Repurposed antiviral drugs for COVID-19; interim WHO SOLIDARITY trial results
, NEJM, doi:10.1056/NEJMoa2023184, SOLIDARITY, NCT04315948, Oct 2020 (preprint)
{kind=link}
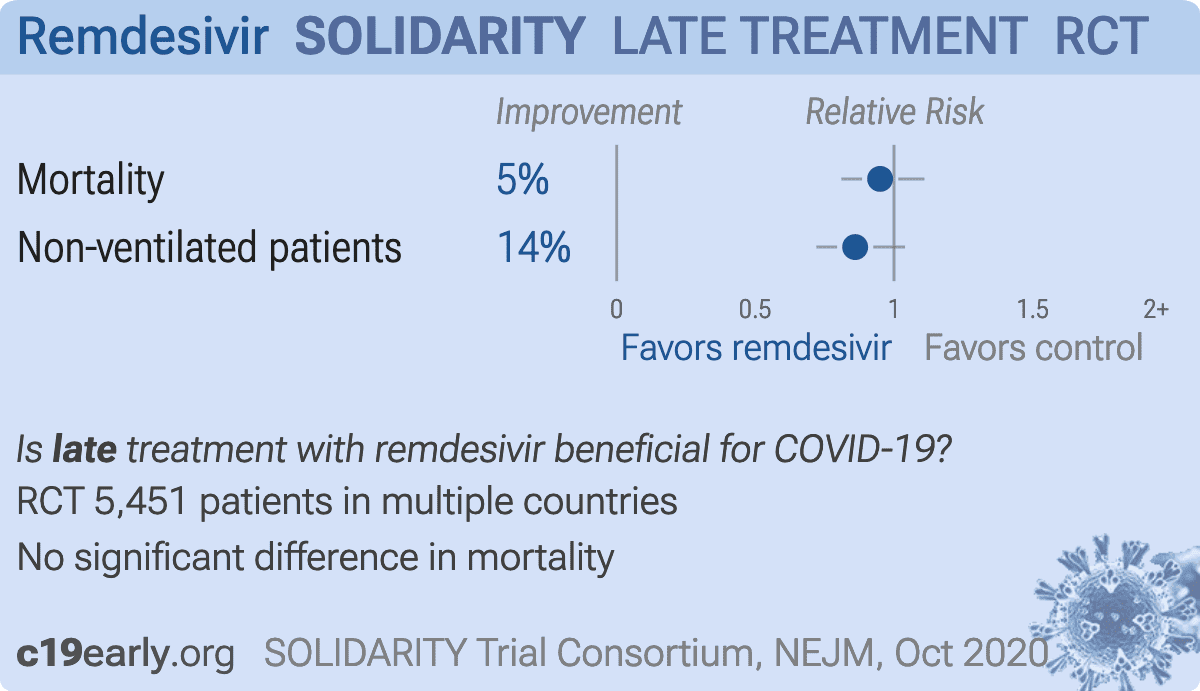
WHO SOLIDARITY open-label RCT with 2,750 very late stage (76% on oxygen/ventilation) remdesivir patients, mortality relative risk RR 0.95 [0.81-1.11], p=0.50. Non-ventilated patients show a greater benefit, RR 0.86 [0.72-1.04], p = 0.13.
Gérard, Zhou, Wu, Kamo, Choi, Kim show increased risk of acute kidney injury, Leo, Briciu, Muntean, Petrov, Arch show increased risk of liver injury, Negru, Cheng, Mohammed, Kwok, Zhu show increased risk of cardiac disorders, and Kwok, Merches, Akinci, Tang, Bagheri show increased risk of mitochondrial toxicity with remdesivir.
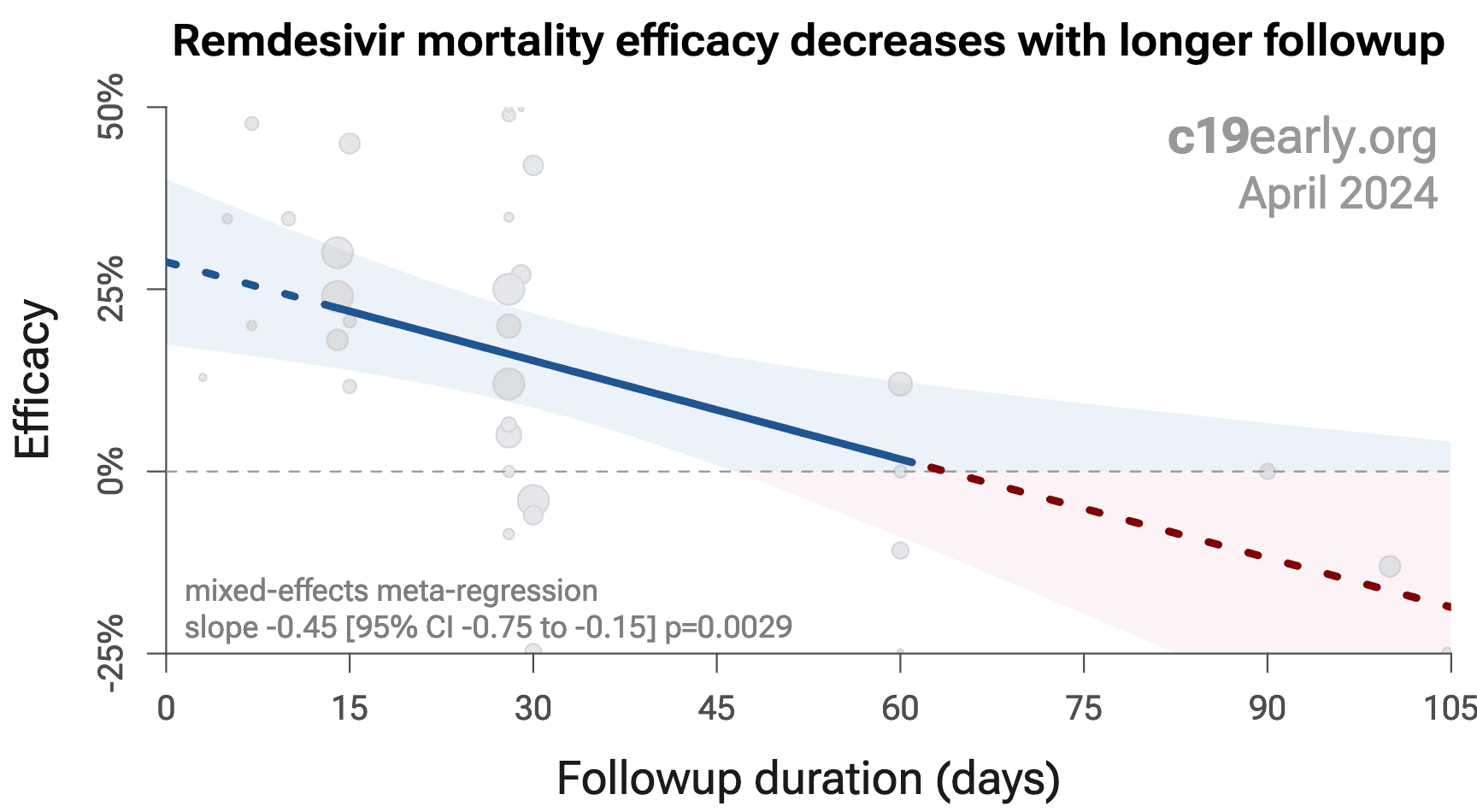
Remdesivir efficacy disappears with longer
followup. Mixed-effects meta-regression of efficacy as a function of
followup duration across all remdesivir studies shows decreasing efficacy with
longer followup21. This may reflect
antiviral efficacy being offset by serious adverse effects of treatment.
{kind=link}
Study covers lopinavir/ritonavir, remdesivir, and HCQ.
|
risk of death, 5.0% lower, RR 0.95, p = 0.53, treatment 301 of 2,743 (11.0%), control 303 of 2,708 (11.2%), NNT 464, day 28.
|
|
non-ventilated patients, 14.0% lower, RR 0.86, p = 0.13, day 28.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
1.
Gérard et al., Remdesivir and Acute Renal Failure: A Potential Safety Signal From Disproportionality Analysis of the WHO Safety Database, Clinical Pharmacology & Therapeutics, doi:10.1002/cpt.2145.
2.
Zhou et al., Acute Kidney Injury and Drugs Prescribed for COVID-19 in Diabetes Patients: A Real-World Disproportionality Analysis, Frontiers in Pharmacology, doi:10.3389/fphar.2022.833679.
3.
Wu et al., Acute Kidney Injury Associated With Remdesivir: A Comprehensive Pharmacovigilance Analysis of COVID-19 Reports in FAERS, Frontiers in Pharmacology, doi:10.3389/fphar.2022.692828.
4.
Kamo et al., Association of Antiviral Drugs for the Treatment of COVID-19 With Acute Renal Failure, In Vivo, doi:10.21873/invivo.13637.
5.
Choi et al., Comparative effectiveness of combination therapy with nirmatrelvir–ritonavir and remdesivir versus monotherapy with remdesivir or nirmatrelvir–ritonavir in patients hospitalised with COVID-19: a target trial emulation study, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(24)00353-0.
6.
Kim et al., Investigating the Safety Profile of Fast‐Track COVID‐19 Drugs Using the FDA Adverse Event Reporting System Database: A Comparative Observational Study, Pharmacoepidemiology and Drug Safety, doi:10.1002/pds.70043.
7.
Leo et al., Hepatocellular liver injury in hospitalized patients affected by COVID-19: Presence of different risk factors at different time points, Digestive and Liver Disease, doi:10.1016/j.dld.2021.12.014.
8.
Briciu et al., Evolving Clinical Manifestations and Outcomes in COVID-19 Patients: A Comparative Analysis of SARS-CoV-2 Variant Waves in a Romanian Hospital Setting, Pathogens, doi:10.3390/pathogens12121453.
9.
Muntean et al., Effects of COVID-19 on the Liver and Mortality in Patients with SARS-CoV-2 Pneumonia Caused by Delta and Non-Delta Variants: An Analysis in a Single Centre, Pharmaceuticals, doi:10.3390/ph17010003.
10.
Petrov et al., The Effect of Potentially Hepatotoxic Medicinal Products on Alanine Transaminase Levels in COVID-19 Patients: A Case–Control Study, Safety and Risk of Pharmacotherapy, doi:10.30895/2312-7821-2025-458.
11.
Arch et al., Evaluation of the effectiveness of remdesivir in treating severe COVID-19 using data from the ISARIC WHO Clinical Characterisation Protocol UK: a prospective, national cohort study, medRxiv, doi:10.1101/2021.06.18.21259072.
12.
Negru et al., Comparative Pharmacovigilance Analysis of Approved and Repurposed Antivirals for COVID-19: Insights from EudraVigilance Data, Biomedicines, doi:10.3390/biomedicines13061387.
13.
Cheng et al., Cardiovascular Safety of COVID-19 Treatments: A Disproportionality Analysis of Adverse Event Reports from the WHO VigiBase, Infectious Diseases and Therapy, doi:10.1007/s40121-025-01225-z.
14.
Mohammed et al., Bradycardia associated with remdesivir treatment in coronavirus disease 2019 patients: A propensity score-matched analysis, Medicine, doi:10.1097/MD.0000000000044501.
15.
Kwok et al., Remdesivir induces persistent mitochondrial and structural damage in human induced pluripotent stem cell-derived cardiomyocytes, Cardiovascular Research, doi:10.1093/cvr/cvab311.
16.
Zhu et al., Cardiovascular Risks of COVID-19 Therapeutics: Integrated Analysis of FAERS, Electronic Health Records, and Transcriptomics, Pharmaceuticals, doi:10.3390/ph19040574.
17.
Merches et al., The potential of remdesivir to affect function, metabolism and proliferation of cardiac and kidney cells in vitro, Archives of Toxicology, doi:10.1007/s00204-022-03306-1.
18.
Akinci et al., Elucidation of remdesivir cytotoxicity pathways through genome-wide CRISPR-Cas9 screening and transcriptomics, bioRxiv, doi:10.1101/2020.08.27.270819.
19.
Tang et al., Modeling drug-induced mitochondrial toxicity with human primary cardiomyocytes, Science China Life Sciences, doi:10.1007/s11427-023-2369-3.
SOLIDARITY Trial Consortium et al., 15 Oct 2020, Randomized Controlled Trial, multiple countries, peer-reviewed, 15 authors, trial NCT04315948 (history) (SOLIDARITY).
Abstract: new england
journal of medicine
The
February 11, 2021
established in 1812
vol. 384
no. 6
Repurposed Antiviral Drugs for Covid-19 — Interim WHO
Solidarity Trial Results
WHO Solidarity Trial Consortium*
a bs t r ac t
BACKGROUND
World Health Organization expert groups recommended mortality trials of four
repurposed antiviral drugs — remdesivir, hydroxychloroquine, lopinavir, and interferon beta-1a — in patients hospitalized with coronavirus disease 2019 (Covid-19).
METHODS
We randomly assigned inpatients with Covid-19 equally between one of the trial
drug regimens that was locally available and open control (up to five options, four
active and the local standard of care). The intention-to-treat primary analyses examined in-hospital mortality in the four pairwise comparisons of each trial drug
and its control (drug available but patient assigned to the same care without that
drug). Rate ratios for death were calculated with stratification according to age
and status regarding mechanical ventilation at trial entry.
RESULTS
At 405 hospitals in 30 countries, 11,330 adults underwent randomization; 2750
were assigned to receive remdesivir, 954 to hydroxychloroquine, 1411 to lopinavir
(without interferon), 2063 to interferon (including 651 to interferon plus lopinavir),
and 4088 to no trial drug. Adherence was 94 to 96% midway through treatment,
with 2 to 6% crossover. In total, 1253 deaths were reported (median day of death,
day 8; interquartile range, 4 to 14). The Kaplan–Meier 28-day mortality was 11.8%
(39.0% if the patient was already receiving ventilation at randomization and 9.5%
otherwise). Death occurred in 301 of 2743 patients receiving remdesivir and in 303
of 2708 receiving its control (rate ratio, 0.95; 95% confidence interval [CI], 0.81 to
1.11; P = 0.50), in 104 of 947 patients receiving hydroxychloroquine and in 84 of
906 receiving its control (rate ratio, 1.19; 95% CI, 0.89 to 1.59; P = 0.23), in 148 of
1399 patients receiving lopinavir and in 146 of 1372 receiving its control (rate ratio,
1.00; 95% CI, 0.79 to 1.25; P = 0.97), and in 243 of 2050 patients receiving interferon and in 216 of 2050 receiving its control (rate ratio, 1.16; 95% CI, 0.96 to 1.39;
P = 0.11). No drug definitely reduced mortality, overall or in any subgroup, or reduced initiation of ventilation or hospitalization duration.
CONCLUSIONS
These remdesivir, hydroxychloroquine, lopinavir, and interferon regimens had little
or no effect on hospitalized patients with Covid-19, as indicated by overall mortality, initiation of ventilation, and duration of hospital stay. (Funded by the World
Health Organization; ISRCTN Registry number, ISRCTN83971151; ClinicalTrials.gov
number, NCT04315948.)
n engl j med 384;6
nejm.org
The members of the writing and steering
committees (H. Pan, R. Peto, A.-M.
Henao‑Restrepo, M.-P. Preziosi, V. Sathiyamoorthy, Q. Abdool Karim, M.M. Alejandria, C. Hernández García, M.-P. Kieny, R. Malekzadeh, S. Murthy, K.S.
Reddy, M. Roses Periago, P. Abi Hanna,
F. Ader, A.M. Al‑Bader, A. Alhasawi, E. Allum, A. Alotaibi, C.A. Alvarez‑Moreno, S.
Appadoo, A. Asiri, P. Aukrust, A. Barratt‑Due, S. Bellani, M. Branca, H.B.C.
Cappel‑Porter, N. Cerrato, T.S. Chow, N.
Como, J. Eustace, P.J. García, S. Godbole,
E. Gotuzzo, L. Griskevicius, R. Hamra, M.
Hassan, M. Hassany, D. Hutton, I. Irmansyah, L. Jancoriene, J. Kirwan, S. Kumar, P. Lennon, G. Lopardo, P. Lydon, N.
Magrini, T. Maguire, S. Manevska, O.
Manuel, S. McGinty, M.T. Medina, M.L.
Mesa..
DOI record:
{
"DOI": "10.1056/nejmoa2023184",
"ISSN": [
"0028-4793",
"1533-4406"
],
"URL": "http://dx.doi.org/10.1056/NEJMoa2023184",
"alternative-id": [
"10.1056/NEJMoa2023184"
],
"author": [
{
"affiliation": [],
"name": "WHO Solidarity Trial Consortium",
"sequence": "first"
}
],
"container-title": "New England Journal of Medicine",
"container-title-short": "N Engl J Med",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2020,
12,
2
]
],
"date-time": "2020-12-02T22:03:18Z",
"timestamp": 1606946598000
},
"deposited": {
"date-parts": [
[
2023,
8,
10
]
],
"date-time": "2023-08-10T18:05:51Z",
"timestamp": 1691690751000
},
"funder": [
{
"DOI": "10.13039/100004423",
"doi-asserted-by": "publisher",
"name": "World Health Organization"
}
],
"indexed": {
"date-parts": [
[
2024,
4,
7
]
],
"date-time": "2024-04-07T23:13:51Z",
"timestamp": 1712531631524
},
"is-referenced-by-count": 1670,
"issue": "6",
"issued": {
"date-parts": [
[
2021,
2,
11
]
]
},
"journal-issue": {
"issue": "6",
"published-print": {
"date-parts": [
[
2021,
2,
11
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://www.nejmgroup.org/legal/terms-of-use.htm",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
2,
11
]
],
"date-time": "2021-02-11T00:00:00Z",
"timestamp": 1613001600000
}
}
],
"link": [
{
"URL": "http://www.nejm.org/doi/pdf/10.1056/NEJMoa2023184",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "150",
"original-title": [],
"page": "497-511",
"prefix": "10.1056",
"published": {
"date-parts": [
[
2021,
2,
11
]
]
},
"published-print": {
"date-parts": [
[
2021,
2,
11
]
]
},
"publisher": "Massachusetts Medical Society",
"reference": [
{
"DOI": "10.1371/journal.pmed.1003252",
"doi-asserted-by": "publisher",
"key": "r4"
},
{
"DOI": "10.1016/S0140-6736(05)66544-0",
"doi-asserted-by": "publisher",
"key": "r5"
},
{
"DOI": "10.1056/NEJMoa2007764",
"doi-asserted-by": "publisher",
"key": "r6"
},
{
"DOI": "10.1016/S0140-6736(20)31022-9",
"doi-asserted-by": "publisher",
"key": "r7"
},
{
"DOI": "10.1001/jama.2020.16349",
"doi-asserted-by": "publisher",
"key": "r8"
},
{
"DOI": "10.1056/NEJMoa2015301",
"doi-asserted-by": "publisher",
"key": "r9"
},
{
"DOI": "10.1038/bjc.2011.79",
"doi-asserted-by": "publisher",
"key": "r10"
},
{
"DOI": "10.1056/NEJMoa2022926",
"doi-asserted-by": "publisher",
"key": "r12"
},
{
"DOI": "10.1016/S0140-6736(20)32013-4",
"doi-asserted-by": "publisher",
"key": "r13"
},
{
"DOI": "10.1056/NEJMoa2001282",
"doi-asserted-by": "publisher",
"key": "r15"
},
{
"DOI": "10.1016/j.antiviral.2020.104866",
"doi-asserted-by": "publisher",
"key": "r16"
},
{
"DOI": "10.1093/jac/dkaa195",
"doi-asserted-by": "publisher",
"key": "r17"
},
{
"DOI": "10.1089/10799900050163226",
"doi-asserted-by": "publisher",
"key": "r18"
},
{
"DOI": "10.1186/s13054-020-03048-5",
"doi-asserted-by": "publisher",
"key": "r19"
},
{
"DOI": "10.1007/s00134-020-06086-3",
"doi-asserted-by": "publisher",
"key": "r20"
},
{
"DOI": "10.1128/MCB.00146-10",
"doi-asserted-by": "publisher",
"key": "r21"
},
{
"DOI": "10.1056/NEJMoa2021436",
"doi-asserted-by": "publisher",
"key": "r22"
}
],
"reference-count": 17,
"references-count": 17,
"relation": {
"has-preprint": [
{
"asserted-by": "object",
"id": "10.1101/2020.10.15.20209817",
"id-type": "doi"
}
]
},
"resource": {
"primary": {
"URL": "http://www.nejm.org/doi/10.1056/NEJMoa2023184"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"General Medicine"
],
"subtitle": [],
"title": "Repurposed Antiviral Drugs for Covid-19 — Interim WHO Solidarity Trial Results",
"type": "journal-article",
"volume": "384"
}
Late treatment
is less effective
is less effective

solidarity