
A Study of Immune System Proteins in Participants With Mild to Moderate COVID-19 Illness
, NCT04634409, NCT04634409, Feb 2022
{kind=link}
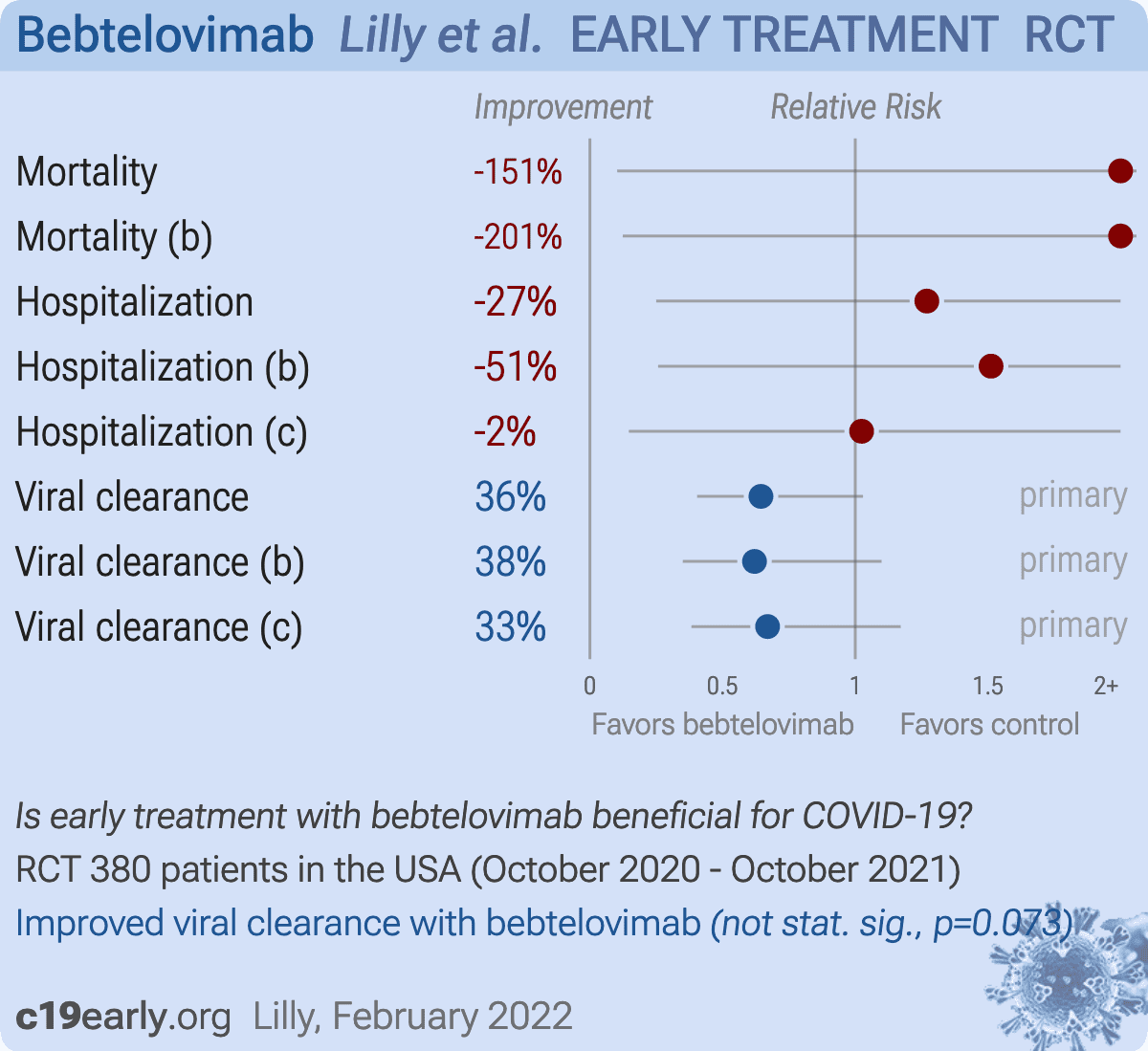
RCT with 127 bamlanivimab, etesevimab, and bebtelovimab patients, 125 bebtelovimab patients, and 128 control patients, showing no significant differences in hospitalization and mortality. Viral clearance was improved although not statistically significant. NCT04634409 (history).
Efficacy is variant dependent. In Vitro research suggests a lack of efficacy for omicron BQ.1.11, BA.5, BA.2.75, XBB2,3, XBB.1.5, XBB.1.9.13.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments4.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of death, 150.8% higher, RR 2.51, p = 1.00, treatment 1 of 252 (0.4%), control 0 of 128 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), combined bebtelovimab arms.
|
|
risk of death, 200.8% higher, RR 3.01, p = 0.50, treatment 1 of 127 (0.8%), control 0 of 128 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), bamlanivimab, etesevimab, and bebtelovimab.
|
|
risk of hospitalization, 27.0% higher, RR 1.27, p = 1.00, treatment 5 of 252 (2.0%), control 2 of 128 (1.6%), combined bebtelovimab arms.
|
|
risk of hospitalization, 51.2% higher, RR 1.51, p = 0.68, treatment 3 of 127 (2.4%), control 2 of 128 (1.6%), bamlanivimab, etesevimab, and bebtelovimab.
|
|
risk of hospitalization, 2.4% higher, RR 1.02, p = 1.00, treatment 2 of 125 (1.6%), control 2 of 128 (1.6%), bebtelovimab.
|
|
risk of no viral clearance, 35.5% lower, RR 0.64, p = 0.07, treatment 33 of 252 (13.1%), control 26 of 128 (20.3%), NNT 14, day 7 persistently high viral load, combined bebtelovimab arms, primary outcome.
|
|
risk of no viral clearance, 38.0% lower, RR 0.62, p = 0.13, treatment 16 of 127 (12.6%), control 26 of 128 (20.3%), NNT 13, day 7 persistently high viral load, bamlanivimab, etesevimab, and bebtelovimab, primary outcome.
|
|
risk of no viral clearance, 33.0% lower, RR 0.67, p = 0.18, treatment 17 of 125 (13.6%), control 26 of 128 (20.3%), NNT 15, day 7 persistently high viral load, bebtelovimab, primary outcome.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
1.
Planas et al., Resistance of Omicron subvariants BA.2.75.2, BA.4.6 and BQ.1.1 to neutralizing antibodies, bioRxiv, doi:10.1101/2022.11.17.516888.
2.
Haars et al., Prevalence of SARS-CoV-2 Omicron Sublineages and Spike Protein Mutations Conferring Resistance against Monoclonal Antibodies in a Swedish Cohort during 2022–2023, Microorganisms, doi:10.3390/microorganisms11102417.
Lilly et al., 12 Feb 2022, Randomized Controlled Trial, USA, preprint, 1 author, study period 29 October, 2020 - 18 October, 2021, average treatment delay 3.6 days, trial NCT04634409 (history).
{kind=link}
FACT SHEET FOR HEALTHCARE PROVIDERS: EMERGENCY USE AUTHORIZATION FOR BEBTELOVIMAB HIGHLIGHTS OF EMERGENCY USE AUTHORIZATION (EUA) These highlights of the EUA do not include all the information needed to use BEBTELOVIMAB under the EUA. See the FULL FACT SHEET FOR HEALTHCARE PROVIDERS for BEBTELOVIMAB. BEBTELOVIMAB injection for intravenous use Original EUA Authorized Date: 02/2022
The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for the emergency use of bebtelovimab for the treatment of mild-to-moderate coronavirus disease 2019 in adults and pediatric patients (12 years of age and older weighing at least 40 kg): • with positive results of direct SARS-CoV-2 viral testing, and • who are at high risk for progression to severe COVID-19, including hospitalization or death, and • for whom alternative COVID-19 treatment options approved or authorized by FDA are not accessible or clinically appropriate. (14.4) LIMITATIONS OF AUTHORIZED USE • Bebtelovimab is not authorized for treatment of mild-to-moderate COVID-19 in geographic regions where infection is likely to have been caused by a non-susceptible SARS-CoV-2 variant based on available information including variant susceptibility to this drug and regional variant frequency. o FDA will monitor conditions to determine whether use in a geographic region is consistent with this scope of authorization, referring to available information, including information on variant susceptibility, and CDC regional variant frequency data available at: https://covid.cdc.gov/covid-data-tracker/#variant-proportions. (12.4) o FDA's determination and any updates will be available at: https://www.fda.gov/emergency-preparedness-andresponse/mcm-legal-regulatory-and-policy-framework/emergencyuse-authorization#coviddrugs • Bebtelovimab is not authorized for use in patients who: o are hospitalized due to COVID-19, OR o require oxygen therapy and/or respiratory support due to COVID-19, OR o require an increase in baseline oxygen flow rate and/or respiratory support due to COVID-19 and are on chronic oxygen therapy and/or respiratory support due to underlying non-COVID-19 related comorbidity. Bebtelovimab is not approved for any use, including for use as treatment of COVID-19. (1) * Sections or subsections omitted from the EUA are not listed