Efficacy and Safety of Fixed Combination of Hydroxychloroquine with Azithromycin Versus Hydroxychloroquine and Placebo in Patients with Mild COVID-19: Randomized, double blind, Placebo controlled trial
et al., medRxiv, doi:10.1101/2022.04.06.22273531, NCT04964583, Apr 2022
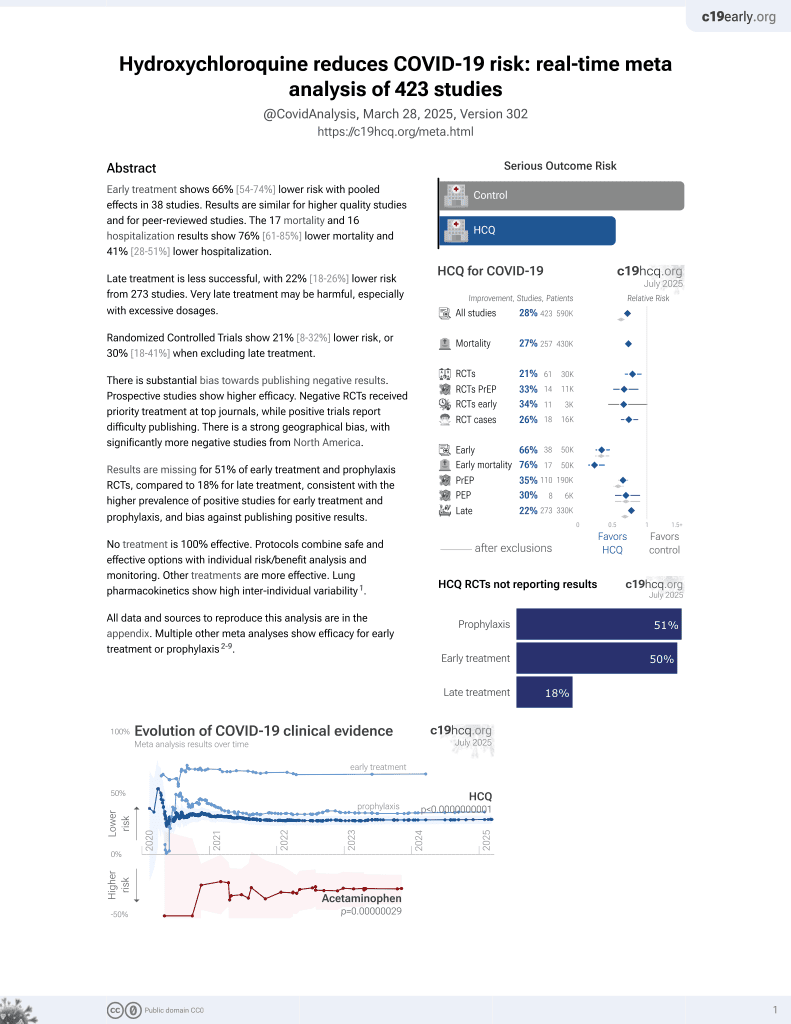
HCQ for COVID-19
1st treatment shown to reduce risk in
March 2020, now with p < 0.00000000001 from 424 studies, used in 59 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
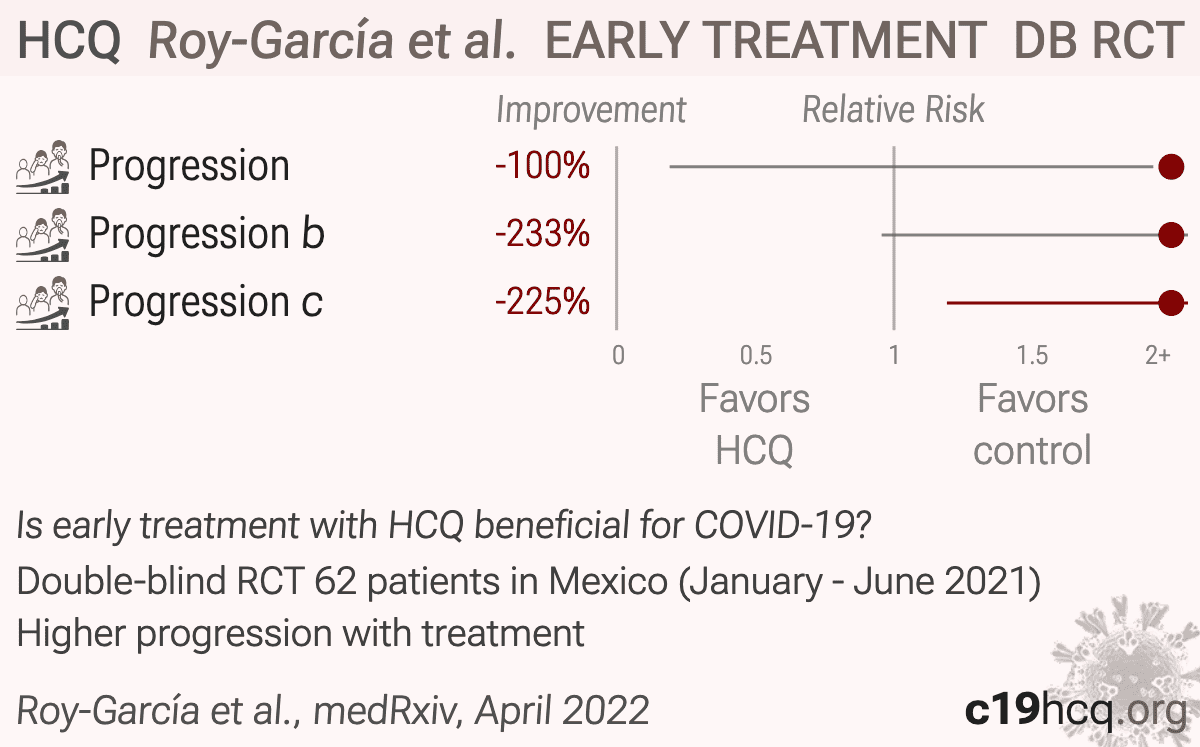
Small early terminated RCT in Mexico with 31 HCQ and 31 control patients, showing higher progression with treatment. There were no hospitalizations in the HCQ and control groups. HCQ patients were older, 38 vs. 32. There were no differences in QT segment duration and no cardiovascular complications.
This paper contains multiple data issues, protocol violations, and other issues:
Outcomes changed: the main conclusion is from outcomes (disease progression, pneumonia, supplemental oxygen) that were not pre-registered. The registered outcomes were hospitalization, viral load, and adverse events. Viral load was not reported, only clearance.
Outcomes reported for patients withdrawing consent: authors report that 6 participants were excluded in the per-protocol analysis (4 for withdrawing consent in the HCQ+AZT group, 1 for medication error, and 1 for withdrawing consent in the HCQ group). However, the efficacy outcomes in Table 3 use the originally randomized denominators. It is not clear how outcome data was obtained for patients that withdrew consent.
Retrospective registration presented as prospective: enrollment began 20 Jan 2021, but the trial was not registered until June 25, 2021. Both papers state it "was registered" while claiming Helsinki/CONSORT compliance, without disclosing that registration was retrospective.
Enrollment period differs between versions: the preprint claims enrollment January-June 2021 (with registration likely after enrollment ended), while the journal version has changed this to January-August 2021 without explanation, while the number of patients did not change.
Third site data missing: the registration shows three sites but the paper reports only two, without explanation.
Severity: the baseline oxygenation data does not match the "mild" claim: the median SpO₂ was only 94% (IQR 93-96). The CDC severe-illness cutoff is <94% on room air1. Therefore at least 25% and potentially close to 50% of patients were actually severe at baseline according to the CDC definition.
Unreported baseline radiograph results: the study performed chest radiography at baseline and day 11, and pneumonia was a key component of the disease-progression endpoint. However, baseline radiograph findings are not reported, and the paper does not state whether pneumonia outcomes were incident, worsening, or prevalent cases detected during follow-up.
Impossible CONSORT diagram: the published flow diagram shows all three arms "received allocated intervention (n=31)," which sums to 93 (not 92) and assigns 31 patients to an arm that randomized only 30.
Unreconciled reporting numbers: day-11 PCR percentages imply denominators that don't match the stated missing-data footnote, and the adverse-event table column totals don't sum in the two active arms (off by 3 and 2; placebo reconciles).
Authors specifically note that early treatment may be required to show benefit, yet they perform no analysis by treatment delay and the logistic regression for pneumonia does not include treatment delay. It is possible that many of the progressions were in patients that had very late treatment more than 5 days from onset.
No maximum time from onset - there was no maximum delay from symptom onset, which is inconsistent with the authors belief that early treatment may be necessary. Patients that progressed could have had unlimited time from symptom onset.
Selective edits between versions: number-needed-to-harm/treat metrics, a vaccination-status eligibility criterion, and parts of the exclusion list and sample-size method present in the preprint were dropped or changed in the published version without explanation.
Severity mismatch: the registry describes mild-to-moderate disease ("study focuses on characterizing the possible synergy of the fixed combination of hydroxychloroquine associated with azithromycin in the treatment of Covid-19 from mild to moderate manifestations"), while the papers only mention mild disease. The criterion of NEWS ≤4 could include patients that would be considered moderate under many COVID severity frameworks. As above, many patients were actually severe according to the CDC definition.
Inconsistencies: the pneumonia CI lower bound was reported as both 1.01 and 1.10. The age range is reported as 18-75 in the registry and 18-76 in the papers.
The placebo group had a median age of 32 years, whereas the HCQ+AZT group was markedly older with a median age of 41 years, and the HCQ group had a median age of 38, however adjusted results are only provided for pneumonia.
Pneumonia outcome not clear: radiographs were taken at baseline and day 11, and pneumonia is used as a component of disease progression, but the paper does not clearly state whether pneumonia means new pneumonia after randomization, worsening pneumonia, or any pneumonia detected during follow-up.
Blinding integrity is not clearly establised, for example the HCQ+AZ arm had a different pill regimen.
Primary-outcome window changed: registered as 15 days, reported as 21 days, with no amendment noted.
Masking discrepancy: registered as quadruple-blind; described as double-blind in both papers.
The dosing regimen is poor. Dosing studies and HCQ trials show that a loading dose is beneficial to reach therapeutic concentrations quickly2,3, and that excessive cumulative doses over time may be harmful, especially with late stage patients.
Uninformative primary endpoint: the pre-specified primary outcome (hospitalization) had only 2 events total. The trial was stopped early and was underpowered for its own primary question.
With the already late treatment (IQR 4-6 days for the HCQ arm) and non-weight-specific dosing, therapeutic concentrations may not be reached early enough during the viral phase in most patients, and the continued treatment for 10 days suggests that potentially harmful tissue concentrations could be reached for some patients.
Inappropriate sample size calculation: authors claim the sample size was powered for "an expected difference of 40% in the clinical response". However, their registered primary outcome is hospitalization and the baseline hospitalization rate was only 2.2%. The sample size calculation does not match the primary endpoint.
Hospitalizations are classified as “lost to follow-up” in the CONSORT diagram, however hospitalization was the primary outcome.
Post-hoc p-value hacking. Table 3 reframes the comparison as placebo versus pooled active treatment for progression and pneumonia. This post-hoc pooling was not part of the stated three-arm parallel design and is the reason that authors were able to achieve a significant p-value. It also combines HCQ+AZT and HCQ despite different regimens and different effects across endpoints.
Table 2 shows identical values for lymphocytes for all three groups (1.2 ± 0.4).
The abstract and Table 3 show 3/31 = 9.6%, which should be 9.7%.
Table 5 appears to treat “n (%)” as a fraction of total adverse-event entries rather than participants, but this is not clear in the table labeling and may be misleading. The sum is correct for placebo but not for the active groups.
Results for the desaturation and dyspnea components of the progression outcome are not provided.
This study is excluded in the after exclusion results of meta-analysis:
multiple data issues - pending author response.
|
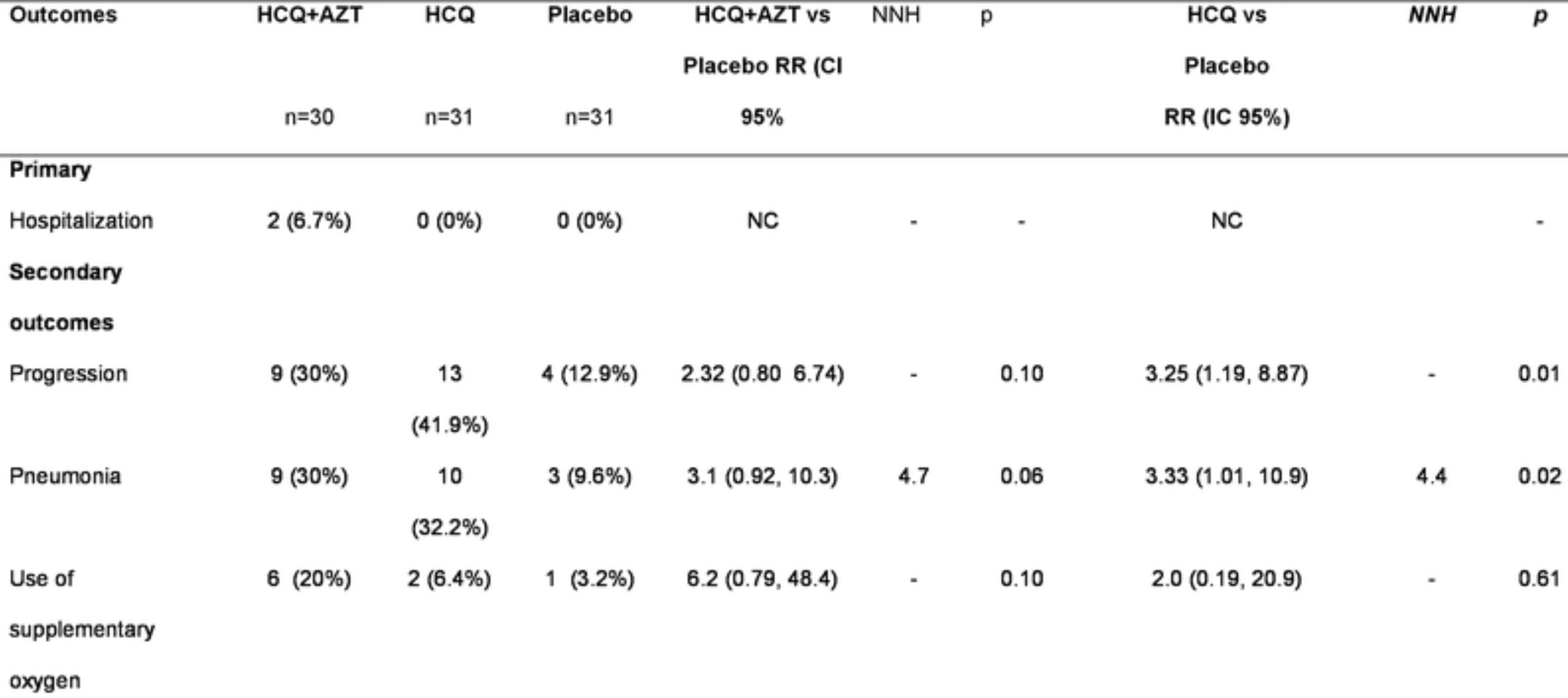
risk of progression, 100% higher, RR 2.00, p = 1.00, treatment 2 of 31 (6.5%), control 1 of 31 (3.2%), HCQ, supplemental oxygen.
|
|
risk of progression, 233.3% higher, RR 3.33, p = 0.06, treatment 10 of 31 (32.3%), control 3 of 31 (9.7%), HCQ, pneumonia.
|
|
risk of progression, 225.0% higher, RR 3.25, p = 0.02, treatment 13 of 31 (41.9%), control 4 of 31 (12.9%), HCQ, oxygen saturation less than 90%, dyspnea, or pneumonia.
|
|
risk of hospitalization, 406.7% higher, RR 5.07, p = 0.24, treatment 2 of 30 (6.7%), control 0 of 31 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), HCQ+AZ, supplemental oxygen.
|
|
risk of progression, 520.0% higher, RR 6.20, p = 0.05, treatment 6 of 30 (20.0%), control 1 of 31 (3.2%), HCQ+AZ, supplemental oxygen.
|
|
risk of progression, 210.0% higher, RR 3.10, p = 0.06, treatment 9 of 30 (30.0%), control 3 of 31 (9.7%), HCQ+AZ, pneumonia.
|
|
risk of progression, 132.5% higher, RR 2.33, p = 0.13, treatment 9 of 30 (30.0%), control 4 of 31 (12.9%), HCQ+AZ, oxygen saturation less than 90%, dyspnea, or pneumonia.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Roy-García et al., 16 Apr 2022, Double Blind Randomized Controlled Trial, Mexico, preprint, 11 authors, study period January 2021 - June 2021, average treatment delay 5.0 days, dosage 200mg bid days 1-10, trial NCT04964583 (history).
Contact: ivonne3316@gmail.com, sesby14@gmail.com.
{kind=link}
“Efficacy and Safety of Fixed Combination of Hydroxychloroquine with Azithromycin Versus Hydroxychloroquine and Placebo in Patients with Mild COVID-19: Randomized, double blind, Placebo controlled trial”
doi:10.1101/2022.04.06.22273531
To determine the efficacy and safety of fixed combination of hydroxychloroquine/azithromycin (HCQ+AZT) compared to hydroxychloroquine (HCQ) alone or placebo in mild COVID-19 outpatients to avoid hospitalization.
Materials and methods This randomized, parallel, double-blind clinical trial included male and female patients aged 18 and 76 years non COVID vaccinated, who were diagnosed with mild COVID-19 infection. All patients underwent liver and kidney profile test, as well as a health questionnaire and clinical revision to document that they did not have uncontrolled comorbidities. They were randomly assigned to one of the three treatment arms: 1) hydroxychloroquine with azithromycin 200 mg/250 mg every 12 hours for five days followed by hydroxychloroquine 200 mg every 12 hours for 5 days; 2) hydroxychloroquine 200 mg every 12 hours for ten days; or 3) placebo every 12 hours for ten days. The primary outcome of the study was hospitalization, while the secondary outcomes were disease progression, pneumonia, use of supplemental oxygen, and adverse events. This study was registered in clinicaltrials.gov with the NCT number of 04964583.
Results A total of 92 participants were randomized. Of whom, 30 received HCQ+AZT, 31 received HCQ, and 31 received placebo. The median age was 37 years, 27.2% of the participants had comorbidities, and the global incidence of hospitalization was .
References
Albani, Fusina, Giovannini, Ferretti, Granato et al., Impact of Azithromycin and/or Hydroxychloroquine on Hospital Mortality in COVID-19, J Clin Med
Andreani, Le Bideau, Duflot, Jardot, Rolland et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microb Pathog
Andreani, Le Bideau, Duflot, Prolland, Boxberger et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microb Pathog
Cavalcanti, Zampieri, Rosa, Azevedo, Veiga et al., Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19
Chen, Liu, Liu, Liu, Xu et al., A pilot study of hydroxychloroquine in treatment of patients with moderate COVID-19
Echeverría-Esnal, Martin-Ontiyuelo, Navarrete-Rouco, Cuscó, Ferrández et al., Azithromycin in the treatment of COVID-19: a review, Expert Rev Anti Infect Ther
Garcia-Zamora, Lee, Haseeb, Bazoukis, Tse et al., Arrhythmias and electrocardiographic findings in Coronavirus disease 2019: A systematic review and meta-analysis, Pacing Clin Electrophysiol
Gautret, Lagier, Parola, Hoang, Meddeb et al., Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a sixday follow up: A pilot observational study, Travel Med Infect Dis
Gautret, Lagier, Parola, Hoang, Meddeb et al., Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial, Int J Antimicrob Agents
Gautret, Million, Jarrot, Camoin-Jau, Colson et al., Natural history of COVID-19 and therapeutic options, Expert Rev Clin Immunol
Geleris, Sun, Platt, Zucker, Baldwin et al., Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19, N Engl J Med
Huang, Yang, Shang, Zheng, Zhao et al., Clinical Characteristics and Predictors of Disease Progression in Severe Patients with COVID-19 Infection in Jiangsu Province, China: A Descriptive Study, Am J Med Sci
Kelly, Connor, Townsend, Coghlan, Relihan et al., Clinical outcomes and adverse events in patients hospitalised with COVID-19, treated with off-label hydroxychloroquine and azithromycin, Br J Clin Pharmacol
Kim, Coppa, Hirsch, Abrahams, Johnson et al., Examination of patient characteristics and hydroxychloroquine use based on the US Food and Drug Administration's recommendation: a cross-sectional analysis in New York, BMJ Open
Kuderer, Choueiri, Shah, Shyr, Rubinstein et al., Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study, Lancet
Maisonnasse, Guedj, Contreras, Behillil, Solas et al., Hydroxychloroquine use against SARS-CoV-2 infection in non-human primates, Nature
Manolis, Manolis, Manolis, Apostolopoulos, Papatheou et al., COVID-19 infection and cardiac arrhythmias, Trends Cardiovasc Med
Morgenstern-Kaplan, Buitano-Tang, Martínez-Gil, Pavón, Talavera, U-shaped-aggressiveness of SARS-CoV-2: Period between initial symptoms and clinical progression to COVID-19 suspicion. A population-based cohort study, PLoS One
Ramadan, Bertolino, Zampino, Mangoni, Hospital et al., Study Group. Cardiac sequelae after coronavirus disease 2019 recovery: a systematic review, Clin Microbiol Infect
Reis, Silva, Silva, Thabane, Singh et al., Effect of Early Treatment With Hydroxychloroquine or Lopinavir and Ritonavir on Risk of Hospitalization Among Patients With COVID-19: The TOGETHER Randomized Clinical Trial, JAMA Netw Open
Rivas-Ruiz, Roy-García, Pérez-Rodríguez, Berea, Moreno-Palacios et al., The relevance and irrelevance of charts in clinical research, Rev Alerg Mex
Roques, Thiberville, Dupuis-Maguiraga, Lum, Labadie et al., Paradoxical Effect of Chloroquine Treatment in Enhancing Chikungunya Virus Infection, Viruses
Savarino, Boelaert, Cassone, Majori, Cauda, Effects of chloroquine on viral infections: an old drug against today's diseases?, Lancet Infect Dis
Schwartz, Boesen, Cerchiaro, Doram, Edwards et al., Assessing the efficacy and safety of hydroxychloroquine as outpatient treatment of COVID-19: a randomized controlled trial, CMAJ Open
Skipper, Da, Hydroxychloroquine in Nonhospitalized Adults With Early COVID-19 : A Randomized Trial, Ann Intern Med
Talavera, Rivas-Ruiz, Clinical research IV. Relevancy of the statistical test chosen, Rev Med Inst Mex Seguro Soc
Wang, Cao, Zhang, Yang, Liu et al., Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro, Cell Res
Álvarez-Maldonado, Hernández-Ríos, Ambríz-Mondragón, Gordillo-Mena, Morales-Serrano et al., Characteristics and mortality of Mexican patients with COVID-19 and mechanical ventilation, Gac Med Mex
DOI record:
{
"DOI": "10.1101/2022.04.06.22273531",
"URL": "http://dx.doi.org/10.1101/2022.04.06.22273531",
"abstract": "<jats:p>To determine the efficacy and safety of fixed combination of hydroxychloroquine/azithromycin (HCQ+AZT) compared to hydroxychloroquine (HCQ) alone or placebo in mild COVID-19 outpatients to avoid hospitalization.Materials and methods This randomized, parallel, double-blind clinical trial included male and female patients aged 18 and 76 years non COVID vaccinated, who were diagnosed with mild COVID-19 infection. All patients underwent liver and kidney profile test, as well as a health questionnaire and clinical revision to document that they did not have uncontrolled comorbidities. They were randomly assigned to one of the three treatment arms: 1) hydroxychloroquine with azithromycin 200 mg/250 mg every 12 hours for five days followed by hydroxychloroquine 200 mg every 12 hours for 5 days; 2) hydroxychloroquine 200 mg every 12 hours for ten days; or 3) placebo every 12 hours for ten days. The primary outcome of the study was hospitalization, while the secondary outcomes were disease progression, pneumonia, use of supplemental oxygen, and adverse events. This study was registered in clinicaltrials.gov with the NCT number of 04964583.ResultsA total of 92 participants were randomized. Of whom, 30 received HCQ+AZT, 31 received HCQ, and 31 received placebo. The median age was 37 years, 27.2% of the participants had comorbidities, and the global incidence of hospitalization was 2.2%. The incidence of hospitalization was 6.7% (2/30) in the HCQ+AZT group compared to the HCQ or placebo groups, in which there were no hospitalizations. Progression of disease was higher in the HCQ group [RR=3.25 (95% CI, 1.19-8.87)] compared with placebo group. There was no statistical difference between the HCQ+AZT group and the placebo group in progression of disease. The incidence of pneumonia was 30% in the HCQ+AZT group, 32.2% in the HCQ group, and 9.6% in the placebo group (HCQ + AZT vs Placebo; p=0.06). There was a significant risk of pneumonia versus placebo only in the HCQ group [RR=3.33 (95% CI, 1.01-10.9)]. Supplemental oxygen was required by 20% (6/30) of the patients in the HCQ+AZT group, 6.4 (2/31) of the patients in the HCQ group, and 3.2% (1/31) of the patients in the placebo group,[(HCQ + AZT vs Placebo; p=0.100), (HCQ vs Placebo, p=0.610)]. There was no statistical difference between groups for negative test (PCR) on day 11. The most frequent adverse events were gastrointestinal symptoms. No lengthening of the QT interval was observed in patients receiving HCQ+AZT or HCQ.ConclusionThe use of HCQ+AZT does not decrease the risk of hospitalization in patients with mild COVID-19. The use of HCQ increases the risk of progression and pneumonia.</jats:p>",
"accepted": {
"date-parts": [
[
2022,
4,
16
]
]
},
"author": [
{
"affiliation": [],
"family": "Roy-García",
"given": "Ivonne A",
"sequence": "first"
},
{
"affiliation": [],
"family": "Moreno-Noguez",
"given": "Moises",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Rivas-Ruiz",
"given": "Rodolfo",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Zapata-Tarres",
"given": "Marta",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Pérez-Rodríguez",
"given": "Marcela",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Ortiz-Zamora",
"given": "Magaly A",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Navarro-Susano",
"given": "Gabriela",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Guzman-Rivas",
"given": "Lilia",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Garcia-Cortes",
"given": "Luis R",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Palma-Lara",
"given": "Icela",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Gutierrez-Catrellón",
"given": "Pedro",
"sequence": "additional"
}
],
"container-title": [],
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2022,
4,
16
]
],
"date-time": "2022-04-16T19:20:18Z",
"timestamp": 1650136818000
},
"deposited": {
"date-parts": [
[
2022,
4,
16
]
],
"date-time": "2022-04-16T19:20:18Z",
"timestamp": 1650136818000
},
"group-title": "Infectious Diseases (except HIV/AIDS)",
"indexed": {
"date-parts": [
[
2022,
4,
16
]
],
"date-time": "2022-04-16T19:41:15Z",
"timestamp": 1650138075120
},
"institution": [
{
"name": "medRxiv"
}
],
"is-referenced-by-count": 0,
"issued": {
"date-parts": [
[
2022,
4,
16
]
]
},
"link": [
{
"URL": "https://syndication.highwire.org/content/doi/10.1101/2022.04.06.22273531",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "246",
"original-title": [],
"posted": {
"date-parts": [
[
2022,
4,
16
]
]
},
"prefix": "10.1101",
"published": {
"date-parts": [
[
2022,
4,
16
]
]
},
"publisher": "Cold Spring Harbor Laboratory",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "http://medrxiv.org/lookup/doi/10.1101/2022.04.06.22273531"
}
},
"score": 1,
"short-container-title": [],
"short-title": [],
"source": "Crossref",
"subtitle": [],
"subtype": "preprint",
"title": [
"Efficacy and Safety of Fixed Combination of Hydroxychloroquine with Azithromycin Versus Hydroxychloroquine and Placebo in Patients with Mild COVID-19: Randomized, double blind, Placebo controlled trial"
],
"type": "posted-content"
}