A Randomised Phase II Trial in Early COVID-19, Assessing Use of Camostat by Blocking SARS-CoV-2 Spike Protein-initiated Membrane Fusion
et al., NCT04455815, SPIKE-1, NCT04455815, Mar 2022
{kind=link}
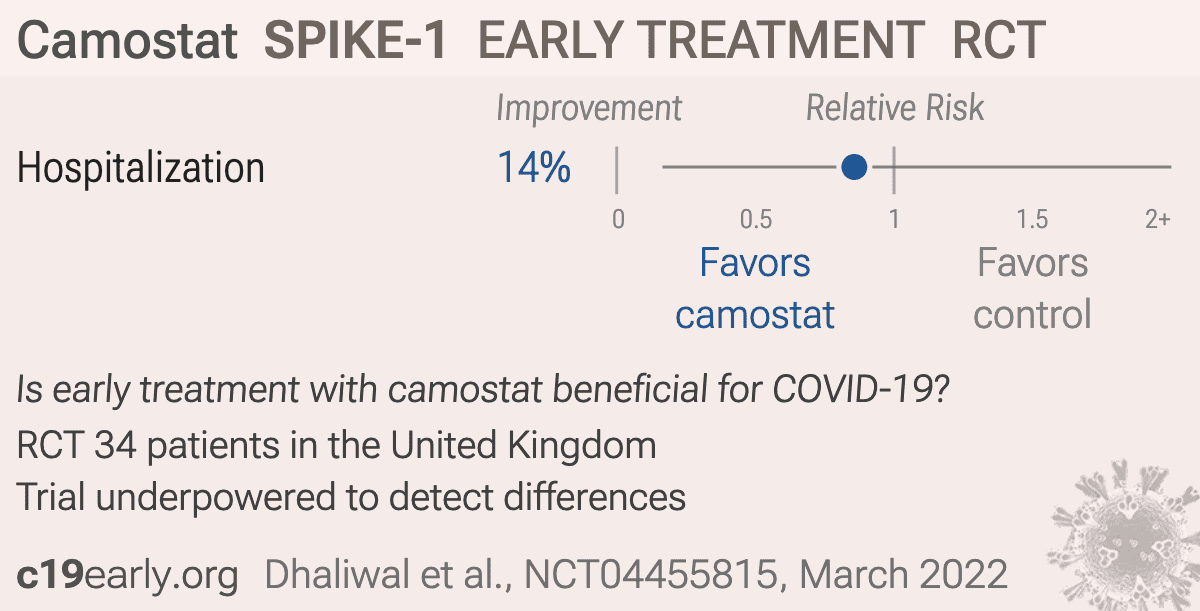
Early terminated RCT with 34 patients showing no significant differences with camostat treatment.
Standard of Care (SOC) for COVID-19 in the study country,
the United Kingdom, is very poor with very low average efficacy for approved treatments1.
The United Kingdom focused on expensive high-profit treatments, approving only one low-cost early treatment, which required a prescription and had limited adoption. The high-cost prescription treatment strategy reduces the probability of early treatment due to access and cost barriers, and eliminates complementary and synergistic benefits seen with many low-cost treatments.
Study covers TMPRSS2 inhibitors and camostat.
|
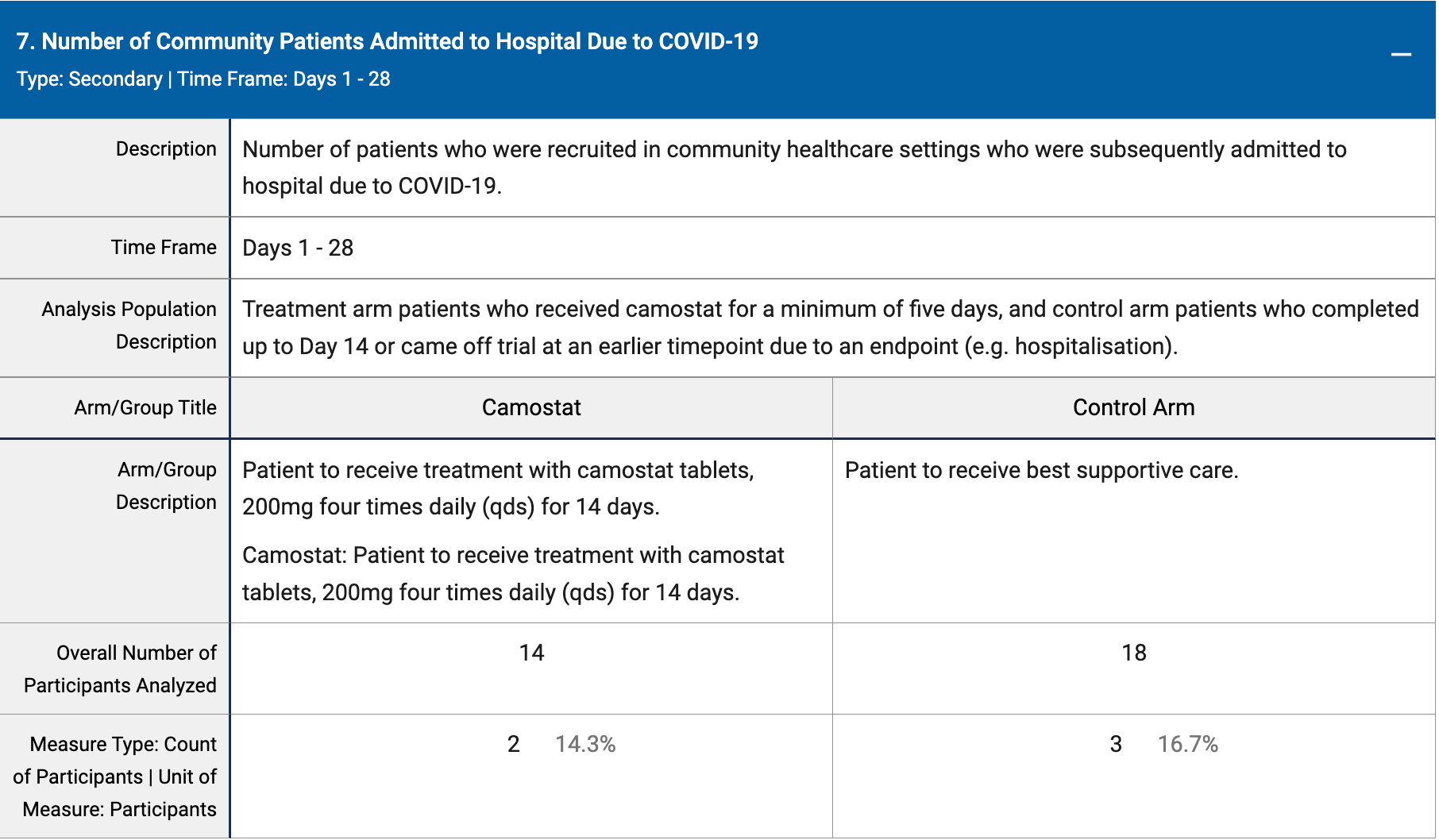
risk of hospitalization, 14.3% lower, RR 0.86, p = 1.00, treatment 2 of 14 (14.3%), control 3 of 18 (16.7%), NNT 42.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Dhaliwal et al., 3 Mar 2022, Randomized Controlled Trial, United Kingdom, preprint, 1 author, trial NCT04455815 (history) (SPIKE-1).
{kind=link}
dhaliwal