The relationship between serum 25-hydroxyvitamin D levels and the severity of COVID-19 disease and its mortality
et al., Scientific Reports, doi:10.1038/s41598-021-97017-9, Jan 2021 (preprint)
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


{kind=link}
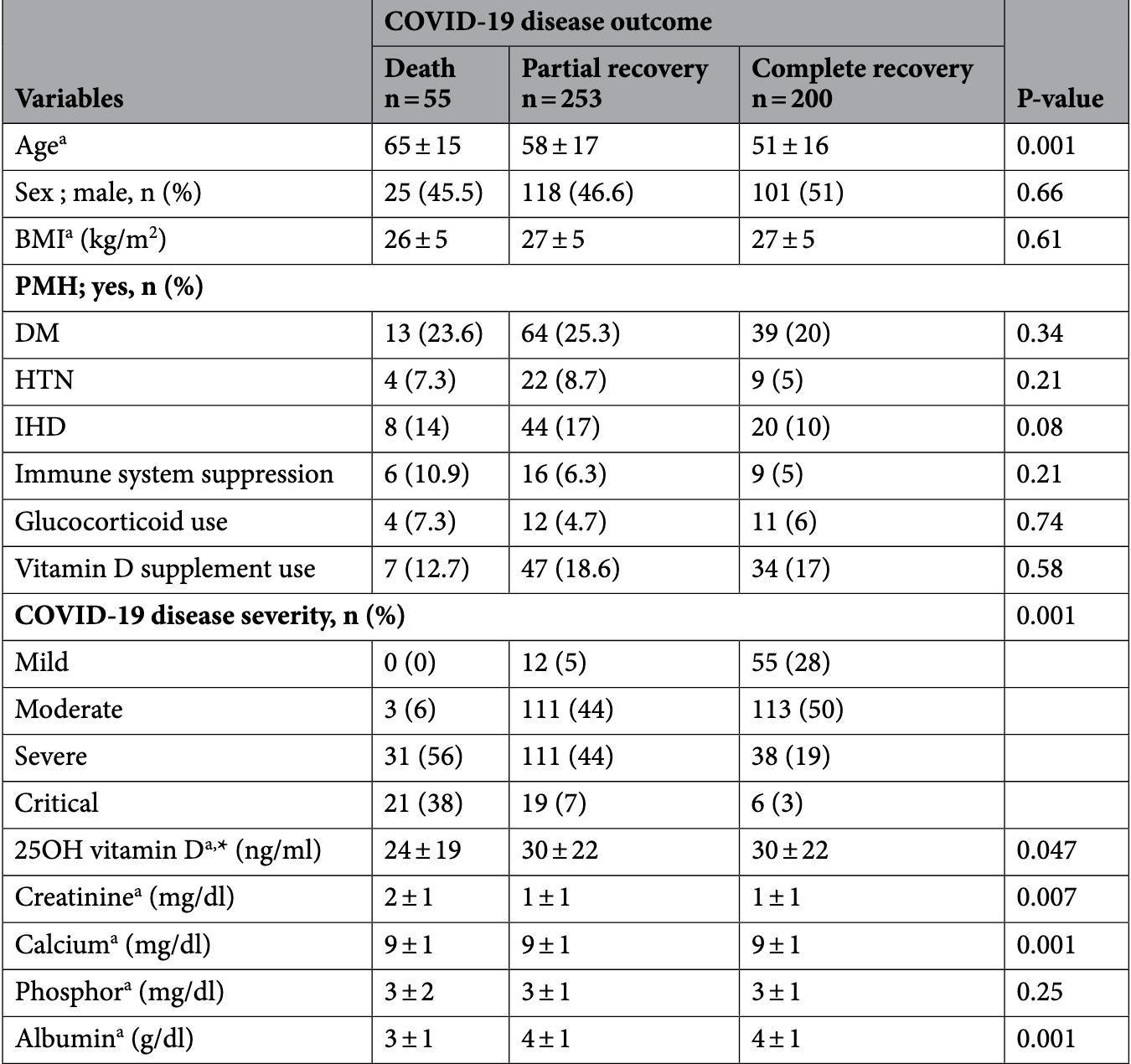
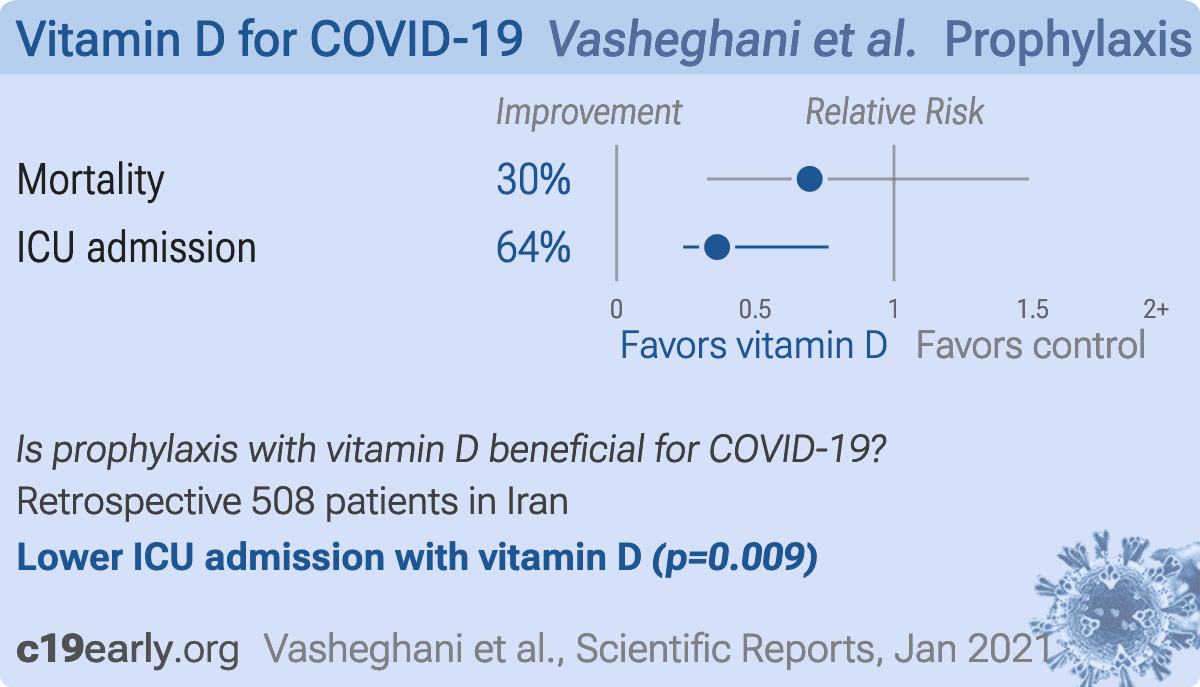
Retrospective 508 hospitalized COVID-19 patients in Iran showing lower mortality with vitamin D supplementation (not reaching statistical significance), and an association between lower vitamin D levels and disease severity, ICU admission, and increased mortality. Details of supplementation are not provided. The multivariate result for vitamin D deficiency is in the preprint, the journal version only contains the multivariate result for serum level.
This is the 18th of 138 COVID-19 controlled studies for vitamin D, which collectively show efficacy with p<0.0000000001.
41 studies are RCTs, which show efficacy with p=0.00000049.
|
risk of death, 30.4% lower, RR 0.70, p = 0.45, treatment 7 of 88 (8.0%), control 48 of 420 (11.4%), NNT 29, vitamin D supplementation.
|
|
risk of ICU admission, 63.8% lower, RR 0.36, p = 0.009, treatment 13 of 185 (7.0%), control 53 of 323 (16.4%), NNT 11, adjusted per study, inverted to make RR<1 favor treatment, vitamin D levels >30ng/mL.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Vasheghani et al., 18 Jan 2021, retrospective, Iran, preprint, 6 authors, dosage not specified.
{kind=link}
The relationship between serum 25-hydroxyvitamin D levels and the severity of COVID-19 disease and its mortality
Scientific Reports, doi:10.1038/s41598-021-97017-9
Supplemental vitamin D can reduce the risk and mortality of viral pneumonia. The relationship between 25 hydroxyvitamin D [25(OH)D] levels and the severity and mortality of Coronavirus disease 2019 (COVID-19) was evaluated. In this cross-sectional study, the admitted patients with COVID-19 were categorized as mild, moderate, severe, and critical based on clinical and radiologic characteristics. Calcium, phosphorus, albumin, creatinine, and serum 25(OH)D were measured and their correlation with the severity of disease and mortality were analyzed. During 2 months, 508 patients (442 patients in general wards and 66 patients in the intensive care unit (ICU)) were included. The participants were 56 ± 17 years old (52% male, 37% with comorbidity). Concerning severity, 13%, 42%, 36%, and 9% had mild, moderate, severe, and critical diseases, respectively. The mortality rate was 10.8%. Admission to ICU, severity of disease and mortality decreased significantly across quartiles of 25(OH)D. According to multivariate logistic regression analysis, disease mortality had a positive correlation with age and had a negative correlation with the serum level of 25(OH)D, calcium, and albumin. In hospitalized patients with COVID-19, low 25(OH)D was associated with severe disease and increased ICU admission and mortality rate. In late 2019, a new coronavirus was identified as a cause of a cluster of pneumonia cases in China which is named COVID-19 disease 1 . Currently, COVID-19 is pandemic 2 . In Iran, 612,772 people as the definitive cases of COVID-19 have been reported by November 10, 2020, and 34,864 people have died 3 . Manifestations of the COVID-19 range from asymptomatic carriers to acute respiratory failure and death 4 . Complications include acute respiratory failure, cytokine release syndrome, increased coagulation factors, and multi-organ damage which are associated with poor prognosis 5, 6 . The overall mortality rate until November 18, 2020, is about 2.4% (1,333,742 deaths between 55,326,907 patients) 7 . Old age, cardiovascular disease, diabetes, high blood pressure, chronic lung disease, cancer, chronic kidney disease, people with defective or suppressed immune systems, obesity, and chronic liver disease have been identified as risk factors for severe disease or mortality 4, 6, 8, 9 . There is currently no specific treatment against COVID-19 disease 10 . Currently, the most important way to deal with this disease is prevention and control of the conditions that are considered as a risk factor for the more severe course, and complications. There is evidence from influenza A and severe acute respiratory syndrome (SARS) epidemics suggesting a role for vitamin D in these diseases 11 . Previous studies have suggested an association between vitamin D deficiency and an increased chance of developing bacterial and/or viral pneumonia due to viruses such as SARS, MERS, and Influenza A. COVID-19 disease is more prevalent and severe in winter and is more common..
Author contributions M.V. designed and worked in all steps of project. She wrote the manuscript and reviewed it. She revised and edited the article in all steps; N.J. collected data; P.B. Analyzed data; MR: had done laboratory tests. She reviewed and edited manuscript. R.A.: Analyzed data, corrected manuscript after revision. M.M.: supervised investigation and edited the manuscript.
Funding The authors do not receive any funding for this study.
Competing interests The authors declare no competing interests.
References
Abate, Ahmed Ali, Mantfardo, Basu, Rate of intensive care unit admission and outcomes among patients with coronavirus: A systematic review and Meta-analysis, PLoS ONE, doi:10.1371/journal.pone.0235653
Adams, Baker, Sobieraj, myth busters: Dietary supplements and COVID-19, Ann. Pharmacother, doi:10.1177/1060028020928052
Ali, Role of vitamin D in preventing of COVID-19 infection, progression and severity, J Infect Public Health, doi:10.1016/j.jiph.2020.06.021
Annweiler, Vitamin D supplementation associated to better survival in hospitalized frail elderly COVID-19 patients: The GERIA-COVID quasi-experimental study, Nutrients, doi:10.3390/nu12113377
Araki, Vitamin D intoxication with severe hypercalcemia due to manufacturing and labeling errors of two dietary supplements made in the United States, J. Clin. Endocrinol. Metab, doi:10.1210/jc.2011-1443
Bajgain, Badal, Bajgain, Santana, Prevalence of comorbidities among individuals with COVID-19: A rapid review of current literature, Am. J. Infect. Control, doi:10.1016/j.ajic.2020.06.213
Bakhshayeshkaram, Haseli, Iranpour, Radiological mimickers of COVID-19 pneumonia: A pictorial review, Tanaffos
Baktash, Vitamin D status and outcomes for hospitalised older patients with COVID-19, Postgrad. Med. J, doi:10.1136/postgradmedj-2020-138712
Bassatne, The link between COVID-19 and VItamin D (VIVID): A systematic review and meta-analysis, Metabolism, doi:10.1016/j.metabol.2021.154753
Beard, Bearden, Striker, Vitamin D and the anti-viral state, J. Clin. Virol, doi:10.1016/j.jcv.2010.12.00
Blagosklonny, From causes of aging to death from COVID-19, Aging, doi:10.18632/aging.103493
Brandão, No association between vitamin D status and COVID-19 infection in São Paulo Brazil, Arch. Endocrinol. Metab, doi:10.20945/2359-3997000000343
Carpagnano, Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19, J. Endocrinol. Investig, doi:10.1007/s40618-020-01370-x
Castillo, Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study, J. Steroid Biochem. Mol. Biol, doi:10.1016/j.jsbmb.2020.105751
Cereda, Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Nutrition, doi:10.1016/j.nut.2020.111055
Chen, Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study, BMJ, doi:10.1136/bmj.m1091
D' Avolio, 25-Hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2, Nutrients, doi:10.3390/nu12051359
Ebadi, Montano-Loza, Perspective: Improving vitamin D status in the management of COVID-19, Eur. J. Clin. Nutr, doi:10.1038/s41430-020-0661-0
Ejtahed, Shab-Bidar, Hosseinpanah, Mirmiran, Azizi, Estimation of vitamin D intake based on a scenario for fortification of dairy products with vitamin D in a tehranian population, Iran. J. Am. Coll. Nutr, doi:10.1080/07315724.2015.1022269
Ferrari, Locatelli, No significant association between vitamin D and COVID-19. A retrospective study from a northern Italian hospital, Int. J. Vitam. Nutr. Res, doi:10.1024/0300-9831/a000687
French, Mcdonnell, Vieth, 25-Hydroxyvitamin D variability within-person due to diurnal rhythm and illness: A case report, J. Med. Case Rep, doi:10.1186/s13256-018-1948-9
Garcia, Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort, doi:10.1016/j.eclinm.2020.100449
Gebhard, Regitz-Zagrosek, Neuhauser, Morgan, Klein, Impact of sex and gender on COVID-19 outcomes in Europe, Biol. Sex Differ, doi:10.1186/s13293-020-00304-9
Giustina, Consensus statement from 2nd international conference on controversies in vitamin D, Rev. Endocr. Metab. Disord, doi:10.1007/s11154-019-09532-w
Grant, Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths, Nutrients, doi:10.3390/nu12040988
Greiller, Martineau, Modulation of the immune response to respiratory viruses by vitamin D, Nutrients, doi:10.3390/nu7064240
Griffin, Vitamin D and COVID-19: Evidence and recommendations for supplementation, R. Soc. Open Sci, doi:10.1098/rsos.201912
Holick, The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention, Rev. Endocr. Metab. Disord, doi:10.1007/s11154-017-9424-1
Huang, Hypoalbuminemia predicts the outcome of COVID-19 independent of age and co-morbidity, J. Med. Virol, doi:10.1002/jmv.26003
Jain, Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers, Sci. Rep, doi:10.1038/s41598-020-77093-z
Jevalikar, Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID-19, Sci Rep, doi:10.1038/s41598-021-85809-y
Kabootari, Akbarpour, Azizi, Hadaegh, Sex specific impact of different obesity phenotypes on the risk of incident hypertension: Tehran lipid and glucose study, Nutr. Metab. (Lond.), doi:10.1186/s12986-019-0340-0
Kim, Meza, Clarke, Kim, Hickner, Vitamin D and endothelial function, Nutrients, doi:10.3390/nu12020575
Ling, High-dose cholecalciferol booster therapy is associated with a reduced risk of mortality in patients with COVID-19: A cross-sectional multi-centre observational study, Nutrients, doi:10.3390/nu12123799
Mahmoudi, Rezaei, Mansouri, Marjani, Mansouri, Immunologic features in coronavirus disease 2019: Functional exhaustion of T cells and cytokine storm, J. Clin. Immunol, doi:10.1007/s10875-020-00824-4
Malacova, Prevalence and predictors of vitamin D deficiency in a nationally representative sample of adults participating in the 2011-2013 Australian Health Survey, Br. J. Nutr, doi:10.1017/S0007114519000151
Mamani, Muceli, Ghasemi Basir, Vasheghani, Poorolajal, Association between serum concentration of 25-hydroxyvitamin D and community-acquired pneumonia: A case-control study, Int. J. Gen. Med, doi:10.2147/IJGM.S149049
Mccartney, Byrne, Optimization of vitamin D status for enhanced immuno-protection against COVID-19, Iran. Med. J
Meltzer, Association of vitamin D status and other clinical characteristics with COVID-19 test results, JAMA Netw. Open, doi:10.1001/jamanetworkopen.2020.19722
Miroliaee, Salamzadeh, Shokouhi, Sahraei, The study of vitamin D administration effect on CRP and Interleukin-6 as prognostic biomarkers of ventilator associated pneumonia, J. Crit. Care, doi:10.1016/j.jcrc.2017.08.040
Onder, Rezza, Brusaferro, Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy, JAMA, doi:10.1001/jama.2020.4683
Panagiotou, Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalized with COVID-19 are associated with greater disease severity, Clin. Endocrinol, doi:10.1111/cen.14276
Pereira, Dantas Damascena, Galvão Azevedo, De Almeida, Da Mota, Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis, Crit. Rev. Food Sci. Nutr, doi:10.1080/10408398.2020.1841090
Price-Haywood, Burton, Fort, Seoane, Hospitalization and mortality among black patients and white patients with COVID-19, N. Engl. J. Med, doi:10.1056/NEJMsa2011686
Radujkovic, Vitamin D deficiency and outcome of COVID-19 patients, Nutrients, doi:10.3390/nu12092757
Richardson, Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area, JAMA, doi:10.1001/jama.2020.6775
Shim, Tariq, Choi, Lee, Chowell, Transmission potential and severity of COVID-19 in South Korea, Int. J. Infect. Dis, doi:10.1016/j.ijid.2020.03.031
Smolders, Van Den Ouweland, Geven, Pickkers, Kox, Letter to the Editor: Vitamin D deficiency in COVID-19: Mixing up cause and consequence, Metabolism, doi:10.1016/j.metabol.2020.154434
Sun, Serum calcium as a biomarker of clinical severity and prognosis in patients with coronavirus disease 2019, Aging, doi:10.18632/aging.103526
Tabrizi, High prevalence of vitamin D deficiency among iranian population: A systematic review and meta-analysis, Iran. J. Med. Sci
Van Schoor, Lips, Global overview of vitamin D status, Endocrinol. Metab. Clin. N. Am, doi:10.1016/j.ecl.2017.07.002
Vatandost, Prevalence of vitamin D deficiency in Iran: A systematic review and meta-analysis, Nutr. Health, doi:10.1177/0260106018802968
Wang, Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China, JAMA, doi:10.1001/jama.2020.1585
Wiersinga, Rhodes, Cheng, Peacock, Prescott, Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review, JAMA, doi:10.1001/jama.2020.12839
Wong, Saier, The SARS-coronavirus infection cycle: A survey of viral membrane proteins, their functional interactions and pathogenesis, Int. J. Mol. Sci, doi:10.3390/ijms22031308
Wu, Mcgoogan, Characteristics of and important lessons from the coronavirus disease, doi:10.1001/jama.2020.2648
Yang, Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and metaanalysis, Int. J. Infect. Dis, doi:10.1016/j.ijid.2020.03.017
Yuen, Ye, Fung, Chan, Jin, SARS-CoV-2 and COVID-19: The most important research questions, Cell Biosci, doi:10.1186/s13578-020-00404-4
Zheng, Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis, J. Infect, doi:10.1016/j.jinf.2020.04.021
Zheng, Vitamin D attenuates lung injury via stimulating epithelial repair, reducing epithelial cell apoptosis and inhibits TGF-β induced epithelial to mesenchymal transition, Biochem. Pharmacol, doi:10.1016/j.bcp.2020.113955
DOI record:
{
"DOI": "10.1038/s41598-021-97017-9",
"ISSN": [
"2045-2322"
],
"URL": "http://dx.doi.org/10.1038/s41598-021-97017-9",
"abstract": "<jats:title>Abstract</jats:title><jats:p>Supplemental vitamin D can reduce the risk and mortality of viral pneumonia. The relationship between 25 hydroxyvitamin D [25(OH)D] levels and the severity and mortality of Coronavirus disease 2019 (COVID-19) was evaluated. In this cross-sectional study, the admitted patients with COVID-19 were categorized as mild, moderate, severe, and critical based on clinical and radiologic characteristics. Calcium, phosphorus, albumin, creatinine, and serum 25(OH)D were measured and their correlation with the severity of disease and mortality were analyzed. During 2 months, 508 patients (442 patients in general wards and 66 patients in the intensive care unit (ICU)) were included. The participants were 56 ± 17 years old (52% male, 37% with comorbidity). Concerning severity, 13%, 42%, 36%, and 9% had mild, moderate, severe, and critical diseases, respectively. The mortality rate was 10.8%. Admission to ICU, severity of disease and mortality decreased significantly across quartiles of 25(OH)D. According to multivariate logistic regression analysis, disease mortality had a positive correlation with age and had a negative correlation with the serum level of 25(OH)D, calcium, and albumin. In hospitalized patients with COVID-19, low 25(OH)D was associated with severe disease and increased ICU admission and mortality rate.</jats:p>",
"alternative-id": [
"97017"
],
"article-number": "17594",
"assertion": [
{
"group": {
"label": "Article History",
"name": "ArticleHistory"
},
"label": "Received",
"name": "received",
"order": 1,
"value": "5 January 2021"
},
{
"group": {
"label": "Article History",
"name": "ArticleHistory"
},
"label": "Accepted",
"name": "accepted",
"order": 2,
"value": "10 August 2021"
},
{
"group": {
"label": "Article History",
"name": "ArticleHistory"
},
"label": "First Online",
"name": "first_online",
"order": 3,
"value": "2 September 2021"
},
{
"group": {
"label": "Competing interests",
"name": "EthicsHeading"
},
"name": "Ethics",
"order": 1,
"value": "The authors declare no competing interests."
}
],
"author": [
{
"affiliation": [],
"family": "Vasheghani",
"given": "Maryam",
"sequence": "first"
},
{
"affiliation": [],
"family": "Jannati",
"given": "Nasrin",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Baghaei",
"given": "Parvaneh",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Rezaei",
"given": "Mitra",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Aliyari",
"given": "Roqayeh",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Marjani",
"given": "Majid",
"sequence": "additional"
}
],
"container-title": "Scientific Reports",
"container-title-short": "Sci Rep",
"content-domain": {
"crossmark-restriction": false,
"domain": [
"link.springer.com"
]
},
"created": {
"date-parts": [
[
2021,
9,
23
]
],
"date-time": "2021-09-23T14:32:14Z",
"timestamp": 1632407534000
},
"deposited": {
"date-parts": [
[
2022,
12,
3
]
],
"date-time": "2022-12-03T15:37:12Z",
"timestamp": 1670081832000
},
"indexed": {
"date-parts": [
[
2024,
3,
27
]
],
"date-time": "2024-03-27T18:34:07Z",
"timestamp": 1711564447598
},
"is-referenced-by-count": 19,
"issue": "1",
"issued": {
"date-parts": [
[
2021,
9,
2
]
]
},
"journal-issue": {
"issue": "1",
"published-online": {
"date-parts": [
[
2021,
12
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://creativecommons.org/licenses/by/4.0",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
9,
2
]
],
"date-time": "2021-09-02T00:00:00Z",
"timestamp": 1630540800000
}
},
{
"URL": "https://creativecommons.org/licenses/by/4.0",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
9,
2
]
],
"date-time": "2021-09-02T00:00:00Z",
"timestamp": 1630540800000
}
}
],
"link": [
{
"URL": "https://www.nature.com/articles/s41598-021-97017-9.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://www.nature.com/articles/s41598-021-97017-9",
"content-type": "text/html",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://www.nature.com/articles/s41598-021-97017-9.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "297",
"original-title": [],
"prefix": "10.1038",
"published": {
"date-parts": [
[
2021,
9,
2
]
]
},
"published-online": {
"date-parts": [
[
2021,
9,
2
]
]
},
"publisher": "Springer Science and Business Media LLC",
"reference": [
{
"author": "World Health Organization",
"key": "97017_CR1",
"unstructured": "World Health Organization. WHO Director-General’s Opening Remarks at the World Health Assembly—9 November 2020 (WHO, 2020).",
"volume-title": "WHO Director-General’s Opening Remarks at the World Health Assembly—9 November 2020",
"year": "2020"
},
{
"author": "World Health Organization",
"key": "97017_CR2",
"unstructured": "World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19) (WHO, 2020).",
"volume-title": "Rolling Updates on Coronavirus Disease (COVID-19)",
"year": "2020"
},
{
"DOI": "10.1596/34819",
"author": "World Health Organization",
"doi-asserted-by": "publisher",
"key": "97017_CR3",
"unstructured": "World Health Organization. Weekly Epidemiological Update—3 November 2020 (WHO, 2020).",
"volume-title": "Weekly Epidemiological Update—3 November 2020",
"year": "2020"
},
{
"DOI": "10.1001/jama.2020.2648",
"author": "Z Wu",
"doi-asserted-by": "publisher",
"journal-title": "JAMA",
"key": "97017_CR4",
"unstructured": "Wu, Z. & McGoogan, J. M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China summary of a report of 72,314 cases from the Chinese center for disease control and prevention. JAMA. https://doi.org/10.1001/jama.2020.2648 (2020).",
"year": "2020"
},
{
"DOI": "10.1001/jama.2020.1585",
"author": "D Wang",
"doi-asserted-by": "publisher",
"first-page": "1061",
"issue": "11",
"journal-title": "China. JAMA.",
"key": "97017_CR5",
"unstructured": "Wang, D. et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 323(11), 1061–1069. https://doi.org/10.1001/jama.2020.1585 (2020).",
"volume": "323",
"year": "2020"
},
{
"DOI": "10.1136/bmj.m1091",
"author": "T Chen",
"doi-asserted-by": "publisher",
"first-page": "m1091",
"journal-title": "BMJ",
"key": "97017_CR6",
"unstructured": "Chen, T. et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 368, m1091. https://doi.org/10.1136/bmj.m1091 (2020).",
"volume": "368",
"year": "2020"
},
{
"author": "World Health Organization",
"key": "97017_CR7",
"unstructured": "World Health Organization. Coronavirus Disease (COVID-19) Pandemic, Coronavirus Disease (COVID-19) Outbreak Situation (WHO, 2020).",
"volume-title": "Coronavirus Disease (COVID-19) Pandemic, Coronavirus Disease (COVID-19) Outbreak Situation",
"year": "2020"
},
{
"DOI": "10.1001/jama.2020.4683",
"author": "G Onder",
"doi-asserted-by": "publisher",
"journal-title": "JAMA",
"key": "97017_CR8",
"unstructured": "Onder, G., Rezza, G. & Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. https://doi.org/10.1001/jama.2020.4683 (2020).",
"year": "2020"
},
{
"DOI": "10.1016/j.ijid.2020.03.031",
"author": "E Shim",
"doi-asserted-by": "publisher",
"journal-title": "Int. J. Infect. Dis.",
"key": "97017_CR9",
"unstructured": "Shim, E., Tariq, A., Choi, W., Lee, Y. & Chowell, G. Transmission potential and severity of COVID-19 in South Korea. Int. J. Infect. Dis. https://doi.org/10.1016/j.ijid.2020.03.031 (2020).",
"year": "2020"
},
{
"DOI": "10.1186/s13578-020-00404-4",
"author": "KS Yuen",
"doi-asserted-by": "publisher",
"first-page": "40",
"journal-title": "Cell Biosci.",
"key": "97017_CR10",
"unstructured": "Yuen, K. S., Ye, Z. W., Fung, S. Y., Chan, C. P. & Jin, D. Y. SARS-CoV-2 and COVID-19: The most important research questions. Cell Biosci. 10, 40. https://doi.org/10.1186/s13578-020-00404-4 (2020).",
"volume": "10",
"year": "2020"
},
{
"DOI": "10.1098/rsos.201912",
"author": "G Griffin",
"doi-asserted-by": "publisher",
"first-page": "201912",
"issue": "12",
"journal-title": "R. Soc. Open Sci.",
"key": "97017_CR11",
"unstructured": "Griffin, G. et al. Vitamin D and COVID-19: Evidence and recommendations for supplementation. R. Soc. Open Sci. 7(12), 201912. https://doi.org/10.1098/rsos.201912 (2020).",
"volume": "7",
"year": "2020"
},
{
"DOI": "10.3390/nu12040988",
"author": "WB Grant",
"doi-asserted-by": "publisher",
"first-page": "E988",
"issue": "4",
"journal-title": "Nutrients",
"key": "97017_CR12",
"unstructured": "Grant, W. B. et al. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients 12(4), E988. https://doi.org/10.3390/nu12040988 (2020).",
"volume": "12",
"year": "2020"
},
{
"author": "DM McCartney",
"first-page": "58",
"issue": "4",
"journal-title": "Iran. Med. J.",
"key": "97017_CR13",
"unstructured": "McCartney, D. M. & Byrne, D. G. Optimization of vitamin D status for enhanced immuno-protection against COVID-19. Iran. Med. J. 113(4), 58 (2020).",
"volume": "113",
"year": "2020"
},
{
"author": "R Tabrizi",
"first-page": "125",
"issue": "2",
"journal-title": "Iran. J. Med. Sci.",
"key": "97017_CR14",
"unstructured": "Tabrizi, R. et al. High prevalence of vitamin D deficiency among iranian population: A systematic review and meta-analysis. Iran. J. Med. Sci. 43(2), 125–139 (2018).",
"volume": "43",
"year": "2018"
},
{
"key": "97017_CR15",
"unstructured": "https://www.siemens-healthineers.com/en-us/laboratory-diagnostics/assays-by-diseases-conditions/bone-metabolism-assays-global/vitamin-d-total-assay. Accessed 5 Jan 2021."
},
{
"author": "M Bakhshayeshkaram",
"first-page": "100",
"issue": "2",
"journal-title": "Tanaffos",
"key": "97017_CR16",
"unstructured": "Bakhshayeshkaram, M., Haseli, S. & Iranpour, P. Radiological mimickers of COVID-19 pneumonia: A pictorial review. Tanaffos 19(2), 100–107 (2020).",
"volume": "19",
"year": "2020"
},
{
"DOI": "10.2147/IJGM.S149049",
"author": "M Mamani",
"doi-asserted-by": "publisher",
"first-page": "423",
"journal-title": "Int. J. Gen. Med.",
"key": "97017_CR17",
"unstructured": "Mamani, M., Muceli, N., Ghasemi Basir, H. R., Vasheghani, M. & Poorolajal, J. Association between serum concentration of 25-hydroxyvitamin D and community-acquired pneumonia: A case-control study. Int. J. Gen. Med. 10, 423–429. https://doi.org/10.2147/IJGM.S149049 (2017).",
"volume": "10",
"year": "2017"
},
{
"DOI": "10.1007/s11154-017-9424-1",
"author": "MF Holick",
"doi-asserted-by": "publisher",
"first-page": "153",
"issue": "2",
"journal-title": "Rev. Endocr. Metab. Disord.",
"key": "97017_CR18",
"unstructured": "Holick, M. F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 18(2), 153–165. https://doi.org/10.1007/s11154-017-9424-1 (2017).",
"volume": "18",
"year": "2017"
},
{
"DOI": "10.1007/s11154-019-09532-w",
"author": "A Giustina",
"doi-asserted-by": "publisher",
"first-page": "89",
"issue": "1",
"journal-title": "Rev. Endocr. Metab. Disord.",
"key": "97017_CR19",
"unstructured": "Giustina, A. et al. Consensus statement from 2nd international conference on controversies in vitamin D. Rev. Endocr. Metab. Disord. 21(1), 89–116. https://doi.org/10.1007/s11154-019-09532-w (2020).",
"volume": "21",
"year": "2020"
},
{
"DOI": "10.1210/jc.2011-1443",
"author": "T Araki",
"doi-asserted-by": "publisher",
"first-page": "3603",
"issue": "12",
"journal-title": "J. Clin. Endocrinol. Metab.",
"key": "97017_CR20",
"unstructured": "Araki, T. et al. Vitamin D intoxication with severe hypercalcemia due to manufacturing and labeling errors of two dietary supplements made in the United States. J. Clin. Endocrinol. Metab. 96(12), 3603–3608. https://doi.org/10.1210/jc.2011-1443 (2011).",
"volume": "96",
"year": "2011"
},
{
"key": "97017_CR21",
"unstructured": "World Health Organization. Clinical Management of COVID-19. Interim Guidance. COVID-19: Clinical care. WHO/Publications/Overview/Clinical management of COVID-19. WHO Reference Number: WHO/2019-nCoV/clinical/2020.5 (2020). https://www.who.int/publications/i/item/clinical-management-of-COVID-19. Accessed 5 Jan 2021."
},
{
"DOI": "10.1186/s12986-019-0340-0",
"author": "M Kabootari",
"doi-asserted-by": "publisher",
"first-page": "16",
"journal-title": "Nutr. Metab. (Lond.).",
"key": "97017_CR22",
"unstructured": "Kabootari, M., Akbarpour, S., Azizi, F. & Hadaegh, F. Sex specific impact of different obesity phenotypes on the risk of incident hypertension: Tehran lipid and glucose study. Nutr. Metab. (Lond.). 16, 16. https://doi.org/10.1186/s12986-019-0340-0 (2019).",
"volume": "16",
"year": "2019"
},
{
"DOI": "10.1056/NEJMsa2011686",
"author": "EG Price-Haywood",
"doi-asserted-by": "publisher",
"first-page": "2534",
"issue": "26",
"journal-title": "N. Engl. J. Med.",
"key": "97017_CR23",
"unstructured": "Price-Haywood, E. G., Burton, J., Fort, D. & Seoane, L. Hospitalization and mortality among black patients and white patients with COVID-19. N. Engl. J. Med. 382(26), 2534–2543. https://doi.org/10.1056/NEJMsa2011686 (2020).",
"volume": "382",
"year": "2020"
},
{
"DOI": "10.1016/j.jinf.2020.04.021",
"author": "Z Zheng",
"doi-asserted-by": "publisher",
"first-page": "e16",
"issue": "2",
"journal-title": "J. Infect.",
"key": "97017_CR24",
"unstructured": "Zheng, Z. et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 81(2), e16–e25. https://doi.org/10.1016/j.jinf.2020.04.021 (2020).",
"volume": "81",
"year": "2020"
},
{
"DOI": "10.18632/aging.103493",
"author": "MV Blagosklonny",
"doi-asserted-by": "publisher",
"first-page": "10004",
"issue": "11",
"journal-title": "Aging (Albany NY).",
"key": "97017_CR25",
"unstructured": "Blagosklonny, M. V. From causes of aging to death from COVID-19. Aging (Albany NY). 12(11), 10004–10021. https://doi.org/10.18632/aging.103493 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1186/s13293-020-00304-9",
"author": "C Gebhard",
"doi-asserted-by": "publisher",
"first-page": "29",
"issue": "1",
"journal-title": "Biol. Sex Differ.",
"key": "97017_CR26",
"unstructured": "Gebhard, C., Regitz-Zagrosek, V., Neuhauser, H. K., Morgan, R. & Klein, S. L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol. Sex Differ. 11(1), 29. https://doi.org/10.1186/s13293-020-00304-9 (2020).",
"volume": "11",
"year": "2020"
},
{
"DOI": "10.1016/j.ajic.2020.06.213",
"author": "KT Bajgain",
"doi-asserted-by": "publisher",
"first-page": "238",
"issue": "2",
"journal-title": "Am. J. Infect. Control.",
"key": "97017_CR27",
"unstructured": "Bajgain, K. T., Badal, S., Bajgain, B. B. & Santana, M. J. Prevalence of comorbidities among individuals with COVID-19: A rapid review of current literature. Am. J. Infect. Control. 49(2), 238–246. https://doi.org/10.1016/j.ajic.2020.06.213 (2021).",
"volume": "49",
"year": "2021"
},
{
"DOI": "10.1016/j.ijid.2020.03.017",
"author": "J Yang",
"doi-asserted-by": "publisher",
"first-page": "91",
"journal-title": "Int. J. Infect. Dis.",
"key": "97017_CR28",
"unstructured": "Yang, J. et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 94, 91–95. https://doi.org/10.1016/j.ijid.2020.03.017 (2020).",
"volume": "94",
"year": "2020"
},
{
"DOI": "10.1016/j.eclinm.2020.100449",
"author": "PD Wendel Garcia",
"doi-asserted-by": "publisher",
"journal-title": "EClinicalMedicine.",
"key": "97017_CR29",
"unstructured": "Wendel Garcia, P. D. et al. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine. https://doi.org/10.1016/j.eclinm.2020.100449 (2020).",
"year": "2020"
},
{
"DOI": "10.1001/jama.2020.6775",
"doi-asserted-by": "publisher",
"key": "97017_CR30",
"unstructured": "Richardson, S., et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 323(20), 2052–2059 (2020). https://doi.org/10.1001/jama.2020.6775. Erratum in: JAMA 323(20), 2098 (2020)."
},
{
"key": "97017_CR31",
"unstructured": "https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports. Accessed 5 Jan 2021."
},
{
"key": "97017_CR32",
"unstructured": "The Ministry of Health of Iran. Identification of 13843 New Patients with Covid 19 in the Country/5832 Patients are Admitted to the Intensive Care Unit, Number 217880. https://behdasht.gov.ir/news/NEWS. Accessed 5 Jan 2021."
},
{
"DOI": "10.1001/jama.2020.12839",
"author": "WJ Wiersinga",
"doi-asserted-by": "publisher",
"first-page": "782",
"issue": "8",
"journal-title": "JAMA",
"key": "97017_CR33",
"unstructured": "Wiersinga, W. J., Rhodes, A., Cheng, A. C., Peacock, S. J. & Prescott, H. C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 324(8), 782–793. https://doi.org/10.1001/jama.2020.12839 (2020).",
"volume": "324",
"year": "2020"
},
{
"DOI": "10.1371/journal.pone.0235653",
"author": "SM Abate",
"doi-asserted-by": "publisher",
"first-page": "e0235653",
"issue": "7",
"journal-title": "PLoS ONE",
"key": "97017_CR34",
"unstructured": "Abate, S. M., Ahmed Ali, S., Mantfardo, B. & Basu, B. Rate of intensive care unit admission and outcomes among patients with coronavirus: A systematic review and Meta-analysis. PLoS ONE 15(7), e0235653. https://doi.org/10.1371/journal.pone.0235653 (2020).",
"volume": "15",
"year": "2020"
},
{
"DOI": "10.1016/j.ecl.2017.07.002",
"author": "N van Schoor",
"doi-asserted-by": "publisher",
"first-page": "845",
"issue": "4",
"journal-title": "Endocrinol. Metab. Clin. N. Am.",
"key": "97017_CR35",
"unstructured": "van Schoor, N. & Lips, P. Global overview of vitamin D status. Endocrinol. Metab. Clin. N. Am. 46(4), 845–870. https://doi.org/10.1016/j.ecl.2017.07.002 (2017).",
"volume": "46",
"year": "2017"
},
{
"DOI": "10.1177/0260106018802968",
"author": "S Vatandost",
"doi-asserted-by": "publisher",
"first-page": "269",
"issue": "4",
"journal-title": "Nutr. Health",
"key": "97017_CR36",
"unstructured": "Vatandost, S. et al. Prevalence of vitamin D deficiency in Iran: A systematic review and meta-analysis. Nutr. Health 24(4), 269–278. https://doi.org/10.1177/0260106018802968 (2018).",
"volume": "24",
"year": "2018"
},
{
"DOI": "10.1080/07315724.2015.1022269",
"author": "HS Ejtahed",
"doi-asserted-by": "publisher",
"first-page": "383",
"issue": "5",
"journal-title": "Iran. J. Am. Coll. Nutr.",
"key": "97017_CR37",
"unstructured": "Ejtahed, H. S., Shab-Bidar, S., Hosseinpanah, F., Mirmiran, P. & Azizi, F. Estimation of vitamin D intake based on a scenario for fortification of dairy products with vitamin D in a tehranian population. Iran. J. Am. Coll. Nutr. 35(5), 383–391. https://doi.org/10.1080/07315724.2015.1022269 (2016).",
"volume": "35",
"year": "2016"
},
{
"DOI": "10.18632/aging.103526",
"author": "JK Sun",
"doi-asserted-by": "publisher",
"first-page": "11287",
"issue": "12",
"journal-title": "Aging (Albany NY).",
"key": "97017_CR38",
"unstructured": "Sun, J. K. et al. Serum calcium as a biomarker of clinical severity and prognosis in patients with coronavirus disease 2019. Aging (Albany NY). 12(12), 11287–11295. https://doi.org/10.18632/aging.103526 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1002/jmv.26003",
"author": "J Huang",
"doi-asserted-by": "publisher",
"journal-title": "J. Med. Virol.",
"key": "97017_CR39",
"unstructured": "Huang, J. et al. Hypoalbuminemia predicts the outcome of COVID-19 independent of age and co-morbidity. J. Med. Virol. https://doi.org/10.1002/jmv.26003 (2020).",
"year": "2020"
},
{
"DOI": "10.1038/s41598-020-77093-z",
"author": "A Jain",
"doi-asserted-by": "publisher",
"first-page": "20191",
"issue": "1",
"journal-title": "Sci. Rep.",
"key": "97017_CR40",
"unstructured": "Jain, A. et al. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 10(1), 20191. https://doi.org/10.1038/s41598-020-77093-z (2020).",
"volume": "10",
"year": "2020"
},
{
"DOI": "10.1136/postgradmedj-2020-138712",
"author": "V Baktash",
"doi-asserted-by": "publisher",
"journal-title": "Postgrad. Med. J.",
"key": "97017_CR41",
"unstructured": "Baktash, V. et al. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad. Med. J. https://doi.org/10.1136/postgradmedj-2020-138712 (2020).",
"year": "2020"
},
{
"DOI": "10.1038/s41598-021-85809-y",
"author": "G Jevalikar",
"doi-asserted-by": "publisher",
"first-page": "6258",
"issue": "1",
"journal-title": "Sci Rep.",
"key": "97017_CR42",
"unstructured": "Jevalikar, G. et al. Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID-19. Sci Rep. 11(1), 6258. https://doi.org/10.1038/s41598-021-85809-y (2021).",
"volume": "11",
"year": "2021"
},
{
"DOI": "10.1111/cen.14276",
"author": "G Panagiotou",
"doi-asserted-by": "publisher",
"journal-title": "Clin. Endocrinol. (Oxf.).",
"key": "97017_CR43",
"unstructured": "Panagiotou, G. et al. Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalized with COVID-19 are associated with greater disease severity. Clin. Endocrinol. (Oxf.). https://doi.org/10.1111/cen.14276 (2020).",
"year": "2020"
},
{
"DOI": "10.1016/j.jsbmb.2020.105751",
"author": "M Entrenas Castillo",
"doi-asserted-by": "publisher",
"first-page": "105751",
"journal-title": "J. Steroid Biochem. Mol. Biol.",
"key": "97017_CR44",
"unstructured": "Entrenas Castillo, M. et al. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 203, 105751. https://doi.org/10.1016/j.jsbmb.2020.105751 (2020).",
"volume": "203",
"year": "2020"
},
{
"DOI": "10.3390/nu12123799",
"author": "SF Ling",
"doi-asserted-by": "publisher",
"first-page": "3799",
"issue": "12",
"journal-title": "Nutrients",
"key": "97017_CR45",
"unstructured": "Ling, S. F. et al. High-dose cholecalciferol booster therapy is associated with a reduced risk of mortality in patients with COVID-19: A cross-sectional multi-centre observational study. Nutrients 12(12), 3799. https://doi.org/10.3390/nu12123799 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.3390/nu12113377",
"author": "G Annweiler",
"doi-asserted-by": "publisher",
"first-page": "3377",
"issue": "11",
"journal-title": "Nutrients",
"key": "97017_CR46",
"unstructured": "Annweiler, G. et al. Vitamin D supplementation associated to better survival in hospitalized frail elderly COVID-19 patients: The GERIA-COVID quasi-experimental study. Nutrients 12(11), 3377. https://doi.org/10.3390/nu12113377 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.3390/nu12051359",
"author": "A D'Avolio",
"doi-asserted-by": "publisher",
"first-page": "1359",
"issue": "5",
"journal-title": "Nutrients",
"key": "97017_CR47",
"unstructured": "D’Avolio, A. et al. 25-Hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2. Nutrients 12(5), 1359. https://doi.org/10.3390/nu12051359 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1016/j.nut.2020.111055",
"author": "E Cereda",
"doi-asserted-by": "publisher",
"first-page": "111055",
"journal-title": "Nutrition",
"key": "97017_CR48",
"unstructured": "Cereda, E. et al. Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy. Nutrition 82, 111055. https://doi.org/10.1016/j.nut.2020.111055 (2020).",
"volume": "82",
"year": "2020"
},
{
"DOI": "10.3390/nu12092757",
"author": "A Radujkovic",
"doi-asserted-by": "publisher",
"first-page": "2757",
"issue": "9",
"journal-title": "Nutrients",
"key": "97017_CR49",
"unstructured": "Radujkovic, A. et al. Vitamin D deficiency and outcome of COVID-19 patients. Nutrients 12(9), 2757. https://doi.org/10.3390/nu12092757 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1001/jamanetworkopen.2020.19722",
"author": "DO Meltzer",
"doi-asserted-by": "publisher",
"first-page": "e2019722",
"issue": "9",
"journal-title": "JAMA Netw. Open",
"key": "97017_CR50",
"unstructured": "Meltzer, D. O. et al. Association of vitamin D status and other clinical characteristics with COVID-19 test results. JAMA Netw. Open 3(9), e2019722. https://doi.org/10.1001/jamanetworkopen.2020.19722 (2020).",
"volume": "3",
"year": "2020"
},
{
"DOI": "10.1080/10408398.2020.1841090",
"author": "M Pereira",
"doi-asserted-by": "publisher",
"journal-title": "Crit. Rev. Food Sci. Nutr.",
"key": "97017_CR51",
"unstructured": "Pereira, M., Dantas Damascena, A., Galvão Azevedo, L. M., de Almeida, O. T. & da Mota, S. J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. https://doi.org/10.1080/10408398.2020.1841090 (2020).",
"year": "2020"
},
{
"DOI": "10.1007/s40618-020-01370-x",
"author": "GE Carpagnano",
"doi-asserted-by": "publisher",
"first-page": "765",
"issue": "4",
"journal-title": "J. Endocrinol. Investig.",
"key": "97017_CR52",
"unstructured": "Carpagnano, G. E. et al. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 44(4), 765–771. https://doi.org/10.1007/s40618-020-01370-x (2021).",
"volume": "44",
"year": "2021"
},
{
"DOI": "10.20945/2359-3997000000343",
"author": "CMÁ Brandão",
"doi-asserted-by": "publisher",
"journal-title": "Arch. Endocrinol. Metab.",
"key": "97017_CR53",
"unstructured": "Brandão, C. M. Á. et al. No association between vitamin D status and COVID-19 infection in São Paulo Brazil. Arch. Endocrinol. Metab. https://doi.org/10.20945/2359-3997000000343 (2021).",
"year": "2021"
},
{
"DOI": "10.1024/0300-9831/a000687",
"author": "D Ferrari",
"doi-asserted-by": "publisher",
"journal-title": "Int. J. Vitam. Nutr. Res.",
"key": "97017_CR54",
"unstructured": "Ferrari, D. & Locatelli, M. No significant association between vitamin D and COVID-19. A retrospective study from a northern Italian hospital. Int. J. Vitam. Nutr. Res. https://doi.org/10.1024/0300-9831/a000687 (2020).",
"year": "2020"
},
{
"DOI": "10.1177/1060028020928052",
"author": "KK Adams",
"doi-asserted-by": "publisher",
"first-page": "820",
"issue": "8",
"journal-title": "Ann. Pharmacother.",
"key": "97017_CR55",
"unstructured": "Adams, K. K. & Baker, W. L. Sobieraj DM myth busters: Dietary supplements and COVID-19. Ann. Pharmacother. 54(8), 820–826. https://doi.org/10.1177/1060028020928052 (2020).",
"volume": "54",
"year": "2020"
},
{
"DOI": "10.1007/s10875-020-00824-4",
"author": "S Mahmoudi",
"doi-asserted-by": "publisher",
"first-page": "974",
"issue": "7",
"journal-title": "J. Clin. Immunol.",
"key": "97017_CR56",
"unstructured": "Mahmoudi, S., Rezaei, M., Mansouri, N., Marjani, M. & Mansouri, D. Immunologic features in coronavirus disease 2019: Functional exhaustion of T cells and cytokine storm. J. Clin. Immunol. 40(7), 974–976. https://doi.org/10.1007/s10875-020-00824-4 (2020).",
"volume": "40",
"year": "2020"
},
{
"DOI": "10.1016/j.jiph.2020.06.021",
"author": "N Ali",
"doi-asserted-by": "publisher",
"journal-title": "J Infect Public Health.",
"key": "97017_CR57",
"unstructured": "Ali, N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J Infect Public Health. https://doi.org/10.1016/j.jiph.2020.06.021 (2020).",
"year": "2020"
},
{
"DOI": "10.1016/j.jcv.2010.12.00",
"author": "JA Beard",
"doi-asserted-by": "publisher",
"first-page": "194",
"issue": "3",
"journal-title": "J. Clin. Virol.",
"key": "97017_CR58",
"unstructured": "Beard, J. A., Bearden, A. & Striker, R. Vitamin D and the anti-viral state. J. Clin. Virol. 50(3), 194–200. https://doi.org/10.1016/j.jcv.2010.12.00 (2011).",
"volume": "50",
"year": "2011"
},
{
"DOI": "10.1038/s41430-020-0661-0",
"author": "M Ebadi",
"doi-asserted-by": "publisher",
"first-page": "856",
"issue": "6",
"journal-title": "Eur. J. Clin. Nutr.",
"key": "97017_CR59",
"unstructured": "Ebadi, M. & Montano-Loza, A. J. Perspective: Improving vitamin D status in the management of COVID-19. Eur. J. Clin. Nutr. 74(6), 856–859. https://doi.org/10.1038/s41430-020-0661-0 (2020).",
"volume": "74",
"year": "2020"
},
{
"DOI": "10.3390/ijms22031308",
"author": "NA Wong",
"doi-asserted-by": "publisher",
"first-page": "1308",
"issue": "3",
"journal-title": "Int. J. Mol. Sci.",
"key": "97017_CR60",
"unstructured": "Wong, N. A. & Saier, M. H. Jr. The SARS-coronavirus infection cycle: A survey of viral membrane proteins, their functional interactions and pathogenesis. Int. J. Mol. Sci. 22(3), 1308. https://doi.org/10.3390/ijms22031308 (2021).",
"volume": "22",
"year": "2021"
},
{
"DOI": "10.3390/nu7064240",
"author": "CL Greiller",
"doi-asserted-by": "publisher",
"first-page": "4240",
"issue": "6",
"journal-title": "Nutrients",
"key": "97017_CR61",
"unstructured": "Greiller, C. L. & Martineau, A. R. Modulation of the immune response to respiratory viruses by vitamin D. Nutrients 7(6), 4240–4270. https://doi.org/10.3390/nu7064240 (2015).",
"volume": "7",
"year": "2015"
},
{
"DOI": "10.1016/j.jcrc.2017.08.040",
"author": "AE Miroliaee",
"doi-asserted-by": "publisher",
"first-page": "300",
"journal-title": "J. Crit. Care",
"key": "97017_CR62",
"unstructured": "Miroliaee, A. E., Salamzadeh, J., Shokouhi, S. & Sahraei, Z. The study of vitamin D administration effect on CRP and Interleukin-6 as prognostic biomarkers of ventilator associated pneumonia. J. Crit. Care 44, 300–305. https://doi.org/10.1016/j.jcrc.2017.08.040 (2018).",
"volume": "44",
"year": "2018"
},
{
"DOI": "10.3390/nu12020575",
"author": "DH Kim",
"doi-asserted-by": "publisher",
"first-page": "575",
"issue": "2",
"journal-title": "Nutrients",
"key": "97017_CR63",
"unstructured": "Kim, D. H., Meza, C. A., Clarke, H., Kim, J. S. & Hickner, R. C. Vitamin D and endothelial function. Nutrients 12(2), 575. https://doi.org/10.3390/nu12020575 (2020).",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1016/j.bcp.2020.113955",
"author": "S Zheng",
"doi-asserted-by": "publisher",
"first-page": "113955",
"journal-title": "Biochem. Pharmacol.",
"key": "97017_CR64",
"unstructured": "Zheng, S. et al. Vitamin D attenuates lung injury via stimulating epithelial repair, reducing epithelial cell apoptosis and inhibits TGF-β induced epithelial to mesenchymal transition. Biochem. Pharmacol. 177, 113955. https://doi.org/10.1016/j.bcp.2020.113955 (2020).",
"volume": "177",
"year": "2020"
},
{
"DOI": "10.1016/j.metabol.2021.154753",
"author": "A Bassatne",
"doi-asserted-by": "publisher",
"journal-title": "Metabolism",
"key": "97017_CR65",
"unstructured": "Bassatne, A. et al. The link between COVID-19 and VItamin D (VIVID): A systematic review and meta-analysis. Metabolism. https://doi.org/10.1016/j.metabol.2021.154753 (2021).",
"year": "2021"
},
{
"DOI": "10.1016/j.metabol.2020.154434",
"author": "J Smolders",
"doi-asserted-by": "publisher",
"first-page": "154434",
"journal-title": "Metabolism",
"key": "97017_CR66",
"unstructured": "Smolders, J., van den Ouweland, J., Geven, C., Pickkers, P. & Kox, M. Letter to the Editor: Vitamin D deficiency in COVID-19: Mixing up cause and consequence. Metabolism 115, 154434. https://doi.org/10.1016/j.metabol.2020.154434 (2021).",
"volume": "115",
"year": "2021"
},
{
"DOI": "10.1186/s13256-018-1948-9",
"author": "CB French",
"doi-asserted-by": "publisher",
"first-page": "29",
"issue": "1",
"journal-title": "J. Med. Case Rep.",
"key": "97017_CR67",
"unstructured": "French, C. B., McDonnell, S. L. & Vieth, R. 25-Hydroxyvitamin D variability within-person due to diurnal rhythm and illness: A case report. J. Med. Case Rep. 13(1), 29. https://doi.org/10.1186/s13256-018-1948-9 (2019).",
"volume": "13",
"year": "2019"
},
{
"DOI": "10.1017/S0007114519000151",
"author": "E Malacova",
"doi-asserted-by": "publisher",
"first-page": "894",
"issue": "8",
"journal-title": "Br. J. Nutr.",
"key": "97017_CR68",
"unstructured": "Malacova, E. et al. Prevalence and predictors of vitamin D deficiency in a nationally representative sample of adults participating in the 2011–2013 Australian Health Survey. Br. J. Nutr. 121(8), 894–904. https://doi.org/10.1017/S0007114519000151 (2019).",
"volume": "121",
"year": "2019"
}
],
"reference-count": 68,
"references-count": 68,
"relation": {},
"resource": {
"primary": {
"URL": "https://www.nature.com/articles/s41598-021-97017-9"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Multidisciplinary"
],
"subtitle": [],
"title": "The relationship between serum 25-hydroxyvitamin D levels and the severity of COVID-19 disease and its mortality",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1007/springer_crossmark_policy",
"volume": "11"
}