An observational study of the association of vitamin D status and other patient characteristics with COVID-19 severity and mortality
et al., Proceedings of the Nutrition Society, doi:10.1017/S0029665121002482, Aug 2021
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


{kind=link}
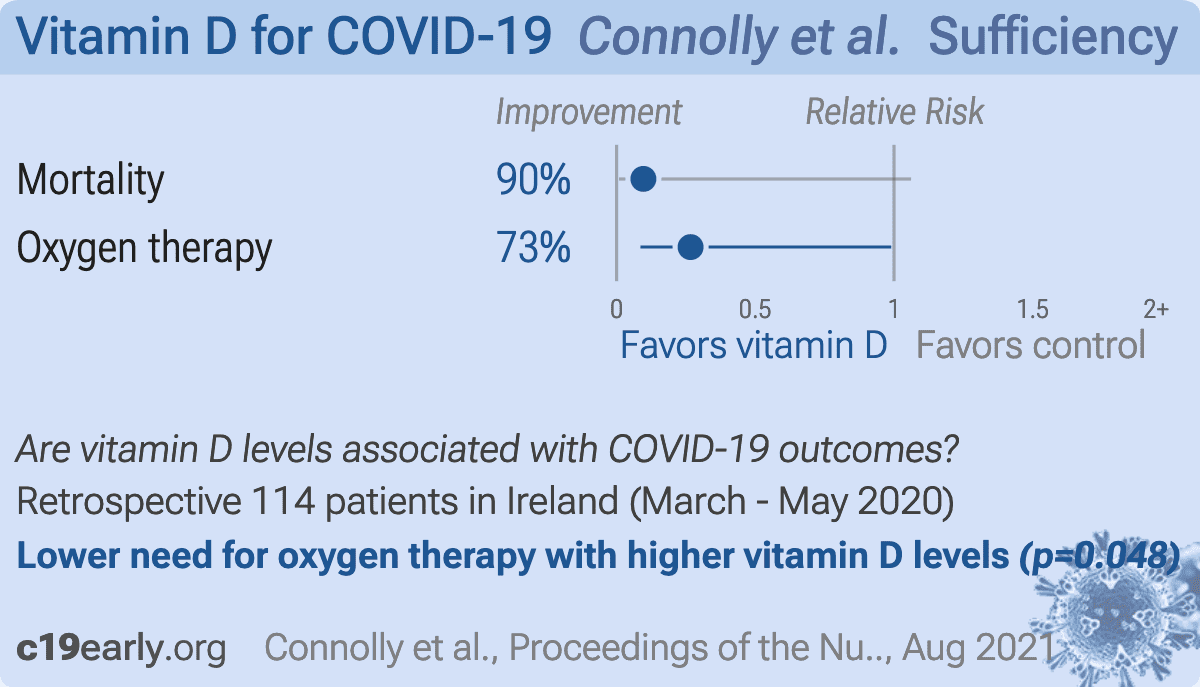
Retrospective 114 hospitalized COVID-19 patients in Ireland, showing higher risk of mortality and oxygen therapy with vitamin D deficiency, with statistical significance for oxygen therapy.
This is the 89th of 232 COVID-19 sufficiency studies for vitamin D, which collectively show higher levels reduce risk with p<0.0000000001.
|
risk of death, 90.4% lower, OR 0.10, p = 0.06, high D levels (≥30nmol/l) 65, low D levels (<30nmol/l) 49, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/l), multivariable, RR approximated with OR.
|
|
risk of oxygen therapy, 73.3% lower, OR 0.27, p = 0.048, high D levels (≥30nmol/l) 65, low D levels (<30nmol/l) 49, adjusted per study, inverted to make OR<1 favor high D levels (≥30nmol/l), multivariable, RR approximated with OR.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Connolly et al., 17 Aug 2021, retrospective, Ireland, peer-reviewed, 8 authors, study period March 2020 - May 2020.
{kind=link}
Abstract: Proceedings of the Nutrition Society (2021), 80 (OCE3), E125
doi:10.1017/S0029665121002482
Irish Section Conference, 22–24 June 2021, Nutrition, health and ageing — translating science into practice – Part A
An observational study of the association of vitamin D status and other
patient characteristics with COVID-19 severity and mortality
M. Connolly1,2, M. Youssef3, A. O’Shea1,2, A. Al Lawati3, S.I. Shah3, S. Walsh3, D. McCartney1
and J. Faul3,4
1
Proceedings of the Nutrition Society
School of Biological and Health Sciences, Technological University Dublin, Ireland,
2
School of Medicine, Trinity College Dublin, Dublin, Ireland,
3
Department of Respiratory Medicine, Connolly Hospital Blanchardstown, Dublin, Ireland and
4
James Connolly Memorial Asthma Research Centre, Royal College of Surgeons in Ireland, Connolly Hospital
Blanchardstown, Dublin, Ireland
Vitamin D deficiency has been proposed to adversely affect COVID-19 severity and clinical outcome(1–4). The current study aimed to
evaluate the association between vitamin D status and COVID-19 severity and clinical outcome after adjustment for other factors
thought to affect outcome including age and gender.
The study included 114 patients from Connolly Hospital, Blanchardstown, Dublin, all of whom tested positive for COVID-19
between March 2020 and May 2020. The independent variables examined included vitamin D status and age, gender, ethnicity,
BMI, smoking status and number of comorbidities. Vitamin D status was classified as ‘deficient’ (serum 25(OH)D <30nmol/L),
‘insufficient’ (serum 25(OH)D of 30–49.9nmol/L) and ‘sufficient’ (serum 25(OH)D ≥50nmol/L). The clinical outcomes assessed
were ICU admission, oxygen requirement and mortality.
Out of the full cohort (n = 114), 64% were male and 17% were over the age of 70. One fifth (n = 23) of the participants did not
survive. The most common comorbidity was hypertension (64%). When categorised according to vitamin D status (n = 94), 49
patients (52%) were deficient, 20 (21%) were insufficient and 25 (27%) had sufficient serum 25(OH)D levels. Low vitamin D status
was associated with greater mortality on univariate analysis, with 80% of those who died presenting with 25(OH)D levels
<30nmol/L vs. 46% of those who survived (P = 0.048). On multivariate regression analysis, the association between vitamin D deficiency (25(OH)D <30nmol/l) and mortality was attenuated (OR 10.37, 95% CI = 0.942-114.1, p = 0.056), but the association of vitamin
D deficiency with increased requirement for oxygen therapy persisted (OR = 3.75, 95% CI = 1.01-13.9, P = 0.048). Males were more
likely to require ICU admission (OR = 3.43, 95%CI = 1.01-11.65, P = 0.048) and oxygen therapy (OR = 3.34, 95% CI = 1.04-10.71,
P = 0.042) than females. When adjusted for other confounders, patients over the age of 70 years were 21.5 times more likely to die
than those under the age of 50 years (OR = 21.5, 95% CI = 2.25-205.4, P = 0.008).
In addition to older age (>70 years) and male gender which both predict poorer clinical outcome, low vitamin D status appears to
be an independent risk factor for more severe disease and mortality in COVID-19.
References
1. Pereira M, Dantas Damascena A, et al. (2020) Crit Rev Food Sci Nutr 1–9
2. Ali N (2020) J Infect Public Health 13(10), 1373–80
3. Faul JL, Kerley CP, Love B, et al. (2020) Ir Med J 113(5), 84
4. Ilie PC, Stefanescu S & Smith L (2020) Aging Clin Exp Res 32(7), 1195–8
https://doi.org/10.1017/S0029665121002482 Published online by..
DOI record:
{
"DOI": "10.1017/s0029665121002482",
"ISSN": [
"0029-6651",
"1475-2719"
],
"URL": "http://dx.doi.org/10.1017/S0029665121002482",
"alternative-id": [
"S0029665121002482"
],
"article-number": "E125",
"assertion": [
{
"group": {
"label": "Copyright and Licensing",
"name": "copyright_and_licensing"
},
"label": "Copyright",
"name": "copyright",
"value": "Copyright © The Authors 2021"
}
],
"author": [
{
"affiliation": [],
"family": "Connolly",
"given": "M.",
"sequence": "first"
},
{
"affiliation": [],
"family": "Youssef",
"given": "M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "O'Shea",
"given": "A.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Al Lawati",
"given": "A.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Shah",
"given": "S.I.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Walsh",
"given": "S.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "McCartney",
"given": "D.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Faul",
"given": "J.",
"sequence": "additional"
}
],
"container-title": "Proceedings of the Nutrition Society",
"container-title-short": "Proc. Nutr. Soc.",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"cambridge.org"
]
},
"created": {
"date-parts": [
[
2021,
8,
17
]
],
"date-time": "2021-08-17T09:18:12Z",
"timestamp": 1629191892000
},
"deposited": {
"date-parts": [
[
2021,
10,
15
]
],
"date-time": "2021-10-15T15:58:53Z",
"timestamp": 1634313533000
},
"indexed": {
"date-parts": [
[
2022,
4,
3
]
],
"date-time": "2022-04-03T05:47:04Z",
"timestamp": 1648964824601
},
"is-referenced-by-count": 1,
"issue": "OCE3",
"issued": {
"date-parts": [
[
2021
]
]
},
"journal-issue": {
"issue": "OCE3",
"published-print": {
"date-parts": [
[
2021
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://www.cambridge.org/core/terms",
"content-version": "unspecified",
"delay-in-days": 228,
"start": {
"date-parts": [
[
2021,
8,
17
]
],
"date-time": "2021-08-17T00:00:00Z",
"timestamp": 1629158400000
}
}
],
"link": [
{
"URL": "https://www.cambridge.org/core/services/aop-cambridge-core/content/view/S0029665121002482",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "56",
"original-title": [],
"prefix": "10.1017",
"published": {
"date-parts": [
[
2021
]
]
},
"published-online": {
"date-parts": [
[
2021,
8,
17
]
]
},
"published-print": {
"date-parts": [
[
2021
]
]
},
"publisher": "Cambridge University Press (CUP)",
"reference": [
{
"author": "Pereira",
"first-page": "1",
"journal-title": "Crit Rev Food Sci Nutr",
"key": "S0029665121002482_ref1",
"year": "2020"
},
{
"author": "Faul",
"first-page": "84",
"journal-title": "Ir Med J",
"key": "S0029665121002482_ref3",
"volume": "113",
"year": "2020"
},
{
"DOI": "10.1007/s40520-020-01570-8",
"doi-asserted-by": "publisher",
"key": "S0029665121002482_ref4"
},
{
"DOI": "10.1016/j.jiph.2020.06.021",
"doi-asserted-by": "publisher",
"key": "S0029665121002482_ref2"
}
],
"reference-count": 4,
"references-count": 4,
"relation": {},
"resource": {
"primary": {
"URL": "https://www.cambridge.org/core/product/identifier/S0029665121002482/type/journal_article"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Nutrition and Dietetics",
"Medicine (miscellaneous)"
],
"subtitle": [],
"title": "An observational study of the association of vitamin D status and other patient characteristics with COVID-19 severity and mortality",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1017/policypage",
"volume": "80"
}