
A Randomized Phase 2 Study of Anti-IL-8 Therapy Versus Standard of Care in the Treatment of Hospitalized Patients With Severe COVID-19
et al., NCT04347226, NCT04347226, May 2025
{kind=link}
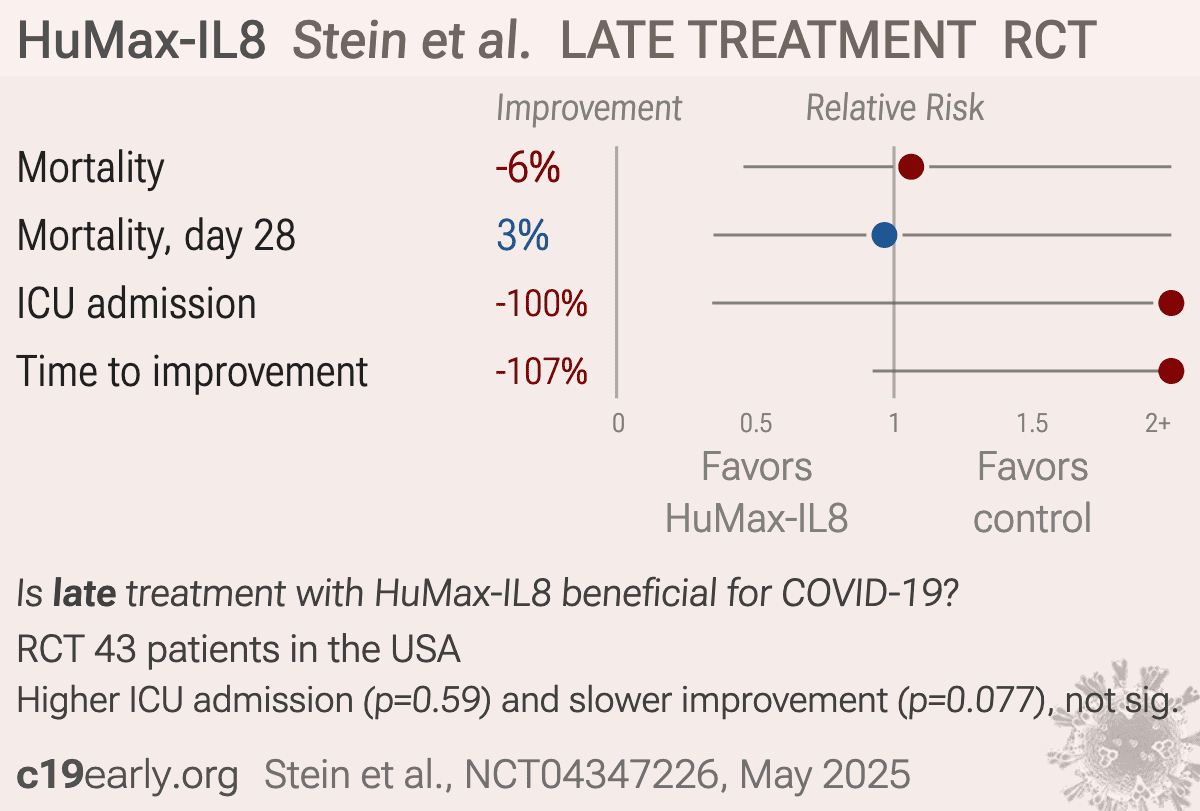
RCT 43 hospitalized patients in the USA showing no significant benefit with HuMax-IL8 (BMS-986253) treatment.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
This may explain in part the very high mortality seen in this study.
Results may differ in countries with improved SOC.
|
risk of death, 6.2% higher, RR 1.06, p = 1.00, treatment 11 of 29 (37.9%), control 5 of 14 (35.7%).
|
|
risk of death, 3.4% lower, RR 0.97, p = 1.00, treatment 8 of 29 (27.6%), control 4 of 14 (28.6%), NNT 102, day 28.
|
|
risk of ICU admission, 100% higher, RR 2.00, p = 0.59, treatment 9 of 18 (50.0%), control 1 of 4 (25.0%).
|
|
time to improvement, 107.1% higher, relative time 2.07, p = 0.08, treatment 29.0 [5.0-27.0] n=29, control 14.0 [4.0-13.0] n=14.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Stein et al., 22 May 2025, Randomized Controlled Trial, USA, preprint, 1 author, trial NCT04347226 (history).
Contact: mns2146@cumc.columbia.edu.
{kind=link}
Late treatment
is less effective
is less effective
