Vitamin D Deficiency and ARDS after SARS-CoV-2 Infection
et al., Irish Medical Journal, 113:5, 84, Jun 2020
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


{kind=link}
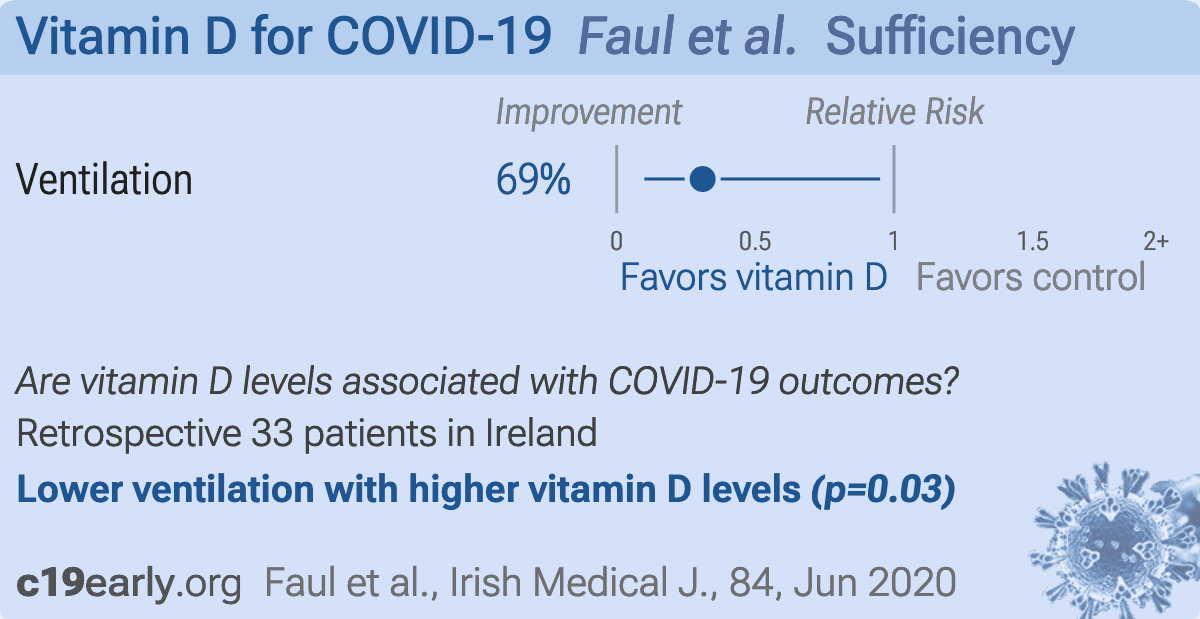
Analysis of 33 hospitalized COVID-19 patients with respiratory failure requiring FiO2 greater than 0.4.
Intubation hazard ratio for vitamin D sufficiency HR 0.31, p = 0.03.
This is the 5th of 232 COVID-19 sufficiency studies for vitamin D, which collectively show higher levels reduce risk with p<0.0000000001.
|
risk of mechanical ventilation, 69.0% lower, RR 0.31, p = 0.03, high D levels 4 of 21 (19.0%), low D levels 8 of 12 (66.7%), NNT 2.1, adjusted per study, >30nmol/L.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
Faul et al., 30 Jun 2020, retrospective, Ireland, peer-reviewed, 9 authors.
{kind=link}
Abstract: Issue: Ir Med J; Vol 113; No. 5; P84
Vitamin D Deficiency and ARDS after SARS-CoV-2 Infection
J.L. Faul1, C.P. Kerley1, B. Love2, E. O’Neill3, C. Cody4, W. Tormey5, K. Hutchinson6, L.J. Cormican1, C.M. Burke1
1.
2.
3.
4.
5.
6.
Asthma Research Centre, James Connolly Memorial Asthma Research Centre, Connolly Hospital
Blanchardstown, Ireland.
Department of Pharmacy, Connolly Hospital Blanchardstown, Ireland.
Department of Microbiology, Connolly Hospital Blanchardstown and Department of Clinical Microbiology,
Royal College of Surgeons in Ireland.
Department of Intensive Care Medicine, Connolly Hospital Blanchardstown, Ireland.
Department of Clinical Chemistry, Connolly Hospital Blanchardstown, Ireland.
Eurofins-Biomnis Limited, Sandyford, Dublin, Ireland.
In Response to Article Entitled ‘Optimisation of Vitamin D Status for Enhanced Immuno-Protection against Covid-19’ by D.M
McCartney et al - Ir Med J; Vol 113; No. 4; P58
Dear Sir,
Male gender, age over 40 years, cancer, diabetes mellitus, and chronic respiratory and cardiovascular disease have
each been associated with increased severity of disease, including ARDS, after SARS-CoV-2 infection.1,2 We
hypothesize that nutrition might also play a role. Vitamin D (25OHD) deficiency has previously been linked to a
greater susceptibility to viral infection, ARDS, and pneumonia.3,4 Since 25OHD deficiency is both highly prevalent and
easily treatable and the morbidity, mortality, and costs of SARS-CoV-2 related ARDS are great, we wanted to explore
whether 25OHD levels might be associated with an increased risk of the development of ARDS due to SARS-CoV-2.
Following institutional review board approval and informed consent from participants, we analyzed serum 25OHD
levels in 33 adult, male, Caucasian patients, over the age of 40 years, who were admitted to Connolly Hospital
Blanchardstown for SARS-CoV-2 related pneumonia (four quadrant infiltrates on chest radiograph, with respiratory
failure requiring FiO2 greater than 0.4, with SARS-CoV-2 detectable by RT-PCR of nasopharyngeal swab) during March
2020. None had cancer, diabetes mellitus, cardiovascular disease, or had received chronic immunosuppressive
therapy. Twelve progressed to ARDS and required intubation and mechanical ventilation. There were four deaths
after mechanical ventilation (at days 3, 6, 7, and 15) in the ARDS group and none in the non-ARDS group. Overall,
the twelve patients who progressed to ARDS (mean age 60 years, SD 15) had a lower serum 25OHD level on
presentation to hospital (mean = 27, SD = 12 nmol.l-1), compared to the twenty one patients hospitalized with less
severe pneumonia who did not progress to ARDS (mean age 56 years, SD 14). Their 25OHD level was 41 nmol.l-1 (SD
19) (p = 0.03).
Vitamin D (25OHD) deficiency is highly prevalent in Ireland, a country with low levels of sunlight. Using our measures
of 25OHD levels from 5374 Irish males aged between 40 and 60 years, the median is 47 nmol.l-1, with 31 and 65
nmol.l-1 representing the 25th and 75th centiles, respectively. We took a cutoff of 30 nmol.l-1, or less, as being very
likely to have Vitamin D deficiency. In this cohort of thirty three patients, twelve had a baseline 25OHD level less
than 30 nmol.l-1. In patients with SARS-CoV-2 related pneumonia a baseline serum 25OHD level less than 30 nmol.l-1
was associated with a hazard ratio (HR) for intubation of 3.19 (95 percent confidence interval, 1.05 to 9.7), (p = 0.03).
A plausible interpretation of these early..