significantly affect efficacy
and safety. Williams et al. analyze ivermectin from 11 different sources,
showing highly variable antiparasitic efficacy across different manufacturers.
Xu (C) et al. analyze a treatment from two different manufacturers, showing 9
different impurities, with significantly different concentrations for each
manufacturer.
Non-prescription supplements may show very wide variations in quality1,2.
Across all
studies there is a strong association between different outcomes, for example
improved recovery is strongly associated with lower mortality. However,
efficacy may differ depending on the effect measured, for example a treatment
may be more effective against secondary complications and have minimal effect
on viral clearance.
The
distribution of studies will alter the outcome of a meta-analysis. Consider a
simplified example where everything is equal except for the treatment delay,
and effectiveness decreases to zero or below with increasing delay. If there
are many studies using very late treatment, the outcome may be negative, even
though early treatment is very effective.
All meta-analyses combine heterogeneous studies, varying in population,
variants, and potentially all factors above, and therefore may obscure
efficacy by including studies where treatment is less effective. Generally, we
expect the estimated effect size from meta-analysis to be less than that for
the optimal case.
Looking at all studies is valuable for providing an overview of all research,
important to avoid cherry-picking, and informative when a positive result is
found despite combining less-optimal situations. However, the resulting
estimate does not apply to specific cases such as
early treatment in high-risk populations.
While we present results for all studies, we also present treatment time and
individual outcome analyses, which may be more informative for specific use
cases.
This section validates the use of pooled effects for COVID-19, which enables
earlier detection of efficacy, however pooled effects are no longer required
for quercetin as of January 2023. Efficacy is now known based on specific outcomes for all studies and when restricted to RCTs. Efficacy based on specific outcomes was delayed by 12.5 months compared to using pooled outcomes. Efficacy based on specific outcomes in RCTs was delayed by 17.5 months compared to using pooled outcomes in RCTs.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes" is not a good reason for
disregarding results.
Pooling the results of studies reporting different outcomes allows us to use
more of the available information. Logically we should, and do, use additional
information when evaluating treatments—for example dose-response and
treatment delay-response relationships provide additional evidence of efficacy
that is considered when reviewing the evidence for a treatment.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster and safer collection of evidence.
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 226
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
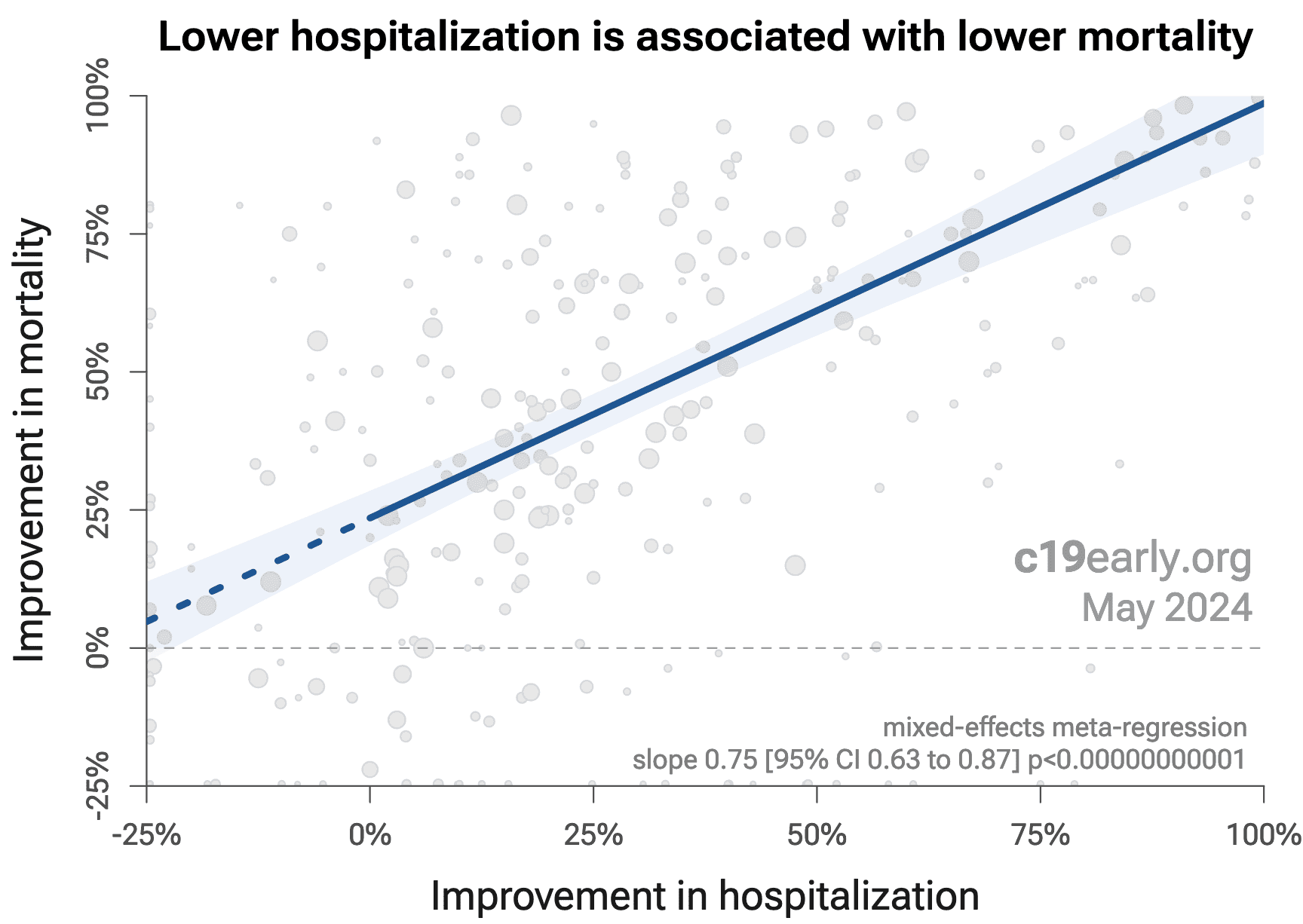
Fig. 18 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
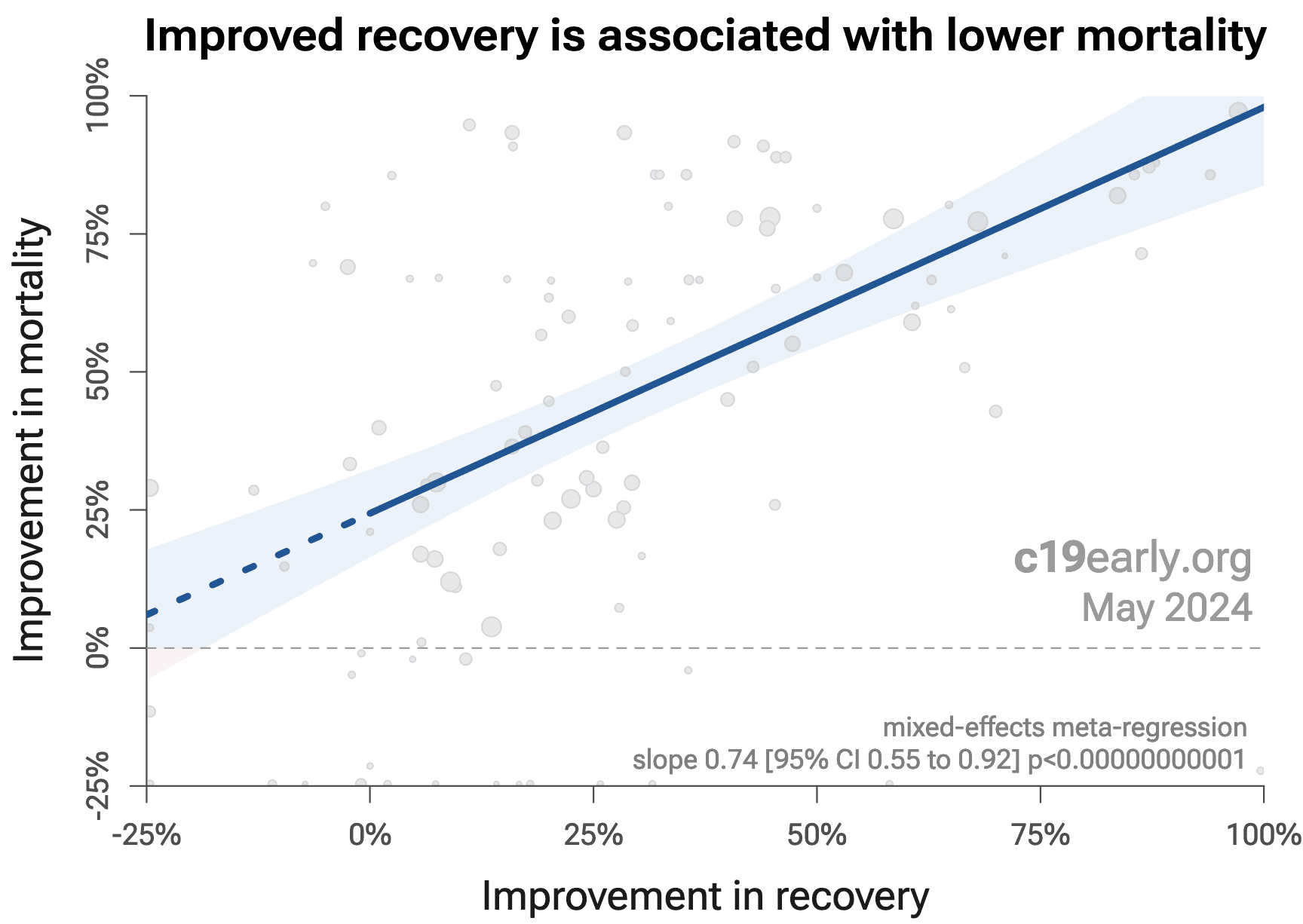
Similarly, Fig. 19 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
Considering the extremes, Singh (D) et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
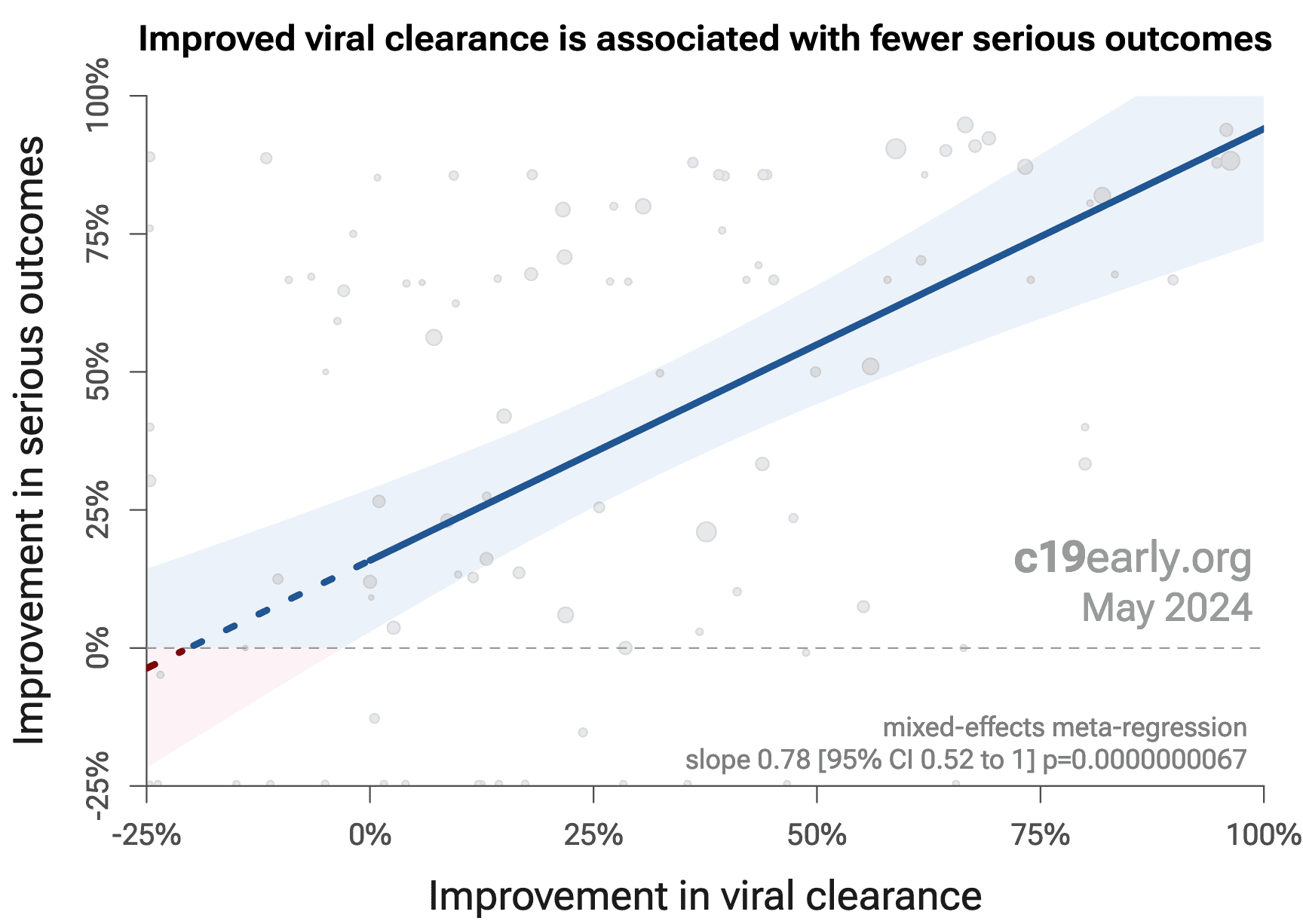
Fig. 20 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh (D) et al., with higher confidence due to the larger number of
studies. As with Singh (D) et al., the confidence increases
when excluding the outlier treatment, from p = 0.000000011 to p = 0.00000000032.
{kind=link}
Fig. 18. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Fig. 19. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Fig. 18. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
Currently, 59 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 85% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.6 months. When restricting to RCTs only, 53% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 7.4 months.
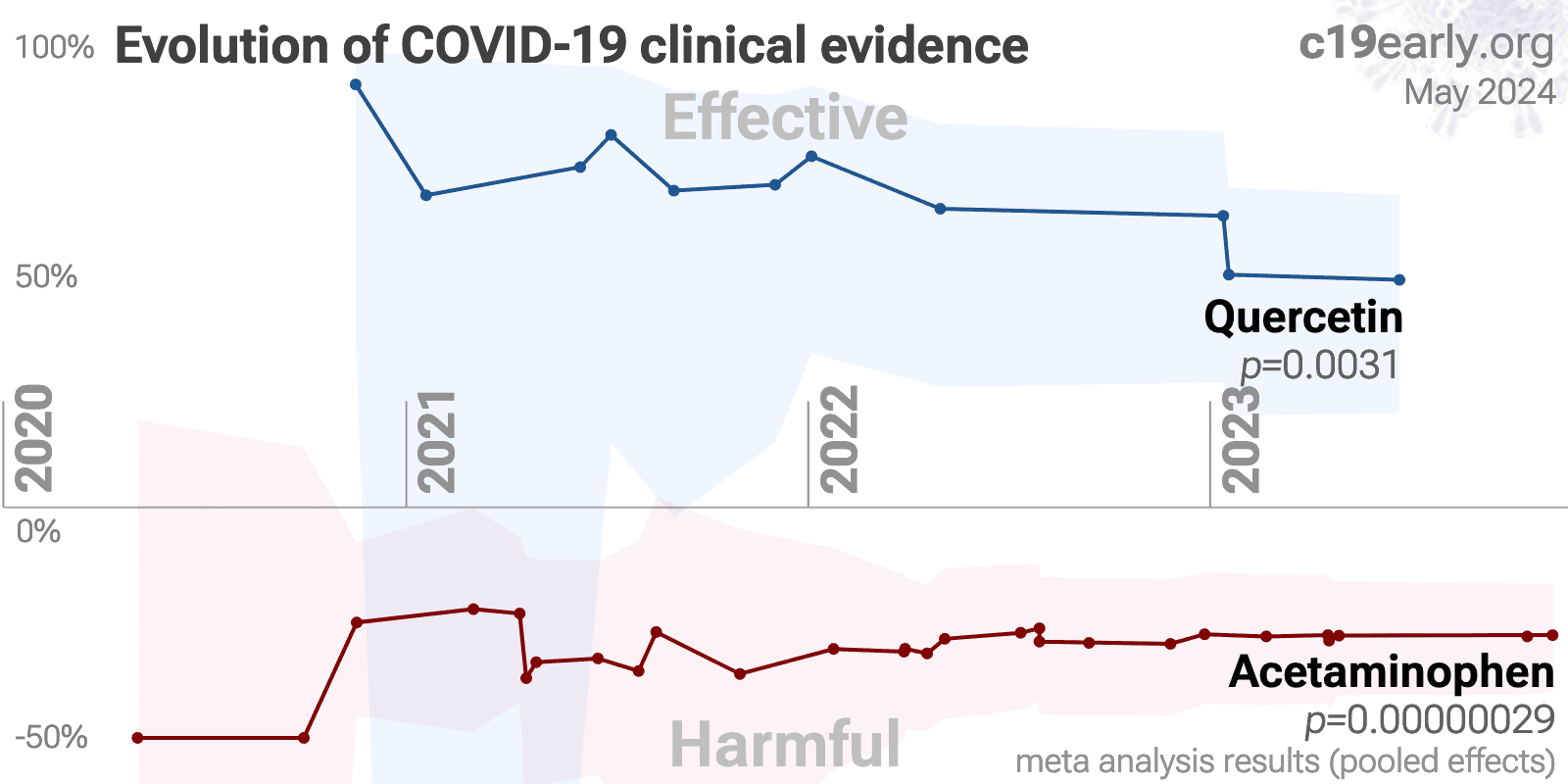
Fig. 21 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
{kind=link}
Fig. 21. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as differences in treatment delay are more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta-analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
Publishing is often biased
towards positive results, however evidence suggests that there may be a negative bias for
inexpensive treatments for COVID-19. Both negative and positive results are
very important for COVID-19, media in many countries prioritizes negative
results for inexpensive treatments (inverting the typical incentive for
scientists that value media recognition), and there are many reports of
difficulty publishing positive results177-180.
For quercetin, there is currently not
enough data to evaluate publication bias with high confidence.
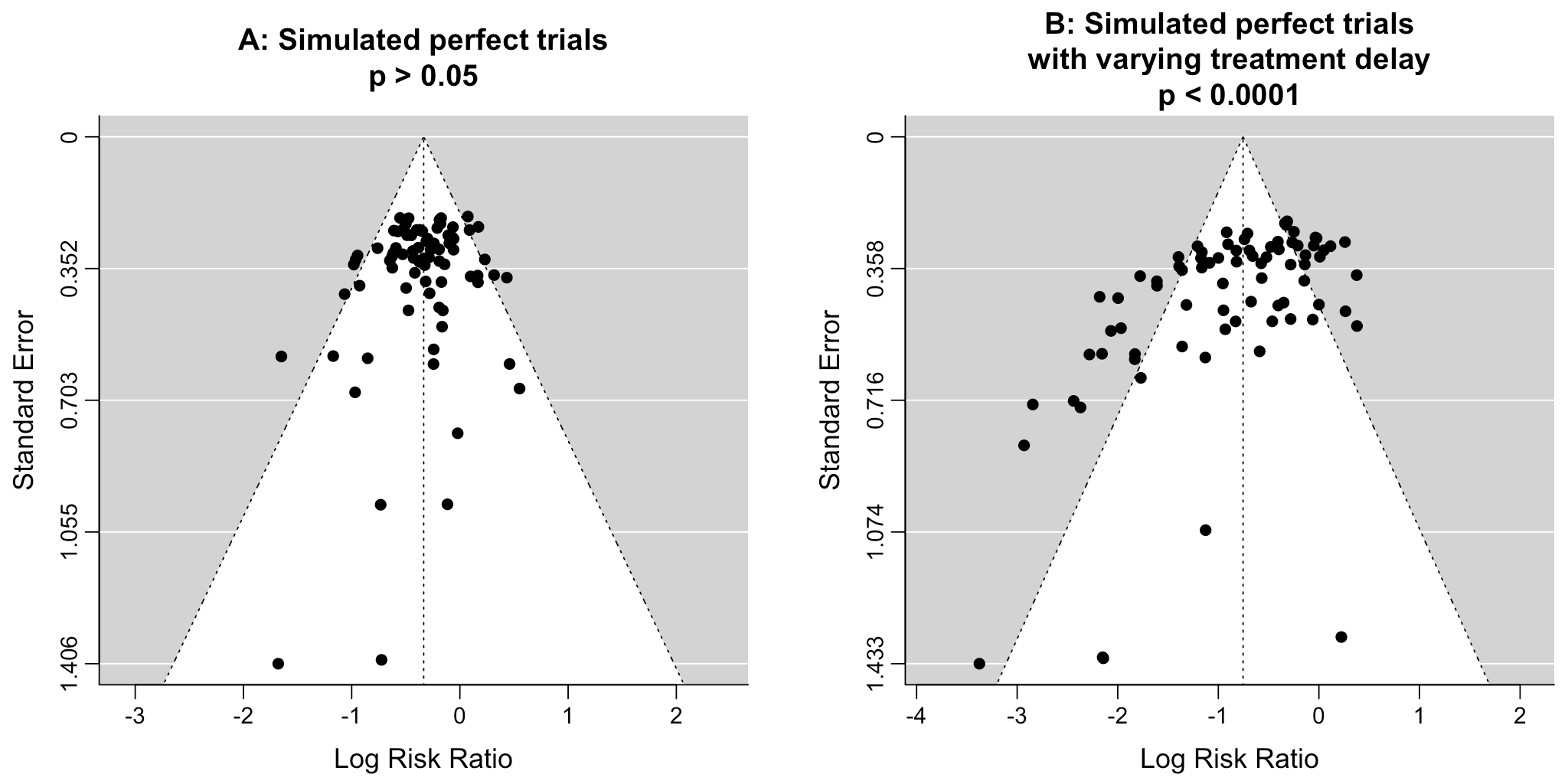
Funnel
plots have traditionally been used for analyzing publication bias. This is
invalid for COVID-19 acute treatment trials — the underlying assumptions
are invalid, which we can demonstrate with a simple example. Consider a set of
hypothetical perfect trials with no bias. Fig. 22 plot A
shows a funnel plot for a simulation of 80 perfect trials, with random group
sizes, and each patient's outcome randomly sampled (10% control event
probability, and a 30% effect size for treatment). Analysis shows no asymmetry
(p > 0.05). In plot B, we add a single typical variation in COVID-19 treatment
trials — treatment delay. Consider that efficacy varies from 90% for
treatment within 24 hours, reducing to 10% when treatment is delayed 3 days.
In plot B, each trial's treatment delay is randomly selected. Analysis now
shows highly significant asymmetry, p < 0.0001, with six variants of
Egger's test all showing p < 0.05181-188.
Note that these tests fail even though treatment delay is uniformly
distributed. In reality treatment delay is more complex — each trial has
a different distribution of delays across patients, and the distribution
across trials may be biased (e.g., late treatment trials may be more common).
Similarly, many other variations in trials may produce asymmetry, including
dose, administration, duration of treatment, differences in SOC,
comorbidities, age, variants, and bias in design, implementation, analysis,
and reporting.
{kind=link}
Fig. 22. Example funnel plot analysis for simulated perfect trials.
Pharmaceutical drug
trials often have conflicts of interest whereby sponsors or trial staff have a
financial interest in the outcome being positive. Quercetin for COVID-19
lacks this because it is an inexpensive and widely available supplement.
In contrast, most COVID-19 quercetin trials have been run by
physicians on the front lines with the primary goal of finding the best
methods to save human lives and minimize the collateral damage caused by
COVID-19. While pharmaceutical companies are careful to run trials under
optimal conditions (for example, restricting patients to those most likely to
benefit, only including patients that can be treated soon after onset when
necessary, and ensuring accurate dosing), not all quercetin trials
represent the optimal conditions for efficacy.
Table 5 shows the reported results of physicians that used combined
early treatment protocols for COVID-19, compared to results for physicians following
guidelines focusing on late treatment (Dr. Uip reportedly prescribed early treatment for
himself, but not for patients189). The protocols vary, but include ivermectin,
HCQ, vitamin D, vitamin C, zinc, melatonin, quercetin, budesonide, and other treatments.
These results are subject to selection and ascertainment bias and more accurate analysis
requires details of the patient populations and follow-up, however results are consistently
better across many teams, and consistent with the extensive controlled trial evidence that
shows a significant reduction in risk with many early treatments, and improved results
with the use of multiple treatments in combination.
| LATE TREATMENT | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. David Uip (*) | Brazil | 2,200 | 38.6% (850) | 2.5% (54) |
| Dr. Jake Scott (**) | USA | 1,000 | 10.0% (100) | |
| Average | 38.6% | 6.2% | ||
| EARLY TREATMENT PROTOCOLS - 40 physicians/teams | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. Roberto Alfonso Accinelli 0/360 deaths for treatment within 3 days |
Peru | 1,265 | 0.6% (7) | |
| Dr. Mohammed Tarek Alam patients up to 84 years old |
Bangladesh | 100 | 0.0% (0) | |
| Dr. Oluwagbenga Alonge | Nigeria | 310 | 0.0% (0) | |
| Dr. Raja Bhattacharya up to 88yo, 81% comorbidities |
India | 148 | 1.4% (2) | |
| Dr. Flavio Cadegiani | Brazil | 3,450 | 0.1% (4) | 0.0% (0) |
| Dr. Alessandro Capucci | Italy | 350 | 4.6% (16) | |
| Dr. Shankara Chetty | South Africa | 8,000 | 0.0% (0) | |
| Dr. Deborah Chisholm | USA | 100 | 0.0% (0) | |
| Dr. Ryan Cole | USA | 400 | 0.0% (0) | 0.0% (0) |
| Dr. Marco Cosentino earlier treatment results were better |
Italy | 392 | 6.4% (25) | 0.3% (1) |
| Dr. Jeff Davis | USA | 6,000 | 0.0% (0) | |
| Dr. Dhanajay | India | 500 | 0.0% (0) | |
| Dr. Bryan Tyson & Dr. George Fareed | USA | 20,000 | 0.0% (6) | 0.0% (4) |
| Dr. Raphael Furtado | Brazil | 170 | 0.6% (1) | 0.0% (0) |
| Rabbi Yehoshua Gerzi | Israel | 860 | 0.1% (1) | 0.0% (0) |
| Dr. Heather Gessling | USA | 1,500 | 0.1% (1) | |
| Dr. Ellen Guimarães | Brazil | 500 | 1.6% (8) | 0.4% (2) |
| Dr. Syed Haider | USA | 4,000 | 0.1% (5) | 0.0% (0) |
| Dr. Mark Hancock | USA | 24 | 0.0% (0) | |
| Dr. Sabine Hazan | USA | 1,000 | 0.0% (0) | |
| Dr. Mollie James | USA | 3,500 | 1.1% (40) | 0.0% (1) |
| Dr. Roberta Lacerda | Brazil | 550 | 1.5% (8) | 0.4% (2) |
| Dr. Katarina Lindley | USA | 100 | 5.0% (5) | 0.0% (0) |
| Dr. Ben Marble | USA | 150,000 | 0.0% (4) | |
| Dr. Edimilson Migowski | Brazil | 2,000 | 0.3% (7) | 0.1% (2) |
| Dr. Abdulrahman Mohana | Saudi Arabia | 2,733 | 0.0% (0) | |
| Dr. Carlos Nigro | Brazil | 5,000 | 0.9% (45) | 0.5% (23) |
| Dr. Benoit Ochs | Luxembourg | 800 | 0.0% (0) | |
| Dr. Ortore | Italy | 240 | 1.2% (3) | 0.0% (0) |
| Dr. Valerio Pascua one patient already on oxygen died |
Honduras | 415 | 6.3% (26) | 0.2% (1) |
| Dr. Sebastian Pop | Romania | 300 | 0.0% (0) | |
| Dr. Brian Proctor | USA | 869 | 2.3% (20) | 0.2% (2) |
| Dr. Anastacio Queiroz | Brazil | 700 | 0.0% (0) | |
| Dr. Didier Raoult | France | 8,315 | 2.6% (214) | 0.1% (5) |
| Dr. Karin Ried up to 99yo, 73% comorbidities |
Turkey | 237 | 0.4% (1) | |
| Dr. Roman Rozencwaig patients up to 86 years old |
Canada | 80 | 0.0% (0) | |
| Dr. Vipul Shah | India | 8,000 | 0.1% (5) | |
| Dr. Silvestre Sobrinho | Brazil | 116 | 8.6% (10) | 0.0% (0) |
| Dr. Unknown | Brazil | 957 | 1.7% (16) | 0.2% (2) |
| Dr. Vladimir Zelenko | USA | 2,200 | 0.5% (12) | 0.1% (2) |
| Average | 2.2% | 0.1% | ||
Summary statistics from
meta-analysis necessarily lose information. As with all meta-analyses, studies
are heterogeneous, with differences
in treatment delay, treatment regimen, patient demographics, variants,
conflicts of interest, standard of care, and other factors. We provide analyses for specific
outcomes and by treatment delay, and we aim to identify key characteristics in
the forest plots and summaries. Results should be viewed in the context of
study characteristics.
Some analyses classify treatment based on early or late
administration, as done here, while others distinguish between mild, moderate,
and severe cases. Viral load does not indicate degree of symptoms — for
example patients may have a high viral load while being asymptomatic. With
regard to treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.
Details of treatment delay per patient is often not available.
For example, a study may treat 90% of patients relatively early, but the
events driving the outcome may come from 10% of patients treated very late.
Our 5 day cutoff for early treatment may be too conservative, 5 days may be too late in many cases.
Comparison across treatments is confounded by differences in
the studies performed, for example dose, variants, and conflicts of interest.
Trials with conflicts of interest may use designs better suited to the
preferred outcome.
In some cases, the most serious outcome has very few events,
resulting in lower confidence results being used in pooled analysis, however
the method is simpler and more transparent. This is less critical as the
number of studies increases. Restriction to outcomes with sufficient power may
be beneficial in pooled analysis and improve accuracy when there are few
studies, however we maintain our pre-specified method to avoid any
retrospective changes.
Studies show that combinations of treatments can be highly
synergistic and may result in many times greater efficacy than individual
treatments alone153-175.
Therefore standard of care may be critical and benefits may diminish or
disappear if standard of care does not include certain treatments.
This real-time analysis is constantly updated based on
submissions. Accuracy benefits from widespread review and submission of
updates and corrections from reviewers. Less popular treatments may receive
fewer reviews.
No treatment or intervention is 100% available and
effective for all current and future variants. Efficacy may vary significantly
with different variants and within different populations. All treatments have
potential side effects. Propensity to experience side effects may be predicted
in advance by qualified physicians. We do not provide medical advice. Before
taking any medication, consult a qualified physician who can compare all
options, provide personalized advice, and provide details of risks and
benefits based on individual medical history and situations.
SARS-CoV-2 infection and replication involves a complex
interplay of 500+ host and viral proteins and other
factors37-44, providing many therapeutic
targets.
Over 11,000 compounds have been predicted to reduce COVID-19
risk45, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
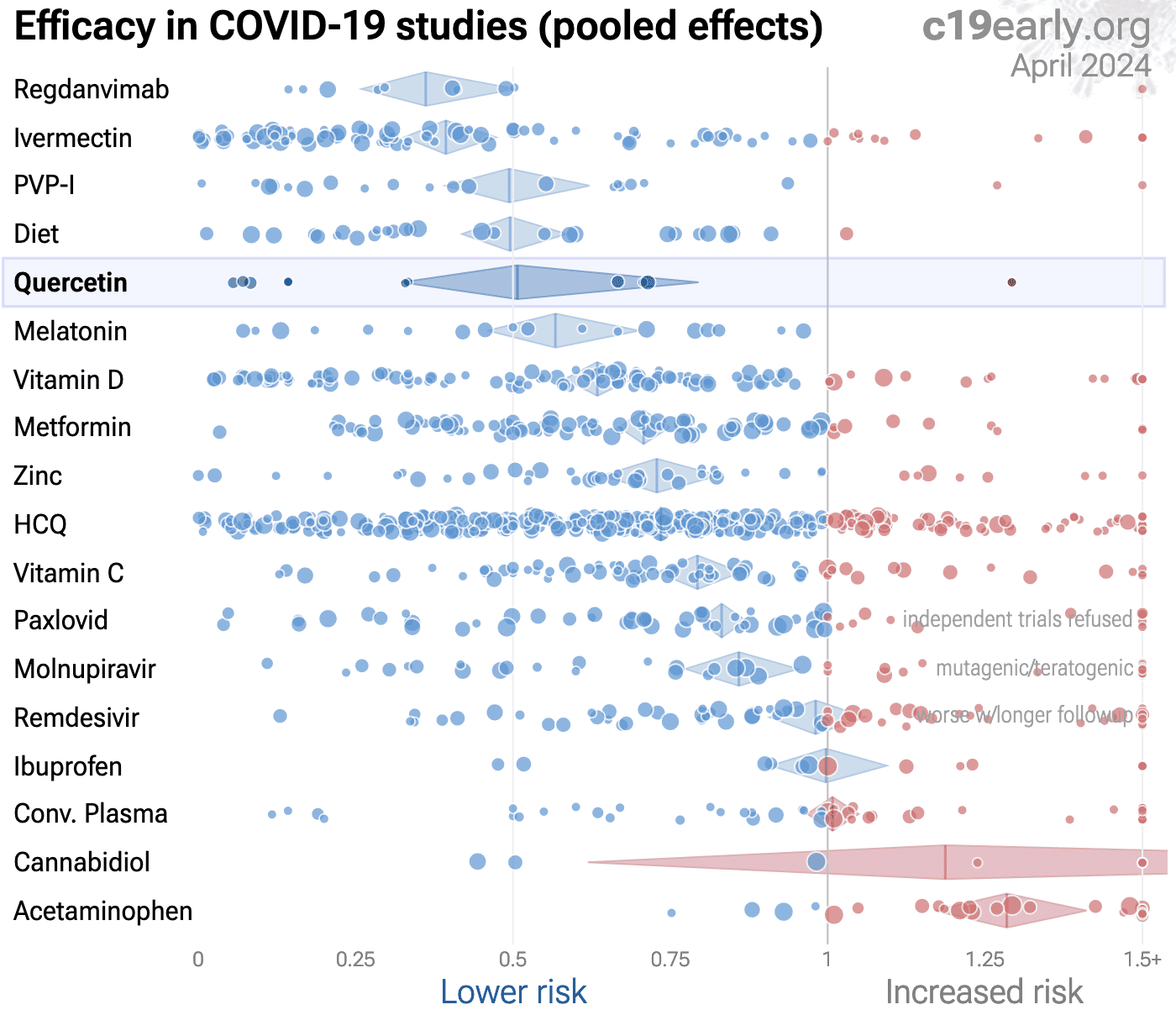
Fig. 23 shows an overview of the results for quercetin
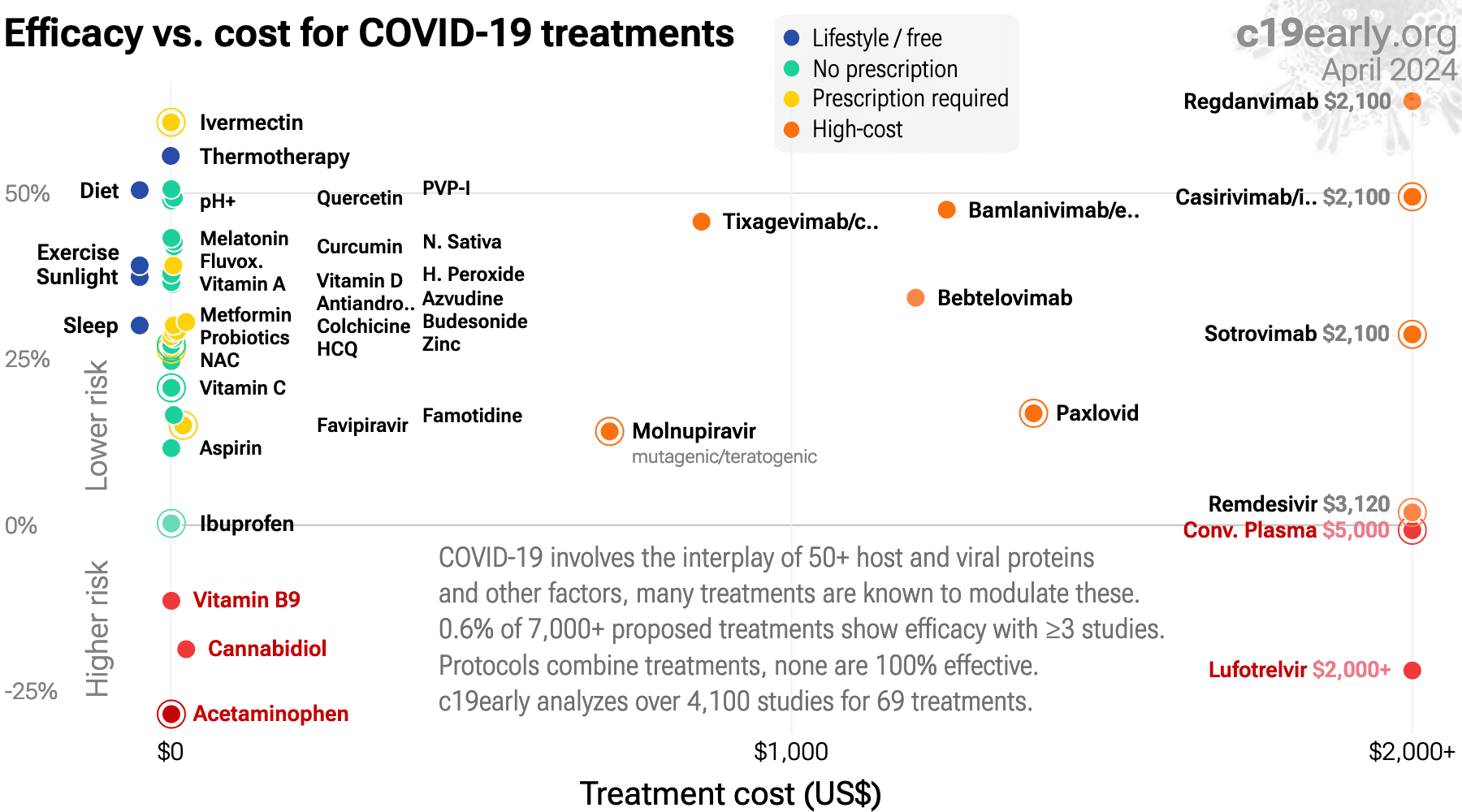
in the context of multiple COVID-19 treatments, and Fig. 24 shows a plot
of efficacy vs. cost for COVID-19 treatments.
{kind=link}
{kind=link}
Fig. 24. Efficacy vs. cost for COVID-19 treatments.
Studies to date show that quercetin is
an effective treatment for COVID-19.
Significantly lower risk is seen for mortality, ICU admission, hospitalization, recovery, cases, and viral clearance. 9 studies from 7 independent teams in 5 countries show significant
benefit.
Meta-analysis using the most serious outcome reported shows
35% [15‑51%] lower risk. Results are similar for higher quality studies and better after excluding studies using combined treatment.
Currently all studies are RCTs.
Currently there is limited data, with only 841 patients in trials to date.
Studies typically use advanced formulations for greatly improved bioavailability.
Other meta-analyses show significant improvements with quercetin for mortality5, ICU admission5,6, and hospitalization5,6.
Contact.
Contact us on X at @CovidAnalysis.
Funding.
We have received no funding or
compensation in any form, and do not accept donations. This is entirely volunteer work.
Conflicts of interest.
We have no conflicts of interest.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.AI.
We use AI models (Gemini, Grok, Claude, and
ChatGPT) tasked with functioning as additional peer-reviewers to check for errors, suggest
improvements, and review spelling and grammar. Any corrections are verified and applied
manually. Our preference for em dashes is independent of AI.Updates.
Our COVID-19 meta-analyses involve the extraction of over 226,000
datapoints from thousands of papers for 226 treatments. We thank the
thousands of scientists, physicians, and other contributors that have provided updates,
suggestions, feedback, and corrections. These are all welcome and can be submitted
at https://c19early.org/qmeta.html.
Dedication.
This work is dedicated to top
evidence-based physicians that worked tirelessly to analyze evidence and greatly reduce
mortality and morbidity during the pandemic. In alphabetical order:
Dr. Thomas J. Borody, Dr. Mary Talley Bowden, Dr. Flavio Cadegiani, Dr. Shankara Chetty,
Dr. Ryan Cole, Dr. George Fareed, Dr. Sabine Hazan, Dr. Pierre Kory, Dr. Tess Lawrie, Dr.
Robert Malone, Dr. Paul Marik, Dr. Peter McCullough, Dr. Didier Raoult, Dr. Harvey Risch,
Dr. Jackie Stone, Dr. Brian Tyson, Dr. Joseph Varon, and Dr. Vladimir (Zev) Zelenko.
Public domain.
This is a public domain work
distributed in accordance with the Creative Commons CC0 1.0 Universal license, which
dedicates the work to the public domain by waiving all rights worldwide under copyright law.
You can distribute, remix, adapt, and build upon this work in any medium or format,
including for commercial purposes, without asking permission. Referenced material and
third-party images retain any original copyrights or restrictions.
See: https://creativecommons.org/publicdomain/zero/1.0/.
{kind=link}
RCT 100 outpatients in Pakistan, 50 treated with quercetin phytosome, showing faster viral clearance and improved recovery with treatment.
Patients in the treatment group were significantly younger (41 vs. 54). Authors report performing a covariance analysis but do not provide any data.
Table 1 reports the standard deviation for age as exactly 2.03 in both the control group and the quercetin group, which is possible but relatively unlikely. The text states the overall mean age was 47.6 +/- 15.7 years. However, mathematically pooling two groups of n=50 with means of 54.1 and 41.1 and standard deviations of 2.03 yields a combined standard deviation of approximately 6.83, not 15.7. The text states the modal age group was between 30-40 years, comprising 23% of total cases. However, given the reported means and assuming a normal distribution, virtually 0% of the patients would fall into the 30-40 age bracket. It is likely that one or both of the 2.03 standard deviations is a typo/incorrect.
The text claims that by week two, 98% in the quercetin group tested negative for SARS-CoV-2. However, Figure 3 shows 2 patients (4%) positive at day 14 in the quercetin group, meaning only 96% tested negative.
Patients in the treatment group were significantly younger (41 vs. 54). Authors report performing a covariance analysis but do not provide any data.
Table 1 reports the standard deviation for age as exactly 2.03 in both the control group and the quercetin group, which is possible but relatively unlikely. The text states the overall mean age was 47.6 +/- 15.7 years. However, mathematically pooling two groups of n=50 with means of 54.1 and 41.1 and standard deviations of 2.03 yields a combined standard deviation of approximately 6.83, not 15.7. The text states the modal age group was between 30-40 years, comprising 23% of total cases. However, given the reported means and assuming a normal distribution, virtually 0% of the patients would fall into the 30-40 age bracket. It is likely that one or both of the 2.03 standard deviations is a typo/incorrect.
The text claims that by week two, 98% in the quercetin group tested negative for SARS-CoV-2. However, Figure 3 shows 2 patients (4%) positive at day 14 in the quercetin group, meaning only 96% tested negative.
{kind=link}
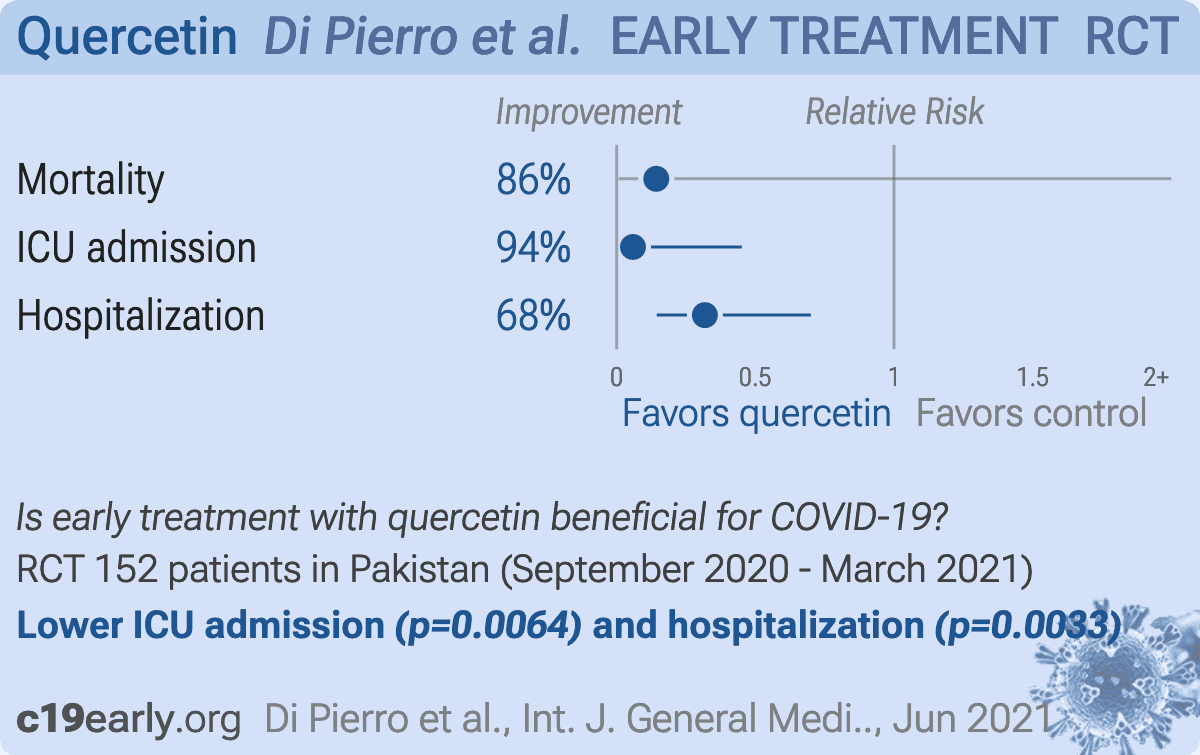
RCT 152 outpatients in Pakistan, 76 treated with quercetin phytosome, showing lower mortality, ICU admission, and hospitalization with treatment.
Potential data issues include:
Table 5 hospitalization frequency mismatch: Table 5 reports 7 hospitalized patients for the SC group. The mean length of stay (5.14) matches 36 days across 7 patients. However, the explicit frequency counts below list 15 patients with a total of 90 days. Similarly, Table 5 reports 4 hospitalized patients for the QP group, however the frequency column explicitly lists 3 patients at 1 day and 4 patients at 2 days (summing to 7 patients). This may be a typographical error with several values matching Table 2.
Baseline age matching: the age distribution across 7 distinct brackets is very close between the control and treatment groups (maximum difference of 2 patients in any bracket). This level of balance is unusual for a 1:1 simple randomization of 152 patients.
Large unadjusted baseline comorbidity imbalance: despite near-perfect age matching, there is a large and statistically significant imbalance in baseline comorbidities (59.2% SC vs 38.2% QP, p=0.0092), without adjustment. The imbalance in comorbidities despite equal group sizes suggests failure of the randomization sequence or allocation concealment.
Lack of any missing data or dropouts: the study reports 100% adherence and zero dropouts or loss to follow-up over a 30-day period for 152 outpatients, which is unusual for a trial of this nature.
Potential data issues include:
Table 5 hospitalization frequency mismatch: Table 5 reports 7 hospitalized patients for the SC group. The mean length of stay (5.14) matches 36 days across 7 patients. However, the explicit frequency counts below list 15 patients with a total of 90 days. Similarly, Table 5 reports 4 hospitalized patients for the QP group, however the frequency column explicitly lists 3 patients at 1 day and 4 patients at 2 days (summing to 7 patients). This may be a typographical error with several values matching Table 2.
Baseline age matching: the age distribution across 7 distinct brackets is very close between the control and treatment groups (maximum difference of 2 patients in any bracket). This level of balance is unusual for a 1:1 simple randomization of 152 patients.
Large unadjusted baseline comorbidity imbalance: despite near-perfect age matching, there is a large and statistically significant imbalance in baseline comorbidities (59.2% SC vs 38.2% QP, p=0.0092), without adjustment. The imbalance in comorbidities despite equal group sizes suggests failure of the randomization sequence or allocation concealment.
Lack of any missing data or dropouts: the study reports 100% adherence and zero dropouts or loss to follow-up over a 30-day period for 152 outpatients, which is unusual for a trial of this nature.
{kind=link}
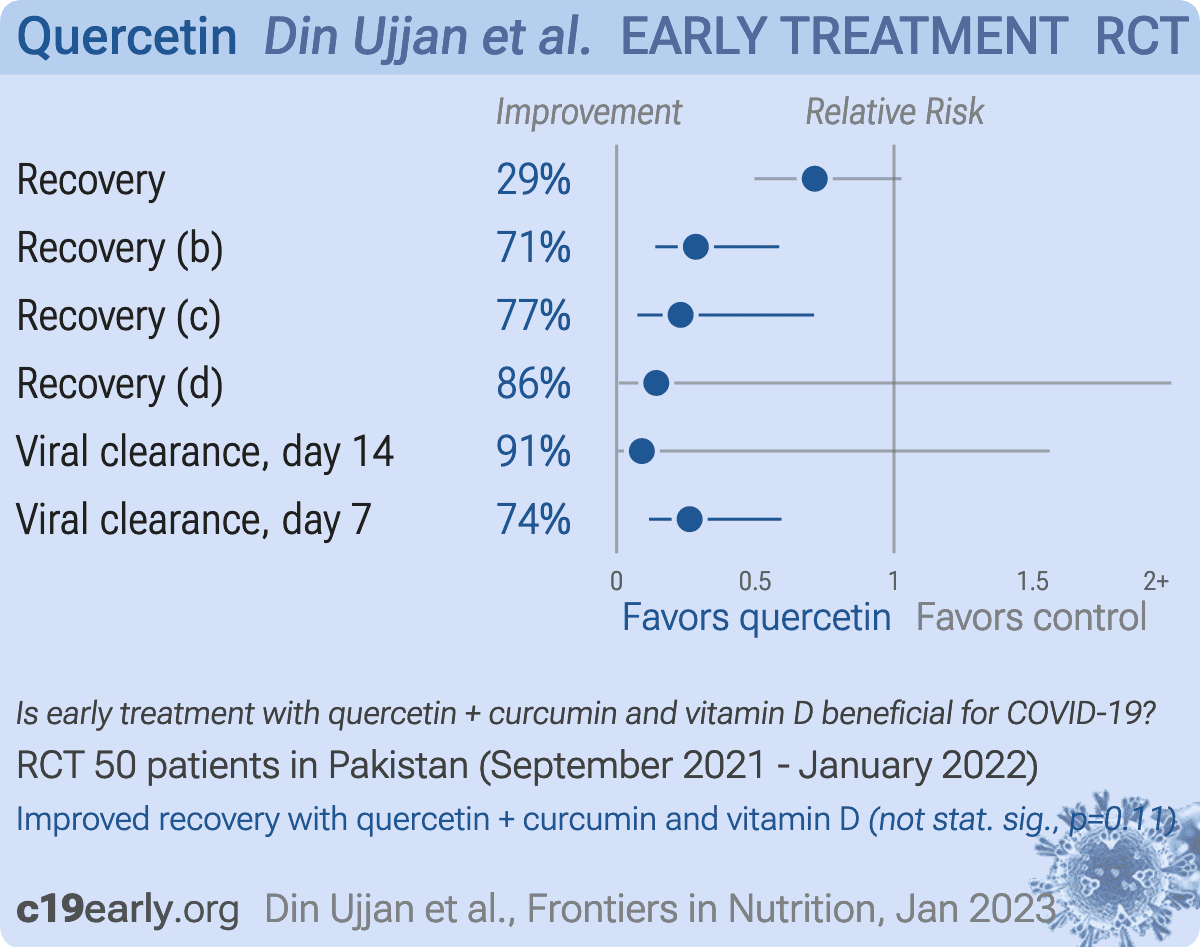
Small RCT with 50 outpatients, 25 treated with curcumin, quercetin, and vitamin D, showing improved recovery and viral clearance with treatment. 168mg curcumin, 260mg, 360IU vitamin D3 daily for 14 days.
Unadjusted baseline differences: the treatment arm had significantly more comorbidities, but the control arm had significantly more myalgia and asthenia, suggesting poor randomization and potential selection bias. In Table 1, the control arm value for '>=5 symptoms' is listed as '15 (60.05)', where 60.05 is a typo for 60.0%.
Unadjusted baseline differences: the treatment arm had significantly more comorbidities, but the control arm had significantly more myalgia and asthenia, suggesting poor randomization and potential selection bias. In Table 1, the control arm value for '>=5 symptoms' is listed as '15 (60.05)', where 60.05 is a typo for 60.0%.
{kind=link}
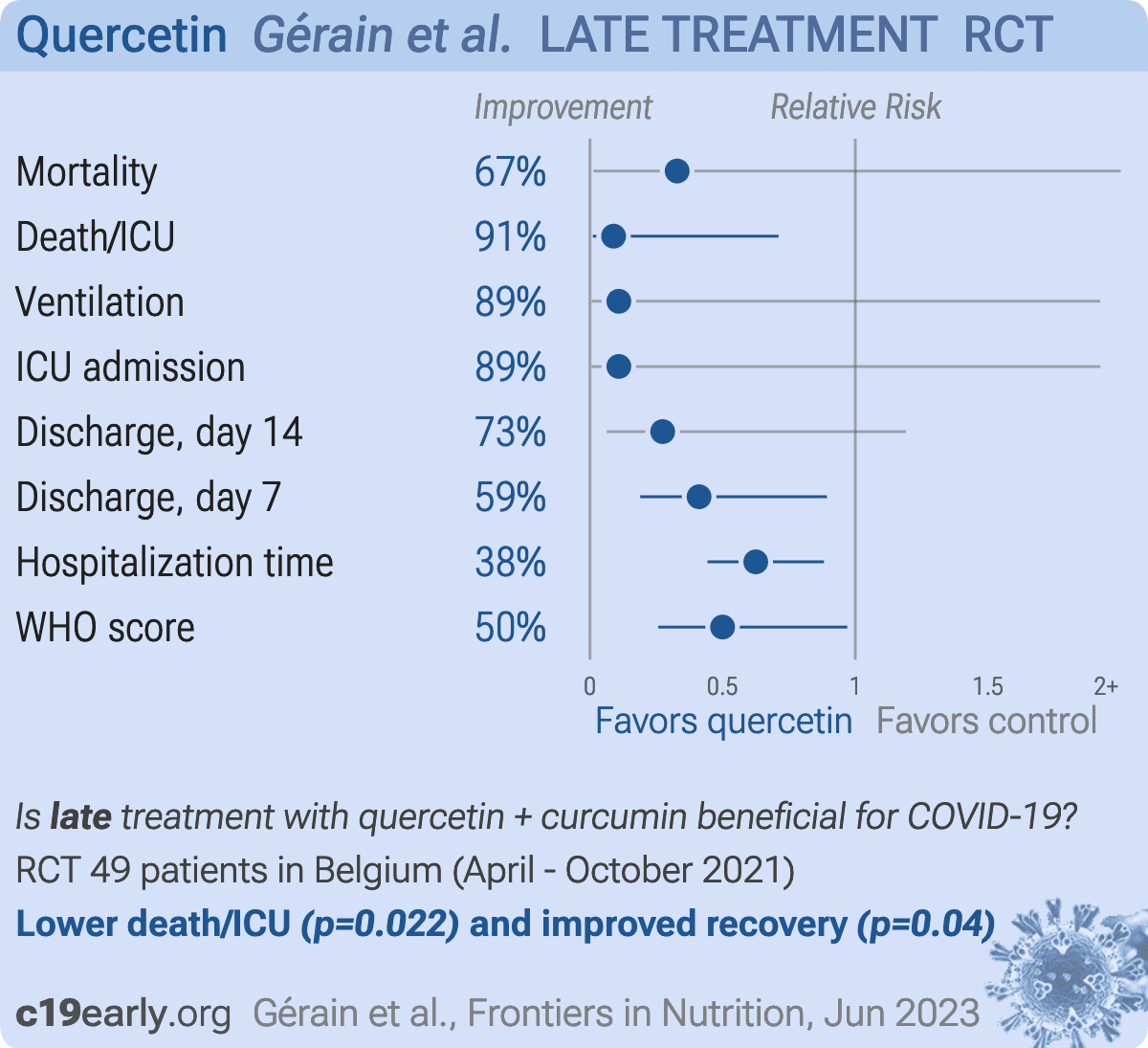
RCT 49 hospitalized COVID-19 patients, 25 treated with curcumin and quercetin, shower lower mortality/ICU admission and improved recovery with treatment. All patients received vitamin D.
336mg curcumin, 520mg quercetin, and 18μg vitamin D3 daily for 14 days. The control arm received 20μg vitamin D3 daily. The baseline differences in fever favors the treatment group while the difference in vaccination favors the control group.
Figure 1 indicates that 8 patients (2 in Nasafytol, 6 in Fultium) discontinued the supplement or withdrew. However, Section 3 explicitly states, 'All patients included in the FAS population were compliant with the protocol; the PP population was therefore the same as the FAS population.'
Unexplained missing data in the day 7 outcome evaluation: Table 2 reports an N=22 for the Nasafytol group for the Day 7 score change. With an original N=25 and 2 withdrawals noted in Figure 1, the evaluated N should be 23. The absence of the 3rd patient is not explained.
The inclusion criteria specify a severity of 3-4-5 according to a '7-point ordinal scale', but Figure 2 presents baseline and outcome data plotted on a 9-point scale (0 to 8).
336mg curcumin, 520mg quercetin, and 18μg vitamin D3 daily for 14 days. The control arm received 20μg vitamin D3 daily. The baseline differences in fever favors the treatment group while the difference in vaccination favors the control group.
Figure 1 indicates that 8 patients (2 in Nasafytol, 6 in Fultium) discontinued the supplement or withdrew. However, Section 3 explicitly states, 'All patients included in the FAS population were compliant with the protocol; the PP population was therefore the same as the FAS population.'
Unexplained missing data in the day 7 outcome evaluation: Table 2 reports an N=22 for the Nasafytol group for the Day 7 score change. With an original N=25 and 2 withdrawals noted in Figure 1, the evaluated N should be 23. The absence of the 3rd patient is not explained.
The inclusion criteria specify a severity of 3-4-5 according to a '7-point ordinal scale', but Figure 2 presents baseline and outcome data plotted on a 9-point scale (0 to 8).
{kind=link}
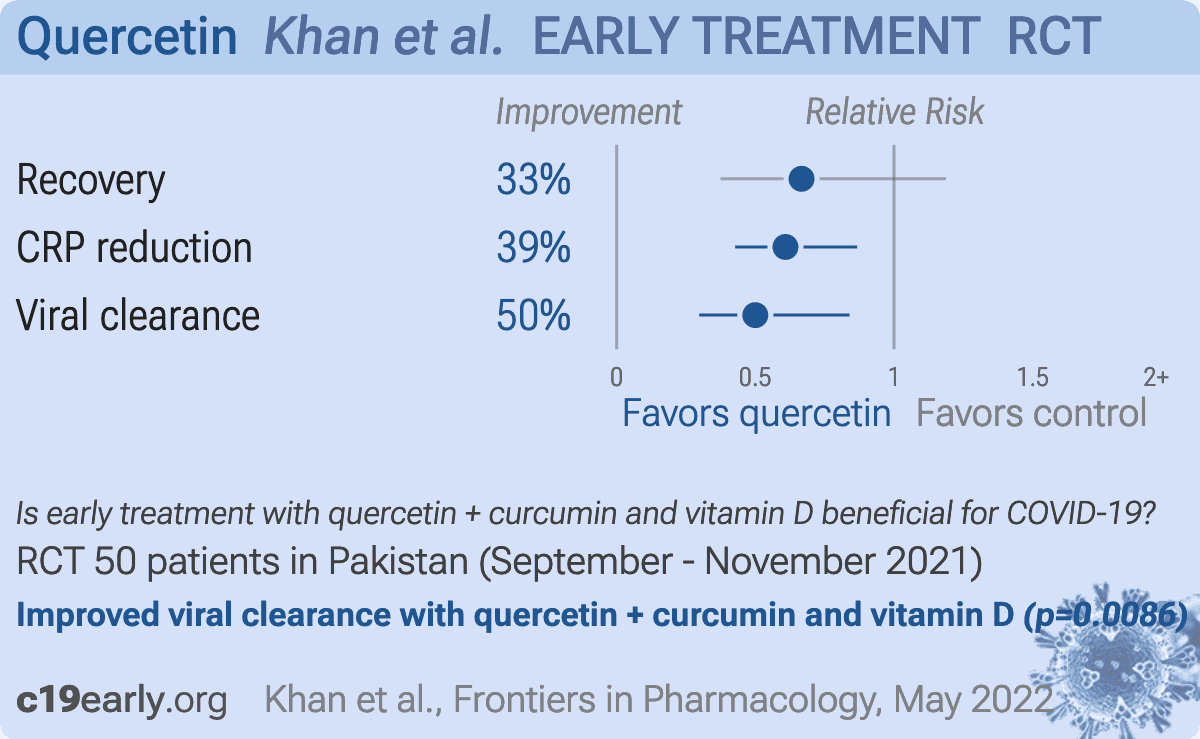
RCT 50 COVID+ outpatients in Pakistan, 25 treated with curcumin, quercetin, and vitamin D, showing significantly faster viral clearance, significantly improved CRP, and faster resolution of acute symptoms (p=0.154). 168mg curcumin, 260mg quercetin and 360IU cholecalciferol.
{kind=link}
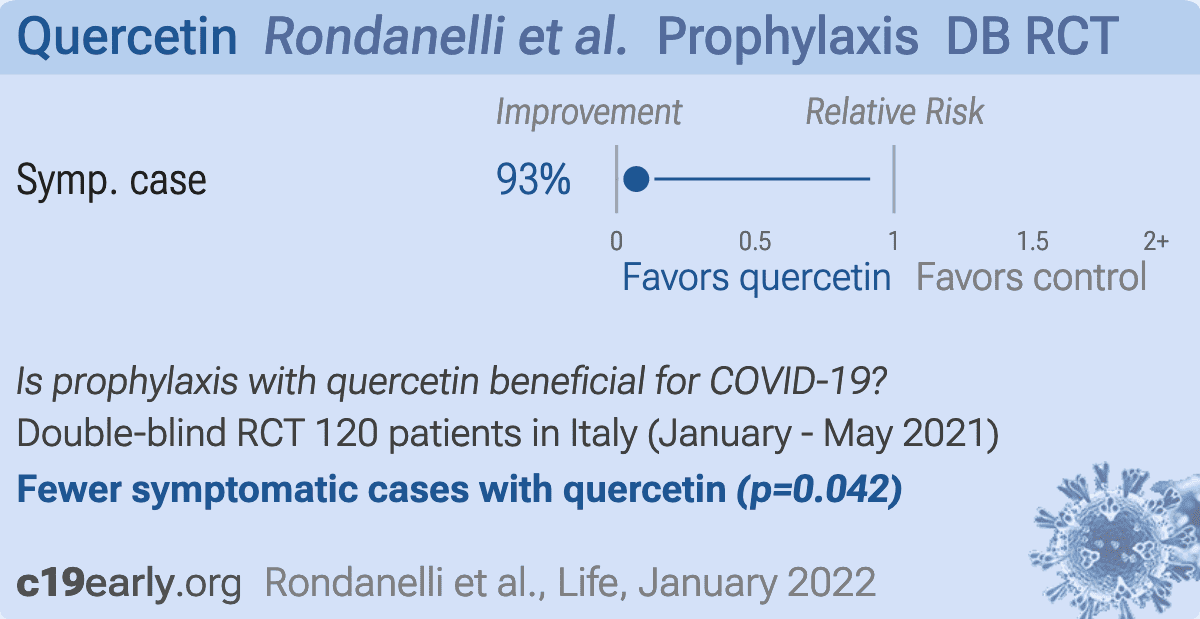
RCT 120 healthcare workers, 60 treated with quercetin phytosome, showing lower risk of cases with treatment. Quercetin phytosome 250mg twice a day.
Section 2.1 states: 'A maximal follow-up period was determined to be at 3 months.' However, Section 3 (Results) and Figure 4 report data and Kaplan-Meier survival curves extending to 5 months.
The authors declare no conflict of interest, however several authors list their affiliation as 'Research and Development Unit, Indena SpA'. Indena SpA is the manufacturer and patent holder of the specific Quercetin Phytosome delivery system tested in this trial.
Section 2.1 defines the primary endpoint as 'The termination of the participant's use of the quercetin supplement earlier than 3 months or having an active coronavirus infection' (a prevention endpoint). However, Section 3 states 'The primary endpoint was time to clinical improvement up to day 17 of the infection' (a treatment efficacy endpoint).
The text in Section 3 states 'A hazard ratio of 14.04 means that subjects...', but Table 4 shows Exp(B) as 14.097.
Section 2.1 states: 'A maximal follow-up period was determined to be at 3 months.' However, Section 3 (Results) and Figure 4 report data and Kaplan-Meier survival curves extending to 5 months.
The authors declare no conflict of interest, however several authors list their affiliation as 'Research and Development Unit, Indena SpA'. Indena SpA is the manufacturer and patent holder of the specific Quercetin Phytosome delivery system tested in this trial.
Section 2.1 defines the primary endpoint as 'The termination of the participant's use of the quercetin supplement earlier than 3 months or having an active coronavirus infection' (a prevention endpoint). However, Section 3 states 'The primary endpoint was time to clinical improvement up to day 17 of the infection' (a treatment efficacy endpoint).
The text in Section 3 states 'A hazard ratio of 14.04 means that subjects...', but Table 4 shows Exp(B) as 14.097.
{kind=link}
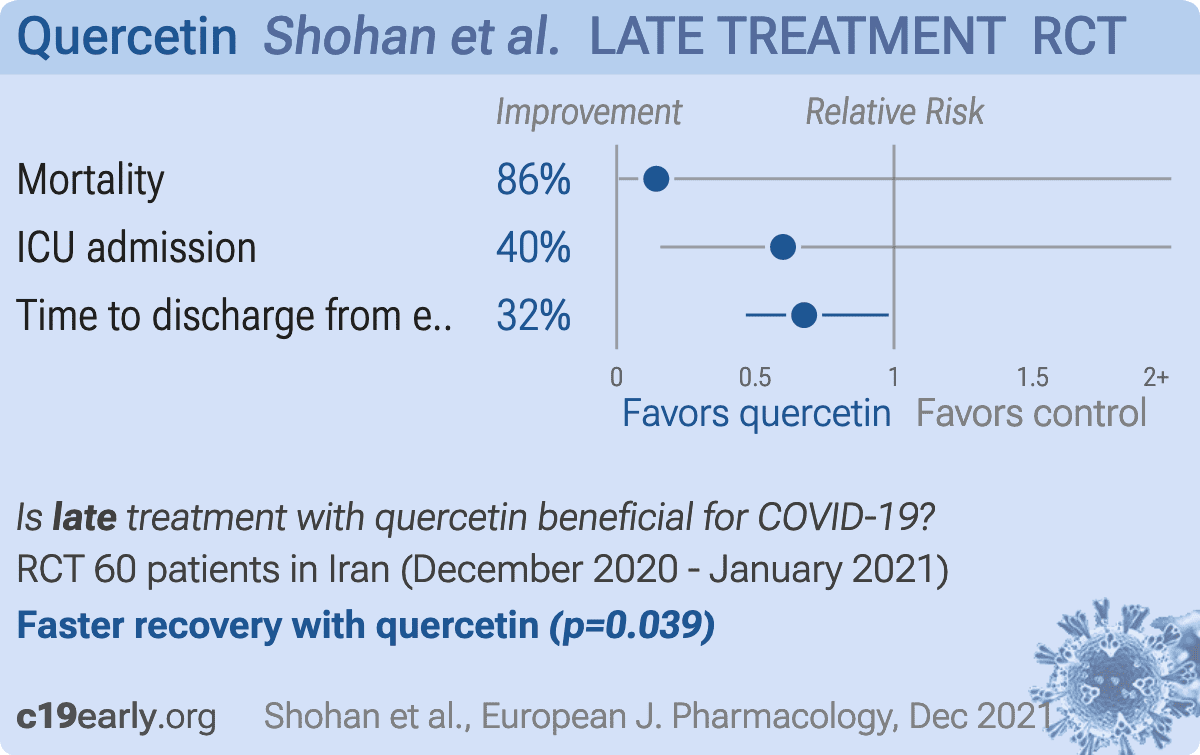
Small RCT with 60 severe hospitalized patients in Iran, 30 treated with quercetin, showing shorter time until discharge. All patients received remdesivir or favipiravir, and vitamin C, vitamin D, famotidine, zinc, dexamethasone, and magnesium (depending on serum levels). Quercetin 1000mg daily for 7 days.
Table 1 shows the duration of symptoms before randomization was 9.43 days in the Control group and 7.77 days in the quercetin group (P=0.043). Table 1 also shows that fever at baseline was present in 50% of the control group but 80% of the quercetin group (P=0.015).
The study was unblinded, and one of the primary endpoints that achieved significance was 'time to discharge'. Hospital discharge is a subjective clinical decision.
Table 1 shows the duration of symptoms before randomization was 9.43 days in the Control group and 7.77 days in the quercetin group (P=0.043). Table 1 also shows that fever at baseline was present in 50% of the control group but 80% of the quercetin group (P=0.015).
The study was unblinded, and one of the primary endpoints that achieved significance was 'time to discharge'. Hospital discharge is a subjective clinical decision.
{kind=link}
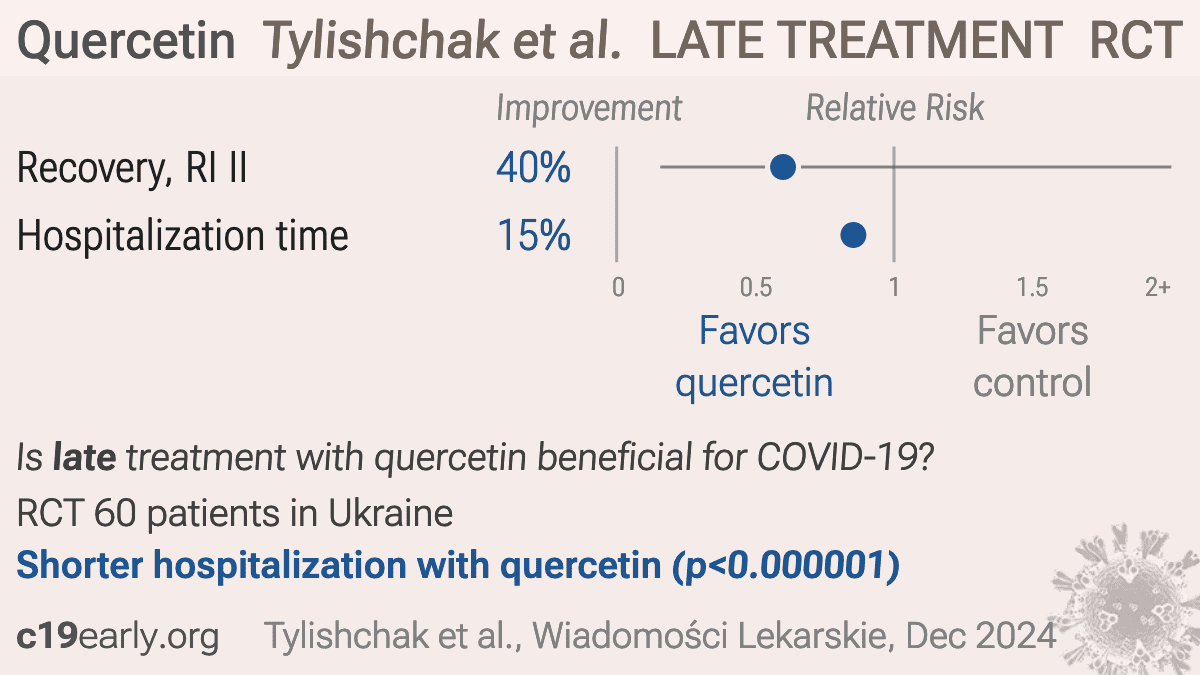
RCT 60 hospitalized COVID-19 patients with type 2 diabetes showing quercetin treatment decreased levels of inflammatory markers (interleukin-6, CRP, ferritin), reduced length of hospital stay, and improved capillaroscopy measures compared to standard care. Quercetin was administered at 0.5g intravenously once daily for 10 days. The authors hypothesize the benefits may be due to the anti-inflammatory, antioxidant and endothelium-protective effects of quercetin,
Authors explicitly used independent groups Chi-square (Pearson's) and independent groups Student's t-tests to evaluate paired before-and-after data within the exact same groups (e.g., saturation before vs after, χ² for edema before vs after).
Table 3 reports values as M±m. The reported t-test values in the text indicate 'm' was treated as the Standard Error of the Mean (SEM). However, the SEM values for the Main Group baseline parameters are very large (e.g., arterial capillary diameter 8.31 ± 1.93). For a sample size of 30, an SEM of 1.93 translates to a Standard Deviation of roughly 10.5. This suggests potential incorrect labeling or other error.
The paper provides an overall age and gender breakdown but fails to report baseline demographics per group.
Authors explicitly used independent groups Chi-square (Pearson's) and independent groups Student's t-tests to evaluate paired before-and-after data within the exact same groups (e.g., saturation before vs after, χ² for edema before vs after).
Table 3 reports values as M±m. The reported t-test values in the text indicate 'm' was treated as the Standard Error of the Mean (SEM). However, the SEM values for the Main Group baseline parameters are very large (e.g., arterial capillary diameter 8.31 ± 1.93). For a sample size of 30, an SEM of 1.93 translates to a Standard Deviation of roughly 10.5. This suggests potential incorrect labeling or other error.
The paper provides an overall age and gender breakdown but fails to report baseline demographics per group.
{kind=link}
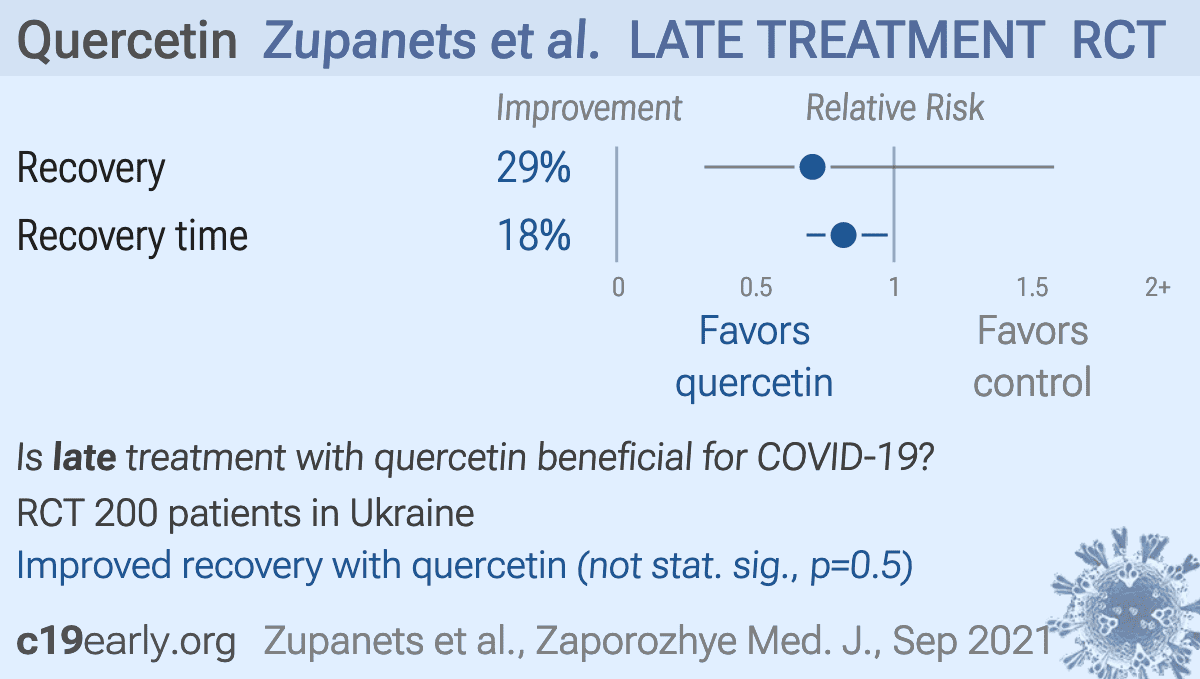
RCT 200 patients in Ukraine, 99 treated with IV quercetin/polyvinylirolidone followed by oral quercetin/pectin, showing improved recovery with treatment.
The paper states 'authors have no conflict of interest to declare.' However, author M. F. Pasichnyk is listed in the affiliations block as the 'General Director of PJSC SIC Borshchahivskiy CPP'. This entity is the Ukrainian pharmaceutical company that manufactures and holds the patents/trademarks for the proprietary intravenous and oral quercetin formulations (Corvitin/Quertin) evaluated in this study.
The study was unblinded (open-label). The treatment group received daily intravenous infusions for 10 days, while the control group only received 'basic therapy' without a placebo IV. Because primary measures of efficacy included subjective symptoms like 'general weakness evaluated by VAS' and 'cough,' the lack of blinding and uneven care administration introduces potential bias.
The study lacks a CONSORT flow diagram.
Mathematical discrepancies in text versus table data.: The text states that in the main group, the average increase in D-dimer at visit 16 was 149.6 ng/ml, but calculating the difference from Table 3 means (1147.0 at visit 16 minus 1004.2 at baseline) yields 142.8 ng/ml. Similar small discrepancies exist for the other visit calculations, suggesting a potential mix-up between 'mean of differences' and 'difference of means' or improper handling of missing data points.
The paper states 'authors have no conflict of interest to declare.' However, author M. F. Pasichnyk is listed in the affiliations block as the 'General Director of PJSC SIC Borshchahivskiy CPP'. This entity is the Ukrainian pharmaceutical company that manufactures and holds the patents/trademarks for the proprietary intravenous and oral quercetin formulations (Corvitin/Quertin) evaluated in this study.
The study was unblinded (open-label). The treatment group received daily intravenous infusions for 10 days, while the control group only received 'basic therapy' without a placebo IV. Because primary measures of efficacy included subjective symptoms like 'general weakness evaluated by VAS' and 'cough,' the lack of blinding and uneven care administration introduces potential bias.
The study lacks a CONSORT flow diagram.
Mathematical discrepancies in text versus table data.: The text states that in the main group, the average increase in D-dimer at visit 16 was 149.6 ng/ml, but calculating the difference from Table 3 means (1147.0 at visit 16 minus 1004.2 at baseline) yields 142.8 ng/ml. Similar small discrepancies exist for the other visit calculations, suggesting a potential mix-up between 'mean of differences' and 'difference of means' or improper handling of missing data points.
We perform ongoing searches of PubMed, medRxiv, Europe PMC, ClinicalTrials.gov, The Cochrane
Library, Google Scholar, Research Square, ScienceDirect, Oxford University Press, the
reference lists of other studies and meta-analyses, and submissions to the site c19early.org, which regularly receives notification of studies upon
publication.
Search terms are quercetin and COVID-19 or SARS-CoV-2. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of quercetin for COVID-19 that report a comparison with a
control group are included in the main analysis.
Sensitivity analysis is performed, excluding studies with major issues, epidemiological
studies, and studies with minimal available information.
Studies with major unexplained data issues, for example major outcome data that is
impossible to be correct with no response from the authors, are excluded.
{kind=link}

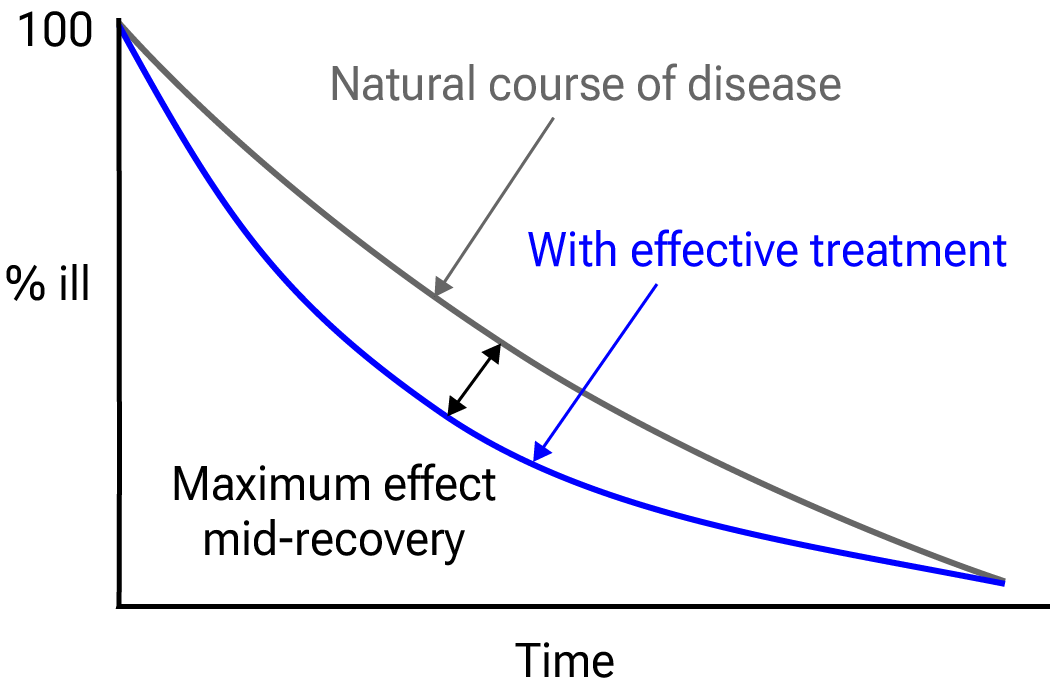
Fig. 25.
Mid-recovery results can more accurately reflect efficacy when almost all patients
recover. Mateja et al. confirm that intermediate viral load results more accurately
reflect hospitalization/death.
We extracted effect sizes and associated data from all studies. If studies report multiple
kinds of effects then the most serious outcome is used in pooled analysis, while
other outcomes are included in the outcome-specific analyses. For example, if effects for
mortality and cases are reported then they are both used in specific outcome analyses,
while mortality is used for pooled analysis.
If symptomatic results are reported at multiple times, we use the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28 days have
preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious outcome with
one or more events is used. For example, in low-risk populations with no mortality, a
reduction in mortality with treatment is not possible, however a reduction in
hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral outcomes.
When basically all patients recover in both treatment and control groups, preference for
viral clearance and recovery is given to results mid-recovery where available. After most
or all patients have recovered there is little or no room for an effective treatment to do
better, however faster recovery is valuable.
An IPD meta-analysis confirms that intermediate viral load reduction is more closely
associated with hospitalization/death than later viral load reduction383.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
Forest plots are computed using PythonMeta384 with the DerSimonian and
Laird random-effects model (the fixed effect assumption is not plausible in this case) and
inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
When results provide an odds ratio, we compute the relative risk when possible, or convert
to a relative risk according to Zhang (E) et al.
Reported confidence intervals and p-values are used when available, and adjusted
values are used when provided. If multiple types of adjustments are reported propensity
score matching and multivariable regression has preference over propensity score matching
or weighting, which has preference over multivariable regression. Adjusted results have
preference over unadjusted results for a more serious outcome when the adjustments
significantly alter results.
When needed, conversion between reported p-values and confidence intervals followed
Altman, Altman (B), and Fisher's exact test was used to calculate
p-values for event data. If continuity correction for zero values is required, we
use the reciprocal of the opposite arm with the sum of the correction factors equal to
1388.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of a negative
outcome when applicable (for example, the risk of death rather than the risk of survival).
If studies only report relative continuous values such as relative times, the ratio of the
time for the treatment group versus the time for the control group is used. Calculations
are done in Python (3.14.6) with
scipy (1.18.0), pythonmeta (1.26), numpy (2.5.1), statsmodels (0.14.6), and plotly (6.9.0).
Mixed-effects meta-regression results are computed with R (4.4.0) using the metafor
(4.6-0) and rms (6.8-0) packages, and using the most serious sufficiently powered outcome.
For all statistical tests, a p-value less than 0.05 was considered statistically
significant.
Grobid 0.8.2 is used to parse PDF documents.
When evaluating potential effect modification across groups, we use an
interaction test as described by Altman (C) et al. We compared the log-transformed
relative risks using a z-test, deriving the standard error of the difference from
the 95% confidence intervals. A two-sided interaction p-value of < 0.05 was
considered a statistically significant difference in treatment effect between the
groups.
Cochrane RoB 2/ROBINS-I are often used to evaluate studies, and have the advantage of
providing standardized rules that can be applied with minimal understanding of the domain
and study. However, the rules do not account for many real-world issues, often
overemphasize or underemphasize others, and studies show low inter-rater
reliability396.
Certain domains are more applicable for these tools, however the time-sensitive nature of
a pandemic, with significant mortality for every day of delay in evidence assessment, and
the characteristics of COVID-19 make them inappropriate for this domain.
This can be demonstrated with examples where expert RoB 2/ROBINS-I ratings do not match
reality for COVID-19. Popp et al. use RoB 2 to classify Reis et al. as low
risk of bias, however this is the opposite of reality—the trial not only has very
high risk of bias, but has very high actual known bias, refusing to release data despite
pledging to, reporting multiple impossible numbers, having blinding and randomization
failure, and many other issues398.
Axfors et al. use RoB 2 to classify Horby et al. as low risk of bias, however
this is the opposite of reality—the very late treatment and excessive dosage used
produces results with no relevance to recommended usage.
HCQ shows poor results with
late treatment and excessive dosage, and the combination shows harmAQ.
Hempenius et al. use ROBINS-I to classify 33 studies for HCQ. The two rated as having
the lowest risk of bias394,395 are far from the most informative. Both
involve very late treatment, providing no information on recommended usage, and ROBINS-I
does a very poor job of accounting for the impact of confounding factorsAR.
Our quality evaluation focuses on known issues and bias, and the potential
impact on outcomes, rather than just the risk of bias.
The estimated potential impact of each confounding factor, and the direction of the impact
is considered. For example, consider a study that shows significantly lower risk, the
value of the study varies significantly if confounding points to an underestimate or an
overestimate of efficacy. In one case, the real effect may be null, while the other case
provides stronger evidence of efficacy (which may be greater than the study shows).
Analysis focusing on the risk of bias, while simpler, may penalize studies for theoretical
or technical issues that have no or minimal impact on outcomes. Analysis also depends on
the outcome, for example certain issues are less relevant for objective outcomes such as
mortality.
Inaccurate penalization, and inaccurate high-quality evaluation in the face of known major
issues affecting outcomes, increases in significance during a pandemic when immediate
recognition of new evidence is critical, and when considering all global studies, as
required during a pandemic. Investigators in other countries may have different customs
for design, analysis, and reporting, and different English language skills, however they
may not be less diligent or have greater bias.
Investigators in lower-pharmaceutical-profit countries may have lower bias towards
profitable interventions.
We have classified studies as
early treatment if most patients are not already at a severe stage at the time of
treatment (for example based on oxygen status or lung involvement), and treatment started
within 5 days of the onset of symptoms. If studies contain a mix of early treatment and
late treatment patients, we consider the treatment time of patients contributing most to
the events (for example, consider a study where most patients are treated early but late
treatment patients are included, and all mortality events were observed with late
treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only considered
effective when used within a shorter timeframe, for example 0-36 or 0-48 hours for
oseltamivir, with longer delays not being effective138,139.
This is a living analysis and is updated regularly.
We received no funding, this research is done in our spare time.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/qmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Di Pierro, 1/13/2023, Randomized Controlled Trial, Pakistan, peer-reviewed, mean age 47.6, 13 authors, study period December 2020 - September 2021, trial NCT04861298 (history), excluded in exclusion analyses: randomization resulted in significant baseline differences that were not adjusted for. | risk of death, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 50 (0.0%), control 1 of 50 (2.0%), NNT 50, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of ICU admission, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 50 (0.0%), control 1 of 50 (2.0%), NNT 50, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| risk of hospitalization, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 50 (0.0%), control 1 of 50 (2.0%), NNT 50, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| risk of no recovery, 36.8% lower, RR 0.63, p = 0.007, treatment 24 of 50 (48.0%), control 38 of 50 (76.0%), NNT 3.6, day 7. | |
| risk of no viral clearance, 57.9% lower, RR 0.42, p < 0.001, treatment 16 of 50 (32.0%), control 38 of 50 (76.0%), NNT 2.3, mid-recovery, day 7. | |
| risk of no viral clearance, 50.0% higher, RR 1.50, p = 1.00, treatment 3 of 50 (6.0%), control 2 of 50 (4.0%), day 14. | |
| risk of no viral clearance, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 50 (0.0%), control 1 of 50 (2.0%), NNT 50, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 21. | |
| Di Pierro (B), 6/8/2021, Randomized Controlled Trial, Pakistan, peer-reviewed, 19 authors, study period September 2020 - March 2021, trial NCT04578158 (history), excluded in exclusion analyses: multiple data issues - pending author response. | risk of death, 85.7% lower, RR 0.14, p = 0.25, treatment 0 of 76 (0.0%), control 3 of 76 (3.9%), NNT 25, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of ICU admission, 94.1% lower, RR 0.06, p = 0.006, treatment 0 of 76 (0.0%), control 8 of 76 (10.5%), NNT 9.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| risk of hospitalization, 68.2% lower, RR 0.32, p = 0.003, treatment 7 of 76 (9.2%), control 22 of 76 (28.9%), NNT 5.1. | |
| Din Ujjan, 1/18/2023, Randomized Controlled Trial, Pakistan, peer-reviewed, 6 authors, study period 21 September, 2021 - 21 January, 2022, this trial uses multiple treatments in the treatment arm (combined with curcumin and vitamin D) - results of individual treatments may vary, trial NCT04603690 (history), excluded in exclusion analyses: combined treatments may contribute significantly to the effect seen; unadjusted differences between groups. | risk of no recovery, 28.6% lower, RR 0.71, p = 0.11, treatment 15 of 25 (60.0%), control 21 of 25 (84.0%), NNT 4.2, no symptoms, day 7. |
| risk of no recovery, 71.4% lower, RR 0.29, p < 0.001, treatment 6 of 25 (24.0%), control 21 of 25 (84.0%), NNT 1.7, ≤1 symptom, day 7. | |
| risk of no recovery, 76.9% lower, RR 0.23, p = 0.005, treatment 3 of 25 (12.0%), control 13 of 25 (52.0%), NNT 2.5, ≤2 symptoms, day 7. | |
| risk of no recovery, 85.7% lower, RR 0.14, p = 0.23, treatment 0 of 25 (0.0%), control 3 of 25 (12.0%), NNT 8.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), ≤3 symptoms, day 7. | |
| risk of no viral clearance, 90.9% lower, RR 0.09, p = 0.05, treatment 0 of 25 (0.0%), control 5 of 25 (20.0%), NNT 5.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 14. | |
| risk of no viral clearance, 73.7% lower, RR 0.26, p < 0.001, treatment 5 of 25 (20.0%), control 19 of 25 (76.0%), NNT 1.8, day 7. | |
| Khan, 5/1/2022, Randomized Controlled Trial, Pakistan, peer-reviewed, 7 authors, study period 2 September, 2021 - 28 November, 2021, this trial uses multiple treatments in the treatment arm (combined with curcumin and vitamin D) - results of individual treatments may vary, trial NCT05130671 (history). | risk of no recovery, 33.3% lower, RR 0.67, p = 0.15, treatment 10 of 25 (40.0%), control 15 of 25 (60.0%), NNT 5.0. |
| relative CRP reduction, 39.1% better, RR 0.61, p = 0.006, treatment 25, control 25. | |
| risk of no viral clearance, 50.0% lower, RR 0.50, p = 0.009, treatment 10 of 25 (40.0%), control 20 of 25 (80.0%), NNT 2.5. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Gérain, 6/22/2023, Randomized Controlled Trial, Belgium, peer-reviewed, 8 authors, study period 1 April, 2021 - 29 October, 2021, this trial uses multiple treatments in the treatment arm (combined with curcumin) - results of individual treatments may vary, trial NCT04844658 (history). | risk of death, 67.1% lower, RR 0.33, p = 0.49, treatment 0 of 25 (0.0%), control 1 of 24 (4.2%), NNT 24, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 7. |
| risk of death/ICU, 91.1% lower, RR 0.09, p = 0.02, treatment 0 of 25 (0.0%), control 5 of 24 (20.8%), NNT 4.8, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 7. | |
| risk of mechanical ventilation, 89.1% lower, RR 0.11, p = 0.05, treatment 0 of 25 (0.0%), control 4 of 24 (16.7%), NNT 6.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 7. | |
| risk of ICU admission, 89.1% lower, RR 0.11, p = 0.05, treatment 0 of 25 (0.0%), control 4 of 24 (16.7%), NNT 6.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 7. | |
| risk of no hospital discharge, 72.6% lower, RR 0.27, p = 0.07, treatment 2 of 25 (8.0%), control 7 of 24 (29.2%), NNT 4.7, day 14. | |
| risk of no hospital discharge, 58.9% lower, RR 0.41, p = 0.02, treatment 6 of 25 (24.0%), control 14 of 24 (58.3%), NNT 2.9, day 7. | |
| hospitalization time, 37.5% lower, relative time 0.62, p = 0.008, treatment median 5.0 IQR 4.0 n=25, control median 8.0 IQR 6.0 n=24. | |
| relative WHO score, 50.0% better, RR 0.50, p = 0.04, treatment 22, control 24, day 7. | |
| Shohan, 12/2/2021, Randomized Controlled Trial, Iran, peer-reviewed, mean age 50.9 (treatment) 52.7 (control), 8 authors, study period December 2020 - January 2021, average treatment delay 7.8 days, trial IRCT20200419047128N2. | risk of death, 85.7% lower, RR 0.14, p = 0.24, treatment 0 of 30 (0.0%), control 3 of 30 (10.0%), NNT 10.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of ICU admission, 40.0% lower, RR 0.60, p = 0.71, treatment 3 of 30 (10.0%), control 5 of 30 (16.7%), NNT 15. | |
| time to discharge from end of intervention, 32.4% lower, relative time 0.68, p = 0.04, treatment 30, control 30. | |
| Tylishchak, 12/6/2024, Randomized Controlled Trial, Ukraine, peer-reviewed, 7 authors. | risk of no recovery, 40.0% lower, RR 0.60, p = 0.71, treatment 3 of 30 (10.0%), control 5 of 30 (16.7%), NNT 15, SpO2<90. |
| hospitalization time, 14.6% lower, relative time 0.85, p < 0.001, treatment mean 13.77 (±0.75) n=30, control mean 16.13 (±0.79) n=30. | |
| Zupanets, 9/1/2021, Randomized Controlled Trial, Ukraine, peer-reviewed, 14 authors. | risk of no recovery, 29.4% lower, RR 0.71, p = 0.50, treatment 9 of 99 (9.1%), control 13 of 101 (12.9%), NNT 26. |
| recovery time, 18.2% lower, relative time 0.82, p = 0.03, treatment 99, control 101. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Rondanelli, 1/4/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Italy, peer-reviewed, 12 authors, study period 12 January, 2021 - 25 May, 2021, trial NCT05037240 (history). | risk of symptomatic case, 92.9% lower, HR 0.07, p = 0.04, treatment 1 of 60 (1.7%), control 4 of 60 (6.7%), adjusted per study, inverted to make HR<1 favor treatment, Cox proportional risk. |
Viral infection and replication involves attachment, entry, uncoating and release, genome replication and transcription, translation and protein processing, assembly and budding, and release. Each step can be disrupted by therapeutics.
The trimeric spike (S) protein is a glycoprotein that mediates viral entry by binding to the host ACE2 receptor, is critical for SARS-CoV-2's ability to infect host cells, and is a target of neutralizing antibodies. Inhibition of the spike protein prevents viral attachment, halting infection at the earliest stage.
The receptor binding domain is a specific region of the spike protein that binds ACE2 and is a major target of neutralizing antibodies. Focusing on the precise binding site allows highly specific disruption of viral attachment with reduced potential for off-target effects.
The main protease or Mpro, also known as 3CLpro or nsp5, is a cysteine protease that cleaves viral polyproteins into functional units needed for replication. Inhibiting Mpro disrupts the SARS-CoV-2 lifecycle within the host cell, preventing the creation of new copies.
RNA-dependent RNA polymerase (RdRp), also called nsp12, is the core enzyme of the viral replicase-transcriptase complex that copies the positive-sense viral RNA genome into negative-sense templates for progeny RNA synthesis. Inhibiting RdRp blocks viral genome replication and transcription.
The papain-like protease (PLpro) has multiple functions including cleaving viral polyproteins and suppressing the host immune response by deubiquitination and deISGylation of host proteins. Inhibiting PLpro may block viral replication and help restore normal immune responses.
The angiotensin converting enzyme 2 (ACE2) protein is a host cell transmembrane protein that serves as the cellular receptor for the SARS-CoV-2 spike protein. ACE2 is expressed on many cell types, including epithelial cells in the lungs, and allows the virus to enter and infect host cells. Inhibition may affect ACE2's physiological function in blood pressure control.
Transmembrane protease serine 2 (TMPRSS2) is a host cell protease that primes the spike protein, facilitating cellular entry. TMPRSS2 activity helps enable cleavage of the spike protein required for membrane fusion and virus entry. Inhibition may especially protect respiratory epithelial cells, buy may have physiological effects.
The nucleocapsid (N) protein binds and encapsulates the viral genome by coating the viral RNA. N enables formation and release of infectious virions and plays additional roles in viral replication and pathogenesis. N is also an immunodominant antigen used in diagnostic assays.
The helicase, or nsp13, protein unwinds the double-stranded viral RNA, a crucial step in replication and transcription. Inhibition may prevent viral genome replication and the creation of new virus components.
The endoribonuclease, also known as NendoU or nsp15, cleaves specific sequences in viral RNA which may help the virus evade detection by the host immune system. Inhibition may hinder the virus's ability to mask itself from the immune system, facilitating a stronger immune response.
The NSP16/10 complex consists of non-structural proteins 16 and 10, forming a 2'-O-methyltransferase that modifies the viral RNA cap structure. This modification helps the virus evade host immune detection by mimicking host mRNA, making NSP16/10 a promising antiviral target.
Cathepsin L is a host lysosomal cysteine protease that can prime the spike protein through an alternative pathway when TMPRSS2 is unavailable. Dual targeting of cathepsin L and TMPRSS2 may maximize disruption of alternative pathways for virus entry.
Wingless-related integration site (Wnt) ligand 3 is a host signaling molecule that activates the Wnt signaling pathway, which is important in development, cell growth, and tissue repair. Some studies suggest that SARS-CoV-2 infection may interfere with the Wnt signaling pathway, and that Wnt3a is involved in SARS-CoV-2 entry.
The frizzled (FZD) receptor is a host transmembrane receptor that binds Wnt ligands, initiating the Wnt signaling cascade. FZD serves as a co-receptor, along with ACE2, in some proposed mechanisms of SARS-CoV-2 infection. The virus may take advantage of this pathway as an alternative entry route.
Low-density lipoprotein receptor-related protein 6 is a cell surface co-receptor essential for Wnt signaling. LRP6 acts in tandem with FZD for signal transduction and has been discussed as a potential co-receptor for SARS-CoV-2 entry.
The ezrin protein links the cell membrane to the cytoskeleton (the cell's internal support structure) and plays a role in cell shape, movement, adhesion, and signaling. Drugs that occupy the same spot on ezrin where the viral spike protein would bind may hindering viral attachment, and drug binding could further stabilize ezrin, strengthening its potential natural capacity to impede viral fusion and entry.
The Adipocyte Differentiation-Related Protein (ADRP, also known as Perilipin 2 or PLIN2) is a lipid droplet protein regulating the storage and breakdown of fats in cells. SARS-CoV-2 may hijack the lipid handling machinery of host cells and ADRP may play a role in this process. Disrupting ADRP's interaction with the virus may hinder the virus's ability to use lipids for replication and assembly.
Neuropilin-1 (NRP1) is a cell surface receptor with roles in blood vessel development, nerve cell guidance, and immune responses. NRP1 may function as a co-receptor for SARS-CoV-2, facilitating viral entry into cells. Blocking NRP1 may disrupt an alternative route of viral entry.
EP300 (E1A Binding Protein P300) is a transcriptional coactivator involved in several cellular processes, including growth, differentiation, and apoptosis, through its acetyltransferase activity that modifies histones and non-histone proteins. EP300 facilitates viral entry into cells and upregulates inflammatory cytokine production.
Prostaglandin G/H synthase 2 (PTGS2, also known as COX-2) is an enzyme crucial for the production of inflammatory molecules called prostaglandins. PTGS2 plays a role in the inflammatory response that can become severe in COVID-19 and inhibitors (like some NSAIDs) may have benefits in dampening harmful inflammation, but note that prostaglandins have diverse physiological functions.
Heat Shock Protein 90 Alpha Family Class A Member 1 (HSP90AA1) is a chaperone protein that helps other proteins fold correctly and maintains their stability. HSP90AA1 plays roles in cell signaling, survival, and immune responses. HSP90AA1 may interact with numerous viral proteins, but note that it has diverse physiological functions.
Matrix metalloproteinase 9 (MMP9), also called gelatinase B, is a zinc-dependent enzyme that breaks down collagen and other components of the extracellular matrix. MMP9 levels increase in severe COVID-19. Overactive MMP9 can damage lung tissue and worsen inflammation. Inhibition of MMP9 may prevent excessive tissue damage and help regulate the inflammatory response.
The interleukin-6 (IL-6) pro-inflammatory cytokine (signaling molecule) has a complex role in the immune response and may trigger and perpetuate inflammation. Elevated IL-6 levels are associated with severe COVID-19 cases and cytokine storm. Anti-IL-6 therapies may be beneficial in reducing excessive inflammation in severe COVID-19 cases.
The interleukin-10 (IL-10) anti-inflammatory cytokine helps regulate and dampen immune responses, preventing excessive inflammation. IL-10 levels can also be elevated in severe COVID-19. IL-10 could either help control harmful inflammation or potentially contribute to immune suppression.
Vascular Endothelial Growth Factor A (VEGFA) promotes the growth of new blood vessels (angiogenesis) and has roles in inflammation and immune responses. VEGFA may contribute to blood vessel leakiness and excessive inflammation associated with severe COVID-19.
RELA is a transcription factor subunit of NF-kB and is a key regulator of inflammation, driving pro-inflammatory gene expression. SARS-CoV-2 may hijack and modulate NF-kB pathways.
The interaction between the SARS-CoV-2 spike protein and the human ACE2 receptor is a primary method of viral entry, inhibiting this interaction can prevent the virus from attaching to and entering host cells, halting infection at an early stage.
Calu-3 is a human lung adenocarcinoma cell line with moderate ACE2 and TMPRSS2 expression and SARS-CoV-2 susceptibility. It provides a model of the human respiratory epithelium, but many not be ideal for modeling early stages of infection due to the moderate expression levels of ACE2 and TMPRSS2.
A549 is a human lung carcinoma cell line with low ACE2 expression and SARS-CoV-2 susceptibility. Viral entry/replication can be studied but the cells may not replicate all aspects of lung infection.
HEK293-ACE2+ is a human embryonic kidney cell line engineered for high ACE2 expression and SARS-CoV-2 susceptibility.
Huh-7 cells were derived from a liver tumor (hepatoma).
Caco-2 cells come from a colorectal adenocarcinoma (cancer). They are valued for their ability to form a polarized cell layer with properties similar to the intestinal lining.
Vero E6 is an African green monkey kidney cell line with low/no ACE2 expression and high SARS-CoV-2 susceptibility. The cell line is easy to maintain and supports robust viral replication, however the monkey origin may not accurately represent human responses.
mTEC is a mouse tubular epithelial cell line.
RAW264.7 is a mouse macrophage cell line.
HLMEC (Human Lung Microvascular Endothelial Cells) are primary endothelial cells derived from the lung microvasculature. They are used to study endothelial function, inflammation, and viral interactions, particularly in the context of lung infections such as SARS-CoV-2. HLMEC express ACE2 and are susceptible to SARS-CoV-2 infection, making them a relevant model for studying viral entry and endothelial responses in the lung.
A mouse model expressing the human ACE2 receptor under the control of the K18 promoter.
A mouse model of obesity and severe insulin resistance leading to type 2 diabetes due to a mutation in the leptin receptor gene that impairs satiety signaling.
A mouse model commonly used in infectious disease and cancer research due to higher immune response and susceptibility to infection.
Monoclonal antibodies were
previously included. Other treatments such as dexamethasone, tocilizumab, and baricitinib
were recommended for late stage hospitalized patients.
Smoking was
known to cause lung cancer since at least 1939, but this was not widely recognized in the
US until 1964, 25 years later. Surgeon general Leroy Burney tried publicizing the danger
starting in 1957, with limited success. Surgeon general Luther Terry, appointed in 1961,
prompted by President Kennedy in 1962 amid pressure from health advocates, finally got
recognition in 1964. The 1964 report reviewed 7,000+ studies, but these could (and should)
have been reviewed and acted upon in real-time as they were published.
Historians attribute the 25 year delay to an industry campaign to manufacture doubt and
controversy, through tactics like funding biased and fraudulent research from
"independent" organizations, attacking scientists, and political lobbying.
The success of the industry campaign is only possible because officials did not analyze
the research in detail. Fraudulent industry research supported prior failures, but would
have been called out as fraudulent by officials that analyzed and understood the research
in real-time.
When administered late in infection, HCQ may enhance viral egress by further increasing
lysosomal pH beyond the effect of ORF3a's water channel activity, thereby promoting
lysosomal exocytosis, inactivating degradative enzymes, and facilitating the release of
SARS-CoV-2 particles into the extracellular environment390,391.
Research also suggests potential cardioprotective effects at lower doses, but
cardiotoxicity with excessive dosage392. Bobrowski et al. also
indicate negative effects if HCQ and remdesivir are combined.
Peters (B) et al. is subject to confounding by calendar-time (SOC evolved rapidly early in
the pandemic, the linear covariate does not reflect non-linear SOC changes and hospital
specific effects), hospital type (non-treatment hospitals were tertiary university
centers), confounding by indication (4/7 hospitals initiated treatment on deterioration),
immortal-time bias for as-treated (exposure assigned after baseline), significant
differences for other experimental treatments, potential overadjustment from collider bias
(steroid use and indication bias), limited baseline severity information, differences in
hospice referral propensity across hospitals, unadjusted difference in time from onset to
admission, difference in PCR positivity, and other factors.
Mahévas et al. is subject to confounding by hospital (treatment highly dependent on
the hospital, different SOC/ICU transfer practices, not included in PS), immortal time
(only partly addressed in sensitivity analysis), co-treatment differences, calendar-time
(SOC evolved rapidly early in the pandemic), binary coding for age (age ≥65 despite steep
age-risk gradient), residual imbalance (variables dropped from PS), a composite outcome
dependent on hospital triage/capacity, and other factors.
Crawford et al., Analysis of Select Dietary Supplement Products Marketed to Support or Boost the Immune System, JAMA Network Open, doi:10.1001/jamanetworkopen.2022.26040.
Crighton et al., Toxicological screening and DNA sequencing detects contamination and adulteration in regulated herbal medicines and supplements for diet, weight loss and cardiovascular health, Journal of Pharmaceutical and Biomedical Analysis, doi:10.1016/j.jpba.2019.112834.
Chanyandura et al., Evaluation of The Pharmaceutical Quality of the Most Commonly Purchased Vitamin C (Ascorbic Acid) Formulations in COVID-19 Infection in South Africa, J. Basic Appl. Pharm. Sci., doi:10.33790/jbaps1100105.
García Alvarez et al., The Quercetin Paradox, Evaluation of its Therapeutic Efficacy as a Nutraceutical in Clinical Trials: Evidence and Speculation, Dose-Response, doi:10.1177/15593258261419728.
Ziaei et al., The effect of quercetin supplementation on clinical outcomes in COVID‐19 patients: A systematic review and meta‐analysis, Food Science & Nutrition, doi:10.1002/fsn3.3715.
Cheema et al., Quercetin for the treatment of COVID-19 patients: A systematic review and meta-analysis, Reviews in Medical Virology, doi:10.1002/rmv.2427.
Ryu et al., Fibrin drives thromboinflammation and neuropathology in COVID-19, Nature, doi:10.1038/s41586-024-07873-4.
Rong et al., Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19, Cell Host & Microbe, doi:10.1016/j.chom.2024.11.007.
Yang et al., SARS-CoV-2 infection causes dopaminergic neuron senescence, Cell Stem Cell, doi:10.1016/j.stem.2023.12.012.
Scardua-Silva et al., Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19, Scientific Reports, doi:10.1038/s41598-024-52005-7.
Hampshire et al., Cognition and Memory after Covid-19 in a Large Community Sample, New England Journal of Medicine, doi:10.1056/NEJMoa2311330.
Duloquin et al., Is COVID-19 Infection a Multiorganic Disease? Focus on Extrapulmonary Involvement of SARS-CoV-2, Journal of Clinical Medicine, doi:10.3390/jcm13051397.
Sodagar et al., Pathological Features and Neuroinflammatory Mechanisms of SARS-CoV-2 in the Brain and Potential Therapeutic Approaches, Biomolecules, doi:10.3390/biom12070971.
Sagar et al., COVID-19-associated cerebral microbleeds in the general population, Brain Communications, doi:10.1093/braincomms/fcae127.
Verma et al., Persistent Neurological Deficits in Mouse PASC Reveal Antiviral Drug Limitations, bioRxiv, doi:10.1101/2024.06.02.596989.
Panagea et al., Neurocognitive Impairment in Long COVID: A Systematic Review, Archives of Clinical Neuropsychology, doi:10.1093/arclin/acae042.
Ariza et al., COVID-19: Unveiling the Neuropsychiatric Maze—From Acute to Long-Term Manifestations, Biomedicines, doi:10.3390/biomedicines12061147.
Vashisht et al., Neurological Complications of COVID-19: Unraveling the Pathophysiological Underpinnings and Therapeutic Implications, Viruses, doi:10.3390/v16081183.
Ahmad et al., Neurological Complications and Outcomes in Critically Ill Patients With COVID-19: Results From International Neurological Study Group From the COVID-19 Critical Care Consortium, The Neurohospitalist, doi:10.1177/19418744241292487.
Wang et al., SARS-CoV-2 membrane protein induces neurodegeneration via affecting Golgi-mitochondria interaction, Translational Neurodegeneration, doi:10.1186/s40035-024-00458-1.
Freitas et al., Central nervous system and systemic inflammatory networks associated with acute neurological outcomes in COVID-19, Scientific Reports, doi:10.1038/s41598-025-08632-9.
Lu et al., Risk of neuropsychiatric and related conditions associated with SARS-CoV-2 infection: a difference-in-differences analysis, Nature Communications, doi:10.1038/s41467-025-61961-1.
Jachman-Kapułka et al., Cross-Section of Neurological Manifestations Among SARS-CoV-2 Omicron Subvariants—Single-Center Study, Brain Sciences, doi:10.3390/brainsci14111161.
Beckman et al., SARS-CoV-2 infects neurons and induces neuroinflammation in a non-human primate model of COVID-19, Cell Reports, doi:10.1016/j.celrep.2022.111573.
Eberhardt et al., SARS-CoV-2 infection triggers pro-atherogenic inflammatory responses in human coronary vessels, Nature Cardiovascular Research, doi:10.1038/s44161-023-00336-5.
Van Tin et al., Spike Protein of SARS-CoV-2 Activates Cardiac Fibrogenesis through NLRP3 Inflammasomes and NF-κB Signaling, Cells, doi:10.3390/cells13161331.
Borka Balas et al., COVID-19 and Cardiac Implications—Still a Mystery in Clinical Practice, Reviews in Cardiovascular Medicine, doi:10.31083/j.rcm2405125.
AlTaweel et al., An In-Depth Insight into Clinical, Cellular and Molecular Factors in COVID19-Associated Cardiovascular Ailments for Identifying Novel Disease Biomarkers, Drug Targets and Clinical Management Strategies, Archives of Microbiology & Immunology, doi:10.26502/ami.936500177.
Saha et al., COVID-19 beyond the lungs: Unraveling its vascular impact and cardiovascular complications—mechanisms and therapeutic implications, Science Progress, doi:10.1177/00368504251322069.
Yin et al., COVID-19: a vascular nightmare unfolding, Frontiers in Immunology, doi:10.3389/fimmu.2025.1593885.
Bruno et al., Accelerated vascular ageing after COVID-19 infection: the CARTESIAN study, European Heart Journal, doi:10.1093/eurheartj/ehaf430.
Abiri et al., The silent legacy of COVID-19: exploring genomic instability in long-term COVID-19 survivors, BMC Infectious Diseases, doi:10.1186/s12879-025-11419-y.
Gioia et al., SARS-CoV-2 infection induces DNA damage, through CHK1 degradation and impaired 53BP1 recruitment, and cellular senescence, Nature Cell Biology, doi:10.1038/s41556-023-01096-x.
Doğan et al., Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients, Current Issues in Molecular Biology, doi:10.3390/cimb45020062.
Rueda-Torres et al., Longitudinal Assessment of DNA Damage in PBMCs From Hospitalized COVID‐19 Patients via Alkaline Comet Assay, Environmental and Molecular Mutagenesis, doi:10.1002/em.70055.
Trender et al., Changes in memory and cognition during the SARS-CoV-2 human challenge study, eClinicalMedicine, doi:10.1016/j.eclinm.2024.102842.
Dugied et al., Multimodal SARS-CoV-2 interactome sketches the virus-host spatial organization, Communications Biology, doi:10.1038/s42003-025-07933-z.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Katiyar et al., SARS-CoV-2 Assembly: Gaining Infectivity and Beyond, Viruses, doi:10.3390/v16111648.
Wu et al., Decoding the genome of SARS-CoV-2: a pathway to drug development through translation inhibition, RNA Biology, doi:10.1080/15476286.2024.2433830.
Alavi et al., Interaction of Epigallocatechin Gallate and Quercetin with Spike Glycoprotein (S-Glycoprotein) of SARS-CoV-2: In Silico Study, Biomedicines, doi:10.3390/biomedicines10123074.
Azmi et al., The role of vitamin D receptor and IL‐6 in COVID‐19, Molecular Genetics & Genomic Medicine, doi:10.1002/mgg3.2172.
Chandran et al., Molecular docking analysis of quercetin with known CoVid-19 targets, Bioinformation, doi:10.6026/973206300191081.
Kandeil et al., Bioactive Polyphenolic Compounds Showing Strong Antiviral Activities against Severe Acute Respiratory Syndrome Coronavirus 2, Pathogens, doi:10.3390/pathogens10060758.
Mandal et al., In silico anti-viral assessment of phytoconstituents in a traditional (Siddha Medicine) polyherbal formulation – Targeting Mpro and pan-coronavirus post-fusion Spike protein, Journal of Traditional and Complementary Medicine, doi:10.1016/j.jtcme.2023.07.004.
Moschovou et al., Exploring the Binding Effects of Natural Products and Antihypertensive Drugs on SARS-CoV-2: An In Silico Investigation of Main Protease and Spike Protein, International Journal of Molecular Sciences, doi:10.3390/ijms242115894.
Nguyen et al., The Potential of Ameliorating COVID-19 and Sequelae From Andrographis paniculata via Bioinformatics, Bioinformatics and Biology Insights, doi:10.1177/11779322221149622.
Pan et al., Quercetin: A promising drug candidate against the potential SARS-CoV-2-Spike mutants with high viral infectivity, Computational and Structural Biotechnology Journal, doi:10.1016/j.csbj.2023.10.029.
Thapa et al., In-silico Approach for Predicting the Inhibitory Effect of Home Remedies on Severe Acute Respiratory Syndrome Coronavirus-2, Makara Journal of Science, doi:10.7454/mss.v27i3.1609.
Raman et al., Phytoconstituents of Citrus limon (Lemon) as Potential Inhibitors Against Multi Targets of SARS‐CoV‐2 by Use of Molecular Modelling and In Vitro Determination Approaches, ChemistryOpen, doi:10.1002/open.202300198.
Şimşek et al., In silico identification of SARS-CoV-2 cell entry inhibitors from selected natural antivirals, Journal of Molecular Graphics and Modelling, doi:10.1016/j.jmgm.2021.108038.
Asad et al., Exploring the antiviral activity of Adhatoda beddomei bioactive compounds in interaction with coronavirus spike protein, Archives of Medical Reports, 1:1, archmedrep.com/index.php/amr/article/view/3.
Haque et al., Exploring potential therapeutic candidates against COVID-19: a molecular docking study, Discover Molecules, doi:10.1007/s44345-024-00005-5.
Al balawi et al., Assessing multi-target antiviral and antioxidant activities of natural compounds against SARS-CoV-2: an integrated in vitro and in silico study, Bioresources and Bioprocessing, doi:10.1186/s40643-024-00822-z.
Rajamanickam et al., Exploring the Potential of Siddha Formulation MilagaiKudineer-Derived Phytotherapeutics Against SARS-CoV-2: An In-Silico Investigation for Antiviral Intervention, Journal of Pharmacy and Pharmacology Research, doi:10.26502/fjppr.0105.
Akinwumi et al., Evaluation of therapeutic potentials of some bioactive compounds in selected African plants targeting main protease (Mpro) in SARS-CoV-2: a molecular docking study, Egyptian Journal of Medical Human Genetics, doi:10.1186/s43042-023-00456-4.
Alanzi et al., Structure-based virtual identification of natural inhibitors of SARS-CoV-2 and its Delta and Omicron variant proteins, Future Virology, doi:10.2217/fvl-2022-0184.
Ibeh et al., Computational studies of potential antiviral compounds from some selected Nigerian medicinal plants against SARS-CoV-2 proteins, Informatics in Medicine Unlocked, doi:10.1016/j.imu.2023.101230.
Qin et al., Exploring the bioactive compounds of Feiduqing formula for the prevention and management of COVID-19 through network pharmacology and molecular docking, Medical Data Mining, doi:10.53388/MDM202407003.
Rehman et al., Natural Compounds as Inhibitors of SARS-CoV-2 Main Protease (3CLpro): A Molecular Docking and Simulation Approach to Combat COVID-19, Current Pharmaceutical Design, doi:10.2174/1381612826999201116195851.
Sekiou et al., In-Silico Identification of Potent Inhibitors of COVID-19 Main Protease (Mpro) and Angiotensin Converting Enzyme 2 (ACE2) from Natural Products: Quercetin, Hispidulin, and Cirsimaritin Exhibited Better Potential Inhibition than Hydroxy-Chloroquine Against COVID-19 Main Protease Active Site and ACE2, ChemRxiv, doi:10.26434/chemrxiv.12181404.v1.
Singh et al., Unlocking the potential of phytochemicals in inhibiting SARS-CoV-2 M Pro protein - An in-silico and cell-based approach, Research Square, doi:10.21203/rs.3.rs-3888947/v1.
Wang (B) et al., Computational Analysis of Lianhua Qingwen as an Adjuvant Treatment in Patients with COVID-19, Society of Toxicology Conference, 2023, www.researchgate.net/publication/370491709_Y_Wang_A_E_Tan_O_Chew_A_Hsueh_and_D_E_Johnson_2023_Computational_Analysis_of_Lianhua_Qingwen_as_an_Adjuvant_Treatment_in_Patients_with_COVID-19_Toxicologist_1921_507.
Zhang et al., In silico screening of Chinese herbal medicines with the potential to directly inhibit 2019 novel coronavirus, Journal of Integrative Medicine, doi:10.1016/j.joim.2020.02.005.
Shaik et al., Computational identification of selected bioactive compounds from Cedrus deodara as inhibitors against SARS-CoV-2 main protease: a pharmacoinformatics study, Indian Drugs, doi:10.53879/id.61.02.13859.
Waqas et al., Discovery of Novel Natural Inhibitors Against SARS-CoV-2 Main Protease: A Rational Approach to Antiviral Therapeutics, Current Medicinal Chemistry, doi:10.2174/0109298673292839240329081008.
Nalban et al., Targeting COVID-19 (SARS-CoV-2) main protease through phytochemicals of Albizia lebbeck: molecular docking, molecular dynamics simulation, MM–PBSA free energy calculations, and DFT analysis, Journal of Proteins and Proteomics, doi:10.1007/s42485-024-00136-w.
Irfan et al., Phytoconstituents of Artemisia Annua as potential inhibitors of SARS CoV2 main protease: an in silico study, BMC Infectious Diseases, doi:10.1186/s12879-024-09387-w.
Sunita et al., Characterization of Phytochemical Inhibitors of the COVID-19 Primary Protease Using Molecular Modelling Approach, Asian Journal of Microbiology and Biotechnology, doi:10.56557/ajmab/2024/v9i28800.
Bano et al., Biochemical Screening of Phytochemicals and Identification of Scopoletin as a Potential Inhibitor of SARS-CoV-2 Mpro, Revealing Its Biophysical Impact on Structural Stability, Viruses, doi:10.3390/v17030402.
Abian et al., Structural stability of SARS-CoV-2 3CLpro and identification of quercetin as an inhibitor by experimental screening, International Journal of Biological Macromolecules, doi:10.1016/j.ijbiomac.2020.07.235.
Corbo et al., Inhibitory potential of phytochemicals on five SARS-CoV-2 proteins: in silico evaluation of endemic plants of Bosnia and Herzegovina, Biotechnology & Biotechnological Equipment, doi:10.1080/13102818.2023.2222196.
Metwaly et al., Integrated study of Quercetin as a potent SARS-CoV-2 RdRp inhibitor: Binding interactions, MD simulations, and In vitro assays, PLOS ONE, doi:10.1371/journal.pone.0312866.
Alkafaas et al., A study on the effect of natural products against the transmission of B.1.1.529 Omicron, Virology Journal, doi:10.1186/s12985-023-02160-6.
Wang (C) et al., Investigating the Mechanism of Qu Du Qiang Fei 1 Hao Fang Formula against Coronavirus Disease 2019 Based on Network Pharmacology Method, World Journal of Traditional Chinese Medicine, doi:10.4103/2311-8571.395061.
Singh (B) et al., Flavonoids as Potent Inhibitor of SARS-CoV-2 Nsp13 Helicase: Grid Based Docking Approach, Middle East Research Journal of Pharmaceutical Sciences, doi:10.36348/merjps.2023.v03i04.001.
Tamil Selvan et al., Computational Investigations to Identify Potent Natural Flavonoid Inhibitors of the Nonstructural Protein (NSP) 16/10 Complex Against Coronavirus, Cureus, doi:10.7759/cureus.68098.
Ahmed et al., Evaluation of the Effect of Zinc, Quercetin, Bromelain and Vitamin C on COVID-19 Patients, International Journal of Diabetes Management, doi:10.61797/ijdm.v2i2.259.
Chellasamy et al., Docking and molecular dynamics studies of human ezrin protein with a modelled SARS-CoV-2 endodomain and their interaction with potential invasion inhibitors, Journal of King Saud University - Science, doi:10.1016/j.jksus.2022.102277.
Hasanah et al., Decoding the therapeutic potential of empon-empon: a bioinformatics expedition unraveling mechanisms against COVID-19 and atherosclerosis, International Journal of Applied Pharmaceutics, doi:10.22159/ijap.2024v16i2.50128.
Sai Ramesh et al., Computational analysis of the phytocompounds of Mimusops elengi against spike protein of SARS CoV2 – An Insilico model, International Journal of Biological Macromolecules, doi:10.1016/j.ijbiomac.2023.125553.
Yang (B) et al., Active ingredient and mechanistic analysis of traditional Chinese medicine formulas for the prevention and treatment of COVID-19: Insights from bioinformatics and in vitro experiments, Medicine, doi:10.1097/MD.0000000000036238.
Yang (C) et al., In silico evidence implicating novel mechanisms of Prunella vulgaris L. as a potential botanical drug against COVID-19-associated acute kidney injury, Frontiers in Pharmacology, doi:10.3389/fphar.2023.1188086.
Moharram et al., Secondary metabolites of Alternaria alternate appraisal of their SARS-CoV-2 inhibitory and anti-inflammatory potentials, PLOS ONE, doi:10.1371/journal.pone.0313616.
Bahun et al., Inhibition of the SARS-CoV-2 3CLpro main protease by plant polyphenols, Food Chemistry, doi:10.1016/j.foodchem.2021.131594.
Zhang (B) et al., Discovery of the covalent SARS‐CoV‐2 Mpro inhibitors from antiviral herbs via integrating target‐based high‐throughput screening and chemoproteomic approaches, Journal of Medical Virology, doi:10.1002/jmv.29208.
Aguilera-Rodriguez et al., Inhibition of SARS-CoV-2 3CLpro by chemically modified tyrosinase from Agaricus bisporus, RSC Medicinal Chemistry, doi:10.1039/D4MD00289J.
Emam et al., Establishment of in-house assay for screening of anti-SARS-CoV-2 protein inhibitors, AMB Express, doi:10.1186/s13568-024-01739-8.
DiGuilio et al., Quercetin improves and protects Calu-3 airway epithelial barrier function, Frontiers in Cell and Developmental Biology, doi:10.3389/fcell.2023.1271201.
Singh (C) et al., The spike protein of SARS-CoV-2 virus induces heme oxygenase-1: Pathophysiologic implications, Biochimica et Biophysica Acta (BBA) - Molecular Basis of Disease, doi:10.1016/j.bbadis.2021.166322.
Roy et al., Quercetin inhibits SARS-CoV-2 infection and prevents syncytium formation by cells co-expressing the viral spike protein and human ACE2, Virology Journal, doi:10.1186/s12985-024-02299-w.
El-Megharbel et al., Chemical and spectroscopic characterization of (Artemisinin/Quercetin/ Zinc) novel mixed ligand complex with assessment of its potent high antiviral activity against SARS-CoV-2 and antioxidant capacity against toxicity induced by acrylamide in male rats, PeerJ, doi:10.7717/peerj.15638.
Wu (B) et al., SARS-CoV-2 N protein induced acute kidney injury in diabetic db/db mice is associated with a Mincle-dependent M1 macrophage activation, Frontiers in Immunology, doi:10.3389/fimmu.2023.1264447.
Aguado et al., Senolytic therapy alleviates physiological human brain aging and COVID-19 neuropathology, bioRxiv, doi:10.1101/2023.01.17.524329.
Wu (C) et al., Treatment with Quercetin inhibits SARS-CoV-2 N protein-induced acute kidney injury by blocking Smad3-dependent G1 cell cycle arrest, Molecular Therapy, doi:10.1016/j.ymthe.2022.12.002.
Shaker et al., Anti-cytokine Storm Activity of Fraxin, Quercetin, and their Combination on Lipopolysaccharide-Induced Cytokine Storm in Mice: Implications in COVID-19, Iranian Journal of Medical Sciences, doi:10.30476/ijms.2023.98947.3102.
Xu et al., Quercetin inhibited LPS-induced cytokine storm by interacting with the AKT1-FoxO1 and Keap1-Nrf2 signaling pathway in macrophages, Scientific Reports, doi:10.1038/s41598-024-71569-y.
Manikyam et al., INP-Guided Network Pharmacology Discloses Multi-Target Therapeutic Strategy Against Cytokine and IgE Storms in the SARS-CoV-2 NB.1.8.1 Variant, Research Square, doi:10.21203/rs.3.rs-6819274/v1.
Shokri-Afra et al., Targeting SIRT1: A Potential Strategy for Combating Severe COVID‐19, BioMed Research International, doi:10.1155/bmri/9507417.
Fam et al., Channel activity of SARS-CoV-2 viroporin ORF3a inhibited by adamantanes and phenolic plant metabolites, Scientific Reports, doi:10.1038/s41598-023-31764-9.
Gupta et al., Harnessing phytoconstituents to treat COVID-19 triggered acute respiratory distress syndrome: Insights from network pharmacology, and molecular modeling, Phytochemistry Letters, doi:10.1016/j.phytol.2025.104105.
Fadel et al., Targeting asparagine and cysteine in SARS-CoV-2 variants and human pro-inflammatory mediators to alleviate COVID-19 severity; a cross-section and in-silico study, Scientific Reports, doi:10.1038/s41598-025-19359-y.
Xie et al., Identification of key genes modules linking brain aging signatures and COVID-19-associated cognitive impairment, Virus Research, doi:10.1016/j.virusres.2026.199707.
web.archive.org, web.archive.org/web/20211117052139/https://astralcodexten.substack.com/p/ivermectin-much-more-than-you-wanted.
Hayward et al., Ivermectin for COVID-19 in adults in the community (PRINCIPLE): an open, randomised, controlled, adaptive platform trial of short- and longer-term outcomes, Journal of Infection, doi:10.1016/j.jinf.2024.106130.
Tata et al., Allosteric Interactions of Flavonoids with ACE2 and Potential Implications for COVID-19: Computational Insights, Metabolic and Mitochondrial Effects of Rutin in A549 Cells, Cell Biochemistry and Biophysics, doi:10.1007/s12013-026-02093-1.
Sun et al., Feasibility of the inhibitor development for SARS-CoV-2: a systematic approach for drug design, Journal of Molecular Modeling, doi:10.1007/s00894-025-06541-2.
Torabfam et al., Improving quercetin solubility via structural modification enhances dual-target coronavirus entry: an integrated in-vitro and in-silico study, Scientific Reports, doi:10.1038/s41598-025-27374-2.
Abdelhameed et al., Phytochemical and antiviral investigation of Cynanchum acutum L. extract and derived semi-synthetic analogs targeting SARS-CoV-2 main protease, Future Journal of Pharmaceutical Sciences, doi:10.1186/s43094-025-00907-2.
Makoana et al., Integration of metabolomics and chemometrics with in-silico and in-vitro approaches to unravel SARS-Cov-2 inhibitors from South African plants, PLOS ONE, doi:10.1371/journal.pone.0320415.
Pan (B) et al., Decoding the mechanism of Qingjie formula in the prevention of COVID-19 based on network pharmacology and molecular docking, Heliyon, doi:10.1016/j.heliyon.2024.e39167.
Wu (D) et al., Biomarkers Prediction and Immune Landscape in Covid-19 and “Brain Fog”, Elsevier BV, doi:10.2139/ssrn.4897774.
Yuan et al., Network pharmacology and molecular docking reveal the mechanisms of action of Panax notoginseng against post-COVID-19 thromboembolism, Review of Clinical Pharmacology and Pharmacokinetics - International Edition, doi:10.61873/DTFA3974.
Zhou et al., Bioinformatics and system biology approaches to determine the connection of SARS-CoV-2 infection and intrahepatic cholangiocarcinoma, PLOS ONE, doi:10.1371/journal.pone.0300441.
Azmi (B) et al., Utilization of quercetin flavonoid compounds in onion (Allium cepa L.) as an inhibitor of SARS-CoV-2 spike protein against ACE2 receptors, 11th International Seminar on New Paradigm and Innovation on Natural Sciences and its Application, doi:10.1063/5.0140285.
Sisti et al., Evaluation of respiratory virus transmissibility and resilience from fomites: the case of 11 SARS-CoV-2 clinical isolates, Applied and Environmental Microbiology, doi:10.1128/aem.00774-25.
Spinelli et al., Amphibian‐Derived Peptides as Natural Inhibitors of SARS‐CoV‐2 Main Protease (Mpro): A Combined In Vitro and In Silico Approach, Chemistry & Biodiversity, doi:10.1002/cbdv.202403202.
Fang et al., Development of nanoparticles incorporated with quercetin and ACE2-membrane as a novel therapy for COVID-19, Journal of Nanobiotechnology, doi:10.1186/s12951-024-02435-2.
Xu (B) et al., Bioactive compounds from Huashi Baidu decoction possess both antiviral and anti-inflammatory effects against COVID-19, Proceedings of the National Academy of Sciences, doi:10.1073/pnas.2301775120.
Goc et al., Inhibitory effects of specific combination of natural compounds against SARS-CoV-2 and its Alpha, Beta, Gamma, Delta, Kappa, and Mu variants, European Journal of Microbiology and Immunology, doi:10.1556/1886.2021.00022.
Munafò et al., Quercetin and Luteolin Are Single-digit Micromolar Inhibitors of the SARS-CoV-2 RNA-dependent RNA Polymerase, Research Square, doi:10.21203/rs.3.rs-1149846/v1.
Vaiss et al., Curcumin and quercetin co-encapsulated in nanoemulsions for nasal administration: a promising therapeutic and prophylactic treatment for viral respiratory infections, European Journal of Pharmaceutical Sciences, doi:10.1016/j.ejps.2024.106766.
Di Pierro et al., Quercetin as a possible complementary agent for early-stage COVID-19: Concluding results of a randomized clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1096853.
Di Pierro (B) et al., Possible Therapeutic Effects of Adjuvant Quercetin Supplementation Against Early-Stage COVID-19 Infection: A Prospective, Randomized, Controlled, and Open-Label Study, International Journal of General Medicine, doi:10.2147/IJGM.S318720.
Din Ujjan et al., The possible therapeutic role of curcumin and quercetin in the early-stage of COVID-19—Results from a pragmatic randomized clinical trial, Frontiers in Nutrition, doi:10.3389/fnut.2022.1023997.
help.altmetric.com, help.altmetric.com/support/solutions/articles/6000235983-attention-sources-tracked-by-altmetric.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Ikematsu et al., Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts, New England Journal of Medicine, doi:10.1056/NEJMoa1915341.
Hayden et al., Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents, New England Journal of Medicine, doi:10.1056/NEJMoa1716197.
Kumar et al., Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(21)00469-2.
López-Medina et al., Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2021.3071.
Korves et al., SARS-CoV-2 Genetic Variants and Patient Factors Associated with Hospitalization Risk, medRxiv, doi:10.1101/2024.03.08.24303818.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
Karita et al., Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection, medRxiv, doi:10.1101/2021.08.27.21262754.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
Willett et al., The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism, medRxiv, doi:10.1101/2022.01.03.21268111.
Peacock et al., The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry, bioRxiv, doi:10.1101/2021.12.31.474653.
Williams, T., Not All Ivermectin Is Created Equal: Comparing The Quality of 11 Different Ivermectin Sources, Do Your Own Research, doyourownresearch.substack.com/p/not-all-ivermectin-is-created-equal.
Xu (C) et al., A study of impurities in the repurposed COVID-19 drug hydroxychloroquine sulfate by UHPLC-Q/TOF-MS and LC-SPE-NMR, Rapid Communications in Mass Spectrometry, doi:10.1002/rcm.9358.
Jitobaom et al., Favipiravir and Ivermectin Showed in Vitro Synergistic Antiviral Activity against SARS-CoV-2, Research Square, doi:10.21203/rs.3.rs-941811/v1.
Jitobaom (B) et al., Synergistic anti-SARS-CoV-2 activity of repurposed anti-parasitic drug combinations, BMC Pharmacology and Toxicology, doi:10.1186/s40360-022-00580-8.
Jeffreys et al., Remdesivir-ivermectin combination displays synergistic interaction with improved in vitro activity against SARS-CoV-2, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2022.106542.
Ostrov et al., Highly Specific Sigma Receptor Ligands Exhibit Anti-Viral Properties in SARS-CoV-2 Infected Cells, Pathogens, doi:10.3390/pathogens10111514.
Alsaidi et al., Griffithsin and Carrageenan Combination Results in Antiviral Synergy against SARS-CoV-1 and 2 in a Pseudoviral Model, Marine Drugs, doi:10.3390/md19080418.
Andreani et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microbial Pathogenesis, doi:10.1016/j.micpath.2020.104228.
De Forni et al., Synergistic drug combinations designed to fully suppress SARS-CoV-2 in the lung of COVID-19 patients, PLoS ONE, doi:10.1371/journal.pone.0276751.
Wan et al., Synergistic inhibition effects of andrographolide and baicalin on coronavirus mechanisms by downregulation of ACE2 protein level, Scientific Reports, doi:10.1038/s41598-024-54722-5.
Said et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1011522.
Fiaschi et al., In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants, Viruses, doi:10.3390/v16020168.
Xing et al., Published anti-SARS-CoV-2 in vitro hits share common mechanisms of action that synergize with antivirals, Briefings in Bioinformatics, doi:10.1093/bib/bbab249.
Chen et al., Synergistic Inhibition of SARS-CoV-2 Replication Using Disulfiram/Ebselen and Remdesivir, ACS Pharmacology & Translational Science, doi:10.1021/acsptsci.1c00022.
Hempel et al., Synergistic inhibition of SARS-CoV-2 cell entry by otamixaban and covalent protease inhibitors: pre-clinical assessment of pharmacological and molecular properties, Chemical Science, doi:10.1039/D1SC01494C.
Schultz et al., Pyrimidine inhibitors synergize with nucleoside analogues to block SARS-CoV-2, Nature, doi:10.1038/s41586-022-04482-x.
Ohashi et al., Potential anti-COVID-19 agents, cepharanthine and nelfinavir, and their usage for combination treatment, iScience, doi:10.1016/j.isci.2021.102367.
Al Krad et al., The protease inhibitor Nirmatrelvir synergizes with inhibitors of GRP78 to suppress SARS-CoV-2 replication, bioRxiv, doi:10.1101/2025.03.09.642200.
Abd Elsalam et al., Anti-COVID-19 activity and simple HPLC method for concurrent detection of repurposed drugs in novel binary mixtures, AMB Express, doi:10.1186/s13568-026-02030-8.
Rana et al., Ivermectin and Doxycycline combination as a promising anti-viral drug candidate: an in-silico and DFT study, In Silico Pharmacology, doi:10.1007/s40203-026-00576-w.
Setz et al., Synergistic Virus Neutralizing Activities of European Black Elderberry Fruit Extract and Iota-Carrageenan Against SARS-CoV-2, Influenza A Virus and Respiratory Syncytial Virus, Nutrients, doi:10.3390/nu18081205.
Ali et al., Preclinical Screening Platform Identifies Azatadine‐Dimaleate as a Potent Repurposed Therapeutic Against SARS‐CoV‐2 Infection, Journal of Medical Virology, doi:10.1002/jmv.70713.
Lew et al., Combination of Remdesivir and Ivermectin Exerts Highly Potent and Synergistic Antiviral Activity Against Murine Coronavirus and SARS-CoV-2 Infections, Cells, doi:10.3390/cells15131146.
Khatun et al., An All-Oral Antiviral Combination Strategy against COVID-19 Enabled by the Synergistic Mechanism of Action of Auranofin and Remdesivir, Elsevier BV, doi:10.2139/ssrn.6942990.
Thairu et al., A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2022/v34i44A36328.
Singh (D) et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Boulware, D., Comments regarding paper rejection, twitter.com/boulware_dr/status/1311331372884205570.
Rothstein, H., Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments, www.wiley.com/en-ae/Publication+Bias+in+Meta+Analysis:+Prevention,+Assessment+and+Adjustments-p-9780470870143.
Stanley et al., Meta-regression approximations to reduce publication selection bias, Research Synthesis Methods, doi:10.1002/jrsm.1095.
Rücker et al., Arcsine test for publication bias in meta-analyses with binary outcomes, Statistics in Medicine, doi:10.1002/sim.2971.
Peters, J., Comparison of Two Methods to Detect Publication Bias in Meta-analysis, JAMA, doi:10.1001/jama.295.6.676.
Moreno et al., Assessment of regression-based methods to adjust for publication bias through a comprehensive simulation study, BMC Medical Research Methodology, doi:10.1186/1471-2288-9-2.
Macaskill et al., A comparison of methods to detect publication bias in meta-analysis, Statistics in Medicine, doi:10.1002/sim.698.
Egger et al., Bias in meta-analysis detected by a simple, graphical test, BMJ, doi:10.1136/bmj.315.7109.629.
Harbord et al., A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints, Statistics in Medicine, doi:10.1002/sim.2380.
medicospelavidacovid19.com.br, medicospelavidacovid19.com.br/editoriais/folha-de-s-paulo-revela-numeros-de-david-uip-veja-a-comparacao-com-medicos-que-fazem-tratamento-precoce/.
Ricke, D., Mast cells and histamine receptor-targeted adjunctive treatments for COVID-19: A literature review, Innovative Medicines & Omics, doi:10.36922/IMO025440058.
Sanduzzi Zamparelli et al., Immune-Boosting and Antiviral Effects of Antioxidants in COVID-19 Pneumonia: A Therapeutic Perspective, Life, doi:10.3390/life15010113.
Duan et al., Bioactive compounds,quercetin, curcumin and β-glucan,regulate innate immunity via the gut-liver-brain axis, Trends in Food Science & Technology, doi:10.1016/j.tifs.2024.104864.
Beşler et al., Investigation of potential effects of quercetin on COVID-19 treatment: a systematic review of randomized controlled trials, Clinical Science of Nutrition, doi:10.62210/ClinSciNutr.2024.86.
Ho et al., Therapeutic Implications of Quercetin and its Derived-products in COVID-19 Protection and Prophylactic, Heliyon, doi:10.1016/j.heliyon.2024.e30080.
Vajdi et al., Effect of polyphenols against complications of COVID-19: current evidence and potential efficacy, Pharmacological Reports, doi:10.1007/s43440-024-00585-6.
Chen (B) et al., Effect and mechanism of quercetin or quercetin‐containing formulas against COVID‐19: From bench to bedside, Phytotherapy Research, doi:10.1002/ptr.8175.
Yong et al., Natural Products-Based Inhaled Formulations for Treating Pulmonary Diseases, International Journal of Nanomedicine, doi:10.2147/ijn.s451206.
Agrawal et al., Antiviral Significance of Isoquercetin (Quercetin-3-O-Glucoside) With Special Reference to its Anti-Coronaviral Potential, Natural Product Communications, doi:10.1177/1934578X231219560.
Matías-Pérez et al., Relationship of quercetin intake and oxidative stress in persistent Covid, Frontiers in Nutrition, doi:10.3389/fnut.2023.1278039.
Donzelli, A., Neglected Effective Early Therapies against COVID-19: Focus on Functional Foods and Related Active Substances. A Review, MDPI AG, doi:10.20944/preprints202312.1178.v1.
Dinda et al., Anti-SARS-CoV-2, antioxidant and immunomodulatory potential of dietary flavonol quercetin: Focus on molecular targets and clinical efficacy, European Journal of Medicinal Chemistry Reports, doi:10.1016/j.ejmcr.2023.100125.
Mirza et al., Quercetin as a Therapeutic Product: Evaluation of Its Pharmacological Action and Clinical Applications—A Review, Pharmaceuticals, doi:10.3390/ph16111631.
Massimo Magro et al., Use of Quercetin for Therapeutic Purposes in COVID-19 Infections: The Opinion of the Geriatrician Doctor, Journal of Modern Biology and Drug Discovery, doi:10.53964/jmbdd.2023004.
Shorobi et al., Quercetin: A Functional Food-Flavonoid Incredibly Attenuates Emerging and Re-Emerging Viral Infections through Immunomodulatory Actions, Molecules, doi:10.3390/molecules28030938.
Gasmi et al., Quercetin in the Prevention and Treatment of Coronavirus Infections: A Focus on SARS-CoV-2, Pharmaceuticals, doi:10.3390/ph15091049.
Rizky et al., The pharmacological mechanism of quercetin as adjuvant therapy of COVID-19, Life Research, doi:10.53388/life2022-0205-302.
Imran et al., The Therapeutic and Prophylactic Potential of Quercetin against COVID-19: An Outlook on the Clinical Studies, Inventive Compositions, and Patent Literature, Antioxidants, doi:10.3390/antiox11050876.
Derosa et al., A role for quercetin in coronavirus disease 2019 (COVID-19), Phytotherapy Research, doi:10.1002/ptr.6887.
Biancatelli et al., Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19), Frontiers in Immunology, doi:10.3389/fimmu.2020.01451.
Zheng et al., Effects of Lianhuaqingwen Capsules in adults with mild-to-moderate coronavirus disease 2019: an international, multicenter, double-blind, randomized controlled trial, Virology Journal, doi:10.1186/s12985-023-02144-6.
Shah et al., Jinhua Qinggan Granules for Nonhospitalized COVID-19 Patients: a Double-Blind, Placebo-Controlled, Randomized Controlled Trial, medRxiv, doi:10.1101/2022.05.16.22275074.
Khan et al., Oral Co-Supplementation of Curcumin, Quercetin, and Vitamin D3 as an Adjuvant Therapy for Mild to Moderate Symptoms of COVID-19—Results From a Pilot Open-Label, Randomized Controlled Trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.898062.
Di Pierro (C) et al., Potential Clinical Benefits of Quercetin in the Early Stage of COVID-19: Results of a Second, Pilot, Randomized, Controlled and Open-Label Clinical Trial, International Journal of General Medicine, doi:10.2147/IJGM.S318949.
Tylishchak et al., Effectiveness of the quercetin use in patients with COVID-19 with concomitant type 2 diabetes mellitus, Wiadomości Lekarskie, doi:10.36740/WLek/191875.
Gérain et al., NASAFYTOL® supplementation in adults hospitalized with COVID-19 infection: results from an exploratory open-label randomized controlled trial, Frontiers in Nutrition, doi:10.3389/fnut.2023.1137407.
Shohan et al., The therapeutic efficacy of quercetin in combination with antiviral drugs in hospitalized COVID-19 patients: A randomized controlled trial, European Journal of Pharmacology, doi:10.1016/j.ejphar.2021.1746158.
Zupanets et al., Quercetin effectiveness in patients with COVID-19 associated pneumonia, Zaporozhye Med. J., doi:10.14739/2310-1210.2021.5.231714.
Onal et al., Treatment of COVID-19 patients with quercetin: a prospective, single center, randomized, controlled trial, Turk. J. Biol., 45:518-529 (preprint 1/19/2021), journals.tubitak.gov.tr/biology/vol45/iss7/13/.
Turobkulovich et al., Applications of quercetin for the prevention of COVID-19 in healthcare workers, Emergent: Journal of Educational Discoveries and Lifelong Learning, doi:10.17605/OSF.IO/NSJ6B.
Rondanelli et al., Promising Effects of 3-Month Period of Quercetin Phytosome® Supplementation in the Prevention of Symptomatic COVID-19 Disease in Healthcare Workers: A Pilot Study, Life, doi:10.3390/life12010066.
Margolin et al., 20-Week Study of Clinical Outcomes of Over-the-Counter COVID-19 Prophylaxis and Treatment, Journal of Evidence-Based Integrative Medicine, doi:10.1177/2515690X211026193.
Arslan et al., Synergistic Effect of Quercetin and Vitamin C Against COVID-19: Is a Possible Guard for Front Liners, SSRN, doi:10.2139/ssrn.3682517.
Patacchini et al., Structure–Activity Relationships of Pyrrolyl-Containing Diketo Acid and Non-Diketo Acid Derivatives as Inhibitors of SARS-CoV-2 nsp13-Associated Activities, Molecules, doi:10.3390/molecules31132376.
Ma et al., Mechanisms of Xiangxue decoction in treating COVID-19 via HPLC‒Q-TOF‒MS/MS, network pharmacology, molecular docking and molecular dynamics simulation, Scientific Reports, doi:10.1038/s41598-026-45496-z.
Ferreira et al., From Traditional Knowledge to SARS-CoV-2 Entry Inhibitor Metabolites: Ethnopharmacological Investigation of Uncaria tomentosa (Willd. ex Schult.) DC, Plants, doi:10.3390/plants15131998.
Chiririwa, H., Selected Cannabinoids, Cannabimimetic Agents and Artemisia Combinations as Theoretical Adjunct Strategies Against COVID-19, Pharmaceuticals, doi:10.3390/ph19060869.
Nguyen (B) et al., Bioassay-Guided Phytochemical Investigation of Vietnamese Vitex rotundifolia Leaves and the Liverwort Ptychanthus striatus as Sources of SARS-CoV-2 Main Protease Inhibitors, Molecules, doi:10.3390/molecules31122009.
Akbas et al., Integrated Evaluation of Urtica dioica Extract Assessing Physiochemical Analysis with Antioxidant, Antiviral, and Immunomodulatory Effects Against SARS-CoV-2, Pharmaceuticals, doi:10.3390/ph19050693.
Chang et al., Tea Polyphenols in the COVID-19 Era: Mechanistic Insights and Translational Challenges, Current Issues in Molecular Biology, doi:10.3390/cimb48040379.
Ananto et al., Unlocking the Potential of Papuan Red Fruit (<i>Pandanus conoideus</i> Lamk): A Comprehensive Exploration of Its Role in COVID-19 Inhibition Through Molecular Docking and Molecular Dynamics Simulation, Indonesian Journal of Chemistry, doi:10.22146/ijc.99486.
Issa et al., Targeting SARS-CoV-2 Main Protease: A Bacteria-Based Colorimetric Assay for Screening Natural Antiviral Inhibitors, Viruses, doi:10.3390/v18020178.
Zhang (C) et al., Xuebijing injection in the treatment of COVID-19: An update on clinical studies, potentially active metabolites and mechanisms, Frontiers in Pharmacology, doi:10.3389/fphar.2025.1667022.
Trung et al., Eco-friendly synthesis of silver nanoparticles from Camellia Chrysantha (Hu) Tuyama with potential anti-COVID application: Exploration via computational and experimental methods, Inorganic Chemistry Communications, doi:10.1016/j.inoche.2026.116196.
Chao et al., Bioactive Compounds of Momordica charantia L. Downregulate the Protein Expression of ACE2 and TMPRSS2 In Vivo and In Vitro, International Journal of Molecular Sciences, doi:10.3390/ijms27020868.
Hernández-Rodríguez et al., Fisetin as an Antiviral Agent Targeting the RNA-Dependent RNA Polymerase of SARS-CoV-2: Computational Prediction and In Vitro Experimental Validation, Microorganisms, doi:10.3390/microorganisms13122809.
Kaya et al., Phytochemical Profiling and in Vitro Anti-Sars-Cov-2 Evaluation of Verbascum Zerdust: Integration of Ace2-Spike Inhibition Assay and Computational Approaches, Bitlis Eren University Journal of Science and Technology, doi:10.17678/beuscitech.1725713.
Shaer et al., Potential of Artemisia annua Bioactives as Antiviral Agents Against SARS-CoV-2 and Other Health Complications, Pharmaceuticals, doi:10.3390/ph18121904.
Kim et al., Therapeutic Potential of Gynostemma pentaphyllum (Thunb.) Makino Against COVID-19 Identified Through Network Pharmacology, Pharmaceuticals, doi:10.3390/ph18121851.
Fan et al., Analysis of molecular mechanism of Chinese medicine Jinhong decoction (JHD) in synergistically treating sepsis and COVID-19 based on network pharmacology, PLOS One, doi:10.1371/journal.pone.0339457.
Kianfar et al., Nanomaterials and Vitamins to Combat Future Pandemics: Lessons from COVID-19: A Review, Trends in Sciences, doi:10.48048/tis.2026.11481.
Khamto et al., Discovery of Galloyl–Flavonoid Conjugates as SARS-CoV-2 3CLpro Inhibitors: Understanding Binding Interactions Through Computational Approaches, International Journal of Molecular Sciences, doi:10.3390/ijms26199742.
Bhowmik et al., Evaluation of flavonoids as 2019-nCoV cell entry inhibitor through molecular docking and pharmacological analysis, Heliyon, doi:10.1016/j.heliyon.2021.e06515.
Chi et al., Ethnobotanical survey of herbal medicines for anti-COVID-19 used by traditional Chinese medicine pharmacies in Taiwan, Frontiers in Pharmacology, doi:10.3389/fphar.2025.1586334.
Abayomi Banjo et al., Tumor Necrosis Factor-Alpha (TNF- α) and Antiviral Activities of Artemisia SPP. Extracts on SARS-COV2, Rwanda Journal of Medicine and Health Sciences, doi:10.4314/rjmhs.v8i2.2.
Bolinger et al., Lessons learnt from broad-spectrum coronavirus antiviral drug discovery, Expert Opinion on Drug Discovery, doi:10.1080/17460441.2024.2385598.
Guo et al., Network Pharmacology and Experiment Verification-Based Strategy for Exploring the Mechanisms of Shuqing Granule in the Treatment of COVID-19, Pharmaceuticals, doi:10.3390/ph18081216.
Singirisetty et al., Drug repurposing in silico screening of antiviral drugs and evidence-based plant-derived anti-oxidant molecules targeting nsp15, main protease, and nsp16-nsp10 complex of SARS-CoV-2: strategic insights for managing future recurrence, Green Technology, Resilience, and Sustainability, doi:10.1007/s44173-025-00017-5.
Wu (E) et al., Utilizing natural compounds as ligands to disrupt the binding of SARS-CoV-2 receptor-binding domain to angiotensin-converting enzyme 2, impeding viral infection, Phytochemistry Letters, doi:10.1016/j.phytol.2025.102999.
Zeng et al., Novel receptor, mutation, vaccine, and establishment of coping mode for SARS-CoV-2: current status and future, Frontiers in Microbiology, doi:10.3389/fmicb.2023.1232453.
Zhao et al., Mechanistic insights into the dual anti-COVID-19 and anti-inflammatory actions of Zhengqi tablets, Journal of Ethnopharmacology, doi:10.1016/j.jep.2025.120249.
Zhao (B) et al., Multi-target mechanisms against coronaviruses of constituents from Chinese Dagang Tea revealed by experimental and docking studies, Journal of Ethnopharmacology, doi:10.1016/j.jep.2022.115528.
Xiong et al., Discovery of naturally occurring inhibitors against SARS-CoV-2 3CLpro from Ginkgo biloba leaves via large-scale screening, Fitoterapia, doi:10.1016/j.fitote.2021.104909.
Hariono et al., Potential SARS-CoV-2 3CLpro inhibitors from chromene, flavonoid and hydroxamic acid compound based on FRET assay, docking and pharmacophore studies, Results in Chemistry, doi:10.1016/j.rechem.2021.100195.
Du et al., Epigallocatechin-3-gallate, an active ingredient of Traditional Chinese Medicines, inhibits the 3CLpro activity of SARS-CoV-2, International Journal of Biological Macromolecules, doi:10.1016/j.ijbiomac.2021.02.012.
Singh (E) et al., Virtual Screening of Phytoconstituents in Indian Spices Based on their
Inhibitory Potential against SARS-CoV-2, Protein & Peptide Letters, doi:10.2174/0109298665366911250416113831.
Naveed et al., Exploring the therapeutic potential of Thymus vulgaris ethanol extract: a computational screening for antimicrobial compounds against COVID-19 induced mucormycosis, Scientific Reports, doi:10.1038/s41598-025-00937-z.
Odunowo, O., In-silico Investigation and Potential Therapeutic Approaches of Acanthus montanus for COVID-19: Computer-aided Drug Design Perspective, Journal of Advances in Medicine and Medical Research, doi:10.9734/jammr/2025/v37i45806.
Hasan et al., Potential medicinal plants used in the treatment of COVID-19: a review, Vegetable crops of Russia, doi:10.18619/2072-9146-2025-2-61-69.
Song et al., Natural products for targeting SARS-CoV-2 enzymes, RNA-dependent RNA polymerase and main protease, Journal of Applied Biological Chemistry, doi:10.3839/jabc.2025.022.
Chen (C) et al., Multitarget-based in silico screening from phytoactive compounds of Garcinia linii fighting toward severe acute respiratory syndrome coronavirus-2, Tzu Chi Medical Journal, doi:10.4103/tcmj.tcmj_226_24.
Wang (D) et al., Role of innate immunity in SARS-CoV-2 infection, Biosafety and Health, doi:10.1016/j.bsheal.2023.08.005.
Li et al., Pharmacological mechanism of action of Lianhua Qingwen in the treatment of COVID‐19 and facial neuritis, World Journal of Otorhinolaryngology - Head and Neck Surgery, doi:10.1002/wjo2.185.
Vahekeni et al., Historical texts as a potential resource for plant-based antiviral agents against SARS-CoV-2: the example of the Receptarium of Burkhard III von Hallwyl from 16th-century Switzerland, Frontiers in Pharmacology, doi:10.3389/fphar.2025.1731629.
Fu et al., Deep learning-based network pharmacology for exploring the mechanism of licorice for the treatment of COVID-19, Scientific Reports, doi:10.1038/s41598-023-31380-7.
Zhu et al., Uncovering the covalent inhibitors of SARS-CoV-2 Mpro in Tibetan edible herb Rhodiola crenulata and their synergistic anti-Mpro mechanism, Journal of Pharmaceutical Analysis, doi:10.1016/j.jpha.2025.101224.
Atatreh et al., Exploring covalent inhibitors of SARS-CoV-2 main protease: from peptidomimetics to novel scaffolds, Journal of Enzyme Inhibition and Medicinal Chemistry, doi:10.1080/14756366.2025.2460045.
Sergiel, I., Wybrane aspekty przeciwwirusowej aktywności flawonoidów względem SARS-CoV-2, Postępy Biochemii, doi:10.18388/pb.2021_562.
Świątek et al., Flavonoids as potential inhibitors targeting SARS-CoV-2, Traditional Medicines and Natural Products as Preventive and Therapeutic Agents Against COVID-19, doi:10.1016/B978-0-443-18757-5.00008-6.
Lu (B), L., Chinese herbal medicines for the treatment of COVID-19, Traditional Medicines and Natural Products as Preventive and Therapeutic Agents Against COVID-19, doi:10.1016/B978-0-443-18757-5.00001-3.
Motyl et al., SARS-CoV-2 Infection and Alpha-Synucleinopathies: Potential Links and Underlying Mechanisms, International Journal of Molecular Sciences, doi:10.3390/ijms252212079.
Navacchia et al., Insights into SARS-CoV-2: Small-Molecule Hybrids for COVID-19 Treatment, Molecules, doi:10.3390/molecules29225403.
Smail et al., Decoding the intricacies: a comprehensive analysis of microRNAs in the pathogenesis, diagnosis, prognosis and therapeutic strategies for COVID-19, Frontiers in Medicine, doi:10.3389/fmed.2024.1430974.
Chatatikun et al., Potential of traditional medicines in alleviating COVID-19 symptoms, Frontiers in Pharmacology, doi:10.3389/fphar.2024.1452616.
Guan et al., Exploring new therapeutic potential of five commonly used Pteris medicinal plants through pharmaphylogenomics and network pharmacology, Chinese Herbal Medicines, doi:10.1016/j.chmed.2024.09.003.
Jabeen et al., Insights for Future Pharmacology: Exploring Phytochemicals as Potential Inhibitors Targeting SARS-CoV-2 Papain-like Protease, Future Pharmacology, doi:10.3390/futurepharmacol4030029.
Al Adem et al., 3-chymotrypsin-like protease in SARS-CoV-2, Bioscience Reports, doi:10.1042/BSR20231395.
Shanmugam et al., Targeting SARS-CoV-2 Spike and Main protease with phytochemicals from Herbs and spices: Molecular Docking and dynamics simulation studies., Journal of Physics: Conference Series, doi:10.1088/1742-6596/2801/1/012013.
Zagórska et al., Inhibitors of SARS-CoV-2 Main Protease (Mpro) as Anti-Coronavirus Agents, Biomolecules, doi:10.3390/biom14070797.
Ebrahimi et al., Systems biology approaches to identify driver genes and drug combinations for treating COVID-19, Scientific Reports, doi:10.1038/s41598-024-52484-8.
Sathishkumar, K., From nature to medicine: bioactive compounds in the battle against SARS-CoV-2, Natural Product Research, doi:10.1080/14786419.2024.2375754.
Nur Hannani Ahmad Rozani et al., Molecular Docking of Phytochemicals from M. Charantia Targeting SARS-CoV-2 Main Protease, Journal of Advanced Research in Applied Sciences and Engineering Technology, doi:10.37934/araset.47.1.152165.
Trischitta et al., Pseudovirus-Based Systems for Screening Natural Antiviral Agents: A Comprehensive Review, International Journal of Molecular Sciences, doi:10.3390/ijms25105188.
Gupta (B) et al., Exploring Binding Pockets in the Conformational States of the SARS-CoV-2 Spike Trimers for the Screening of Allosteric Inhibitors Using Molecular Simulations and Ensemble-Based Ligand Docking, International Journal of Molecular Sciences, doi:10.3390/ijms25094955.
Chavda et al., SARS-CoV-2 Variants and Global Population Vulnerability, Apple Academic Press, doi:10.1201/9781003467939.
Lei et al., Small molecules in the treatment of COVID-19, Signal Transduction and Targeted Therapy, doi:10.1038/s41392-022-01249-8.
Xu (D) et al., Discovery of common molecular signatures and drug repurposing for COVID-19/Asthma comorbidity: ACE2 and multi-partite networks, Cell Cycle, doi:10.1080/15384101.2024.2340859.
Al-Jamal et al., Treating COVID-19 with Medicinal Plants: Is It Even Conceivable? A Comprehensive Review, Viruses, doi:10.3390/v16030320.
Yousefi Rad et al., Moringa oleifera and Its Biochemical Compounds: Potential Multi-targeted Therapeutic Agents Against COVID-19 and Associated Cancer Progression, Biochemical Genetics, doi:10.1007/s10528-024-10758-w.
Masoudi-Sobhanzadeh et al., Structure-based drug repurposing against COVID-19 and emerging infectious diseases: methods, resources and discoveries, Briefings in Bioinformatics, doi:10.1093/bib/bbab113.
Jamal, Q., Antiviral Potential of Plants against COVID-19 during Outbreaks—An Update, International Journal of Molecular Sciences, doi:10.3390/ijms232113564.
Szabó et al., Natural products as a source of Coronavirus entry inhibitors, Frontiers in Cellular and Infection Microbiology, doi:10.3389/fcimb.2024.1353971.
Sharun et al., A comprehensive review on pharmacologic agents, immunotherapies and supportive therapeutics for COVID-19, Narra J, doi:10.52225/narra.v2i3.92.
Bizzoca et al., Natural compounds may contribute in preventing SARS-CoV-2 infection: a narrative review, Food Science and Human Wellness, doi:10.1016/j.fshw.2022.04.005.
Dong et al., Development of SARS-CoV-2 entry antivirals, Cell Insight, doi:10.1016/j.cellin.2023.100144.
Abubakar et al., Potential benefits and challenges on the use of phytochemicals for obese COVID-19 patients: A review, Phytomedicine Plus, doi:10.1016/j.phyplu.2024.100526.
Banerjee et al., Potential SARS-CoV-2 main protease inhibitors, Drug Discovery Today, doi:10.1016/j.drudis.2020.12.005.
Liu et al., Plant‐derived compounds as potential leads for new drug development targeting COVID‐19, Phytotherapy Research, doi:10.1002/ptr.8105.
Taguchi et al., Novel Method for Detection of Genes With Altered Expression Caused by Coronavirus Infection and Screening of Candidate Drugs for SARS-CoV-2, MDPI AG, doi:10.20944/preprints202004.0431.v1.
Taguchi (B) et al., A New Advanced In Silico Drug Discovery Method for Novel Coronavirus (SARS-CoV-2) with Tensor Decomposition-Based Unsupervised Feature Extraction, MDPI AG, doi:10.20944/preprints202004.0524.v1.
Gysi et al., Network Medicine Framework for Identifying Drug Repurposing Opportunities for COVID-19, arXiv, doi:10.48550/arXiv.2004.07229.
Glinsky, G., Harnessing powers of genomics to build molecular maps of coronavirus targets in human cells: a guide for existing drug repurposing and experimental studies identifying candidate therapeutics to mitigate the pandemic COVID-19., American Chemical Society (ACS), doi:10.26434/chemrxiv.12052512.v2.
Smith et al., Repurposing Therapeutics for COVID-19: Supercomputer-Based Docking to the SARS-CoV-2 Viral Spike Protein and Viral Spike Protein-Human ACE2 Interface, American Chemical Society (ACS), doi:10.26434/chemrxiv.11871402.v4.
Abarova et al., Emerging Therapeutic Potential of Polyphenols from Geranium sanguineum L. in Viral Infections, Including SARS-CoV-2, Biomolecules, doi:10.3390/biom14010130.
Huang et al., Signaling pathways and potential therapeutic targets in acute respiratory distress syndrome (ARDS), Respiratory Research, doi:10.1186/s12931-024-02678-5.
Shukla et al., Virtual Screening of Orally Active Lead Compounds of Pearl Millet and Their Structural Activity Against Target Protein of COVID-19, Russian Journal of Bioorganic Chemistry, doi:10.1134/S1068162023080058.
Khalifa et al., After the Hurricane: Anti-COVID-19 Drugs Development, Molecular Mechanisms of Action and Future Perspectives, International Journal of Molecular Sciences, doi:10.3390/ijms25020739.
Velásquez et al., Effectiveness of Drug Repurposing and Natural Products Against SARS-CoV-2: A Comprehensive Review, Clinical Pharmacology: Advances and Applications, doi:10.2147/CPAA.S429064.
Dofuor et al., The Global Impact of COVID-19: Historical Development, Molecular Characterization, Drug Discovery and Future Directions, Clinical Pathology, doi:10.1177/2632010x231218075.
Olanike et al., Phytochemical compounds present in COVI-MXG herbal preparation inhibits RNA-Dependent RNA polymerase from SARS-CoV-2: A molecular docking study, Journal of Medicinal Plants Research, doi:10.5897/JMPR2020.7065.
Fauquet et al., Microfluidic Diffusion Sizing Applied to the Study of Natural Products and Extracts That Modulate the SARS-CoV-2 Spike RBD/ACE2 Interaction, Molecules, doi:10.3390/molecules28248072.
Zaa et al., Neuroprotective Agents with Therapeutic Potential for COVID-19, Biomolecules, doi:10.3390/biom13111585.
Comunale et al., The Functional Implications of Broad Spectrum Bioactive Compounds Targeting RNA-Dependent RNA Polymerase (RdRp) in the Context of the COVID-19 Pandemic, Viruses, doi:10.3390/v15122316.
Syamsi et al., Efek Potensial Moringa Oleifera pada Infeksi COVID-19, Malahayati Nursing Journal, doi:10.33024/mnj.v5i3.8144.
Yang (D) et al., Network Pharmacology and Experimental Validation of Qingwen Baidu
Decoction Therapeutic Potential in COVID-19-related Lung Injury, Combinatorial Chemistry & High Throughput Screening, doi:10.2174/0113862073236899230919062725.
Beg et al., Are herbal drugs effective in COVID management? A review to demystify the current facts and claims, ScienceOpen, doi:10.14293/s2199-1006.1.sor-.ppxfif7.v2.
Zeng (B) et al., Jinhua Qinggan Granule UHPLC-Q-extractive-Orbitrap-MS assay: Putative identification of 45 potential anti-Covid-19 constituents, confidential addition, and pharmacopoeia quality-markers recommendation, Journal of Food and Drug Analysis, doi:10.38212/2224-6614.3466.
Li (B) et al., Molecular mechanism of the effect of Gegen Qinlian decoction on COVID-19 comorbid with diabetes mellitus based on network pharmacology and molecular docking: A review, Medicine, doi:10.1097/MD.0000000000034683.
Souza et al., Molecular Docking and ADME-TOX Profiling of Moringa oleifera Constituents against SARS-CoV-2, Advances in Respiratory Medicine, doi:10.3390/arm91060035.
Singh (F) et al., Medicinal plants, phytoconstituents and traditional formulation as potential therapies for SARS-CoV-2: a review update, Vegetos, doi:10.1007/s42535-023-00706-1.
Biswas et al., Antiviral Phytocompounds Against Animal-to-Human Transmittable SARS-CoV-2, Ethnopharmacology and Drug Discovery for COVID-19: Anti-SARS-CoV-2 Agents from Herbal Medicines and Natural Products, doi:10.1007/978-981-99-3664-9_7.
He et al., Recent advances towards natural plants as potential inhibitors of SARS-Cov-2 targets, Pharmaceutical Biology, doi:10.1080/13880209.2023.2241518.
Jaber, S., The effect of a small polyphenolic and terpenoids phytochemical constituent on curing and preventing of Covid-19 infections, Pharmacia, doi:10.3897/pharmacia.70.e106534.
Mushebenge et al., Assessing the Potential Contribution of in Silico Studies in Discovering Drug Candidates that Interact with Various SARS-CoV-2 Receptors, MDPI AG, doi:10.20944/preprints202308.0434.v1.
Onyango, O., In Silico Models for Anti-COVID-19 Drug Discovery: A Systematic Review, Advances in Pharmacological and Pharmaceutical Sciences, doi:10.1155/2023/4562974.
Akter et al., Plausibility of natural immunomodulators in the treatment of COVID-19–A comprehensive analysis and future recommendations, Heliyon, doi:10.1016/j.heliyon.2023.e17478.
Rafiq et al., A Comprehensive Update of Various Attempts by Medicinal Chemists to Combat COVID-19 through Natural Products, Molecules, doi:10.3390/molecules28124860.
Badrunanto et al., In-silico approaches potential compounds in ginger (Zingiber officinale) as inhibitors of membrane, envelope, nucleocapsid, Plpro, and Helicase proteins of the SARS-CoV-2, INTERNATIONAL CONFERENCE ON APPLIED COMPUTATIONAL INTELLIGENCE AND ANALYTICS (ACIA-2022), doi:10.1063/5.0127236.
Jaka Fajar Fatriansyah et al., Molecular Docking and Molecular Dynamics of Herbal Plants Phylantus Niruri Linn (Green Meniran) towards of SARS-CoV-2 Main Protease, Evergreen, doi:10.5109/6792822.
Schake et al., An interaction-based drug discovery screen explains known SARS-CoV-2 inhibitors and predicts new compound scaffolds, Scientific Reports, doi:10.1038/s41598-023-35671-x.
Xie (B) et al., Exploring the mechanism of Ge-Gen-Qin-Lian-Wan against Novel coronavirus pneumonia based on network pharmacology and molecular docking techniques, Medical Data Mining, doi:10.53388/MDM202306016.
Tiwari et al., Virtual Screening of Phytochemicals in Search of a Potential Drug Candidate for COVID-19: DFT Study and Molecular Docking, COVID-19: Origin, Impact and Management (Part 2), doi:10.2174/9789815165944123010012.
Fan (B) et al., Pharmaceutical approaches for COVID-19: An update on current therapeutic opportunities, Acta Pharmaceutica, doi:10.2478/acph-2023-0014.
Lundstrom et al., COVID-19 signalome: Potential therapeutic interventions, Cellular Signalling, doi:10.1016/j.cellsig.2022.110559.
Mehyar, N., Coronaviruses SARS-CoV, MERS-CoV, and SARS-CoV-2 helicase inhibitors: A systematic review of in vitro studies, Journal of Virus Eradication, doi:10.1016/j.jve.2023.100327.
Wang (E) et al., Inflammasomes: a rising star on the horizon of COVID-19 pathophysiology, Frontiers in Immunology, doi:10.3389/fimmu.2023.1185233.
Oliver et al., Different drug approaches to COVID-19 treatment worldwide: an update of new drugs and drugs repositioning to fight against the novel coronavirus, Therapeutic Advances in Vaccines and Immunotherapy, doi:10.1177/25151355221144845.
Priyandoko et al., Inflammation Inhibitory Activity of Green Tea, Soybean, and Guava Extracts During Sars-Cov-2 Infection Through TNF Protein in Cytokine Storm, Computational Biology and Chemistry, doi:10.1016/j.compbiolchem.2023.107898.
Fu (B) et al., The mechanism of TCM prevention and treatment of heavy COVID-19 based on data mining and network pharmacology, Drug Combination Therapy, doi:10.53388/DCT20230010.
Abou Baker et al., An overview on medicinal plants used for combating coronavirus: Current potentials and challenges, Journal of Agriculture and Food Research, doi:10.1016/j.jafr.2023.100632.
Xue et al., Repurposing clinically available drugs and therapies for pathogenic targets to combat SARS‐CoV‐2, MedComm, doi:10.1002/mco2.254.
Akanchise et al., Ginkgo Biloba and Long COVID: In Vivo and In Vitro Models for the Evaluation of Nanotherapeutic Efficacy, Pharmaceutics, doi:10.3390/pharmaceutics15051562.
Toigo et al., Flavonoid as possible therapeutic targets against COVID-19: a scoping review of in silico studies, DARU Journal of Pharmaceutical Sciences, doi:10.1007/s40199-023-00461-3.
Srivastava et al., A Brief Review on Medicinal Plants-At-Arms against COVID-19, Interdisciplinary Perspectives on Infectious Diseases, doi:10.1155/2023/7598307.
Peralta-Moreno et al., Autochthonous Peruvian Natural Plants as Potential SARS-CoV-2 Mpro Main Protease Inhibitors, Pharmaceuticals, doi:10.3390/ph16040585.
Giordano et al., Food Plant Secondary Metabolites Antiviral Activity and Their Possible Roles in SARS-CoV-2 Treatment: An Overview, Molecules, doi:10.3390/molecules28062470.
England et al., Plants as Biofactories for Therapeutic Proteins and Antiviral Compounds to Combat COVID-19, Life, doi:10.3390/life13030617.
Yang (E) et al., A Comprehensive Review of Natural Flavonoids with Anti-SARS-CoV-2 Activity, Molecules, doi:10.3390/molecules28062735.
Trivedi et al., Antiviral and Anti-Inflammatory Plant-Derived Bioactive Compounds and Their Potential Use in the Treatment of COVID-19-Related Pathologies, Journal of Xenobiotics, doi:10.3390/jox12040020.
Taguchi (C) et al., A new advanced in silico drug discovery method for novel coronavirus (SARS-CoV-2) with tensor decomposition-based unsupervised feature extraction, PLOS ONE, doi:10.1371/journal.pone.0238907.
Khaerunnisa et al., Potential Inhibitor of COVID-19 Main Protease (M<sup>pro</sup>) From Several Medicinal Plant Compounds by Molecular Docking Study, MDPI AG, doi:10.20944/preprints202003.0226.v1.
Mardaneh et al., Inhibiting NF-κB During Cytokine Storm in COVID-19: Potential Role of Natural Products as a Promising Therapeutic Approach, MDPI AG, doi:10.20944/preprints202106.0130.v1.
Bekheit et al., Potential RNA-dependent RNA polymerase inhibitors as prospective drug candidates for SARS-CoV-2, European Journal of Medicinal Chemistry, doi:10.1016/j.ejmech.2023.115292.
Dutta et al., A systemic review on medicinal plants and their bioactive constituents against avian influenza and further confirmation through in-silico analysis, Heliyon, doi:10.1016/j.heliyon.2023.e14386.
Heleno et al., Plant Extracts and SARS-CoV-2: Research and Applications, Life, doi:10.3390/life13020386.
Zeyad Bazbouz et al., Plant phytochemicals as potential candidates for treating post‐COVID‐19 lung infections, Phytotherapy Research, doi:10.1002/ptr.7650.
Jiang et al., Exploration of Fuzheng Yugan Mixture on COVID-19 based on network pharmacology and molecular docking, Medicine, doi:10.1097/MD.0000000000032693.
Guo (B) et al., Enhanced compound-protein binding affinity prediction by representing protein multimodal information via a coevolutionary strategy, Briefings in Bioinformatics, doi:10.1093/bib/bbac628.
Zhang (D) et al., Herbal medicines exhibit a high affinity for ACE2 in treating COVID-19, BioScience Trends, doi:10.5582/bst.2022.01534.
Supianto et al., Cluster-based text mining for extracting drug candidates for the prevention of COVID-19 from the biomedical literature, Journal of Taibah University Medical Sciences, doi:10.1016/j.jtumed.2022.12.015.
Guerra et al., Critical Review of Plant-Derived Compounds as Possible Inhibitors of SARS-CoV-2 Proteases: A Comparison with Experimentally Validated Molecules, ACS Omega, doi:10.1021/acsomega.2c05766.
Fatriansyah et al., Molecular Dynamics Simulation of Ligands from Anredera cordifolia (Binahong) to the Main Protease (Mpro) of SARS-CoV-2, Journal of Tropical Medicine, doi:10.1155/2022/1178228.
Chen (D) et al., The exploration of phytocompounds theoretically combats SARS-CoV-2 pandemic against virus entry, viral replication and immune evasion, Journal of Infection and Public Health, doi:10.1016/j.jiph.2022.11.022.
Azeem et al., Virtual screening of phytochemicals by targeting multiple proteins of severe acute respiratory syndrome coronavirus 2: Molecular docking and molecular dynamics simulation studies, International Journal of Immunopathology and Pharmacology, doi:10.1177/03946320221142793.
Bijelić et al., Phytochemicals in the Prevention and Treatment of SARS-CoV-2—Clinical Evidence, Antibiotics, doi:10.3390/antibiotics11111614.
Milton-Laskibar et al., Potential usefulness of Mediterranean diet polyphenols against COVID-19-induced inflammation: a review of the current knowledge, Journal of Physiology and Biochemistry, doi:10.1007/s13105-022-00926-0.
Ur Rehman et al., Flavonoids and other polyphenols against SARS-CoV-2, Application of Natural Products in SARS-CoV-2, doi:10.1016/B978-0-323-95047-3.00014-9.
de Matos et al., Bioactive compounds as potential angiotensin-converting enzyme II inhibitors against COVID-19: a scoping review, Inflammation Research, doi:10.1007/s00011-022-01642-7.
Youn et al., Robust therapeutic effects on COVID-19 of novel small molecules: Alleviation of SARS-CoV-2 S protein induction of ACE2/TMPRSS2, NOX2/ROS, and MCP-1, Frontiers in Cardiovascular Medicine, doi:10.3389/fcvm.2022.957340.
Amalia et al., The Potential of Phyllanthus Niruri Plant Secondary Metabolites in Providing Antiviral Protection Against Sars-Cov-2: A Literature Review, KnE Medicine, doi:10.18502/kme.v2i3.11915.
Tiwari (B) et al., Molecular docking studies on the phytoconstituents as therapeutic leads against SARS-CoV-2, Polimery, doi:10.14314/polimery.2022.7.8.
Liu (B) et al., Investigating the Potential Bioactive Components of Qing-Fei-Pai-Du Decoction Against COVID-19 in Diabetes/Diabetic Patients Based on Network Pharmacology and Molecular Docking, Natural Product Communications, doi:10.1177/1934578X221124769.
Dinda (B) et al., Some natural compounds and their analogues having potent anti- SARS-CoV-2 and anti-proteases activities as lead molecules in drug discovery for COVID-19, European Journal of Medicinal Chemistry Reports, doi:10.1016/j.ejmcr.2022.100079.
Babu et al., Identification of differentially expressed genes and their major pathways among the patient with COVID-19, cystic fibrosis, and chronic kidney disease, Informatics in Medicine Unlocked, doi:10.1016/j.imu.2022.101038.
Rieder et al., A Review of In Silico Research, SARS-CoV-2, and Neurodegeneration: Focus on Papain-Like Protease, Neurotoxicity Research, doi:10.1007/s12640-022-00542-2.
Liu (C) et al., Network Pharmacology and Molecular Docking Elucidate the Underlying Pharmacological Mechanisms of the Herb Houttuynia cordata in Treating Pneumonia Caused by SARS-CoV-2, Viruses, doi:10.3390/v14071588.
Sperry et al., Target-agnostic drug prediction integrated with medical record analysis uncovers differential associations of statins with increased survival in COVID-19 patients, PLOS Computational Biology, doi:10.1371/journal.pcbi.1011050.
Negru et al., Virtual Screening of Substances Used in the Treatment of SARS-CoV-2 Infection and Analysis of Compounds With Known Action on Structurally Similar Proteins From Other Viruses, Biomedicine & Pharmacotherapy, doi:10.1016/j.biopha.2022.113432.
Mortezaei et al., Variations of SARS-CoV-2 in the Iranian Population and Candidate Putative Drug-like Compounds to Inhibit the Mutated Proteins, Heliyon, doi:10.1016/j.heliyon.2022.e09910.
Shahhamzehei et al., In Silico and In Vitro Identification of Pan-Coronaviral Main Protease Inhibitors from a Large Natural Product Library, Pharmaceuticals, doi:10.3390/ph15030308.
Mateja et al., The choice of viral load endpoint in early phase trials of COVID-19 treatments aiming to reduce 28-day hospitalization and/or death, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf282.
Zhang (E) et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Sweeting et al., What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data, Statistics in Medicine, doi:10.1002/sim.1761.
Altman (C) et al., Interaction revisited: the difference between two estimates, BMJ, doi:10.1136/bmj.326.7382.219.
Michelucci et al., SARS-CoV-2 ORF3a accessory protein is a water-permeable channel that induces lysosome swelling, Communications Biology, doi:10.1038/s42003-024-07442-5.
Ghosh et al., β-Coronaviruses Use Lysosomes for Egress Instead of the Biosynthetic Secretory Pathway, Cell, doi:10.1016/j.cell.2020.10.039.
Kamga Kapchoup et al., In vitro effect of hydroxychloroquine on pluripotent stem cells and their cardiomyocytes derivatives, Frontiers in Pharmacology, doi:10.3389/fphar.2023.1128382.
Bobrowski et al., Synergistic and Antagonistic Drug Combinations against SARS-CoV-2, Molecular Therapy, doi:10.1016/j.ymthe.2020.12.016.
Peters (B) et al., Outcomes of Persons With COVID-19 in Hospitals With and Without Standard Treatment With (Hydroxy)chloroquine, Clinical Microbiology and Infection, doi:10.1016/j.cmi.2020.10.004.
Mahévas et al., Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data, BMJ 2020, doi:10.1136/bmj.m1844.
Minozzi et al., The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2020.06.015.
Popp et al., Ivermectin for preventing and treating COVID-19, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.CD015017.pub3.
Reis et al., Effect of Early Treatment with Ivermectin among Patients with Covid-19, New England Journal of Medicine, doi:10.1056/NEJMoa2115869.
Axfors et al., Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative meta-analysis of randomized trials, Nature, doi:10.1038/s41467-021-22446-z.