Characteristics and outcomes of COVID-19 patients admitted to a regional health system in the southeast
et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofaa439.560, Dec 2020
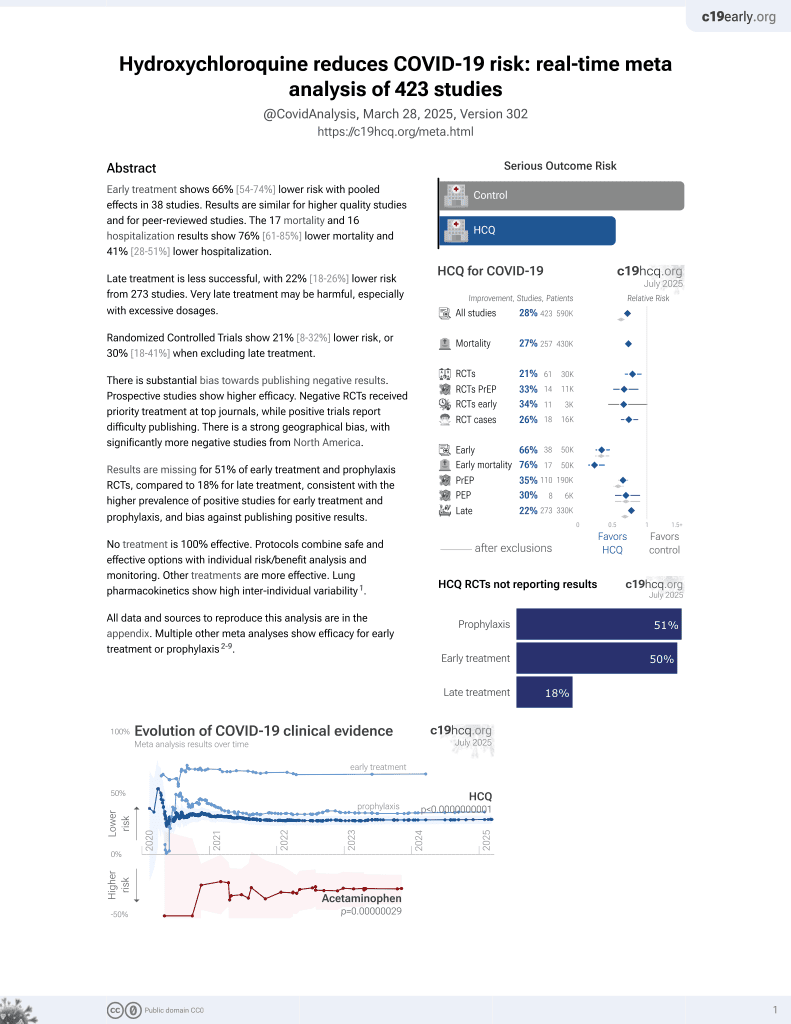
HCQ for COVID-19
1st treatment shown to reduce risk in
March 2020, now with p < 0.00000000001 from 424 studies, used in 59 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
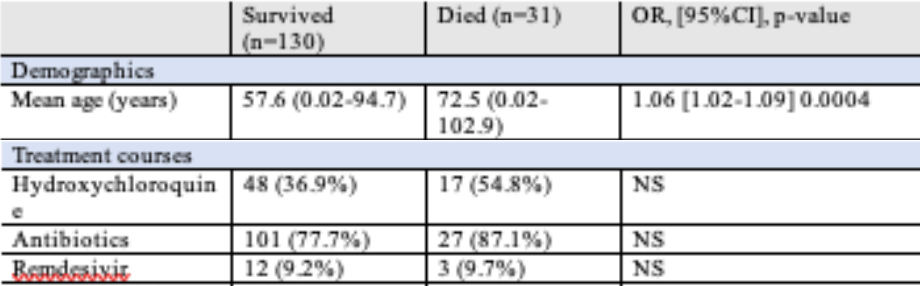
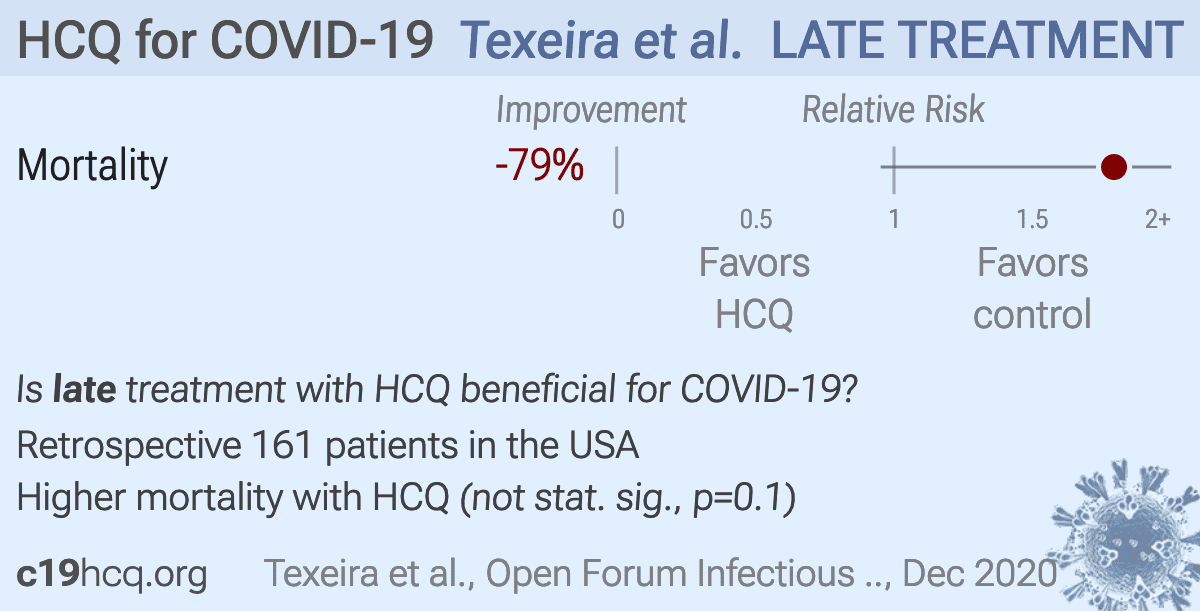
Retrospective 161 hospitalized patients in the USA showing non-statistically significant unadjusted increased mortality with HCQ. Confounding by indication is likely.
Time varying confounding is likely. HCQ became controversial and was suspended towards the end of the period studied, therefore HCQ use was likely more frequent toward the beginning of the study period, a time when overall treatment protocols were significantly worse.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
This study is excluded in the after exclusion results of meta-analysis:
unadjusted results with no group details; no treatment details; substantial confounding by time likely due to declining usage over the early stages of the pandemic when overall treatment protocols improved dramatically; substantial unadjusted confounding by indication likely.
|
risk of death, 79.3% higher, RR 1.79, p = 0.10, treatment 17 of 65 (26.2%), control 14 of 96 (14.6%).
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Texeira et al., 31 Dec 2020, retrospective, USA, peer-reviewed, 6 authors.
{kind=link}
Poster Abstracts • OFID 2020:7 (Suppl 1) • S251
Session: P-12. COVID-19 Complications, Co-infections, and Clinical Outcomes Background: The novel coronavirus disease (COVID-19) results in severe illness in a significant proportion of patients, necessitating a way to discern which patients will become critically ill and which will not. In one large case series, 5.0% of patients required an intensive care unit (ICU) and 1.4% died. Several models have been developed to assess decompensating patients. However, research examining their applicability to COVID-19 patients is limited. An accurate predictive model for patients at risk of decompensation is critical for health systems to optimally triage emergencies, care for patients, and allocate resources. Methods: An early warning score (EWS) algorithm created within a large academic medical center, with methodology previously described, was applied to COVID-19 patients admitted to this institution. 122 COVID-19 patients were included. A decompensation event was defined as inpatient mortality or an unanticipated transfer to an ICU from an intermediate medical ward. The EWS was calculated at 12-hour and 24-hour intervals. Results: Of 122 patients admitted with COVID-19, 28 had a decompensation event, yielding an event rate of 23.0%. 8 patients died, 13 transferred to the ICU, and 6 both transferred to the ICU and died. Decompensation within 12 and 24 hours were predicted with areas under the curve (AUC) of 0.850 and 0.817, respectively. Using a three-tiered risk model, use of the customized EWS score for patients identified as high risk of decompensation had a positive predictive value of 44.4% and 11.1% and specificity of 99.3% and 99.6% and 12-and 24-hour intervals. Amongst medium-risk patients, the score had a specificity of 85.0% and 85.4%, respectively. Conclusion: This EWS allows for prediction of decompensation, defined as transfer to an ICU or death, in COVID-19 patients with excellent specificity and a high positive predictive value. Clinically, implementation of this score can help to identify patients before they decompensate in order to triage at time of presentation and allocate step-down beds, ICU beds, and treatments such as remdesivir.
Poster Abstracts • OFID 2020:7 (Suppl 1) • S253 pts admitted to our southeast U.S. HS had significant comorbidities, most commonly obesity, HTN, and diabetes. Additionally, AA comprised a disproportionate share (72%) of our cohort compared to the general population of our state (30%), those tested in our region (32.9%), and those found to be positive for . In-hospital mortality was 19.3% and intubation, particularly if delayed, was associated with death as were several complications, most notably arrhythmia, ARDS, and renal failure with HD. Disclosures: All Authors: No reported disclosures
Characteristics and Outcomes of COVID-19 Patients with Fungal Infections Erica Herc, MD 1 ; Nicholas F. Yared, MD 2 ; Adam Kudirka, MD 1 ; Geehan Suleyman, MD 1 ; 1 Henry Ford Hospital, Detroit, MI; 2 Henry Ford Health System, Detroit, Michigan
Session: P-12. COVID-19 Complications, Co-infections, and Clinical Outcomes Background: There is concern that patients with coronavirus disease 2019 (COVID-19) are at risk of developing secondary bacterial and fungal infections; however, data on the clinical characteristics and outcomes of COVID-19 patients with fungal infections are limited. We evaluated the risk factors and mortality of hospitalized COVID-19 patients with fungal infections. Methods: This was a retrospective chart review of 51 patients with fungal infections at an 877-bed teaching hospital in Detroit, Michigan from March through May 2020. Demographic data, comorbidities,..
DOI record:
{
"DOI": "10.1093/ofid/ofaa439.560",
"ISSN": [
"2328-8957"
],
"URL": "http://dx.doi.org/10.1093/ofid/ofaa439.560",
"abstract": "<jats:title>Abstract</jats:title>\n <jats:sec>\n <jats:title>Background</jats:title>\n <jats:p>COVID-19, first described in Wuhan, China, is now a global pandemic. We describe a cohort of patients (pts) admitted to our academic health system (HS) in the southeast, where demographics and comorbidities differ significantly from other regions in the U.S.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Methods</jats:title>\n <jats:p>This was a retrospective review of 161 consecutive pts admitted with COVID-19 from 3/12/20 to 6/1/20. We assessed demographics, comorbidities, presenting symptoms, treatments and outcomes and compared pts who died during hospitalization to those who survived to discharge (EpiInfo 7.2, Atlanta, GA).</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Results</jats:title>\n <jats:p>Mean age was 60.5 years, 51.6% were female, 72% African American (AA) and 69.6% admitted from home. 54.5% had a BMI &gt;30, 72% had HTN, 47.2% diabetes, and 33.6% COPD or asthma. The majority (68.8%) presented with fever (&gt;38.0) and required supplemental oxygen within 8 hours of admission (63.4%). Cough (65.6%), dyspnea (57.5%), myalgias (30.6%) and diarrhea (23.8%) were also common. 40.4% received hydroxychloroquine, 23.6% steroids and 19.9% convalescent plasma. 42.9% required ICU care, 27.3% were intubated, and 19.3% died. Characteristics associated with death included older age, male sex, HTN, ESRD on HD, and cancer. Symptoms associated with death included absence of cough, absence of myalgias, previous admission for COVID-19, tachypnea, need for supplemental oxygen, elevated BUN and creatinine, and elevated ferritin. Interventions associated with death included use of steroids, receipt of ICU care, intubation, delay to intubation, and use of vasopressors or inotropes. Complications associated with death included development of a new arrhythmia, bacteremia, pneumonia, ARDS, thrombosis, and new renal failure requiring HD (Table).</jats:p>\n <jats:p>Table 1. Patient Characteristics by Death</jats:p>\n <jats:p />\n <jats:p>Table 2. Patient Characteristics by Death</jats:p>\n <jats:p />\n <jats:p>Table 3. Patient Characteristics by Death</jats:p>\n <jats:p />\n </jats:sec>\n <jats:sec>\n <jats:title>Conclusion</jats:title>\n <jats:p>COVID-19 pts admitted to our southeast U.S. HS had significant comorbidities, most commonly obesity, HTN, and diabetes. Additionally, AA comprised a disproportionate share (72%) of our cohort compared to the general population of our state (30%), those tested in our region (32.9%), and those found to be positive for COVID-19 (35.8%). In-hospital mortality was 19.3% and intubation, particularly if delayed, was associated with death as were several complications, most notably arrhythmia, ARDS, and renal failure with HD.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Disclosures</jats:title>\n <jats:p>All Authors: No reported disclosures</jats:p>\n </jats:sec>",
"author": [
{
"affiliation": [
{
"name": "Medical University of South Carolina, Charleston, South Carolina"
}
],
"family": "Teixeira",
"given": "Charles",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Medical University of South Carolina, Charleston, South Carolina"
}
],
"family": "Shiflett",
"given": "Henry",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Medical University of South Carolina, Charleston, South Carolina"
}
],
"family": "Jandhyala",
"given": "Deeksha",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Medical University of South Carolina, Charleston, South Carolina"
}
],
"family": "Lewis",
"given": "Jessica",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Medical University of South Carolina, Charleston, South Carolina"
}
],
"family": "Curry",
"given": "Scott R",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Medical University of South Carolina, Charleston, South Carolina"
}
],
"family": "Salgado",
"given": "Cassandra",
"sequence": "additional"
}
],
"container-title": "Open Forum Infectious Diseases",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2021,
1,
2
]
],
"date-time": "2021-01-02T08:23:08Z",
"timestamp": 1609575788000
},
"deposited": {
"date-parts": [
[
2021,
1,
2
]
],
"date-time": "2021-01-02T08:23:09Z",
"timestamp": 1609575789000
},
"indexed": {
"date-parts": [
[
2022,
4,
4
]
],
"date-time": "2022-04-04T01:42:18Z",
"timestamp": 1649036538809
},
"is-referenced-by-count": 0,
"issue": "Supplement_1",
"issued": {
"date-parts": [
[
2020,
10,
1
]
]
},
"journal-issue": {
"issue": "Supplement_1",
"published-print": {
"date-parts": [
[
2020,
12,
31
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://creativecommons.org/licenses/by-nc-nd/4.0/",
"content-version": "vor",
"delay-in-days": 93,
"start": {
"date-parts": [
[
2021,
1,
2
]
],
"date-time": "2021-01-02T00:00:00Z",
"timestamp": 1609545600000
}
}
],
"link": [
{
"URL": "http://academic.oup.com/ofid/article-pdf/7/Supplement_1/S251/35343547/ofaa439.560.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "syndication"
},
{
"URL": "http://academic.oup.com/ofid/article-pdf/7/Supplement_1/S251/35343547/ofaa439.560.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "286",
"original-title": [],
"page": "S251-S253",
"prefix": "10.1093",
"published": {
"date-parts": [
[
2020,
10,
1
]
]
},
"published-online": {
"date-parts": [
[
2020,
12,
31
]
]
},
"published-other": {
"date-parts": [
[
2020,
10,
1
]
]
},
"published-print": {
"date-parts": [
[
2020,
12,
31
]
]
},
"publisher": "Oxford University Press (OUP)",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "https://academic.oup.com/ofid/article/7/Supplement_1/S251/6058327"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Infectious Diseases",
"Oncology"
],
"subtitle": [],
"title": "365. Characteristics and outcomes of COVID-19 patients admitted to a regional health system in the southeast",
"type": "journal-article",
"volume": "7"
}
Late treatment
is less effective
is less effective
