Genetically predicted serum vitamin D and COVID-19: a Mendelian randomization study
et al., BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000255, Feb 2021
Vitamin D for COVID-19
8th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 138 studies, recognized in 18 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|


{kind=link}
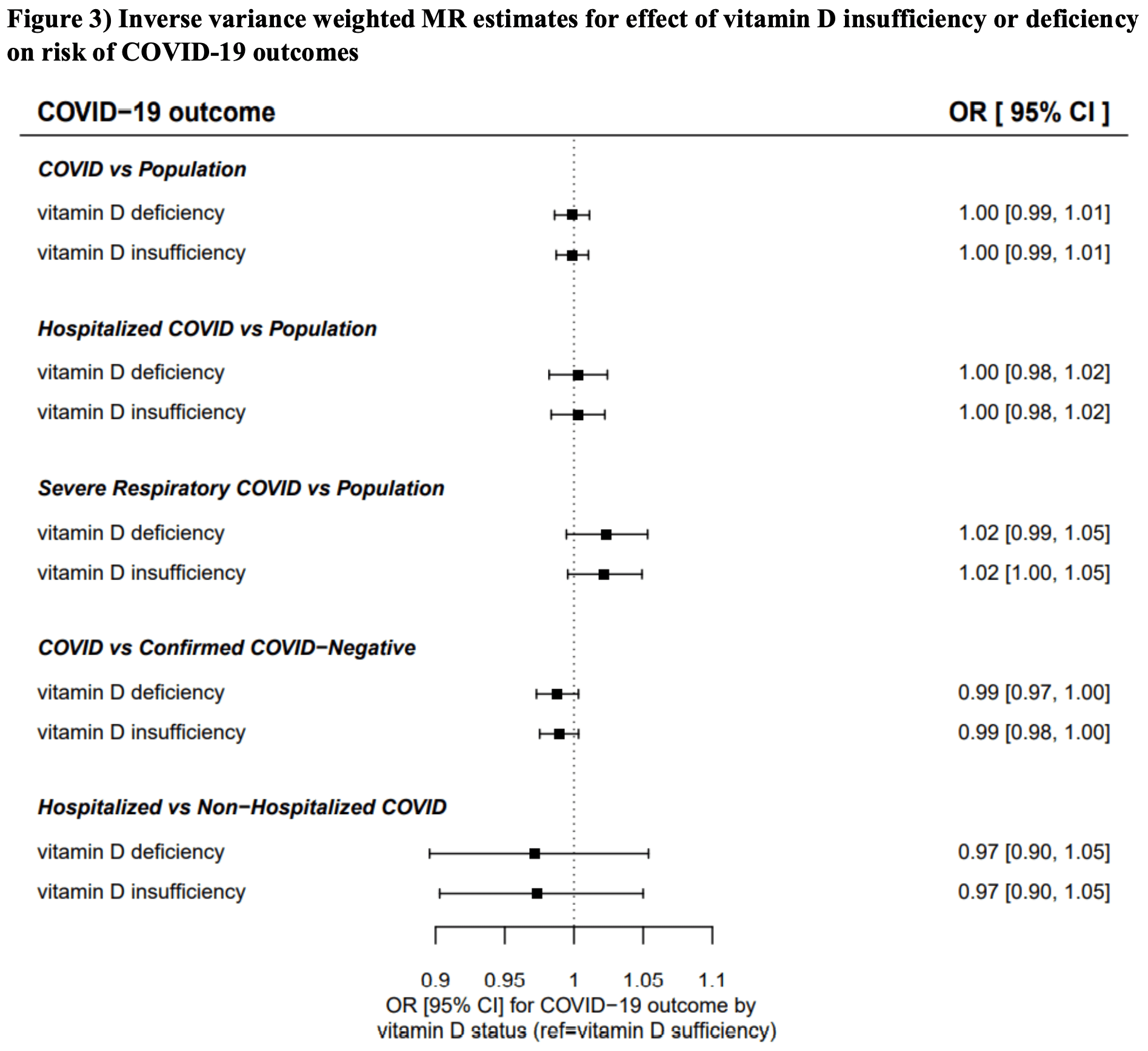
UK Biobank Mendelian randomization study not finding significant differences in COVID-19 risk. The number of people predicted to have vitamin D deficiency does not appear to be provided.
Mendelian randomization studies compare the estimated effect of SNPs
associated with variation in vitamin D levels on the health outcomes in large
numbers of patients. For more background on Mendelian randomization studies
and their limitations see1.
For reasons why Mendelian randomization may fail in this case,
see2.
Authors suggest that it may come down to the use of 25(OH)D concentration in
serum as a less than ideal proxy for vitamin D status of cells involved in the
immune response. For most other purposes, it may not matter much that unbound
(free) 25(OH)D is the better predictor of vitamin D deficiency and the
resulting unfavourable outcomes. But for the MR analysis, the genetic
instrument is strongly dominated by variation in the GC gene which modulates
the concentration of vitamin D-binding protein (VDBP) in blood and thereby
indirectly the concentrations of 25(OH)D and 1,25-dihydroxy vitamin D. Thus,
the common GC alleles rs4588A and rs7041T are both associated with much lower
than average vitamin D concentrations. In contrast, directly measured unbound
(free) vitamin D concentrations are minimally affected by these alleles, if at
all.
3 suggest that the primary reasons for Mendelien
randomization failure include that the total SNP-induced variation in 25(OH)D
has often been less than assay variance, and that genome-wide association
studies of SNP effects have been made on the full range of 25(OH)D levels,
while the data is non-linear with a significant percentage in the low and high
plateaus of the outcome relationships.
Standard of Care (SOC) for COVID-19 in the study country,
the United Kingdom, is very poor with very low average efficacy for approved treatments4.
The United Kingdom focused on expensive high-profit treatments, approving only one low-cost early treatment, which required a prescription and had limited adoption. The high-cost prescription treatment strategy reduces the probability of early treatment due to access and cost barriers, and eliminates complementary and synergistic benefits seen with many low-cost treatments.
|
risk of severe case, 2.0% lower, RR 0.98, p = 0.11, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >50nmol/L, baseline risk approximated with overall risk.
|
|
risk of hospitalization, no change, RR 1.00, p = 1.00, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >50nmol/L, baseline risk approximated with overall risk.
|
|
risk of case, no change, RR 1.00, p = 1.00, inverted to make RR<1 favor high D levels, odds ratio converted to relative risk, >50nmol/L, baseline risk approximated with overall risk.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Patchen et al., 1 Feb 2021, retrospective, United Kingdom, peer-reviewed, 5 authors.
{kind=link}
Genetically predicted serum vitamin D and COVID-19: a Mendelian randomisation study
BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000255
Objectives To investigate causality of the association of serum vitamin D with the risk and severity of COVID-19 infection. Design Two-sample Mendelian randomisation study. Setting Summary data from genome-wide analyses in the population-based UK Biobank and SUNLIGHT Consortium, applied to meta-analysed results of genome-wide analyses in the COVID-19 Host Genetics Initiative. Participants 17 965 COVID-19 cases including 11 085 laboratory or physician-confirmed cases, 7885 hospitalised cases and 4336 severe respiratory cases, and 1 370 547 controls, primarily of European ancestry. Exposures Genetically predicted variation in serum vitamin D status, instrumented by genome-wide significant single nucleotide polymorphisms (SNPs) associated with serum vitamin D or risk of vitamin D deficiency/insufficiency. Main outcome measures Susceptibility to and severity of COVID-19 infection, including severe respiratory infection and hospitalisation. Results Mendelian randomisation analysis, sufficiently powered to detect effects comparable to those seen in observational studies, provided little to no evidence for an effect of genetically predicted serum vitamin D on susceptibility to or severity of COVID-19 infection. Using SNPs in loci related to vitamin D metabolism as genetic instruments for serum vitamin D concentrations, the OR per SD higher serum vitamin D was 1.04 (95% CI 0.92 to 1.18) for any COVID-19 infection versus population controls, 1.05 (0.84 to 1.31) for hospitalised COVID-19 versus population controls, 0.96 (0.64 to 1.43) for severe respiratory COVID-19 versus population controls, 1.15 (0.99 to 1.35) for COVID-19 positive versus COVID-19 negative and 1.44 (0.75 to 2.78) for hospitalised COVID-19 versus non-hospitalised COVID-19. Results were similar in analyses using SNPs with genomewide significant associations with serum vitamin D (ie, including SNPs in loci with no known relationship to vitamin D metabolism) and in analyses using SNPs with genomewide significant associations with risk of vitamin D deficiency or insufficiency. Conclusions These findings suggest that genetically predicted differences in long-term vitamin D nutritional status do not causally affect susceptibility to and severity of COVID-19 infection, and that associations observed in previous studies may have been driven by confounding. These results do not exclude the possibility of low-magnitude causal effects or causal effects of acute responses to therapeutic doses of vitamin D.
BMJ Nutrition, Prevention & Health Provenance and peer review Not commissioned; externally peer reviewed by Xia Jiang, Karolinska Institute, Sweden and Dr Emmanuel Baah, University of North Carolina System. Data availability statement All data used for this analysis are publicly available. UK Biobank and COVID-19 Host Genetics Initiative data used for the main analysis are available in a public, open access repository. UK Biobank data used for stratified anayses of SNP-vitamin D associations are available on reasonable request from the UK Biobank. Code implementing the MR analysis is available on request from the corresponding author. Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0)..
References
Afzal, Brøndum-Jacobsen, Bojesen, Genetically low vitamin D concentrations and increased mortality: Mendelian randomisation analysis in three large cohorts, BMJ, doi:10.1136/bmj.g6330
Ahn, Yu, Stolzenberg-Solomon, Genome-wide association study of circulating vitamin D levels, Hum Mol Genet, doi:10.1093/hmg/ddq155
Amin, Drenos, No evidence that vitamin D is able to prevent or affect the severity of COVID-19 in individuals with European ancestry: a Mendelian randomisation study of open data, BMJ Nutr Prev Health, doi:10.1136/bmjnph-2020-000151
Annweiler, Hanotte, De L'eprevier, Vitamin D and survival in COVID-19 patients: a quasi-experimental study, J Steroid Biochem Mol Biol, doi:10.1016/j.jsbmb.2020.105771
Arabi, Khoueiry-Zgheib, Awada, CYP2R1 polymorphisms are important modulators of circulating 25-hydroxyvitamin D levels in elderly females with vitamin insufficiency, but not of the response to vitamin D supplementation, Osteoporos Int, doi:10.1007/s00198-016-3713-5
Bae, Lee, Vitamin D level and risk of systemic lupus erythematosus and rheumatoid arthritis: a Mendelian randomization, Clin Rheumatol, doi:10.1007/s10067-018-4152-9
Baktash, Hosack, Patel, Vitamin D status and outcomes for hospitalised older patients with COVID-19, Postgrad Med J, doi:10.1136/postgradmedj-2020-138712
Bikle, Schwartz, Vitamin D binding protein, total and free vitamin D levels in different physiological and pathophysiological conditions, Front Endocrinol, doi:10.3389/fendo.2019.00317
Bikle, The free hormone hypothesis: when, why, and how to measure the free hormone levels to assess vitamin D, thyroid, sex hormone, and cortisol status, JBMR Plus, doi:10.1002/jbm4.10418
Bowden, Smith, Burgess, Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression, Int J Epidemiol, doi:10.1093/ije/dyv080
Bowden, Smith, Haycock, Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator, Genet Epidemiol, doi:10.1002/gepi.21965
Brenner, Holleczek, Schöttker, Vitamin D insufficiency and deficiency and mortality from respiratory diseases in a cohort of older adults: potential for limiting the death toll during and beyond the COVID-19 pandemic?, Nutrients, doi:10.3390/nu12082488
Brion, Shakhbazov, Visscher, Calculating statistical power in Mendelian randomization studies, Int J Epidemiol, doi:10.1093/ije/dyt179
Brøndum-Jacobsen, Afzal, No evidence that genetically reduced 25-hydroxyvitamin D is associated with increased risk of ischaemic heart disease or myocardial infarction: a Mendelian randomization study, Int J Epidemiol, doi:10.1093/ije/dyv078
Burgess, Butterworth, Thompson, Mendelian randomization analysis with multiple genetic variants using summarized data, Genet Epidemiol, doi:10.1002/gepi.21758
Burgess, Davies, Thompson, Bias due to participant overlap in two-sample Mendelian randomization, Genet Epidemiol, doi:10.1002/gepi.21998
Burgess, Thompson, Chd Genetics, Collaboration, Avoiding bias from weak instruments in Mendelian randomization studies, Int J Epidemiol, doi:10.1093/ije/dyr036
Castillo, Costa, Barrios, Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study, J Steroid Biochem Mol Biol, doi:10.1016/j.jsbmb.2020.105751
Cui, Xu, Li, Vitamin D receptor activation regulates microglia polarization and oxidative stress in spontaneously hypertensive rats and angiotensin II-exposed microglial cells: role of renin-angiotensin system, Redox Biol, doi:10.1016/j.redox.2019.101295
D'avolio, Avataneo, Manca, 25-Hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2, Nutrients, doi:10.3390/nu12051359
Gogarten, Sofer, Chen, Genetic association testing using the genesis R/Bioconductor package, Bioinformatics, doi:10.1093/bioinformatics/btz567
Guillot, Semerano, Saidenberg-Kermanac'h N, Vitamin D and inflammation, Joint Bone Spine, doi:10.1016/j.jbspin.2010.09.018
Hartwig, Smith, Bowden, Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption, Int J Epidemiol, doi:10.1093/ije/dyx102
Hastie, Mackay, Ho, Vitamin D concentrations and COVID-19 infection in UK Biobank, Diabetes Metab Syndr, doi:10.1016/j.dsx.2020.04.050
Hemani, Bowden, Smith, Evaluating the potential role of pleiotropy in Mendelian randomization studies, Hum Mol Genet, doi:10.1093/hmg/ddy163
Hemani, Zheng, Elsworth, The MR-Base platform supports systematic causal inference across the human phenome, Elife, doi:10.7554/eLife.34408
Hoffmann, Choquet, Yin, A large multiethnic genomewide association study of adult body mass index identifies novel loci, Genetics, doi:10.1534/genetics.118.301479
Hong, Hatchell, Bradfield, Transethnic evaluation identifies low-frequency loci associated with 25-hydroxyvitamin D concentrations, J Clin Endocrinol Metab, doi:10.1210/jc.2017-01802
Hysinger, Roizen, Mentch, Mendelian randomization analysis demonstrates that low vitamin D is unlikely causative for pediatric asthma, J Allergy Clin Immunol, doi:10.1016/j.jaci.2016.06.056
Ilie, Stefanescu, Smith, The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality, Aging Clin Exp Res, doi:10.1007/s40520-020-01570-8
Jiang, Reilly, Aschard, Genome-wide association study in 79,366 European-ancestry individuals informs the genetic architecture of 25-hydroxyvitamin D levels, Nat Commun, doi:10.1038/s41467-017-02662-2
Jones, Lucock, Chaplin, Distribution of variants in multiple vitamin D-related loci (DHCR7/NADSYN1, GC, CYP2R1, CYP11A1, CYP24A1, VDR, RXRα and RXRγ) vary between European, East-Asian and sub-Saharan African-ancestry populations, Genes Nutr, doi:10.1186/s12263-020-00663-3
Kai, Kai, Interactions of coronaviruses with ACE2, angiotensin II, and Ras inhibitors-lessons from available evidence and insights into COVID-19, Hypertens Res
Kaufman, Niles, Kroll, SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels, PLoS One, doi:10.1371/journal.pone.0239252
Kohlmeier, Avoidance of vitamin D deficiency to slow the COVID-19 pandemic, BMJ Nutr Prev Health, doi:10.1136/bmjnph-2020-000096
Liefaard, Ligthart, Vitezova, Vitamin D and Creactive protein: a Mendelian randomization study, PLoS One, doi:10.1371/journal.pone.0131740
Liu, Jiang, Wedow, Association studies of up to 1.2 million individuals yield new insights into the genetic etiology of tobacco and alcohol use, Nat Genet, doi:10.1038/s41588-018-0307-5
Locke, Kahali, Berndt, Genetic studies of body mass index yield new insights for obesity biology, Nature, doi:10.1038/nature14177
Macaya, Paeres, Valls, Interaction between age and vitamin D deficiency in severe COVID-19 infection, Nutr Hosp, doi:10.20960/nh.03193
Machiela, Chanock, LDlink: a web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants, Bioinformatics, doi:10.1093/bioinformatics/btv402
Maghbooli, Sahraian, Ebrahimi, Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection, PLoS One, doi:10.1371/journal.pone.0239799
Manousaki, Mitchell, Dudding, Genome-wide association study for vitamin D levels reveals 69 independent loci, Am J Hum Genet, doi:10.1016/j.ajhg.2020.01.017
Manousaki, Mokry, Ross, Mendelian randomization studies do not support a role for vitamin D in coronary artery disease, Circ Cardiovasc Genet, doi:10.1161/CIRCGENETICS.116.001396
Manousaki, Paternoster, Standl, Vitamin D levels and susceptibility to asthma, elevated immunoglobulin E levels, and atopic dermatitis: a Mendelian randomization study, PLoS Med, doi:10.1371/journal.pmed.1002294
Mao, Zhan, Huang, Vitamin D and asthma: a Mendelian randomization study, Ann Allergy Asthma Immunol, doi:10.1016/j.anai.2017.05.018
Meltzer, Best, Zhang, Association of vitamin D status and other clinical characteristics with COVID-19 test results, JAMA Netw Open, doi:10.1001/jamanetworkopen.2020.19722
Mok, Ng, Ahidjo, Calcitriol, the active form of vitamin D, is a promising candidate for COVID-19 prophylaxis, doi:10.1101/2020.06.21.162396
Mokry, Ross, Morris, Genetically decreased vitamin D and risk of Alzheimer disease, Neurology, doi:10.1212/WNL.0000000000003430
Ong, Cuellar-Partida, Lu, Association of vitamin D levels and risk of ovarian cancer: a Mendelian randomization study, Int J Epidemiol, doi:10.1093/ije/dyw207
Pritchard, Stephens, Donnelly, Auton, Brooks, Inference of population structure using multilocus genotype data, Genetics, doi:10.1038/nature15393
Schwartz, Gallagher, Jorde, Determination of free 25(OH)D concentrations and their relationships to total 25(OH) D in multiple clinical populations, J Clin Endocrinol Metab, doi:10.1210/jc.2018-00295
Shungin, Winkler, Croteau-Chonka, New genetic loci link adipose and insulin biology to body fat distribution, Nature, doi:10.1038/nature14132
Skaaby, Husemoen, Martinussen, Vitamin D status, filaggrin genotype, and cardiovascular risk factors: a Mendelian randomization approach, PLoS One, doi:10.1371/journal.pone.0057647
Taylor, Burgess, Ware, Investigating causality in the association between 25(OH)D and schizophrenia, Sci Rep, doi:10.1038/srep26496
Trummer, Pilz, Hoffmann, Vitamin D and mortality: a Mendelian randomization study, Clin Chem, doi:10.1373/clinchem.2012.193185
Tsuprykov, Chen, Hocher, Why should we measure free 25(OH) vitamin D?, J Steroid Biochem Mol Biol, doi:10.1016/j.jsbmb.2017.11.014
Viatte, Yarwood, Mcallister, The role of genetic polymorphisms regulating vitamin D levels in rheumatoid arthritis outcome: a Mendelian randomisation approach, Ann Rheum Dis, doi:10.1136/annrheumdis-2013-204972
Vimaleswaran, Berry, Lu, Causal relationship between obesity and vitamin D status: bi-directional Mendelian randomization analysis of multiple cohorts, PLoS Med, doi:10.1371/journal.pmed.1001383
Vimaleswaran, Cavadino, Berry, Association of vitamin D status with arterial blood pressure and hypertension risk: a Mendelian randomisation study, Lancet Diabetes Endocrinol, doi:10.1016/S2213-8587(14)70113-5
Wang, Zhang, Richards, Common genetic determinants of vitamin D insufficiency: a genome-wide association study, Lancet, doi:10.1016/S0140-6736(10)60588-0
Whittemore, COVID-19 fatalities, latitude, sunlight, and vitamin D, Am J Infect Control, doi:10.1016/j.ajic.2020.06.193
Williams, Gingery, Joint guidance on vitamin D in the era of COVID-19
Ye, Sharp, Burgess, Association between circulating 25-hydroxyvitamin D and incident type 2 diabetes: a Mendelian randomisation study, Lancet Diabetes Endocrinol, doi:10.1016/S2213-8587(14)70184-6
Ye, Tang, Liao, Does serum vitamin D level affect COVID-19 infection and its severity?-a case-control study, J Am Coll Nutr, doi:10.1080/07315724.2020.1826005
DOI record:
{
"DOI": "10.1136/bmjnph-2021-000255",
"ISSN": [
"2516-5542"
],
"URL": "http://dx.doi.org/10.1136/bmjnph-2021-000255",
"abstract": "<jats:sec><jats:title>Objectives</jats:title><jats:p>To investigate causality of the association of serum vitamin D with the risk and severity of COVID-19 infection.</jats:p></jats:sec><jats:sec><jats:title>Design</jats:title><jats:p>Two-sample Mendelian randomisation study.</jats:p></jats:sec><jats:sec><jats:title>Setting</jats:title><jats:p>Summary data from genome-wide analyses in the population-based UK Biobank and SUNLIGHT Consortium, applied to meta-analysed results of genome-wide analyses in the COVID-19 Host Genetics Initiative.</jats:p></jats:sec><jats:sec><jats:title>Participants</jats:title><jats:p>17 965 COVID-19 cases including 11 085 laboratory or physician-confirmed cases, 7885 hospitalised cases and 4336 severe respiratory cases, and 1 370 547 controls, primarily of European ancestry.</jats:p></jats:sec><jats:sec><jats:title>Exposures</jats:title><jats:p>Genetically predicted variation in serum vitamin D status, instrumented by genome-wide significant single nucleotide polymorphisms (SNPs) associated with serum vitamin D or risk of vitamin D deficiency/insufficiency.</jats:p></jats:sec><jats:sec><jats:title>Main outcome measures</jats:title><jats:p>Susceptibility to and severity of COVID-19 infection, including severe respiratory infection and hospitalisation.</jats:p></jats:sec><jats:sec><jats:title>Results</jats:title><jats:p>Mendelian randomisation analysis, sufficiently powered to detect effects comparable to those seen in observational studies, provided little to no evidence for an effect of genetically predicted serum vitamin D on susceptibility to or severity of COVID-19 infection. Using SNPs in loci related to vitamin D metabolism as genetic instruments for serum vitamin D concentrations, the OR per SD higher serum vitamin D was 1.04 (95% CI 0.92 to 1.18) for any COVID-19 infection versus population controls, 1.05 (0.84 to 1.31) for hospitalised COVID-19 versus population controls, 0.96 (0.64 to 1.43) for severe respiratory COVID-19 versus population controls, 1.15 (0.99 to 1.35) for COVID-19 positive versus COVID-19 negative and 1.44 (0.75 to 2.78) for hospitalised COVID-19 versus non-hospitalised COVID-19. Results were similar in analyses using SNPs with genome-wide significant associations with serum vitamin D (ie, including SNPs in loci with no known relationship to vitamin D metabolism) and in analyses using SNPs with genome-wide significant associations with risk of vitamin D deficiency or insufficiency.</jats:p></jats:sec><jats:sec><jats:title>Conclusions</jats:title><jats:p>These findings suggest that genetically predicted differences in long-term vitamin D nutritional status do not causally affect susceptibility to and severity of COVID-19 infection, and that associations observed in previous studies may have been driven by confounding. These results do not exclude the possibility of low-magnitude causal effects or causal effects of acute responses to therapeutic doses of vitamin D.</jats:p></jats:sec>",
"alternative-id": [
"10.1136/bmjnph-2021-000255"
],
"author": [
{
"ORCID": "http://orcid.org/0000-0003-3361-6744",
"affiliation": [],
"authenticated-orcid": false,
"family": "Patchen",
"given": "Bonnie K",
"sequence": "first"
},
{
"affiliation": [],
"family": "Clark",
"given": "Andrew G",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Gaddis",
"given": "Nathan",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Hancock",
"given": "Dana B",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-4827-5073",
"affiliation": [],
"authenticated-orcid": false,
"family": "Cassano",
"given": "Patricia A",
"sequence": "additional"
}
],
"container-title": "BMJ Nutrition, Prevention & Health",
"container-title-short": "BMJNPH",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"bmj.com"
]
},
"created": {
"date-parts": [
[
2021,
5,
4
]
],
"date-time": "2021-05-04T16:35:15Z",
"timestamp": 1620146115000
},
"deposited": {
"date-parts": [
[
2021,
7,
27
]
],
"date-time": "2021-07-27T21:06:48Z",
"timestamp": 1627420008000
},
"funder": [
{
"DOI": "10.13039/100000050",
"award": [
"R01 HL149352"
],
"doi-asserted-by": "publisher",
"name": "National Heart, Lung, and Blood Institute"
},
{
"DOI": "10.13039/100000051",
"award": [
"R01 HG006849"
],
"doi-asserted-by": "publisher",
"name": "National Human Genome Research Institute"
},
{
"DOI": "10.13039/100000062",
"award": [
"T32 DK007158"
],
"doi-asserted-by": "publisher",
"name": "National Institute of Diabetes and Digestive and Kidney Diseases"
}
],
"indexed": {
"date-parts": [
[
2024,
4,
6
]
],
"date-time": "2024-04-06T07:08:01Z",
"timestamp": 1712387281233
},
"is-referenced-by-count": 22,
"issue": "1",
"issued": {
"date-parts": [
[
2021,
5,
4
]
]
},
"journal-issue": {
"issue": "1",
"published-online": {
"date-parts": [
[
2021,
6,
30
]
]
},
"published-print": {
"date-parts": [
[
2021,
6
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://creativecommons.org/licenses/by-nc/4.0/",
"content-version": "unspecified",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
5,
4
]
],
"date-time": "2021-05-04T00:00:00Z",
"timestamp": 1620086400000
}
}
],
"link": [
{
"URL": "https://syndication.highwire.org/content/doi/10.1136/bmjnph-2021-000255",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "239",
"original-title": [],
"page": "213-225",
"prefix": "10.1136",
"published": {
"date-parts": [
[
2021,
5,
4
]
]
},
"published-online": {
"date-parts": [
[
2021,
5,
4
]
]
},
"published-print": {
"date-parts": [
[
2021,
6
]
]
},
"publisher": "BMJ",
"reference": [
{
"key": "2021072714055093000_4.1.213.1",
"unstructured": "Home . Johns hopkins coronavirus resource center. Available: https://coronavirus.jhu.edu/"
},
{
"DOI": "10.1016/j.jbspin.2010.09.018",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.2"
},
{
"DOI": "10.3390/nu12082488",
"doi-asserted-by": "crossref",
"key": "2021072714055093000_4.1.213.3",
"unstructured": "Brenner H , Holleczek B , Schöttker B . Vitamin D insufficiency and deficiency and mortality from respiratory diseases in a cohort of older adults: potential for limiting the death toll during and beyond the COVID-19 pandemic? Nutrients 2020;12:2488. doi:10.3390/nu12082488"
},
{
"DOI": "10.1016/j.redox.2019.101295",
"article-title": "Vitamin D receptor activation regulates microglia polarization and oxidative stress in spontaneously hypertensive rats and angiotensin II-exposed microglial cells: role of renin-angiotensin system",
"author": "Cui",
"doi-asserted-by": "crossref",
"journal-title": "Redox Biol",
"key": "2021072714055093000_4.1.213.4",
"volume": "26",
"year": "2019"
},
{
"DOI": "10.1038/s41440-020-0455-8",
"doi-asserted-by": "crossref",
"key": "2021072714055093000_4.1.213.5",
"unstructured": "Kai H , Kai M . Interactions of coronaviruses with ACE2, angiotensin II, and Ras inhibitors—lessons from available evidence and insights into COVID-19. Hypertens Res 2020:1–7."
},
{
"DOI": "10.1101/2020.06.21.162396",
"doi-asserted-by": "crossref",
"key": "2021072714055093000_4.1.213.6",
"unstructured": "Mok CK , Ng YL , Ahidjo BA . Calcitriol, the active form of vitamin D, is a promising candidate for COVID-19 prophylaxis. bioRxiv.doi:10.1101/2020.06.21.162396"
},
{
"DOI": "10.1016/j.jsbmb.2020.105751",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.7"
},
{
"DOI": "10.1016/j.jsbmb.2020.105771",
"article-title": "Vitamin D and survival in COVID-19 patients: a quasi-experimental study",
"author": "Annweiler",
"doi-asserted-by": "crossref",
"journal-title": "J Steroid Biochem Mol Biol",
"key": "2021072714055093000_4.1.213.8",
"volume": "204",
"year": "2020"
},
{
"DOI": "10.1007/s40520-020-01570-8",
"article-title": "The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality",
"author": "Ilie",
"doi-asserted-by": "crossref",
"first-page": "1195",
"journal-title": "Aging Clin Exp Res",
"key": "2021072714055093000_4.1.213.9",
"volume": "32",
"year": "2020"
},
{
"DOI": "10.1016/j.ajic.2020.06.193",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.10"
},
{
"DOI": "10.1136/bmjnph-2020-000096",
"article-title": "Avoidance of vitamin D deficiency to slow the COVID-19 pandemic",
"author": "Kohlmeier",
"doi-asserted-by": "crossref",
"journal-title": "BMJ Nutr Prev Health",
"key": "2021072714055093000_4.1.213.11",
"volume": "3",
"year": "2020"
},
{
"DOI": "10.1371/journal.pone.0239252",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.12"
},
{
"DOI": "10.1001/jamanetworkopen.2020.19722",
"article-title": "Association of vitamin D status and other clinical characteristics with COVID-19 test results",
"author": "Meltzer",
"doi-asserted-by": "crossref",
"journal-title": "JAMA Netw Open",
"key": "2021072714055093000_4.1.213.13",
"volume": "3",
"year": "2020"
},
{
"article-title": "25-Hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2",
"author": "D'Avolio",
"journal-title": "Nutrients",
"key": "2021072714055093000_4.1.213.14",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1080/07315724.2020.1826005",
"article-title": "Does serum vitamin D level affect COVID-19 infection and its severity?-a case-control study",
"author": "Ye",
"doi-asserted-by": "crossref",
"first-page": "1",
"journal-title": "J Am Coll Nutr",
"key": "2021072714055093000_4.1.213.15",
"year": "2020"
},
{
"DOI": "10.1371/journal.pone.0239799",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.16"
},
{
"article-title": "Interaction between age and vitamin D deficiency in severe COVID-19 infection",
"author": "Macaya",
"first-page": "1039",
"journal-title": "Nutr Hosp",
"key": "2021072714055093000_4.1.213.17",
"volume": "37",
"year": "2020"
},
{
"DOI": "10.1136/postgradmedj-2020-138712",
"article-title": "Vitamin D status and outcomes for hospitalised older patients with COVID-19",
"author": "Baktash",
"doi-asserted-by": "crossref",
"journal-title": "Postgrad Med J",
"key": "2021072714055093000_4.1.213.18",
"year": "2020"
},
{
"key": "2021072714055093000_4.1.213.19",
"unstructured": "COVID-19 Treatment Guidelines Panel . Coronavirus disease 2019 (COVID-19) treatment guidelines. COVID-19 treatment guidelines. Available: https://www.covid19treatmentguidelines.nih.gov/adjunctive-therapy/vitamin-d/"
},
{
"key": "2021072714055093000_4.1.213.20",
"unstructured": "Williams C , Gingery JG . Joint guidance on vitamin D in the era of COVID-19. Endocrine Society, 2020. Available: https://www.endocrine.org/news-and-advocacy/news-room/2020/joint-guidance-on-vitamin-d"
},
{
"DOI": "10.1016/j.dsx.2020.04.050",
"article-title": "Vitamin D concentrations and COVID-19 infection in UK Biobank",
"author": "Hastie",
"doi-asserted-by": "crossref",
"first-page": "561",
"journal-title": "Diabetes Metab Syndr",
"key": "2021072714055093000_4.1.213.21",
"volume": "14",
"year": "2020"
},
{
"DOI": "10.1016/j.ajhg.2020.01.017",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.22"
},
{
"DOI": "10.1038/s41467-017-02662-2",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.23"
},
{
"DOI": "10.1016/S0140-6736(10)60588-0",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.24"
},
{
"DOI": "10.1093/hmg/ddq155",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.25"
},
{
"DOI": "10.1210/jc.2017-01802",
"article-title": "Transethnic evaluation identifies low-frequency loci associated with 25-hydroxyvitamin D concentrations",
"author": "Hong",
"doi-asserted-by": "crossref",
"first-page": "1380",
"journal-title": "J Clin Endocrinol Metab",
"key": "2021072714055093000_4.1.213.26",
"volume": "103",
"year": "2018"
},
{
"DOI": "10.1007/s00198-016-3713-5",
"article-title": "CYP2R1 polymorphisms are important modulators of circulating 25-hydroxyvitamin D levels in elderly females with vitamin insufficiency, but not of the response to vitamin D supplementation",
"author": "Arabi",
"doi-asserted-by": "crossref",
"first-page": "279",
"journal-title": "Osteoporos Int",
"key": "2021072714055093000_4.1.213.27",
"volume": "28",
"year": "2017"
},
{
"DOI": "10.1186/s12263-020-00663-3",
"article-title": "Distribution of variants in multiple vitamin D-related loci (DHCR7/NADSYN1, GC, CYP2R1, CYP11A1, CYP24A1, VDR, RXRα and RXRγ) vary between European, East-Asian and sub-Saharan African-ancestry populations",
"author": "Jones",
"doi-asserted-by": "crossref",
"first-page": "5",
"journal-title": "Genes Nutr",
"key": "2021072714055093000_4.1.213.28",
"volume": "15",
"year": "2020"
},
{
"DOI": "10.1371/journal.pone.0131740",
"article-title": "Vitamin D and C-reactive protein: a Mendelian randomization study",
"author": "Liefaard",
"doi-asserted-by": "crossref",
"journal-title": "PLoS One",
"key": "2021072714055093000_4.1.213.29",
"volume": "10",
"year": "2015"
},
{
"DOI": "10.1136/bmj.g6330",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.30"
},
{
"DOI": "10.1093/ije/dyv078",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.31"
},
{
"DOI": "10.1007/s10067-018-4152-9",
"article-title": "Vitamin D level and risk of systemic lupus erythematosus and rheumatoid arthritis: a Mendelian randomization",
"author": "Bae",
"doi-asserted-by": "crossref",
"first-page": "2415",
"journal-title": "Clin Rheumatol",
"key": "2021072714055093000_4.1.213.32",
"volume": "37",
"year": "2018"
},
{
"DOI": "10.1016/j.jaci.2016.06.056",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.33"
},
{
"DOI": "10.1161/CIRCGENETICS.116.001396",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.34"
},
{
"DOI": "10.1371/journal.pmed.1002294",
"article-title": "Vitamin D levels and susceptibility to asthma, elevated immunoglobulin E levels, and atopic dermatitis: a Mendelian randomization study",
"author": "Manousaki",
"doi-asserted-by": "crossref",
"journal-title": "PLoS Med",
"key": "2021072714055093000_4.1.213.35",
"volume": "14",
"year": "2017"
},
{
"DOI": "10.1016/j.anai.2017.05.018",
"article-title": "Vitamin D and asthma: a Mendelian randomization study",
"author": "Mao",
"doi-asserted-by": "crossref",
"first-page": "95",
"journal-title": "Ann Allergy Asthma Immunol",
"key": "2021072714055093000_4.1.213.36",
"volume": "119",
"year": "2017"
},
{
"DOI": "10.1212/WNL.0000000000003430",
"article-title": "Genetically decreased vitamin D and risk of Alzheimer disease",
"author": "Mokry",
"doi-asserted-by": "crossref",
"first-page": "2567",
"journal-title": "Neurology",
"key": "2021072714055093000_4.1.213.37",
"volume": "87",
"year": "2016"
},
{
"DOI": "10.1093/ije/dyw207",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.38"
},
{
"DOI": "10.1371/journal.pone.0057647",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.39"
},
{
"DOI": "10.1038/srep26496",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.40"
},
{
"DOI": "10.1373/clinchem.2012.193185",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.41"
},
{
"DOI": "10.1136/annrheumdis-2013-204972",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.42"
},
{
"DOI": "10.1371/journal.pmed.1001383",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.43"
},
{
"DOI": "10.1016/S2213-8587(14)70113-5",
"article-title": "Association of vitamin D status with arterial blood pressure and hypertension risk: a Mendelian randomisation study",
"author": "Vimaleswaran",
"doi-asserted-by": "crossref",
"first-page": "719",
"journal-title": "Lancet Diabetes Endocrinol",
"key": "2021072714055093000_4.1.213.44",
"volume": "2",
"year": "2014"
},
{
"DOI": "10.1016/S2213-8587(14)70184-6",
"article-title": "Association between circulating 25-hydroxyvitamin D and incident type 2 diabetes: a Mendelian randomisation study",
"author": "Ye",
"doi-asserted-by": "crossref",
"first-page": "35",
"journal-title": "Lancet Diabetes Endocrinol",
"key": "2021072714055093000_4.1.213.45",
"volume": "3",
"year": "2015"
},
{
"DOI": "10.1136/bmjnph-2020-000151",
"doi-asserted-by": "crossref",
"key": "2021072714055093000_4.1.213.46",
"unstructured": "Amin HA , Drenos F . No evidence that vitamin D is able to prevent or affect the severity of COVID-19 in individuals with European ancestry: a Mendelian randomisation study of open data. BMJ Nutr Prev Health 2021;8:bmjnph-2020-000151. doi:10.1136/bmjnph-2020-000151"
},
{
"DOI": "10.1002/gepi.21758",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.47"
},
{
"article-title": "The COVID-19 host genetics initiative, a global initiative to elucidate the role of host genetic factors in susceptibility and severity of the SARS-CoV-2 virus pandemic",
"first-page": "1",
"journal-title": "Eur J Hum Genet",
"key": "2021072714055093000_4.1.213.48",
"volume": "28",
"year": "2020"
},
{
"DOI": "10.1002/gepi.21998",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.49"
},
{
"DOI": "10.1093/ije/dyr036",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.50"
},
{
"DOI": "10.1093/bioinformatics/btv402",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.51"
},
{
"DOI": "10.1534/genetics.118.301479",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.52"
},
{
"DOI": "10.1038/nature14132",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.53"
},
{
"DOI": "10.1038/s41588-018-0307-5",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.54"
},
{
"DOI": "10.1038/nature14177",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.55"
},
{
"DOI": "10.7554/eLife.34408",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.56"
},
{
"DOI": "10.1093/bioinformatics/btz567",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.57"
},
{
"DOI": "10.1111/j.1471-8286.2005.01155.x",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.58"
},
{
"DOI": "10.1038/nature15393",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.59"
},
{
"key": "2021072714055093000_4.1.213.60",
"unstructured": "Nature . An integrated map of structural variation in 2,504 human genomes. Available: https://www.nature.com/articles/nature15394"
},
{
"DOI": "10.1093/hmg/ddy163",
"article-title": "Evaluating the potential role of pleiotropy in Mendelian randomization studies",
"author": "Hemani",
"doi-asserted-by": "crossref",
"first-page": "R195",
"journal-title": "Hum Mol Genet",
"key": "2021072714055093000_4.1.213.61",
"volume": "27",
"year": "2018"
},
{
"DOI": "10.1093/ije/dyv080",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.62"
},
{
"DOI": "10.1002/gepi.21965",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.63"
},
{
"DOI": "10.1093/ije/dyx102",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.64"
},
{
"DOI": "10.1093/ije/dyt179",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.65"
},
{
"DOI": "10.3389/fendo.2019.00317",
"article-title": "Vitamin D binding protein, total and free vitamin D levels in different physiological and pathophysiological conditions",
"author": "Bikle",
"doi-asserted-by": "crossref",
"journal-title": "Front Endocrinol",
"key": "2021072714055093000_4.1.213.66",
"volume": "10",
"year": "2019"
},
{
"DOI": "10.1002/jbm4.10418",
"article-title": "The free hormone hypothesis: when, why, and how to measure the free hormone levels to assess vitamin D, thyroid, sex hormone, and cortisol status",
"author": "Bikle",
"doi-asserted-by": "crossref",
"first-page": "e10418",
"journal-title": "JBMR Plus",
"key": "2021072714055093000_4.1.213.67",
"volume": "5",
"year": "2021"
},
{
"DOI": "10.1210/jc.2018-00295",
"article-title": "Determination of free 25(OH)D concentrations and their relationships to total 25(OH)D in multiple clinical populations",
"author": "Schwartz",
"doi-asserted-by": "crossref",
"first-page": "3278",
"journal-title": "J Clin Endocrinol Metab",
"key": "2021072714055093000_4.1.213.68",
"volume": "103",
"year": "2018"
},
{
"DOI": "10.1016/j.jsbmb.2017.11.014.",
"doi-asserted-by": "publisher",
"key": "2021072714055093000_4.1.213.69"
}
],
"reference-count": 69,
"references-count": 69,
"relation": {
"has-preprint": [
{
"asserted-by": "object",
"id": "10.1101/2021.01.29.21250759",
"id-type": "doi"
}
]
},
"resource": {
"primary": {
"URL": "https://nutrition.bmj.com/lookup/doi/10.1136/bmjnph-2021-000255"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Nutrition and Dietetics",
"Medicine (miscellaneous)",
"Health (social science)"
],
"subtitle": [],
"title": "Genetically predicted serum vitamin D and COVID-19: a Mendelian randomisation study",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1136/crossmarkpolicy",
"volume": "4"
}