Ursodeoxycholic acid for coronavirus disease 2019 prevention
et al., Journal of Internal Medicine, doi:10.1111/joim.13704, Jul 2023
{kind=link}
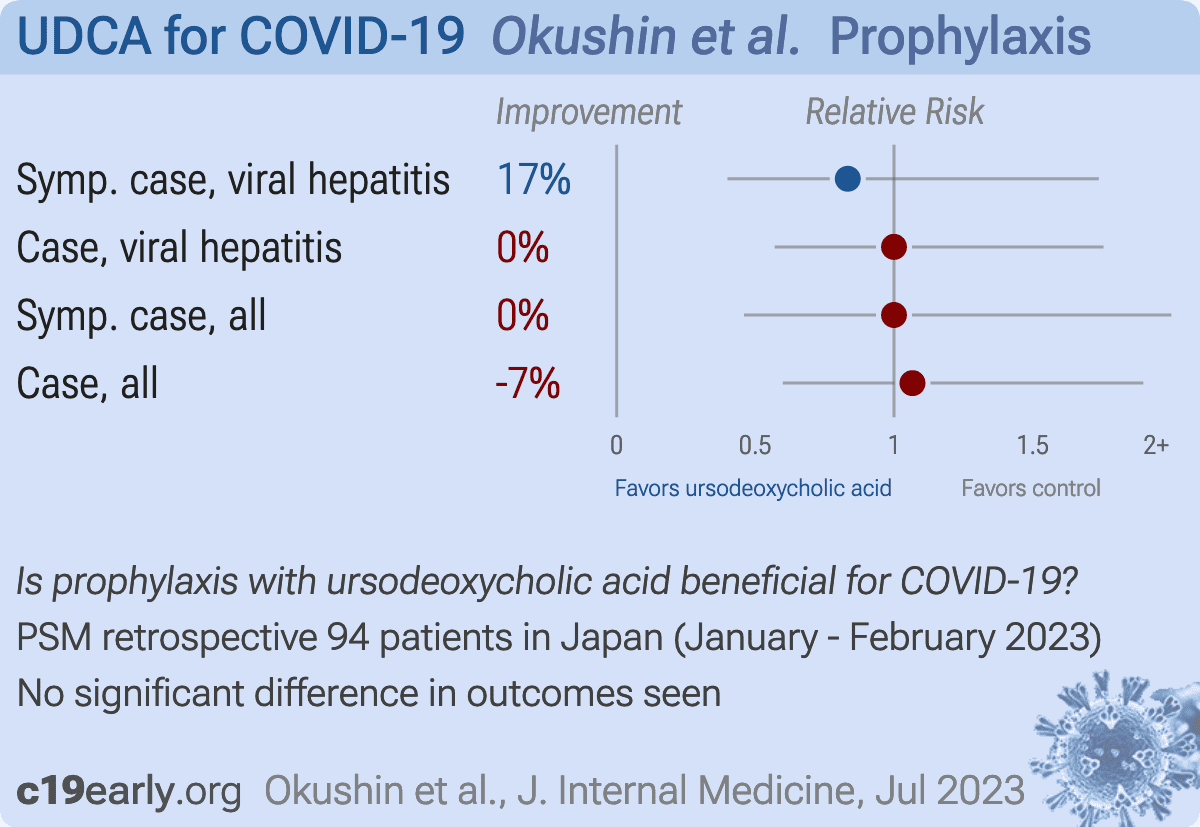
Retrospective 94 outpatients attending a university hospital gastroenterology clinic in Japan showing no significant difference in SARS-CoV-2 infection rates between ursodeoxycholic acid (UDCA)-treated patients and control groups without UDCA treatment. However, UDCA-treated patients tended to have higher rates of subclinical infection based on serology, suggesting UDCA may reduce COVID-19 severity.
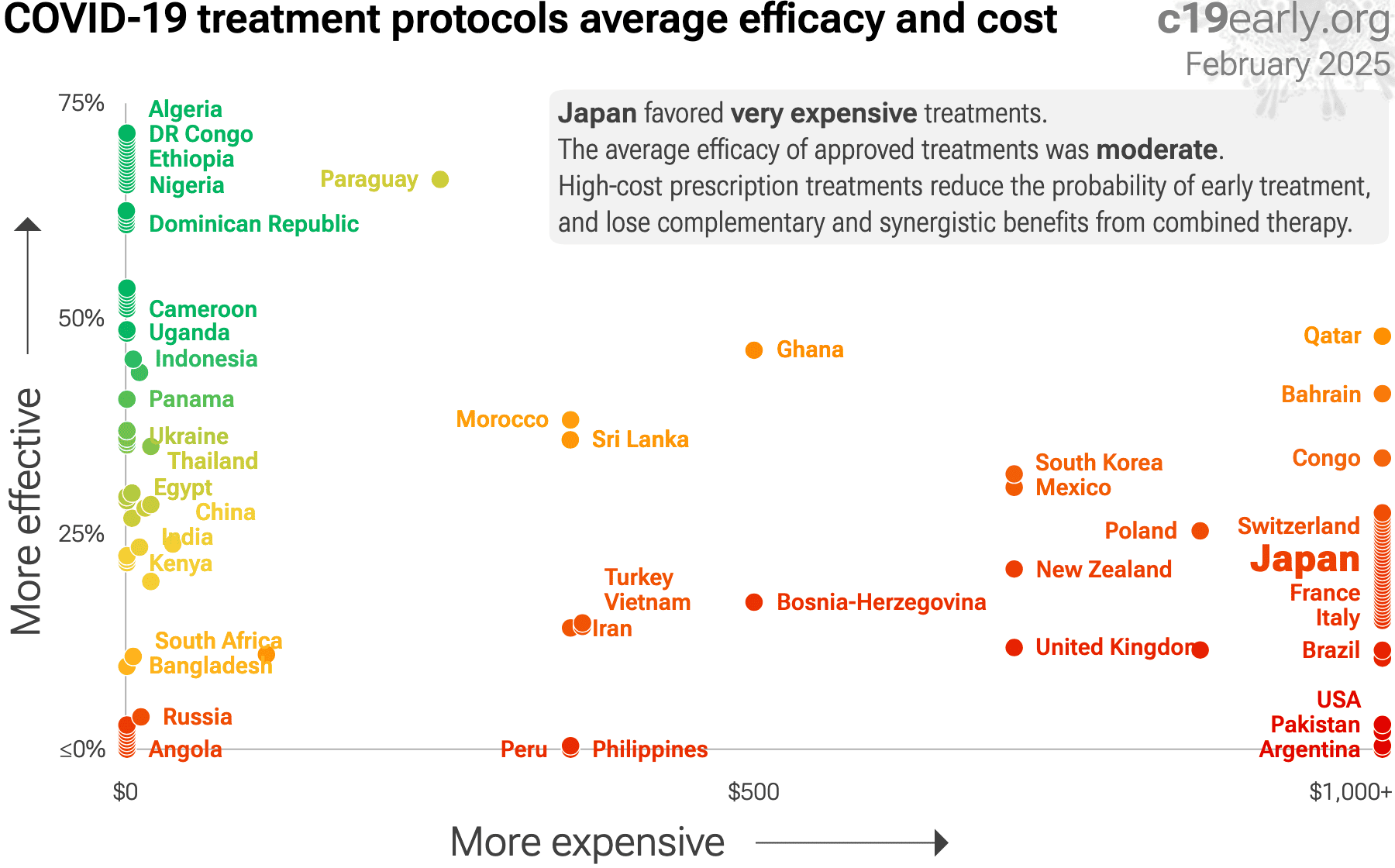
Standard of Care (SOC) for COVID-19 in the study country,
Japan, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of symptomatic case, 16.7% lower, RR 0.83, p = 0.81, treatment 10 of 47 (21.3%), control 12 of 47 (25.5%), NNT 24, viral hepatitis, propensity score matching.
|
|
risk of case, no change, RR 1.00, p = 1.00, treatment 16 of 47 (34.0%), control 16 of 47 (34.0%), viral hepatitis, propensity score matching.
|
|
risk of symptomatic case, no change, RR 1.00, p = 1.00, treatment 10 of 47 (21.3%), control 10 of 47 (21.3%), all, propensity score matching.
|
|
risk of case, 6.7% higher, RR 1.07, p = 1.00, treatment 16 of 47 (34.0%), control 15 of 47 (31.9%), all, propensity score matching.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
Okushin et al., 27 Jul 2023, retrospective, Japan, peer-reviewed, 7 authors, study period 1 January, 2023 - 10 February, 2023.
{kind=link}
Abstract: Research Letter
doi: 10.1111/joim.13704
Ursodeoxycholic acid for coronavirus disease 2019
prevention
Dear Editor,
The novel coronavirus disease 2019 (COVID-19)
has had a tremendous impact worldwide [1].
Although the management of COVID-19 has
improved, the chemoprevention of severe acute
respiratory syndrome coronavirus (SARS-CoV2) infection remains a challenge. In 2022, the
potential of ursodeoxycholic acid (UDCA) against
COVID-19 was first reported [2]. Furthermore,
the association of UDCA with a decrease in
SARS-CoV-2 infection and reduction in symptomatic COVID-19 was retrospectively demonstrated [3]. These reports suggested the utility
of UDCA in preventing COVID-19. However, the
Omicron variant—predominant since early 2022—
causes milder disease, including asymptomatic
infection, compared to previously predominant
variants [4]. If the infected patients had no or
mild symptoms, they might not have tested for
COVID-19; therefore, they might be unaware of
their infection. A more objective evaluation of
infection proportions in a cross-sectional cohort
is needed to accurately evaluate the preventive
ability.
Here, we cross-sectionally examined the impact of
UDCA on SARS-CoV-2 infection in early 2023. The
infection was defined based on medical interviews
and SARS-CoV-2 immunoglobulin G against the
nucleocapsid protein (IgG-N), which could detect
the previous SARS-CoV-2 infection regardless of
vaccination [5]. The cutoff value for IgG-N was
set at 5 AU/mL [6], which identifies infections for
approximately 1 year (unpublished data), covering
the Omicron variant–dominant period in Japan.
Subclinical infection was defined as IgG-N positivity without interview-based infection.
Outpatients attending the Department of Gastroenterology at The University of Tokyo Hospital
between January 1, 2023, and February 10, 2023,
were included (Fig. S1). The UDCA treatment
group was compared with patients without a
history of UDCA prescription (non-UDCA group)
and patients with viral hepatitis without a history
of UDCA prescription (non-UDCA viral hepatitis
group). Age, sex, and the number of vaccinations
were matched using propensity score-matching
(PSM) analysis (nearest-neighbor matching at a
ratio of 1:1 was performed using a caliper of 0.1).
The study protocol was approved by the Research
Ethics Committee of the Faculty of Medicine at the
University of Tokyo (approval number:2019300NI4-(3)). Informed consent was obtained through an
opt-out form.
In the entire cohort, the SARS-CoV-2 infection
proportion was not significantly different between
the UDCA and non-UDCA groups (Fig. 1A and
Table S1). The UDCA group tended to be older and
had a higher proportion of women, while the vaccination status was similar. After PSM, there was no
difference in the SARS-CoV-2 infection proportion
between the two groups; however, the subclinical
infection proportion tended to be higher in the
UDCA group than non-UDCA group (Fig. 1B and
Table S1).
Between the UDCA and non-UDCA viral hepatitis groups, the SARS-CoV-2 infection proportion
was not significantly different in the entire cohort
(Fig. 1A and Table S2). Background factors were
similar, except the proportion of women was higher
in the UDCA group. After PSM, there was no difference in the SARS-CoV-2 infection proportion
between the two groups; however, the subclinical infection proportion tended to be higher in the
UDCA group than in the non-UDCA viral hepatitis
group (Fig. 1C and Table S2).
In this..
DOI record:
{
"DOI": "10.1111/joim.13704",
"ISSN": [
"0954-6820",
"1365-2796"
],
"URL": "http://dx.doi.org/10.1111/joim.13704",
"alternative-id": [
"10.1111/joim.13704"
],
"assertion": [
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Published",
"name": "published",
"order": 2,
"value": "2023-07-27"
}
],
"author": [
{
"affiliation": [
{
"name": "Department of Infection Control and Prevention, Graduate School of Medicine The University of Tokyo Tokyo Japan"
},
{
"name": "Department of Gastroenterology, Graduate School of Medicine The University of Tokyo Tokyo Japan"
}
],
"family": "Okushin",
"given": "Kazuya",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Department of Clinical Laboratory The University of Tokyo Hospital Tokyo Japan"
},
{
"name": "Department of Clinical Laboratory Medicine, Graduate School of Medicine The University of Tokyo Tokyo Japan"
}
],
"family": "Kurano",
"given": "Makoto",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Clinical Laboratory The University of Tokyo Hospital Tokyo Japan"
},
{
"name": "Department of Clinical Laboratory Medicine, Graduate School of Medicine The University of Tokyo Tokyo Japan"
}
],
"family": "Yatomi",
"given": "Yutaka",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Infection Control and Prevention, Graduate School of Medicine The University of Tokyo Tokyo Japan"
}
],
"family": "Moriya",
"given": "Kyoji",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Gastroenterology, Graduate School of Medicine The University of Tokyo Tokyo Japan"
}
],
"family": "Fujishiro",
"given": "Mitsuhiro",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-0851-1887",
"affiliation": [
{
"name": "Department of Infection Control and Prevention, Graduate School of Medicine The University of Tokyo Tokyo Japan"
}
],
"authenticated-orcid": false,
"family": "Tsutsumi",
"given": "Takeya",
"sequence": "additional"
},
{
"affiliation": [],
"name": "UTH‐UDCA Study Group",
"sequence": "additional"
}
],
"container-title": "Journal of Internal Medicine",
"container-title-short": "J Intern Med",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"onlinelibrary.wiley.com"
]
},
"created": {
"date-parts": [
[
2023,
7,
20
]
],
"date-time": "2023-07-20T07:44:51Z",
"timestamp": 1689839091000
},
"deposited": {
"date-parts": [
[
2023,
8,
17
]
],
"date-time": "2023-08-17T04:00:56Z",
"timestamp": 1692244856000
},
"indexed": {
"date-parts": [
[
2023,
8,
18
]
],
"date-time": "2023-08-18T04:48:36Z",
"timestamp": 1692334116609
},
"is-referenced-by-count": 0,
"issued": {
"date-parts": [
[
2023,
7,
27
]
]
},
"language": "en",
"license": [
{
"URL": "http://onlinelibrary.wiley.com/termsAndConditions#vor",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2023,
7,
27
]
],
"date-time": "2023-07-27T00:00:00Z",
"timestamp": 1690416000000
}
}
],
"link": [
{
"URL": "https://onlinelibrary.wiley.com/doi/pdf/10.1111/joim.13704",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "311",
"original-title": [],
"prefix": "10.1111",
"published": {
"date-parts": [
[
2023,
7,
27
]
]
},
"published-online": {
"date-parts": [
[
2023,
7,
27
]
]
},
"publisher": "Wiley",
"reference": [
{
"DOI": "10.1016/S0140-6736(21)02796-3",
"doi-asserted-by": "publisher",
"key": "e_1_2_6_2_1"
},
{
"DOI": "10.1038/s41586-022-05594-0",
"doi-asserted-by": "publisher",
"key": "e_1_2_6_3_1"
},
{
"DOI": "10.1111/joim.13630",
"doi-asserted-by": "publisher",
"key": "e_1_2_6_4_1"
},
{
"DOI": "10.1002/jmv.28066",
"doi-asserted-by": "publisher",
"key": "e_1_2_6_5_1"
},
{
"DOI": "10.3390/v15040930",
"doi-asserted-by": "publisher",
"key": "e_1_2_6_6_1"
},
{
"DOI": "10.1038/s41598-021-82428-5",
"doi-asserted-by": "publisher",
"key": "e_1_2_6_7_1"
}
],
"reference-count": 6,
"references-count": 6,
"relation": {},
"resource": {
"primary": {
"URL": "https://onlinelibrary.wiley.com/doi/10.1111/joim.13704"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Internal Medicine"
],
"subtitle": [],
"title": "Ursodeoxycholic acid for coronavirus disease 2019 prevention",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1002/crossmark_policy"
}