The Effect of Vitamin D Supplementation on Severe COVID-19 Outcomes in Patients With Vitamin D Insufficiency
et al., Journal of the Endocrine Society, doi: 10.1210/jendso/bvab048.567, May 2021
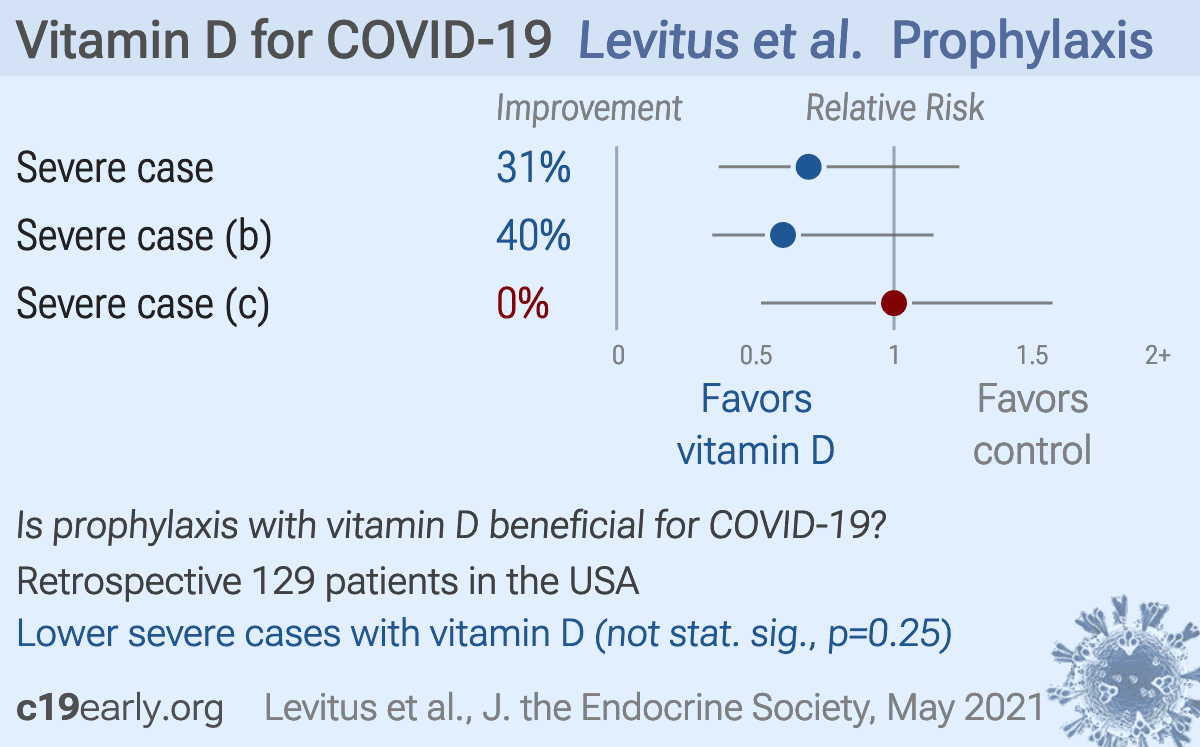
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


{kind=link}
Retrospective 129 hospitalized patients with vitamin D levels measured within 90 days prior to admission, showing lower, but not statistically significant, risk of severe cases with vitamin D supplementation among patients with levels <20ng/mL or <12ng/mL. For <30ng/mL, lower (but not statistically significant) risk was seen overall but not for ≥50,000IU (the sample size is not given, it may be extremely small for this case). Only minimal details for <30ng/mL are provided, and no details for <20ng/mL or <12ng/mL are provided. The potential effect of supplementation on the risk of a case severe enough for hospitalization is not included.
This is the 33rd of 138 COVID-19 controlled studies for vitamin D, which collectively show efficacy with p<0.0000000001.
41 studies are RCTs, which show efficacy with p=0.00000049.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of severe case, 30.8% lower, RR 0.69, p = 0.25, treatment 65, control 64, odds ratio converted to relative risk, ≥1,000IU, control prevalence approximated with overall prevalence.
|
|
risk of severe case, 40.0% lower, RR 0.60, p = 0.15, treatment 65, control 64, odds ratio converted to relative risk, ≥5,000IU, control prevalence approximated with overall prevalence.
|
|
risk of severe case, no change, RR 1.00, p = 0.92, treatment 65, control 64, odds ratio converted to relative risk, ≥50,000IU, control prevalence approximated with overall prevalence.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Levitus et al., 3 May 2021, retrospective, USA, peer-reviewed, 9 authors, dosage varies.
{kind=link}
The Effect of Vitamin D Supplementation on Severe COVID-19 Outcomes in Patients With Vitamin D Insufficiency
doi:10.1210/jendso/bvab048
patients undergoing RYGB and SG, according to the time of surgery and percent weight loss. Methods: we studied 117 patients (91% female, 51% RYGB, mean age 41.8 ± 6.7 years, mean time of surgery 4.3 ± 3.4 years) who were divided into two groups according to the surgical procedure adopted (SG vs. RYGB). They were evaluated at different times after surgery (1-2 years, > 2 and <5 years and ≥5 years) and according to the percentage of weight loss (10-20%, >20% and <40%, ≥40%). Anthropometric measurements, body composition and BMD, bone parameters (PTH, corrected serum calcium, 25OHD, alkaline phosphatase -AP, C-telopeptide -CTX), and biochemical tests were compared. Results: The prevalence of SHPT (PTH ≥ 65pg/ml) was 26%, higher in the RYGB vs. SG (35% vs. 17%, respectively, p = 0.039), despite no significant differences in serum 25OHD (28.5 ± 7.3 vs. 27.6 ± 7.7 ng/ml, p=0.519) and corrected serum calcium (9.8 ± 0.6 vs. 9.8 ± 0.5 mg/dl, p = 0.466) between the groups. Mean serum PTH, CTX and AP was higher in the RYGB vs. SG (61.3 ± 29.5 vs 49.5 ± 32.3 pg/mL, p = 0.001; 0.596 ± 0.24 vs. 0.463 ± 0.23 ng/mL; 123.9 ± 60.8 vs. 100.7 ± 62.0 U/L, respectively). There were 13.5% decreases in femoral neck BMD in all patients, over the study period. After 5 years of surgery, the RYGB group showed greater bone loss in total body BMD (1.016 vs. 1.151g/cm 2 , -8.1%, p = 0.003) and total femur BMD (1.164 vs. 1.267g/cm 2 , -11.7%, p = 0.007). Mean serum leptin was lower in the RYGB group, when compared to SG (7.6 ± 5.8ng/mL vs. 14.0 ± 9.9, p = 0.001), with no correlation with BMD in any site. There were no significant differences between the RYGB and SG regarding the other metabolic parameters. Conclusion: We found a more deleterious effect of RYGB on bone health up to 5 years postoperatively in comparison with SG.