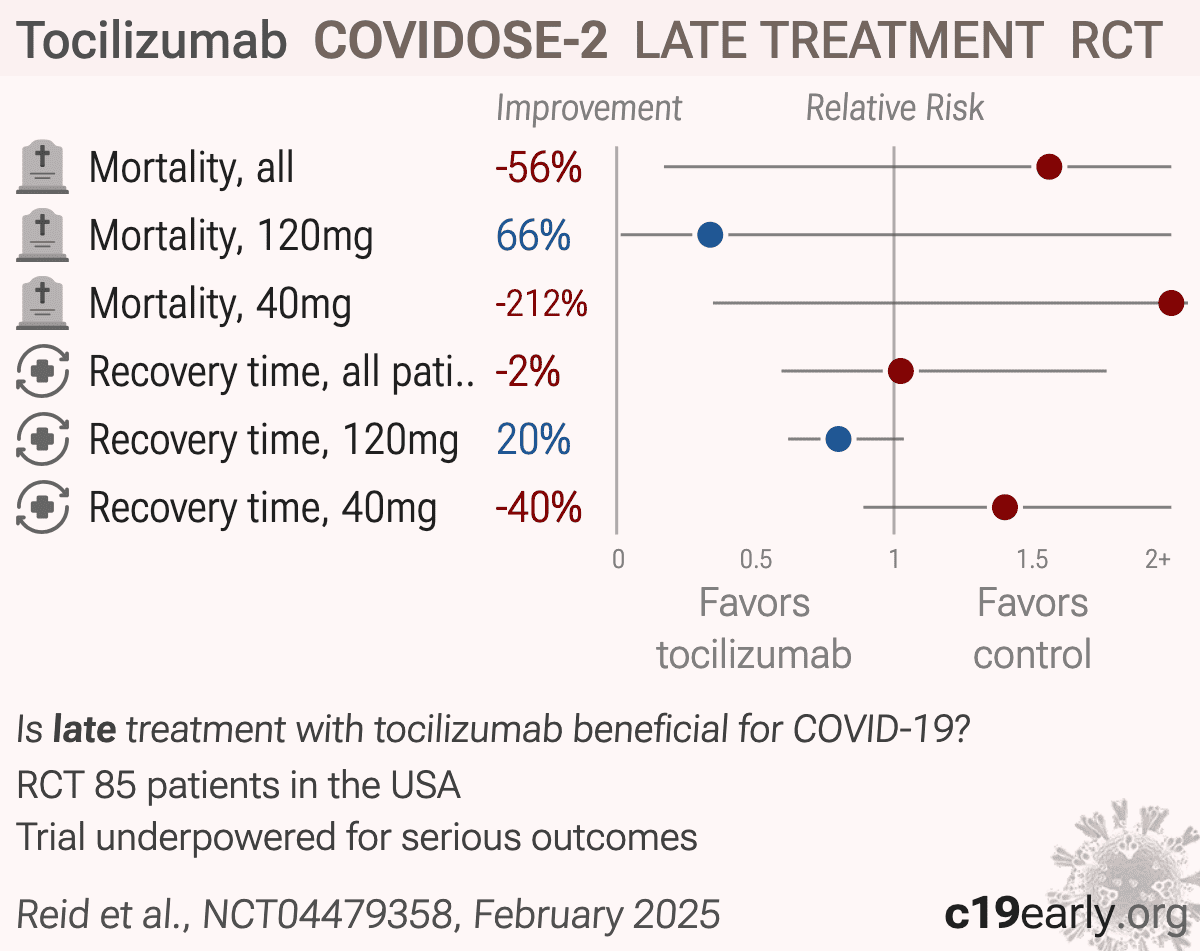
COVIDOSE-2: A Multi-center, Randomized, Controlled Phase 2 Trial Comparing Early Administration of Low-dose Tocilizumab to Standard of Care in Hospitalized Patients With COVID-19 Pneumonitis Not Requiring Invasive Ventilation
et al., NCT04479358, COVIDOSE-2, NCT04479358, Feb 2025
{kind=link}
RCT 85 patients in the USA showing no significant differences with tocilizumab treatment.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
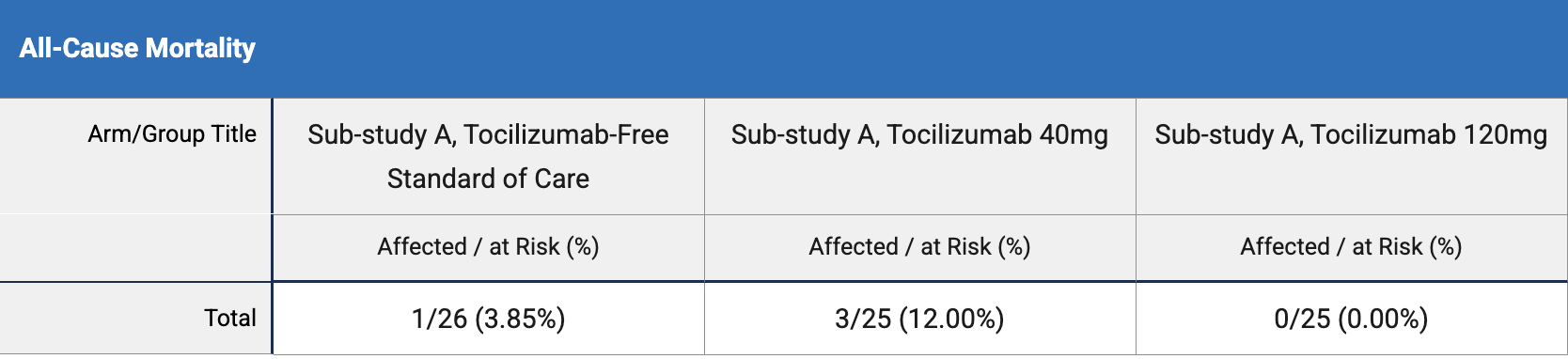
risk of death, 56.0% higher, RR 1.56, p = 1.00, treatment 3 of 50 (6.0%), control 1 of 26 (3.8%), all patients.
|
|
risk of death, 66.2% lower, RR 0.34, p = 1.00, treatment 0 of 25 (0.0%), control 1 of 26 (3.8%), NNT 26, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), 120mg.
|
|
risk of death, 212.0% higher, RR 3.12, p = 0.35, treatment 3 of 25 (12.0%), control 1 of 26 (3.8%), 40mg.
|
|
recovery time, 2.5% higher, relative time 1.02, p = 0.94, treatment 25, control 26, all patients.
|
|
recovery time, 20.0% lower, relative time 0.80, p = 0.09, treatment 4.0 [4.0-5.0] n=25, control 5.0 [4.0-6.0] n=26, 120mg.
|
|
recovery time, 40.0% higher, relative time 1.40, p = 0.15, treatment 7.0 [4.0-9.0] n=25, control 5.0 [4.0-6.0] n=26, 40mg.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Reid et al., 10 Feb 2025, Randomized Controlled Trial, USA, preprint, 1 author, trial NCT04479358 (history) (COVIDOSE-2).
Contact: pankti.reid@bsd.uchicago.edu.
{kind=link}
Late treatment
is less effective
is less effective
