Vitamin D Deficiency and Thrombosis in Hospitalized SARS-CoV-2 Patients with Suspected Pulmonary Embolism
et al., AJRCCM Conference, 205:A4571, May 2022
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


{kind=link}
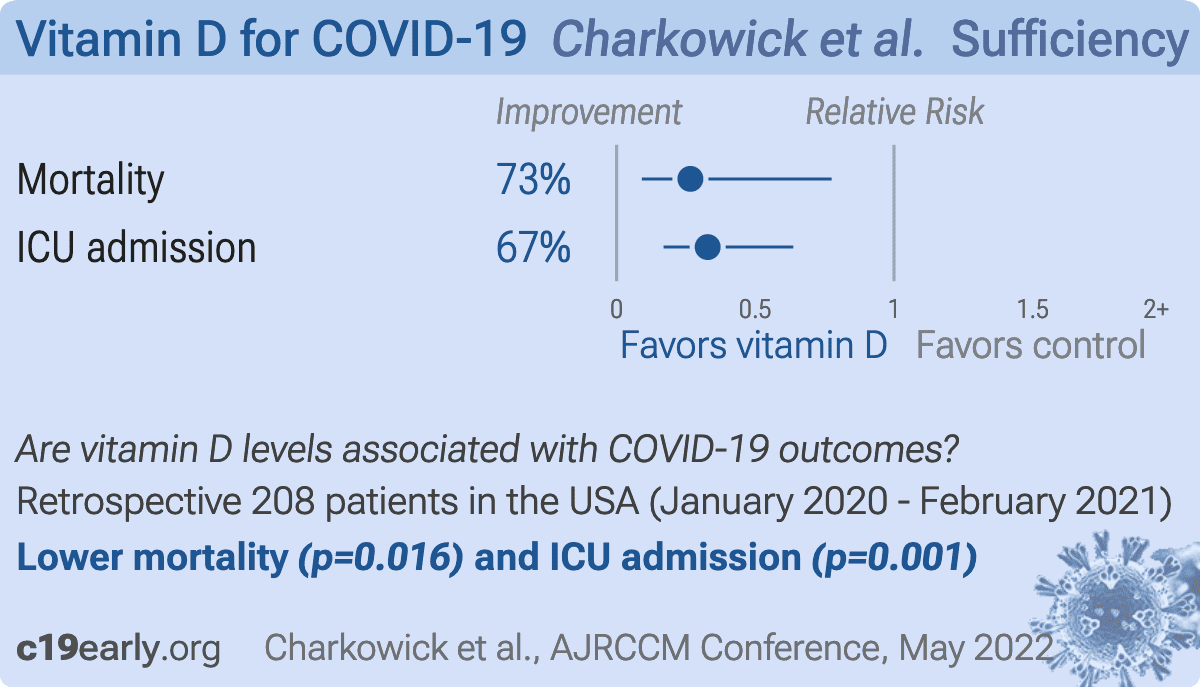
Retrospective 208 hospitalized COVID+ patients in the USA, showing vitamin D deficiency associated with higher mortality and ICU admission.
This is the 133rd of 232 COVID-19 sufficiency studies for vitamin D, which collectively show higher levels reduce risk with p<0.0000000001.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of death, 73.4% lower, OR 0.27, p = 0.02, high D levels 140, low D levels 68, adjusted per study, inverted to make OR<1 favor high D levels, multivariable, RR approximated with OR.
|
|
risk of ICU admission, 67.2% lower, OR 0.33, p = 0.001, high D levels 140, low D levels 68, adjusted per study, inverted to make OR<1 favor high D levels, multivariable, RR approximated with OR.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Charkowick et al., 5 May 2022, retrospective, USA, peer-reviewed, 10 authors, study period 1 January, 2020 - 5 February, 2021.
Contact: scharkowick@usf.edu.
{kind=link}
Abstract: C62 EXPANDING OUR INSIGHT INTO COVID-19 / Thematic Poster Session / Tuesday, May 17/09:30 AM-03:45 PM / Area D, Hall
F (North Building, Exhibition Level), Moscone Center
Vitamin D Deficiency and Thrombosis in Hospitalized SARS-CoV-2
Patients with Suspected Pulmonary Embolism
S. V. Charkowick, C. N. Logothetis, A. Jordan, C. Hanna, S. Zhang, K. Tsay, E. Coughlin, R.
Mhaskar, T. A. Weppelmann, A. Oxner; USF Health Morsani College of Medicine, Tampa, FL,
United States.
Corresponding author's email: scharkowick@usf.edu
RATIONALE Despite the use of anticoagulation therapy in hospitalized patients with severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2), there are high rates of pulmonary embolism
(PE) and deep vein thrombosis (DVT). Vitamin D is a potent immunomodulator with anticoagulative properties that may play a role in suppressing the formation of thrombotic emboli.
Supplementation with vitamin D has an excellent safety profile and provides protection against
acute respiratory infections. Recent studies have indicated that there is a positive association
between vitamin D deficiency and the severity of SARS-CoV-2. However, the relationship between
vitamin D deficiency and the incidence of thrombotic events in patients with SARS-CoV-2 has not
been thoroughly investigated. The main objective of this study was to evaluate the association
between vitamin D deficiency and thrombotic events (PE or DVT) in hospitalized SARS-CoV-2
patients. METHODS This was a retrospective, cross-sectional study including 208 hospitalized
SARS-CoV-2 patients who received a computed tomographic pulmonary angiography (CTPA)
based on clinical suspicion of PE between January 1, 2020, and February 5, 2021. A serum vitamin
D level of <20 ng/mL was used to categorize vitamin D deficiency. Nonparametric tests and
multivariate binary logistic regression were used to evaluate the association between serum vitamin
D level at hospital admission and the incidence of thrombotic events. Several other clinical
outcomes (intensive care unit (ICU) admission, mechanical ventilation, and mortality) were also
analyzed. RESULTS The mean vitamin D level at hospital admission was 26.7±13.0 ng/mL
(N=208). Approximately one-third of patients had vitamin D deficiency (n=68, 32.7%). No
relationship was found between vitamin D deficiency and the occurrence of thrombotic events. The
incidence of PE was 19.1% in vitamin D deficient patients and 11.4% in vitamin D sufficient
patients (p=0.13). The incidence of DVT was 8.6% in vitamin D deficient patients and 9.6% in
vitamin D sufficient patients (p=0.46). After adjusting for confounders, vitamin D deficiency was
positively correlated with admission to the ICU (OR 3.047, 95% CI 1.57-5.91, p=0.001) and overall
mortality (OR 3.76, 95% CI 1.29-11.01, p=0.016). Vitamin D deficiency was not associated with the
need for mechanical ventilation. CONCLUSIONS This study found no significant associations
between vitamin D deficiency and thrombotic events or the need for mechanical ventilation in
hospitalized SARS-CoV-2 patients. Patients with vitamin D deficiency were more likely to be
admitted to the ICU and had increased overall mortality.
This abstract is funded by: USF Health Morsani College of Medicine
Am J Respir Crit Care Med 2022;205:A4571
Internet address: www.atsjournals.org
Online Abstracts Issue