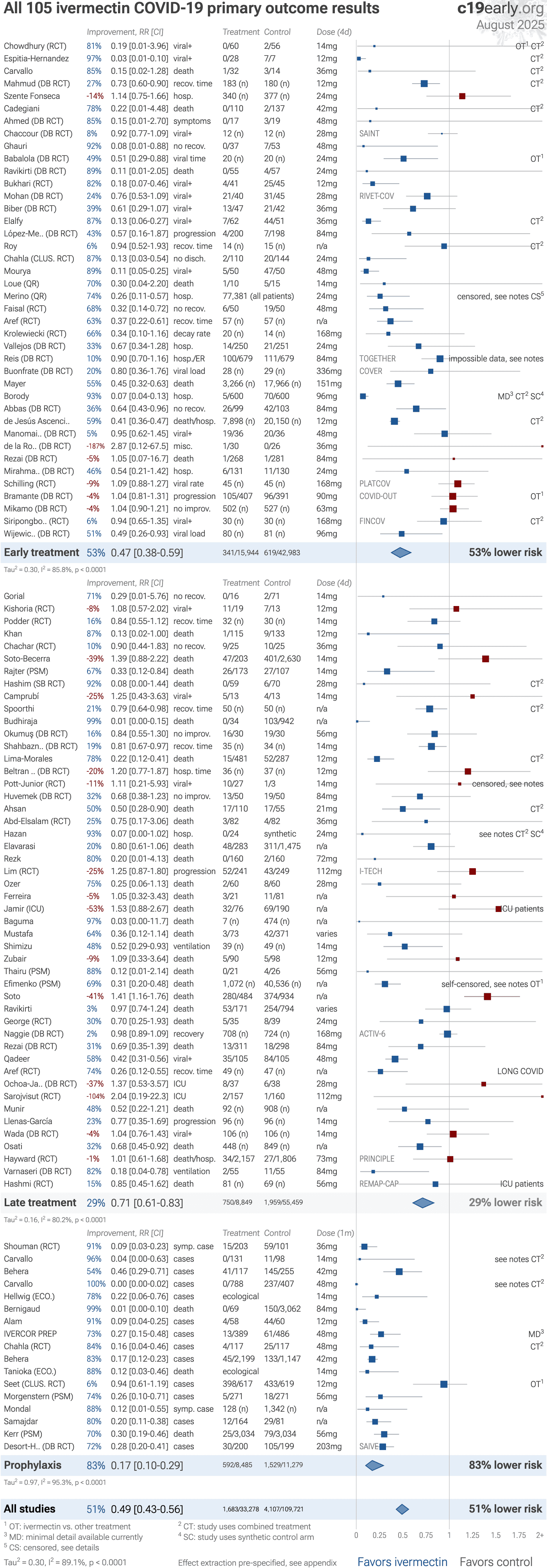
106 ivermectin COVID-19 controlled studies,
54 RCTs
Supplementary Data — Ivermectin reduces COVID-19 risk: real-time meta-analysis of 106 studies (c19ivm ivmmeta)
0
0.25
0.5
0.75
1
1.25
1.5
1.75
2+ Chowdhury (RCT) 81% 0.19 [0.01-3.96] 14mg viral+ 0/60 2/56 OT1 CT2 Improvement, RR [CI] Dose (4d) Treatment Control Espitia-Hernandez 97% 0.03 [0.01-0.10] 12mg viral+ 0/28 7/7 CT2 Carvallo 85% 0.15 [0.02-1.28] 36mg death 1/32 3/14 CT2 Mahmud (DB RCT) 27% 0.73 [0.60-0.90] 12mg recov. time 183 (n) 180 (n) CT2 Szente Fonseca -14% 1.14 [0.75-1.66] 24mg hosp. 340 (n) 377 (n) Cadegiani 78% 0.22 [0.01-4.48] 42mg death 0/110 2/137 CT2 Ahmed (DB RCT) 85% 0.15 [0.01-2.70] 48mg symptoms 0/17 3/19 SAINT Chaccour (DB RCT) 8% 0.92 [0.77-1.09] 28mg viral+ 12 (n) 12 (n) Ghauri 92% 0.08 [0.01-0.88] 48mg no recov. 0/37 7/53 Babalola (DB RCT) 49% 0.51 [0.29-0.88] 24mg viral time 20 (n) 20 (n) OT1 Bukhari (RCT) 82% 0.18 [0.07-0.46] 12mg viral+ 4/41 25/45 RIVET-COV Mohan (DB RCT) 24% 0.76 [0.53-1.09] 28mg viral+ 21/40 31/45 Biber (DB RCT) 39% 0.61 [0.29-1.07] 36mg viral+ 13/47 21/42 Elalfy 87% 0.13 [0.06-0.27] 36mg viral+ 7/62 44/51 CT2 López-Me.. (DB RCT) 43% 0.57 [0.16-1.87] 84mg progression 4/200 7/198 Chahla (CLUS. RCT) 87% 0.13 [0.03-0.54] 24mg no disch. 2/110 20/144 Mourya 89% 0.11 [0.05-0.25] 48mg viral+ 5/50 47/50 Loue (QR) 70% 0.30 [0.04-2.20] 14mg death 1/10 5/15 Merino (QR) 74% 0.26 [0.11-0.57] 24mg hosp. 77,381 (all patients) censored, see notes 5 Faisal (RCT) 68% 0.32 [0.14-0.72] 48mg no recov. 6/50 19/50 Aref (RCT) 63% 0.37 [0.22-0.61] n/a recov. time 57 (n) 57 (n) Krolewiecki (RCT) 66% 0.34 [0.10-1.16] 168mg decay rate 20 (n) 12 (n) Vallejos (DB RCT) 33% 0.67 [0.34-1.28] 24mg hosp. 14/250 21/251 TOGETHER Reis (DB RCT) 10% 0.90 [0.70-1.16] 84mg hosp./ER 100/679 111/679 impossible data, see notes COVER Buonfrate (DB RCT) 20% 0.80 [0.36-1.76] 336mg viral load 28 (n) 29 (n) Mayer 55% 0.45 [0.32-0.63] 151mg death 3,266 (n) 17,966 (n) Borody 93% 0.07 [0.04-0.13] 96mg hosp. 5/600 70/600 MD3 CT2 SC4 Abbas (DB RCT) 36% 0.64 [0.43-0.96] 84mg no recov. 26/99 42/103 de Jesús Ascenci.. 59% 0.41 [0.36-0.47] 12mg death/hosp. 7,898 (n) 20,150 (n) CT2 Manomai.. (DB RCT) 5% 0.95 [0.62-1.45] 48mg viral+ 19/36 20/36 de la Ro.. (DB RCT) -187% 2.87 [0.12-67.5] 36mg misc. 1/30 0/26 Rezai (DB RCT) -5% 1.05 [0.07-16.7] 84mg death 1/268 1/281 Mirahma.. (DB RCT) 46% 0.54 [0.21-1.42] 24mg hosp. 6/131 11/130 PLATCOV Schilling (RCT) -9% 1.09 [0.88-1.27] 168mg viral rate 45 (n) 45 (n) COVID-OUT Bramante (DB RCT) -4% 1.04 [0.81-1.31] 90mg progression 105/407 96/391 OT1 IVERMILCO Mikamo (DB RCT) -4% 1.04 [0.90-1.21] 63mg no improv. 502 (n) 527 (n) FINCOV Siripongbo.. (RCT) 6% 0.94 [0.65-1.35] 168mg viral+ 30 (n) 30 (n) CT2 Wijewic.. (DB RCT) 51% 0.49 [0.26-0.93] 96mg viral load 80 (n) 81 (n) Mouawia (RCT) 56% 0.44 [0.14-1.37] 12mg hosp. 4/63 9/63 Tau2 = 0.30, I2 = 86.1%, p < 0.0001 Early treatment 54% 0.46 [0.37-0.58] 345/15,938 624/42,972 54% lower risk Gorial 71% 0.29 [0.01-5.76] 14mg no recov. 0/16 2/71 Improvement, RR [CI] Dose (4d) Treatment Control Kishoria (RCT) -8% 1.08 [0.57-2.02] 12mg viral+ 11/19 7/13 Podder (RCT) 16% 0.84 [0.55-1.12] 14mg recov. time 32 (n) 30 (n) Khan 87% 0.13 [0.02-1.00] 12mg death 1/115 9/133 Chachar (RCT) 10% 0.90 [0.44-1.83] 36mg no recov. 9/25 10/25 Soto-Becerra -39% 1.39 [0.88-2.22] 14mg death 47/203 401/2,630 Rajter (PSM) 67% 0.33 [0.12-0.84] 14mg death 26/173 27/107 Hashim (SB RCT) 92% 0.08 [0.00-1.44] 28mg death 0/59 6/70 CT2 Camprubí -25% 1.25 [0.43-3.63] 14mg viral+ 5/13 4/13 Spoorthi 21% 0.79 [0.64-0.98] n/a recov. time 50 (n) 50 (n) CT2 Budhiraja 99% 0.01 [0.00-0.15] n/a death 0/34 103/942 Ravikirti (DB RCT) 89% 0.11 [0.01-2.05] 24mg death 0/55 4/57 Okumuş (DB RCT) 16% 0.84 [0.55-1.30] 56mg no improv. 16/30 19/30 Shahbazn.. (DB RCT) 19% 0.81 [0.67-0.97] 14mg recov. time 35 (n) 34 (n) Lima-Morales 78% 0.22 [0.12-0.41] 12mg death 15/481 52/287 CT2 Beltran .. (DB RCT) -20% 1.20 [0.77-1.87] 12mg hosp. time 36 (n) 37 (n) Pott-Junior (RCT) -11% 1.11 [0.21-5.93] 14mg viral+ 10/27 1/3 censored, see notes Huvemek (DB RCT) 32% 0.68 [0.38-1.23] 84mg no improv. 13/50 19/50 Ahsan 50% 0.50 [0.28-0.90] 21mg death 17/110 17/55 CT2 Abd-Elsalam (RCT) 25% 0.75 [0.17-3.06] 36mg death 3/82 4/82 Hazan 93% 0.07 [0.00-1.02] 24mg hosp. 0/24 synthetic see notes 2 SC4 Elavarasi 20% 0.80 [0.61-1.06] n/a death 48/283 311/1,475 Rezk 80% 0.20 [0.01-4.13] 72mg death 0/160 2/160 I-TECH Lim (RCT) -25% 1.25 [0.87-1.80] 112mg progression 52/241 43/249 Ozer 75% 0.25 [0.06-1.13] 28mg death 2/60 8/60 Ferreira -5% 1.05 [0.32-3.43] n/a death 3/21 11/81 Jamir (ICU) -53% 1.53 [0.88-2.67] n/a death 32/76 69/190 ICU patients Baguma 97% 0.03 [0.00-11.7] n/a death 7 (n) 474 (n) Mustafa 64% 0.36 [0.12-1.14] varies death 3/73 42/371 Shimizu 48% 0.52 [0.29-0.93] 14mg ventilation 39 (n) 49 (n) Zubair -9% 1.09 [0.33-3.64] 12mg death 5/90 5/98 Thairu (PSM) 88% 0.12 [0.01-2.14] 56mg death 0/21 4/26 Efimenko (PSM) 69% 0.31 [0.20-0.48] n/a death 1,072 (n) 40,536 (n) self-censored, see notes 1 Soto -41% 1.41 [1.16-1.76] n/a death 280/484 374/934 Ravikirti 3% 0.97 [0.74-1.24] varies death 53/171 254/794 George (RCT) 30% 0.70 [0.25-1.93] 24mg death 5/35 8/39 ACTIV-6 Naggie (DB RCT) 2% 0.98 [0.89-1.09] 168mg recovery 708 (n) 724 (n) Rezai (DB RCT) 31% 0.69 [0.35-1.39] 84mg death 13/311 18/298 Qadeer 58% 0.42 [0.31-0.56] 48mg viral+ 35/105 84/105 Aref (RCT) 74% 0.26 [0.12-0.55] n/a recov. time 49 (n) 47 (n) LONG COVID Ochoa-Ja.. (DB RCT) -37% 1.37 [0.53-3.57] 28mg ICU 8/37 6/38 Sarojvisut (RCT) -104% 2.04 [0.19-22.3] 112mg ICU 2/157 1/160 Munir 48% 0.52 [0.22-1.21] n/a death 92 (n) 908 (n) Llenas-García 23% 0.77 [0.35-1.69] 14mg progression 96 (n) 96 (n) Wada (DB RCT) -4% 1.04 [0.76-1.43] 14mg viral+ 106 (n) 106 (n) Osati 32% 0.68 [0.45-0.92] n/a death 448 (n) 849 (n) PRINCIPLE Hayward (RCT) -1% 1.01 [0.61-1.68] 73mg death/hosp. 34/2,157 27/1,806 Varnaseri (DB RCT) 82% 0.18 [0.04-0.78] 84mg ventilation 2/55 11/55 REMAP-CAP Hashmi (RCT) 26% 0.74 [0.38-1.47] 56mg death 81 (n) 69 (n) ICU patients Tau2 = 0.16, I2 = 80.2%, p < 0.0001 Late treatment 29% 0.71 [0.60-0.83] 750/8,904 1,963/55,516 29% lower risk Shouman (RCT) 91% 0.09 [0.03-0.23] 36mg symp. case 15/203 59/101 Improvement, RR [CI] Dose (1m) Treatment Control Carvallo 96% 0.04 [0.00-0.63] 14mg cases 0/131 11/98 see notes 2 Behera 54% 0.46 [0.29-0.71] 42mg cases 41/117 145/255 Carvallo 100% 0.00 [0.00-0.02] 48mg cases 0/788 237/407 see notes 2 Hellwig (ECO.) 78% 0.22 [0.06-0.76] 14mg cases ecological Bernigaud 99% 0.01 [0.00-0.10] 84mg death 0/69 150/3,062 Alam 91% 0.09 [0.04-0.25] 12mg cases 4/58 44/60 IVERCOR PREP 73% 0.27 [0.15-0.48] 48mg cases 13/389 61/486 MD3 Chahla (RCT) 84% 0.16 [0.04-0.46] 48mg cases 4/117 25/117 CT2 Behera 83% 0.17 [0.12-0.23] 42mg cases 45/2,199 133/1,147 Tanioka (ECO.) 88% 0.12 [0.03-0.46] 14mg death ecological Seet (CLUS. RCT) 6% 0.94 [0.61-1.19] 12mg cases 398/617 433/619 OT1 Morgenstern (PSM) 74% 0.26 [0.10-0.71] 56mg cases 5/271 18/271 Mondal 88% 0.12 [0.01-0.55] n/a symp. case 128 (n) 1,342 (n) Samajdar 80% 0.20 [0.11-0.38] n/a cases 12/164 29/81 Kerr (PSM) 70% 0.30 [0.19-0.46] 56mg death 25/3,034 79/3,034 SAIVE Desort-H.. (DB RCT) 72% 0.28 [0.20-0.41] 203mg cases 30/200 105/199 Wagstaff (DB RCT) 55% 0.45 [0.22-1.00] DAFS 36 (n) 32 (n) Tau2 = 0.94, I2 = 95.0%, p < 0.0001 Prophylaxis 82% 0.18 [0.11-0.31] 592/8,521 1,529/11,311 82% lower risk All studies 51% 0.49 [0.43-0.56] 1,687/33,363 4,116/109,799 51% lower risk All 106 ivermectin COVID-19 primary outcome results c19 early .org August 2026 Tau2 = 0.29, I2 = 89.1%, p < 0.0001 Effect extraction pre-specified, see appendix 1 OT: ivermectin vs. other treatment 3 MD: minimal detail available currently 5 CS: censored, see details 2 CT: study uses combined treatment 4 SC: study uses synthetic control arm Favors ivermectin Favors control
Fig. S1. Random-effects meta-analysis for
primary outcomes (as defined before the trial started).
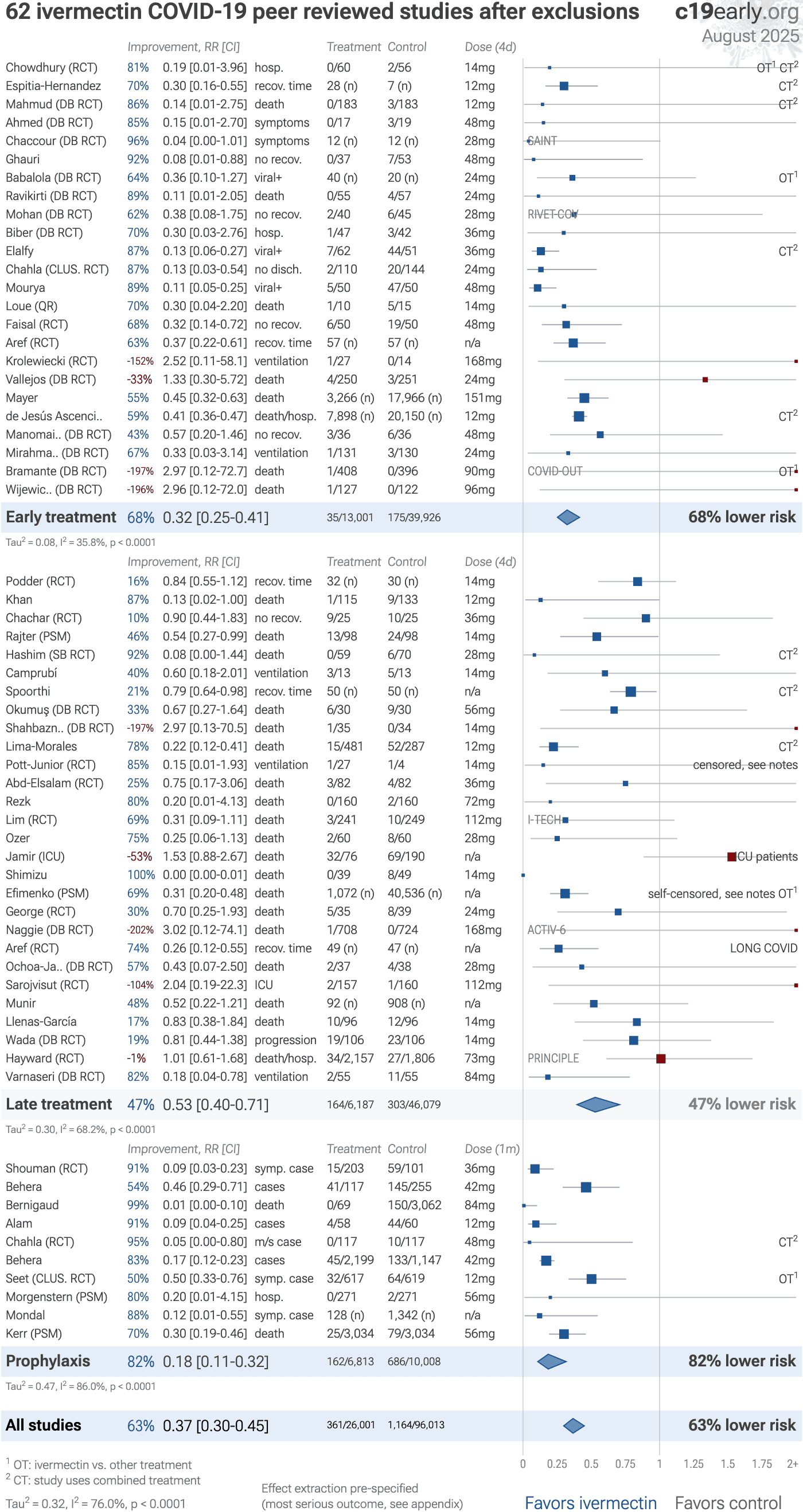
Fig. S2. Random-effects meta-analysis for
peer-reviewed studies after exclusions.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below .
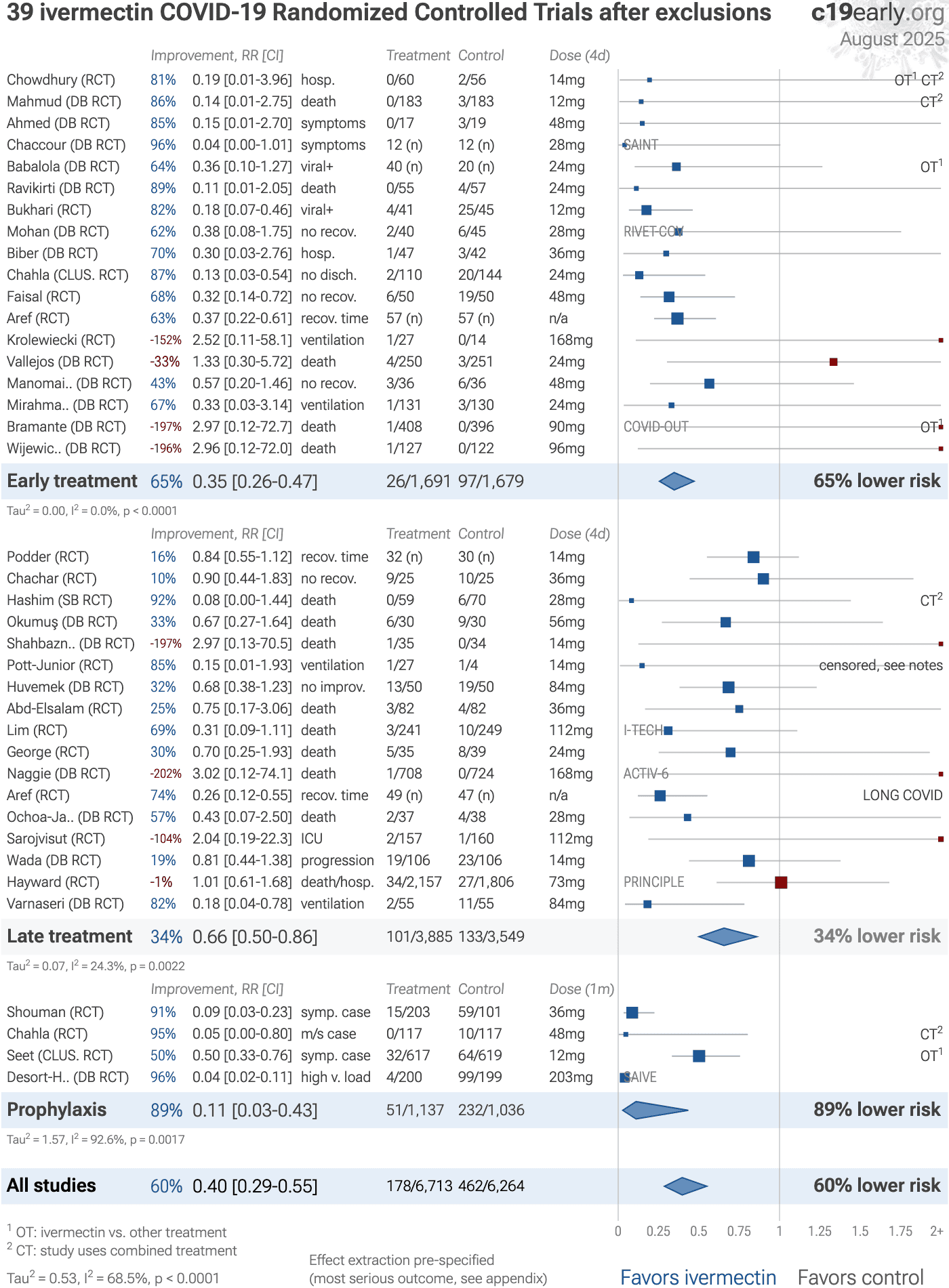
Fig. S3. Random-effects meta-analysis for
RCT studies after exclusions.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below .
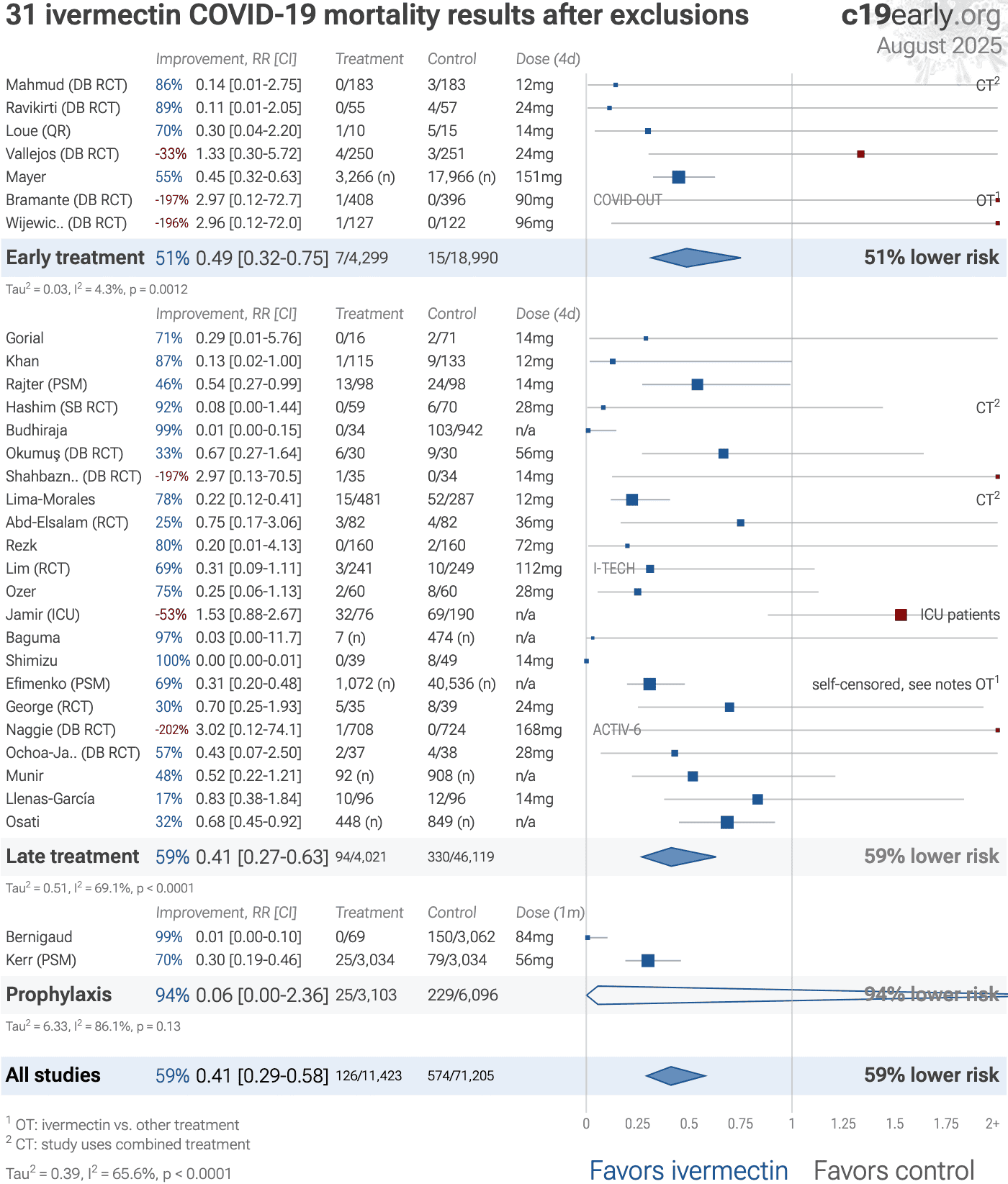
Fig. S4. Random-effects meta-analysis for
mortality after exclusions.
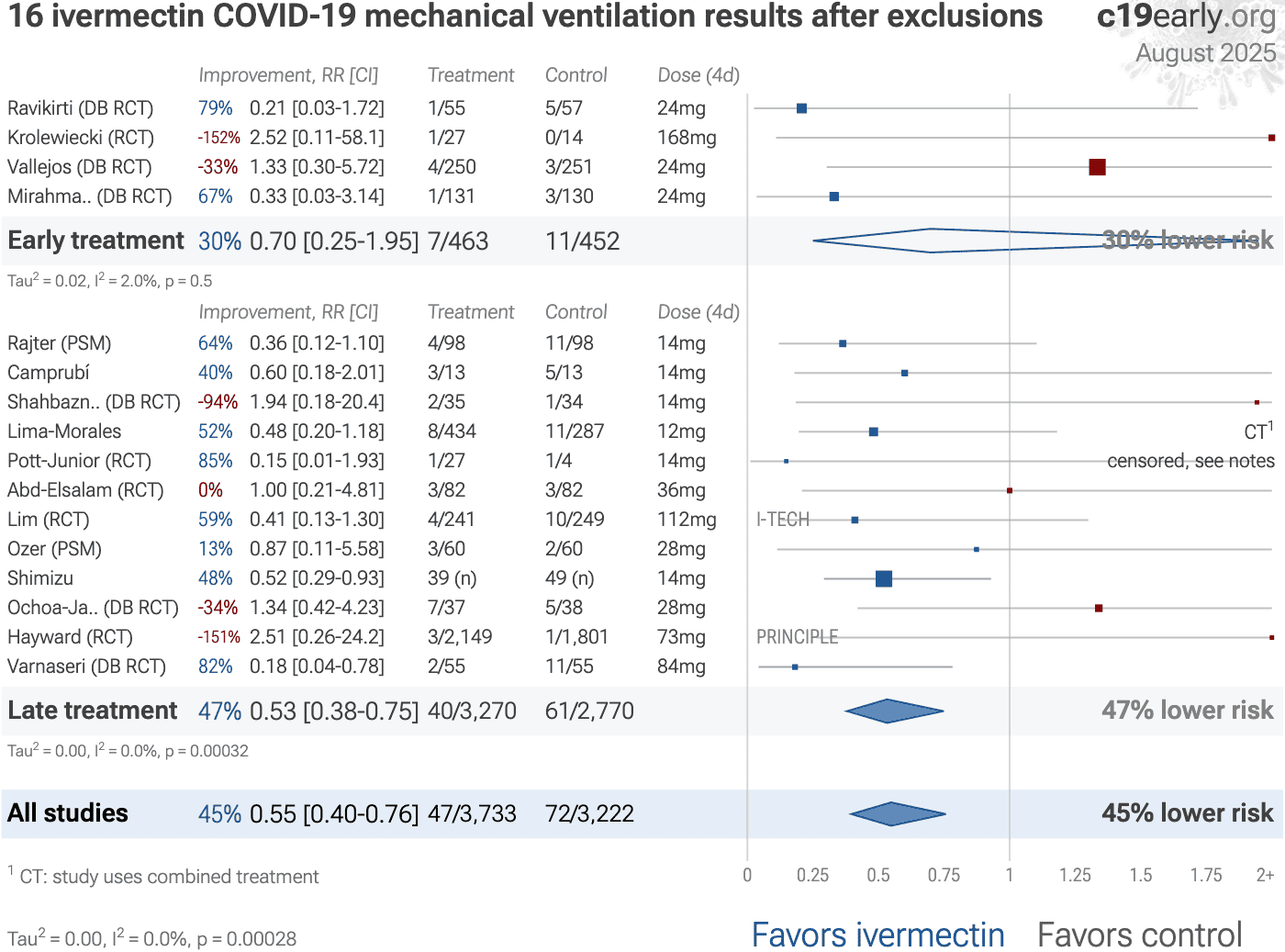
Fig. S5. Random-effects meta-analysis for
mechanical ventilation after exclusions.
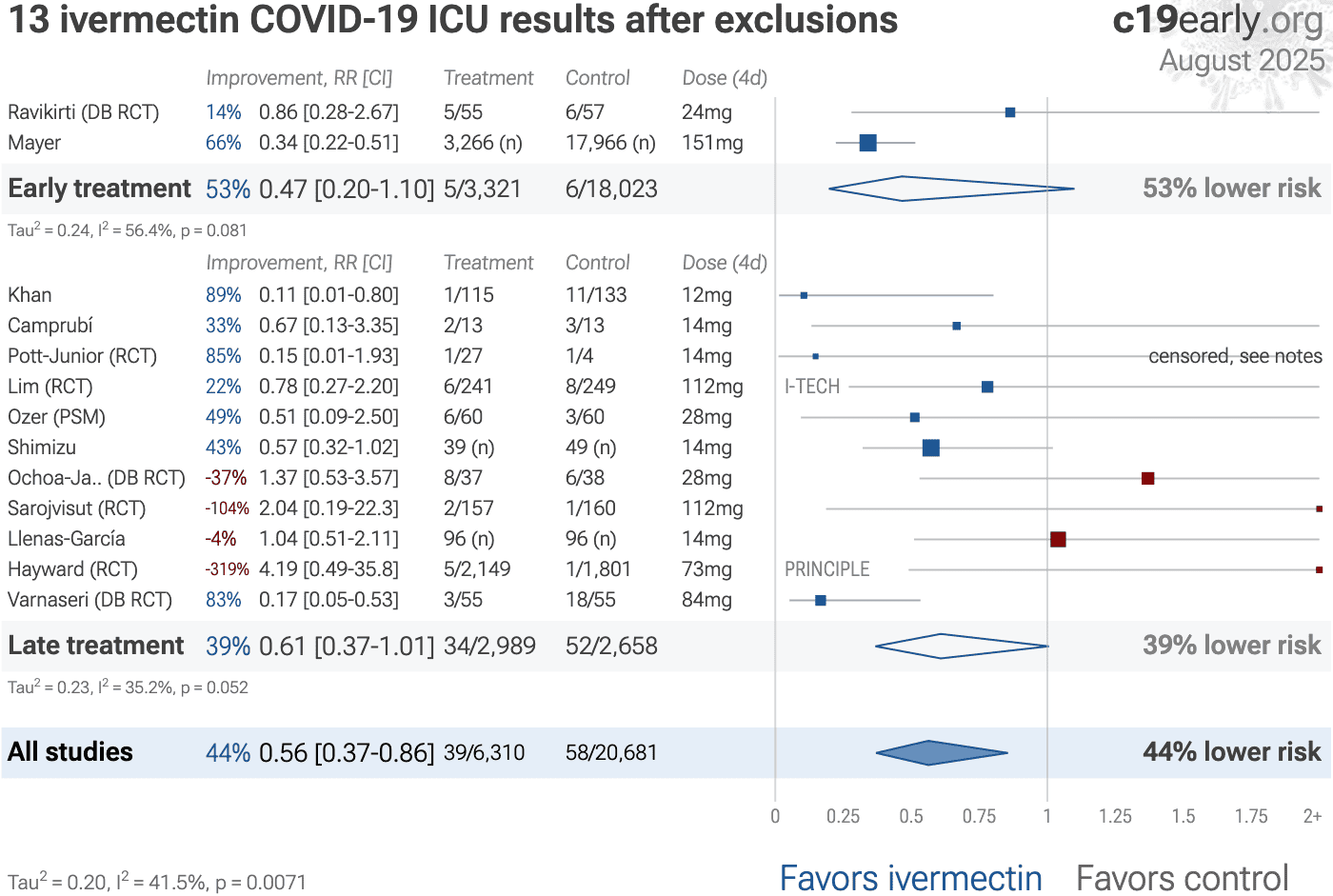
Fig. S6. Random-effects meta-analysis for
ICU admission after exclusions.
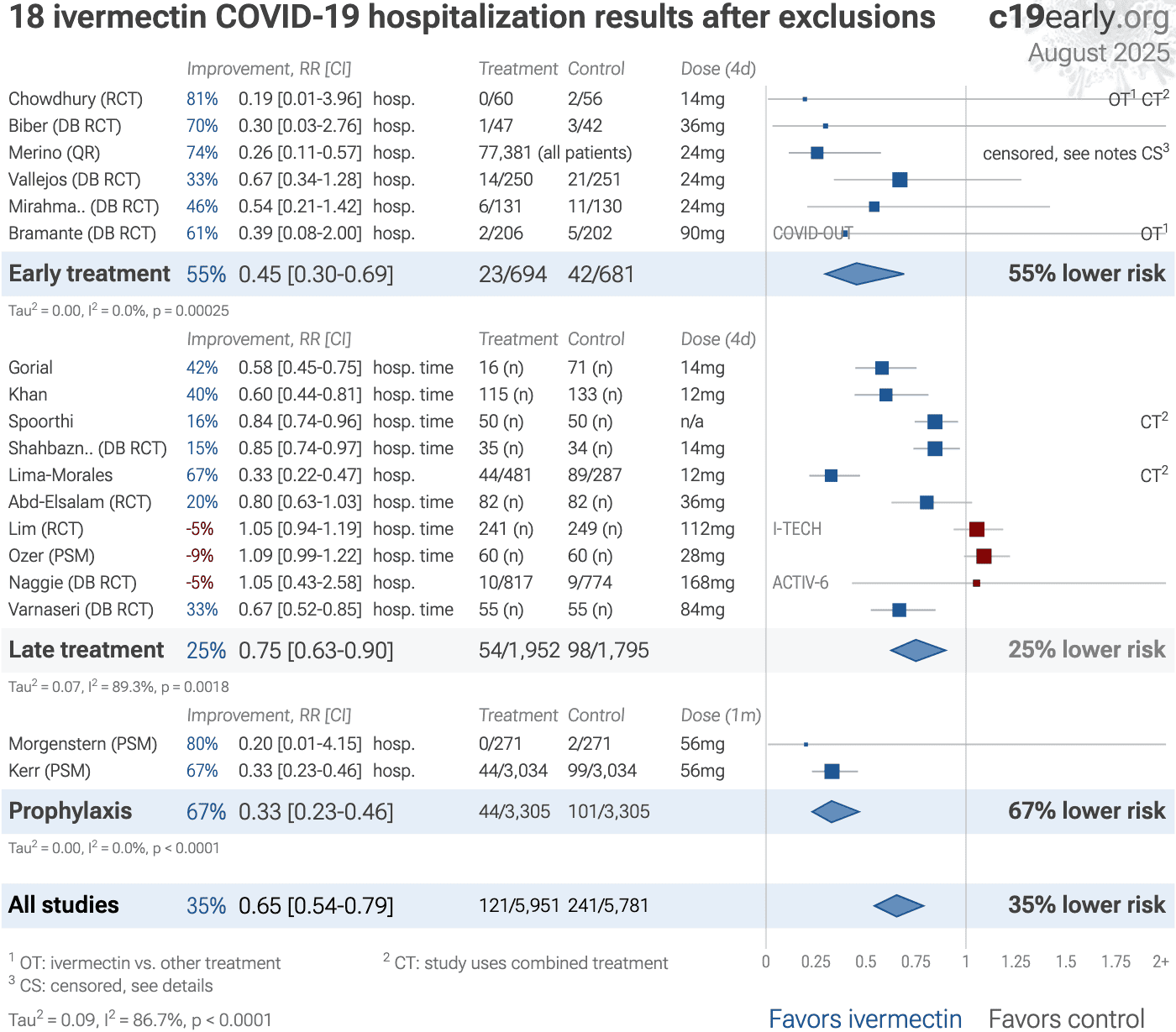
Fig. S7. Random-effects meta-analysis for
hospitalization after exclusions.
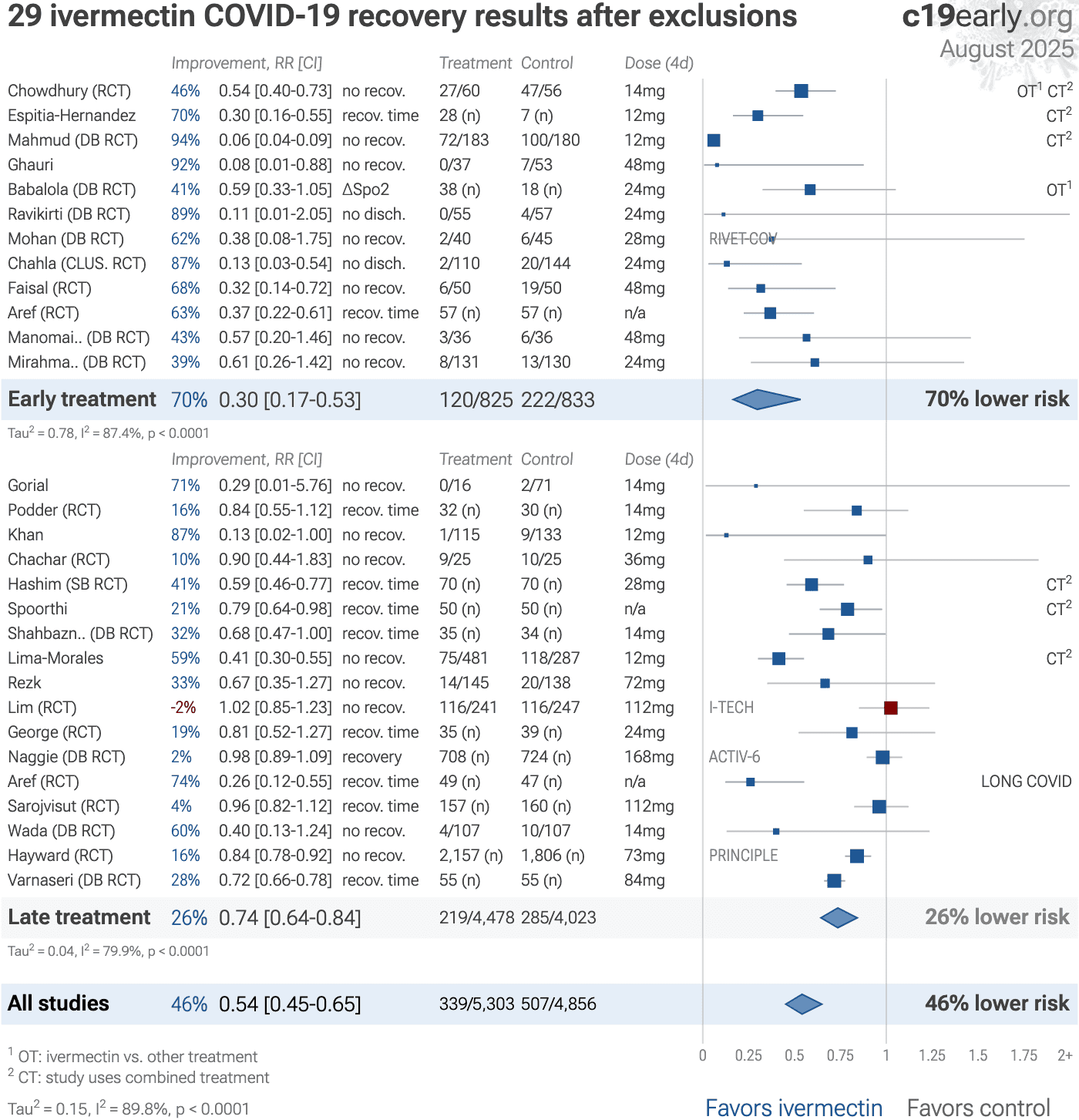
Fig. S8. Random-effects meta-analysis for
recovery results only after exclusions.
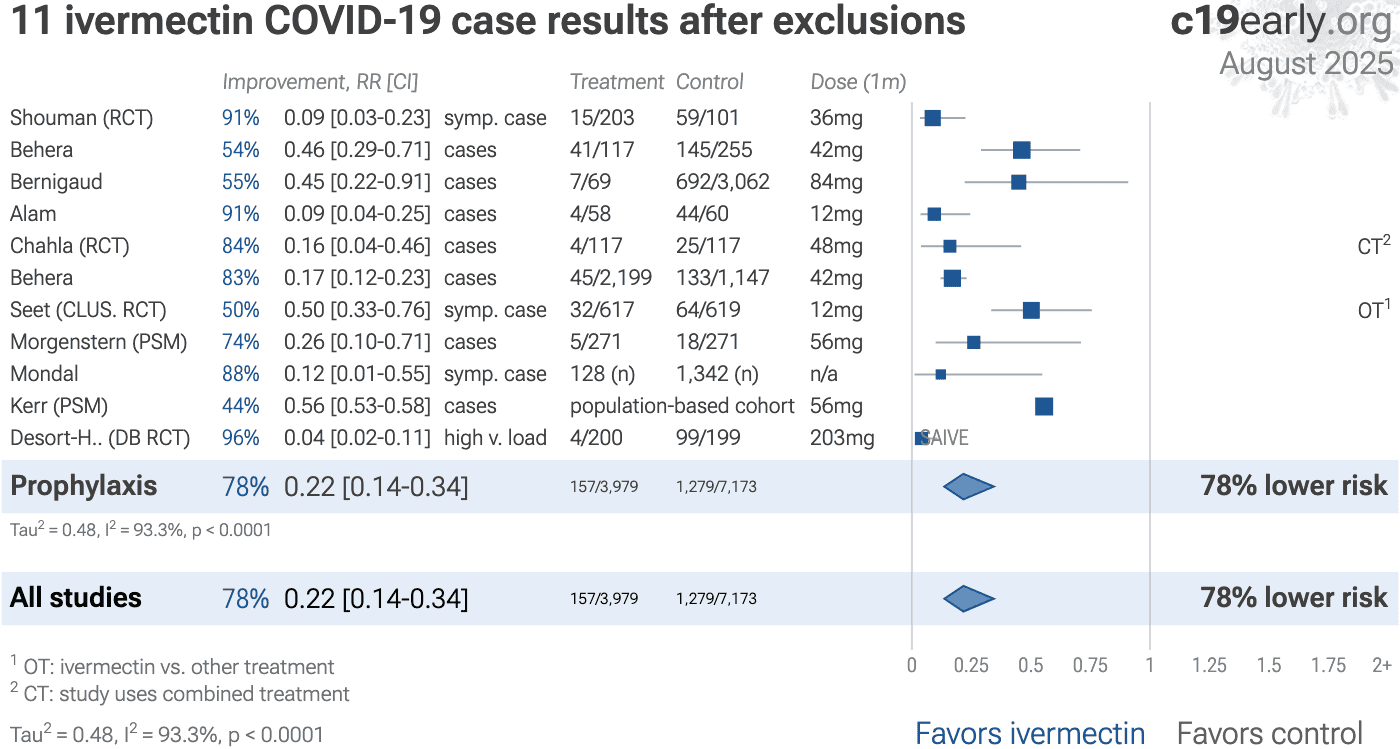
Fig. S9. Random-effects meta-analysis for
COVID-19 case results after exclusions.
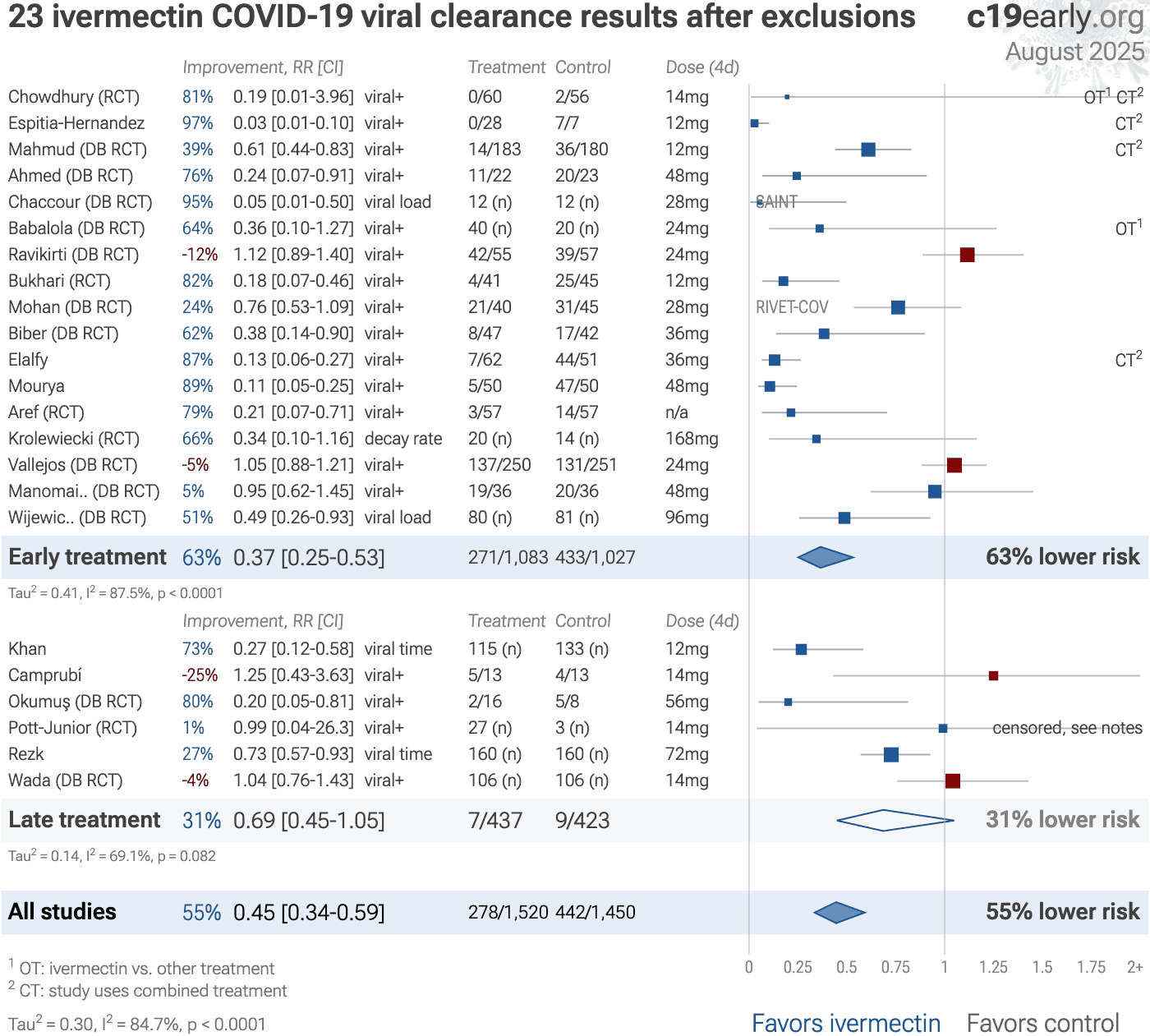
Fig. S10. Random-effects meta-analysis for
viral clearance after exclusions.
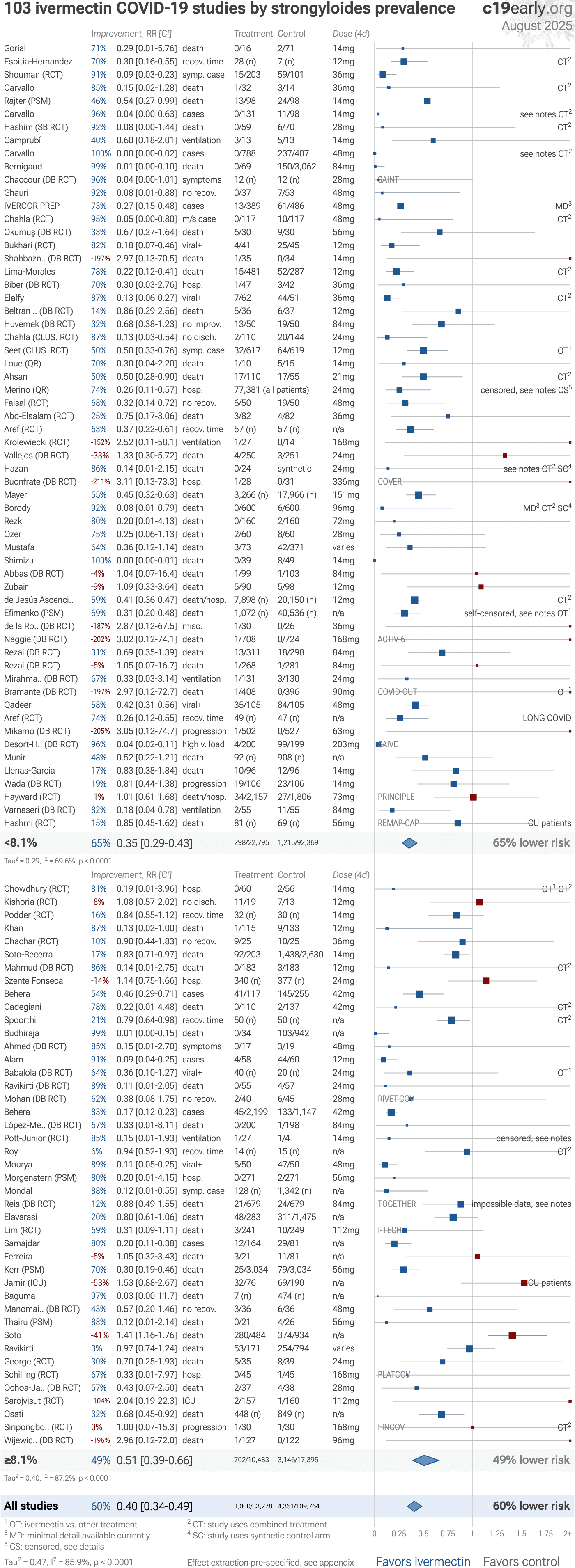
Fig. S11. Random-effects meta-analysis
for studies grouped by strongyloides prevalence.
Data is by
country and from Buonfrate
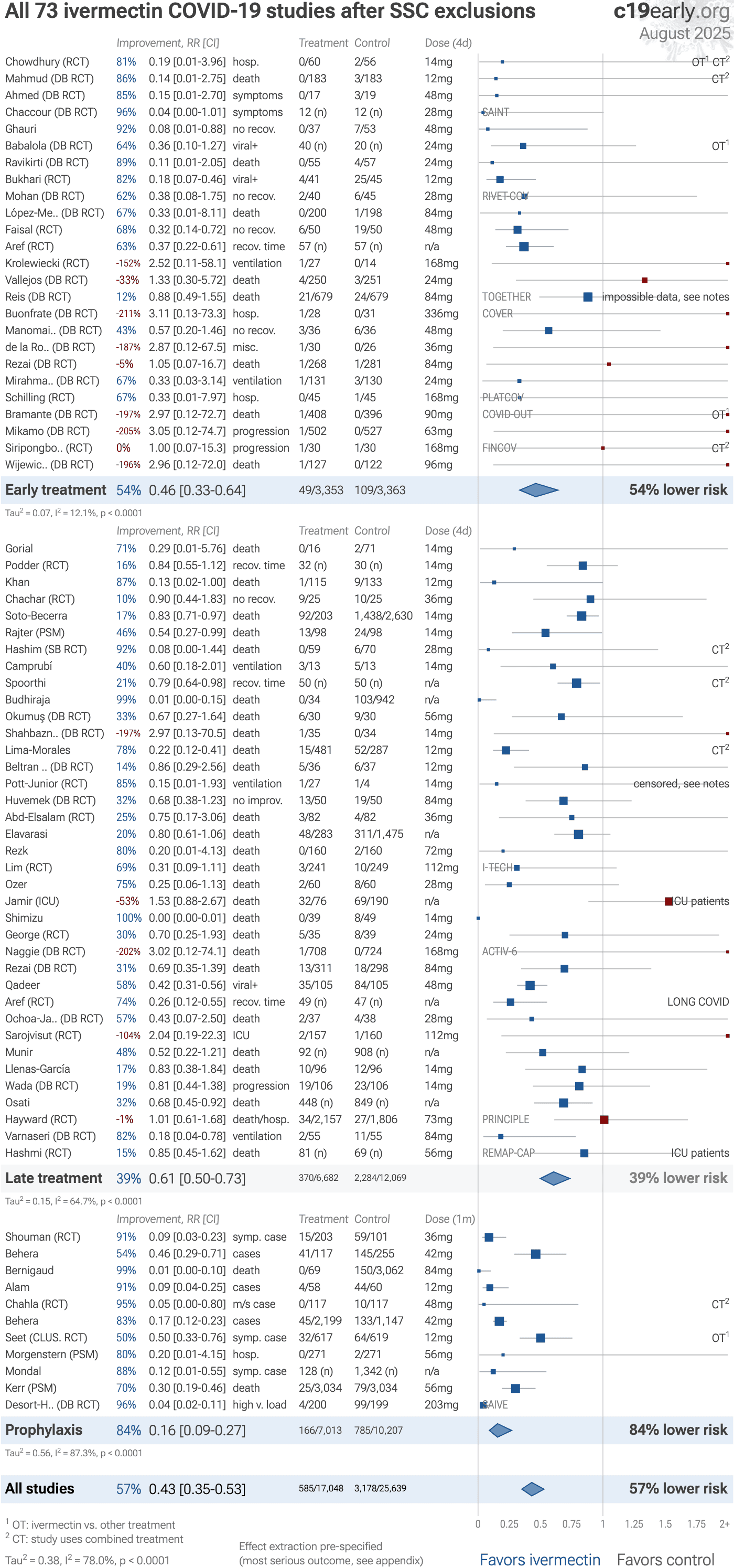
Fig. S12. Random-effects meta-analysis
with SSC exclusions.
SSC has not reviewed late treatment and prophylaxis
trials. SSC exclusions are from Nov 27, 2021.
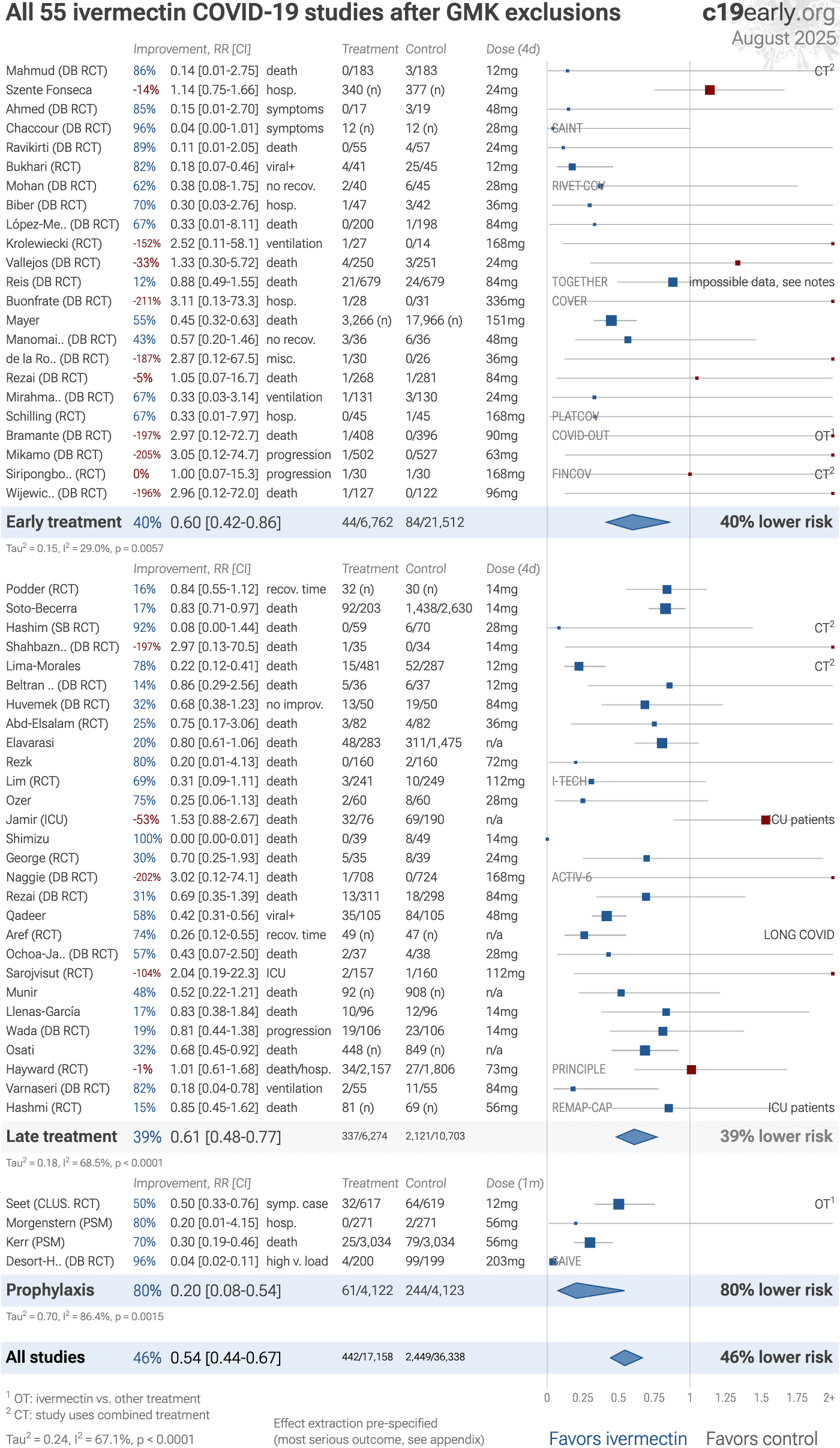
Fig. S13. Random-effects meta-analysis
with GMK exclusions.
Our main exclusion analyses already exclude all studies
where the GMK team believes there are major data issues. This analysis
corresponds with GMK's recommendation for meta-analysis as of Oct 26, 2021.
GMK excludes most non-RCT studies, with the notable exception of several
studies with major issues that report negative or relatively poor results
— Szente Fonseca Elavarasi Soto-Becerra details .
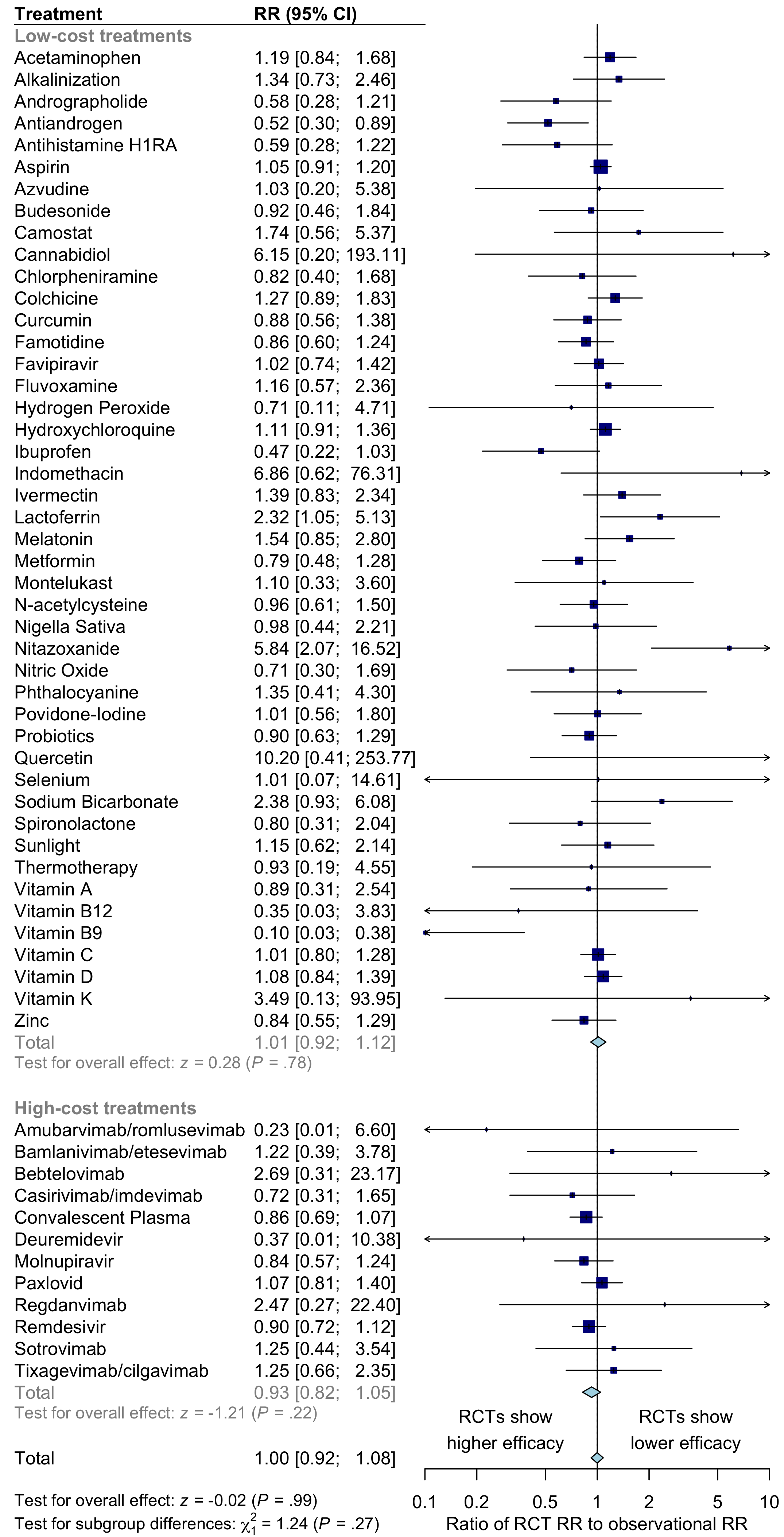
Fig. S14. Comparison of results for RCTs versus observational studies.
For COVID-19 treatments, there is no significant difference between the results of RCTs and observational studies. Observational studies do not systematically over or underestimate efficacy. For high-cost treatments, there is a non-significant trend towards RCTs showing greater efficacy.
Please send us corrections, updates, or comments.
c19early involves the extraction of 200,000+ datapoints from
thousands of papers.
Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation.
IMA and
WCH
provide treatment protocols.
Submit
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}