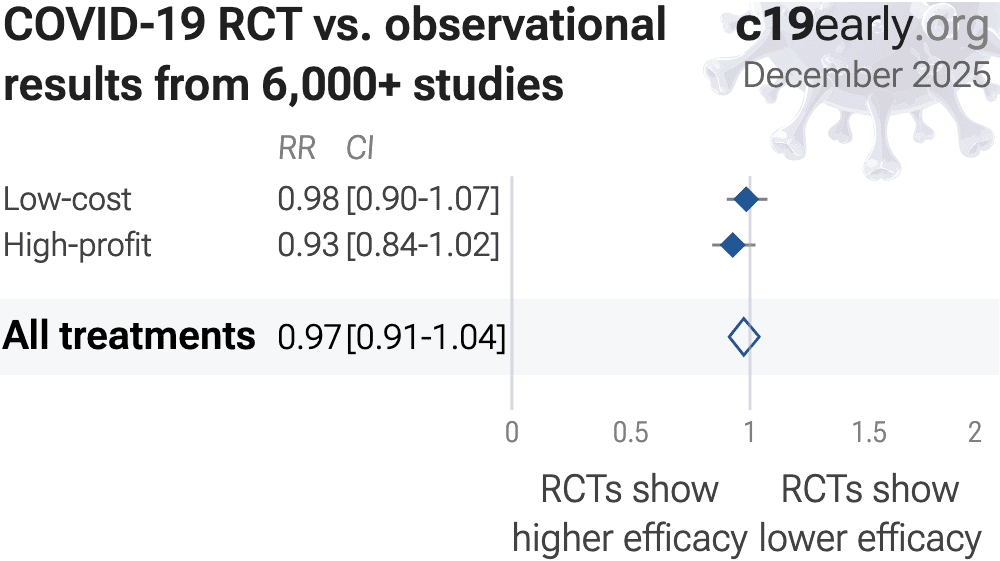
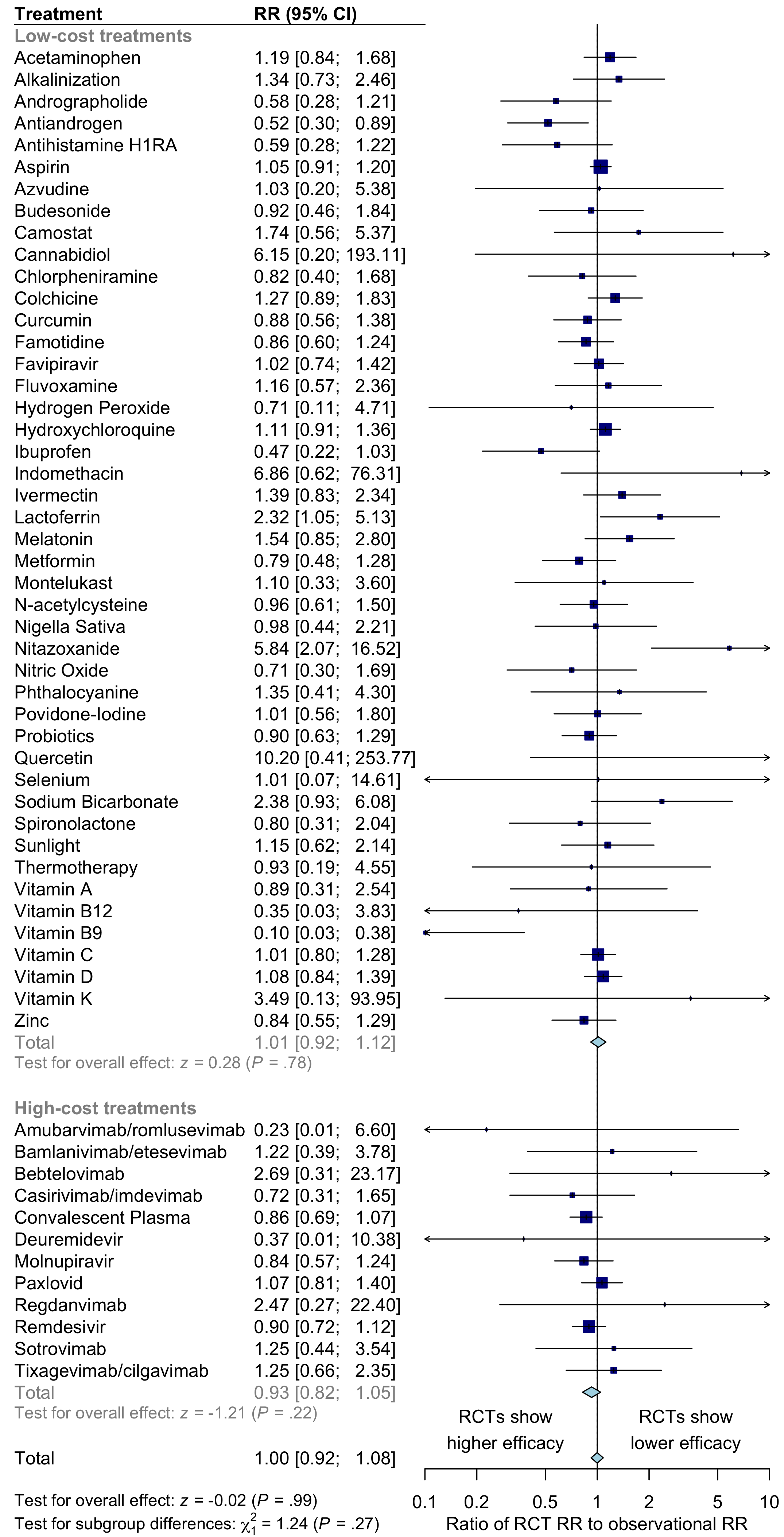
For COVID-19, across the 226 treatments we analyze, there
is no systematic difference in the results
for RCTs and observational studies, RR 0.97 [0.91‑1.03].
Restricting to, or waiting for, RCTs provided no benefit.
Observational studies for COVID-19 do not systematically overestimate or underestimate
efficacy when compared with RCTs, and they provided confirmation of efficacy 8+ months faster1.
Two additional large analyses also find no systematic difference between RCTs and observational studies2,3.
Concato et al. also report a paradoxical finding—RCT results had higher
variability, and only RCTs were found to sometimes report significant results the opposite
of the overall result. The same trend is seen for the most popular (most politicized)
COVID-19 treatments—considering all statistically significant results reported in
studies, RCTs are slightly more likely to report a result in the opposite direction. In
other words, assuming causality from a single study would have a higher error rate for
RCTs.
Neither observational studies nor RCTs prove causation—any study can be
flawed or fraudulent. We need much more, for example a combination of results from many
independent teams, detailed understanding of each study, knowledge of conflicts/team
reliability, dose-response relationships, delay-response relationships, logical results across outcomes, details consistent with preclinical expectations, etc.
RCTs aim to equalize study groups, but add
their own biases. For acute diseases with strong benefits for earlier treatment,
the typical increased treatment delay adds a major confounding factor.
RCTs for drugs with significant DDI risk may overestimate real-world efficacy because they
do a better job of excluding patients at DDI risk.
RCTs may be more
likely to have funding or staff with conflicts of interest.
RCTs may encourage monotherapy for simplicity at the cost of efficacy, which may rely on combined or synergistic effects.
RCT participants may not reflect real-world usage or the population that benefits most in terms of age, comorbidities, severity of illness, or other factors.
Both RCTs and observational studies span the bias spectrum, from minimal to extreme.
Studies must be evaluated individually.
While observational studies require greater expertise to analyze, the advantages in
practicality, cost, time, and ethics are substantial.
{kind=link}
{kind=link}