NIH COVID-19 treatment analysis
• NIH reviewed very few RCTs for low-cost treatments, while claiming insufficient evidence
• Only three high-profit drugs from top lobbying companies were found beneficial
Authority review was extremely slow
and overlooked most research
Official treatment recommendations were often made based on a small fraction of
the evidence, with substantial bias in the selection of studies.
Just as 78% of experts polled regarding the origin of COVID-19 were not familiar with the
DEFUSE protocol4, experts on COVID-19 treatments were not familiar with
much of the key evidence.
In some cases, recommendations were made without reviewing any clinical evidence,
for example the US FDA recommended against ivermectin in an article that stated
"The FDA has not reviewed data to support use of ivermectin in COVID-19"5.
In cases where the people involved in recommendations are known, they were
often busy professionals that could not realistically have time to
carefully review all evidence6.
| NIH treatment analysis | ||||
| Treatment | NIH status | Studies referenced | ||
|---|---|---|---|---|
| Vitamin D | Insufficient evidence | 5 of 138 4% | ||
| Vitamin C | Insufficient evidence | 6 of 72 8% | ||
| Zinc | Insufficient evidence | 3 of 41 7% | ||
| Metformin | Insufficient evidence | 4 of 113 4% | ||
| Fluvoxamine | Against | 6 of 21 29% | ||
| Curcumin | No analysis | 0 of 28 - | ||
| PVP-I | No analysis | 0 of 21 - | ||
| Melatonin | No analysis | 0 of 18 - | ||
| Quercetin | No analysis | 0 of 9 - | ||
| N. Sativa | No analysis | 0 of 14 - | ||
 c19early.org | ||||
Table 1. The NIH did not review most evidence for
low-cost treatments—reviewing 2% of studies (7% of RCTs), while
including very low quality studies.
NIH reviews
NIH treatment reviews were done by a panel of 40+ external experts with
extensive conflicts of interest towards high-profit treatments6,7.
Out of 11,903 proposed treatments8,
they found only three high-profit drugs from top lobbying companies to be beneficial for
early treatment(a).
Most others received either "insufficient evidence" or no review at all,
despite extensive unreviewed evidence.
Across all low-cost treatments that reduce risk (within the 226
we cover), the NIH only referenced 2% of the
studies.
For vitamin D, the NIH claims "insufficient evidence ... to recommend either for or against"9.
No authors are listed, they provide only a brief narrative review, and they reference only 5 of the
138 controlled studies
(41 RCTs). The state is
similar or worse for other treatments (Table 1). The NIH provides no
quantitative analysis for any of the treatments listed.
Considering RCTs for vitamin D, the NIH references only
410-13 of 41 (Figure 114). The NIH selection does not have above average relevance or quality, for example
including two very late treatment studies using bolus doses of
cholecalciferol11,12—a trifecta of poor design and low relevance compared to recommended use:
early treatment is better, continuous dosing is more effective than bolus doses, and calcifediol,
calcitriol, or analogs avoid long delays in conversion.
They include none of the early treatment RCTs. We provide similar analysis for vitamin
C15 and
zinc16.
Figure 1. NIH vitamin D analysis—37 RCTs missing.
Figure 2. NIH vitamin C analysis—14 RCTs missing.
Figure 3. NIH zinc analysis—6 RCTs missing.
Waiting for RCTs costs lives
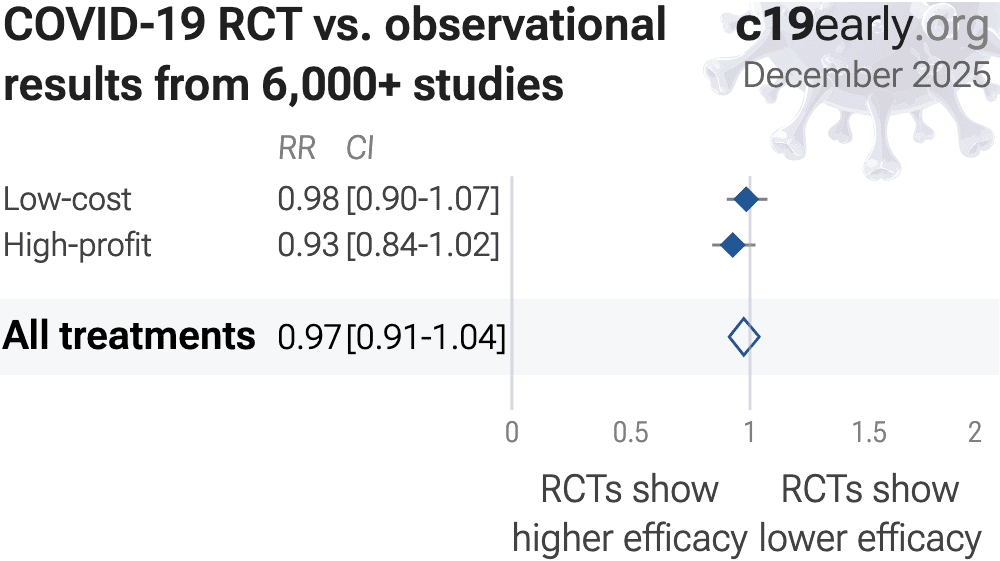
While the NIH examined few of the RCTs, they dismissed almost all observational studies.
RCTs can provide significant advantages, however they show no benefit for COVID-19 and they introduce significantly delay.
For the 226 treatments analyzed, there is no difference in results
between RCTs and observational studies, RR 0.97 [0.91‑1.03]17 (Figure 4).
Observational studies do not systematically over- or underestimate
efficacy, as found in previous research18,19, and they
provided confirmation of efficacy 8+ months faster. RCTs aim to equalize study groups, but add
their own biases. For acute diseases with strong benefits for earlier treatment,
the typical increased treatment delay adds a major confounding factor.
Both RCTs and observational studies span the bias spectrum, from minimal to extreme.
Studies must be evaluated individually.
While observational studies require greater expertise to analyze, the advantages in
practicality, cost, time, and ethics are substantial.
{kind=link}
Waiting for specific outcomes costs
lives While patented treatments may be approved with a single
non-clinical
result20, authorities
often dismiss results for low-cost treatments where studies report different
outcomes.
To avoid delay and unnecessary mortality, we must use all available evidence.
Logically, minimizing viral replication will minimize serious outcomes. Singh
et al.21 confirm, showing improved viral clearance
significantly associated with lower hospitalization/death.
We confirm this across all 226 treatments—improved viral
clearance is strongly associated with lower serious outcomes, p = 0.00000000032 (see the appendix for
details).
Authorities may not pool any outcomes, e.g., separating studies reporting mortality
and studies reporting ICU admission, however data shows that—for COVID-19—it
is valid to combine outcomes from viral clearance to mortality.
85% of treatments showing significant efficacy/harm with pooled
effects have been confirmed without pooling, with a mean delay of
4.6 months.
Novel treatments are high risk,
existing treatments have a critical safety advantage Existing treatments
have a strong advantage with known pharmacokinetics and safety profiles. New
agents are more risky. Long-term risks cannot be known, and
known risks may not be acknowledged for some time. For example, molnupiravir's
potential risks include the creation of dangerous
variants22-26,
mutagenicity, carcinogenicity, teratogenicity, and
embryotoxicity27-41.
While the risk always exceeded the benefits within the context of
all treatments, and confirmation of harm continues to accumulate, the
treatment is still used in 2026 in some locations.
Novel treatments saw limited use during the pandemic42,43,
partly due to prescription requirements, limited availability, high cost, and,
for certain treatments, administration requirements and drug interactions.
c19early.org
Low-cost existing treatments
Can reduce risk
Known safety profile
More widely available
Available immediately
Can be distributed in advance for immediate treatment
High-profit novel treatments
Can reduce risk
Inherently risky—long-term and rare side effects unknown
High cost limits use
Limited production
High profit incentivizes unethical behavior
Substantial delay for development and testing
Delayed treatment due to access barriers
Contact.
Contact us on X at @CovidAnalysis.
Funding.
We have received no funding or
compensation in any form, and do not accept donations. This is entirely volunteer work.
Conflicts of interest.
We have no conflicts of interest.
We have no affiliation with any pharmaceutical companies, supplement companies, governments, political parties, or advocacy organizations.AI.
We use AI models (Gemini, Grok, Claude, and
ChatGPT) tasked with functioning as additional peer-reviewers to check for errors, suggest
improvements, and review spelling and grammar. Any corrections are verified and applied
manually. Our preference for em dashes is independent of AI.Updates.
Our COVID-19 meta-analyses involve the extraction of over 226,000
datapoints from thousands of papers for 226 treatments. We thank the
thousands of scientists, physicians, and other contributors that have provided updates,
suggestions, feedback, and corrections. These are all welcome and can be submitted
below.
Dedication.
This work is dedicated to top
evidence-based physicians that worked tirelessly to analyze evidence and greatly reduce
mortality and morbidity during the pandemic. In alphabetical order:
Dr. Thomas J. Borody, Dr. Mary Talley Bowden, Dr. Flavio Cadegiani, Dr. Shankara Chetty,
Dr. Ryan Cole, Dr. George Fareed, Dr. Sabine Hazan, Dr. Pierre Kory, Dr. Tess Lawrie, Dr.
Robert Malone, Dr. Paul Marik, Dr. Peter McCullough, Dr. Didier Raoult, Dr. Harvey Risch,
Dr. Jackie Stone, Dr. Brian Tyson, Dr. Joseph Varon, and Dr. Vladimir (Zev) Zelenko.
Public domain.
This is a public domain work
distributed in accordance with the Creative Commons CC0 1.0 Universal license, which
dedicates the work to the public domain by waiving all rights worldwide under copyright law.
You can distribute, remix, adapt, and build upon this work in any medium or format,
including for commercial purposes, without asking permission. Referenced material and
third-party images retain any original copyrights or restrictions.
See: https://creativecommons.org/publicdomain/zero/1.0/.
Monoclonal antibodies were also included in earlier versions. Other treatments such as dexamethasone, tocilizumab, and baricitinib were recommended for late stage hospitalized patients.
Schilling et al., Evaluation of hydroxychloroquine or chloroquine for the prevention of COVID-19 (COPCOV): A double-blind, randomised, placebo-controlled trial, PLOS Medicine, doi:10.1371/journal.pmed.1004428.
Hobbs et al., The PRINCIPLE randomised controlled open label platform trial of hydroxychloroquine for treating COVID19 in community based patients at high risk, Scientific Reports, doi:10.1038/s41598-025-09275-6.
Enserink, M., Virologists and epidemiologists back natural origin for COVID-19, survey suggests, Science, doi:10.1126/science.zz3ed3v.
web.archive.org, web.archive.org/web/20210305163946/https://www.fda.gov/consumers/consumer-updates/why-you-should-not-use-ivermectin-treat-or-prevent-covid-19.
covid19treatmentguidelines.nih.gov, www.covid19treatmentguidelines.nih.gov/therapies/supplements/vitamin-d/.
Villasis-Keever et al., Efficacy and Safety of Vitamin D Supplementation to Prevent COVID-19 in Frontline Healthcare Workers. A Randomized Clinical Trial, Archives of Medical Research, doi:10.1016/j.arcmed.2022.04.003.
Murai et al., Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients With Moderate to Severe COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2020.26848.
Mariani et al., High-dose vitamin D versus placebo to prevent complications in COVID-19 patients: Multicentre randomized controlled clinical trial, PLOS ONE, doi:10.1371/journal.pone.0267918.
Elamir et al., A Randomized Pilot Study Using Calcitriol in Hospitalized Patients, Bone, doi:10.1016/j.bone.2021.116175.
Anglemyer et al., Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.MR000034.pub2.
Concato et al., Randomized, Controlled Trials, Observational Studies, and the Hierarchy of Research Designs, New England Journal of Medicine, doi:10.1056/NEJM200006223422507.
Singh et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Focosi et al., The fitness of molnupiravir-signed SARS-CoV-2 variants: imputation analysis based on prescription counts and GISAID analyses by country, Intervirology, doi:10.1159/000540282.
Sanderson et al., A molnupiravir-associated mutational signature in global SARS-CoV-2 genomes, Nature, doi:10.1038/s41586-023-06649-6.
Fountain-Jones et al., Effect of molnupiravir on SARS-CoV-2 evolution in immunocompromised patients: a retrospective observational study, The Lancet Microbe, doi:10.1016/S2666-5247(23)00393-2.
Kosakovsky Pond et al., Anti-COVID drug accelerates viral evolution, Nature, doi:10.1038/d41586-023-03248-3.
Swanstrom et al., Lethal mutagenesis as an antiviral strategy, Science, doi:10.1126/science.abn0048.
Hadj Hassine et al., Lethal Mutagenesis of RNA Viruses and Approved Drugs with Antiviral Mutagenic Activity, Viruses, doi:10.3390/v14040841.
Shum, C., An investigational study into the drug-associated mutational signature in SARS-CoV-2 viruses, The University of Hong Kong, PhD Thesis, hub.hku.hk/handle/10722/344396.
Waters et al., Human genetic risk of treatment with antiviral nucleoside analog drugs that induce lethal mutagenesis: the special case of molnupiravir, Environmental and Molecular Mutagenesis, doi:10.1002/em.22471.
Huntsman, M., An assessment of the reproductive toxicity of the anti-COVID-19 drug molnupiravir using stem cell-based embryo models, Master's Thesis, scholarspace.manoa.hawaii.edu/items/cd11342c-b4dc-44c0-8b44-ce6e3369c40b.
Huntsman (B) et al., Detection of developmental toxicity of the anti-COVID-19 drug molnupiravir using gastruloid-based in vitro assays, Toxicological Sciences, doi:10.1093/toxsci/kfaf093.
Zibat et al., N4-hydroxycytidine, the active compound of Molnupiravir, promotes SARS-CoV-2 mutagenesis and escape from a neutralizing nanobody, iScience, doi:10.1016/j.isci.2023.107786.
Shiraki et al., Convenient screening of the reproductive toxicity of favipiravir and antiviral drugs in Caenorhabditis elegans, Heliyon, doi:10.1016/j.heliyon.2024.e35331.
Gruber et al., Molnupiravir increases SARS‐CoV‐2 genome diversity and complexity: A case‐control cohort study, Journal of Medical Virology, doi:10.1002/jmv.29642.
Marikawa et al., An active metabolite of the anti-COVID-19 drug molnupiravir impairs mouse preimplantation embryos at clinically relevant concentrations, Reproductive Toxicology, doi:10.1016/j.reprotox.2023.108475.
Rahman, M., Elucidation of the DNA repair mechanisms involved in the repair of DNA damage caused by the Arabinosides and Anti-COVID-19 drugs, tokyo-metro-u.repo.nii.ac.jp/records/2000972.
Zhou et al., β-D-N4-hydroxycytidine Inhibits SARS-CoV-2 Through Lethal Mutagenesis But Is Also Mutagenic To Mammalian Cells, The Journal of Infectious Diseases, doi:10.1093/infdis/jiab247.
Chamod et al., Molnupiravir Metabolite--N4-hydroxycytidine Causes Cytotoxicity and DNA Damage in Mammalian Cells in vitro: N4-hydroxycytidine Induced Cytotoxicity DNA Damage, Asian Medical Journal and Alternative Medicine, 23:3, asianmedjam.com/index.php/amjam/article/view/1448.
Standing et al., Randomized controlled trial of molnupiravir SARS-CoV-2 viral and antibody response in at-risk adult outpatients, Nature Communications, doi:10.1038/s41467-024-45641-0.
Mori et al., Reactive oxygen species-mediated cytotoxic and DNA-damaging mechanism of N4-hydroxycytidine, a metabolite of the COVID-19 therapeutic drug molnupiravir, Free Radical Research, doi:10.1080/10715762.2025.2469738.