Oral Nirmatrelvir–Ritonavir for Covid-19 in Higher-Risk Outpatients
et al., New England Journal of Medicine, doi:10.1056/NEJMoa2502457 (results released 9/10/2025), PANORAMIC, ISRCTN30448031, Sep 2025
{kind=link}
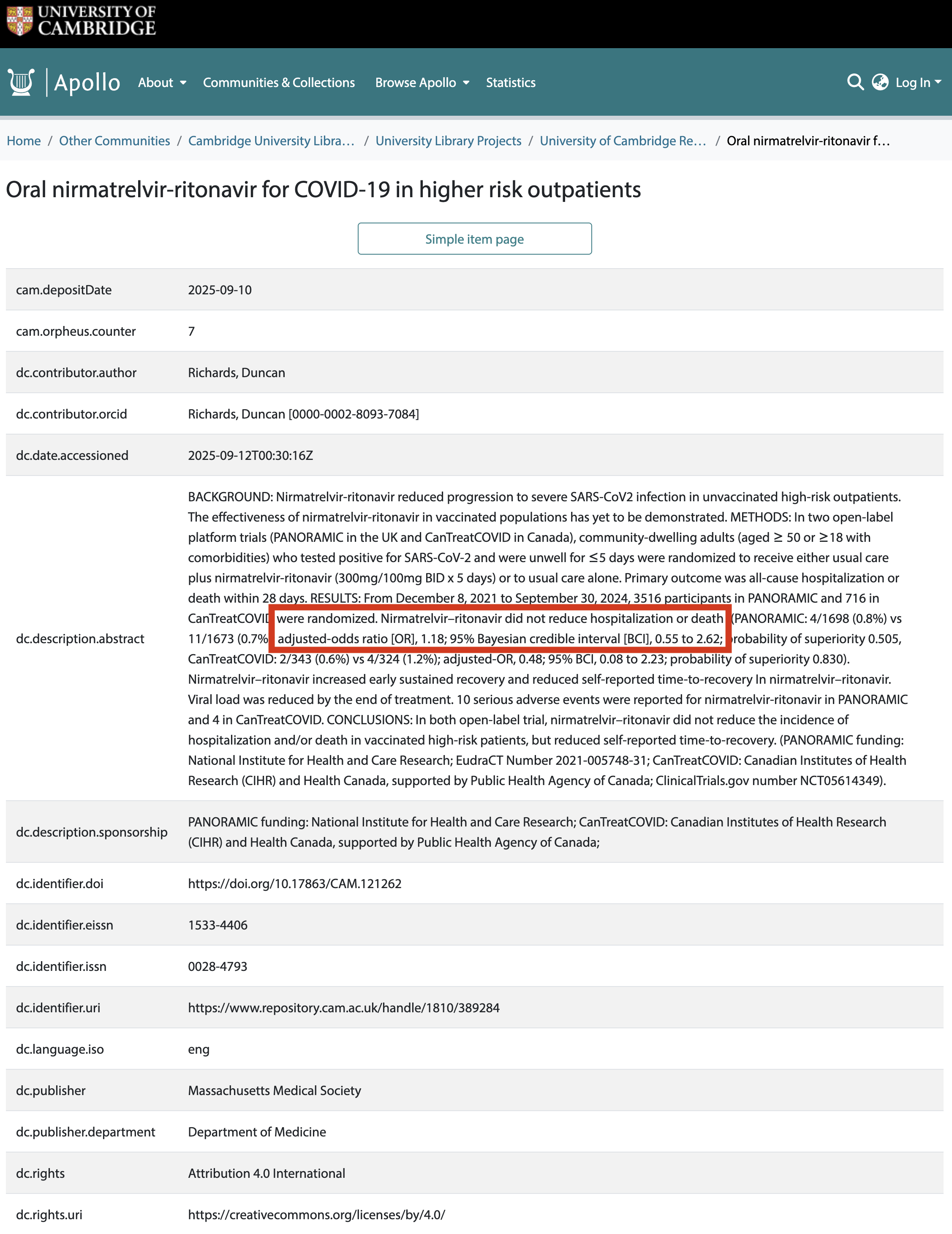
PANORAMIC/CanTreatCOVID results showing that paxlovid did not reduce hospitalization or death, adjusted OR 1.18, 95% Bayesian credible interval [0.55-2.62] for PANORAMIC and adjusted OR 0.48, 95% Bayesian credible interval [0.08-2.23] for CanTreatCOVID.
The results were first posted on the University of Cambridge Apollo repository on 9/10/2025 but were subsequently deleted and kept hidden until April 2026. Neither NEJM nor the trial teams responded to multiple requests regarding the suppression of these results. The accepted paper file is dated June 2025, and the database record shows NEJM acceptance 9/9/2025 and publication 9/12/2025. Recruitment for PANORAMIC ended March 28, 20241.
The study shows significantly faster recovery and viral clearance. Several factors points to a real effect, not just open-label bias as suggested by author Prof. Lee2:
1. The same PANORAMIC/PRINCIPLE open-label infrastructure found null recovery results for several other drugs.
2. The viral load reduction is objective and substantial. Participants in the treatment arm had ~87% lower viral load at day 5, i.e., there is an antiviral effect, and the recovery timing tracks the viral suppression timing.
3. Temporal results match pharmacology, not expectancy. The recovery HR is ~0.85 for days 1–2 (limited data), ~2.12 for days 3-7, and then tapers. Results match pharmacological expectations.
4. The symptom-by-symptom pattern matches pharmacological expectations. PANORAMIC data shows faster resolution for COVID symptoms (fever, cough, shortness of breath, fatigue, muscle ache) but slower resolution or more recurrence for known drug side effects (nausea OR 1.45, diarrhea OR 1.50).
5. Independent replication across continents. There were nearly identical relative effects in both trials despite the different location, team, and population. Shared cultural expectancy could in principle affect both, but trial-local biases are not expected to be the same.
6. Participants can't prospectively calibrate a proportional bias. A 33% faster recovery in both trials, despite very different absolute recovery times in each trial's control arm, would require participants to somehow sense their trial's baseline and shave a consistent proportion off. That's not how reporting bias works. An additive expectancy effect would produce different relative effects in the two trials; we don't see that.
7. The EPIC-SR "null" was partly an artifact of endpoint design - they combined COVID symptoms with known drug side effects (diarrhea, nausea, vomiting) in a weakest-link definition where any unresolved symptom means no recovery. EPIC-SR authors later broke it out per-symptom, showing faster resolution for 5/11 symptoms and a 2-day delay for diarrhea - they recommended "refining symptom end points to better differentiate between Covid-19 symptoms and adverse events." Further, Delta is very different from Omicron - Delta's greater lower-airway tropism may shift disease into anatomical compartments where the drug is less effective and into disease processes (established lower-airway pathology) where viral suppression alone is less beneficial. Treatment benefits may be maximized for replication-driven upper-airway disease and diminished once lower-airway involvement is established.
The hospitalization result rules out the EPIC-HR benefit, but is consistent with moderate benefit or harm. The lack of a clear benefit for hospitalization could be due to serious side effects and/or lower efficacy. For EPIC-HR, higher COVID-19 baseline risk may make drug harm proportionally smaller, while lower COVID-19 risk may reveal any drug-harm component.
Notably missing from the paper are any details about the hospitalizations (reasons, timing) which could help explain the results - for example, are they consistent with side effects of the drug, viral rebound, or other reasons? We note that an RCT does not match real-world use though, and likely does a much better job of excluding patients at DDI risk - i.e., real-world harm may be higher.
Many results are missing, including all long-term outcomes. Unreported
results include long-COVID/PASC outcomes, EQ-5D-5L analyses, economic evaluations,
PANORAMIC 3- and 6-month symptom/well-being and work/study-impact outcomes, CanTreatCOVID
day-90 and week-36 long-COVID outcomes, whole-genome-sequencing/resistance analyses, and
antibody-response analyses.
The authors and the journal did not respond to requests.
Standard of Care (SOC) for COVID-19 in the study country,
the United Kingdom, is very poor with very low average efficacy for approved treatments3.
The United Kingdom focused on expensive high-profit treatments, approving only one low-cost early treatment, which required a prescription and had limited adoption. The high-cost prescription treatment strategy reduces the probability of early treatment due to access and cost barriers, and eliminates complementary and synergistic benefits seen with many low-cost treatments.
|
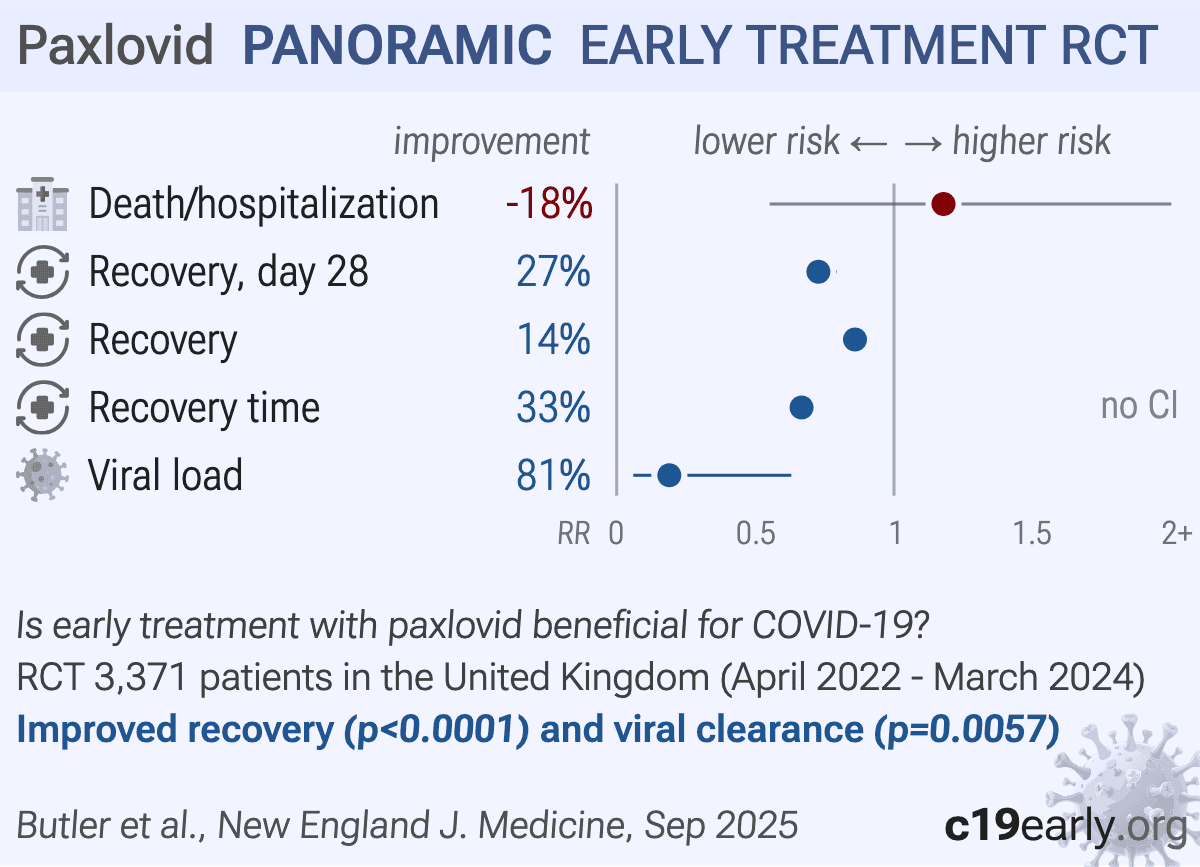
risk of death/hospitalization, 17.9% higher, RR 1.18, p = 0.69, treatment 14 of 1,698 (0.8%), control 11 of 1,673 (0.7%), odds ratio converted to relative risk, day 28.
|
|
risk of no recovery, 27.3% lower, RR 0.73, p < 0.001, treatment 543 of 1,690 (32.1%), control 727 of 1,646 (44.2%), NNT 8.3, day 28.
|
|
risk of no recovery, 14.1% lower, RR 0.86, p < 0.001, treatment 1,036 of 1,546 (67.0%), control 1,162 of 1,492 (77.9%), NNT 9.2, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, no early sustained recovery.
|
|
recovery time, 33.3% lower, relative time 0.67, treatment 1,698, control 1,673.
|
|
viral load, 81.0% lower, relative load 0.19, p = 0.006, treatment 1,698, control 1,673.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Butler et al., 10 Sep 2025, Randomized Controlled Trial, United Kingdom, peer-reviewed, 42 authors, study period 12 April, 2022 - 28 March, 2024, trial ISRCTN30448031 (PANORAMIC).
{kind=link}
Abstract: ## BACKGROUND
Nirmatrelvir-ritonavir has been shown to reduce progression to severe illness from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in unvaccinated highrisk outpatients. The effectiveness of nirmatrelvir-ritonavir in persons who have been vaccinated, infected naturally, or both is unclear.
METHODS
In two open-label platform trials (PANORAMIC in the United Kingdom and CanTreatCOVID in Canada), we enrolled higher-risk adults (≥50 years of age or ≥18 years of age with coexisting conditions) in the community who tested positive for SARS-CoV-2 and had been unwell for 5 days or less. The participants were randomly assigned to receive usual care plus nirmatrelvir (300 mg)-ritonavir (100 mg) twice a day for 5 days or to receive usual care alone. The primary outcome was hospitalization or death from any cause within 28 days after randomization.
RESULTS
From December 8, 2021, to September 30, 2024, a total of 3516 participants in the PANORAMIC trial and 716 participants in the CanTreatCOVID trial underwent randomization. In the PANORAMIC trial, 14 of 1698 participants (0.8%) in the nirmatrelvir-ritonavir group and 11 of 1673 participants (0.7%) in the usual-care group were hospitalized or died (adjusted odds ratio, 1.18; 95% Bayesian credible interval, 0.55 to 2.62; probability of superiority, 0.334). In the CanTreatCOVID trial, 2 of 343 participants (0.6%) in the nirmatrelvir-ritonavir group and 4 of 324 participants (1.2%) in the usual-care group were hospitalized or died (adjusted odds ratio, 0.48; 95% Bayesian credible interval, 0.08 to 2.23; probability of superiority, 0.830). In a substudy involving 634 participants, viral load was reduced by the end of treatment with nirmatrelvir-ritonavir. Serious adverse events with nirmatrelvir-ritonavir were reported in 9 participants in the PANORAMIC trial and in 4 participants in the CanTreatCOVID trial.
CONCLUSIONS
In two open-label trials, nirmatrelvir-ritonavir did not reduce the incidence of hospitalization or death among vaccinated higher-risk participants with SARS-CoV-2 infection. (Funded by the National Institute for Health and Care Research, and others; PANORAMIC ISRCTN number, 2021 - 005748 - 31; CanTreatCOVID ClinicalTrials.gov number, NCT05614349.)
Original Article
Oral Nirmatrelvir-Ritonavir for Covid-19 in Higher-Risk Outpatients
C.C. Butler, 1 A.D. Pinto, 2-5 V. Harris, 1 J. Holmes, 1 N.M. Rahman, 6-8 L. Cureton, 1 G. Hayward, 1 D.B. Richards, 9 D.M. Lowe, 10 J.F. Standing, 10 J. Breuer, 11 K. Hood, 12 M.E. Png, 1 S. Petrou, 1 J. Dorward, 1,13 M.G. Patel, 1 N.P.B. Thomas, 14-16 P. Evans, 14,17 N.D. Hart, 18 B.D. Jani, 19 B. Hosseini, 2,4,5 S. Murthy, 20 K. McBrien, 21,22 A. Condon, 23 E.G. McDonald, 24 P. Daley, 25 M. Greiver, 4,26 B.R. da Costa, 5,27 P. Selby, 4,5 P. Jüni, 5,27 T.C. Lee, 24 H. Shi, 28 M.A. Detry, 29 C.T. Saunders, 29 M. Fitzgerald, 29 N.S. Berry, 29 B.R. Saville, 29,30 S.H. Khoo, 31 J.S. Nguyen-Van-Tam, 32 F.D.R. Hobbs, 1 L.-M. Yu, 1 and P. Little, 33 for the PANORAMIC Trial and CanTreatCOVID Trial Collaborative Groups*
ABSTRACT
The authors' full names, academic degrees, and affiliations are listed at the end of the article. Christopher C. Butler can be contacted at christopher . butler@ phc . ox . ac . uk or at Nuffield Department of Primary Care Health Sciences, University of Oxford, Gibson Bldg., 1st Fl., Radcliffe Observatory Quarter, Woodstock Rd., Oxford, OX2 6GG, United..
DOI record:
{
"DOI": "10.1056/nejmoa2502457",
"ISSN": [
"0028-4793",
"1533-4406"
],
"URL": "http://dx.doi.org/10.1056/NEJMoa2502457",
"alternative-id": [
"10.1056/NEJMoa2502457"
],
"author": [
{
"ORCID": "https://orcid.org/0000-0002-0102-3453",
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"authenticated-orcid": false,
"family": "Butler",
"given": "Christopher C.",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Upstream Lab, MAP Centre for Urban Health Solutions, Li Ka Shing Knowledge Institute, Unity Health Toronto, Toronto"
},
{
"name": "Department of Family and Community Medicine, St. Michael’s Hospital, Toronto"
},
{
"name": "Department of Family and Community Medicine, Faculty of Medicine, University of Toronto, Toronto"
},
{
"name": "Dalla Lana School of Public Health, University of Toronto, Toronto"
}
],
"family": "Pinto",
"given": "Andrew D.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Harris",
"given": "Victoria",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Holmes",
"given": "Jane",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Respiratory Trials Unit, Nuffield, Department of Medicine, University of Oxford, Oxford, United Kingdom"
},
{
"name": "Oxford National Institute for Health and Care Research Biomedical Research Centre, Oxford, United Kingdom"
},
{
"name": "Chinese Academy of Medicine Oxford Institute, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Rahman",
"given": "Najib M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Cureton",
"given": "Lucy",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Hayward",
"given": "Gail",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Medicine, University of Cambridge, Cambridge, United Kingdom"
}
],
"family": "Richards",
"given": "Duncan B.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Institute of Immunity and Transplantation, University College London, London"
}
],
"family": "Lowe",
"given": "David M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Institute of Immunity and Transplantation, University College London, London"
}
],
"family": "Standing",
"given": "Joseph F.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Infection, Inflammation and Immunology, UCL Great Ormond Street Institute of Child Health, London"
}
],
"family": "Breuer",
"given": "Judith",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Centre for Trials Research, Cardiff University, Cardiff, United Kingdom"
}
],
"family": "Hood",
"given": "Kerenza",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Png",
"given": "May Ee",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Petrou",
"given": "Stavros",
"sequence": "additional"
},
{
"ORCID": "https://orcid.org/0000-0001-6072-1430",
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
},
{
"name": "Centre for the AIDS Programme of Research in South Africa (CAPRISA), Durban, South Africa"
}
],
"authenticated-orcid": false,
"family": "Dorward",
"given": "Jienchi",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Patel",
"given": "Mahendra G.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "National Institute Health and Care Research Delivery Network, London"
},
{
"name": "Windrush Medical Practice, Witney, United Kingdom"
},
{
"name": "Royal College of General Practitioners, London"
}
],
"family": "Thomas",
"given": "Nicholas P.B.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "National Institute Health and Care Research Delivery Network, London"
},
{
"name": "Faculty of Health and Life Sciences, University of Exeter, Exeter, United Kingdom"
}
],
"family": "Evans",
"given": "Philip",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "School of Medicine, Dentistry and Biomedical Sciences, Queen’s University Belfast, United Kingdom"
}
],
"family": "Hart",
"given": "Nigel D.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "General Practice and Primary Care, School of Health and Wellbeing, MVLS, University of Glasgow, Glasgow, United Kingdom"
}
],
"family": "Jani",
"given": "Bhautesh D.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Upstream Lab, MAP Centre for Urban Health Solutions, Li Ka Shing Knowledge Institute, Unity Health Toronto, Toronto"
},
{
"name": "Department of Family and Community Medicine, Faculty of Medicine, University of Toronto, Toronto"
},
{
"name": "Dalla Lana School of Public Health, University of Toronto, Toronto"
}
],
"family": "Hosseini",
"given": "Banafshe",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Faculty of Medicine, University of British Columbia, Vancouver, Canada"
}
],
"family": "Murthy",
"given": "Srinivas",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Family Medicine, University of Calgary, Calgary, AB, Canada"
},
{
"name": "Department of Community Health Sciences, University of Calgary, Calgary, AB, Canada"
}
],
"family": "McBrien",
"given": "Kerry",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Family Medicine, Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Canada"
}
],
"family": "Condon",
"given": "Amanda",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Medicine, Faculty of Medicine and Health Sciences, McGill University, Montreal"
}
],
"family": "McDonald",
"given": "Emily G.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Memorial University of Newfoundland, St. John’s, Canada"
}
],
"family": "Daley",
"given": "Peter",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Family and Community Medicine, Faculty of Medicine, University of Toronto, Toronto"
},
{
"name": "Department of Family and Community Medicine, North York General Hospital, Toronto"
}
],
"family": "Greiver",
"given": "Michelle",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Dalla Lana School of Public Health, University of Toronto, Toronto"
},
{
"name": "Clinical Trial Service Unit and Epidemiological Studies Unit, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom"
}
],
"family": "da Costa",
"given": "Bruno R.",
"sequence": "additional"
},
{
"ORCID": "https://orcid.org/0000-0001-5401-2996",
"affiliation": [
{
"name": "Department of Family and Community Medicine, Faculty of Medicine, University of Toronto, Toronto"
},
{
"name": "Dalla Lana School of Public Health, University of Toronto, Toronto"
}
],
"authenticated-orcid": false,
"family": "Selby",
"given": "Peter",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Dalla Lana School of Public Health, University of Toronto, Toronto"
},
{
"name": "Clinical Trial Service Unit and Epidemiological Studies Unit, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Jüni",
"given": "Peter",
"sequence": "additional"
},
{
"ORCID": "https://orcid.org/0000-0002-2267-4239",
"affiliation": [
{
"name": "Department of Medicine, Faculty of Medicine and Health Sciences, McGill University, Montreal"
}
],
"authenticated-orcid": false,
"family": "Lee",
"given": "Todd C.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Statistics and Actuarial Science, Simon Fraser University, Burnaby, BC, Canada"
}
],
"family": "Shi",
"given": "Haolun",
"sequence": "additional"
},
{
"ORCID": "https://orcid.org/0000-0002-2794-1439",
"affiliation": [
{
"name": "Berry Consultants, Austin, TX"
}
],
"authenticated-orcid": false,
"family": "Detry",
"given": "Michelle A.",
"sequence": "additional"
},
{
"ORCID": "https://orcid.org/0000-0003-4325-9568",
"affiliation": [
{
"name": "Berry Consultants, Austin, TX"
}
],
"authenticated-orcid": false,
"family": "Saunders",
"given": "Christina T.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Berry Consultants, Austin, TX"
}
],
"family": "Fitzgerald",
"given": "Mark",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Berry Consultants, Austin, TX"
}
],
"family": "Berry",
"given": "Nicholas S.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Berry Consultants, Austin, TX"
},
{
"name": "Department of Biostatistics, Vanderbilt University School of Medicine, Nashville"
}
],
"family": "Saville",
"given": "Benjamin R.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Centre for Experimental Therapeutics, University of Liverpool, Liverpool, United Kingdom"
}
],
"family": "Khoo",
"given": "Saye H.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Lifespan and Population Health Unit, University of Nottingham School of Medicine, Nottingham, United Kingdom"
}
],
"family": "Nguyen-Van-Tam",
"given": "Jonathan S.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Hobbs",
"given": "F.D. Richard",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom"
}
],
"family": "Yu",
"given": "Ly-Mee",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Primary Care Research Centre, University of Southampton, Southampton, United Kingdom"
}
],
"family": "Little",
"given": "Paul",
"sequence": "additional"
}
],
"container-title": "New England Journal of Medicine",
"container-title-short": "N Engl J Med",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2026,
4,
22
]
],
"date-time": "2026-04-22T21:00:23Z",
"timestamp": 1776891623000
},
"deposited": {
"date-parts": [
[
2026,
4,
22
]
],
"date-time": "2026-04-22T21:00:45Z",
"timestamp": 1776891645000
},
"funder": [
{
"DOI": "10.13039/501100000024",
"doi-asserted-by": "publisher",
"id": [
{
"asserted-by": "publisher",
"id": "10.13039/501100000024",
"id-type": "DOI"
}
],
"name": "Canadian Institutes of Health Research"
},
{
"DOI": "10.13039/501100000276",
"doi-asserted-by": "publisher",
"id": [
{
"asserted-by": "publisher",
"id": "10.13039/501100000276",
"id-type": "DOI"
}
],
"name": "National Institute for Health and Care Research"
}
],
"indexed": {
"date-parts": [
[
2026,
4,
22
]
],
"date-time": "2026-04-22T21:40:09Z",
"timestamp": 1776894009980,
"version": "3.51.2"
},
"is-referenced-by-count": 0,
"issue": "16",
"issued": {
"date-parts": [
[
2026,
4,
23
]
]
},
"journal-issue": {
"issue": "16",
"published-print": {
"date-parts": [
[
2026,
4,
23
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://www.nejmgroup.org/legal/terms-of-use.htm",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2026,
4,
23
]
],
"date-time": "2026-04-23T00:00:00Z",
"timestamp": 1776902400000
}
}
],
"link": [
{
"URL": "http://www.nejm.org/doi/pdf/10.1056/NEJMoa2502457",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "150",
"original-title": [],
"page": "1583-1594",
"prefix": "10.1056",
"published": {
"date-parts": [
[
2026,
4,
23
]
]
},
"published-print": {
"date-parts": [
[
2026,
4,
23
]
]
},
"publisher": "Massachusetts Medical Society",
"reference": [
{
"key": "e_1_3_4_2_2",
"unstructured": "World Health Organization. COVID-19 epidemiological update — 17 September 2024 (https://www.who.int/publications/m/item/covid-19-epidemiological-update-edition-171)."
},
{
"DOI": "10.1056/NEJMoa2118542",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_3_2"
},
{
"DOI": "10.1126/science.abl4784",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_4_2"
},
{
"key": "e_1_3_4_5_2",
"unstructured": "National Institute for Health and Care Excellence (NICE). Nirmatrelvir plus ritonavir sotrovimab and tocilizumab for treating COVID-19. Technology appraisal guidance no. TA878. February 26 2026 (https://www.nice.org.uk/guidance/ta878/chapter/1-Recommendations)."
},
{
"DOI": "10.1093/jac/dkae163",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_6_2"
},
{
"DOI": "10.1093/jac/dkac437",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_7_2"
},
{
"key": "e_1_3_4_8_2",
"unstructured": "Bhimraj A Falck-Ytter Y Baden LR et al. IDSA guidelines on the treatment and management of patients with COVID-19. Arlington VA: Infectious Diseases Society of America October 14 2025 (https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/)."
},
{
"DOI": "10.1056/NEJMoa2309003",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_9_2"
},
{
"article-title": "Nirmatrelvir combined with ritonavir for preventing and treating COVID-19.",
"author": "Reis S",
"first-page": "CD015395",
"journal-title": "Cochrane Database Syst Rev",
"key": "e_1_3_4_10_2",
"unstructured": "Reis S, Metzendorf MI, Kuehn R, et al. Nirmatrelvir combined with ritonavir for preventing and treating COVID-19. Cochrane Database Syst Rev 2023;11:CD015395-CD015395.38032024",
"volume": "11",
"year": "2023"
},
{
"DOI": "10.1136/bmjopen-2022-069176",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_11_2"
},
{
"DOI": "10.1016/S0140-6736(22)02597-1",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_12_2"
},
{
"key": "e_1_3_4_13_2",
"unstructured": "Hosseini B Condon A da Costa BR et al. Canadian Adaptive Platform Trial of Treatments for COVID in Community Settings (CanTreatCOVID): protocol for a randomised controlled adaptive platform trial of treatments for acute SARS-CoV-2 infection in community settings. BMJ Open 2025;15(8):e097134-e097134.40754325"
},
{
"DOI": "10.1016/S2213-2600(21)00310-6",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_14_2"
},
{
"DOI": "10.1016/S0140-6736(21)00461-X",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_15_2"
},
{
"DOI": "10.1016/j.jinf.2024.106130",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_16_2"
},
{
"DOI": "10.3399/BJGP.2022.0083",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_17_2"
},
{
"DOI": "10.1016/S0140-6736(21)01744-X",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_18_2"
},
{
"DOI": "10.1016/j.jinf.2024.106248",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_19_2"
},
{
"DOI": "10.1038/s41598-025-09275-6",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_20_2"
},
{
"DOI": "10.1093/cid/ciae551",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_21_2"
},
{
"DOI": "10.1016/j.jclinepi.2008.12.011",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_22_2"
},
{
"DOI": "10.1056/NEJMra1510059",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_23_2"
},
{
"DOI": "10.1001/jama.287.5.622",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_24_2"
},
{
"DOI": "10.12688/f1000research.17611.2",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_25_2"
},
{
"DOI": "10.1186/s12879-023-08835-3",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_26_2"
},
{
"DOI": "10.1016/S1473-3099(21)00705-2",
"doi-asserted-by": "publisher",
"key": "e_1_3_4_27_2"
}
],
"reference-count": 26,
"references-count": 26,
"relation": {},
"resource": {
"primary": {
"URL": "http://www.nejm.org/doi/10.1056/NEJMoa2502457"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [],
"subtitle": [],
"title": "Oral Nirmatrelvir–Ritonavir for Covid-19 in Higher-Risk Outpatients",
"type": "journal-article",
"volume": "394"
}