
Phase 3 Trial of Coronavir (Favipiravir) in Patients with Mild to Moderate COVID-19
et al., SSRN, doi:10.2139/ssrn.3696907, Oct 2020
{kind=link}
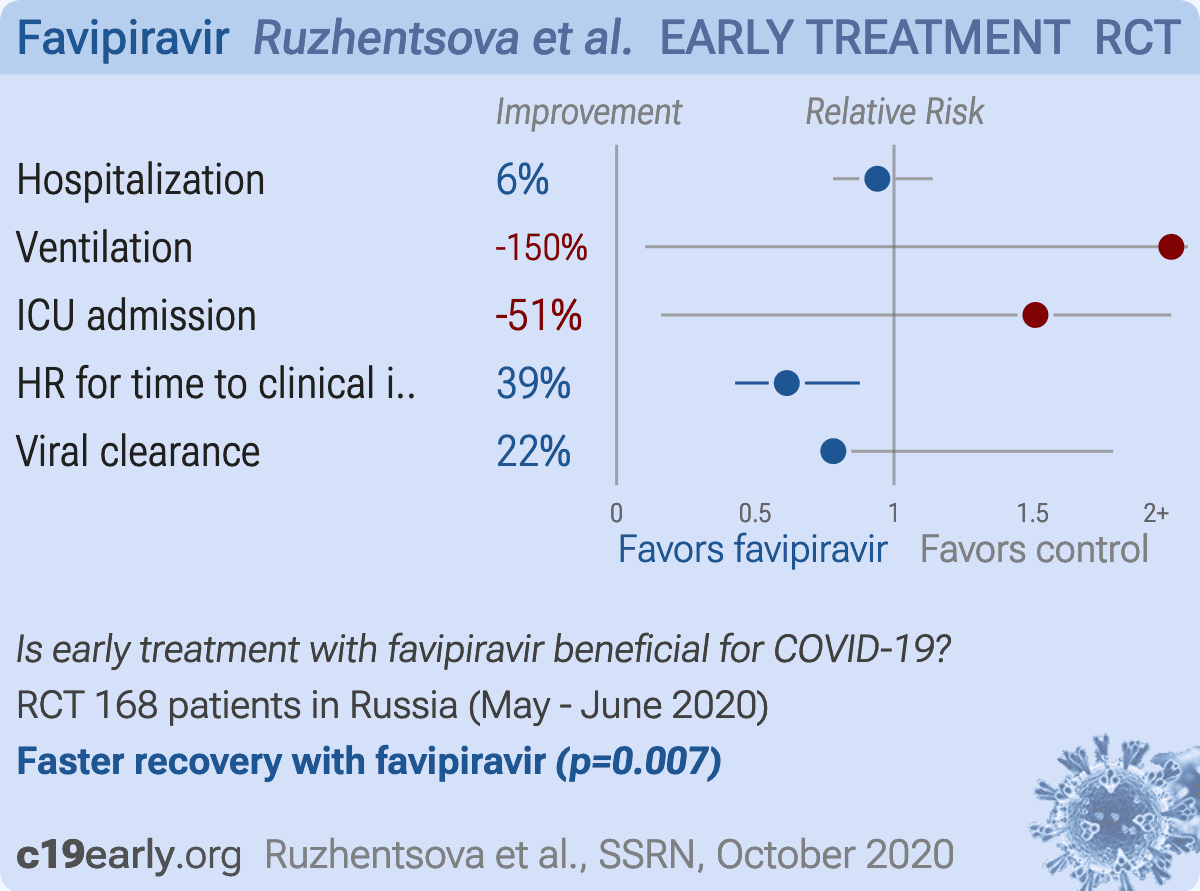
RCT 168 patients, 112 receiving favipiravir and 56 SOC, showing shorter time to clinical improvement and faster viral clearance with favipiravir.
Potential risks of favipiravir include kidney injury1-3, liver injury2-5, cardiovascular events5,6, pulmonary toxicity6,7, and mutagenicity, carcinogenicity, teratogenicity, embryotoxicity, and the creation of dangerous variants8-14.
|
risk of hospitalization, 6.0% lower, RR 0.94, p = 0.49, treatment 3 of 112 (2.7%), control 2 of 56 (3.6%), adjusted per study.
|
|
risk of mechanical ventilation, 150.0% higher, RR 2.50, p = 1.00, treatment 1 of 112 (0.9%), control 0 of 56 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm).
|
|
risk of ICU admission, 51.0% higher, RR 1.51, p = 0.63, treatment 3 of 112 (2.7%), control 1 of 56 (1.8%), adjusted per study.
|
|
HR for time to clinical improvement, 38.7% lower, HR 0.61, p = 0.007, treatment 112, control 56, inverted to make HR<1 favor treatment.
|
|
risk of no viral clearance, 21.9% lower, RR 0.78, p = 0.16, treatment 112, control 56, inverted to make RR<1 favor treatment, day 5 mid-recovery.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
1.
Abdulaziz et al., Clinical Features and Prognosis of Acute Kidney Injury in Hospital-Admitted Patients with COVID-19 in Egypt: A Single-Center Experience, Mansoura Medical Journal, doi:10.58775/2735-3990.1433.
2.
Ülger et al., Experimental evaluation of favipiravir (T-705)-induced liver and kidney toxicity in rats, Food and Chemical Toxicology, doi:10.1016/j.fct.2025.115472.
3.
El-Fetouh et al., Experimental Studies on Some Drugs Used in Covid-19 Treatment (Favipiravir and Dexamethasone) in Albino Rats, Journal of Advanced Veterinary Research, 13:10, www.advetresearch.com/index.php/AVR/article/view/1635.
4.
Almutairi et al., Liver Injury in Favipiravir-Treated COVID-19 Patients: Retrospective Single-Center Cohort Study, Tropical Medicine and Infectious Disease, doi:10.3390/tropicalmed8020129.
5.
Siby et al., Temporal Trends in Serious Adverse Events Associated with Oral Antivirals During the COVID-19 Pandemic: Insights from the FAERS Database (2020–2023), Open Forum Infectious Diseases, doi:10.1093/ofid/ofaf695.1825.
6.
Ozhan et al., Evaluation of the cardiopulmonary effects of repurposed COVID-19 therapeutics in healthy rats, Scientific Reports, doi:10.1038/s41598-025-31048-4.
7.
Ülger (B) et al., Evaluation of the effects of favipiravir (T-705) on the lung tissue of healty rats: An experimental study, Food and Chemical Toxicology, doi:10.1016/j.fct.2025.115235.
8.
Zhirnov et al., Favipiravir: the hidden threat of mutagenic action, Journal of microbiology, epidemiology and immunobiology, doi:10.36233/0372-9311-114.
9.
Waters et al., Human genetic risk of treatment with antiviral nucleoside analog drugs that induce lethal mutagenesis: the special case of molnupiravir, Environmental and Molecular Mutagenesis, doi:10.1002/em.22471.
10.
Hadj Hassine et al., Lethal Mutagenesis of RNA Viruses and Approved Drugs with Antiviral Mutagenic Activity, Viruses, doi:10.3390/v14040841.
11.
Shum, C., An investigational study into the drug-associated mutational signature in SARS-CoV-2 viruses, The University of Hong Kong, PhD Thesis, hub.hku.hk/handle/10722/344396.
12.
Shiraki et al., Convenient screening of the reproductive toxicity of favipiravir and antiviral drugs in Caenorhabditis elegans, Heliyon, doi:10.1016/j.heliyon.2024.e35331.
Ruzhentsova et al., 26 Oct 2020, Randomized Controlled Trial, Russia, preprint, 31 authors, study period 23 May, 2020 - 30 June, 2020, average treatment delay 3.55 days.
{kind=link}
Phase 3 Trial of Coronavir (Favipiravir) in patients with mild to moderate COVID-19
Background Favipiravir is an antiviral drug, an inhibitor of RNA dependent RNA polymerase that is preliminarily effective against SARS-CoV-2 virus. The aim of this study was to evaluate the efficacy and safety of favipiravir for treatment of mild to moderate coronavirus disease (COVID-19).
Methods We conducted an open-labeled, randomized, active-controlled multicenter trial of an oral dosage form of favipiravir in out-and hospitalized patients with mild to moderate COVID-19. The study was organized in 10 clinical centers in Russia. Eligible patients had laboratory confirmed by PCR test infection of SARS-CoV-2 and were aged 18-60 years. Patients were randomly assigned (in a 2:1 ratio) to receive either favipiravir (1800 mg BID on day 1, followed by 800 mg BID for up to 9 days), or standard of care (SOC) treatment (umifenovir + intranasal interferon alpha-2b, or hydroxychloroquine) for up to 10 days. Randomization was performed using a web-response system after stratification by COVID-19 severity, age and CT severity at enrollment. The coprimary outcomes were the time to clinical improvement and the time to viral clearance. An efficacy analysis was performed in intent-to-treat population. The safety population included all participants who received at least one dose of favipiravir or SOC. The trial is registered on ClinicalTrials.gov, identifier: NCT04501783. Findings Between May 23, 2020, and June 30, 2020, 190 patients were assessed for eligibility, of whom 168 were randomly assigned to receive either favipiravir (n = 112), or SOC (n = 56). The median time to clinical improvement was 6.0 (IQR 4•0; 9•3) days in favipiravir group and 10.0 (IQR 5•0; 21•0) days in SOC group; the median difference was 4 days (HR 1•63; 95% CI 1•14-2•34, p = 0•007). The statistically significant difference in the median time to viral clearance was observed only in the hospitalized cohort of patients: 3•0 (IQR 3•0; 3•0) vs. 5•0 (IQR 4•5; 5•5), respectively (HR 2•11; 95% CI 1•04-4•31; p = 0•038). However, the rate of viral elimination on Day 5 in the favipiravir group was significantly higher in the whole population: 81•2% vs. 67•9% respectively (RR 1•22; 05% CI 1•00-1•48; p = 0.022). The rate of clinical improvement on Day 7 in the favipiravir group was 1.5-fold higher compared to SOC: 52•7% vs. 35•8% (RR 1•50; 95% CI 1•02-2•22; p = 0•020). Favipiravir was well tolerated: most of the adverse events (AE) were mild. Any AEs were reported in 74•1% of patients in the favipiravir group vs. 60•0% in the SOC group. Among the most common adverse reactions was asymptomatic hyperuricemia, transient elevation of ALT & AST, and gastrointestinal disorders (diarrhea, nausea, abdominal pain). Interpretation Favipiravir was superior to SOC in shortening the time to clinical improvement in patients with mild to moderate COVID-19.
Favipiravir 3) and decreased oxygen saturation due to COVID-19 progression (gr. 3). § The difference was statistically significant (р < 0•0001). Table 3 : Adverse events of any cause that occurred in 5% or more patients in the Astreated population
References
Cai, Yang, Liu, Experimental Treatment with Favipiravir for COVID19: An Open-Label Control Study
Chen, Huang, Cheng, Favipiravir versus Arbidol for COVID-19: A Randomized Clinical Trial, MedRxiv
Delang, Abdelnabi, Neyts, Favipiravir as a potential countermeasure against neglected and emerging RNA viruses, Antiviral Res, doi:10.1016/j.antiviral.2018.03.003
Furuta, Gowen, Takahashi, Shiraki, Smee et al., Favipiravir (T-705), a novel viral RNA polymerase inhibitor, Antiviral Res, doi:10.1016/j.antiviral.2013.09.015
Furuta, Komeno, Nakamura, Favipiravir (T-705), a broad spectrum inhibitor of viral RNA polymerase, Proc Jpn Acad Ser B Phys Biol Sci, doi:10.2183/pjab.93.027
Furuta, Takahashi, Shiraki, T-705 (favipiravir) and related compounds: Novel broad-spectrum inhibitors of RNA viral infections, Antiviral Res, doi:10.1016/j.antiviral.2009.02.198
Liu, Letter to the Editor. Prolonged virus shedding even after seroconversion in a patient with COVID-19, Journal of Infection, doi:.org/10.1016/j.jinf.2020.03.063
Pmda, Avigan Tablet 200 mg
Tu, Chien, Yarmishyn, A Review of SARS-CoV-2 and the Ongoing Clinical Trials, Int J Mol Sci, doi:10.3390/ijms21072657
Wang, Cao, Zhang, Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro, Cell Res, doi:10.1038/s41422-020-0282-0
DOI record:
{
"DOI": "10.2139/ssrn.3696907",
"ISSN": [
"1556-5068"
],
"URL": "http://dx.doi.org/10.2139/ssrn.3696907",
"author": [
{
"affiliation": [],
"family": "Ruzhentsova",
"given": "Tatiana",
"sequence": "first"
},
{
"affiliation": [],
"family": "Chukhliaev",
"given": "Pavel",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Khavkina",
"given": "Daria",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Garbuzov",
"given": "Alexander",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Oseshnyuk",
"given": "Rodion",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Soluyanova",
"given": "Tatyana",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Shestakova",
"given": "Irina",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Vafin",
"given": "Adel",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Dmitrikova",
"given": "Elena Petrovna",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Mustafaev",
"given": "Dzhavanshir",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Domostroeva",
"given": "Tatyana",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Otpushchennikova",
"given": "Maria",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Pokrovsky",
"given": "Konstantin",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Markova",
"given": "Тatyana",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Kaplun",
"given": "Elena",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Petina",
"given": "Diana",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Rusanova",
"given": "Marina",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Bistritskiy",
"given": "Dmitriy",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Kostina",
"given": "Natalia",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Lesina",
"given": "Viсtoria",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Scherbak",
"given": "Sergey",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Agafina",
"given": "Alina",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Brook",
"given": "Yury",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Bronov",
"given": "Oleg",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Shults",
"given": "Evgeny",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Samsonov",
"given": "Mikhail",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Krasavina",
"given": "Emilia",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Zintchenko",
"given": "Arkadi",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Nikolskaya",
"given": "Maria",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Razzhivina",
"given": "Victoria",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Filon",
"given": "Olga",
"sequence": "additional"
}
],
"container-title": "SSRN Electronic Journal",
"container-title-short": "SSRN Journal",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2020,
10,
27
]
],
"date-time": "2020-10-27T12:04:55Z",
"timestamp": 1603800295000
},
"deposited": {
"date-parts": [
[
2020,
10,
27
]
],
"date-time": "2020-10-27T12:05:04Z",
"timestamp": 1603800304000
},
"indexed": {
"date-parts": [
[
2023,
8,
21
]
],
"date-time": "2023-08-21T12:29:46Z",
"timestamp": 1692620986171
},
"is-referenced-by-count": 6,
"issued": {
"date-parts": [
[
2020
]
]
},
"language": "en",
"member": "78",
"original-title": [],
"prefix": "10.2139",
"published": {
"date-parts": [
[
2020
]
]
},
"published-other": {
"date-parts": [
[
2020
]
]
},
"publisher": "Elsevier BV",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "https://www.ssrn.com/abstract=3696907"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subtitle": [],
"title": "Phase 3 Trial of Coronavir (Favipiravir) in Patients with Mild to Moderate COVID-19",
"type": "journal-article"
}