Abstract: Journal of Steroid Biochemistry and Molecular Biology 203 (2020) 105751
Contents lists available at ScienceDirect
Journal of Steroid Biochemistry and Molecular Biology
journal homepage: www.elsevier.com/locate/jsbmb
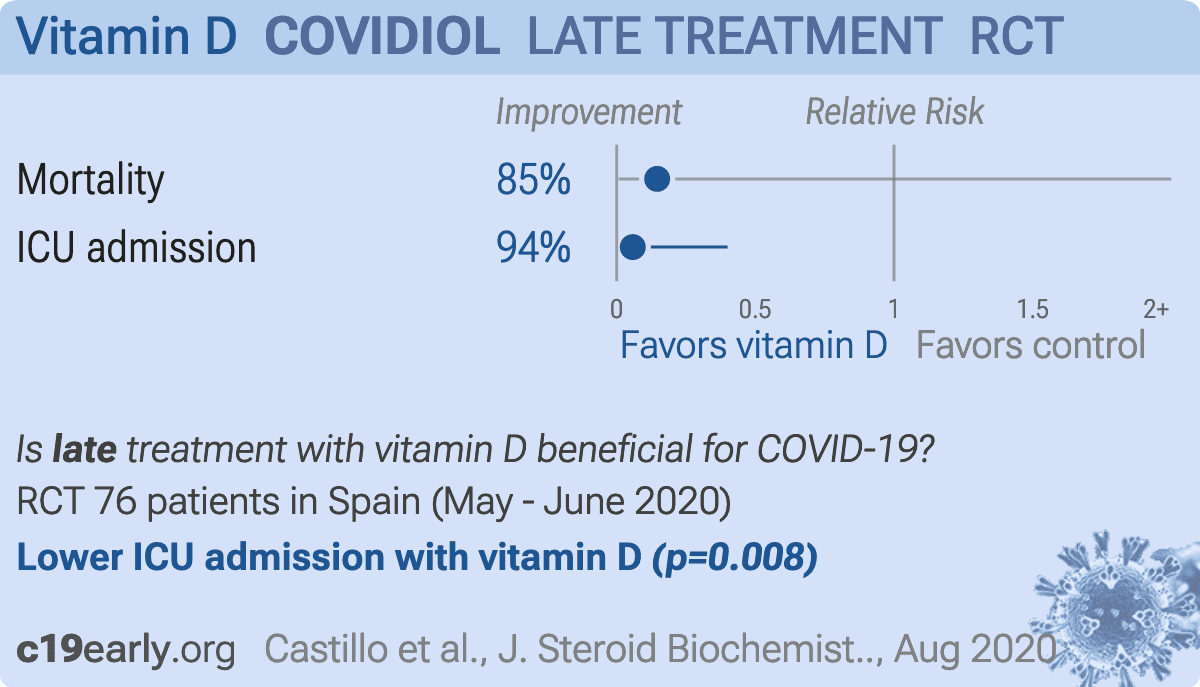
“Effect of calcifediol treatment and best available therapy versus best
available therapy on intensive care unit admission and mortality among
patients hospitalized for COVID-19: A pilot randomized clinical study”
Marta Entrenas Castillo a, Luis Manuel Entrenas Costa a, *, José Manuel Vaquero Barrios a,
Juan Francisco Alcalá Díaz b, José López Miranda b, Roger Bouillon c,
José Manuel Quesada Gomez d
a
UGC de Neumología, Instituto Maimónides de Investigación Biomédica de Córdoba 9 (IMIBIC). Hospital Universitario Reina Sofía, Universidad de Córdoba, Avda.
Menéndez 10 Pidal s/n, 14004 11, Córdoba, Spain
b
Departamento de Medicina Interna. IMIBIC, CIBER de Fisiopatología de la Obesidad y la Nutrición. Hospital Universitario Reina Sofía, Universidad de Córdoba,
Fundación Progreso y Salud. Avda. Menéndez Pidal s/n, 14004 14, Córdoba, Spain
c
Department of Chronic Diseases, Metabolism and Ageing, Laboratory of Clinical and Experimental Endocrinology, KU Leuven, Herestraat, ON1/902, 3000, Leuven,
Belgium
d
IMIBIC. CIBER de Fragilidad y Envejecimiento Saludable. Hospital Universitario Reina Sofía, Universidad de Córdoba, Fundación Progreso y Salud. Avda. Menéndez
Pidal s/n, 18 14004, Córdoba, Spain
A R T I C L E I N F O
A B S T R A C T
Keywords:
COVID-19
SARS-CoV-2
Vitamin D
Vitamin D3 or cholecalciferol
Calcifediol or 25-hydroxyvitamin D3
1α, 25(OH)2D or 1α, 25-dihydroxyvitamin D or
calcitriol
Acute respiratory distress syndrome (ARDS)
Cytokine/Chemokine storm
Renin-angiotensin system
Hypercoagulability
Hydroxychloroquine
Chloroquine
Covidiol
Neutrophil activity
Vitamin D endocrine system
Cuboidal alveolar coating cells type II
Cathelicidin peptide
Defensins
TLR co-receptor CD14
Vitamin D receptor
Objective: The vitamin D endocrine system may have a variety of actions on cells and tissues involved in COVID19 progression especially by decreasing the Acute Respiratory Distress Syndrome. Calcifediol can rapidly in
crease serum 25OHD concentration. We therefore evaluated the effect of calcifediol treatment, on Intensive Care
Unit Admission and Mortality rate among Spanish patients hospitalized for COVID-19.
Design: Parallel pilot randomized open label, double-masked clinical trial.
Setting: University hospital setting (Reina Sofia University Hospital, Córdoba Spain.)
Participants: 76 consecutive patients hospitalized with COVID-19 infection, clinical picture of acute respiratory
infection, confirmed by a radiographic pattern of viral pneumonia and by a positive SARS-CoV-2 PCR with
CURB65 severity scale (recommending hospital admission in case of total score > 1).
Procedures: All hospitalized patients received as best available therapy the same standard care, (per hospital
protocol), of a combination of hydroxychloroquine (400 mg every 12 h on the first day, and 200 mg every 12 h for
the following 5 days), azithromycin (500 mg orally for 5 days. Eligible patients were allocated at a 2 calcifediol:1
no calcifediol ratio through electronic randomization on the day of admission to take oral calcifediol (0.532 mg), or
not. Patients in the calcifediol treatment group continued with oral calcifediol (0.266 mg) on day 3 and 7, and then
weekly until discharge or ICU admission. Outcomes of effectiveness included..
{ 'indexed': {'date-parts': [[2024, 4, 8]], 'date-time': '2024-04-08T08:30:48Z', 'timestamp': 1712565048616},
'reference-count': 45,
'publisher': 'Elsevier BV',
'license': [ { 'start': { 'date-parts': [[2020, 10, 1]],
'date-time': '2020-10-01T00:00:00Z',
'timestamp': 1601510400000},
'content-version': 'tdm',
'delay-in-days': 0,
'URL': 'https://www.elsevier.com/tdm/userlicense/1.0/'},
{ 'start': { 'date-parts': [[2020, 10, 1]],
'date-time': '2020-10-01T00:00:00Z',
'timestamp': 1601510400000},
'content-version': 'stm-asf',
'delay-in-days': 0,
'URL': 'https://doi.org/10.15223/policy-017'},
{ 'start': { 'date-parts': [[2020, 10, 1]],
'date-time': '2020-10-01T00:00:00Z',
'timestamp': 1601510400000},
'content-version': 'stm-asf',
'delay-in-days': 0,
'URL': 'https://doi.org/10.15223/policy-037'},
{ 'start': { 'date-parts': [[2020, 10, 1]],
'date-time': '2020-10-01T00:00:00Z',
'timestamp': 1601510400000},
'content-version': 'stm-asf',
'delay-in-days': 0,
'URL': 'https://doi.org/10.15223/policy-012'},
{ 'start': { 'date-parts': [[2020, 10, 1]],
'date-time': '2020-10-01T00:00:00Z',
'timestamp': 1601510400000},
'content-version': 'stm-asf',
'delay-in-days': 0,
'URL': 'https://doi.org/10.15223/policy-029'},
{ 'start': { 'date-parts': [[2020, 10, 1]],
'date-time': '2020-10-01T00:00:00Z',
'timestamp': 1601510400000},
'content-version': 'stm-asf',
'delay-in-days': 0,
'URL': 'https://doi.org/10.15223/policy-004'}],
'content-domain': {'domain': ['elsevier.com', 'sciencedirect.com'], 'crossmark-restriction': True},
'published-print': {'date-parts': [[2020, 10]]},
'DOI': '10.1016/j.jsbmb.2020.105751',
'type': 'journal-article',
'created': {'date-parts': [[2020, 8, 29]], 'date-time': '2020-08-29T15:13:41Z', 'timestamp': 1598714021000},
'page': '105751',
'update-policy': 'http://dx.doi.org/10.1016/elsevier_cm_policy',
'source': 'Crossref',
'is-referenced-by-count': 486,
'title': '“Effect of calcifediol treatment and best available therapy versus best available therapy on '
'intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot '
'randomized clinical study”',
'prefix': '10.1016',
'volume': '203',
'author': [ { 'ORCID': 'http://orcid.org/0000-0003-2264-3456',
'authenticated-orcid': False,
'given': 'Marta',
'family': 'Entrenas Castillo',
'sequence': 'first',
'affiliation': []},
{ 'given': 'Luis Manuel',
'family': 'Entrenas Costa',
'sequence': 'additional',
'affiliation': []},
{ 'given': 'José Manuel',
'family': 'Vaquero Barrios',
'sequence': 'additional',
'affiliation': []},
{ 'ORCID': 'http://orcid.org/0000-0002-4572-3611',
'authenticated-orcid': False,
'given': 'Juan Francisco',
'family': 'Alcalá Díaz',
'sequence': 'additional',
'affiliation': []},
{ 'ORCID': 'http://orcid.org/0000-0002-8844-0718',
'authenticated-orcid': False,
'given': 'José',
'family': 'López Miranda',
'sequence': 'additional',
'affiliation': []},
{'given': 'Roger', 'family': 'Bouillon', 'sequence': 'additional', 'affiliation': []},
{ 'given': 'José Manuel',
'family': 'Quesada Gomez',
'sequence': 'additional',
'affiliation': []}],
'member': '78',
'reference': [ { 'key': '10.1016/j.jsbmb.2020.105751_bib0005',
'doi-asserted-by': 'crossref',
'first-page': '270',
'DOI': '10.1038/s41586-020-2012-7',
'article-title': 'A pneumonia outbreak associated with a new coronavirus of probable bat '
'origin',
'volume': '579',
'author': 'Zhou',
'year': '2020',
'journal-title': 'Nature'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0010',
'doi-asserted-by': 'crossref',
'first-page': '497',
'DOI': '10.1016/S0140-6736(20)30183-5',
'article-title': 'Clinical features of patients infected with 2019 novel coronavirus in '
'Wuhan, China',
'volume': '395',
'author': 'Huang',
'year': '2020',
'journal-title': 'Lancet'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0015',
'doi-asserted-by': 'crossref',
'first-page': '507',
'DOI': '10.1016/S0140-6736(20)30211-7',
'article-title': 'Epidemiological and clinical characteristics of 99 cases of 2019 novel '
'coronavirus pneumonia in Wuhan, China: a descriptive study',
'volume': '395',
'author': 'Chen',
'year': '2020',
'journal-title': 'Lancet'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0020',
'doi-asserted-by': 'crossref',
'first-page': '698',
'DOI': '10.1001/jama.2017.21907',
'article-title': 'Acute respiratory distress syndrome',
'volume': '319',
'author': 'Fan',
'year': '2018',
'journal-title': 'JAMA'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0025',
'first-page': '2526',
'article-title': 'Acute respiratory distress syndrome: the Berlin definition',
'volume': '307',
'author': 'Ranieri',
'year': '2012',
'journal-title': 'JAMA - J. Am. Med. Assoc.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0030',
'doi-asserted-by': 'crossref',
'DOI': '10.1001/jamainternmed.2020.0994',
'article-title': 'Risk factors associated with acute respiratory distress syndrome and '
'death in patients with coronavirus disease 2019 Pneumonia in Wuhan, '
'China',
'author': 'Wu',
'year': '2020',
'journal-title': 'JAMA Intern. Med.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0035',
'doi-asserted-by': 'crossref',
'first-page': '788',
'DOI': '10.1001/jama.2016.0291',
'article-title': 'Epidemiology, patterns of care, and mortality for patients with acute '
'respiratory distress syndrome in intensive care units in 50 countries',
'volume': '315',
'author': 'Bellani',
'year': '2016',
'journal-title': 'JAMA - J. Am. Med. Assoc.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0040',
'doi-asserted-by': 'crossref',
'first-page': '420',
'DOI': '10.1016/S2213-2600(20)30076-X',
'article-title': 'Pathological findings of COVID-19 associated with acute respiratory '
'distress syndrome',
'volume': '8',
'author': 'Xu',
'year': '2020',
'journal-title': 'Lancet Respir. Med.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0045',
'doi-asserted-by': 'crossref',
'DOI': '10.1001/jama.2020.8115',
'article-title': 'Randomized clinical trials and COVID-19: managing expectations',
'author': 'Bauchner',
'year': '2020',
'journal-title': 'JAMA - J. Am. Med. Assoc.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0050',
'doi-asserted-by': 'crossref',
'first-page': 'e208297',
'DOI': '10.1001/jamanetworkopen.2020.8297',
'article-title': 'Estimated demand for US hospital inpatient and intensive care unit beds '
'for patients with COVID-19 based on comparisons with Wuhan and '
'Guangzhou, China',
'volume': '3',
'author': 'Li',
'year': '2020',
'journal-title': 'JAMA Netw. Open.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0055',
'doi-asserted-by': 'crossref',
'DOI': '10.1016/j.jsbmb.2020.105719',
'article-title': 'Vitamin D receptor stimulation to reduce acute respiratory distress '
'syndrome (ARDS) in patients with coronavirus SARS-CoV-2 infections: '
'revised Ms SBMB 2020_166',
'volume': '202',
'author': 'Quesada-Gomez',
'year': '2020',
'journal-title': 'J. Steroid Biochem. Mol. Biol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0060',
'doi-asserted-by': 'crossref',
'first-page': '1186',
'DOI': '10.3892/mmr.2015.4685',
'article-title': 'Vitamin D/VDR signaling attenuates lipopolysaccharide-induced acute '
'lung injury by maintaining the integrity of the pulmonary epithelial '
'barrier',
'volume': '13',
'author': 'Shi',
'year': '2016',
'journal-title': 'Mol. Med. Rep.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0065',
'doi-asserted-by': 'crossref',
'first-page': '1186',
'DOI': '10.3892/mmr.2015.4685',
'article-title': 'Vitamin D/VDR signaling attenuates lipopolysaccharide-induced acute '
'lung injury by maintaining the integrity of the pulmonary epithelial '
'barrier',
'volume': '13',
'author': 'Shi',
'year': '2016',
'journal-title': 'Mol. Med. Rep.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0070',
'doi-asserted-by': 'crossref',
'first-page': '2116',
'DOI': '10.1210/me.2013-1146',
'article-title': 'VDR attenuates acute lung injury by blocking Ang-2-Tie-2 pathway and '
'renin-angiotensin system',
'volume': '27',
'author': 'Kong',
'year': '2013',
'journal-title': 'Mol. Endocrinol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0075',
'doi-asserted-by': 'crossref',
'DOI': '10.1016/j.bcp.2020.113955',
'article-title': 'Vitamin D attenuates lung injury via stimulating epithelial repair, '
'reducing epithelial cell apoptosis and inhibits TGF-β induced '
'epithelial to mesenchymal transition',
'volume': '177',
'author': 'Zheng',
'year': '2020',
'journal-title': 'Biochem. Pharmacol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0080',
'doi-asserted-by': 'crossref',
'first-page': '1367',
'DOI': '10.1096/fj.15-272872',
'article-title': 'Vitamin D modulates tissue factor and protease-activated receptor 2 '
'expression in vascular smooth muscle cells',
'volume': '30',
'author': 'Martinez-Moreno',
'year': '2016',
'journal-title': 'FASEB J.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0085',
'article-title': 'Vitamin D. And inflammation: potential implications for severity of '
'Covid-19',
'volume': '113',
'author': 'Laird',
'year': '2020',
'journal-title': 'Ir. Med. J.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0090',
'doi-asserted-by': 'crossref',
'first-page': '1195',
'DOI': '10.1007/s40520-020-01570-8',
'article-title': 'The role of vitamin D in the prevention of coronavirus disease 2019 '
'infection and mortality',
'volume': '32',
'author': 'Ilie',
'year': '2020',
'journal-title': 'Aging Clin. Exp. Res.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0095',
'doi-asserted-by': 'crossref',
'DOI': '10.3390/nu12051359',
'article-title': '25-hydroxyvitamin D concentrations are lower in patients with positive '
'PCR for SARS-CoV-2',
'volume': '12',
'author': 'D’avolio',
'year': '2020',
'journal-title': 'Nutrients'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0100',
'article-title': 'Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalised '
'with COVID-19 are associated with greater disease severity',
'author': 'Panagiotou',
'year': '2020',
'journal-title': 'Clin. Endocrinol. (Oxf).'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0105',
'doi-asserted-by': 'crossref',
'first-page': '676',
'DOI': '10.1016/j.clinbiochem.2008.02.003',
'article-title': 'Inappropriate serum levels of retinol, α-tocopherol, 25 hydroxyvitamin '
'D3 and 24,25 dihydroxyvitamin D3 levels in healthy Spanish adults: '
'simultaneous assessment by HPLC',
'volume': '41',
'author': 'Mata-Granados',
'year': '2008',
'journal-title': 'Clin. Biochem.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0110',
'doi-asserted-by': 'crossref',
'first-page': '452',
'DOI': '10.1016/j.jsbmb.2010.03.078',
'article-title': 'Evaluation of vitamin D endocrine system (VDES) status and response to '
'treatment of patients in intensive care units (ICUs) using an on-line '
'SPE-LC-MS/MS method',
'volume': '121',
'author': 'Mata-Granados',
'year': '2010',
'journal-title': 'J. Steroid Biochem. Mol. Biol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0115',
'series-title': 'Gobierno De España, Ministerio De Sanidad, Consumo Y Bienestar Social - '
'Documentos Técnicos Para Profesionales - Coronavirus',
'year': '2020'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0120',
'unstructured': 'Tratamientos disponibles sujetos a condiciones especiales de acceso para '
'el manejo de la infección respiratoria por SARS-CoV-2 - Agencia Española '
'de Medicamentos y Productos Sanitarios, (n.d.). '
'https://www.aemps.gob.es/la-aemps/ultima-informacion-de-la-aemps-acerca-del-covid-19/tratamientos-disponibles-para-el-manejo-de-la-infeccion-respiratoria-por-sars-cov-2/?lang=en '
'(accessed June 22, 2020).'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0125',
'doi-asserted-by': 'crossref',
'first-page': '377',
'DOI': '10.1136/thorax.58.5.377',
'article-title': 'Defining community acquired pneumonia severity on presentation to '
'hospital: an international derivation and validation study',
'volume': '58',
'author': 'Lim',
'year': '2003',
'journal-title': 'Thorax'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0130',
'unstructured': 'In Vitro Antiviral Activity and Projection of Optimized Dosing Design of '
'Hydroxychloroquine for the Treatment of Severe Acute Respiratory '
'Syndrome Coronavirus 2 (SARS-CoV-2) - PubMed, (n.d.). '
'https://pubmed.ncbi.nlm.nih.gov/32150618/ (accessed June 23, 2020).'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0135',
'doi-asserted-by': 'crossref',
'first-page': 'S27',
'DOI': '10.1086/511159',
'article-title': 'Infectious diseases society of America/American thoracic society '
'consensus guidelines on the management of community-acquired pneumonia '
'in adults',
'volume': '44',
'author': 'Mandell',
'year': '2007',
'journal-title': 'Clin. Infect. Dis.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0140',
'doi-asserted-by': 'crossref',
'first-page': '1375',
'DOI': '10.1016/j.jclinepi.2015.04.014',
'article-title': 'A simple formula for the calculation of sample size in pilot studies',
'volume': '68',
'author': 'Viechtbauer',
'year': '2015',
'journal-title': 'J. Clin. Epidemiol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0145',
'doi-asserted-by': 'crossref',
'first-page': '252',
'DOI': '10.1007/s00223-011-9513-1',
'article-title': 'Metabolic changes following 500 μg monthly administration of calcidiol: '
'a study in normal females',
'volume': '89',
'author': 'Russo',
'year': '2011',
'journal-title': 'Calcif. Tissue Int.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0150',
'unstructured': 'Laboratory testing for 2019 novel coronavirus (2019-nCoV) in suspected '
'human cases, (n.d.). '
'https://www.who.int/publications/i/item/10665-331501 (accessed June 23, '
'2020).'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0155',
'doi-asserted-by': 'crossref',
'DOI': '10.1186/1741-7015-8-18',
'article-title': 'CONSORT 2010 Statement: Updated guidelines for reporting parallel group '
'randomised trials',
'volume': '8',
'author': 'Schulz',
'year': '2010',
'journal-title': 'BMC Med.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0160',
'doi-asserted-by': 'crossref',
'first-page': '2411',
'DOI': '10.1056/NEJMoa2012410',
'article-title': 'Observational study of hydroxychloroquine in hospitalized patients with '
'COVID-19',
'volume': '382',
'author': 'Geleris',
'year': '2020',
'journal-title': 'N. Engl. J. Med.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0165',
'doi-asserted-by': 'crossref',
'first-page': '1109',
'DOI': '10.1210/er.2018-00126',
'article-title': 'Skeletal and extraskeletal actions of vitamin d: current evidence and '
'outstanding questions',
'volume': '40',
'author': 'Bouillon',
'year': '2019',
'journal-title': 'Endocr. Rev.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0170',
'doi-asserted-by': 'crossref',
'first-page': '7090',
'DOI': '10.4049/jimmunol.181.10.7090',
'article-title': 'Respiratory epithelial cells convert inactive vitamin d to its active '
'form: potential effects on host defense',
'volume': '181',
'author': 'Hansdottir',
'year': '2008',
'journal-title': 'J. Immunol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0175',
'doi-asserted-by': 'crossref',
'DOI': '10.1371/journal.pone.0215383',
'article-title': '25(OH)D 3 and 1.25(OH) 2 D 3 inhibits TNF-α expression in human '
'monocyte derived macrophages',
'volume': '14',
'author': 'Rafique',
'year': '2019',
'journal-title': 'PLoS One'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0180',
'doi-asserted-by': 'crossref',
'first-page': 'e90301',
'DOI': '10.1371/journal.pone.0090301',
'article-title': 'Both 25-hydroxyvitamin-D3 and 1,25-dihydroxyvitamin- D3 reduces '
'inflammatory response in human periodontal ligament cells',
'volume': '9',
'author': 'Andrukhov',
'year': '2014',
'journal-title': 'PLoS One'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0185',
'doi-asserted-by': 'crossref',
'first-page': '1195',
'DOI': '10.1002/oby.22831',
'article-title': 'High prevalence of obesity in severe acute respiratory syndrome '
'Coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation',
'volume': '28',
'author': 'Simonnet',
'year': '2020',
'journal-title': 'Obesity.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0190',
'doi-asserted-by': 'crossref',
'DOI': '10.1016/S2213-8587(20)30268-0',
'article-title': 'Vitamin D for COVID-19: a case to answer?',
'author': 'Martineau',
'year': '2020',
'journal-title': 'Lancet Diabetes Endocrinol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0195',
'doi-asserted-by': 'crossref',
'first-page': '48',
'DOI': '10.1111/nure.12090',
'article-title': 'Guidelines for optimizing design and analysis of clinical studies of '
'nutrient effects',
'volume': '72',
'author': 'Heaney',
'year': '2014',
'journal-title': 'Nutr. Rev.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0200',
'doi-asserted-by': 'crossref',
'first-page': '266',
'DOI': '10.1016/j.jsbmb.2017.08.009',
'article-title': 'Why vitamin D clinical trials should be based on 25-hydroxyvitamin D '
'concentrations',
'volume': '177',
'author': 'Grant',
'year': '2018',
'journal-title': 'J. Steroid Biochem. Mol. Biol.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0205',
'doi-asserted-by': 'crossref',
'first-page': '1985',
'DOI': '10.1002/jbmr.3884',
'article-title': 'Vitamin D metabolism revised: fall of dogmas',
'volume': '34',
'author': 'Bouillon',
'year': '2019',
'journal-title': 'J. Bone Miner. Res.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0210',
'doi-asserted-by': 'crossref',
'DOI': '10.1164/rccm.201909-1867OC',
'article-title': 'Vitamin D metabolism is dysregulated in Asthma and chronic obstructive '
'pulmonary disease',
'author': 'Jolliffe',
'year': '2020',
'journal-title': 'Am. J. Respir. Crit. Care Med.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0215',
'doi-asserted-by': 'crossref',
'first-page': '1697',
'DOI': '10.1007/s00198-018-4520-y',
'article-title': 'Is calcifediol better than cholecalciferol for vitamin D '
'supplementation?',
'volume': '29',
'author': 'Quesada-Gomez',
'year': '2018',
'journal-title': 'Osteoporos. Int.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0220',
'article-title': 'Dexamethasone in hospitalized patients with Covid-19 - preliminary '
'report',
'author': 'RECOVERY Collaborative Group',
'year': '2020',
'journal-title': 'N. Engl. J. Med.'},
{ 'key': '10.1016/j.jsbmb.2020.105751_bib0225',
'unstructured': 'Corticosteroids (including dexamethasone). NIH website. Updated July 17, '
'2020. Accessed August, 2020. '
'https://www.covid19treatmentguidelines.nih.gov/dexamethasone/.'}],
'container-title': 'The Journal of Steroid Biochemistry and Molecular Biology',
'original-title': [],
'language': 'en',
'link': [ { 'URL': 'https://api.elsevier.com/content/article/PII:S0960076020302764?httpAccept=text/xml',
'content-type': 'text/xml',
'content-version': 'vor',
'intended-application': 'text-mining'},
{ 'URL': 'https://api.elsevier.com/content/article/PII:S0960076020302764?httpAccept=text/plain',
'content-type': 'text/plain',
'content-version': 'vor',
'intended-application': 'text-mining'}],
'deposited': { 'date-parts': [[2024, 1, 27]],
'date-time': '2024-01-27T06:00:47Z',
'timestamp': 1706335247000},
'score': 1,
'resource': {'primary': {'URL': 'https://linkinghub.elsevier.com/retrieve/pii/S0960076020302764'}},
'subtitle': [],
'short-title': [],
'issued': {'date-parts': [[2020, 10]]},
'references-count': 45,
'alternative-id': ['S0960076020302764'],
'URL': 'http://dx.doi.org/10.1016/j.jsbmb.2020.105751',
'relation': {},
'ISSN': ['0960-0760'],
'subject': [ 'Cell Biology', 'Clinical Biochemistry', 'Endocrinology', 'Molecular Biology',
'Molecular Medicine', 'Biochemistry', 'Endocrinology, Diabetes and Metabolism'],
'container-title-short': 'The Journal of Steroid Biochemistry and Molecular Biology',
'published': {'date-parts': [[2020, 10]]},
'assertion': [ {'value': 'Elsevier', 'name': 'publisher', 'label': 'This article is maintained by'},
{ 'value': '“Effect of calcifediol treatment and best available therapy versus best '
'available therapy on intensive care unit admission and mortality among patients '
'hospitalized for COVID-19: A pilot randomized clinical study”',
'name': 'articletitle',
'label': 'Article Title'},
{ 'value': 'The Journal of Steroid Biochemistry and Molecular Biology',
'name': 'journaltitle',
'label': 'Journal Title'},
{ 'value': 'https://doi.org/10.1016/j.jsbmb.2020.105751',
'name': 'articlelink',
'label': 'CrossRef DOI link to publisher maintained version'},
{'value': 'article', 'name': 'content_type', 'label': 'Content Type'},
{'value': '© 2021 Published by Elsevier Ltd.', 'name': 'copyright', 'label': 'Copyright'}],
'article-number': '105751'}


{kind=link}