COVID-19 treatment: real-time analysis of 6,647 studies
{kind=link}

c19early.org
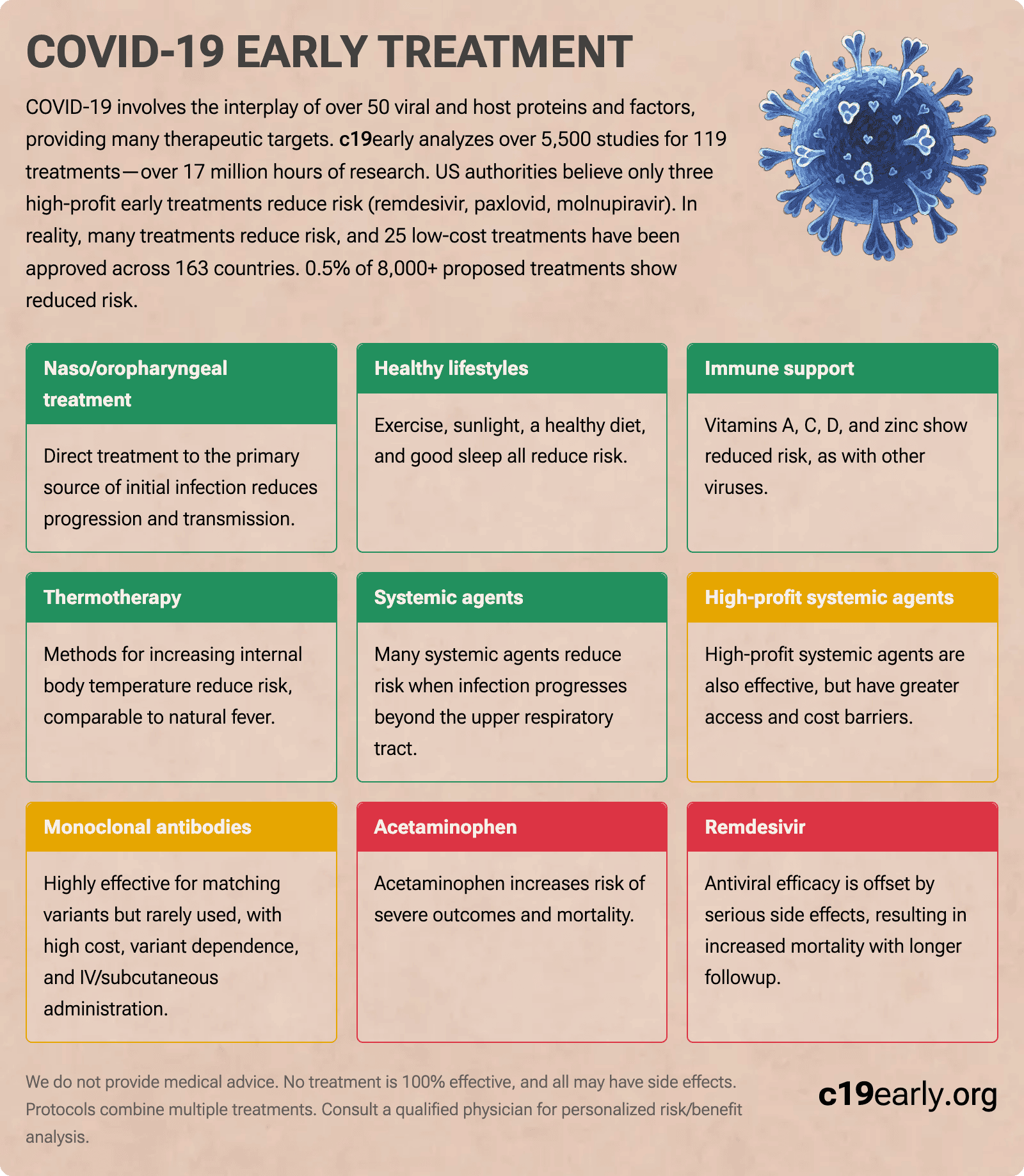
COVID-19 involves the interplay of 500+ viral and host proteins and factors, providing many therapeutic targets.
c19early analyzes 6,600+ studies for 223 treatments—over 17 million hours of research.
Only three high-profit early treatments are approved in the US.
In reality, many treatments reduce risk,
with 25 low-cost treatments approved across 163 countries.
-
Naso/
oropharyngeal treatment Effective Treatment directly to the primary source of initial infection. -
Healthy lifestyles Protective Exercise, sunlight, a healthy diet, and good sleep all reduce risk.
-
Immune support Effective Vitamins A, C, D, and zinc show reduced risk, as with other viruses.
-
Thermotherapy Effective Methods for increasing internal body temperature, enhancing immune system function.
-
Systemic agents Effective Many systemic agents reduce risk, and may be required when infection progresses.
-
High-profit systemic agents Conditional Effective, but with greater access and cost barriers.
-
Monoclonal antibodies Limited Utility Effective but rarely used—high cost, variant dependence, IV/SC admin.
-
Acetaminophen Harmful Increased risk of severe outcomes and mortality.
-
Remdesivir Harmful Increased mortality with longer followup. Increased kidney and liver injury, cardiac disorders.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
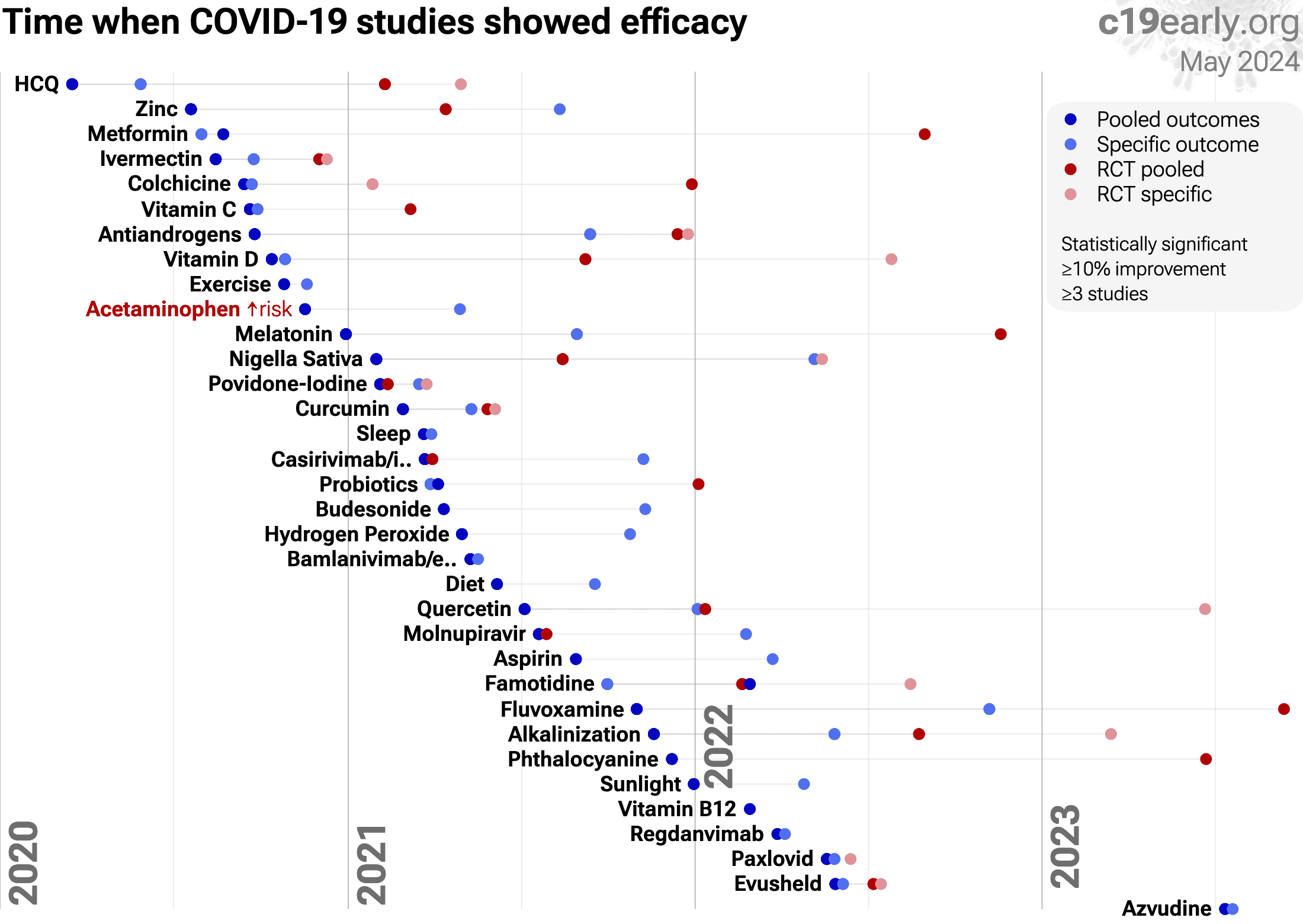
Timeline for when studies showed efficacy - details and limitations.
0.5% of treatments show efficacy.
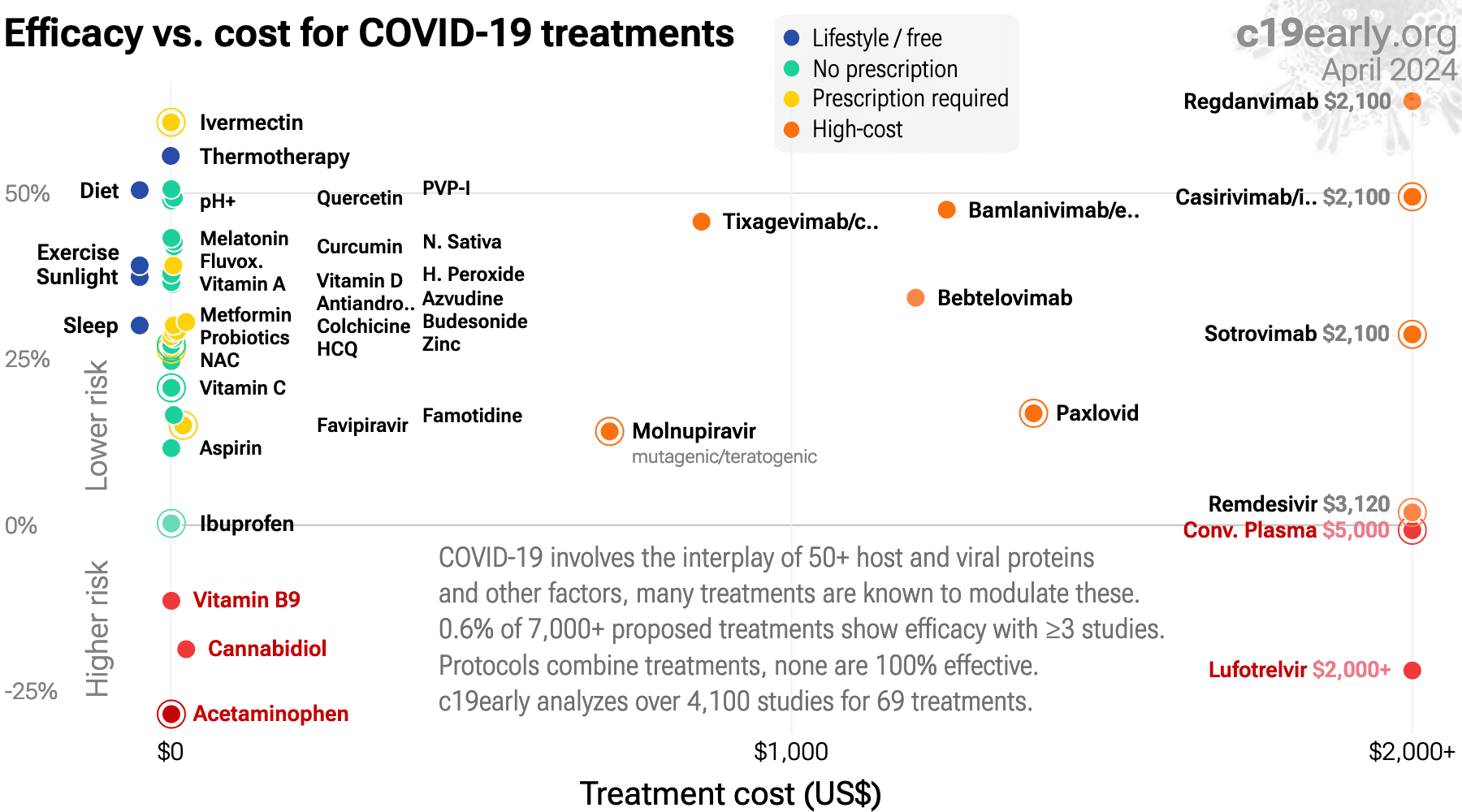
Treatment cost times median NNT - details and limitations.
0.5% of treatments show efficacy.
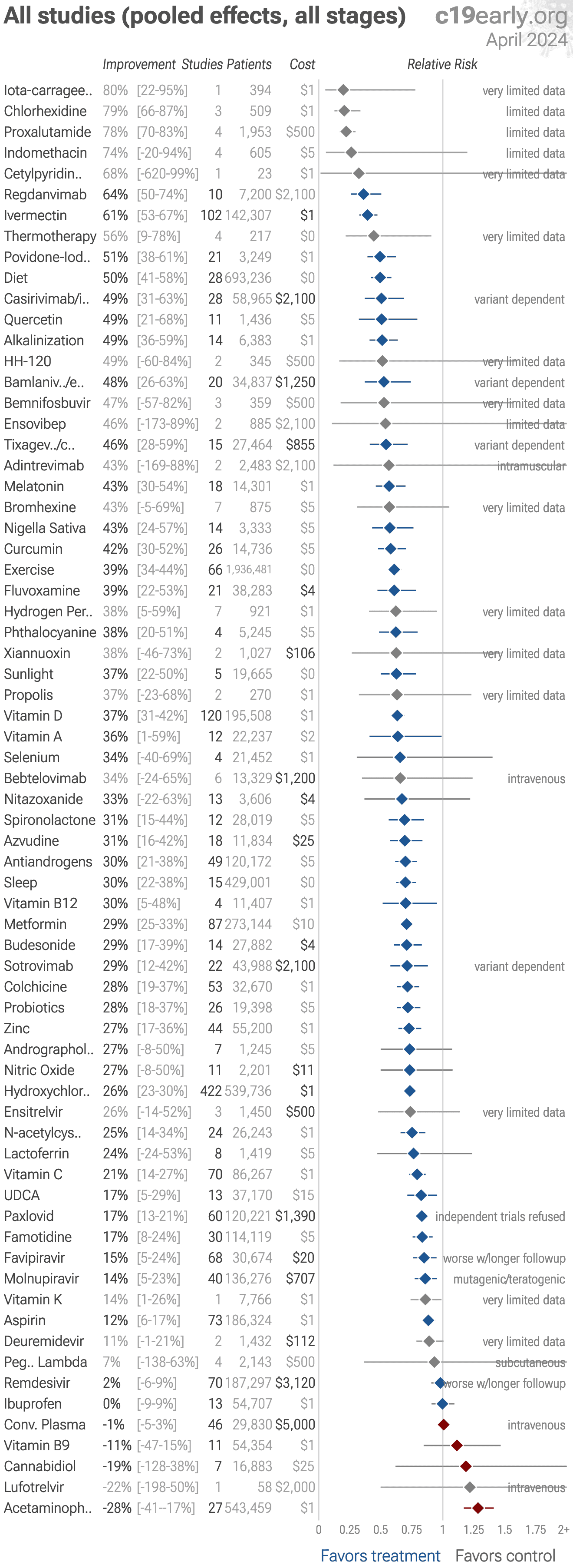
All clinical results for selected treatments. 0.5% of treatments show efficacy.
{kind=link}
{kind=link}
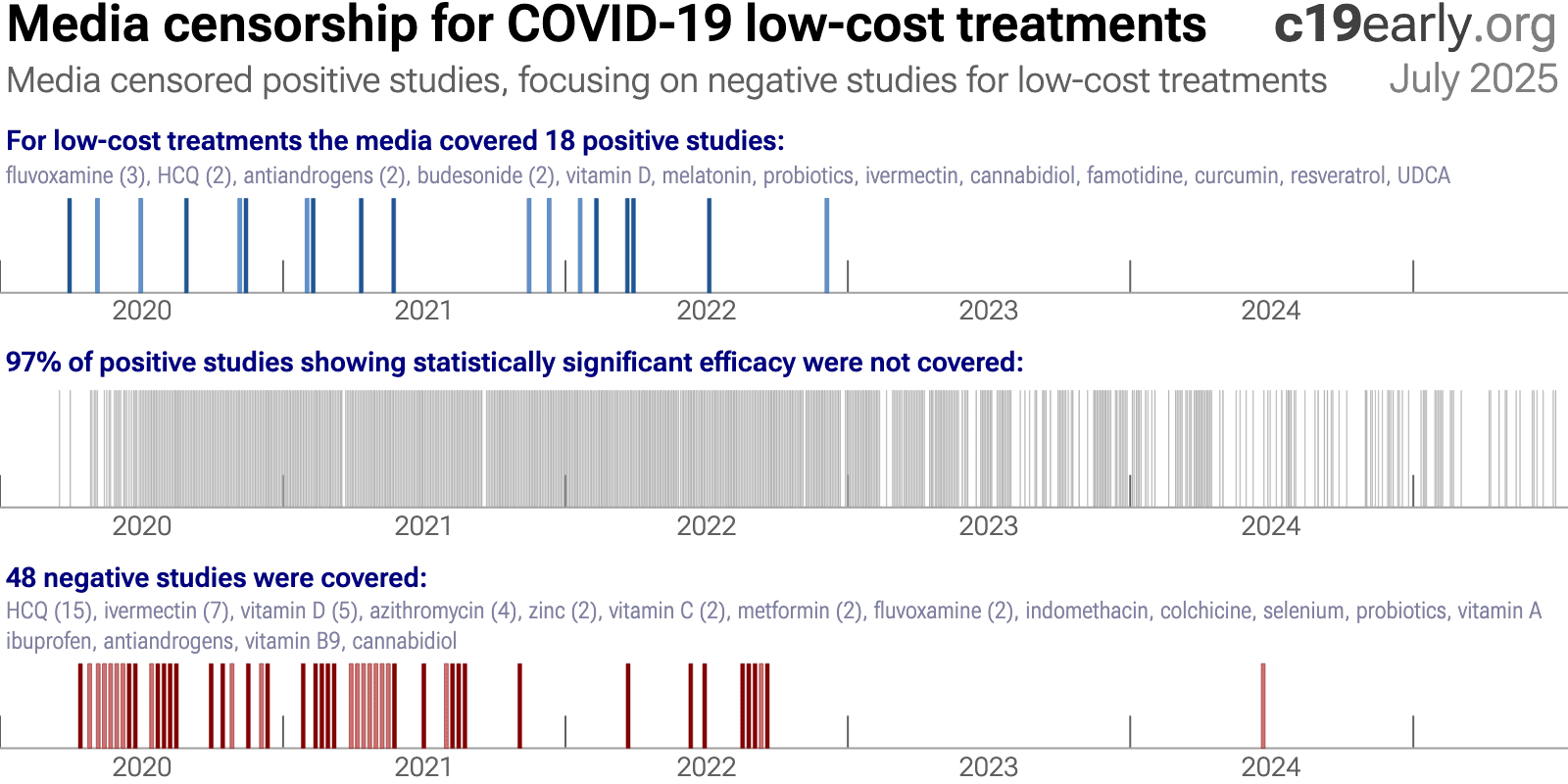
Top journals that accept positive studies for low cost treatments:
Nutrients,
Scientific Reports,
PLOS ONE,
International Journal of Infectious Diseases,
Frontiers in Medicine,
Cureus,
more...
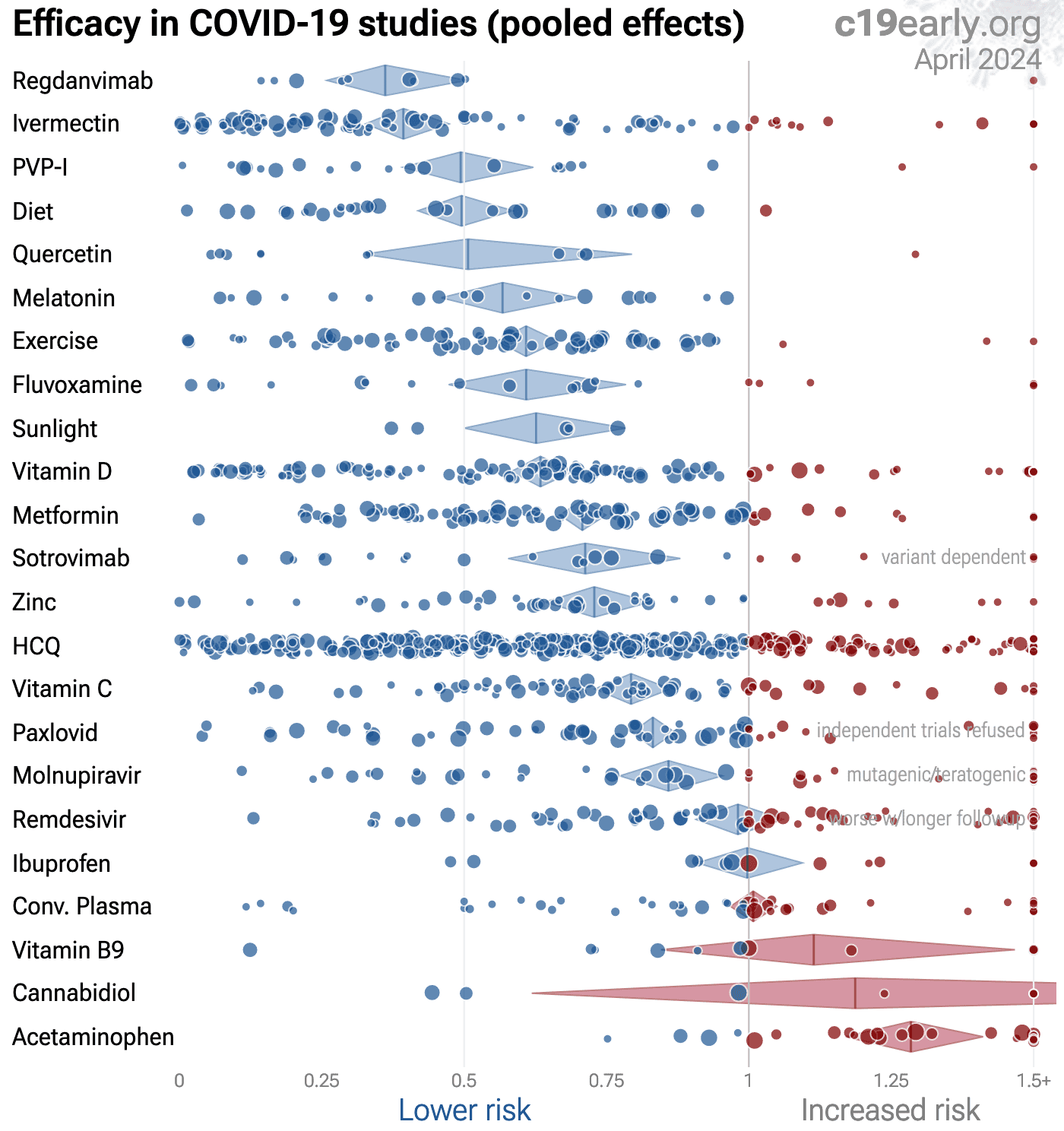
| Random-effects meta-analysis of all studies (pooled effects, all stages). Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all stages and outcomes depend on the distribution of stages and outcomes tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage and outcome analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
| Random-effects meta-analysis of early treatment studies (pooled effects). Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all outcomes are affected by the distribution of outcomes tested, please see detail pages for specific outcome analysis. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
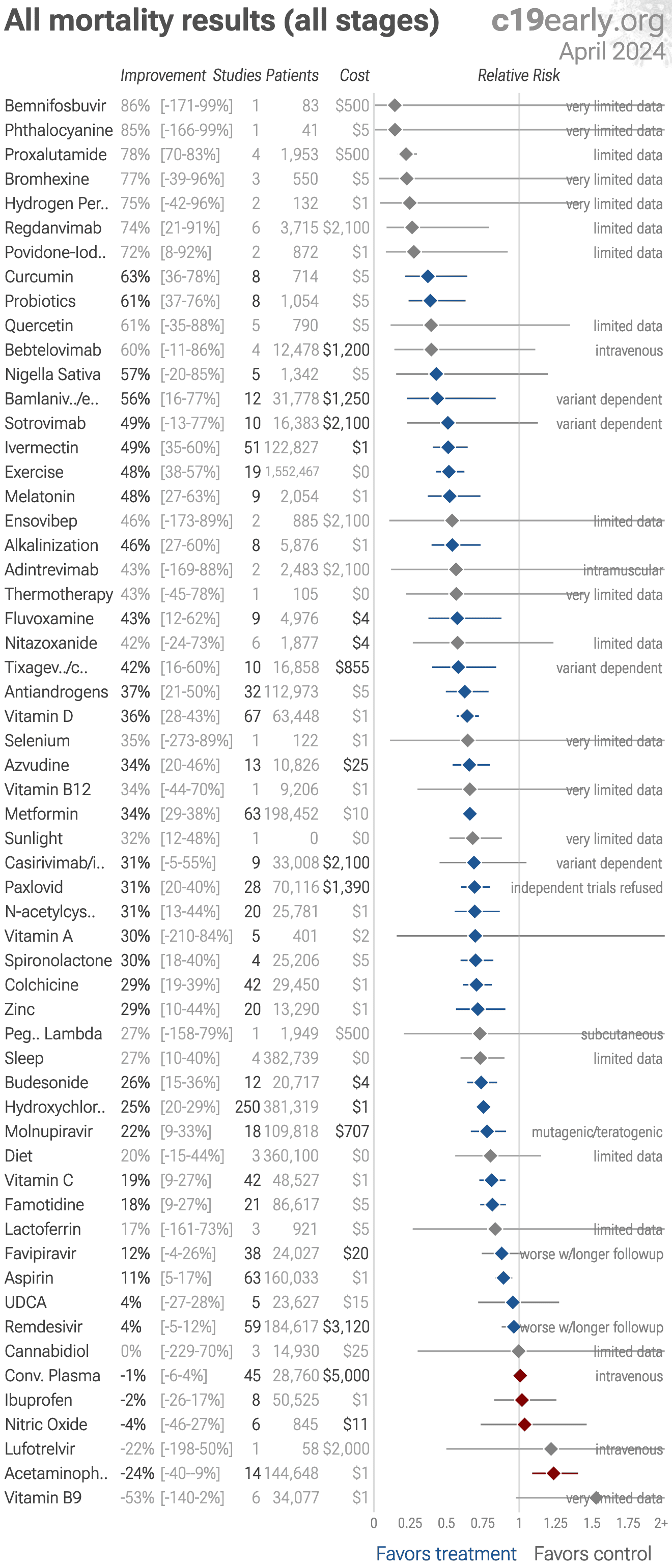
| Random-effects meta-analysis of all mortality results (all stages). Treatments with ≤3 studies with distinct authors or with <25 control events are shown in grey. Pooled results across all stages depend on the distribution of stages tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
| Random-effects meta-analysis of early treatment mortality results. Treatments with ≤3 studies with distinct authors or with <25 control events are shown in grey. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
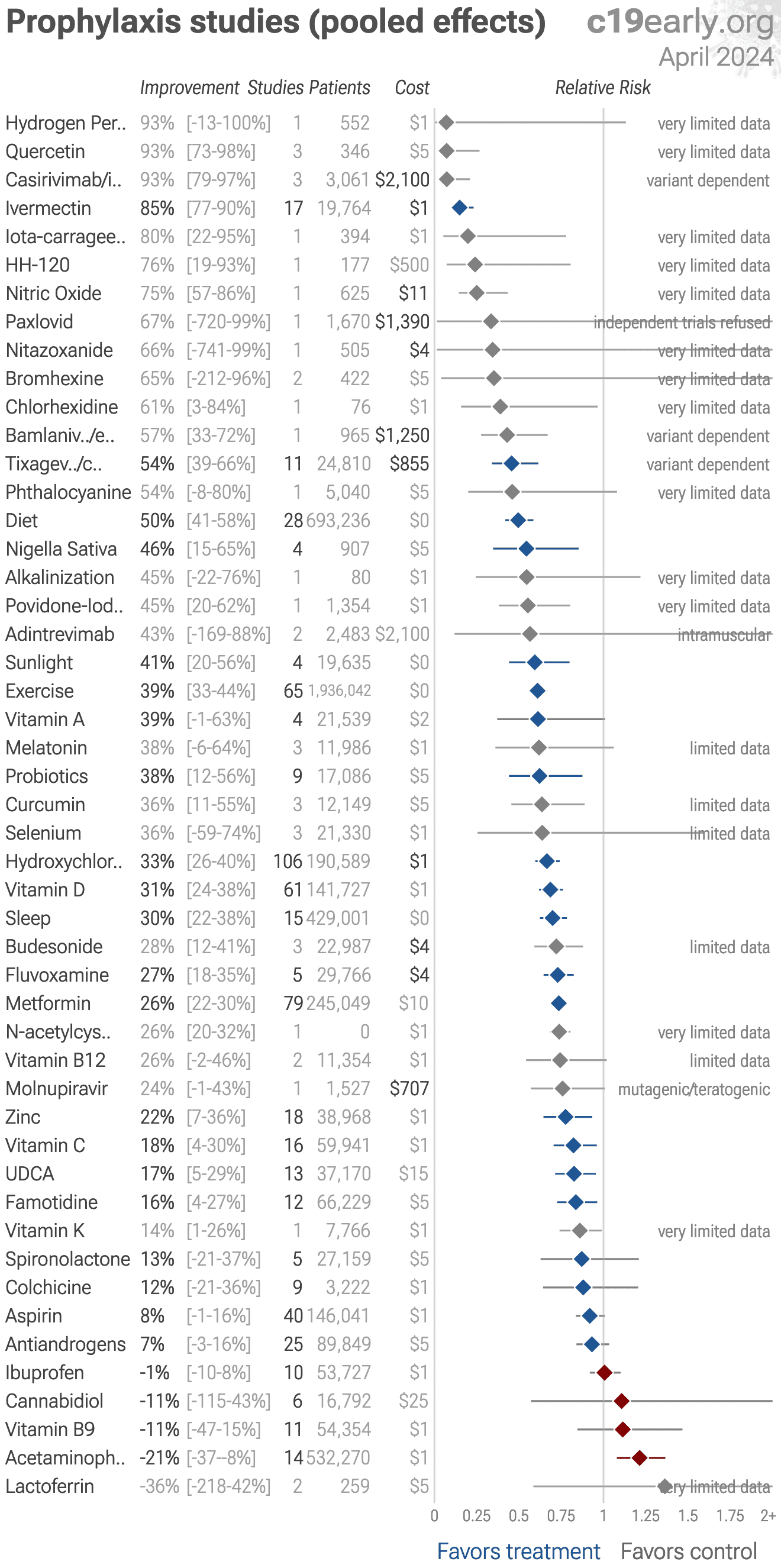
| Random-effects meta-analysis of prophylaxis studies (pooled effects). Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all outcomes are affected by the distribution of outcomes tested, please see detail pages for specific outcome analysis. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
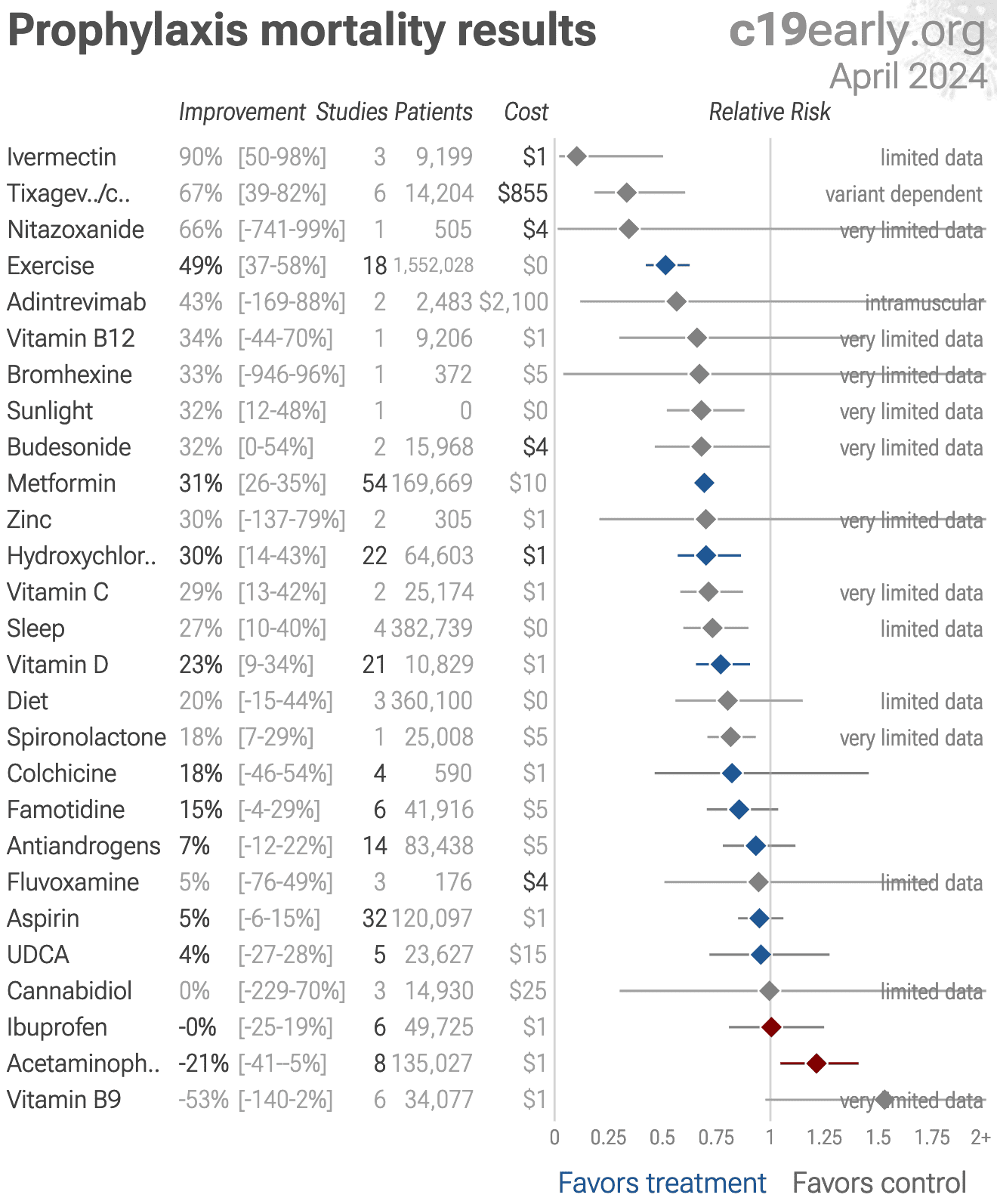
| Random-effects meta-analysis of prophylaxis mortality results. Treatments with ≤3 studies with distinct authors or with <25 control events are shown in grey. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
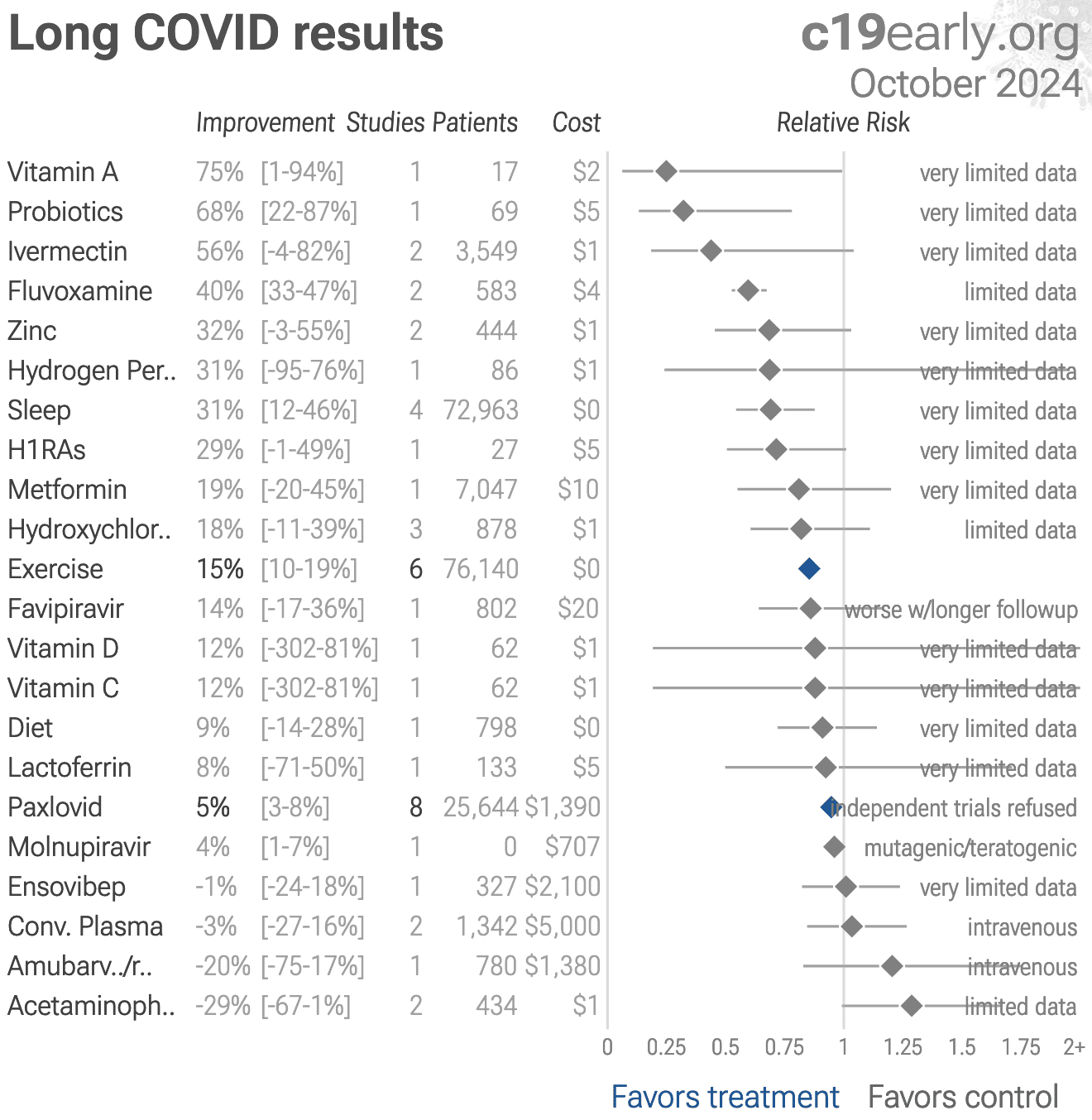
| Random-effects meta-analysis of long covid results. Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all stages and outcomes depend on the distribution of stages and outcomes tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage and outcome analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. | |||||
| Random-effects meta-analysis of transmission results. Treatments with ≤3 studies with distinct authors or with <50 control events are shown in grey. Pooled results across all stages and outcomes depend on the distribution of stages and outcomes tested - for example late stage treatment may be less effective and if the majority of studies are late stage this may obscure the efficacy of early treatment. Please see the specific stage and outcome analyses. Protocols typically combine multiple treatments which may be complementary and synergistic, and the SOC in studies often includes other treatments. 0.5% of proposed treatments show efficacy in clinical studies. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LATE TREATMENT | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. David Uip (*) | Brazil | 2,200 | 38.6% (850) | 2.5% (54) |
| Dr. Jake Scott (**) | USA | 1,000 | 10.0% (100) | |
| Average | 38.6% | 6.2% | ||
| EARLY TREATMENT PROTOCOLS - 40 physicians/teams | ||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath |
| Dr. Roberto Alfonso Accinelli 0/360 deaths for treatment within 3 days |
Peru | 1,265 | 0.6% (7) | |
| Dr. Mohammed Tarek Alam patients up to 84 years old |
Bangladesh | 100 | 0.0% (0) | |
| Dr. Oluwagbenga Alonge | Nigeria | 310 | 0.0% (0) | |
| Dr. Raja Bhattacharya up to 88yo, 81% comorbidities |
India | 148 | 1.4% (2) | |
| Dr. Flavio Cadegiani | Brazil | 3,450 | 0.1% (4) | 0.0% (0) |
| Dr. Alessandro Capucci | Italy | 350 | 4.6% (16) | |
| Dr. Shankara Chetty | South Africa | 8,000 | 0.0% (0) | |
| Dr. Deborah Chisholm | USA | 100 | 0.0% (0) | |
| Dr. Ryan Cole | USA | 400 | 0.0% (0) | 0.0% (0) |
| Dr. Marco Cosentino earlier treatment results were better |
Italy | 392 | 6.4% (25) | 0.3% (1) |
| Dr. Jeff Davis | USA | 6,000 | 0.0% (0) | |
| Dr. Dhanajay | India | 500 | 0.0% (0) | |
| Dr. Bryan Tyson & Dr. George Fareed | USA | 20,000 | 0.0% (6) | 0.0% (4) |
| Dr. Raphael Furtado | Brazil | 170 | 0.6% (1) | 0.0% (0) |
| Rabbi Yehoshua Gerzi | Israel | 860 | 0.1% (1) | 0.0% (0) |
| Dr. Heather Gessling | USA | 1,500 | 0.1% (1) | |
| Dr. Ellen Guimarães | Brazil | 500 | 1.6% (8) | 0.4% (2) |
| Dr. Syed Haider | USA | 4,000 | 0.1% (5) | 0.0% (0) |
| Dr. Mark Hancock | USA | 24 | 0.0% (0) | |
| Dr. Sabine Hazan | USA | 1,000 | 0.0% (0) | |
| Dr. Mollie James | USA | 3,500 | 1.1% (40) | 0.0% (1) |
| Dr. Roberta Lacerda | Brazil | 550 | 1.5% (8) | 0.4% (2) |
| Dr. Katarina Lindley | USA | 100 | 5.0% (5) | 0.0% (0) |
| Dr. Ben Marble | USA | 150,000 | 0.0% (4) | |
| Dr. Edimilson Migowski | Brazil | 2,000 | 0.3% (7) | 0.1% (2) |
| Dr. Abdulrahman Mohana | Saudi Arabia | 2,733 | 0.0% (0) | |
| Dr. Carlos Nigro | Brazil | 5,000 | 0.9% (45) | 0.5% (23) |
| Dr. Benoit Ochs | Luxembourg | 800 | 0.0% (0) | |
| Dr. Ortore | Italy | 240 | 1.2% (3) | 0.0% (0) |
| Dr. Valerio Pascua one patient already on oxygen died |
Honduras | 415 | 6.3% (26) | 0.2% (1) |
| Dr. Sebastian Pop | Romania | 300 | 0.0% (0) | |
| Dr. Brian Proctor | USA | 869 | 2.3% (20) | 0.2% (2) |
| Dr. Anastacio Queiroz | Brazil | 700 | 0.0% (0) | |
| Dr. Didier Raoult | France | 8,315 | 2.6% (214) | 0.1% (5) |
| Dr. Karin Ried up to 99yo, 73% comorbidities |
Turkey | 237 | 0.4% (1) | |
| Dr. Roman Rozencwaig patients up to 86 years old |
Canada | 80 | 0.0% (0) | |
| Dr. Vipul Shah | India | 8,000 | 0.1% (5) | |
| Dr. Silvestre Sobrinho | Brazil | 116 | 8.6% (10) | 0.0% (0) |
| Dr. Unknown | Brazil | 957 | 1.7% (16) | 0.2% (2) |
| Dr. Vladimir Zelenko | USA | 2,200 | 0.5% (12) | 0.1% (2) |
| Average | 2.2% | 0.1% | ||
Physicians using early combined treatment protocols had much lower
hospitalization and mortality rates compared with those following guidelines focusing on
late treatment.
Results are subject to selection and ascertainment bias and accurate analysis requires
details of the patient populations and followup, however the results are consistent across
many teams, and consistent with the extensive controlled clinical evidence showing a
significant reduction in risk with many early treatments, and complementary/synergistic
benefits with combined treatments.
(*) Dr. Uip reportedly prescribed early treatment for himself, but not for
patients1.
(**) Dr. Scott reports treating hundreds of patients and losing over a hundred,
but has not provided specific numbers2.
Dr. Scott reports following (and helping create) US guidelines.
| di Filippo | 114 patients prophylaxis: 50% fewer symptomatic cases (p=0.12) |
| Rahardjo | RCT 30 hospitalized COVID-19 patients in Indonesia showing significantly shorter length of hospital stay with convalescent plasma, however there are.. |
| Morikawa | Retrospective 283 hospitalized COVID-19 patients in Japan showing potential benefit with butyrate-producing Clostridium butyricum (CB)-containing.. |
| Bačić | Analysis of 74 participants (34 receiving a 12-week multi-strain probiotic containing Saccharomyces boulardii, Lacticaseibacillus rhamnosus GG, and.. |
| Soleimani | In vitro study showing benefit with postbiotics derived from Lacticaseibacillus rhamnosus GG and Bifidobacterium animalis subsp. lactis BB-12.. |
| Porta | Review of SARS-CoV-2 non-structural proteins as targets for direct-acting small-molecule antivirals. |
| Soto Albrecht | In vitro study showing that inhibition of mitochondrial oxidative phosphorylation (OXPHOS) enhances SARS-CoV-2 replication, while restoration of.. |
| Jia | Review of strategies for developing and engineering broadly neutralizing antibodies against SARS-CoV-2 to counteract rapid viral mutation and immune.. |
| Akinbolade | Review of existing medicines for viruses with epidemic or pandemic potential (Ebola, Marburg, influenza, mpox, MERS-CoV, SARS-CoV, and SARS-CoV-2),.. |
| Amahong | Integrative meta-analysis identifying conserved host protein targets shared across SARS-CoV-2, influenza A, Zika, and Dengue for potential host.. |
| Liu | Retrospective 300 elderly hospitalized COVID-19 patients in China, showing no mortality benefit with antivirals (paxlovid and molnupiravir) in.. |
| Kueper | 669 patients early treatment: 87% worse recovery (p=0.02) and 148% worse viral clearance (p=0.01) |
| Liu | Retrospective 300 elderly hospitalized COVID-19 patients in China, showing no mortality benefit with antivirals (paxlovid and molnupiravir) in.. |
| Kawai | 1,003 patient prophylaxis RCT: 67% lower hospitalization (p=0.5), 67% lower progression (p=0.5), and 1% fewer cases (p=1) |
| Torrejón-Guirado | 1,051 patients prophylaxis: 154% more cases (p=0.001) |
| Jara Rubio | 150 patient late treatment RCT: 23% higher mortality (p=0.56), 200% higher progression (p=0.14), no change in ICU admission (p=1), and 18% longer hospitalization (p=0.41) |
| Setz | In vitro study showing synergistic antiviral activity of black elderberry fruit extract and iota-carrageenan against SARS-CoV-2 Omicron, influenza A.. |
| Setz | In vitro study showing synergistic antiviral activity of black elderberry fruit extract and iota-carrageenan against SARS-CoV-2 Omicron, influenza A.. |
| Widyarman | RCT 40 COVID-19 outpatients showing lower salivary SARS-CoV-2 viral load with cetylpyridinium chloride (CPC), povidone-iodine (PVP-I), and sodium.. |
| Widyarman | RCT 40 COVID-19 outpatients showing lower salivary SARS-CoV-2 viral load with cetylpyridinium chloride (CPC), povidone-iodine (PVP-I), and sodium.. |
| Lakatos | 10 patient early treatment RCT: 62% lower progression (p=1) |
| Amal | Meta analysis of 17 studies with 229,142 autoimmune patients treated with HCQ, showing significantly lower mortality with HCQ use. |
| Strub-Wourgaft | 894 patient early treatment RCT: 20% higher progression (p=0.87) and 12% lower hospitalization (p=1) |
| Strub-Wourgaft | 960 patient early treatment RCT: 91% lower progression (p=0.37) and 5% lower hospitalization (p=1) |
Recent studies (see the individual treatment pages for all studies):
Jun 5 |
et al., Science Advances, doi:10.1126/sciadv.adz3081 | Mitochondrial OXPHOS restricts SARS-CoV-2 replication |
| In vitro study showing that inhibition of mitochondrial oxidative phosphorylation (OXPHOS) enhances SARS-CoV-2 replication, while restoration of OXPHOS restricts it, suggesting that compounds boosting OXPHOS (such as metformin) may have a.. | ||
Jun 3 |
et al., Viruses, doi:10.3390/v18060642 | Broad Neutralizing Antibodies Against SARS-CoV-2: Current Progress and Engineering Strategies |
| Review of strategies for developing and engineering broadly neutralizing antibodies against SARS-CoV-2 to counteract rapid viral mutation and immune escape. | ||
Jun 3 |
et al., Infectious Diseases and Therapy, doi:10.1007/s40121-026-01362-z | Prior SGLT2 Inhibitor and Metformin Use and Risk of Long COVID in Type 2 Diabetes: A Nationwide Population-Based Cohort Study |
| 20% lower long COVID (p=0.01). Retrospective 71,698 patients with type 2 diabetes in Singapore showing reduced risk of long COVID with prior metformin use and SGLT2 inhibitor use. | ||
Jun 2 |
et al., Interactive Journal of Medical Research, doi:10.2196/80263 | COVID-19 Rebound in Nirmatrelvir Plus Ritonavir Treatment and Control Groups: Prospective Cohort Study |
| 87% worse recovery (p=0.02) and 148% worse viral clearance (p=0.01). Prospective observational study of 669 COVID-19 outpatients in the USA showing higher rates of viral and symptom rebound with paxlovid. | ||
Jun 2 |
et al., Pharmaceutics, doi:10.3390/pharmaceutics18060693 | Targeting SARS-CoV-2 Non-Structural Proteins: A Blueprint for Next-Generation Small-Molecule Coronavirus Antivirals |
| Review of SARS-CoV-2 non-structural proteins as targets for direct-acting small-molecule antivirals. | ||
May 31 |
et al., AJPM Focus, doi:10.1016/j.focus.2026.100517 | Effects of green tea gargling on Coronavirus Disease-2019: A multi-center randomized controlled trial |
| 67% lower hospitalization (p=0.5), 67% lower progression (p=0.5), and 1% fewer cases (p=1). RCT 1,012 adults in Japan showing no statistically significant reduction in COVID-19 incidence with green tea gargling compared to water gargling. In the full analysis set, incidence was 5.4% in both groups. In the per-protocol set (PPS, .. | ||
May 29 |
et al., Medicine, doi:10.1097/MD.0000000000049099 | Independent mortality predictors in older COVID-19 patients with delayed hospitalization: A retrospective study from Eastern China, 2023 |
| Retrospective 300 elderly hospitalized COVID-19 patients in China, showing no mortality benefit with antivirals (paxlovid and molnupiravir) in multivariable analysis, OR 1.15 [0.28-4.74], without statistical significance. | ||
May 18 |
et al., NCT06945276 | A Phase 1 Study to Evaluate Relative Bioavailability and Food Effect of an ALG-097558 Tablet Formulation and the Drug-Drug Interaction Potential of ALG-097558 and Its Metabolite ALG-097730 in Healthy Volunteers |
| Phase 1 randomized study sponsored by NIAID, enrolling 51 healthy volunteers to characterize the bioavailability, food effect, and drug-drug interaction profile of ALG-097558. Co-administration with itraconazole (a strong CYP3A4/P-gp inhi.. | ||
May 18 |
et al., Briefings in Functional Genomics, doi:10.1093/bfgp/elag001 | An integrative meta-analysis of SARS-CoV-2 RNA–protein interactomes identifies conserved host factors shared with other RNA viruses |
| Integrative meta-analysis identifying conserved host protein targets shared across SARS-CoV-2, influenza A, Zika, and Dengue for potential host-directed antivirals. Drug-target annotation of the 275 conserved proteins identified 21 host p.. | ||
May 18 |
et al., Pharmacology Research & Perspectives, doi:10.1002/prp2.70271 | Repurposed Medicines for Viruses With Epidemic or Pandemic Potential: A Horizon Scan |
| Review of existing medicines for viruses with epidemic or pandemic potential (Ebola, Marburg, influenza, mpox, MERS-CoV, SARS-CoV, and SARS-CoV-2), identifying 196 technologies from published literature and 58 in active clinical developme.. | ||
May 17 |
et al., Virulence, doi:10.1080/21505594.2026.2673650 | Multicenter retrospective observational study on the clinical effectiveness of butyrate-producing Clostridium butyricum containing probiotics in patients with COVID-19 |
| Retrospective 283 hospitalized COVID-19 patients in Japan showing potential benefit with butyrate-producing Clostridium butyricum (CB)-containing probiotic preparations, however this study has a number of significant issues: Unreproducibl.. | ||
May 13 |
et al., International Journal of Molecular Sciences, doi:10.3390/ijms27104393 | Association of Serum Vitamin D and Hematological Parameters with SARS-CoV-2 PCR Positivity: A Combined Biomarker Approach in Asymptomatic Children |
| 53% fewer cases (p=0.0003). Retrospective 127 asymptomatic children with household COVID-19 exposure, showing lower vitamin D levels independently associated with SARS-CoV-2 PCR positivity. | ||
May 13 |
et al., Heliyon, doi:10.1016/j.heliyon.2026.e44988 | Vitamin D supplementation benefits COVID-19: A systematic review and meta-analysis |
| Systematic review and meta-analysis of 20 RCTs (n = 2,756) showing significantly lower mortality and ICU admission with vitamin D treatment for COVID-19. | ||
May 13 |
et al., Journal of Translational Medicine, doi:10.1186/s12967-026-08172-4 | In-depth serum proteomics atlas of COVID-19 defines a Severity-Resistance Index from a four-protein panel for disease severity and prognosis |
| Proteomics and machine learning study of 128 COVID-19 patients (57 mild, 51 severe) and 20 healthy controls, identifying a serum panel (CCN1, SELENBP1, PLA2G2A, SFTPB) and deriving a Severity-Resistance Index (SRI) for predicting severe C.. | ||
May 12 |
et al., European Journal of Haematology, doi:10.1111/ejh.70214 | Phase IIB, Randomized, Double‐Blind, Placebo‐Controlled Clinical Trial of Intravenous Defibrotide for the Prevention and Treatment of Respiratory Distress and Cytokine Release Syndrome in COVID-19 |
| 23% higher mortality (p=0.56), 200% higher progression (p=0.14), no change in ICU admission (p=1), and 18% longer hospitalization (p=0.41). RCT 150 hospitalized COVID-19 patients with respiratory failure showing no significant benefit with continuous IV defibrotide versus placebo. | ||
We aim to cover the most promising early treatments for
COVID-19. We use pre-specified effect extraction criteria that prioritizes
more serious outcomes, for details see methods. For specific
outcomes and different treatment stages see the individual pages.
References