COVID-19 mortality increases with northerly latitude after adjustment for age suggesting a link with ultraviolet and vitamin D
et al., BMJ Nutr. Prev. Health, doi:10.1136/bmjnph-2020-000110, Jun 2020
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


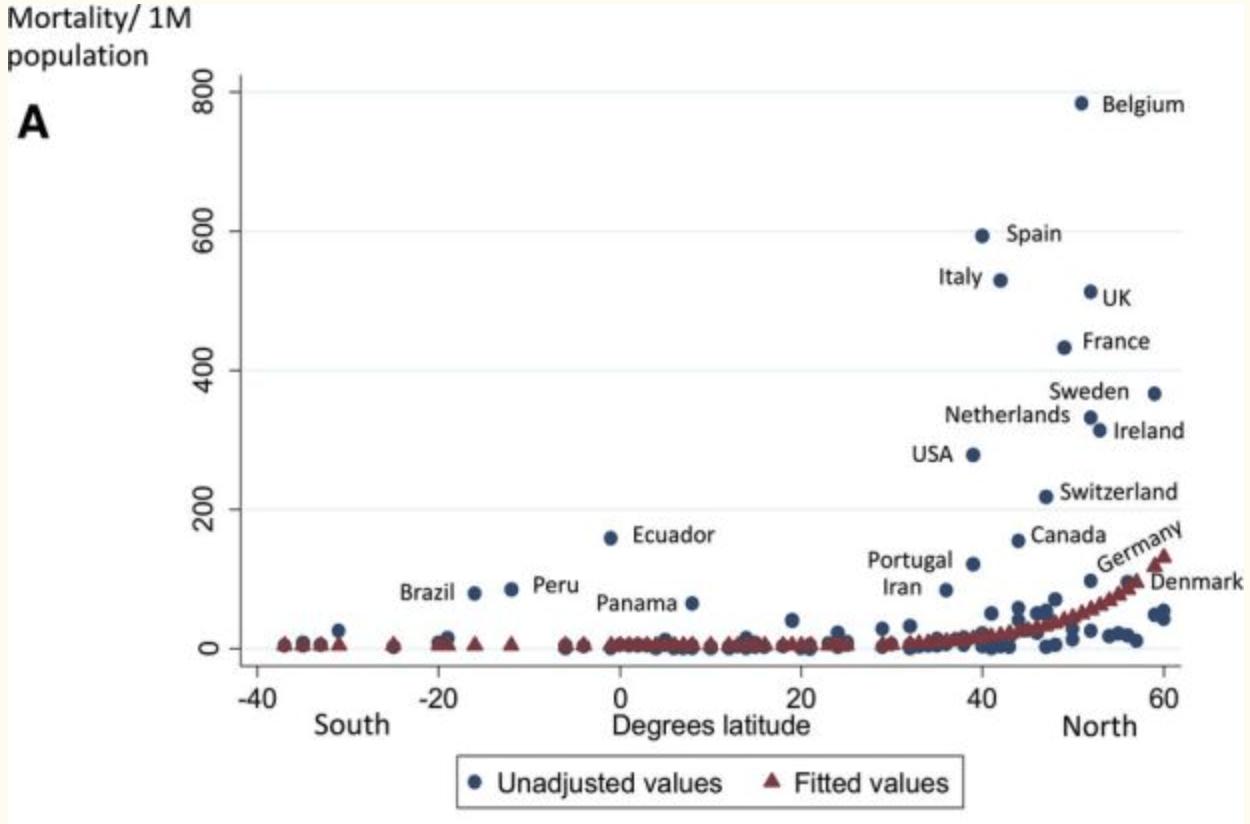
Analysis of COVID-19 mortality and latitude as of May 18, 2020, showing that latitude was significantly associated with mortality (p=0.031), with an estimated 4.4% [0.4%-8.5%] increase in mortality for each 1° further north.
{kind=link}
Rhodes et al., 14 Jun 2020, peer-reviewed, 5 authors.
Abstract: PostScript
Open access
Letter
relationship between mortality and
latitude below a threshold and that
thereafter mortality increased with
COVID-19 mortality
latitude. Mortality data were log
increases with northerly
transformed, and piecewise linear
modelling was used to explore the
latitude after adjustment
relationship with latitude. This was
for age suggesting a link
adjusted for %≥65, and pollution
with ultraviolet and
and population density were investigated to see if they further explained
vitamin D
variability in mortality.
The analysis supported the
hypothesis with a threshold of 28°
Dear Editors,
We read with interest the review north and a model of zero slope
by Dr Kohlmeier in which he below the threshold, and a linear
reported a correlation between model above the threshold was
COVID-19 mortality among African- fitted. The age adjustment was
Americans across the USA and highly significant (p<0.0005), with
northern latitude.1 We previously an estimated mortality increase of
reported a north–south gradient 13.7% (95% CI 7.4% to 20.3%) for
in global COVID-19 mortality but each 1% increase in %≥65. Latitude
were conscious that lack of ultra- was also significant (p=0.031) with
violet exposure and consequent an estimated 4.4% (95% CI 0.4% to
vitamin D insufficiency was not the 8.5%) increase in mortality for each
only possible explanation.2 We have 1° further north (table 1, figure 1).
now investigated the relationships Countries with higher pollution
between latitude, age of population, included many with younger popupopulation density and pollution lations, and pollution was negatively
associated with mortality but added
with COVID-19 mortality.
COVID-19 mortality per million no significant explanatory power to
by country was
https://www. w orldometers. i nfo/ Population density expressed per
coronavirus/ on 18 May 2020.3 country was not significantly associWe included all 117 countries with ated with mortality.
The proportion of older people
population >1 million and ≥150
COVID-19 cases. Data by country in each country impacts greatly on
for population %≥65 years, popula- COVID-19 mortality, but after adjusttion density and air pollution (parti- ment for this, a strong association
cles of matter <2.5 um diameter remains across the Northern hemiµg/m3) were obtained from public sphere between latitude and higher
sources.4–6 Latitude was entered COVID-19 mortality. This association
for each country’s capital city. The exists above 28° north not far from
hypothesis was that there was no the latitude, usually stated as 35°
north, beyond which populations
commonly get insufficient ultraviolet B to maintain normal vitamin
D blood levels throughout winter.
There are exceptions, but COVID-19
mortality correlates with reported
vitamin D levels across Europe,7 and
in sunnier Brazil, where mortality is
rising, 28% prevalence of vitamin D
deficiency is reported.8 An association between vitamin D insufficiency
and COVID-19 severity is supported
by substantial evidence of its impact
on cytokine response to pathogens.7
A direct effect of ultraviolet light on
the environmental survival of severe
acute respiratory syndrome coronavirus 2 is also possible but would
not explain the association between
mortality and ethnicity,9 whereas
people with dark skin need more
ultraviolet exposure for equivalent
vitamin D synthesis.
This analysis supports the link
between latitude and..
DOI record:
{
"DOI": "10.1136/bmjnph-2020-000110",
"ISSN": [
"2516-5542"
],
"URL": "http://dx.doi.org/10.1136/bmjnph-2020-000110",
"alternative-id": [
"10.1136/bmjnph-2020-000110"
],
"author": [
{
"ORCID": "http://orcid.org/0000-0002-1302-260X",
"affiliation": [],
"authenticated-orcid": false,
"family": "Rhodes",
"given": "Jonathan",
"sequence": "first"
},
{
"affiliation": [],
"family": "Dunstan",
"given": "Frank",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Laird",
"given": "Eamon",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Subramanian",
"given": "Sreedhar",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Kenny",
"given": "Rose A",
"sequence": "additional"
}
],
"container-title": "BMJ Nutrition, Prevention & Health",
"container-title-short": "BMJNPH",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"bmj.com"
]
},
"created": {
"date-parts": [
[
2020,
6,
14
]
],
"date-time": "2020-06-14T15:07:08Z",
"timestamp": 1592147228000
},
"deposited": {
"date-parts": [
[
2021,
7,
27
]
],
"date-time": "2021-07-27T22:01:14Z",
"timestamp": 1627423274000
},
"indexed": {
"date-parts": [
[
2024,
4,
2
]
],
"date-time": "2024-04-02T15:02:08Z",
"timestamp": 1712070128895
},
"is-referenced-by-count": 36,
"issue": "1",
"issued": {
"date-parts": [
[
2020,
6
]
]
},
"journal-issue": {
"issue": "1",
"published-online": {
"date-parts": [
[
2020,
7,
9
]
]
},
"published-print": {
"date-parts": [
[
2020,
6
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://creativecommons.org/licenses/by-nc/4.0/",
"content-version": "unspecified",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2020,
4,
16
]
],
"date-time": "2020-04-16T00:00:00Z",
"timestamp": 1586995200000
}
}
],
"link": [
{
"URL": "https://syndication.highwire.org/content/doi/10.1136/bmjnph-2020-000110",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "239",
"original-title": [],
"page": "118-120",
"prefix": "10.1136",
"published": {
"date-parts": [
[
2020,
6
]
]
},
"published-online": {
"date-parts": [
[
2020,
6,
14
]
]
},
"published-print": {
"date-parts": [
[
2020,
6
]
]
},
"publisher": "BMJ",
"reference": [
{
"DOI": "10.1136/bmjnph-2020-000096",
"article-title": "Avoidance of vitamin D deficiency to slow the COVID-19 pandemic",
"author": "Kohlmeier",
"doi-asserted-by": "crossref",
"first-page": "e000096",
"journal-title": "BMJNPH",
"key": "2021072715002532000_3.1.118.1",
"volume": "3",
"year": "2020"
},
{
"DOI": "10.1111/apt.15777",
"article-title": "Editorial: low population mortality from COVID-19 in countries South of latitude 35 degrees North supports vitamin D as a factor determining severity",
"author": "Rhodes",
"doi-asserted-by": "crossref",
"first-page": "1434",
"journal-title": "Aliment Pharmacol Ther",
"key": "2021072715002532000_3.1.118.2",
"volume": "51",
"year": "2020"
},
{
"key": "2021072715002532000_3.1.118.3",
"unstructured": "Coronavirus cases, 2020. Available: https://www.worldometers.info/coronavirus/ [Accessed 18 May 2020]."
},
{
"key": "2021072715002532000_3.1.118.4",
"unstructured": "Population ages 65 and above (% of total population), 2020. Available: https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS [Accessed 18 May 2020]."
},
{
"key": "2021072715002532000_3.1.118.5",
"unstructured": "List of countries and dependencies by population density, 2020. Available: https://en.wikipedia.org/wiki/List of countries and dependencies by population density [Accessed 18 May 2020]."
},
{
"key": "2021072715002532000_3.1.118.6",
"unstructured": "Outdoor air pollution, 2020. Available: https://ourworldindata.org/outdoor-air-pollution [Accessed 18 May 2020]."
},
{
"article-title": "Vitamin D and inflammation: potential implications for severity of COVID-19",
"author": "Laird",
"first-page": "P81",
"journal-title": "Irish Med J",
"key": "2021072715002532000_3.1.118.7",
"volume": "113",
"year": "2020"
},
{
"DOI": "10.1080/10408398.2018.1437711",
"article-title": "Epidemiology of vitamin D insufficiency and deficiency in a population in a sunny country: Geospatial meta-analysis in Brazil",
"author": "Pereira-Santos",
"doi-asserted-by": "crossref",
"first-page": "2102",
"journal-title": "Crit Rev Food Sci Nutr",
"key": "2021072715002532000_3.1.118.8",
"volume": "59",
"year": "2019"
},
{
"key": "2021072715002532000_3.1.118.9",
"unstructured": "Coronavirus (COVID-19) related deaths by ethnic group, England and Wales: 2 March 2020 to 10 April 2020, 2020. Available: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/coronavirusrelateddeathsbyethnicgroupenglandandwales/2march2020to10april2020 [Accessed 29 May 2020]."
},
{
"DOI": "10.1136/bmjnph-2020-000089",
"article-title": "Vitamin D and SARS-CoV-2 virus/COVID-19 disease",
"author": "Lanham-New",
"doi-asserted-by": "crossref",
"first-page": "e000089",
"journal-title": "BMJNPH",
"key": "2021072715002532000_3.1.118.10",
"volume": "3",
"year": "2020"
}
],
"reference-count": 10,
"references-count": 10,
"relation": {},
"resource": {
"primary": {
"URL": "https://nutrition.bmj.com/lookup/doi/10.1136/bmjnph-2020-000110"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [],
"subtitle": [],
"title": "COVID-19 mortality increases with northerly latitude after adjustment for age suggesting a link with ultraviolet and vitamin D",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1136/crossmarkpolicy",
"volume": "3"
}