A Phase 2 Randomized, Double Blinded, Placebo Controlled Study of Oral Camostat Mesilate Compared to Standard of Care in Subjects With Mild-Moderate COVID-19
et al., NCT04524663, COPS-2003, NCT04524663, May 2021
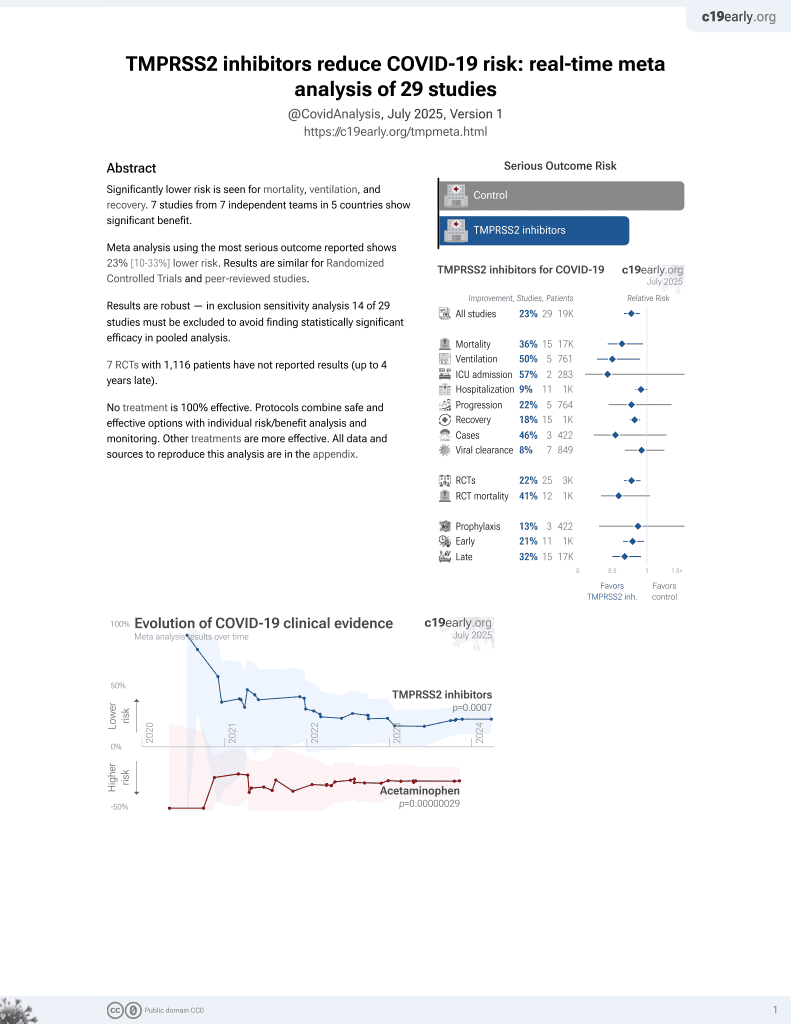
21st treatment shown to reduce risk in
April 2021, now with p = 0.00063 from 29 studies.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
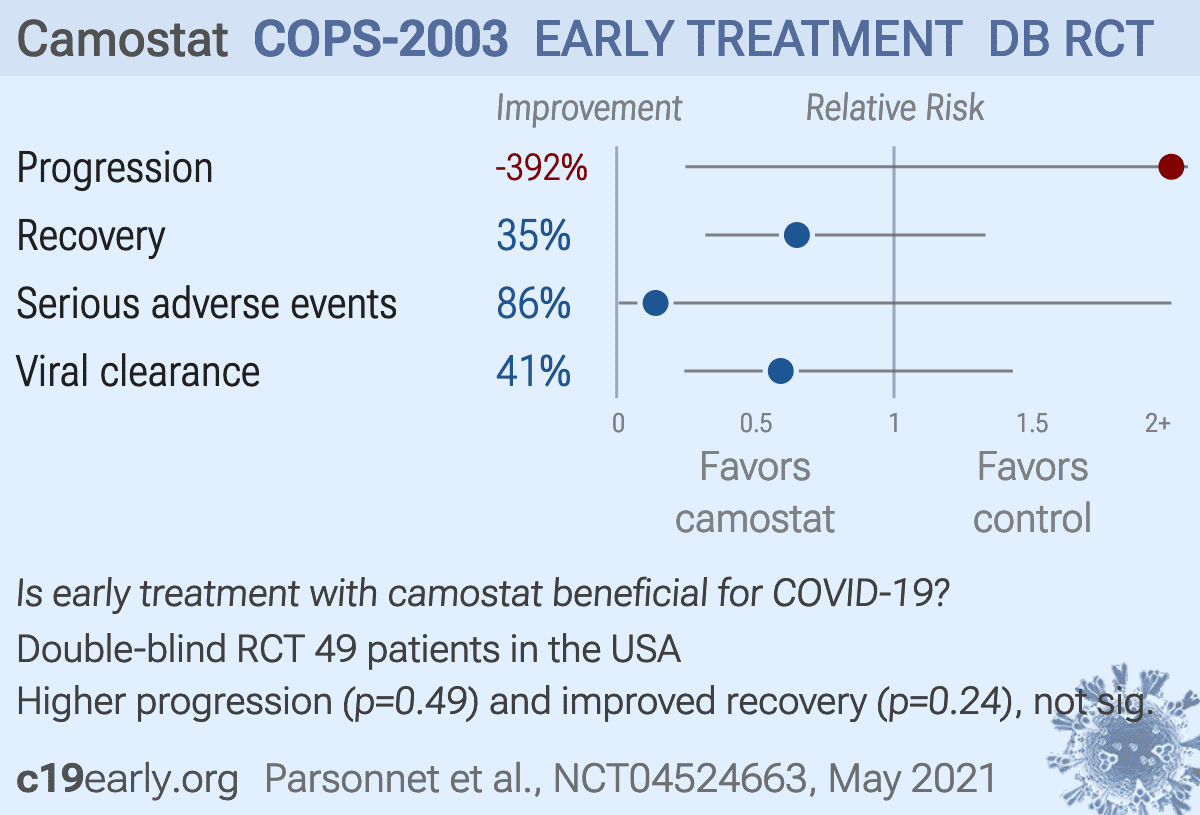
RCT 49 outpatients in the USA, showing no significant differences with camostat treatment.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
Study covers TMPRSS2 inhibitors and camostat.
|
risk of progression, 392.0% higher, RR 4.92, p = 0.49, treatment 2 of 25 (8.0%), control 0 of 24 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm).
|
|
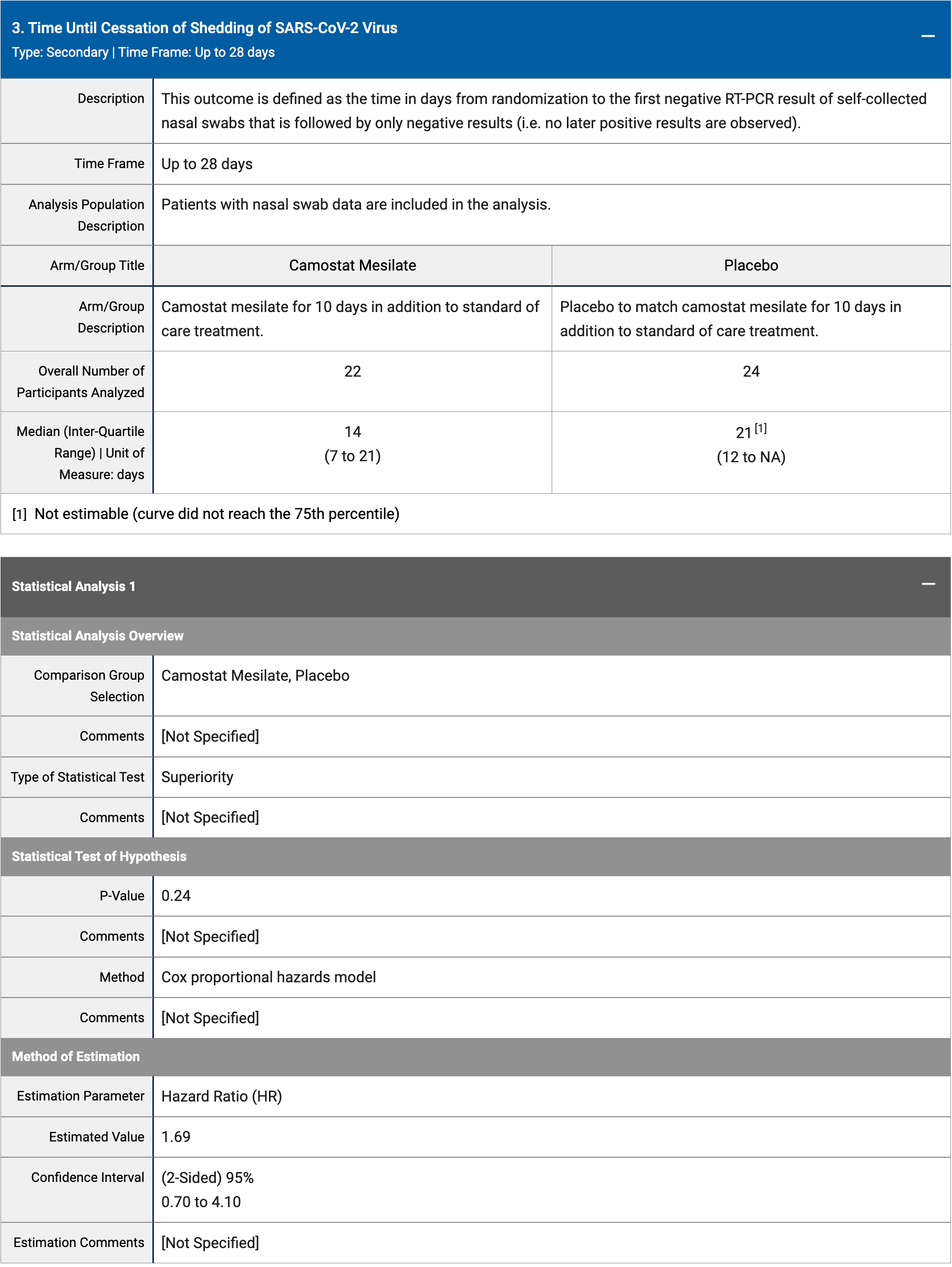
risk of no recovery, 35.0% lower, HR 0.65, p = 0.24, treatment 25, control 24, Cox proportional hazards.
|
|
serious adverse events, 86.0% lower, RR 0.14, p = 0.11, treatment 0 of 25 (0.0%), control 3 of 24 (12.5%), NNT 8.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm).
|
|
risk of no viral clearance, 40.8% lower, HR 0.59, p = 0.24, treatment 25, control 24, inverted to make HR<1 favor treatment, Cox proportional hazards.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Parsonnet et al., 15 May 2021, Double Blind Randomized Controlled Trial, placebo-controlled, USA, preprint, 1 author, trial NCT04524663 (history) (COPS-2003).
Contact: parsonnt@stanford.edu.
{kind=link}