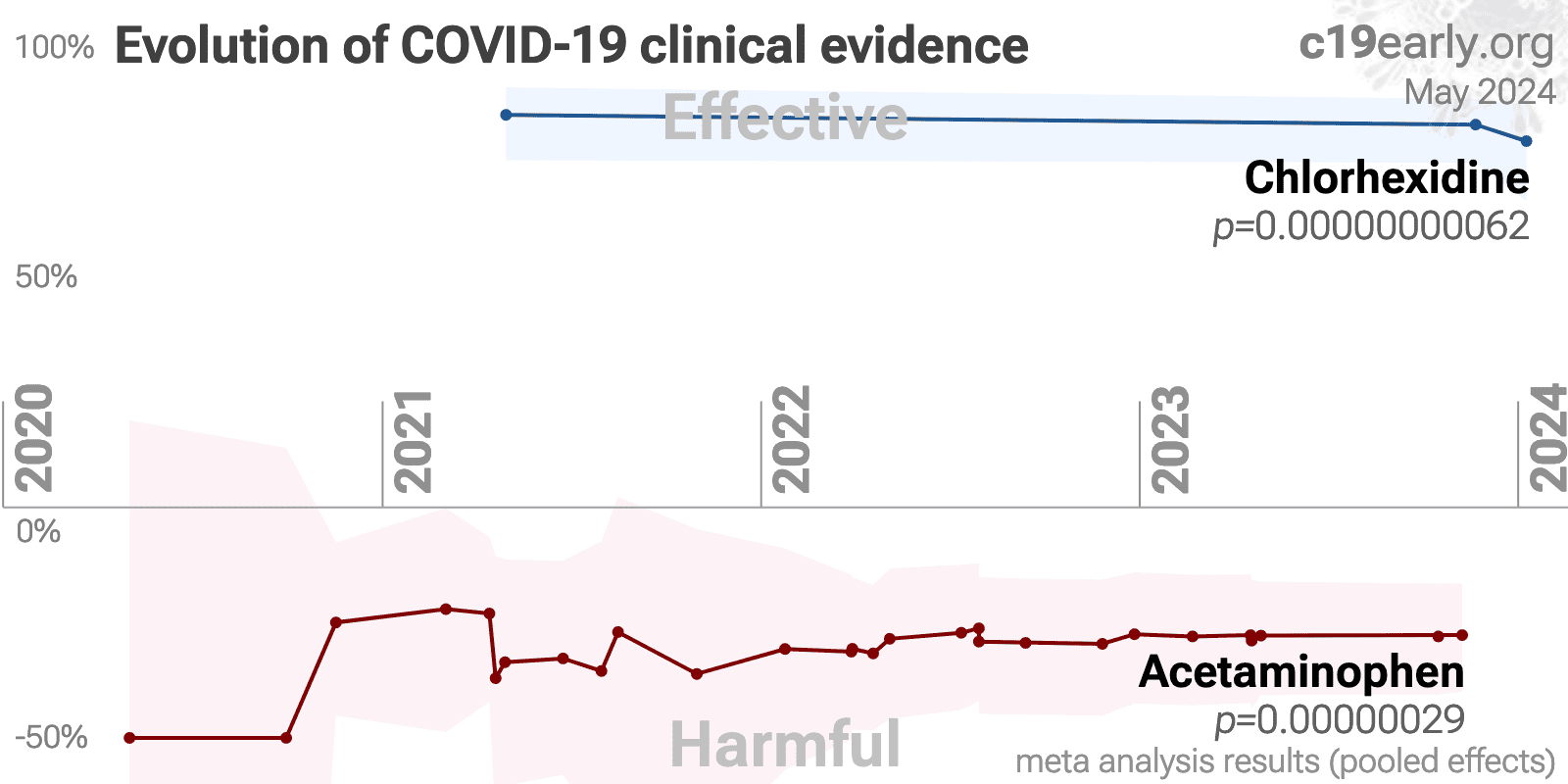
Chlorhexidine reduces COVID-19 risk: real-time meta-analysis of 5 studies
 Control
ControlAbstract
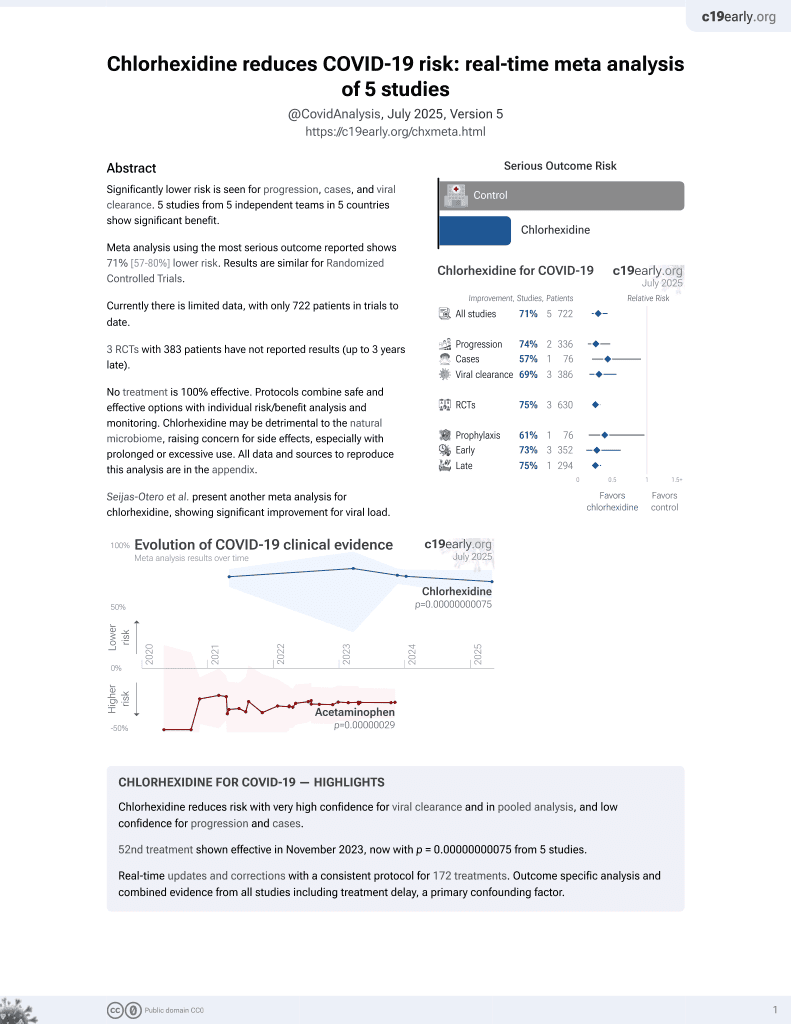
Significantly lower risk is seen for progression, cases, and viral clearance. 4 studies from 4 independent teams in 4 countries show significant
benefit.
Meta-analysis using the most serious outcome reported shows
70% [58‑79%] lower risk. Results are similar for Randomized Controlled Trials.
Currently there is limited data, with only 675 patients in trials to date.
3 RCTs
with 383 patients have not reported results (up to 4 years late).
No treatment is 100%
effective. Protocols combine safe and effective options with individual
risk/benefit analysis and monitoring.
Chlorhexidine may be detrimental to the natural microbiome, raising concern for side effects, especially with prolonged or excessive use.
All data and sources to reproduce this analysis are in the appendix.
Seijas-Otero et al. present another meta-analysis for chlorhexidine, showing significant improvement for viral load.
Chlorhexidine for COVID-19 — Highlights
Chlorhexidine reduces risk with very high confidence for viral clearance and in pooled analysis, and low confidence for progression and cases.
53rd treatment shown effective in November 2023, now with p < 0.00000000001 from 5 studies.
Real-time updates and corrections with a consistent protocol for 226 treatments. Outcome specific analysis and combined evidence from all studies including treatment delay, a primary confounding factor.
B
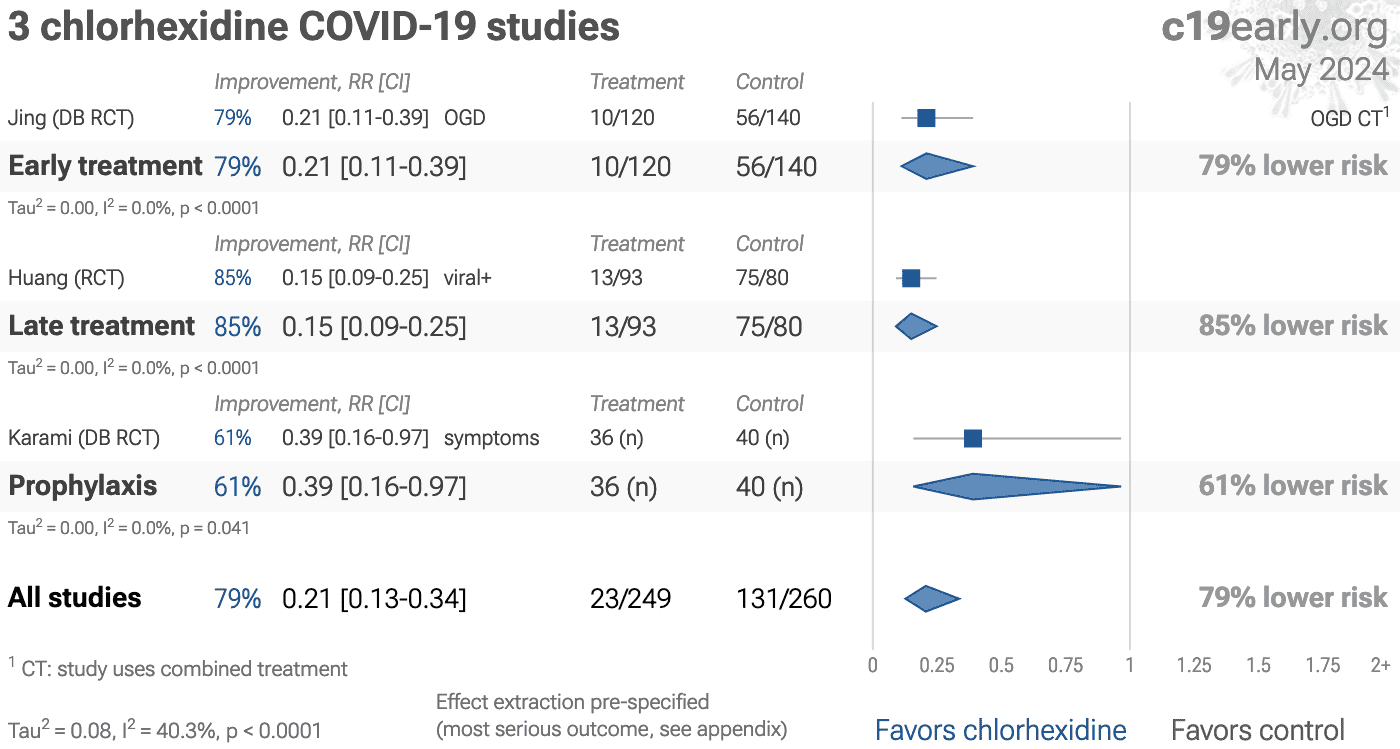
Fig. 1. A. Random-effects meta-analysis. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
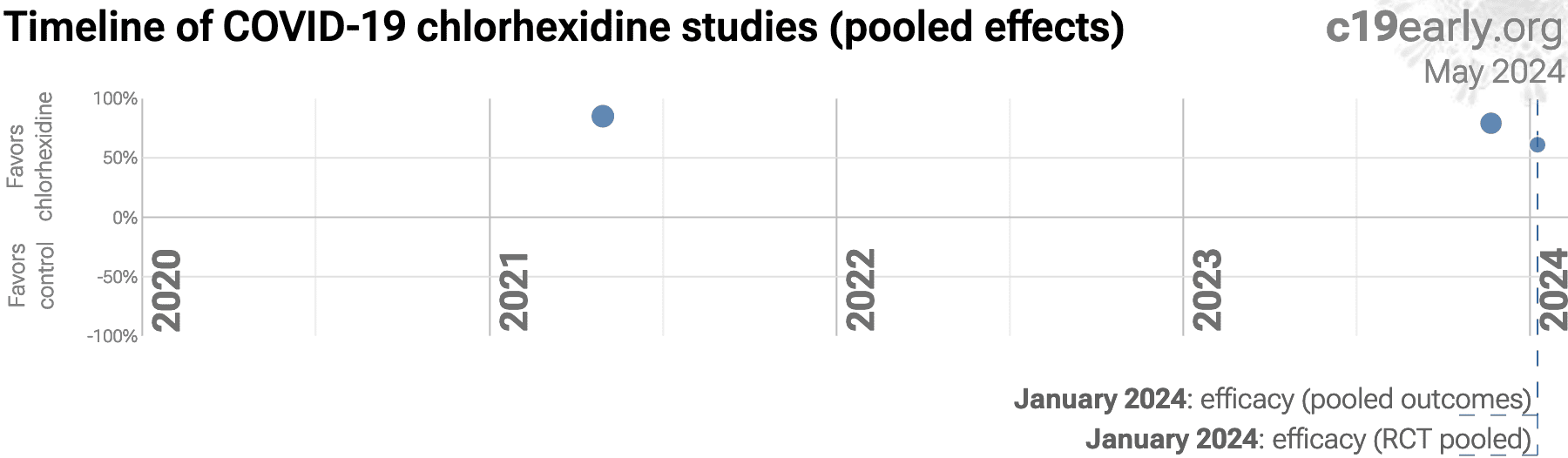
B. Timeline of results in chlorhexidine studies. The marked dates indicate the time when efficacy was known with a statistically significant improvement of ≥10% from ≥3 studies for pooled outcomes, one or more specific outcome, and pooled outcomes in RCTs. Efficacy based on specific outcomes was delayed by 17.3 months, compared to using pooled outcomes.
SARS-CoV-2 infection typically starts in the upper respiratory
tract, and specifically the nasal respiratory epithelium. Entry via the eyes
and gastrointestinal tract is possible, but less common, and entry via other
routes is rare.
Infection may progress to the lower respiratory tract, other tissues, and the
nervous and cardiovascular systems. The primary initial route for entry into
the central nervous system is thought to be the olfactory nerve in the nasal
cavity3.
Progression may lead to cytokine storm, pneumonia, ARDS, neurological
injury4-20 and cognitive
deficits7,12, cardiovascular
complications21-27, DNA
damage28-31, organ failure, and death.
Even mild untreated infections may result in persistent cognitive
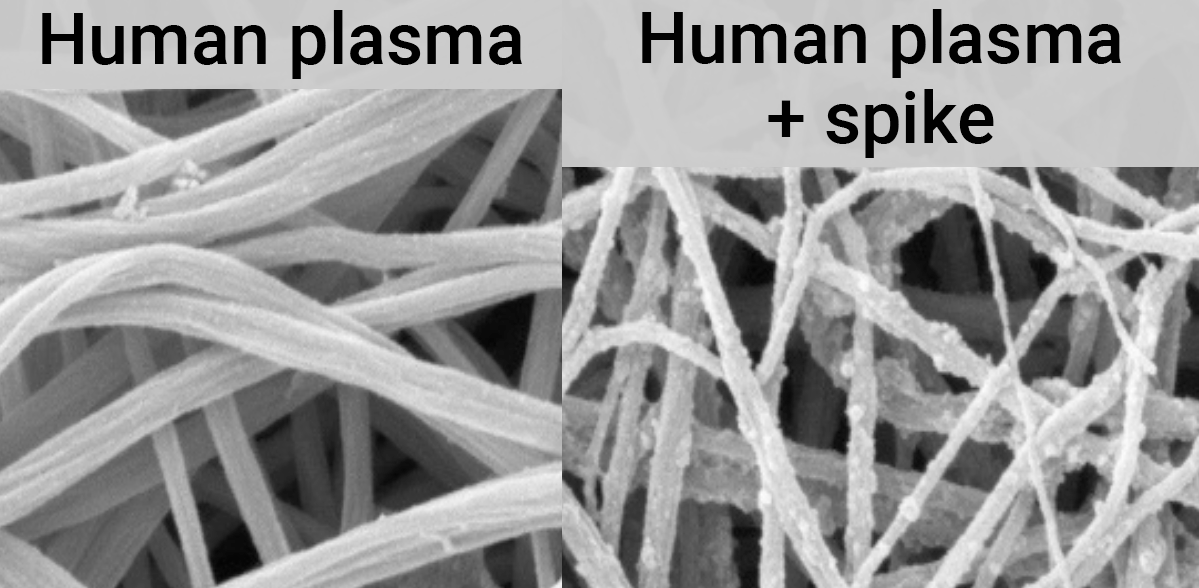
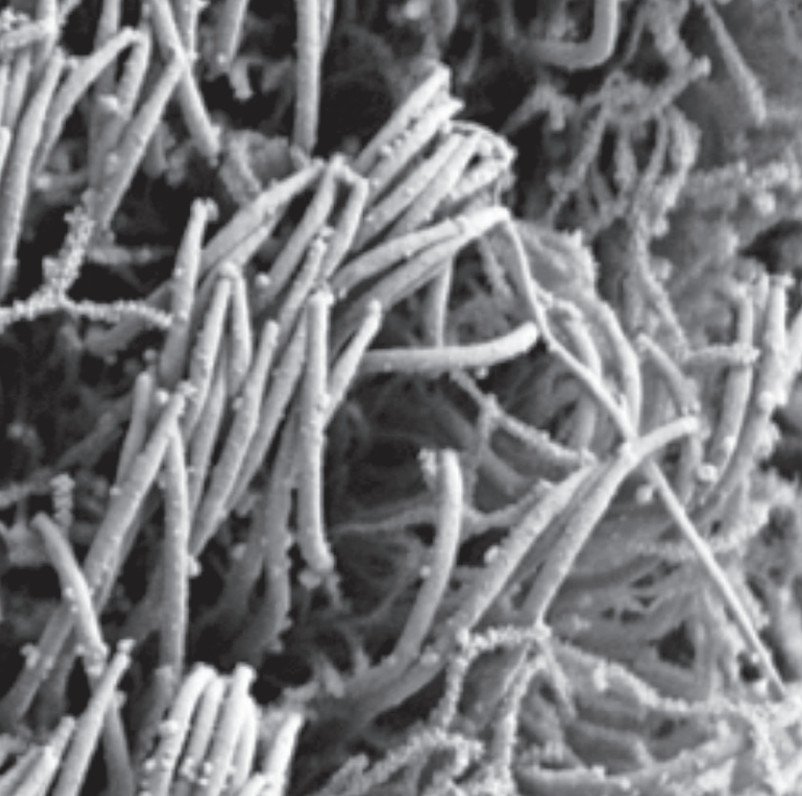
deficits32—the spike protein binds to fibrin leading to
fibrinolysis-resistant blood clots, thromboinflammation, and
neuropathology.
Systemic treatments may be insufficient to prevent
neurological damage11.
Minimizing replication as early as possible is recommended.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Logically, stopping replication in the upper respiratory tract should be
simpler and more effective.
Wu et al., using an airway organoid model incorporating many in
vivo aspects, show that SARS-CoV-2 initially attaches to cilia—hair-like
structures responsible for moving the mucus layer and where ACE2 is
localized in nasal epithelial cells35. The mucus layer and the
need for ciliary transport slow down infection, providing more time for
localized treatments33,34.
Early or prophylactic nasopharyngeal/oropharyngeal treatment may avoid the
consequences of viral replication in other tissues, and avoid the requirement
for systemic treatments with greater potential for side effects.
SARS-CoV-2 infection and replication involves the complex interplay of 500+
host and viral proteins and other factorsA,36-43 , providing many
therapeutic targets for which many existing compounds have known activity.
Scientists have predicted that over 11,000 compounds may
reduce COVID-19 risk44, either by
directly minimizing infection or replication, by supporting immune system
function, or by minimizing secondary complications.
We analyze all significant
controlled studies of
chlorhexidine
for COVID-19.
Search methods, inclusion criteria, effect extraction criteria (more serious
outcomes have priority), all individual study data, PRISMA answers, and
statistical methods are detailed in Appendix 1. We present random-effects
meta-analysis results for all studies, studies within each treatment stage, individual outcomes, and Randomized Controlled Trials (RCTs).
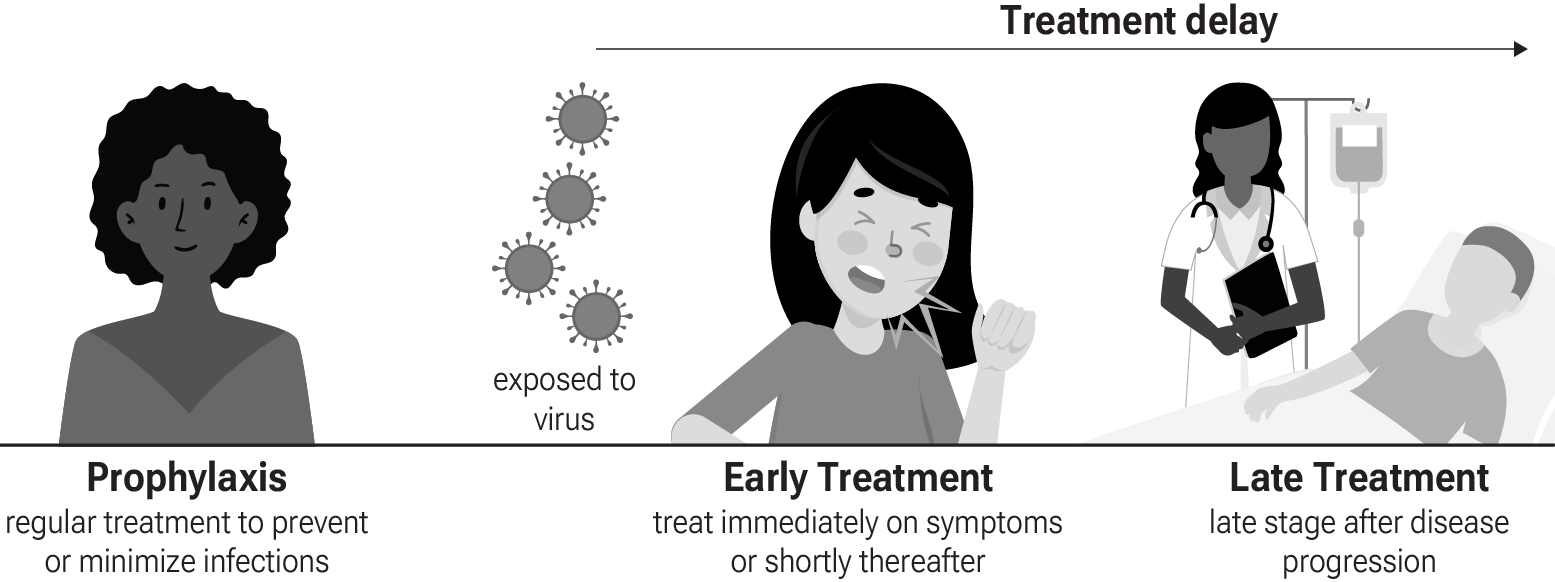
Fig. 4 shows stages of possible treatment for
COVID-19. Prophylaxis refers to regularly taking medication before
becoming sick, in order to prevent or minimize infection. Early
treatment refers to treatment immediately or soon after symptoms appear,
while late treatment refers to more delayed treatment.
{kind=link}
Fig. 4. Treatment stages.
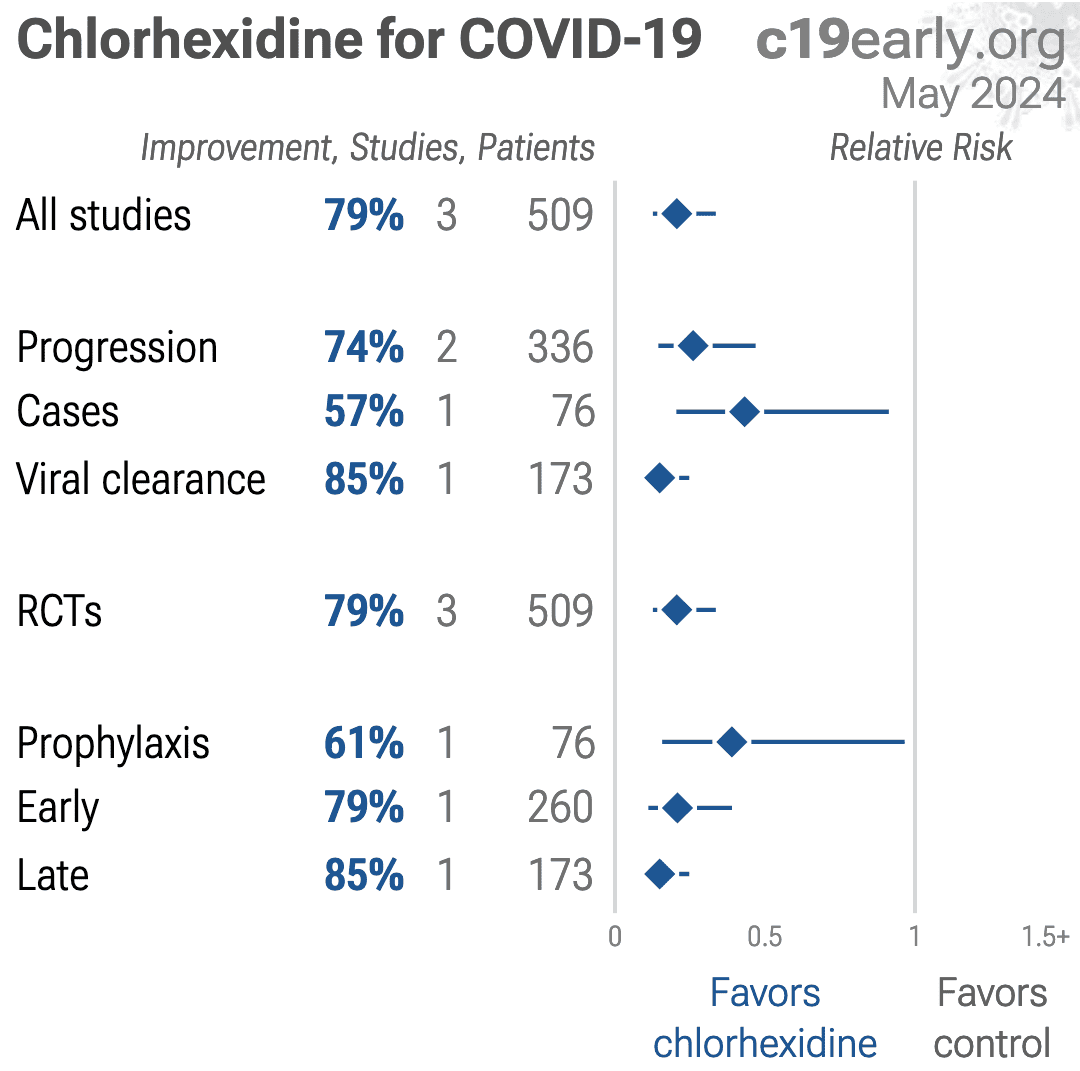
Table 1 summarizes the results for all stages combined, for Randomized Controlled Trials, and for specific outcomes.
Table 2 shows results by treatment stage.
Fig. 5 plots individual results by treatment stage.
Fig. 6, 7, 8, 9, and 10
show forest plots for random-effects meta-analysis of
all studies with pooled effects, progression, cases, viral clearance, and nasopharyngeal/oropharyngeal administration.
| Relative Risk | Studies | Patients | |
|---|---|---|---|
| All studies | 0.30 [0.21‑0.42]**** | 5 | 675 |
| RCTsRCTs | 0.25 [0.20‑0.32]**** | 4 | 645 |
| Viral | 0.32 [0.19‑0.54]**** | 3 | 339 |
| Early treatment | Late treatment | Prophylaxis | |
|---|---|---|---|
| All studies | 0.31 [0.16‑0.60]***0.31*** [0.16‑0.60] | 0.25 [0.19‑0.34]****0.25**** [0.19‑0.34] | 0.39 [0.16‑0.97]*0.39* [0.16‑0.97] |
| RCTsRCTs | 0.21 [0.11‑0.38]****0.21**** [0.11‑0.38] | 0.25 [0.19‑0.34]****0.25**** [0.19‑0.34] | 0.39 [0.16‑0.97]*0.39* [0.16‑0.97] |
| Viral | 0.45 [0.28‑0.70]***0.45*** [0.28‑0.70] | 0.25 [0.19‑0.34]****0.25**** [0.19‑0.34] | |
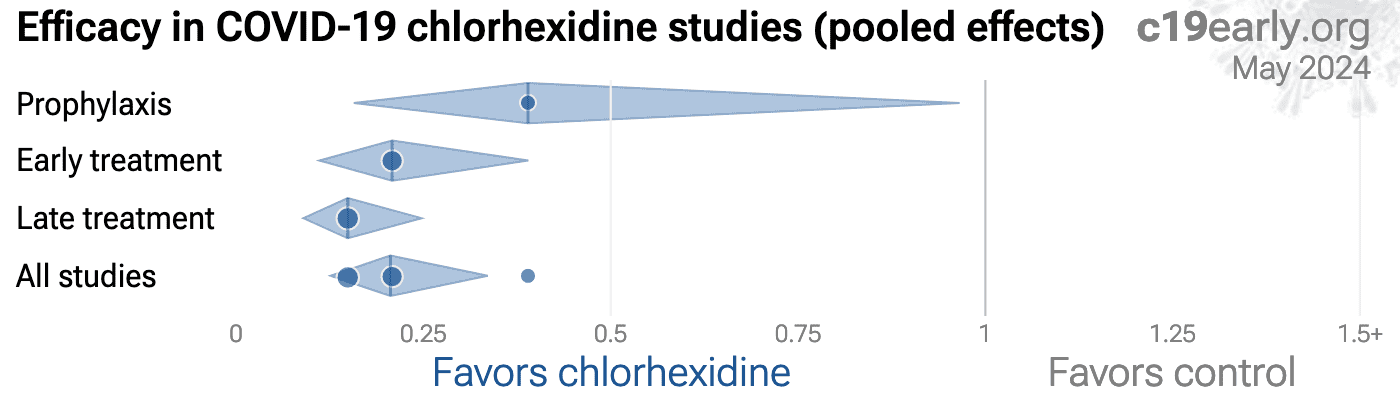{kind=link}
Fig. 5. Scatter plot showing the most serious outcome in all studies, and for studies within each stage. Diamonds shows the results of random-effects meta-analysis.
Loading..
Loading..
Fig. 6. Random-effects meta-analysis for all studies.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
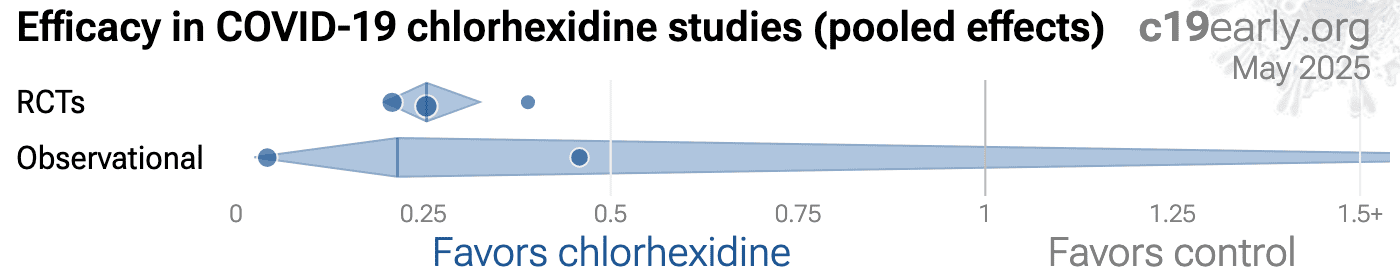
Fig. 11 shows a comparison of results for RCTs and observational studies.
Random-effects meta-analysis of RCTs shows
75% improvement,
compared to 54% for other studies.
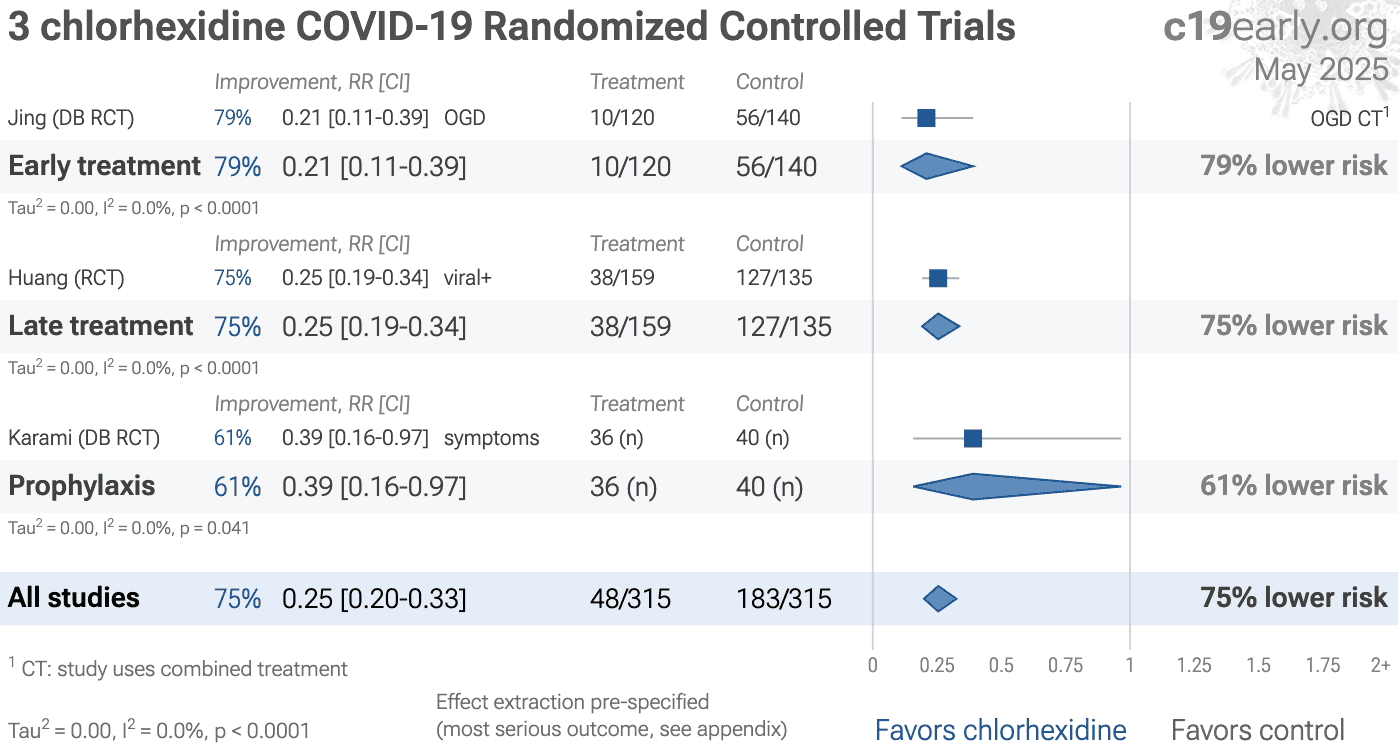
Fig. 12 shows a forest plot for random-effects
meta-analysis of all Randomized Controlled Trials.
RCT results are included in Table 1 and Table 2.
{kind=link}
Fig. 11. Results for RCTs and observational studies.
RCTs help to make study groups more similar and can provide a higher level of
evidence, however they are subject to many biases53, and
analysis of double-blind RCTs has identified extreme levels of bias54.
For COVID-19, the overhead may delay treatment, dramatically compromising
efficacy; they may encourage monotherapy for simplicity at the cost of
efficacy which may rely on combined or synergistic effects; the participants
that sign up may not reflect real world usage or the population that benefits
most in terms of age, comorbidities, severity of illness, or other factors;
standard of care may be compromised and unable to evolve quickly based on
emerging research for new diseases; errors may be made in randomization and
medication delivery; and investigators may have hidden agendas or vested
interests influencing design, operation, analysis, reporting, and the
potential for fraud. All of these biases have been observed with COVID-19
RCTs. There is no guarantee that a specific RCT provides a higher level of
evidence.
RCTs are expensive and many RCTs are funded
by pharmaceutical companies or other organizations with conflicts of interest, for example
governments that previously denied treatment with the study drug.
For COVID-19, this creates an incentive to show efficacy for
patented commercial products, and an incentive to show a lack of efficacy for
inexpensive treatments. The bias is expected to be significant, for example
Als-Nielsen et al. analyzed 370 RCTs from Cochrane reviews, showing that
trials funded by for-profit organizations were 5 times more likely to
recommend the experimental drug compared with those funded by nonprofit
organizations. Bekelman et al. and Lundh et al. show that
industry-sponsored studies are more likely to be favorable.
For COVID-19, some major philanthropic organizations are
largely funded by investments with extreme conflicts of interest for and
against specific COVID-19 interventions.
High quality RCTs for novel acute diseases are more challenging, with
increased ethical issues due to the urgency of treatment, increased risk due
to enrollment delays, and more difficult design with a rapidly evolving
evidence base. For COVID-19, the most common site of initial infection is the
upper respiratory tract. Immediate treatment is likely to be most successful
and may prevent or slow progression to other parts of the body. For a
non-prophylaxis RCT, it makes sense to provide treatment in advance and
instruct patients to use it immediately on symptoms, just as some governments
have done by providing medication kits in advance. Unfortunately, no RCTs have
been done in this way. Every treatment RCT to date involves delayed treatment.
Among the 226 treatments we have analyzed,
67% of RCTs involve very late treatment 5+ days after
onset. No non-prophylaxis COVID-19 RCTs match the potential real-world use of
early treatments. They may more accurately represent results for treatments
that require visiting a medical facility, e.g., those requiring intravenous
administration.
{kind=link}
Evidence shows that observational studies
can also provide reliable results. Concato et al. found that well-designed
observational studies do not systematically overestimate the magnitude of the
effects of treatment compared to RCTs. Anglemyer et al. analyzed reviews
comparing RCTs to observational studies and found little evidence for
significant differences in effect estimates.
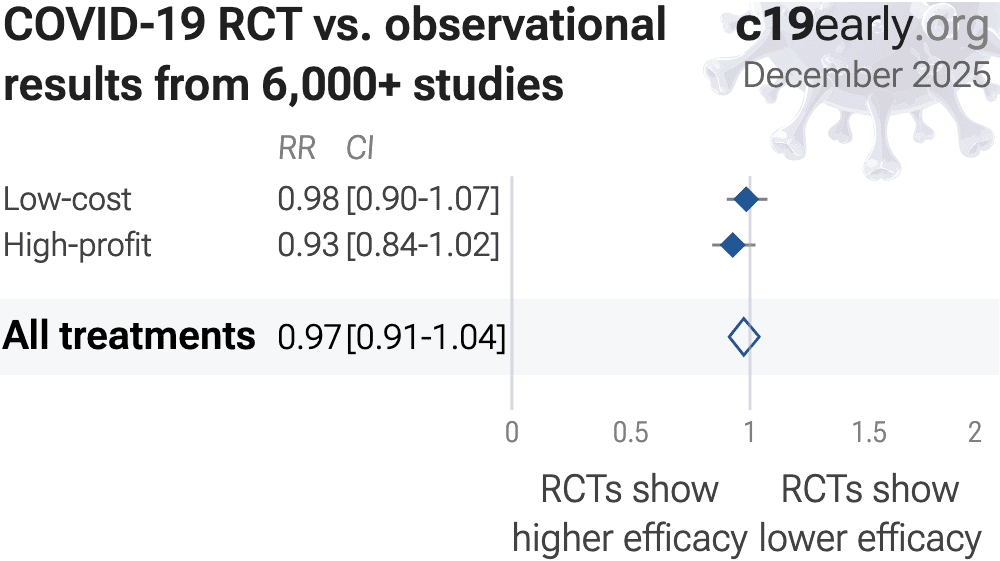
We performed a similar analysis across the 226 treatments
we cover, showing no significant difference in the results of RCTs compared to
observational studies, RR 0.97 [0.91‑1.03]50. Similar results are found for all low-cost treatments, RR
0.98 [0.90‑1.06]. High-cost treatments
show a non-significant trend towards RCTs showing greater efficacy,
RR 0.92 [0.84‑1.02].
Details can be found in the
supplementary data.
Lee (B) et al. showed that only 14% of the guidelines of the Infectious
Diseases Society of America were based on RCTs. Evaluation of studies relies
on an understanding of the study and potential biases. Limitations in an RCT
can outweigh the benefits, for example excessive dosages, excessive treatment
delays, or remote survey bias may have a greater effect on results. Ethical
issues may also prevent running RCTs for known effective treatments. For more
on issues with RCTs see62,63.
Concato et al. report a paradoxical finding—RCT results had higher
variability, and only RCTs were found to sometimes report significant results the opposite
of the overall result. The same trend is seen for the most popular (most politicized)
COVID-19 treatments—considering all statistically significant results reported in
studies, RCTs are slightly more likely to report a result in the opposite direction. In
other words, for these COVID-19 treatments and for the topics covered by Concato et al., assuming causality from a single study is more likely to result in an incorrect conclusion for
RCTs.
Increased risk of inconsistent results for RCTs suggests higher prevalence of
bias, which may arise due to many issues including design bias, conflicts of interest,
treatment differences by physicians aware of allocation, attrition bias, ascertainment
bias, randomization failures, errors, or fraud.
Currently, 59 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. Of these, 54% have been confirmed in RCTs, with a mean delay of 7.8 months (62% with 8.7 months delay for low-cost treatments). The remaining treatments either have no RCTs, or the point estimate is consistent.
Neither observational studies nor RCTs prove causation—any study can be
flawed or fraudulent. We need much more, for example a combination of results from many
independent teams, detailed understanding of each study, knowledge of conflicts/team
reliability, dose-response relationships, delay-response relationships, logical results across outcomes, or details consistent with preclinical expectations.
All studies must be evaluated individually. RCTs for a
given medication and disease may be more reliable, however they may also be
less reliable. For off-patent medications, very high conflict of interest
trials may be more likely to be RCTs, and more likely to be large trials that
dominate meta-analyses.
{kind=link}
Loading..
Fig. 12. Random-effects meta-analysis for all Randomized Controlled Trials.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
{kind=link}
Fig. 14.
Optimal spray angle may increase nasopharyngeal drug delivery 100x for nasal sprays,
adapted from Akash et al.
In addition to the dosage and frequency
of administration, efficacy for nasopharyngeal/oropharyngeal treatments may depend on
many other details. For example considering sprays, viscosity, mucoadhesion, sprayability,
droplet size64,65, dispersion65, and application
angle64 are important.
Akash et al. performed a computational fluid dynamics study
of nasal spray administration showing 100x improvement in nasopharyngeal drug
delivery using a new spray placement protocol, which involves holding the spay
nozzle close to horizontal at the nostril, with a slight tilt towards
the cheeks. The study also found the optimal droplet size range for
nasopharyngeal deposition was ~7-17µm.
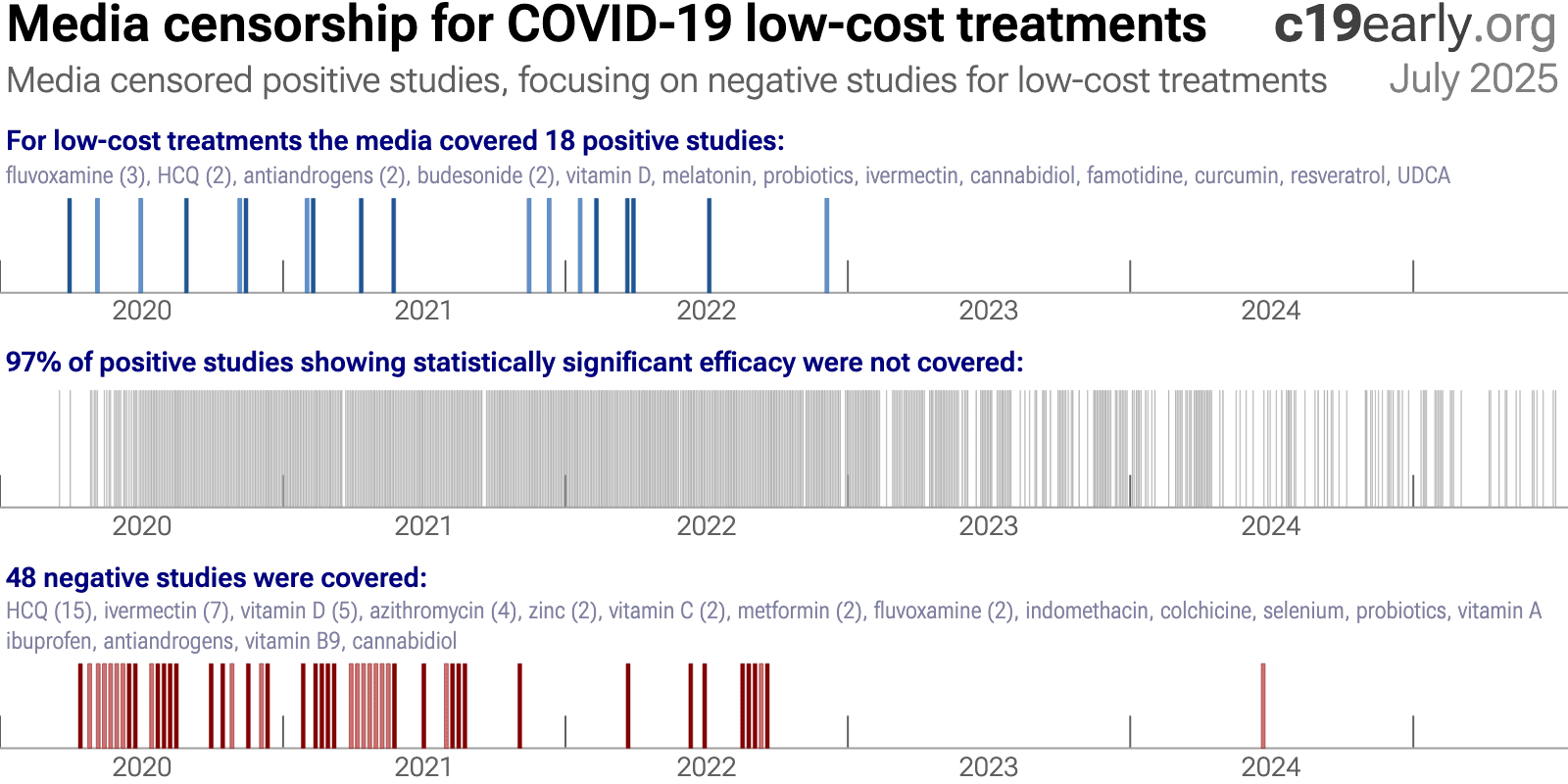
Low-cost treatments were subject to bias and censorship during the pandemic.
Scientific bias is seen in the design, analysis, presentation, and selective
reporting of studies, which often favored negative results. A similar bias is seen in the media
coverage for low-cost treatments.
While broadly seen, bias was particularly notable for ivermectin and hydroxychloroquine, e.g., Scott Alexander noted that "if you say anything in favor of ivermectin you will be cast out of civilization and thrown into the circle of social hell reserved for Klan members and 1/6 insurrectionists. All the health officials in the world will shout 'horse dewormer!' at you and compare you to Josef Mengele."46.
We analyze media coverage for the 226 treatments we cover using
Altmetric69, which reports the number of ~12,000 tracked news outlets that covered each study70. Studies are considered to have received significant media coverage if they were covered by at least 0.5% of the tracked news outlets.
Fig. 15 and 16 show the bias toward negative results for low-cost treatments, in contrast to the opposite bias for high-profit treatments.
This may result in widespread incorrect perceptions on the relative efficacy of high-profit and low-cost treatments. The impact is significant—increased cost limits the use of high-profit
treatments and treatment equity, and high-profit treatments were also more difficult to access, especially for earlier treatment which improves efficacy and minimizes community transmission.
The mainstream media did not cover any of the positive studies for chlorhexidine.
{kind=link}
Fig. 15. Mainstream media was biased against positive results for low-cost treatments.
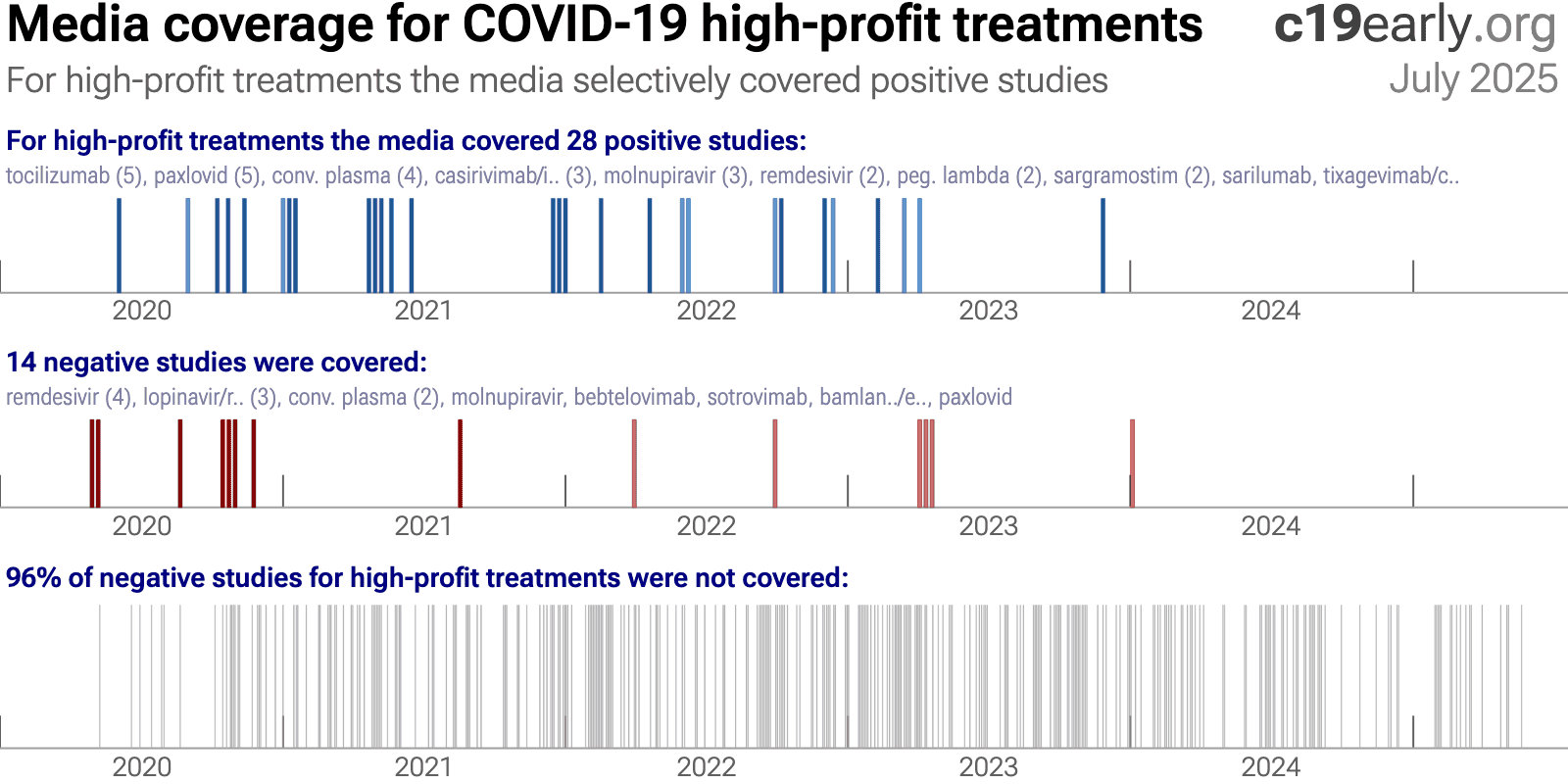{kind=link}
Fig. 16. In contrast to the results for low-cost treatments, mainstream media was biased towards positive results for high-cost treatments.
A combination of factors may have led to the media's suppression of low-cost treatments:
•
Politicization
led to a media environment where coverage was often framed to support a political
narrative rather than to provide objective scientific information. As Scott Alexander
said: "if you say anything in favor of ivermectin you will be cast out
of civilization and thrown into the circle of social hell reserved for Klan members and
1/6 insurrectionists. All the health officials in the world will shout 'horse dewormer!'
at you and compare you to Josef Mengele."
There was strong social pressure to
discredit low-cost treatments.•
Censorship
of
information conflicting with selected authorities. For example, individuals and
organizations presenting conflicting science were often banned on Twitter and
YouTube.•
FDA requires "no
adequate, approved, and available alternatives"
in order to grant an EUA for
novel high-profit interventions, creating a strong incentive for authorities to ignore or
downplay existing low-cost treatments.•
Regulatory
capture
biases authorities towards high-profit interventions.•
Authorities ignored
most evidence for low-cost treatments
, for example the NIH references only 2% of
studies in delayed, rarely-updated, biased commentaries with no quantitive analysis.•
Media coverage of
science is often not very accurate
, e.g., misunderstanding confounding issues. For
example the media widely considered the RECOVERY HCQ RCT to be conclusive on efficacy, but
very late treatment of late stage patients (mostly on oxygen already) with an excessive
toxic dose (shown dangerous in a dose comparison RCT) provides no information on the
recommended early/prophylactic treatment. With difficulting in understanding basic
confounders like treatment delay and dose, the media may favor deferring to authorities.
Many studies for low-cost treatments require greater expertise to analyze. Relatively few
journalists have a strong ability to analyze clinical trials and are outnumbered by the
rest.•
Substantial funding
from pharmaceutical advertising
biases editorial decisions towards high-profit
interventions.•
PR power
-
companies/teams with strong PR presence are favored in the media, which correlates with
high-profit and high conflict of interest studies.•
The media was very
negative in general
, inflating risk, fear, and anxieties. A negative bias may
improve ratings and revenue, increasing motivation to continue watching coverage. A
combination of low-cost treatments greatly reducing risk conflicts with the negative
narrative.25 low-cost treatments were approved in one
or more countries, yet many countries approved no low-cost treatments.
The countries that did adopt low-cost treatments analyzed the evidence early and made
timely approvals. With few exceptions, authorities did not change their initial views,
regardless of how much evidence accumulated showing either efficacy or harm. Why?
The harms of smoking here hidden for 25 yearsC. Authorities did not analyze the data in real-time, failing to act when
harm was known.
Widespread acknowledgement of harm came only after attempts by two new surgeon generals,
along with pressure from health advocates and a new president, and a review of 7,000 studies.
Similarly for COVID-19, most authorities and experts did not proactively
analyze data in real-time. This guarantees delayed recognition of efficacy or harm, by
which time moral, legal, career, and reputational liabilities strongly disincentivize any
admission of error. Claims of no efficacy (for effective treatments) or safety (for
harmful treatments) were often made prior to strong data being available. Correction
would require admitting to errors that increased mortality, which is unlikely with the
same generation of officials.
Analysis of potential treatments was rarely done, and when done these were
typically minimal efforts.
For example, NIH reviews were highly delayed, cover only a tiny fraction of treatments,
reference only 2% of studies for the treatments covered, and include no
quantitative analysis.
They appear as rarely updated side projects from
external panels implicitly tasked with justifying prior failures.
As with smoking, the thousands of studies could (and should)
have been analyzed and acted on in real-time.
A key structural improvement, applicable to all current and future
diseases, is for authorities to implement real-time proactive analysis of clinical
evidence. This does not remove all bias, but does make it possible to act on evidence,
whereas delayed action may be unlikely due to moral, legal, career, and reputational
liabilities.
c19early.org
Delayed public health acknowledgments
Official acknowledgment of efficacy or harm is often delayed—legal, career, and status risks disincentivize admission of error.
| Evidence | Official Acknowledgment | Approx. Delay | |
|---|---|---|---|
| Citrus Fruit (vitamin C) for Scurvy (effectiveness) | 1747: James Lind conducted one of the first-ever controlled clinical trials, proving that oranges and lemons cured scurvy in sailors. | 1795: The British Royal Navy finally made a daily ration of lemon juice a standard issue for all its sailors, effectively eliminating the disease. | 48 years |
| Handwashing (lower mortality) | 1847: Dr. Ignaz Semmelweis provided conclusive proof that having doctors wash their hands with a chlorine solution before delivering babies reduced maternal mortality rates from over 18% to around 1%. | ~1870s: Semmelweis's findings were rejected and he was ridiculed. His work was only validated decades later (after his death). | ~20+ years |
| Helicobacter pylori (bacteria causes ulcers) | 1982-1984: Marshall and Warren discovered that Helicobacter pylori bacteria causes ulcers, confirmed via direct exposure. Officials maintained that ulcers were caused by stress and spicy food. | 1994: The US NIH released a consensus statement officially recommending antibiotics as the standard treatment for peptic ulcers, overturning decades of acid-suppression therapy. | ~12 years |
| Asbestos (causes asbestosis & cancer) | 1924: The British Medical Journal published the first case study of a death from "asbestosis." By 1918, U.S. insurance companies had stopped selling life insurance to asbestos workers. | 1971 (US): The Occupational Safety and Health Administration (OSHA) was formed and began regulating asbestos as a carcinogen, setting the first federal workplace safety standards for it. | ~47 years |
| Leaded Gasoline (neurotoxicity) | ~1924: Dangers of low-level lead exposure were known. Experts like Alice Hamilton warned the U.S. Surgeon General that adding lead to gasoline would cause widespread public poisoning. | 1973 (US): The Environmental Protection Agency (EPA) ordered the first phasedown of lead in gasoline, following the Clean Air Act of 1970. A full ban for on-road vehicles took effect in 1996. | ~49 years |
| Harms of Smoking (causes lung cancer) | 1939: Franz Müller (Germany) published the first case-control epidemiological study strongly linking tobacco smoking to lung cancer. This was followed by major U.S. & U.K. studies in the 1950s. | 1964 (US): The U.S. Surgeon General's report, "Smoking and Health," was released. It was the first U.S. government report to definitively link smoking to lung cancer and heart disease. | 25 years |
Heterogeneity in COVID-19 studies arises from many factors including:
The time between infection or the onset of symptoms and
treatment may critically affect how well a treatment works. For example an
antiviral may be very effective when used early but may not be effective in
late stage disease, and may even be harmful. Oseltamivir, for example, is
generally only considered effective for influenza when used within 0-36 or
0-48 hours71,72. Baloxavir marboxil studies for influenza
also show that treatment delay is critical — Ikematsu et al. report
an 86% reduction in cases for post-exposure prophylaxis, Hayden et al.
show a 33 hour reduction in the time to alleviation of symptoms for treatment
within 24 hours and a reduction of 13 hours for treatment within 24-48 hours,
and Kumar et al. report only 2.5 hours improvement for inpatient
treatment.
| Treatment delay | Result |
| Post-exposure prophylaxis | 86% fewer cases73 |
| <24 hours | -33 hours symptoms74 |
| 24-48 hours | -13 hours symptoms74 |
| Inpatients | -2.5 hours to improvement75 |
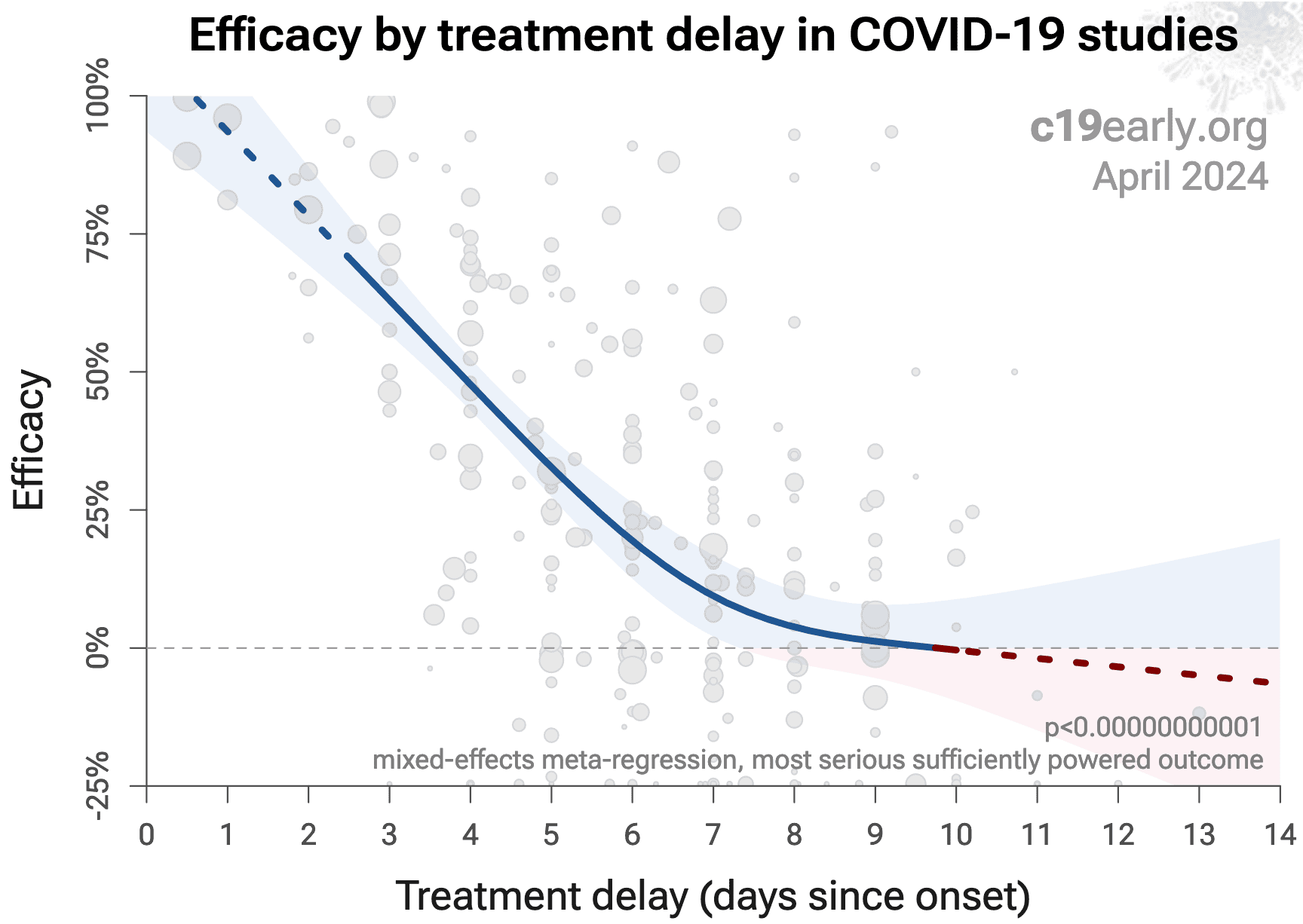
Fig. 17 shows a mixed-effects meta-regression for
efficacy as a function of treatment delay in COVID-19 studies from 226 treatments, showing that efficacy
declines rapidly with treatment delay. Early treatment is critical for COVID-19.
{kind=link}
Fig. 17. Early treatment is more effective. Meta-regression showing efficacy as a function of treatment delay in COVID-19 studies from 226 treatments.
Details of the patient population including age and comorbidities may
critically affect how well a treatment works. For example, many COVID-19
studies with relatively young low-comorbidity patients show all patients
recovering quickly with or without treatment. In such cases, there is little
room for an effective treatment to improve results, for example as in
López-Medina et al.
Efficacy may depend critically on the distribution of
SARS-CoV-2 variants encountered by patients. Risk varies significantly across
variants77, for example the Gamma variant shows significantly
different characteristics78-81. Different
mechanisms of action may be more or less effective depending on variants, for
example the degree to which TMPRSS2 contributes to viral entry can differ
across variants82,83.
Effectiveness may depend strongly on the dosage and treatment regimen.
The quality of medications may vary significantly between
manufacturers and production batches, which may significantly affect efficacy
and safety. Williams et al. analyze ivermectin from 11 different sources,
showing highly variable antiparasitic efficacy across different manufacturers.
Xu et al. analyze a treatment from two different manufacturers, showing 9
different impurities, with significantly different concentrations for each
manufacturer.
Across all
studies there is a strong association between different outcomes, for example
improved recovery is strongly associated with lower mortality. However,
efficacy may differ depending on the effect measured, for example a treatment
may be more effective against secondary complications and have minimal effect
on viral clearance.
The
distribution of studies will alter the outcome of a meta-analysis. Consider a
simplified example where everything is equal except for the treatment delay,
and effectiveness decreases to zero or below with increasing delay. If there
are many studies using very late treatment, the outcome may be negative, even
though early treatment is very effective.
All meta-analyses combine heterogeneous studies, varying in population,
variants, and potentially all factors above, and therefore may obscure
efficacy by including studies where treatment is less effective. Generally, we
expect the estimated effect size from meta-analysis to be less than that for
the optimal case.
Looking at all studies is valuable for providing an overview of all research,
important to avoid cherry-picking, and informative when a positive result is
found despite combining less-optimal situations. However, the resulting
estimate does not apply to specific cases such as
early treatment in high-risk populations.
While we present results for all studies, we also present treatment time and
individual outcome analyses, which may be more informative for specific use
cases.
This section validates the use of pooled effects for COVID-19, which enables
earlier detection of efficacy, however pooled effects are no longer required
for chlorhexidine as of April 2025. Efficacy is now known based on specific outcomes. Efficacy based on specific outcomes was delayed by 17.3 months compared to using pooled outcomes.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes" is not a good reason for
disregarding results.
Pooling the results of studies reporting different outcomes allows us to use
more of the available information. Logically we should, and do, use additional
information when evaluating treatments—for example dose-response and
treatment delay-response relationships provide additional evidence of efficacy
that is considered when reviewing the evidence for a treatment.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster and safer collection of evidence.
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 226
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
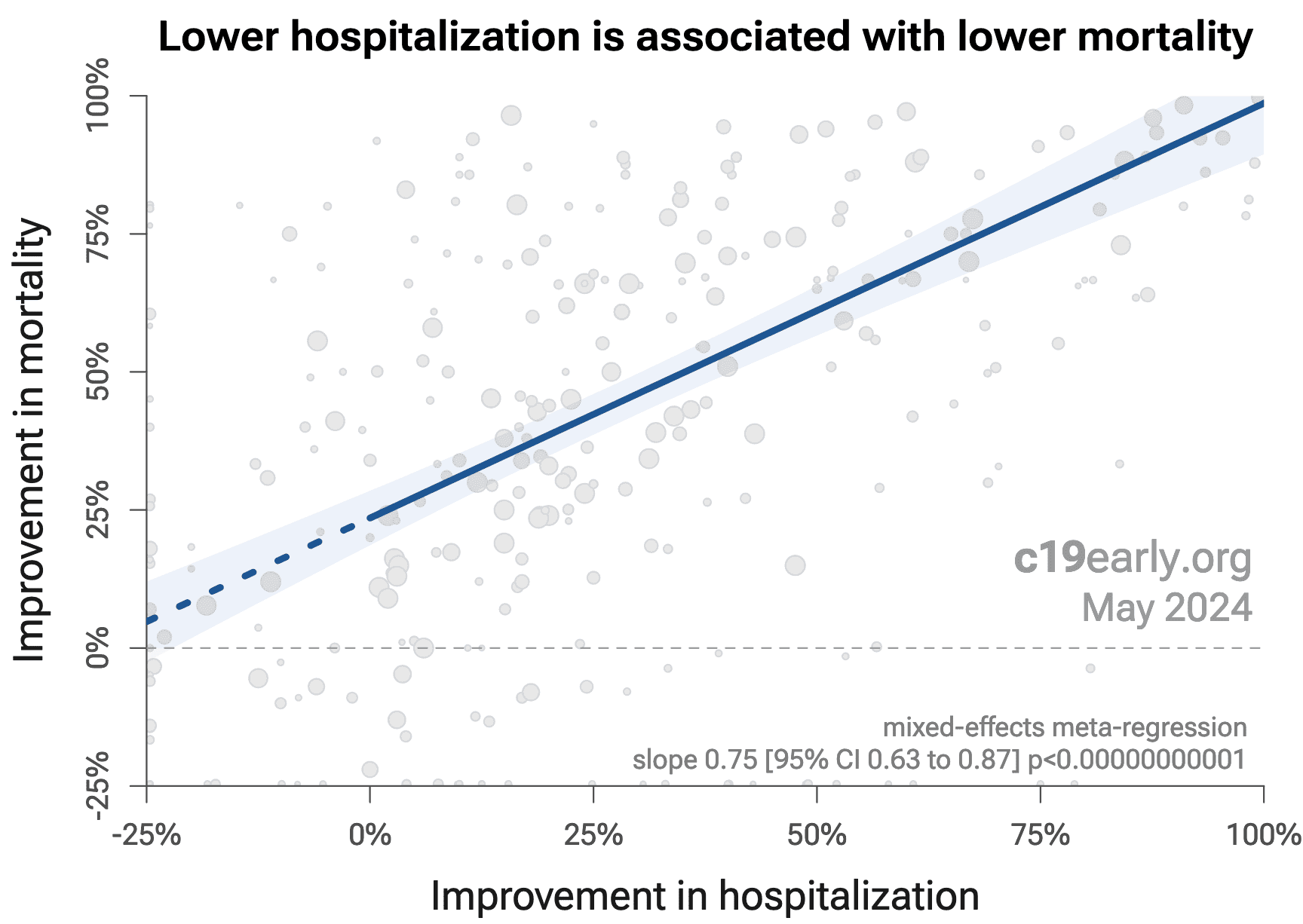
Fig. 18 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
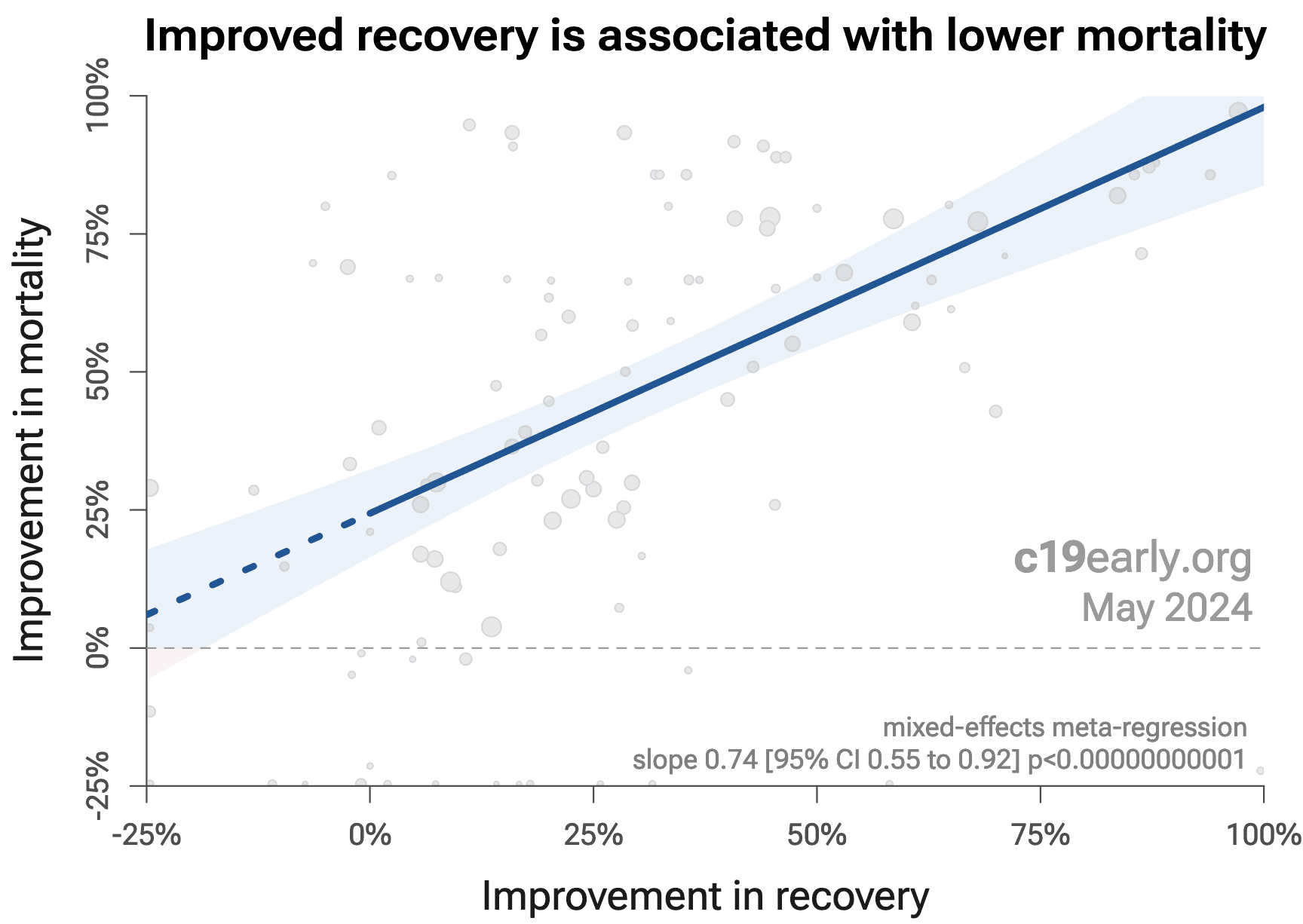
Similarly, Fig. 19 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
Considering the extremes, Singh et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
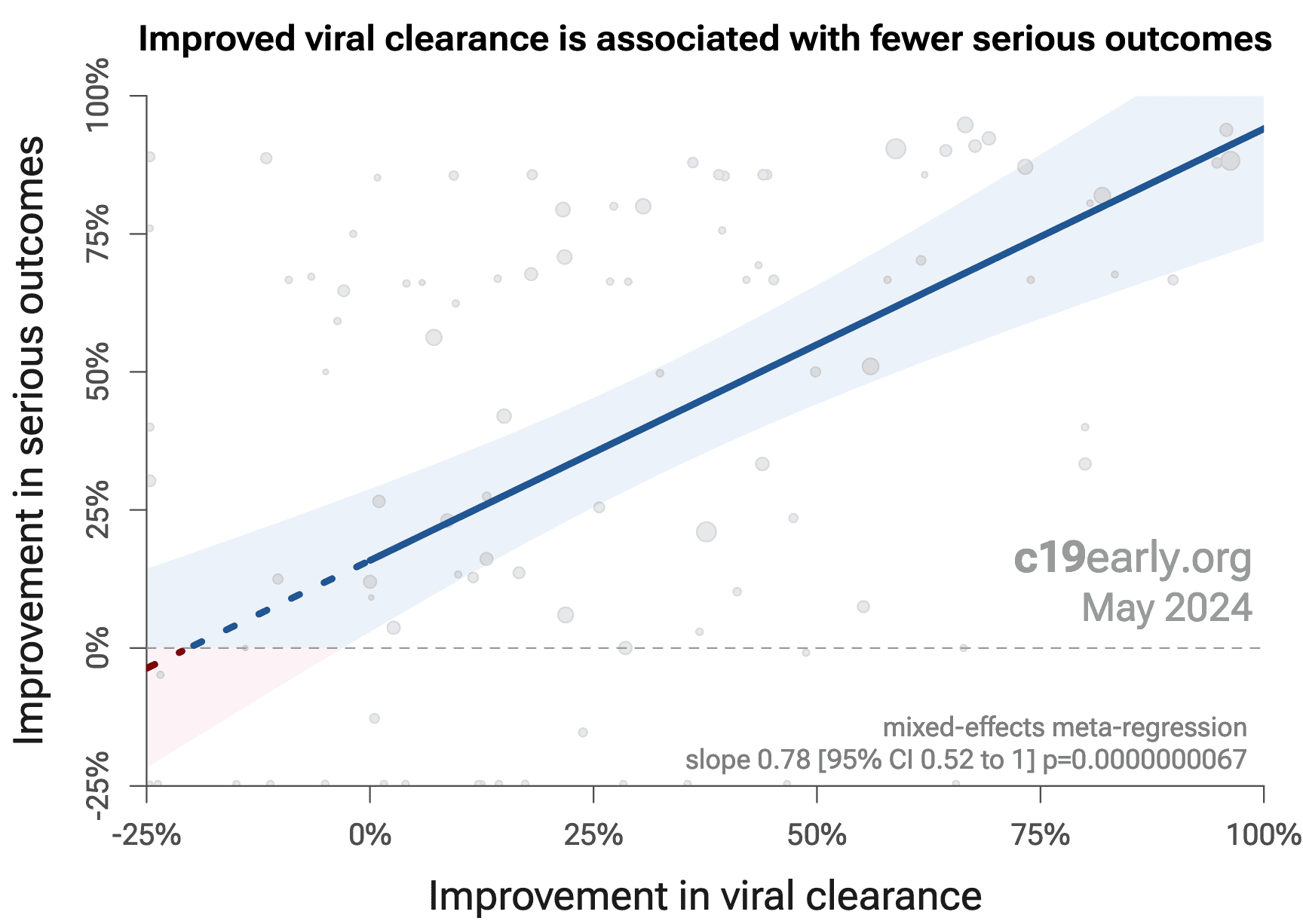
Fig. 20 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh et al., with higher confidence due to the larger number of
studies. As with Singh et al., the confidence increases
when excluding the outlier treatment, from p = 0.000000011 to p = 0.00000000032.
{kind=link}
Fig. 18. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Fig. 19. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Fig. 18. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
Currently, 59 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 85% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.6 months. When restricting to RCTs only, 53% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 7.4 months.
Fig. 21 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
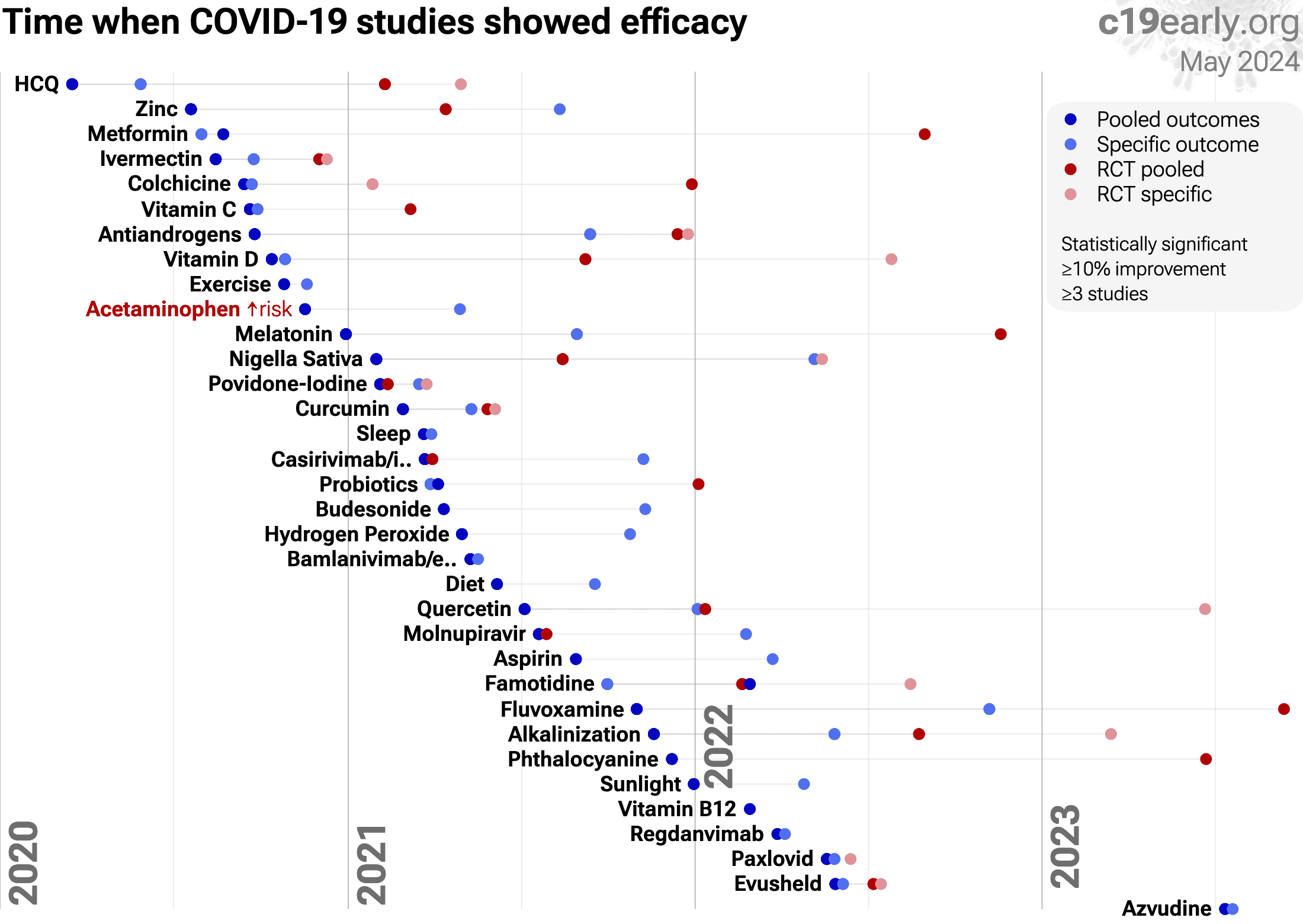{kind=link}
Fig. 21. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as differences in treatment delay are more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta-analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
Analysis of short-term changes in viral load using PCR may not detect
effective treatments because PCR is unable to differentiate between intact
infectious virus and non-infectious or destroyed virus particles. For example
Tarragó-Gil, Alemany perform RCTs with cetylpyridinium chloride
(CPC) mouthwash that show no difference in PCR viral load, however there was
significantly increased detection of SARS-CoV-2 nucleocapsid protein,
indicating viral lysis. CPC inactivates SARS-CoV-2 by degrading its membrane,
exposing the nucleocapsid of the virus. To better estimate changes in viral
load and infectivity, methods like viral culture that can
differentiate intact vs. degraded virus are preferred.
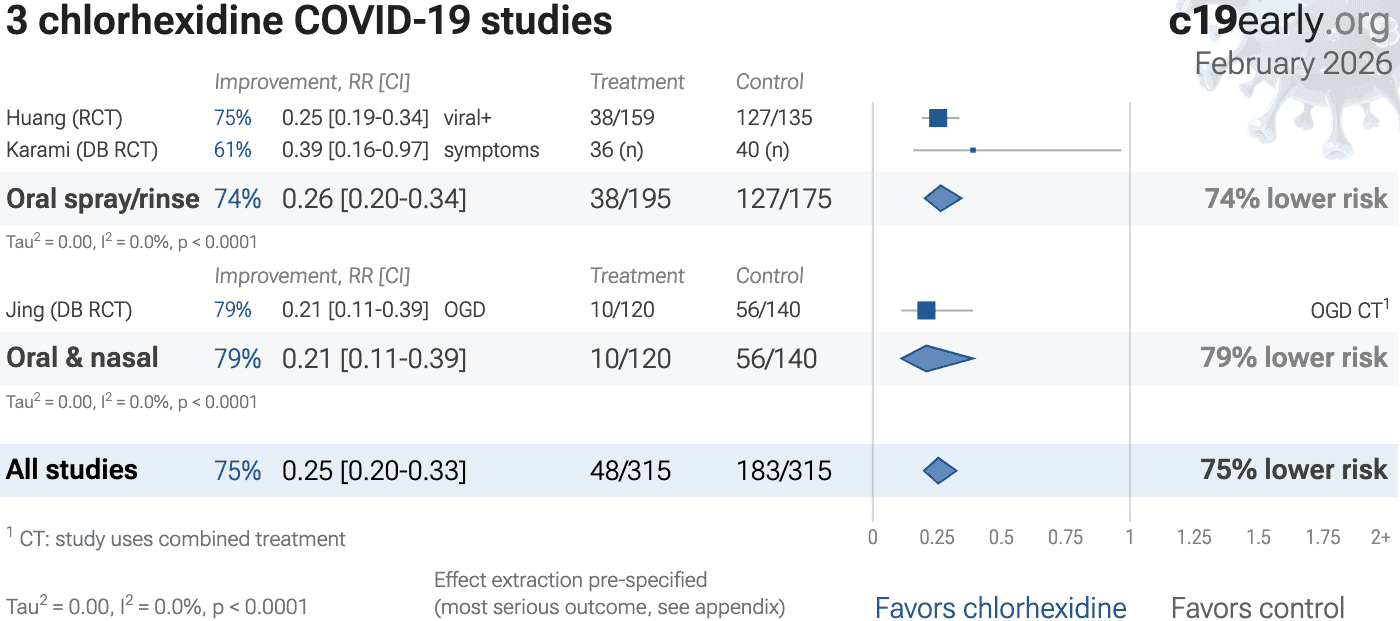
Studies to date use a variety of administration methods to the
respiratory tract, including nasal and oral sprays, nasal irrigation, oral
rinses, and inhalation. Table 4 shows the relative efficacy for
nasal, oral, and combined administration. Combined administration shows the
best results, and nasal administration is more effective than oral. Precise
efficacy depends on the details of administration, e.g., mucoadhesion and
sprayability for sprays.

c19early.org
Combined nasal and oral administration is most effective
Across all nasopharyngeal/oropharyngeal treatments we cover, combined nasal and oral administration shows the highest efficacy, followed by nasal administration, with oral administration alone showing the lowest efficacy.
| Administration | Improvement | Studies |
|---|---|---|
| Nasal & oral | 88% [72‑95%] | 10 |
| Nasal spray/rinse | 59% [50‑66%] | 21 |
| Oral spray/rinse | 38% [25‑49%] | 11 |
Table 4. Respiratory tract administration efficacy. Relative efficacy of nasal, oral, and combined nasal/oral administration for treatments administered directly to the respiratory tract. Results show random-effects meta-analysis for the most serious outcome reported for all prophylaxis and early treatment studies.
Nasopharyngeal/oropharyngeal treatments work via different methods.
Some are drugs with other primary uses and have a greater potential for side effects and drug interactions, for example azelastine and chlorpheniramine are antihistamines. Table 5 summarizes the primary classes of mechanisms of action, and Table 6 shows mechanisms of action for specific treatments.
c19early.org
Nasal/oral sprays and rinses—primary mechanisms
Primary mechanisms of action for nasopharyngeal/oropharyngeal sprays and rinses. Note: sequenced application is possible to maximize efficacy—for example, using a virucidal spray/wash first (to clean), followed by a barrier spray (to protect), with a 5-10 minute drying window in between.
| Virucidal action | Chemically inactivating or destroying the structure of viral particles |
| Blocking attachment | Binding to the virus or host cells to prevent viral attachment to host cells |
| Physical barrier | Forming a physical layer over the nasal mucosa preventing viral access to host cells |
| Physical removal | Mechanical washout/flushing of viral particles and mucus (e.g., large volume irrigation) |
| Mucociliary clearance | Stimulating the natural beating of nasal cilia to accelerate the clearing of trapped pathogens |
Table 5. Primary classes for mechanisms of action for nasopharyngeal/oropharyngeal treatments.
c19early.org
Nasal/oral sprays and rinses—mechanisms of action
Nasopharyngeal/oropharyngeal treatments have many different mechanisms of action. Specific treatments may have significant systemic effects or significantly alter the microbiome.
| Treatment | Mechanisms | Notes |
|---|---|---|
| Azelastine112 |
Antiviral: inhibits interaction between spike protein and ACE2 Antiviral: potential inhibition of viral protease (Mpro) Other: H1-receptor antagonist (antihistamine) Other: mast cell stabilizer |
Antihistamine. Designed to affect human receptors. Risks include dysgeusia, drowsiness, and nasal burning. |
| Cetylpyridinium Chloride113 |
Virucidal: disrupts viral lipid envelope Antiseptic: quaternary ammonium compound |
Chemical virucide. Common in mouthwashes. Can cause temporary staining of teeth or tongue irritation if used frequently. |
| Chlorhexidine |
Virucidal: disrupts viral lipid membranes Antiseptic: cationic polybiguanide |
Chemical virucide. May cause tooth staining and altered taste. |
| Chlorpheniramine114 |
Antiviral: binds to viral spike protein to block entry Antiviral: high affinity for viral transport proteins Other: H1-receptor antagonist (1st generation antihistamine) Other: anticholinergic activity |
Antihistamine. Stronger systemic risks than azelastine. Known to cause significant sedation/drowsiness and cognitive impairment. |
| Hydrogen Peroxide115 |
Virucidal: oxidizing agent that destroys viral parts Other: tissue debridement |
Chemical virucide. Can be toxic to healthy tissue if concentration is too high (>1%). Long-term safety on nasal mucosa is debated. |
| Inhaled Heparin116 |
Antiviral: acts as a decoy receptor (mimics heparan sulfate) Antiviral: anti-inflammatory effects on lung tissue Other: Anticoagulant |
Anticoagulant. Use requires caution regarding bleeding risks. |
| Iota-carrageenan117 |
Barrier: forms a viscous physical layer on mucosa Trap: electrostatistically traps virus particles (mimics cell surface) |
Physical barrier. High safety profile for daily use. |
| NaCl118 |
Cleaning: physically washes away viral particles Support: moisturizes mucosa to support natural immune barrier |
Physical wash. High degree of safety, reduces viral load via physical removal. |
| Nitric Oxide119 |
Virucidal: physically damages viral structure via nitrosylation Other: vasodilator (relaxes blood vessels) in systemic use |
Virucide/drug hybrid. In nasal spray form, it acts primarily as a topical disinfectant. Rapidly cleared, so systemic vasodilation risks are low but present. |
| Phthalocyanine120 |
Virucidal: generates reactive oxygen species (ROS) when exposed to light to kill virus Other: photosensitizer |
Chemical virucide. A synthetic compound often used in photodynamic therapy. Works by creating an oxidative environment hostile to the virus. |
| Povidone-Iodine121 |
Virucidal: oxidizes viral proteins and destabilizes membrane structures Antiseptic: broad-spectrum bacterial/fungal killer |
Chemical virucide. Highly effective but risk of thyroid absorption with chronic use. Can be irritating to mucous membranes. |
| Sodium Bicarbonate122 |
Environment: raises pH to inhibit viral fusion Cleaning: improves mucociliary clearance (washing) |
Physical/chemical environment. Changes the environment rather than attacking the virus directly. High degree of safety. |
Table 6. Mechanisms of action for nasopharyngeal/oropharyngeal treatments.
Nasopharyngeal/oropharyngeal treatments may not be highly selective. In
addition to inhibiting or disabling SARS-CoV-2, they may also be harmful to
beneficial microbes, disrupting the natural microbiome in the oral cavity and
nasal passages that have important protective and metabolic roles123,124. This may be
especially important for prolonged use or overuse.
Table 7 summarizes the potential for common
nasopharyngeal/oropharyngeal treatments to affect the natural
microbiome.
c19early.org
Nasal/oral sprays and rinses may affect the microbiome
Nasopharyngeal/oropharyngeal treatments may significantly alter the microbiome. These effects may be more important with longer-term prophylaxis.
| Treatment | Microbiome disruption potential | Notes |
|---|---|---|
| Iota-carrageenan117 | Low | Primarily antiviral, however extended use may mildly affect the microbiome |
| Nitric Oxide119 | Low to moderate | More selective towards pathogens, however excessive concentrations or prolonged use may disrupt the balance of bacteria |
| Alkalinization125 | Moderate | Increases pH, negatively impacting beneficial microbes that thrive in a slightly acidic environment |
| Cetylpyridinium Chloride113 | Moderate | Quaternary ammonium broad-spectrum antiseptic that can disrupt beneficial and harmful bacteria |
| Phthalocyanine120 | Moderate to high | Photodynamic compound with antimicrobial activity, likely to affect the microbiome |
| Chlorhexidine | High | Potent antiseptic with broad activity, significantly disrupts the microbiome |
| Hydrogen Peroxide115 | High | Strong oxidizer, harming both beneficial and harmful microbes |
| Povidone-Iodine121 | High | Potent broad-spectrum antiseptic harmful to beneficial microbes |
Table 7. Potential effect of nasopharyngeal/oropharyngeal treatments on the microbiome.
Publishing is often biased
towards positive results, however evidence suggests that there may be a negative bias for
inexpensive treatments for COVID-19. Both negative and positive results are
very important for COVID-19, media in many countries prioritizes negative
results for inexpensive treatments (inverting the typical incentive for
scientists that value media recognition), and there are many reports of
difficulty publishing positive results126-129.
For chlorhexidine, there is currently not
enough data to evaluate publication bias with high confidence.
Pharmaceutical drug
trials often have conflicts of interest whereby sponsors or trial staff have a
financial interest in the outcome being positive. Chlorhexidine for COVID-19
lacks this because it is off-patent, has multiple manufacturers, and is very low cost.
In contrast, most COVID-19 chlorhexidine trials have been run by
physicians on the front lines with the primary goal of finding the best
methods to save human lives and minimize the collateral damage caused by
COVID-19. While pharmaceutical companies are careful to run trials under
optimal conditions (for example, restricting patients to those most likely to
benefit, only including patients that can be treated soon after onset when
necessary, and ensuring accurate dosing), not all chlorhexidine trials
represent the optimal conditions for efficacy.
Summary statistics from
meta-analysis necessarily lose information. As with all meta-analyses, studies
are heterogeneous, with differences
in treatment delay, treatment regimen, patient demographics, variants,
conflicts of interest, standard of care, and other factors. We provide analyses for specific
outcomes and by treatment delay, and we aim to identify key characteristics in
the forest plots and summaries. Results should be viewed in the context of
study characteristics.
Some analyses classify treatment based on early or late
administration, as done here, while others distinguish between mild, moderate,
and severe cases. Viral load does not indicate degree of symptoms — for
example patients may have a high viral load while being asymptomatic. With
regard to treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.
Details of treatment delay per patient is often not available.
For example, a study may treat 90% of patients relatively early, but the
events driving the outcome may come from 10% of patients treated very late.
Our 5 day cutoff for early treatment may be too conservative, 5 days may be too late in many cases.
Comparison across treatments is confounded by differences in
the studies performed, for example dose, variants, and conflicts of interest.
Trials with conflicts of interest may use designs better suited to the
preferred outcome.
In some cases, the most serious outcome has very few events,
resulting in lower confidence results being used in pooled analysis, however
the method is simpler and more transparent. This is less critical as the
number of studies increases. Restriction to outcomes with sufficient power may
be beneficial in pooled analysis and improve accuracy when there are few
studies, however we maintain our pre-specified method to avoid any
retrospective changes.
Studies show that combinations of treatments can be highly
synergistic and may result in many times greater efficacy than individual
treatments alone86-108.
Therefore standard of care may be critical and benefits may diminish or
disappear if standard of care does not include certain treatments.
This real-time analysis is constantly updated based on
submissions. Accuracy benefits from widespread review and submission of
updates and corrections from reviewers. Less popular treatments may receive
fewer reviews.
No treatment or intervention is 100% available and
effective for all current and future variants. Efficacy may vary significantly
with different variants and within different populations. All treatments have
potential side effects. Propensity to experience side effects may be predicted
in advance by qualified physicians. We do not provide medical advice. Before
taking any medication, consult a qualified physician who can compare all
options, provide personalized advice, and provide details of risks and
benefits based on individual medical history and situations.
2 of 5 studies
combine treatments. The results of
chlorhexidine
alone may differ.
2 of 4 RCTs use combined treatment.
Currently all studies are peer-reviewed.
Seijas-Otero et al. present another meta-analysis for chlorhexidine, showing significant improvement for viral load.
SARS-CoV-2 infection and replication involves a complex
interplay of 500+ host and viral proteins and other
factors36-43, providing many therapeutic
targets.
Over 11,000 compounds have been predicted to reduce COVID-19
risk44, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
Fig. 22 shows an overview of the results for chlorhexidine
in the context of multiple COVID-19 treatments, and Fig. 23 shows a plot
of efficacy vs. cost for COVID-19 treatments.
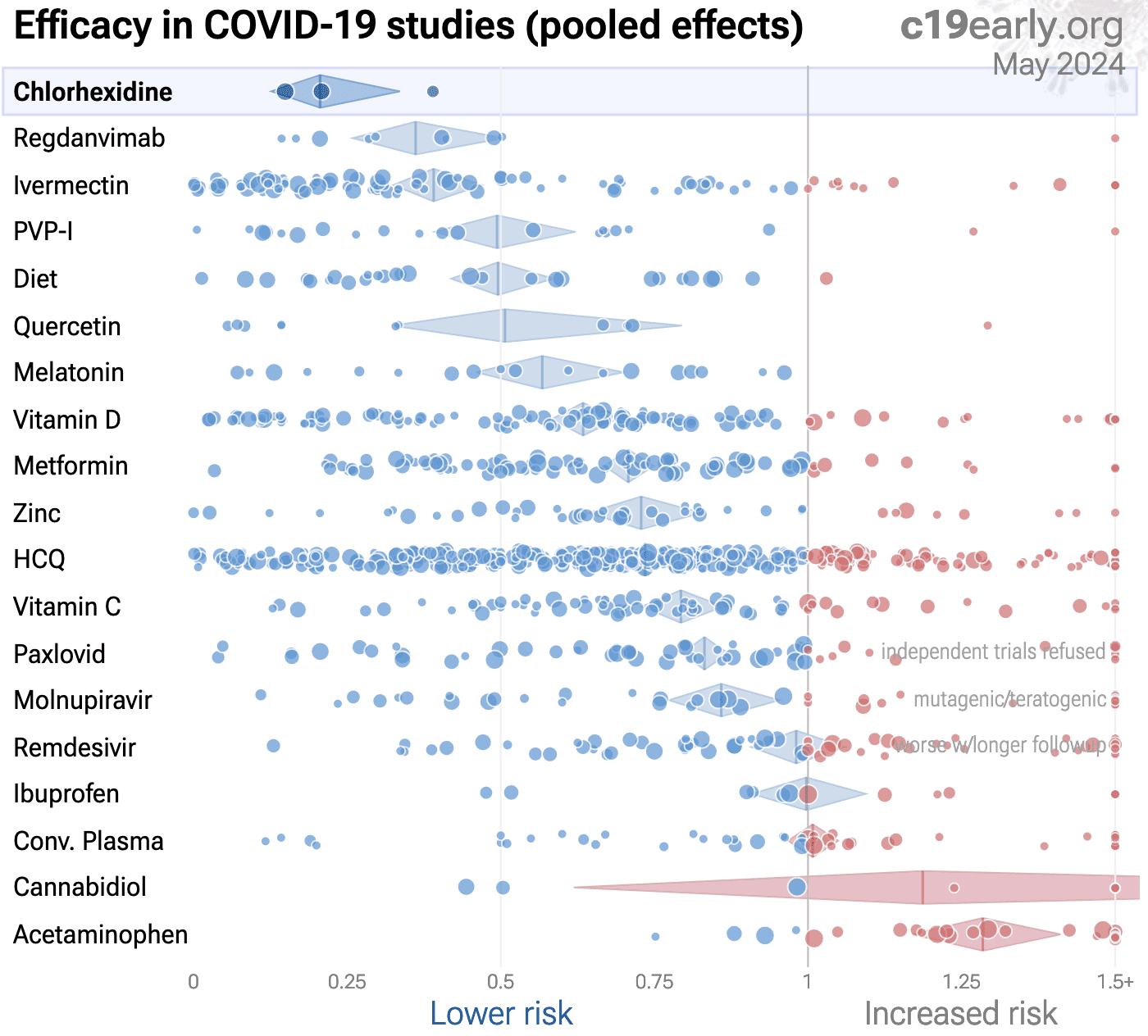{kind=link}
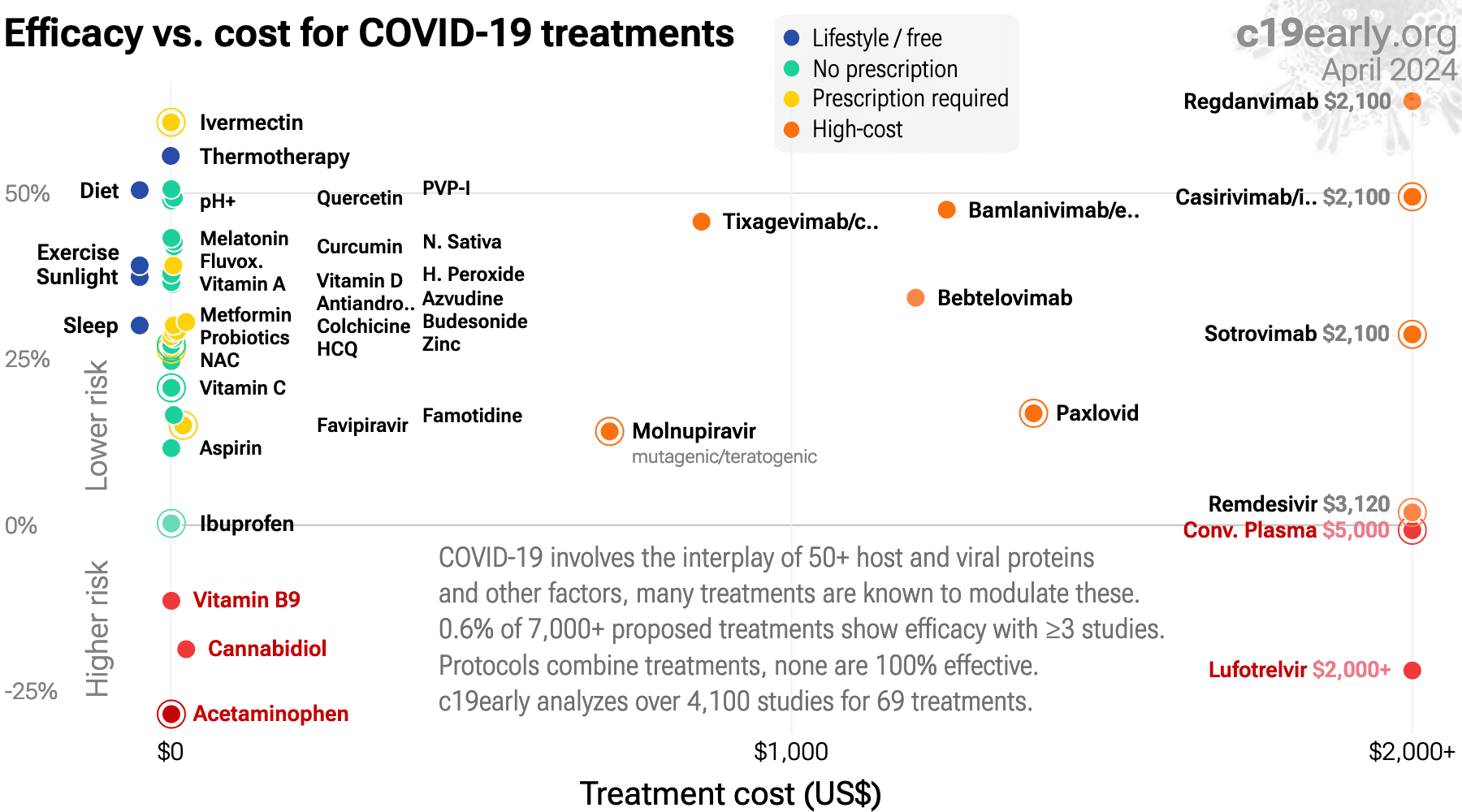{kind=link}
Fig. 23. Efficacy vs. cost for COVID-19 treatments.
SARS-CoV-2 infection typically starts in the upper respiratory tract.
Progression may lead to cytokine storm, pneumonia, ARDS, neurological issues,
organ failure, and death. Stopping replication in the upper respiratory tract,
via early or prophylactic nasopharyngeal/oropharyngeal treatment, can avoid
the consequences of progression to other tissues, and avoid the requirement
for systemic treatments with greater potential for side effects.
Studies to date show that chlorhexidine is
an effective treatment for COVID-19.
Significantly lower risk is seen for progression, cases, and viral clearance. 4 studies from 4 independent teams in 4 countries show significant
benefit.
Meta-analysis using the most serious outcome reported shows
70% [58‑79%] lower risk. Results are similar for Randomized Controlled Trials.
Currently there is limited data, with only 675 patients in trials to date.
Seijas-Otero et al. present another meta-analysis for chlorhexidine, showing significant improvement for viral load.
Chlorhexidine may be detrimental to the natural microbiome, raising concern for side effects, especially with prolonged or excessive use.
Contact.
Contact us on X at @CovidAnalysis.
Funding.
We have received no funding or
compensation in any form, and do not accept donations. This is entirely volunteer work.
Conflicts of interest.
We have no conflicts of interest.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.AI.
We use AI models (Gemini, Grok, Claude, and
ChatGPT) tasked with functioning as additional peer-reviewers to check for errors, suggest
improvements, and review spelling and grammar. Any corrections are verified and applied
manually. Our preference for em dashes is independent of AI.Updates.
Our COVID-19 meta-analyses involve the extraction of over 226,000
datapoints from thousands of papers for 226 treatments. We thank the
thousands of scientists, physicians, and other contributors that have provided updates,
suggestions, feedback, and corrections. These are all welcome and can be submitted
at https://c19early.org/chxmeta.html.
Dedication.
This work is dedicated to top
evidence-based physicians that worked tirelessly to analyze evidence and greatly reduce
mortality and morbidity during the pandemic. In alphabetical order:
Dr. Thomas J. Borody, Dr. Mary Talley Bowden, Dr. Flavio Cadegiani, Dr. Shankara Chetty,
Dr. Ryan Cole, Dr. George Fareed, Dr. Sabine Hazan, Dr. Pierre Kory, Dr. Tess Lawrie, Dr.
Robert Malone, Dr. Paul Marik, Dr. Peter McCullough, Dr. Didier Raoult, Dr. Harvey Risch,
Dr. Jackie Stone, Dr. Brian Tyson, Dr. Joseph Varon, and Dr. Vladimir (Zev) Zelenko.
Public domain.
This is a public domain work
distributed in accordance with the Creative Commons CC0 1.0 Universal license, which
dedicates the work to the public domain by waiving all rights worldwide under copyright law.
You can distribute, remix, adapt, and build upon this work in any medium or format,
including for commercial purposes, without asking permission. Referenced material and
third-party images retain any original copyrights or restrictions.
See: https://creativecommons.org/publicdomain/zero/1.0/.
{kind=link}
RCT 61 COVID+ patients showing improved reduction in viral infectivity with a mouthwash containing 0.05% cetylpyridinium chloride (CPC) and 0.05% chlorhexidine digluconate (CHX), compared to 0.9% NaCl. The study only analyzes short-term changes in viral load 30 minutes after treatment.
{kind=link}
RCT 294 hospitalized patients in the USA, showing faster oropharyngeal viral clearance with chlorhexidine. Results were better with a combination of oropharyngeal rinse and posterior oropharyngeal spray compared with the rinse alone.
{kind=link}
RCT 379 mild COVID-19 cases showing significantly lower prevalence and severity of olfactory and gustatory dysfunction with budesonide nasal spray, chlorhexidine mouthwash, and saline nasal irrigation. The control group received no intervention, the saline group received saline nasal irrigation plus saline nasal spray and mouthwash, and the drug group received saline nasal irrigation plus budesonide nasal spray and chlorhexidine mouthwash. Saline nasal irrigation plus nasal spray and mouthwash were administered once and four times daily, respectively. Both treatment groups had significantly lower prevalence and severity olfactory and gustatory dysfunction. Prevalence was lower for the drug vs. saline group, without statistical significance.
{kind=link}
RCT 116 healthcare workers comparing 0.2% chlorhexidine mouthwash (n=36), 7.5% sodium bicarbonate mouthwash (n=40), and placebo (n=40) twice daily for 2 weeks, with symptoms followed for 4 weeks. There were lower symtoms and cases in both treatment groups, with statistical significance for chlorhexidine only. The treatments were stopped after two weeks, results may be better with continued use, more frequent use, and with the addition of nasal use.
245 participant chlorhexidine + PVP-I prophylaxis RCT with results not reported over 4 years after completion.
48 patient chlorhexidine early treatment RCT with results not reported over 4 years after completion.
{kind=link}
Prospective study of 45 COVID-19 patients showing improved viral clearance with chlorhexidine gluconate and povidone-iodine mouthwash use.
Estimated 90 patient chlorhexidine early treatment RCT with results not reported over 4 years after estimated completion.
We perform ongoing searches of PubMed, medRxiv, Europe PMC, ClinicalTrials.gov, The Cochrane
Library, Google Scholar, Research Square, ScienceDirect, Oxford University Press, the
reference lists of other studies and meta-analyses, and submissions to the site c19early.org, which regularly receives notification of studies upon
publication.
Search terms are chlorhexidine and COVID-19 or SARS-CoV-2. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of chlorhexidine for COVID-19 that report a comparison with a
control group are included in the main analysis.
Studies with major unexplained data issues, for example major outcome data that is
impossible to be correct with no response from the authors, are excluded.
{kind=link}

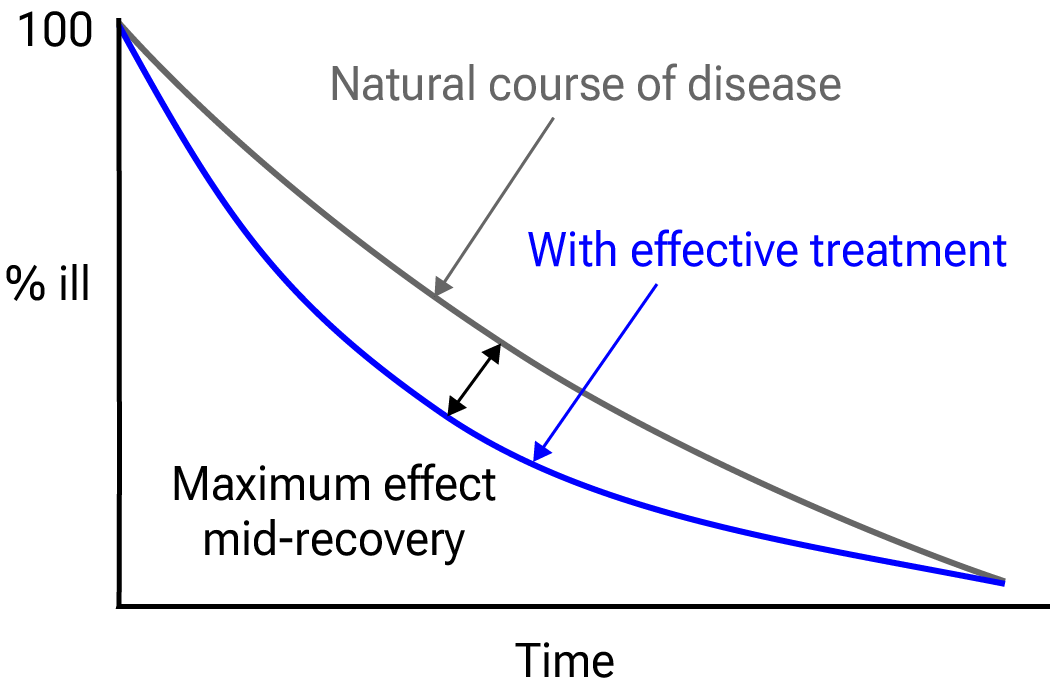
Fig. 24.
Mid-recovery results can more accurately reflect efficacy when almost all patients
recover. Mateja et al. confirm that intermediate viral load results more accurately
reflect hospitalization/death.
We extracted effect sizes and associated data from all studies. If studies report multiple
kinds of effects then the most serious outcome is used in pooled analysis, while
other outcomes are included in the outcome-specific analyses. For example, if effects for
mortality and cases are reported then they are both used in specific outcome analyses,
while mortality is used for pooled analysis.
If symptomatic results are reported at multiple times, we use the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28 days have
preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious outcome with
one or more events is used. For example, in low-risk populations with no mortality, a
reduction in mortality with treatment is not possible, however a reduction in
hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral outcomes.
When basically all patients recover in both treatment and control groups, preference for
viral clearance and recovery is given to results mid-recovery where available. After most
or all patients have recovered there is little or no room for an effective treatment to do
better, however faster recovery is valuable.
An IPD meta-analysis confirms that intermediate viral load reduction is more closely
associated with hospitalization/death than later viral load reduction145.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
Forest plots are computed using PythonMeta146 with the DerSimonian and
Laird random-effects model (the fixed effect assumption is not plausible in this case) and
inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
When results provide an odds ratio, we compute the relative risk when possible, or convert
to a relative risk according to Zhang et al.
Reported confidence intervals and p-values are used when available, and adjusted
values are used when provided. If multiple types of adjustments are reported propensity
score matching and multivariable regression has preference over propensity score matching
or weighting, which has preference over multivariable regression. Adjusted results have
preference over unadjusted results for a more serious outcome when the adjustments
significantly alter results.
When needed, conversion between reported p-values and confidence intervals followed
Altman, Altman (B), and Fisher's exact test was used to calculate
p-values for event data. If continuity correction for zero values is required, we
use the reciprocal of the opposite arm with the sum of the correction factors equal to
1150.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of a negative
outcome when applicable (for example, the risk of death rather than the risk of survival).
If studies only report relative continuous values such as relative times, the ratio of the
time for the treatment group versus the time for the control group is used. Calculations
are done in Python (3.14.6) with
scipy (1.18.0), pythonmeta (1.26), numpy (2.5.1), statsmodels (0.14.6), and plotly (6.9.0).
Mixed-effects meta-regression results are computed with R (4.4.0) using the metafor
(4.6-0) and rms (6.8-0) packages, and using the most serious sufficiently powered outcome.
For all statistical tests, a p-value less than 0.05 was considered statistically
significant.
Grobid 0.8.2 is used to parse PDF documents.
When evaluating potential effect modification across groups, we use an
interaction test as described by Altman (C) et al. We compared the log-transformed
relative risks using a z-test, deriving the standard error of the difference from
the 95% confidence intervals. A two-sided interaction p-value of < 0.05 was
considered a statistically significant difference in treatment effect between the
groups.
Cochrane RoB 2/ROBINS-I are often used to evaluate studies, and have the advantage of
providing standardized rules that can be applied with minimal understanding of the domain
and study. However, the rules do not account for many real-world issues, often
overemphasize or underemphasize others, and studies show low inter-rater
reliability158.
Certain domains are more applicable for these tools, however the time-sensitive nature of
a pandemic, with significant mortality for every day of delay in evidence assessment, and
the characteristics of COVID-19 make them inappropriate for this domain.
This can be demonstrated with examples where expert RoB 2/ROBINS-I ratings do not match
reality for COVID-19. Popp et al. use RoB 2 to classify Reis et al. as low
risk of bias, however this is the opposite of reality—the trial not only has very
high risk of bias, but has very high actual known bias, refusing to release data despite
pledging to, reporting multiple impossible numbers, having blinding and randomization
failure, and many other issues160.
Axfors et al. use RoB 2 to classify Horby et al. as low risk of bias, however
this is the opposite of reality—the very late treatment and excessive dosage used
produces results with no relevance to recommended usage.
HCQ shows poor results with
late treatment and excessive dosage, and the combination shows harmD.
Hempenius et al. use ROBINS-I to classify 33 studies for HCQ. The two rated as having
the lowest risk of bias156,157 are far from the most informative. Both
involve very late treatment, providing no information on recommended usage, and ROBINS-I
does a very poor job of accounting for the impact of confounding factorsE.
Our quality evaluation focuses on known issues and bias, and the potential
impact on outcomes, rather than just the risk of bias.
The estimated potential impact of each confounding factor, and the direction of the impact
is considered. For example, consider a study that shows significantly lower risk, the
value of the study varies significantly if confounding points to an underestimate or an
overestimate of efficacy. In one case, the real effect may be null, while the other case
provides stronger evidence of efficacy (which may be greater than the study shows).
Analysis focusing on the risk of bias, while simpler, may penalize studies for theoretical
or technical issues that have no or minimal impact on outcomes. Analysis also depends on
the outcome, for example certain issues are less relevant for objective outcomes such as
mortality.
Inaccurate penalization, and inaccurate high-quality evaluation in the face of known major
issues affecting outcomes, increases in significance during a pandemic when immediate
recognition of new evidence is critical, and when considering all global studies, as
required during a pandemic. Investigators in other countries may have different customs
for design, analysis, and reporting, and different English language skills, however they
may not be less diligent or have greater bias.
Investigators in lower-pharmaceutical-profit countries may have lower bias towards
profitable interventions.
We have classified studies as
early treatment if most patients are not already at a severe stage at the time of
treatment (for example based on oxygen status or lung involvement), and treatment started
within 5 days of the onset of symptoms. If studies contain a mix of early treatment and
late treatment patients, we consider the treatment time of patients contributing most to
the events (for example, consider a study where most patients are treated early but late
treatment patients are included, and all mortality events were observed with late
treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only considered
effective when used within a shorter timeframe, for example 0-36 or 0-48 hours for
oseltamivir, with longer delays not being effective71,72.
This is a living analysis and is updated regularly.
We received no funding, this research is done in our spare time.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/chxmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
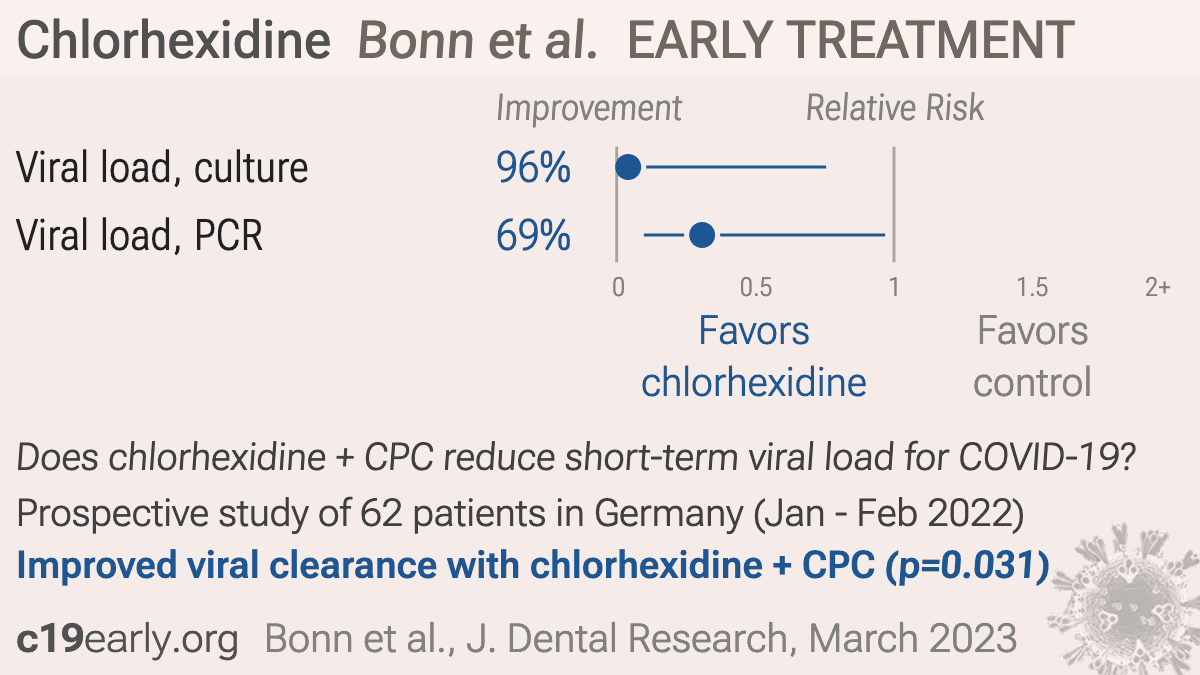
| Bonn, 3/21/2023, Double Blind Randomized Controlled Trial, Germany, peer-reviewed, 14 authors, study period 4 January, 2022 - 22 February, 2022, this trial uses multiple treatments in the treatment arm (combined with CPC) - results of individual treatments may vary, trial DRKS00027812. | viral load, 85.3% lower, relative load 0.15, p = 0.20, treatment 6, control 9, relative reduction in infectious viral load, 30 min vs. baseline, CPC+CHX. |
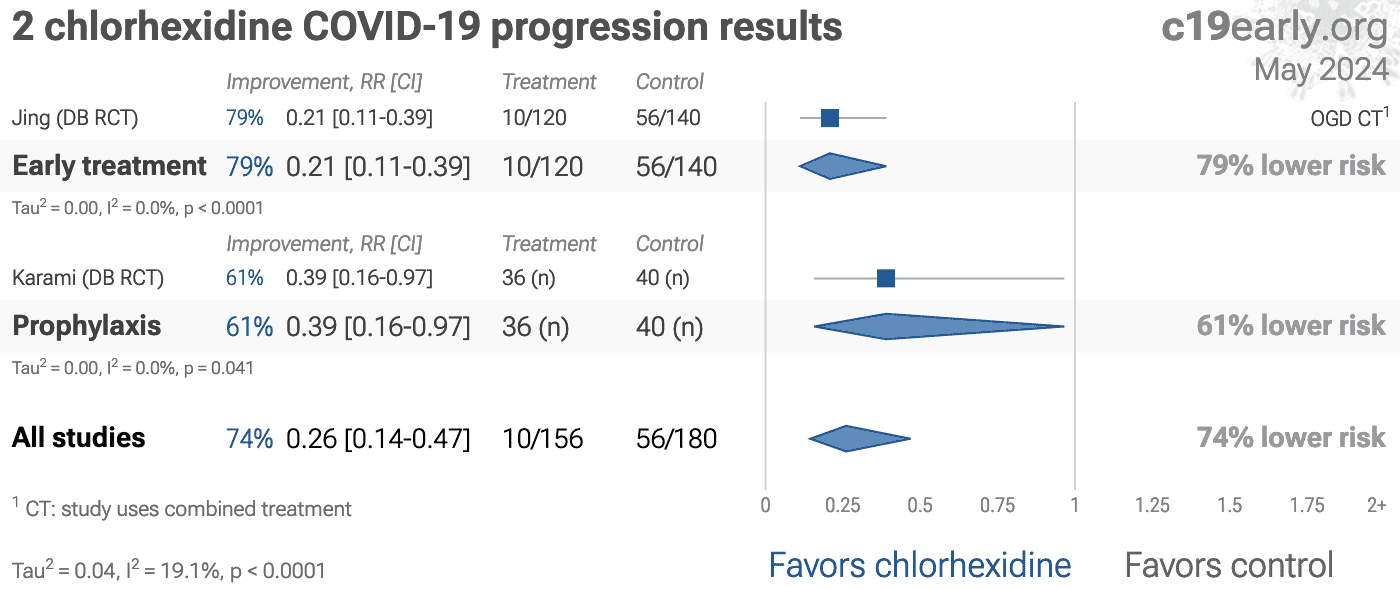
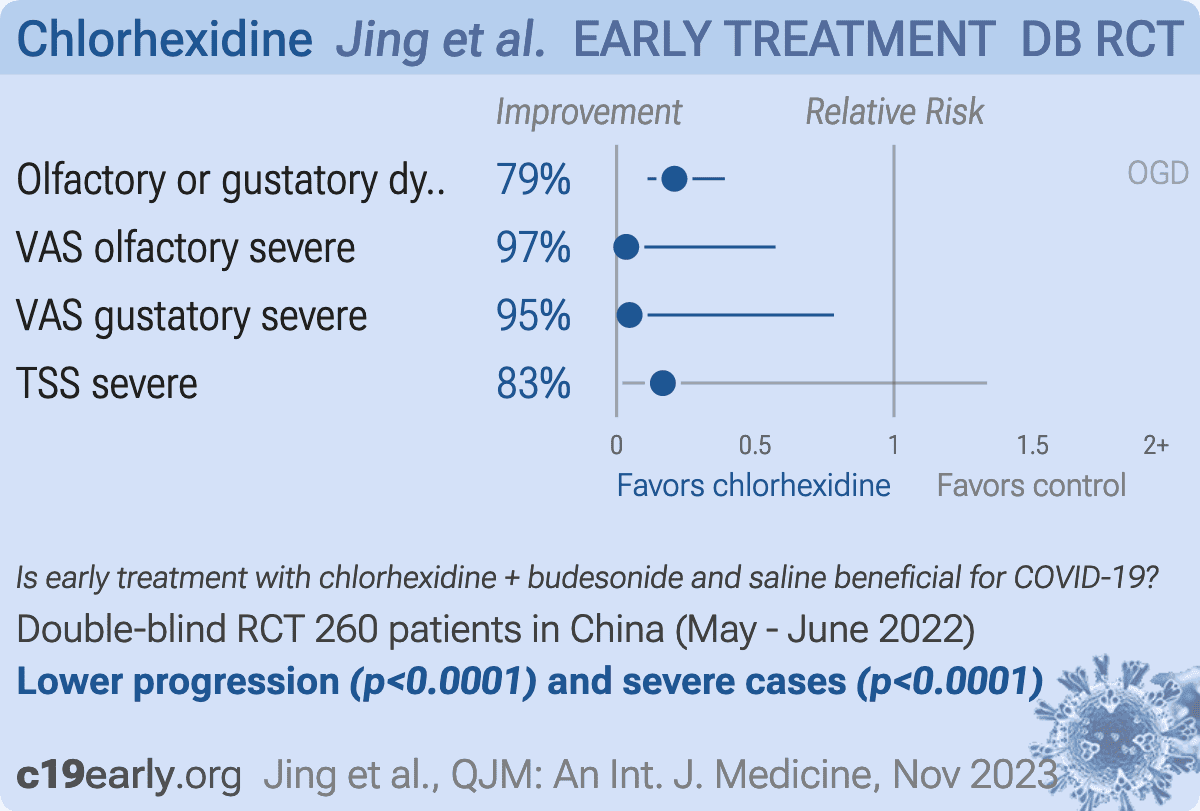
| Jing, 11/21/2023, Double Blind Randomized Controlled Trial, China, peer-reviewed, 7 authors, study period 5 May, 2022 - 16 June, 2022, this trial uses multiple treatments in the treatment arm (combined with budesonide and saline) - results of individual treatments may vary, trial ChiCTR2200059651. | olfactory or gustatory dysfunction, 79.2% lower, RR 0.21, p < 0.001, treatment 10 of 120 (8.3%), control 56 of 140 (40.0%), NNT 3.2, OGD. |
| VAS olfactory severe, 96.5% lower, RR 0.03, p < 0.001, treatment 0 of 120 (0.0%), control 15 of 140 (10.7%), NNT 9.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| VAS gustatory severe, 95.3% lower, RR 0.05, p = 0.001, treatment 0 of 120 (0.0%), control 11 of 140 (7.9%), NNT 13, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| TSS severe, 83.3% lower, RR 0.17, p = 0.07, treatment 1 of 120 (0.8%), control 7 of 140 (5.0%), NNT 24. | Mira, 1/8/2022, Double Blind Randomized Controlled Trial, placebo-controlled, trial NCT05543603 (history). | 48 patient RCT with results unknown and over 4 years late. |
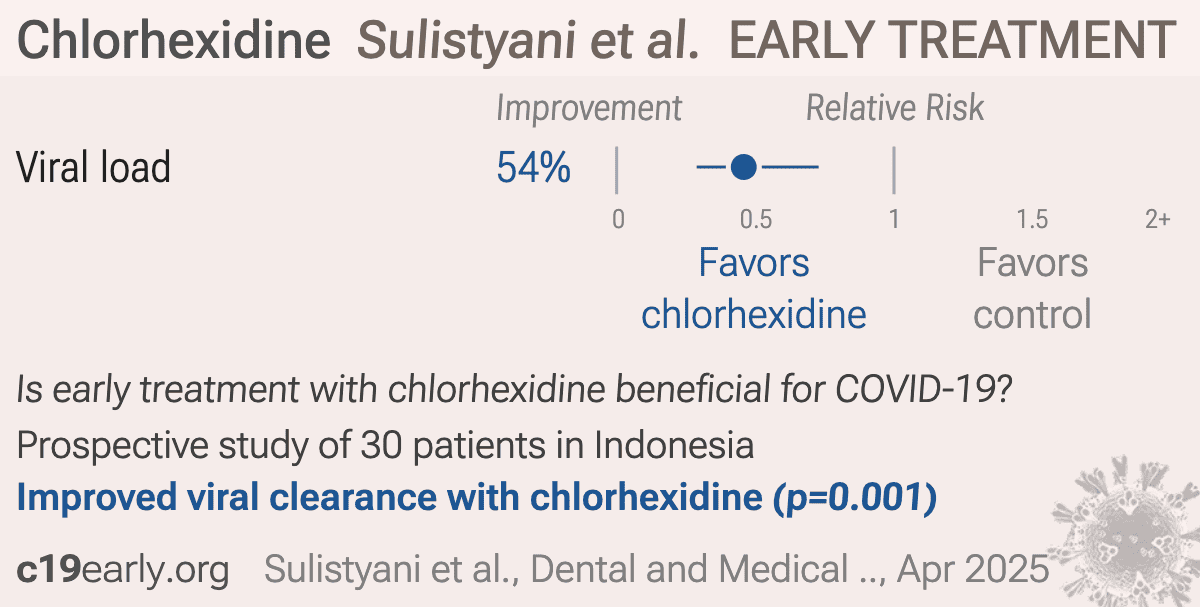
| Sulistyani, 4/30/2025, prospective, Indonesia, peer-reviewed, 8 authors. | viral load, 54.2% lower, relative load 0.46, p = 0.001, treatment 15, control 15, relative increase in Ct value, day 5. | Xie, 2/28/2022, Double Blind Randomized Controlled Trial, placebo-controlled, trial NCT04931004 (history). | Estimated 90 patient RCT with results unknown and over 4 years late. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
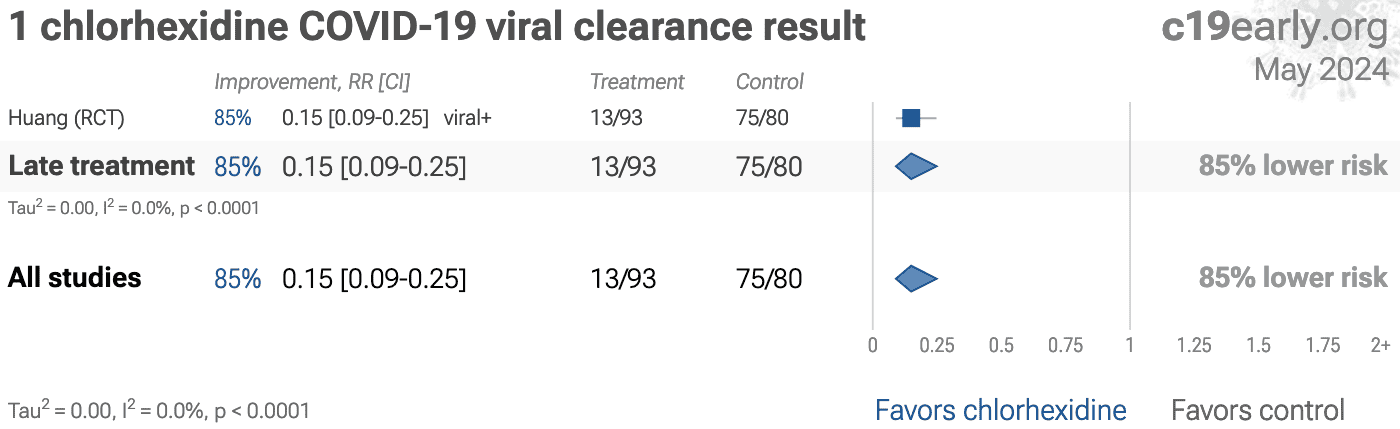
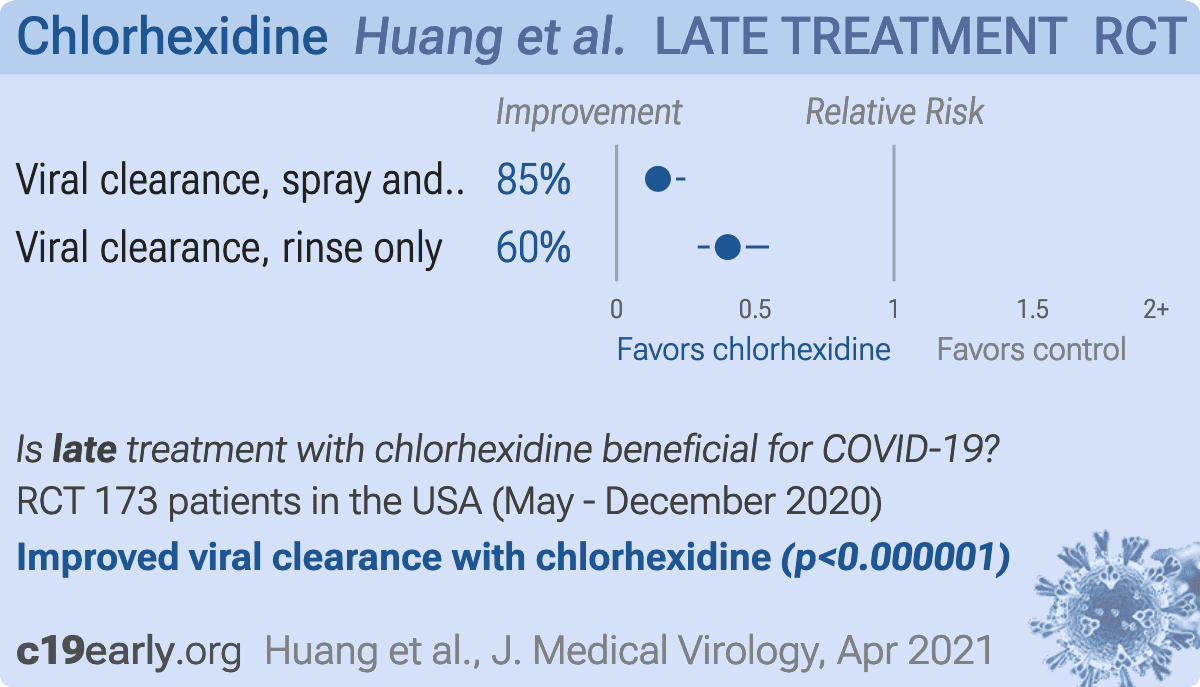
| Huang, 4/30/2021, Randomized Controlled Trial, USA, peer-reviewed, median age 62.0, 2 authors, study period 20 May, 2020 - 15 December, 2020. | risk of no viral clearance, 74.6% lower, RR 0.25, p < 0.001, treatment 38 of 159 (23.9%), control 127 of 135 (94.1%), NNT 1.4, all patients, day 4. |
| risk of no viral clearance, 85.1% lower, RR 0.15, p < 0.001, treatment 13 of 93 (14.0%), control 75 of 80 (93.8%), NNT 1.3, oropharyngeal rinse and spray, day 4. | |
| risk of no viral clearance, 59.9% lower, RR 0.40, p < 0.001, treatment 25 of 66 (37.9%), control 52 of 55 (94.5%), NNT 1.8, oropharyngeal rinse only, day 4. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
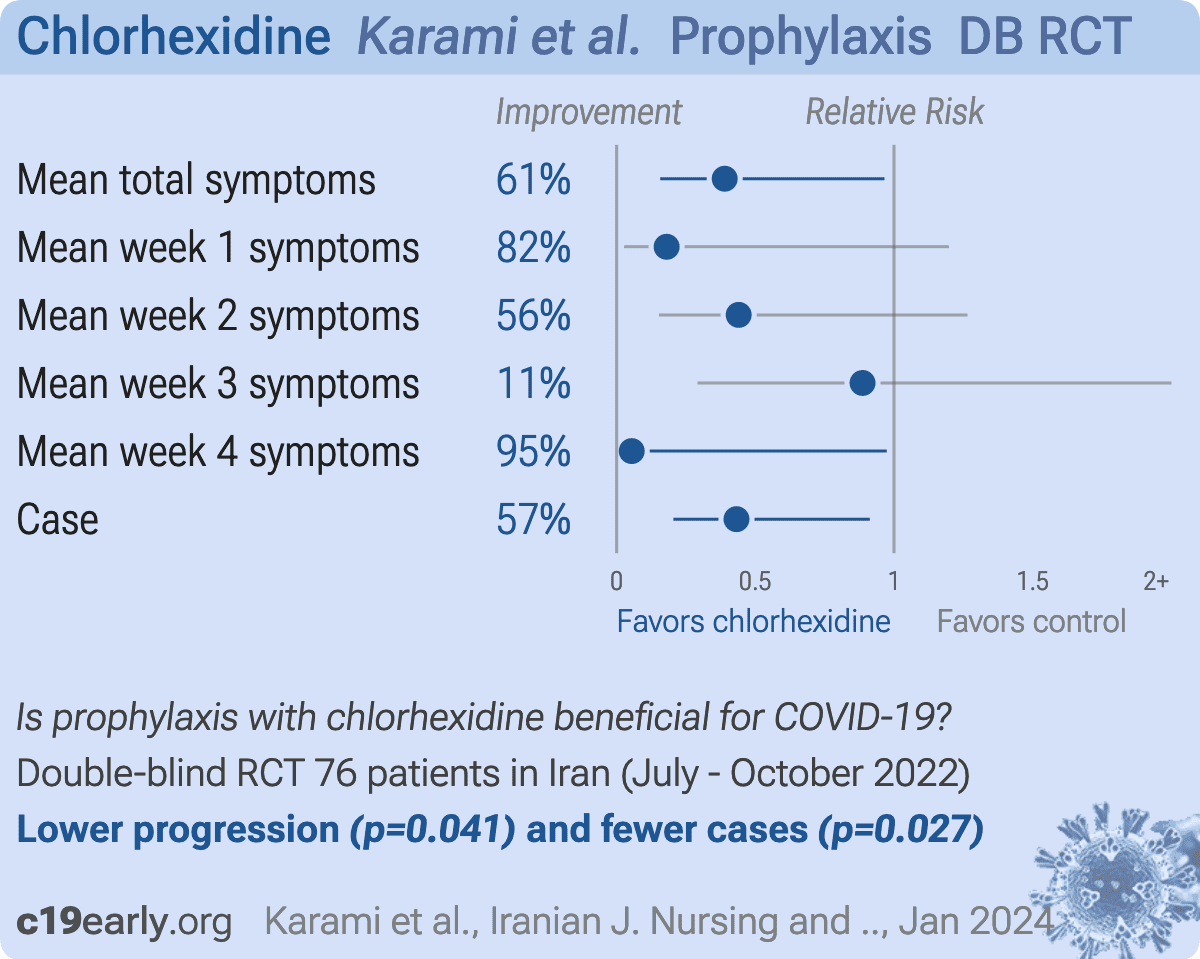
| Karami, 1/9/2024, Double Blind Randomized Controlled Trial, Iran, peer-reviewed, 4 authors, study period July 2022 - October 2022, trial IRCT20220328054364N1. | relative mean total symptoms, 61.0% better, RR 0.39, p = 0.04, treatment mean 1.8 (±3.67) n=36, control mean 4.62 (±7.37) n=40. |
| relative mean week 1 symptoms, 82.0% better, RR 0.18, p = 0.08, treatment mean 0.22 (±1.17) n=36, control mean 1.22 (±3.14) n=40. | |
| relative mean week 2 symptoms, 56.0% better, RR 0.44, p = 0.13, treatment mean 0.66 (±2.05) n=36, control mean 1.5 (±2.63) n=40. | |
| relative mean week 3 symptoms, 11.3% better, RR 0.89, p = 0.84, treatment mean 0.86 (±2.66) n=36, control mean 0.97 (±2.16) n=40. | |
| relative mean week 4 symptoms, 94.6% better, RR 0.05, p = 0.048, treatment mean 0.05 (±0.23) n=36, control mean 0.92 (±2.58) n=40. | |
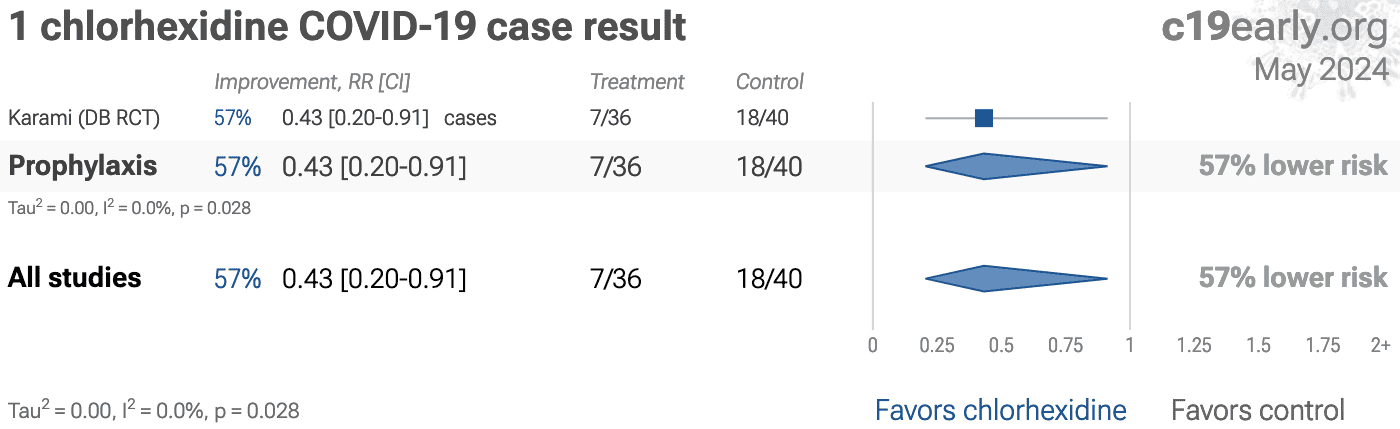
| risk of case, 56.8% lower, RR 0.43, p = 0.03, treatment 7 of 36 (19.4%), control 18 of 40 (45.0%), NNT 3.9. | Keating, 6/30/2022, Randomized Controlled Trial, USA, this trial uses multiple treatments in the treatment arm (combined with PVP-I) - results of individual treatments may vary, trial NCT04478019 (history) (SHIELD). | 245 patient RCT with results unknown and over 4 years late. |
Viral infection and replication involves attachment, entry, uncoating and release, genome replication and transcription, translation and protein processing, assembly and budding, and release. Each step can be disrupted by therapeutics.
Monoclonal antibodies were
previously included. Other treatments such as dexamethasone, tocilizumab, and baricitinib
were recommended for late stage hospitalized patients.
Smoking was
known to cause lung cancer since at least 1939, but this was not widely recognized in the
US until 1964, 25 years later. Surgeon general Leroy Burney tried publicizing the danger
starting in 1957, with limited success. Surgeon general Luther Terry, appointed in 1961,
prompted by President Kennedy in 1962 amid pressure from health advocates, finally got
recognition in 1964. The 1964 report reviewed 7,000+ studies, but these could (and should)
have been reviewed and acted upon in real-time as they were published.
Historians attribute the 25 year delay to an industry campaign to manufacture doubt and
controversy, through tactics like funding biased and fraudulent research from
"independent" organizations, attacking scientists, and political lobbying.
The success of the industry campaign is only possible because officials did not analyze
the research in detail. Fraudulent industry research supported prior failures, but would
have been called out as fraudulent by officials that analyzed and understood the research
in real-time.
When administered late in infection, HCQ may enhance viral egress by further increasing
lysosomal pH beyond the effect of ORF3a's water channel activity, thereby promoting
lysosomal exocytosis, inactivating degradative enzymes, and facilitating the release of
SARS-CoV-2 particles into the extracellular environment152,153.
Research also suggests potential cardioprotective effects at lower doses, but
cardiotoxicity with excessive dosage154. Bobrowski et al. also
indicate negative effects if HCQ and remdesivir are combined.
Peters et al. is subject to confounding by calendar-time (SOC evolved rapidly early in
the pandemic, the linear covariate does not reflect non-linear SOC changes and hospital
specific effects), hospital type (non-treatment hospitals were tertiary university
centers), confounding by indication (4/7 hospitals initiated treatment on deterioration),
immortal-time bias for as-treated (exposure assigned after baseline), significant
differences for other experimental treatments, potential overadjustment from collider bias
(steroid use and indication bias), limited baseline severity information, differences in
hospice referral propensity across hospitals, unadjusted difference in time from onset to
admission, difference in PCR positivity, and other factors.
Mahévas et al. is subject to confounding by hospital (treatment highly dependent on
the hospital, different SOC/ICU transfer practices, not included in PS), immortal time
(only partly addressed in sensitivity analysis), co-treatment differences, calendar-time
(SOC evolved rapidly early in the pandemic), binary coding for age (age ≥65 despite steep
age-risk gradient), residual imbalance (variables dropped from PS), a composite outcome
dependent on hospital triage/capacity, and other factors.
Seijas-Otero et al., Antiseptics as effective virucidal agents against SARS-CoV-2: Systematic review and Bayesian network meta-analysis, Japanese Dental Science Review, doi:10.1016/j.jdsr.2025.05.001.
Ryu et al., Fibrin drives thromboinflammation and neuropathology in COVID-19, Nature, doi:10.1038/s41586-024-07873-4.
Dai et al., Neurological complications of COVID-19, QJM: An International Journal of Medicine, doi:10.1093/qjmed/hcac272.
Rong et al., Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19, Cell Host & Microbe, doi:10.1016/j.chom.2024.11.007.
Yang et al., SARS-CoV-2 infection causes dopaminergic neuron senescence, Cell Stem Cell, doi:10.1016/j.stem.2023.12.012.
Scardua-Silva et al., Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19, Scientific Reports, doi:10.1038/s41598-024-52005-7.
Hampshire et al., Cognition and Memory after Covid-19 in a Large Community Sample, New England Journal of Medicine, doi:10.1056/NEJMoa2311330.
Duloquin et al., Is COVID-19 Infection a Multiorganic Disease? Focus on Extrapulmonary Involvement of SARS-CoV-2, Journal of Clinical Medicine, doi:10.3390/jcm13051397.
Sodagar et al., Pathological Features and Neuroinflammatory Mechanisms of SARS-CoV-2 in the Brain and Potential Therapeutic Approaches, Biomolecules, doi:10.3390/biom12070971.
Sagar et al., COVID-19-associated cerebral microbleeds in the general population, Brain Communications, doi:10.1093/braincomms/fcae127.
Verma et al., Persistent Neurological Deficits in Mouse PASC Reveal Antiviral Drug Limitations, bioRxiv, doi:10.1101/2024.06.02.596989.
Panagea et al., Neurocognitive Impairment in Long COVID: A Systematic Review, Archives of Clinical Neuropsychology, doi:10.1093/arclin/acae042.
Ariza et al., COVID-19: Unveiling the Neuropsychiatric Maze—From Acute to Long-Term Manifestations, Biomedicines, doi:10.3390/biomedicines12061147.
Vashisht et al., Neurological Complications of COVID-19: Unraveling the Pathophysiological Underpinnings and Therapeutic Implications, Viruses, doi:10.3390/v16081183.
Ahmad et al., Neurological Complications and Outcomes in Critically Ill Patients With COVID-19: Results From International Neurological Study Group From the COVID-19 Critical Care Consortium, The Neurohospitalist, doi:10.1177/19418744241292487.
Wang et al., SARS-CoV-2 membrane protein induces neurodegeneration via affecting Golgi-mitochondria interaction, Translational Neurodegeneration, doi:10.1186/s40035-024-00458-1.
Freitas et al., Central nervous system and systemic inflammatory networks associated with acute neurological outcomes in COVID-19, Scientific Reports, doi:10.1038/s41598-025-08632-9.
Lu et al., Risk of neuropsychiatric and related conditions associated with SARS-CoV-2 infection: a difference-in-differences analysis, Nature Communications, doi:10.1038/s41467-025-61961-1.
Jachman-Kapułka et al., Cross-Section of Neurological Manifestations Among SARS-CoV-2 Omicron Subvariants—Single-Center Study, Brain Sciences, doi:10.3390/brainsci14111161.
Beckman et al., SARS-CoV-2 infects neurons and induces neuroinflammation in a non-human primate model of COVID-19, Cell Reports, doi:10.1016/j.celrep.2022.111573.
Eberhardt et al., SARS-CoV-2 infection triggers pro-atherogenic inflammatory responses in human coronary vessels, Nature Cardiovascular Research, doi:10.1038/s44161-023-00336-5.
Van Tin et al., Spike Protein of SARS-CoV-2 Activates Cardiac Fibrogenesis through NLRP3 Inflammasomes and NF-κB Signaling, Cells, doi:10.3390/cells13161331.
Borka Balas et al., COVID-19 and Cardiac Implications—Still a Mystery in Clinical Practice, Reviews in Cardiovascular Medicine, doi:10.31083/j.rcm2405125.
AlTaweel et al., An In-Depth Insight into Clinical, Cellular and Molecular Factors in COVID19-Associated Cardiovascular Ailments for Identifying Novel Disease Biomarkers, Drug Targets and Clinical Management Strategies, Archives of Microbiology & Immunology, doi:10.26502/ami.936500177.
Saha et al., COVID-19 beyond the lungs: Unraveling its vascular impact and cardiovascular complications—mechanisms and therapeutic implications, Science Progress, doi:10.1177/00368504251322069.
Yin et al., COVID-19: a vascular nightmare unfolding, Frontiers in Immunology, doi:10.3389/fimmu.2025.1593885.
Bruno et al., Accelerated vascular ageing after COVID-19 infection: the CARTESIAN study, European Heart Journal, doi:10.1093/eurheartj/ehaf430.
Abiri et al., The silent legacy of COVID-19: exploring genomic instability in long-term COVID-19 survivors, BMC Infectious Diseases, doi:10.1186/s12879-025-11419-y.
Gioia et al., SARS-CoV-2 infection induces DNA damage, through CHK1 degradation and impaired 53BP1 recruitment, and cellular senescence, Nature Cell Biology, doi:10.1038/s41556-023-01096-x.
Doğan et al., Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients, Current Issues in Molecular Biology, doi:10.3390/cimb45020062.
Rueda-Torres et al., Longitudinal Assessment of DNA Damage in PBMCs From Hospitalized COVID‐19 Patients via Alkaline Comet Assay, Environmental and Molecular Mutagenesis, doi:10.1002/em.70055.
Trender et al., Changes in memory and cognition during the SARS-CoV-2 human challenge study, eClinicalMedicine, doi:10.1016/j.eclinm.2024.102842.
Wu et al., SARS-CoV-2 replication in airway epithelia requires motile cilia and microvillar reprogramming, Cell, doi:10.1016/j.cell.2022.11.030.
Demarco, S., Shadowing SARS-CoV-2 Through Mucus and Cilia, DDN, viewonline.drugdiscoverynews.com/hubfs/DDN%20Milestones/Shadowing%20SARS-CoV-2%20Through%20Mucus%20and%20Cilia.pdf.
Lee et al., ACE2 localizes to the respiratory cilia and is not increased by ACE inhibitors or ARBs, Nature Communications, doi:10.1038/s41467-020-19145-6.
Dugied et al., Multimodal SARS-CoV-2 interactome sketches the virus-host spatial organization, Communications Biology, doi:10.1038/s42003-025-07933-z.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Katiyar et al., SARS-CoV-2 Assembly: Gaining Infectivity and Beyond, Viruses, doi:10.3390/v16111648.
Wu (B) et al., Decoding the genome of SARS-CoV-2: a pathway to drug development through translation inhibition, RNA Biology, doi:10.1080/15476286.2024.2433830.
Rius-Salvador et al., Cetylpyridinium chloride and chlorhexidine show antiviral activity against Influenza A virus and Respiratory Syncytial virus in vitro, PLOS ONE, doi:10.1371/journal.pone.0297291.
web.archive.org, web.archive.org/web/20211117052139/https://astralcodexten.substack.com/p/ivermectin-much-more-than-you-wanted.
Hayward et al., Ivermectin for COVID-19 in adults in the community (PRINCIPLE): an open, randomised, controlled, adaptive platform trial of short- and longer-term outcomes, Journal of Infection, doi:10.1016/j.jinf.2024.106130.
Jadad et al., Randomized Controlled Trials: Questions, Answers, and Musings, Second Edition, doi:10.1002/9780470691922.
Gøtzsche, P., Bias in double-blind trials, Doctoral Thesis, University of Copenhagen, www.scientificfreedom.dk/2023/05/16/bias-in-double-blind-trials-doctoral-thesis/.
Als-Nielsen et al., Association of Funding and Conclusions in Randomized Drug Trials, JAMA, doi:10.1001/jama.290.7.921.
Bekelman et al., Scope and Impact of Financial Conflicts of Interest in Biomedical Research, JAMA, doi:10.1001/jama.289.4.454.
Lundh et al., Industry sponsorship and research outcome, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.MR000033.pub3.
Concato et al., Randomized, Controlled Trials, Observational Studies, and the Hierarchy of Research Designs, New England Journal of Medicine, doi:10.1056/NEJM200006223422507.
Anglemyer et al., Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.MR000034.pub2.
Lee (B) et al., Analysis of Overall Level of Evidence Behind Infectious Diseases Society of America Practice Guidelines, Arch Intern Med., 2011, 171:1, 18-22, doi:10.1001/archinternmed.2010.482.
Deaton et al., Understanding and misunderstanding randomized controlled trials, Social Science & Medicine, 210, doi:10.1016/j.socscimed.2017.12.005.
Nichol et al., Challenging issues in randomised controlled trials, Injury, 2010, doi: 10.1016/j.injury.2010.03.033, www.injuryjournal.com/article/S0020-1383(10)00233-0/fulltext.
Akash et al., On a model-based approach to improve intranasal spray targeting for respiratory viral infections, Frontiers in Drug Delivery, doi:10.3389/fddev.2023.1164671.
Hossain et al., Mechanics-guided parametric modeling of intranasal spray devices and formulations for targeted drug delivery to the nasopharynx, Frontiers in Drug Delivery, doi:10.3389/fddev.2025.1721960.
Keating et al., SHIELD Study: Using Naso-oropharyngeal Antiseptic Decolonization to Reduce COVID-19 Viral Shedding (SHIELD), NCT04478019, clinicaltrials.gov/study/NCT04478019.
Xie et al., Oral Rinse to Reduced Expelled Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) During COVID-19 Infection, NCT04931004, clinicaltrials.gov/study/NCT04931004.
Mira et al., Evaluation of the Efficacy of Mouth Rinses With Commercial Mouthwashes to Decrease Viral Load in Saliva in COVID-19 Patients, NCT05543603, clinicaltrials.gov/study/NCT05543603.
help.altmetric.com, help.altmetric.com/support/solutions/articles/6000235983-attention-sources-tracked-by-altmetric.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Ikematsu et al., Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts, New England Journal of Medicine, doi:10.1056/NEJMoa1915341.
Hayden et al., Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents, New England Journal of Medicine, doi:10.1056/NEJMoa1716197.
Kumar et al., Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(21)00469-2.
López-Medina et al., Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2021.3071.
Korves et al., SARS-CoV-2 Genetic Variants and Patient Factors Associated with Hospitalization Risk, medRxiv, doi:10.1101/2024.03.08.24303818.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
Karita et al., Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection, medRxiv, doi:10.1101/2021.08.27.21262754.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
Willett et al., The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism, medRxiv, doi:10.1101/2022.01.03.21268111.
Peacock et al., The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry, bioRxiv, doi:10.1101/2021.12.31.474653.
Williams, T., Not All Ivermectin Is Created Equal: Comparing The Quality of 11 Different Ivermectin Sources, Do Your Own Research, doyourownresearch.substack.com/p/not-all-ivermectin-is-created-equal.
Xu et al., A study of impurities in the repurposed COVID-19 drug hydroxychloroquine sulfate by UHPLC-Q/TOF-MS and LC-SPE-NMR, Rapid Communications in Mass Spectrometry, doi:10.1002/rcm.9358.
Jitobaom et al., Favipiravir and Ivermectin Showed in Vitro Synergistic Antiviral Activity against SARS-CoV-2, Research Square, doi:10.21203/rs.3.rs-941811/v1.
Jitobaom (B) et al., Synergistic anti-SARS-CoV-2 activity of repurposed anti-parasitic drug combinations, BMC Pharmacology and Toxicology, doi:10.1186/s40360-022-00580-8.
Jeffreys et al., Remdesivir-ivermectin combination displays synergistic interaction with improved in vitro activity against SARS-CoV-2, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2022.106542.
Ostrov et al., Highly Specific Sigma Receptor Ligands Exhibit Anti-Viral Properties in SARS-CoV-2 Infected Cells, Pathogens, doi:10.3390/pathogens10111514.
Alsaidi et al., Griffithsin and Carrageenan Combination Results in Antiviral Synergy against SARS-CoV-1 and 2 in a Pseudoviral Model, Marine Drugs, doi:10.3390/md19080418.
Andreani et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microbial Pathogenesis, doi:10.1016/j.micpath.2020.104228.
De Forni et al., Synergistic drug combinations designed to fully suppress SARS-CoV-2 in the lung of COVID-19 patients, PLoS ONE, doi:10.1371/journal.pone.0276751.
Wan et al., Synergistic inhibition effects of andrographolide and baicalin on coronavirus mechanisms by downregulation of ACE2 protein level, Scientific Reports, doi:10.1038/s41598-024-54722-5.
Said et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1011522.
Fiaschi et al., In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants, Viruses, doi:10.3390/v16020168.
Xing et al., Published anti-SARS-CoV-2 in vitro hits share common mechanisms of action that synergize with antivirals, Briefings in Bioinformatics, doi:10.1093/bib/bbab249.
Chen et al., Synergistic Inhibition of SARS-CoV-2 Replication Using Disulfiram/Ebselen and Remdesivir, ACS Pharmacology & Translational Science, doi:10.1021/acsptsci.1c00022.
Hempel et al., Synergistic inhibition of SARS-CoV-2 cell entry by otamixaban and covalent protease inhibitors: pre-clinical assessment of pharmacological and molecular properties, Chemical Science, doi:10.1039/D1SC01494C.
Schultz et al., Pyrimidine inhibitors synergize with nucleoside analogues to block SARS-CoV-2, Nature, doi:10.1038/s41586-022-04482-x.
Ohashi et al., Potential anti-COVID-19 agents, cepharanthine and nelfinavir, and their usage for combination treatment, iScience, doi:10.1016/j.isci.2021.102367.
Al Krad et al., The protease inhibitor Nirmatrelvir synergizes with inhibitors of GRP78 to suppress SARS-CoV-2 replication, bioRxiv, doi:10.1101/2025.03.09.642200.
Abd Elsalam et al., Anti-COVID-19 activity and simple HPLC method for concurrent detection of repurposed drugs in novel binary mixtures, AMB Express, doi:10.1186/s13568-026-02030-8.
Rana et al., Ivermectin and Doxycycline combination as a promising anti-viral drug candidate: an in-silico and DFT study, In Silico Pharmacology, doi:10.1007/s40203-026-00576-w.
Setz et al., Synergistic Virus Neutralizing Activities of European Black Elderberry Fruit Extract and Iota-Carrageenan Against SARS-CoV-2, Influenza A Virus and Respiratory Syncytial Virus, Nutrients, doi:10.3390/nu18081205.
Ali et al., Preclinical Screening Platform Identifies Azatadine‐Dimaleate as a Potent Repurposed Therapeutic Against SARS‐CoV‐2 Infection, Journal of Medical Virology, doi:10.1002/jmv.70713.
Lew et al., Combination of Remdesivir and Ivermectin Exerts Highly Potent and Synergistic Antiviral Activity Against Murine Coronavirus and SARS-CoV-2 Infections, Cells, doi:10.3390/cells15131146.
Khatun et al., An All-Oral Antiviral Combination Strategy against COVID-19 Enabled by the Synergistic Mechanism of Action of Auranofin and Remdesivir, Elsevier BV, doi:10.2139/ssrn.6942990.
Thairu et al., A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2022/v34i44A36328.
Singh et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Tarragó-Gil et al., Randomized clinical trial to assess the impact of oral intervention with cetylpyridinium chloride to reduce salivary SARS‐CoV‐2 viral load, Journal of Clinical Periodontology, doi:10.1111/jcpe.13746.
Alemany et al., Cetylpyridinium Chloride Mouthwash to Reduce Shedding of Infectious SARS-CoV-2: A Double-Blind Randomized Clinical Trial, Journal of Dental Research, doi:10.1177/00220345221102310.
Covid Analysis, Azelastine for COVID-19: real-time meta-analysis of 4 studies (Version 6), c19early.org/azlmeta.html.
Covid Analysis (B), Cetylpyridinium Chloride reduces COVID-19 risk: real-time meta-analysis of 4 studies (Version 6), c19early.org/cpcmeta.html.
Covid Analysis (C), Chlorpheniramine reduces COVID-19 risk: real-time meta-analysis of 3 studies, c19early.org/cpmmeta.html.
Covid Analysis (D), Hydrogen Peroxide reduces COVID-19 risk: real-time meta-analysis of 8 studies (Version 5), c19early.org/hpmeta.html.
Covid Analysis (E), Inhaled Heparin reduces COVID-19 risk: real-time meta-analysis of 3 studies, c19early.org/iufhmeta.html.
Covid Analysis (F), Iota-carrageenan for COVID-19: real-time meta-analysis of 1 study (Version 3), c19early.org/gmeta.html.
Covid Analysis (G), NaCl reduces COVID-19 risk: real-time meta-analysis of 9 studies (Version 6), c19early.org/naclmeta.html.
Covid Analysis (H), Nitric Oxide reduces COVID-19 risk: real-time meta-analysis of 14 studies (Version 16), c19early.org/nometa.html.
Covid Analysis (I), Phthalocyanine reduces COVID-19 risk: real-time meta-analysis of 4 studies (Version 3), c19early.org/ptmeta.html.
Covid Analysis (J), Povidone-Iodine reduces COVID-19 risk: real-time meta-analysis of 21 studies (Version 40), c19early.org/pmeta.html.
Covid Analysis (K), Sodium Bicarbonate reduces COVID-19 risk: real-time meta-analysis of 6 studies (Version 2), c19early.org/sbmeta.html.
Brookes et al., Mouthwash Effects on the Oral Microbiome: Are They Good, Bad, or Balanced?, International Dental Journal, doi:10.1016/j.identj.2023.08.010.
Angjelova et al., Effects of Antiseptic Formulations on Oral Microbiota and Related Systemic Diseases: A Scoping Review, Antibiotics, doi:10.3390/antibiotics14080815.
Covid Analysis (L), Alkalinization reduces COVID-19 risk: real-time meta-analysis of 14 studies (Version 15), c19early.org/phmeta.html.
Boulware, D., Comments regarding paper rejection, twitter.com/boulware_dr/status/1311331372884205570.
Thangamani et al., Rinsing away the threat: Antiviral mouthwashes and their efficacy, World Academy of Sciences Journal, doi:10.3892/wasj.2025.366.
Okeke et al., Antiseptics: An expeditious third force in the prevention and management of coronavirus diseases, Current Research in Microbial Sciences, doi:10.1016/j.crmicr.2024.100293.
Brito-Reia et al., Antiviral Mechanism and Clinical Benefits of Mouthwash Active Against SARS-CoV-2, Current Oral Health Reports, doi:10.1007/s40496-024-00368-1.
Ting et al., The In Vitro Virucidal Effects of Mouthwashes on SARS-CoV-2, International Journal of Translational Medicine, doi:10.3390/ijtm2030030.
Sulistyani et al., Effects of chlorhexidine gluconate and povidone-iodine mouthwash on cycle threshold values in patients infected with SARS-CoV-2, Dental and Medical Problems, doi:10.17219/dmp/192493.
Jing et al., Effective early strategy to prevent olfactory and gustatory dysfunction in COVID-19: a randomized controlled trial, QJM: An International Journal of Medicine, doi:10.1093/qjmed/hcad262.
Bonn et al., Efficacy of a Mouthwash Containing CHX and CPC in SARS-CoV-2–Positive Patients: A Randomized Controlled Clinical Trial, Journal of Dental Research, doi:10.1177/00220345231156415.
Graves et al., A Cetylpyridinium Chloride Oral Rinse Reduces Salivary Viral Load in Randomized Controlled Trials, JDR Clinical & Translational Research, doi:10.1177/23800844241296840.
Huang et al., Use of chlorhexidine to eradicate oropharyngeal SARS‐CoV‐2 in COVID‐19 patients, Journal of Medical Virology, doi:10.1002/jmv.26954.
Karami et al., A Comparison of the Effects of Chlorhexidine and Sodium Bicarbonate Mouthwashes on COVID-19–Related Symptoms, Iranian Journal of Nursing and Midwifery Research, doi:10.4103/ijnmr.ijnmr_38_23.
Jain et al., Chlorhexidine and SARS-CoV-2 main protease: Molecular docking study, Journal of Indian Society of Periodontology, doi:10.4103/jisp.jisp_39_22.
Zeng et al., Novel receptor, mutation, vaccine, and establishment of coping mode for SARS-CoV-2: current status and future, Frontiers in Microbiology, doi:10.3389/fmicb.2023.1232453.
Masoudi-Sobhanzadeh et al., Structure-based drug repurposing against COVID-19 and emerging infectious diseases: methods, resources and discoveries, Briefings in Bioinformatics, doi:10.1093/bib/bbab113.
Wu (C) et al., Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods, Acta Pharmaceutica Sinica B, doi:10.1016/j.apsb.2020.02.008.
Mateja et al., The choice of viral load endpoint in early phase trials of COVID-19 treatments aiming to reduce 28-day hospitalization and/or death, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf282.
Zhang et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Sweeting et al., What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data, Statistics in Medicine, doi:10.1002/sim.1761.
Altman (C) et al., Interaction revisited: the difference between two estimates, BMJ, doi:10.1136/bmj.326.7382.219.
Michelucci et al., SARS-CoV-2 ORF3a accessory protein is a water-permeable channel that induces lysosome swelling, Communications Biology, doi:10.1038/s42003-024-07442-5.
Ghosh et al., β-Coronaviruses Use Lysosomes for Egress Instead of the Biosynthetic Secretory Pathway, Cell, doi:10.1016/j.cell.2020.10.039.
Kamga Kapchoup et al., In vitro effect of hydroxychloroquine on pluripotent stem cells and their cardiomyocytes derivatives, Frontiers in Pharmacology, doi:10.3389/fphar.2023.1128382.
Bobrowski et al., Synergistic and Antagonistic Drug Combinations against SARS-CoV-2, Molecular Therapy, doi:10.1016/j.ymthe.2020.12.016.
Peters et al., Outcomes of Persons With COVID-19 in Hospitals With and Without Standard Treatment With (Hydroxy)chloroquine, Clinical Microbiology and Infection, doi:10.1016/j.cmi.2020.10.004.
Mahévas et al., Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: observational comparative study using routine care data, BMJ 2020, doi:10.1136/bmj.m1844.
Minozzi et al., The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2020.06.015.
Popp et al., Ivermectin for preventing and treating COVID-19, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.CD015017.pub3.
Reis et al., Effect of Early Treatment with Ivermectin among Patients with Covid-19, New England Journal of Medicine, doi:10.1056/NEJMoa2115869.
Axfors et al., Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative meta-analysis of randomized trials, Nature, doi:10.1038/s41467-021-22446-z.