Nirmatrelvir and Molnupiravir and Post–COVID-19 Condition in Older Patients
et al., JAMA Internal Medicine, doi:10.1001/jamainternmed.2023.5099, Oct 2023
{kind=link}
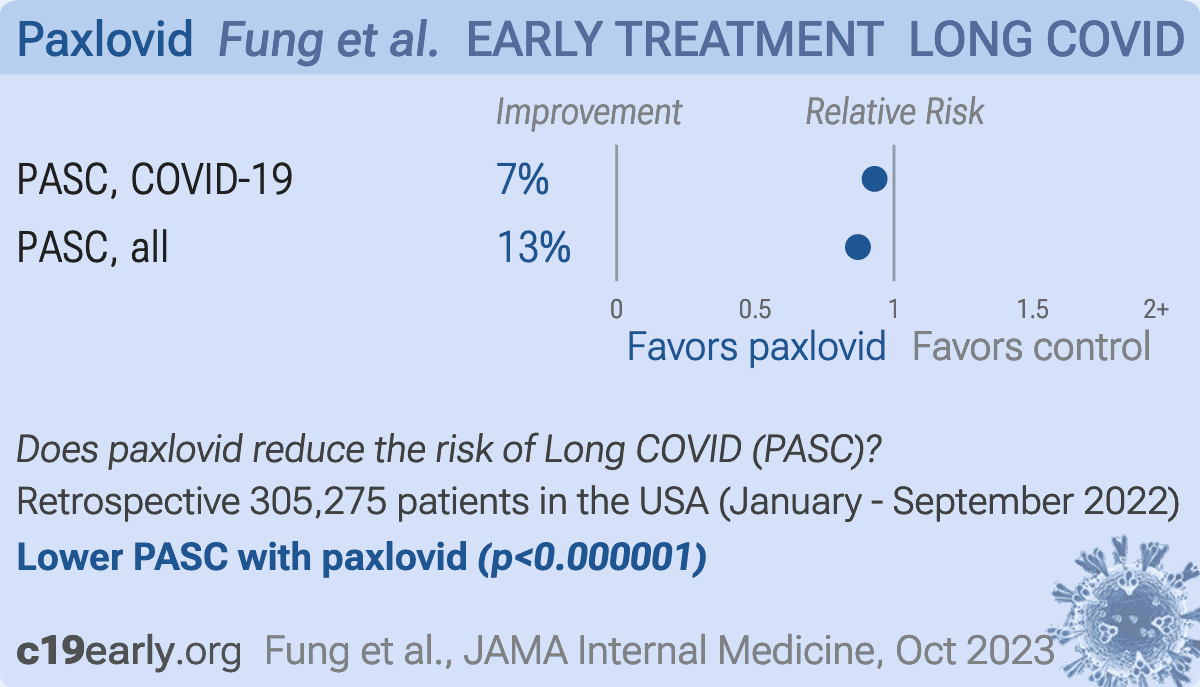
Retrospective 51,658 paxlovid patients in the USA showing a small reduction in long COVID with treatment.
Confounding is likely significant as below, and may eliminate the benefit. Results specific to the COVID-19 code should be closer to the actual efficacy due to likely lower average severity of the additional treatment patients included based on home tests.
Confounding by treatment propensity. This study analyzes a population
where only a fraction of eligible patients received the treatment. Patients
receiving treatment may be more likely to follow other recommendations, more
likely to receive additional care, and more likely to use additional
treatments that are not tracked in the data (e.g., nasal/oral hygiene1,2, vitamin D3, etc.) — either because the physician
recommending paxlovid also recommended them, or
because the patient seeking out paxlovid is more
likely to be familiar with the efficacy of additional treatments and more
likely to take the time to use them.
Malden et al. confirm significant bias in the use of paxlovid, showing that treated
patients are more likely to be from affluent neighborhoods, be more health-conscious, and
have better access to care. Campion et al. also show that female patients were more
likely to receive paxlovid, and studies show that female patients are significantly more
likely to be health-conscious, for example being more likely to take additional
non-prescription treatments.
Therefore, these kind of studies may
overestimate efficacy.
Resistance. Variants may be resistant to paxlovid6-14. Use may promote the emergence of variants that weaken host immunity and potentially contribute to long COVID15. Confounding by contraindication. Hoertel et al. find that over 50% of patients that died had a contraindication for the use of Paxlovid16. Retrospective studies that do not exclude contraindicated patients may significantly overestimate efficacy. Black box warning. The FDA notes that severe, life-threatening, and/or fatal adverse reactions due to drug interactions have been reported in patients treated with paxlovid17. Kidney and liver injury. Studies show significantly increased risk of acute kidney injury18 and liver injury19,20. Viral rebound. Studies show significantly increased risk of replication-competent viral rebound21-23.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments24.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
Study covers paxlovid and molnupiravir.
|
risk of long COVID, 7.0% lower, HR 0.93, p < 0.001, COVID-19 only, Cox proportional hazards.
|
|
risk of long COVID, 13.0% lower, HR 0.87, p < 0.001, including patients without COVID-19 code, Cox proportional hazards.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
4.
Malden et al., Predictors of nirmatrelvir–ritonavir receipt among COVID-19 patients in a large US health system, Scientific Reports, doi:10.1038/s41598-024-57633-7.
5.
Campion et al., Disparities in the Use of nirmatrelvir/ritonavir for COVID-19: A Retrospective Cohort Study, Open Forum Infectious Diseases, doi:10.1093/ofid/ofaf695.1809.
6.
Zhou et al., Nirmatrelvir-resistant SARS-CoV-2 variants with high fitness in an infectious cell culture system, Science Advances, doi:10.1126/sciadv.add7197.
7.
Moghadasi et al., Rapid resistance profiling of SARS-CoV-2 protease inhibitors, npj Antimicrobials and Resistance, doi:10.1038/s44259-023-00009-0.
8.
Jochmans et al., The Substitutions L50F, E166A, and L167F in SARS-CoV-2 3CLpro Are Selected by a Protease Inhibitor In Vitro and Confer Resistance To Nirmatrelvir, mBio, doi:10.1128/mbio.02815-22.
9.
Lopez et al., SARS-CoV-2 Resistance to Small Molecule Inhibitors, Current Clinical Microbiology Reports, doi:10.1007/s40588-024-00229-6.
10.
Zvornicanin et al., Molecular Mechanisms of Drug Resistance and Compensation in SARS-CoV-2 Main Protease: The Interplay Between E166 and L50, bioRxiv, doi:10.1101/2025.01.24.634813.
11.
Vukovikj et al., Impact of SARS-CoV-2 variant mutations on susceptibility to monoclonal antibodies and antiviral drugs: a non-systematic review, April 2022 to October 2024, Eurosurveillance, doi:10.2807/1560-7917.ES.2025.30.10.2400252.
12.
Deschenes et al., Functional and structural characterization of treatment-emergent nirmatrelvir resistance mutations at low frequencies in the main protease (Mpro) reveals a unique evolutionary route for SARS-CoV-2 to gain resistance, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf294.
13.
Zhou (B) et al., SARS-CoV-2 Mpro inhibitor ensitrelvir: asymmetrical cross-resistance with nirmatrelvir and emerging resistance hotspots, Emerging Microbes & Infections, doi:10.1080/22221751.2025.2552716.
14.
Chen et al., SARS-CoV-2 3CLpro mutations T21I and E166A confer differential resistance to simnotrelvir, bofutrelvir, and ensitrelvir, Journal of Virology, doi:10.1128/jvi.02223-25.
15.
Thomas et al., Nirmatrelvir-Resistant Mutations in SARS-CoV-2 Mpro Enhance Host Immune Evasion via Cleavage of NF-κB Essential Modulator, bioRxiv, doi:10.1101/2024.10.18.619137.
16.
Hoertel et al., Prevalence of Contraindications to Nirmatrelvir-Ritonavir Among Hospitalized Patients With COVID-19 at Risk for Progression to Severe Disease, JAMA Network Open, doi:10.1001/jamanetworkopen.2022.42140.
17.
FDA, Fact sheet for healthcare providers: emergency use authorization for paxlovid, www.fda.gov/media/155050/download.
18.
Kamo et al., Association of Antiviral Drugs for the Treatment of COVID-19 With Acute Renal Failure, In Vivo, doi:10.21873/invivo.13637.
19.
Wang et al., Development and validation of a nomogram to assess the occurrence of liver dysfunction in patients with COVID-19 pneumonia in the ICU, BMC Infectious Diseases, doi:10.1186/s12879-025-10684-1.
20.
Siby et al., Temporal Trends in Serious Adverse Events Associated with Oral Antivirals During the COVID-19 Pandemic: Insights from the FAERS Database (2020–2023), Open Forum Infectious Diseases, doi:10.1093/ofid/ofaf695.1825.
21.
Edelstein et al., SARS-CoV-2 virologic rebound with nirmatrelvir-ritonavir therapy, medRxiv, doi:10.1101/2023.06.23.23288598.
22.
Shah et al., SARS-CoV-2 infectious shedding and rebound among adults with and without oral antiviral use: two case-ascertained prospective household studies, The Lancet Microbe, doi:10.1016/j.lanmic.2025.101227.
Fung et al., 23 Oct 2023, retrospective, USA, peer-reviewed, 4 authors, study period January 2022 - September 2022.
Contact: kfung@mail.nih.gov.
{kind=link}
Abstract: Letters
RESEARCH LETTER
Nirmatrelvir and Molnupiravir and Post–COVID-19
Condition in Older Patients
While the COVID-19 pandemic appears to be winding down, its
effects are still felt by the millions of people worldwide experiencing post–COVID-19 condition (PCC, or long COVID).1 The
antiviral drug nirmatrelvir (marketed as Paxlovid [Pfizer], in
combination with ritonavir)
and molnupiravir (Lagevrio
Supplemental content
[Merch]) are recommended as
first- and second-line treatments for acute illness in patients with
specific risk factors (eg, diabetes).2 However, there are still no
US Food and Drug Administration–approved drugs for the treatment or prevention of PCC. Recent studies among US veterans
(mostly male) suggest that nirmatrelvir and molnupiravir reduce the risk of some sequelae of COVID-19.3,4 We performed a
cohort study of the 2 drugs in PCC in older patients who were
Medicare enrollees.
Methods | The cohort came from Medicare enrollees aged 65
years or older diagnosed with COVID-19 between January
and September 2022. COVID-19 was identified with an
outpatient International Statistical Classif ication of
Diseases, Tenth Revision, Clinical Modification code of
U07.1. In January 2022, free home COVID-19 tests became
available and not all positive self-tests were captured in
Medicare data. Therefore, we also considered the prescription of nirmatrelvir or molnupiravir to be indicative of
COVID-19 because no other indications existed. Following
previous work, 5 we identified PCC based on the World
Health Organization (WHO) consensus clinical definition.6
Any new occurrence (not present prior to COVID-19 diagnosis) of the 11 symptoms between 4 to 12 weeks after infection was considered as PCC. We used an extended Cox
regression with propensity score adjustment to examine the
2 drugs and the incidence of PCC. We included age, sex,
race, geographic region, dual eligibility, low-income subsidy, and 51 chronic comorbidities as covariates as included
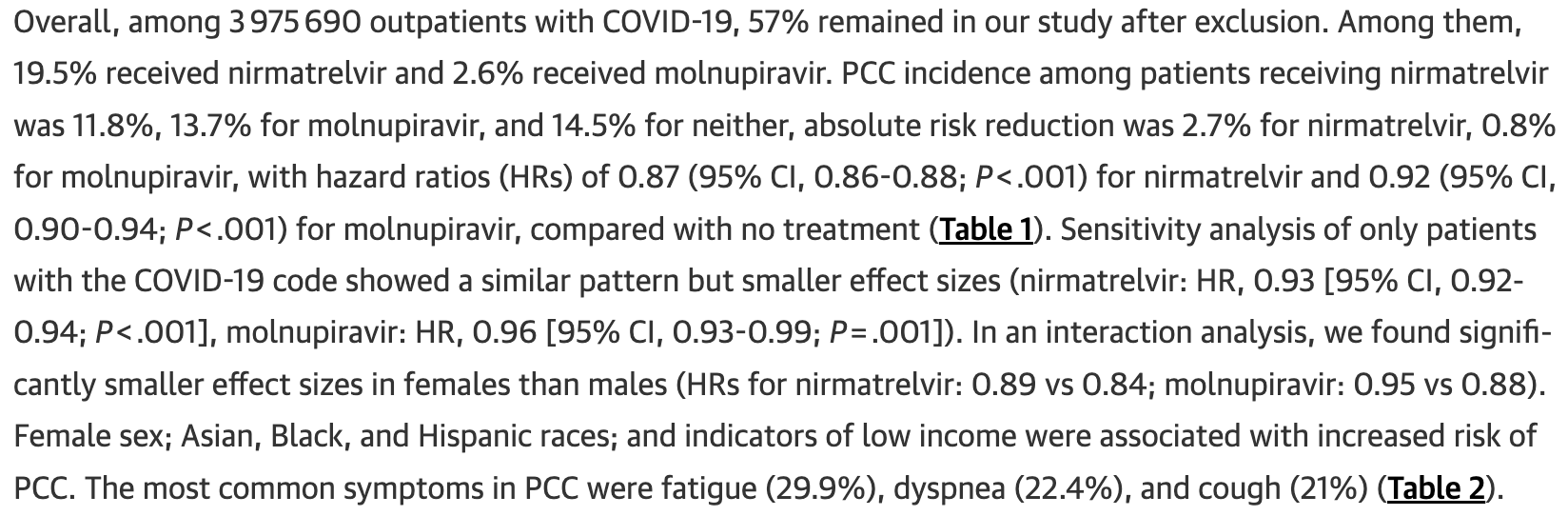
Table 1. Hazard Ratio Based on Cox Regression Modela
Event rate, % (95% CI)
Index variable
Reference
No. (%)
Hazard ratio (95% CI)
Index group
Reference group
Absolute risk
reductionb
Nirmatrelvir
None
439 134 (19.5)
0.87 (0.86 to 0.88)
11.8 (11.7 to 11.9)
14.5 (14.4 to 14.6)
2.7
Molnupiravir
None
58 914 (2.6)
0.92 (0.90 to 0.94)
13.7 (13.5 to 14.0)
14.5 (14.4 to 14.6)
0.8
Female
Male
1 313 415 (58.5)
1.17 (1.16 to 1.18)
14.5 (14.4 to 14.6)
13.2 (13.1 to 13.2)
−1.3
70-74
65-69
656 324 (29.2)
0.78 (0.77 to 0.79)
12.7 (12.7 to 12.8)
12.0 (11.9 to 12.1)
−0.7
75-79
65-69
509 291 (22.7)
0.70 (0.69 to 0.71)
14.2 (14.1 to 14.3)
12.0 (11.9 to 12.1)
−2.2
80-84
65-69
324 008 (14.4)
0.64 (0.63 to 0.66)
15.8 (15.7 to 16.0)
12.0 (11.9 to 12.1)
−3.8
≥85
65-69
313 754 (14.0)
0.61 (0.60 to 0.63)
16.9 (16.7 to 17.0)
12.0 (11.9 to 12.1)
−4.9
Asian
White
81 073 (3.6)
1.10 (1.07 to 1.12)
13.3 (13.0 to 13.5)
13.9 (13.9 to 14.0)
0.6
Black
White
82 249 (3.7)
1.24 (1.22 to 1.27)
15.3 (15.0 to 15.5)
13.9 (13.9 to 14.0)
−1.4
Hispanic
White
93 325 (4.2)
1.02 (1.00 to 1.04)
15.4 (15.1 to 15.6)
13.9 (13.9 to 14.0)
−1.5
Otherd
White
93 011 (4.1)
1.04 (1.02 to 1.06)
12.4 (12.1 to 12.6)
13.9 (13.9 to 14.0)
1.5
Dual eligibility
Nondual
244 874 (10.9)
1.06 (1.05 to 1.08)
16.6 (16.5 to 16.8)
13.6 (13.5 to 13.6)
−3.0
Low-income subsidy
Nondual
21 049 (0.9)
1.07 (1.03 to 1.10)
16.4 (15.9 to 16.9)
13.6 (13.5 to..
DOI record:
{
"DOI": "10.1001/jamainternmed.2023.5099",
"ISSN": [
"2168-6106"
],
"URL": "http://dx.doi.org/10.1001/jamainternmed.2023.5099",
"abstract": "<jats:p>This observational cohort study assesses the occurrence of post–COVID-19 condition symptoms in Medicare enrollees prescribed nirmatrelvir and molnupiravir.</jats:p>",
"author": [
{
"affiliation": [
{
"name": "Lister Hill National Center for Biomedical Communications, National Library of Medicine, Bethesda, Maryland"
}
],
"family": "Fung",
"given": "Kin Wah",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Lister Hill National Center for Biomedical Communications, National Library of Medicine, Bethesda, Maryland"
}
],
"family": "Baye",
"given": "Fitsum",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Lister Hill National Center for Biomedical Communications, National Library of Medicine, Bethesda, Maryland"
},
{
"name": "National Institutes of Health, Bethesda, Maryland"
}
],
"family": "Baik",
"given": "Seo H.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Lister Hill National Center for Biomedical Communications, National Library of Medicine, Bethesda, Maryland"
},
{
"name": "National Institutes of Health, Bethesda, Maryland"
}
],
"family": "McDonald",
"given": "Clement J.",
"sequence": "additional"
}
],
"container-title": "JAMA Internal Medicine",
"container-title-short": "JAMA Intern Med",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2023,
10,
23
]
],
"date-time": "2023-10-23T15:00:50Z",
"timestamp": 1698073250000
},
"deposited": {
"date-parts": [
[
2023,
10,
23
]
],
"date-time": "2023-10-23T15:00:53Z",
"timestamp": 1698073253000
},
"indexed": {
"date-parts": [
[
2023,
10,
24
]
],
"date-time": "2023-10-24T05:21:07Z",
"timestamp": 1698124867571
},
"is-referenced-by-count": 0,
"issued": {
"date-parts": [
[
2023,
10,
23
]
]
},
"language": "en",
"link": [
{
"URL": "https://jamanetwork.com/journals/jamainternalmedicine/articlepdf/2811092/jamainternal_fung_2023_ld_230034_1697659326.29106.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "10",
"original-title": [],
"prefix": "10.1001",
"published": {
"date-parts": [
[
2023,
10,
23
]
]
},
"published-online": {
"date-parts": [
[
2023,
10,
23
]
]
},
"publisher": "American Medical Association (AMA)",
"reference": [
{
"DOI": "10.1038/s41579-022-00846-2",
"article-title": "Long COVID: major findings, mechanisms and recommendations.",
"author": "Davis",
"doi-asserted-by": "publisher",
"first-page": "133",
"issue": "3",
"journal-title": "Nat Rev Microbiol",
"key": "ild230034r1",
"volume": "21",
"year": "2023"
},
{
"DOI": "10.1056/NEJMoa2118542",
"article-title": "Oral nirmatrelvir for high-risk, nonhospitalized adults with COVID-19.",
"author": "Hammond",
"doi-asserted-by": "publisher",
"first-page": "1397",
"issue": "15",
"journal-title": "N Engl J Med",
"key": "ild230034r2",
"volume": "386",
"year": "2022"
},
{
"DOI": "10.1001/jamainternmed.2023.0743",
"article-title": "Association of treatment with nirmatrelvir and the risk of post-COVID-19 condition.",
"author": "Xie",
"doi-asserted-by": "publisher",
"first-page": "554",
"issue": "6",
"journal-title": "JAMA Intern Med",
"key": "ild230034r3",
"volume": "183",
"year": "2023"
},
{
"DOI": "10.1136/bmj-2022-074572",
"article-title": "Molnupiravir and risk of post-acute sequelae of covid-19: cohort study.",
"author": "Xie",
"doi-asserted-by": "publisher",
"journal-title": "BMJ",
"key": "ild230034r4",
"volume": "381",
"year": "2023"
},
{
"DOI": "10.1371/journal.pmed.1004194",
"article-title": "Prevalence and characteristics of long COVID in elderly patients: An observational cohort study of over 2 million adults in the US.",
"author": "Fung",
"doi-asserted-by": "publisher",
"issue": "4",
"journal-title": "PLoS Med",
"key": "ild230034r5",
"volume": "20",
"year": "2023"
},
{
"key": "ild230034r6",
"unstructured": "World Health Organization. A clinical case definition of post COVID-19 condition by a Delphi consensus. October 6, 2021. Accessed August 12, 2023. https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1"
}
],
"reference-count": 6,
"references-count": 6,
"relation": {},
"resource": {
"primary": {
"URL": "https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2811092"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Internal Medicine"
],
"subtitle": [],
"title": "Nirmatrelvir and Molnupiravir and Post–COVID-19 Condition in Older Patients",
"type": "journal-article"
}
fung2