Cardiovascular Outcomes in COVID-19 Patients Treated with Paxlovid: A Multicenter Retrospective Study
et al., Acta Cardiol Sin, doi:10.6515/ACS.202601_42(1).20250726A, Jan 2026
{kind=link}
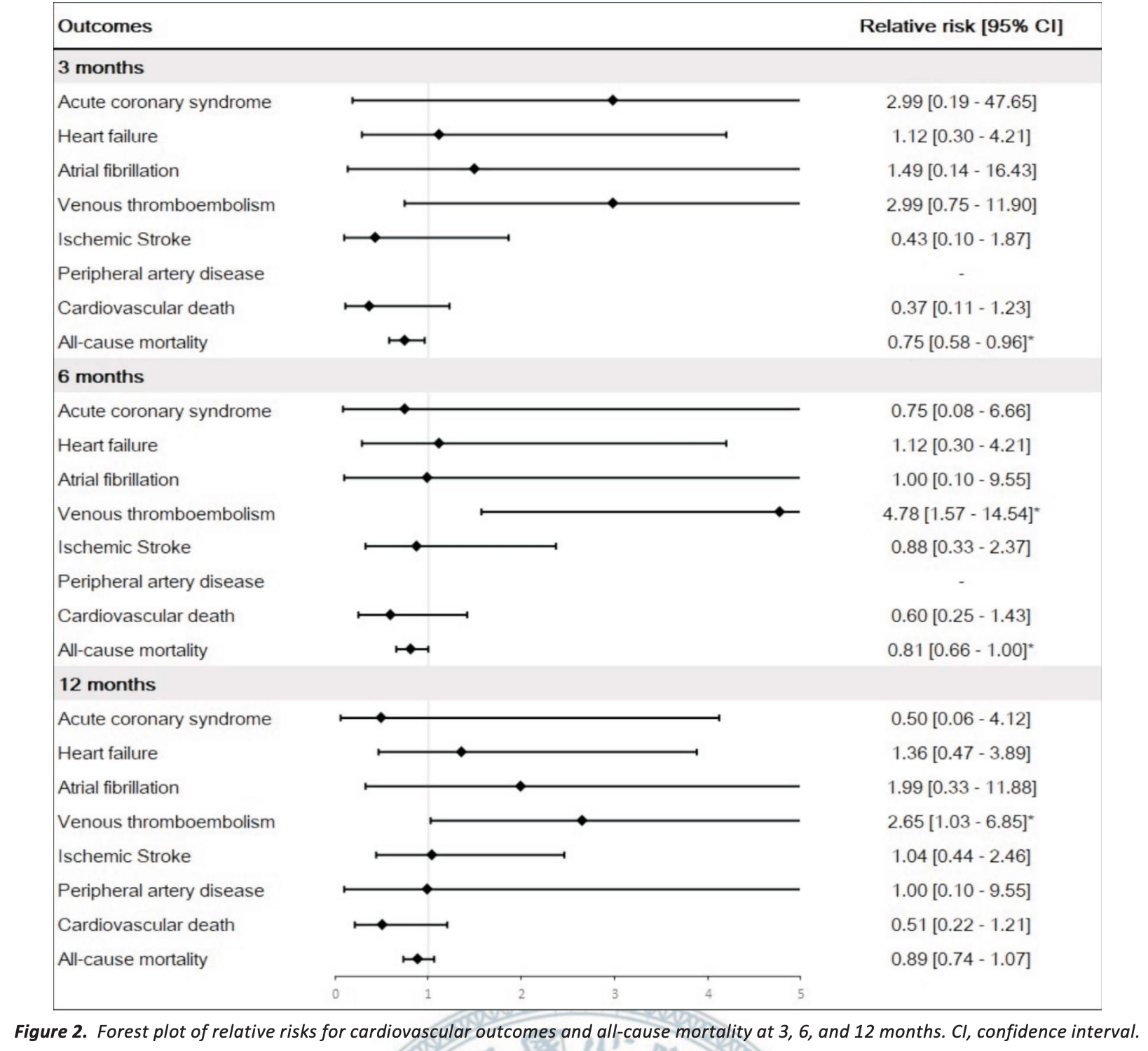
Retrospective 606 COVID-19 patients treated with paxlovid and 1,809 propensity score-matched controls in Taiwan, showing short-term mortality benefits at 3 months, but reduced benefit at 6 months, and no significant benefit at 12 months. The study also found significantly higher risk of venous thromboembolism (VTE) at 6 months and 12 months. Authors excluded patients with pre-existing cardiovascular conditions (potentially at higher risk of increased issues with paxlovid use).
Resistance. Variants may be resistant to paxlovid1-9. Use may promote the emergence of variants that weaken host immunity and potentially contribute to long COVID10. Confounding by contraindication. Hoertel et al. find that over 50% of patients that died had a contraindication for the use of Paxlovid11. Retrospective studies that do not exclude contraindicated patients may significantly overestimate efficacy. Black box warning. The FDA notes that severe, life-threatening, and/or fatal adverse reactions due to drug interactions have been reported in patients treated with paxlovid12. Kidney and liver injury. Studies show significantly increased risk of acute kidney injury13 and liver injury14,15. Viral rebound. Studies show significantly increased risk of replication-competent viral rebound16-18.
|
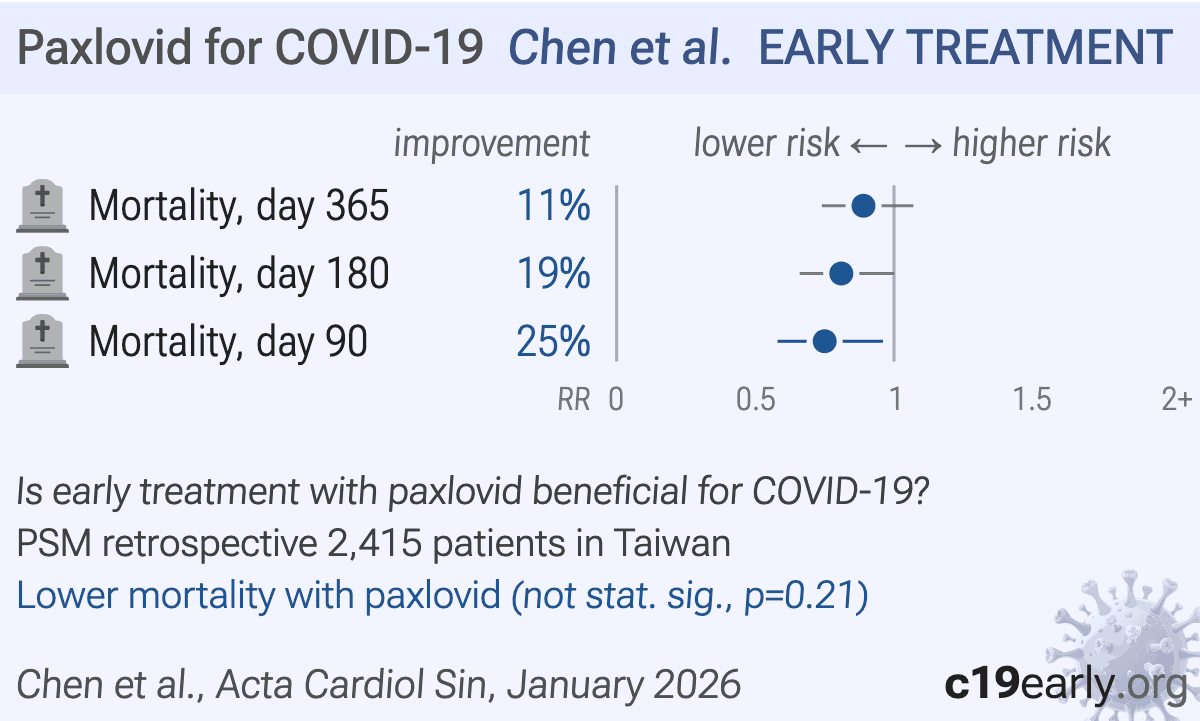
risk of death, 11.0% lower, RR 0.89, p = 0.21, treatment 117 of 606 (19.3%), control 393 of 1,809 (21.7%), NNT 41, propensity score matching, day 365.
|
|
risk of death, 19.0% lower, RR 0.81, p = 0.049, treatment 94 of 606 (15.5%), control 345 of 1,809 (19.1%), NNT 28, propensity score matching, day 180.
|
|
risk of death, 25.0% lower, RR 0.75, p = 0.02, treatment 66 of 606 (10.9%), control 264 of 1,809 (14.6%), NNT 27, propensity score matching, day 90.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
1.
Zhou et al., Nirmatrelvir-resistant SARS-CoV-2 variants with high fitness in an infectious cell culture system, Science Advances, doi:10.1126/sciadv.add7197.
2.
Moghadasi et al., Rapid resistance profiling of SARS-CoV-2 protease inhibitors, npj Antimicrobials and Resistance, doi:10.1038/s44259-023-00009-0.
3.
Jochmans et al., The Substitutions L50F, E166A, and L167F in SARS-CoV-2 3CLpro Are Selected by a Protease Inhibitor In Vitro and Confer Resistance To Nirmatrelvir, mBio, doi:10.1128/mbio.02815-22.
4.
Lopez et al., SARS-CoV-2 Resistance to Small Molecule Inhibitors, Current Clinical Microbiology Reports, doi:10.1007/s40588-024-00229-6.
5.
Zvornicanin et al., Molecular Mechanisms of Drug Resistance and Compensation in SARS-CoV-2 Main Protease: The Interplay Between E166 and L50, bioRxiv, doi:10.1101/2025.01.24.634813.
6.
Vukovikj et al., Impact of SARS-CoV-2 variant mutations on susceptibility to monoclonal antibodies and antiviral drugs: a non-systematic review, April 2022 to October 2024, Eurosurveillance, doi:10.2807/1560-7917.ES.2025.30.10.2400252.
7.
Deschenes et al., Functional and structural characterization of treatment-emergent nirmatrelvir resistance mutations at low frequencies in the main protease (Mpro) reveals a unique evolutionary route for SARS-CoV-2 to gain resistance, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf294.
8.
Zhou (B) et al., SARS-CoV-2 Mpro inhibitor ensitrelvir: asymmetrical cross-resistance with nirmatrelvir and emerging resistance hotspots, Emerging Microbes & Infections, doi:10.1080/22221751.2025.2552716.
9.
Chen et al., SARS-CoV-2 3CLpro mutations T21I and E166A confer differential resistance to simnotrelvir, bofutrelvir, and ensitrelvir, Journal of Virology, doi:10.1128/jvi.02223-25.
10.
Thomas et al., Nirmatrelvir-Resistant Mutations in SARS-CoV-2 Mpro Enhance Host Immune Evasion via Cleavage of NF-κB Essential Modulator, bioRxiv, doi:10.1101/2024.10.18.619137.
11.
Hoertel et al., Prevalence of Contraindications to Nirmatrelvir-Ritonavir Among Hospitalized Patients With COVID-19 at Risk for Progression to Severe Disease, JAMA Network Open, doi:10.1001/jamanetworkopen.2022.42140.
12.
FDA, Fact sheet for healthcare providers: emergency use authorization for paxlovid, www.fda.gov/media/155050/download.
13.
Kamo et al., Association of Antiviral Drugs for the Treatment of COVID-19 With Acute Renal Failure, In Vivo, doi:10.21873/invivo.13637.
14.
Wang et al., Development and validation of a nomogram to assess the occurrence of liver dysfunction in patients with COVID-19 pneumonia in the ICU, BMC Infectious Diseases, doi:10.1186/s12879-025-10684-1.
15.
Siby et al., Temporal Trends in Serious Adverse Events Associated with Oral Antivirals During the COVID-19 Pandemic: Insights from the FAERS Database (2020–2023), Open Forum Infectious Diseases, doi:10.1093/ofid/ofaf695.1825.
16.
Edelstein et al., SARS-CoV-2 virologic rebound with nirmatrelvir-ritonavir therapy, medRxiv, doi:10.1101/2023.06.23.23288598.
Chen et al., 30 Jan 2026, retrospective, Taiwan, peer-reviewed, 11 authors.
{kind=link}
Abstract: Acta Cardiol Sin 2026;42:87-98
Original Article
doi: 10.6515/ACS.202601_42(1).20250726A
General Cardiology
Cardiovascular Outcomes in COVID-19 Patients
Treated with Paxlovid: A Multicenter
Retrospective Study
Wei-Lun Chen,1 Victor Chien-Chia Wu,1,2 Chun-Li Wang,1,2 Yu-Ching Wang,3 Yu-Tung Huang,3 Chien-Hao Huang,2,4
Chih-Hsiang Chang,2,5 Shao-Wei Chen,2,3,6 Shang-Hung Chang,1,2,3,7 Cheng-Hsun Chiu8,9 and Pao-Hsien Chu1,2,10
Background: The Coronavirus disease 2019 (COVID-19) pandemic necessitated rapid advances in treatment, with
Paxlovid emerging as an effective oral antiviral. Despite its efficacy in reducing hospitalizations and mortality among
high-risk patients, the impact of Paxlovid on cardiovascular outcomes remains unclear, especially given the increased
cardiovascular risks associated with COVID-19.
Methods: We conducted a retrospective cohort study using data from the Chang Gung Memorial Hospital System
in Taiwan of patients admitted with COVID-19 from January 1, 2022 to December 31, 2022. Propensity score matching
was used to create comparable cohorts of patients treated with Paxlovid and those not treated with Paxlovid. The
primary outcomes were cardiovascular events and all-cause mortality within a 12-month follow-up period.
Results: The study analyzed 606 patients treated with Paxlovid and 1,809 matched patients who were not. Paxlovid
significantly reduced all-cause mortality at 3 months (relative risk [RR] 0.75, p = 0.0216) and 6 months (RR 0.81, p =
0.0492), but this effect was not sustained at 12 months (p = 0.2069). Notably, venous thromboembolism rates were
significantly higher in the Paxlovid group at 6 months (RR 4.78, p = 0.0057) and 12 months (RR 2.65, p = 0.0477).
Conclusions: While Paxlovid treatment resulted in significant short-term survival improvements among COVID-19
patients, it was also associated with a higher incidence of venous thromboembolic complications. These findings
highlight the need for careful patient selection and monitoring, particularly for those with preexisting cardiovascular
conditions.
Key Words:
Cardiovascular events · COVID-19 · Mortality · Outcome · Paxlovid
Abbreviations
CGMF
CGMH
CGRD
CI
COVID-19
DDI
ICD-9-CM
Received: June 3, 2025
Accepted: July 26, 2025
1
Division of Cardiology, Chang Gung Memorial Hospital, Linkou Medical
Center; 2College of Medicine, Chang Gung University; 3Center for Big
Data Analytics and Statistics; 4Division of Hepatology, Department of
Gastroenterology and Hepatology; 5Department of Nephrology, Kidney
Research Center; 6Department of Cardiothoracic and Vascular Surgery,
Chang Gung Memorial Hospital, Linkou Medical Center; 7Graduate
Institute of Nursing, Chang Gung University of Science and Technology;
8
Molecular Infectious Disease Research Center; 9Division of Pediatric
Infectious Diseases, Department of Pediatrics; 10Institute of Stem Cell
and Translational Cancer Research, Chang Gung Memorial Hospital,
Taoyuan, Taiwan.
Corresponding author: Dr. Pao-Hsien Chu, Division of Cardiology,
Chang Gung Memorial Hospital, Linkou Medical Center, No. 5, Fuxing
Street, Guishan District, Taoyuan 33305, Taiwan. Tel: 886-3-328-1200
ext. 8115; Fax: 886-3-328-1451; E-mail: taipei.chu@gmail.com
ICD-10-CM
IRB
RR
SARS-CoV-2
VTE
87
Chang Gung Medical Foundation
Chang Gung Memorial Hospital
Chang Gung Research Database
Confidence interval
Coronavirus disease 2019
Drug-drug interaction
International Classification of Diseases, Ninth
Revision, Clinical..
DOI record:
{
"DOI": "10.6515/ACS.202601_42(1).20250726A",
"URL": "",
"abstract": "",
"author": [
{
"literal": "Wei-Lun Chen"
},
{
"literal": "Victor Chien-Chia Wu"
},
{
"literal": "Chun-Li Wang"
},
{
"literal": "Yu-Ching Wang"
},
{
"literal": "Yu-Tung Huang"
},
{
"literal": "Chien-Hao Huang"
},
{
"literal": "Chih-Hsiang Chang"
},
{
"literal": "Shao-Wei Chen"
},
{
"literal": "Shang-Hung Chang"
},
{
"literal": "Cheng-Hsun Chiu"
},
{
"literal": "Pao-Hsien Chu"
}
],
"container-title": "Acta Cardiologica Sinica",
"issue": "1",
"issued": {
"date-parts": [
[
"2026",
"1",
"31"
]
]
},
"language": "en",
"page-first": "87",
"title": "Cardiovascular Outcomes in COVID-19 Patients Treated with Paxlovid: A Multicenter Retrospective Study",
"type": "article-journal",
"volume": "42"
}