Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants
et al., The Lancet Global Health, doi:10.1016/S2214-109X(18)30357-7, Oct 2018
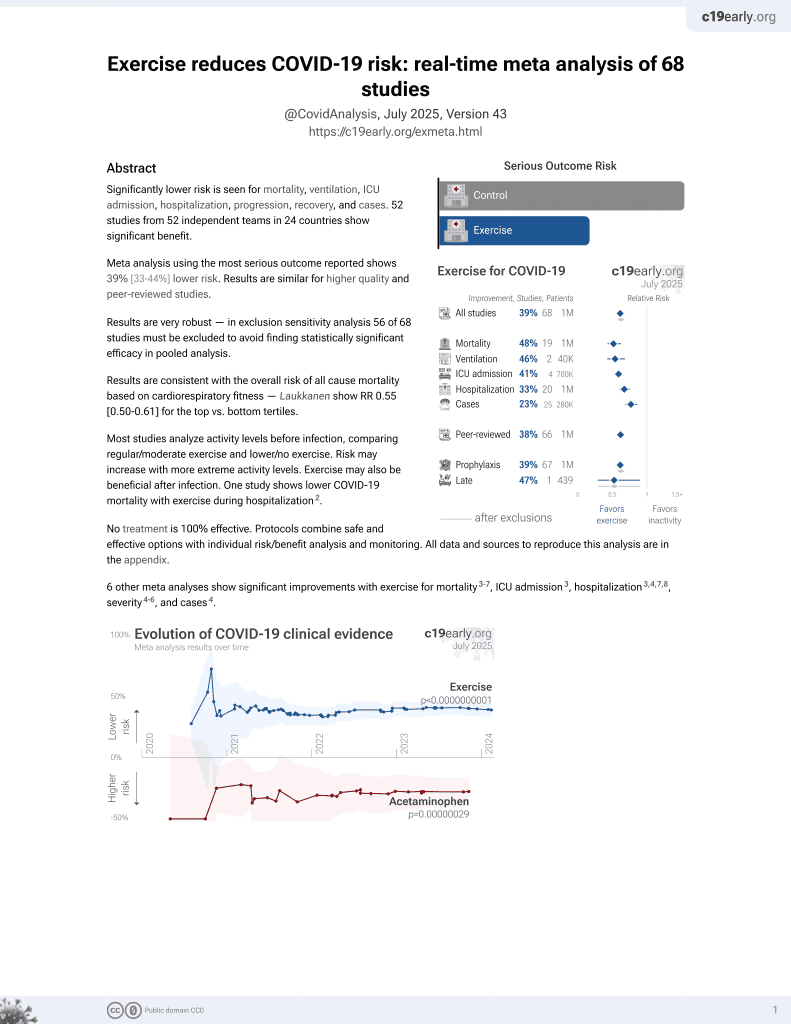
Exercise for COVID-19
9th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 68 studies.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

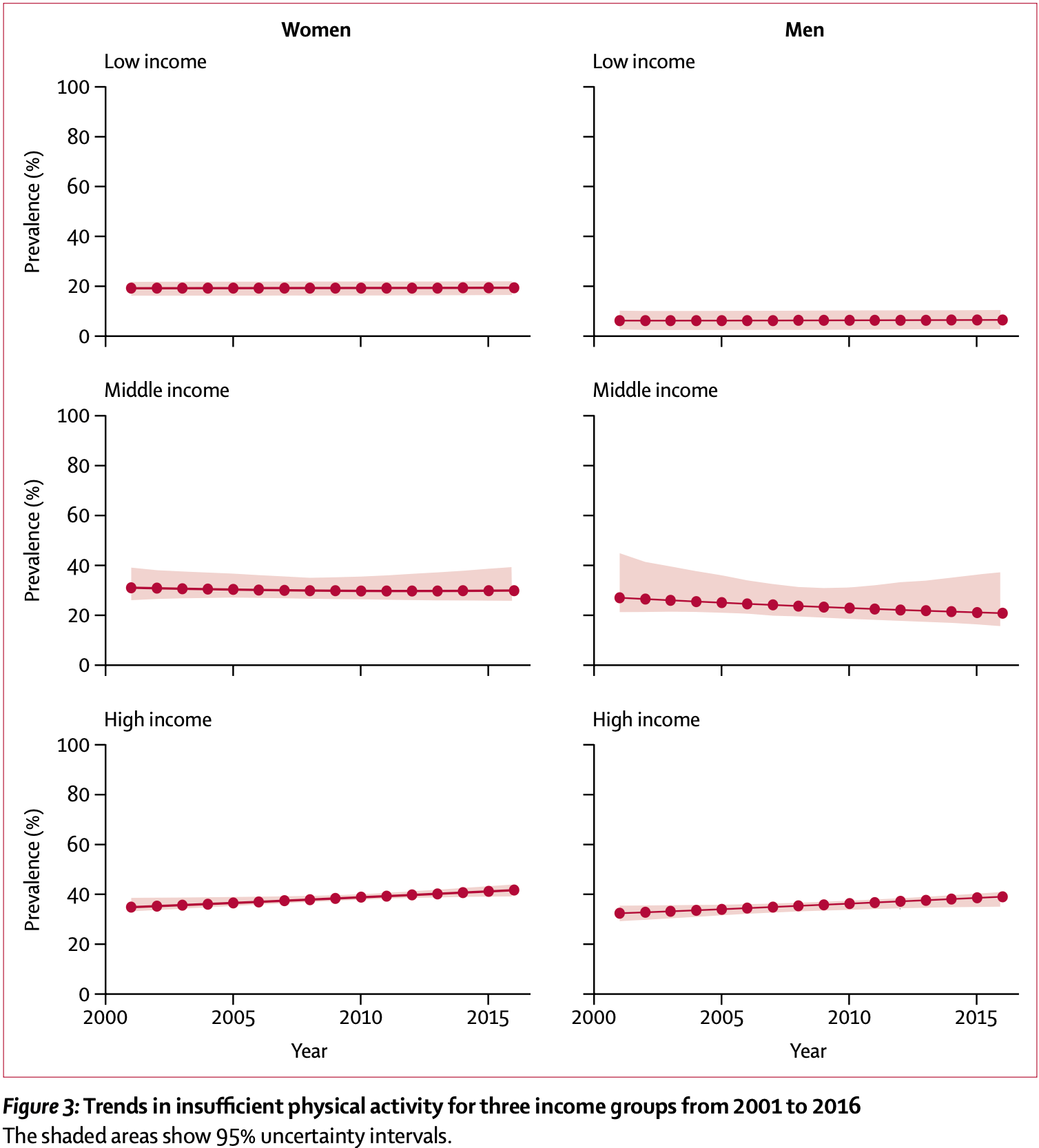
Meta analysis of 358 surveys showing the prevalence of insufficient physical activity around the world. Prevalence in high-income countries was over twice as high, and has increased over time.
6 meta-analyses show significant improvements with exercise for mortality1-5,
ICU admission1,
hospitalization1,2,5,6 ,
severity2-4, and
cases2.
Currently there are 68 exercise for COVID-19 studies, showing 48% lower mortality [38‑57%], 46% lower ventilation [32‑57%], 41% lower ICU admission [35‑47%], 33% lower hospitalization [25‑40%], and 23% fewer cases [14‑31%].
{kind=link}
1.
Rahmati et al., Baseline physical activity is associated with reduced mortality and disease outcomes in COVID-19: A systematic review and meta-analysis, Reviews in Medical Virology, doi:10.1002/rmv.2349.
2.
Ezzatvar et al., Physical activity and risk of infection, severity and mortality of COVID-19: a systematic review and non-linear dose–response meta-analysis of data from 1 853 610 adults, British Journal of Sports Medicine, doi:10.1136/bjsports-2022-105733.
3.
Sittichai et al., Effects of physical activity on the severity of illness and mortality in COVID-19 patients: A systematic review and meta-analysis, Frontiers in Physiology, doi:10.3389/fphys.2022.1030568.
4.
Liu et al., Baseline physical activity and the risk of severe illness and mortality from COVID-19: A dose–response meta-analysis, Preventive Medicine Reports, doi:10.1016/j.pmedr.2023.102130.
Guthold et al., 31 Oct 2018, peer-reviewed, 4 authors.
Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants
The Lancet Global Health, doi:10.1016/s2214-109x(18)30357-7
Background Insufficient physical activity is a leading risk factor for non-communicable diseases, and has a negative effect on mental health and quality of life. We describe levels of insufficient physical activity across countries, and estimate global and regional trends. Methods We pooled data from population-based surveys reporting the prevalence of insufficient physical activity, which included physical activity at work, at home, for transport, and during leisure time (ie, not doing at least 150 min of moderate-intensity, or 75 min of vigorous-intensity physical activity per week, or any equivalent combination of the two). We used regression models to adjust survey data to a standard definition and age groups. We estimated time trends using multilevel mixed-effects modelling.
Findings We included data from 358 surveys across 168 countries, including 1•9 million participants. Global agestandardised prevalence of insufficient physical activity was 27•5% (95% uncertainty interval 25•0-32•2) in 2016, with a difference between sexes of more than 8 percentage points (23•4%, 21•1-30•7, in men vs 31•7%, 28•6-39•0, in women). Between 2001, and 2016, levels of insufficient activity were stable (28•5%, 23•9-33•9, in 2001; change not significant). The highest levels in 2016, were in women in Latin America and the Caribbean (43•7%, 42•9-46•5), south Asia (43•0%, 29•6-74•9), and high-income Western countries (42•3%, 39•1-45•4), whereas the lowest levels were in men from Oceania (12•3%, 11•2-17•7), east and southeast Asia (17•6%, 15•7-23•9), and sub-Saharan Africa (17•9%, 15•1-20•5). Prevalence in 2016 was more than twice as high in high-income countries (36•8%, 35•0-38•0) as in low-income countries (16•2%, 14•2-17•9), and insufficient activity has increased in high-income countries over time (31•6%, 27•1-37•2, in 2001). Interpretation If current trends continue, the 2025 global physical activity target (a 10% relative reduction in insufficient physical activity) will not be met. Policies to increase population levels of physical activity need to be prioritised and scaled up urgently.
References
Ahmad, Boschi-Pinto, Lopez, Murray, Lozano et al., Age standardization of rates: a new WHO standard
Ainsworth, Macera, Jones, Comparison of the 2001 BRFSS and the IPAQ Physical Activity Questionnaires, Med Sci Sports Exerc
Althoff, Sosič, Hicks, King, Delp et al., Large-scale physical activity data reveal worldwide activity inequality, Nature
Ara, Aparicio-Ugarriza, Morales-Barco, De Souza, Mata et al., Physical activity assessment in the general population; validated self-report methods, Nutr Hosp
Armstrong, Bull, Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ), J Public Health
Bull, Armstrong, Dixon, Ham, Neiman et al., Physical Inactivity
Ekelund, Sepp, Brage, Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults, Public Health Nutr
Gesis, The European Commission's Eurobarometer Surveys
Guthold, Louazani, Riley, Physical activity in 22 African countries: results from the World Health Organization STEPwise approach to chronic disease risk factor surveillance, Am J Prev Med
Hallal, Andersen, Bull, Global physical activity levels: surveillance progress, pitfalls, and prospects, Lancet
Hallal, Gomez, Parra, Lessons learned after 10 years of IPAQ use in Brazil and Colombia, J Phys Act Health
Koohpayehzadeh, Etemad, Abbasi, of risk factors of non-communicable diseases
Lee, Shiroma, Lobelo, Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy, Lancet
Mielke, Da Silva, Kolbe-Alexander, Brown, Shifting the physical inactivity curve worldwide by closing the gender gap, Sports Med
Ncd Risk, Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19•1 million participants, Lancet
Ng, Popkin, Time use and physical activity: a shift away from movement across the globe, Obes Rev
Pate, Pratt, Blair, Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine, JAMA
Ranasinghe, Ranasinghe, Jayawardena, Misra, Physical activity patterns among south-Asian adults: a systematic review, Int J Behav Nutr Phys Act
Riley, Guthold, Cowan, The World Health Organization STEPwise Approach to Noncommunicable Disease Risk-Factor Surveillance: methods, challenges, and opportunities, Am J Public Health
Rzewnicki, Vanden Auweele, Bourdeaudhuij, Addressing overreporting on the International Physical Activity Questionnaire (IPAQ) telephone survey with a population sample, Public Health Nutr
Sallis, Bull, Guthold, Progress in physical activity over the Olympic quadrennium, Lancet
Stevens, White, Flaxman, Global prevalence of vision impairment and blindness: magnitude and temporal trends, 1990-2010, Ophthalmology
Stevenson, Thompson, De Sá, Land use, transport, and population health: estimating the health benefits of compact cities, Lancet
Tian, Jiang, Wang, BMI, leisure-time physical activity, and physical fitness in adults in China: results from a series of national surveys, 2000-14, Lancet Diabetes Endocrinol
Tu, Liao, Schuller, Insights from an observational assessment of park-based physical activity in Nanchang, China, Prev Med
Warburton, Charlesworth, Ivey, Nettlefold, Bredin, A systematic review of the evidence for Canada's Physical Activity Guidelines for Adults, Int J Behav Nutr Phys Act
Who, Assessing national capacity for the prevention and control of NCDs
Who, Global Physical Activity Surveillance
Who, Global action plan for the prevention and control of noncommunicable diseases 2013-2020
Who, Global action plan on physical activity 2018-2030
Who, Global recommendations on physical activity for health
Who, STEPwise approach to Surveillance (STEPS
Wijndaele, Westgate, Stephens, Utilization and harmonization of adult accelerometry data: review and expert consensus, Med Sci Sports Exerc
DOI record:
{
"DOI": "10.1016/s2214-109x(18)30357-7",
"ISSN": [
"2214-109X"
],
"URL": "http://dx.doi.org/10.1016/s2214-109x(18)30357-7",
"alternative-id": [
"S2214109X18303577"
],
"assertion": [
{
"label": "This article is maintained by",
"name": "publisher",
"value": "Elsevier"
},
{
"label": "Article Title",
"name": "articletitle",
"value": "Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants"
},
{
"label": "Journal Title",
"name": "journaltitle",
"value": "The Lancet Global Health"
},
{
"label": "CrossRef DOI link to publisher maintained version",
"name": "articlelink",
"value": "https://doi.org/10.1016/S2214-109X(18)30357-7"
},
{
"label": "CrossRef DOI link to the associated document",
"name": "associatedlink",
"value": "https://doi.org/10.1016/S2214-109X(18)30381-4"
},
{
"label": "Content Type",
"name": "content_type",
"value": "article"
},
{
"label": "Copyright",
"name": "copyright",
"value": "© 2018 World Health Organization; licensee Elsevier Ltd."
}
],
"author": [
{
"affiliation": [],
"family": "Guthold",
"given": "Regina",
"sequence": "first"
},
{
"affiliation": [],
"family": "Stevens",
"given": "Gretchen A",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Riley",
"given": "Leanne M",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Bull",
"given": "Fiona C",
"sequence": "additional"
}
],
"container-title": [
"The Lancet Global Health"
],
"content-domain": {
"crossmark-restriction": true,
"domain": [
"clinicalkey.jp",
"clinicalkey.com",
"clinicalkey.es",
"clinicalkey.com.au",
"clinicalkey.fr",
"thelancet.com",
"elsevier.com",
"sciencedirect.com"
]
},
"created": {
"date-parts": [
[
2018,
9,
4
]
],
"date-time": "2018-09-04T22:41:16Z",
"timestamp": 1536100876000
},
"deposited": {
"date-parts": [
[
2019,
3,
25
]
],
"date-time": "2019-03-25T13:02:28Z",
"timestamp": 1553518948000
},
"indexed": {
"date-parts": [
[
2022,
4,
2
]
],
"date-time": "2022-04-02T02:27:57Z",
"timestamp": 1648866477839
},
"is-referenced-by-count": 1306,
"issn-type": [
{
"type": "print",
"value": "2214-109X"
}
],
"issue": "10",
"issued": {
"date-parts": [
[
2018,
10
]
]
},
"journal-issue": {
"issue": "10",
"published-print": {
"date-parts": [
[
2018,
10
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://www.elsevier.com/tdm/userlicense/1.0/",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2018,
10,
1
]
],
"date-time": "2018-10-01T00:00:00Z",
"timestamp": 1538352000000
}
},
{
"URL": "http://creativecommons.org/licenses/by/3.0/igo/",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2018,
7,
16
]
],
"date-time": "2018-07-16T00:00:00Z",
"timestamp": 1531699200000
}
}
],
"link": [
{
"URL": "https://api.elsevier.com/content/article/PII:S2214109X18303577?httpAccept=text/xml",
"content-type": "text/xml",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://api.elsevier.com/content/article/PII:S2214109X18303577?httpAccept=text/plain",
"content-type": "text/plain",
"content-version": "vor",
"intended-application": "text-mining"
}
],
"member": "78",
"original-title": [],
"page": "e1077-e1086",
"prefix": "10.1016",
"published": {
"date-parts": [
[
2018,
10
]
]
},
"published-print": {
"date-parts": [
[
2018,
10
]
]
},
"publisher": "Elsevier BV",
"reference": [
{
"article-title": "Physical Activity Guidelines Advisory Committee report, 2008. To the Secretary of Health and Human Services. Part A: executive summary",
"first-page": "114",
"journal-title": "Nutr Rev",
"key": "10.1016/S2214-109X(18)30357-7_bib1",
"volume": "67",
"year": "2009"
},
{
"DOI": "10.1186/1479-5868-7-39",
"article-title": "A systematic review of the evidence for Canada's Physical Activity Guidelines for Adults",
"author": "Warburton",
"doi-asserted-by": "crossref",
"first-page": "39",
"journal-title": "Int J Behav Nutr Phys Act",
"key": "10.1016/S2214-109X(18)30357-7_bib2",
"volume": "7",
"year": "2010"
},
{
"key": "10.1016/S2214-109X(18)30357-7_bib3",
"series-title": "Global recommendations on physical activity for health",
"year": "2010"
},
{
"DOI": "10.1016/S0140-6736(16)30581-5",
"article-title": "Progress in physical activity over the Olympic quadrennium",
"author": "Sallis",
"doi-asserted-by": "crossref",
"first-page": "1325",
"journal-title": "Lancet",
"key": "10.1016/S2214-109X(18)30357-7_bib4",
"volume": "388",
"year": "2016"
},
{
"DOI": "10.1136/bjsports-2017-098063",
"article-title": "The Bangkok Declaration on Physical Activity for Global Health and Sustainable Development",
"doi-asserted-by": "crossref",
"first-page": "1389",
"journal-title": "Br J Sports Med",
"key": "10.1016/S2214-109X(18)30357-7_bib5",
"volume": "51",
"year": "2017"
},
{
"key": "10.1016/S2214-109X(18)30357-7_bib6",
"series-title": "Global action plan for the prevention and control of noncommunicable diseases 2013–2020",
"year": "2013"
},
{
"article-title": "Physical Inactivity",
"author": "Bull",
"key": "10.1016/S2214-109X(18)30357-7_bib7",
"series-title": "Comparative quantification of health risks. Global and regional burden of disease attributable to selected major risk factors",
"year": "2004"
},
{
"DOI": "10.1007/s10389-006-0024-x",
"article-title": "Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ)",
"author": "Armstrong",
"doi-asserted-by": "crossref",
"first-page": "66",
"journal-title": "J Public Health",
"key": "10.1016/S2214-109X(18)30357-7_bib10",
"volume": "14",
"year": "2006"
},
{
"DOI": "10.2105/AJPH.2015.302962",
"article-title": "The World Health Organization STEPwise Approach to Noncommunicable Disease Risk-Factor Surveillance: methods, challenges, and opportunities",
"author": "Riley",
"doi-asserted-by": "crossref",
"first-page": "74",
"journal-title": "Am J Public Health",
"key": "10.1016/S2214-109X(18)30357-7_bib14",
"volume": "106",
"year": "2016"
},
{
"DOI": "10.1016/S0140-6736(12)60646-1",
"article-title": "Global physical activity levels: surveillance progress, pitfalls, and prospects",
"author": "Hallal",
"doi-asserted-by": "crossref",
"first-page": "247",
"journal-title": "Lancet",
"key": "10.1016/S2214-109X(18)30357-7_bib15",
"volume": "380",
"year": "2012"
},
{
"DOI": "10.1016/S0140-6736(12)61031-9",
"article-title": "Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy",
"author": "Lee",
"doi-asserted-by": "crossref",
"first-page": "219",
"journal-title": "Lancet",
"key": "10.1016/S2214-109X(18)30357-7_bib16",
"volume": "380",
"year": "2012"
},
{
"DOI": "10.1016/S0140-6736(17)32129-3",
"article-title": "Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults",
"doi-asserted-by": "crossref",
"first-page": "2627",
"journal-title": "Lancet",
"key": "10.1016/S2214-109X(18)30357-7_bib19",
"volume": "390",
"year": "2017"
},
{
"DOI": "10.1016/S0140-6736(16)31919-5",
"article-title": "Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants",
"doi-asserted-by": "crossref",
"first-page": "37",
"journal-title": "Lancet",
"key": "10.1016/S2214-109X(18)30357-7_bib20",
"volume": "389",
"year": "2017"
},
{
"DOI": "10.1001/jama.1995.03520290054029",
"article-title": "Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine",
"author": "Pate",
"doi-asserted-by": "crossref",
"first-page": "402",
"journal-title": "JAMA",
"key": "10.1016/S2214-109X(18)30357-7_bib21",
"volume": "273",
"year": "1995"
},
{
"DOI": "10.1079/PHN2002427",
"article-title": "Addressing overreporting on the International Physical Activity Questionnaire (IPAQ) telephone survey with a population sample",
"author": "Rzewnicki",
"doi-asserted-by": "crossref",
"first-page": "299",
"journal-title": "Public Health Nutr",
"key": "10.1016/S2214-109X(18)30357-7_bib23",
"volume": "6",
"year": "2003"
},
{
"DOI": "10.1123/jpah.7.s2.s259",
"article-title": "Lessons learned after 10 years of IPAQ use in Brazil and Colombia",
"author": "Hallal",
"doi-asserted-by": "crossref",
"first-page": "S259",
"issue": "suppl 2",
"journal-title": "J Phys Act Health",
"key": "10.1016/S2214-109X(18)30357-7_bib24",
"volume": "7",
"year": "2010"
},
{
"DOI": "10.1079/PHN2005840",
"article-title": "Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults",
"author": "Ekelund",
"doi-asserted-by": "crossref",
"first-page": "258",
"journal-title": "Public Health Nutr",
"key": "10.1016/S2214-109X(18)30357-7_bib25",
"volume": "9",
"year": "2006"
},
{
"DOI": "10.1249/01.mss.0000229457.73333.9a",
"article-title": "Comparison of the 2001 BRFSS and the IPAQ Physical Activity Questionnaires",
"author": "Ainsworth",
"doi-asserted-by": "crossref",
"first-page": "1584",
"journal-title": "Med Sci Sports Exerc",
"key": "10.1016/S2214-109X(18)30357-7_bib26",
"volume": "38",
"year": "2006"
},
{
"author": "Ahmad",
"key": "10.1016/S2214-109X(18)30357-7_bib28",
"series-title": "Age standardization of rates: a new WHO standard",
"year": "2001"
},
{
"DOI": "10.1016/j.ophtha.2013.05.025",
"article-title": "Global prevalence of vision impairment and blindness: magnitude and temporal trends, 1990–2010",
"author": "Stevens",
"doi-asserted-by": "crossref",
"first-page": "2377",
"journal-title": "Ophthalmology",
"key": "10.1016/S2214-109X(18)30357-7_bib30",
"volume": "120",
"year": "2013"
},
{
"DOI": "10.1111/j.1467-789X.2011.00982.x",
"article-title": "Time use and physical activity: a shift away from movement across the globe",
"author": "Ng",
"doi-asserted-by": "crossref",
"first-page": "659",
"journal-title": "Obes Rev",
"key": "10.1016/S2214-109X(18)30357-7_bib31",
"volume": "13",
"year": "2012"
},
{
"key": "10.1016/S2214-109X(18)30357-7_bib32",
"series-title": "Global action plan on physical activity 2018–2030. More active people for a healthier world",
"year": "2018"
},
{
"DOI": "10.1016/S0140-6736(16)30067-8",
"article-title": "Land use, transport, and population health: estimating the health benefits of compact cities",
"author": "Stevenson",
"doi-asserted-by": "crossref",
"first-page": "2925",
"journal-title": "Lancet",
"key": "10.1016/S2214-109X(18)30357-7_bib33",
"volume": "388",
"year": "2016"
},
{
"DOI": "10.1038/nature23018",
"article-title": "Large-scale physical activity data reveal worldwide activity inequality",
"author": "Althoff",
"doi-asserted-by": "crossref",
"first-page": "336",
"journal-title": "Nature",
"key": "10.1016/S2214-109X(18)30357-7_bib34",
"volume": "547",
"year": "2017"
},
{
"DOI": "10.1186/1479-5868-10-116",
"article-title": "Physical activity patterns among south-Asian adults: a systematic review",
"author": "Ranasinghe",
"doi-asserted-by": "crossref",
"first-page": "116",
"journal-title": "Int J Behav Nutr Phys Act",
"key": "10.1016/S2214-109X(18)30357-7_bib35",
"volume": "10",
"year": "2013"
},
{
"DOI": "10.1007/s00038-013-0529-3",
"article-title": "Gender-specific changes in physical activity pattern in Iran: national surveillance of risk factors of non-communicable diseases (2007–2011)",
"author": "Koohpayehzadeh",
"doi-asserted-by": "crossref",
"first-page": "231",
"journal-title": "Int J Public Health",
"key": "10.1016/S2214-109X(18)30357-7_bib36",
"volume": "59",
"year": "2014"
},
{
"DOI": "10.1007/s40279-017-0754-7",
"article-title": "Shifting the physical inactivity curve worldwide by closing the gender gap",
"author": "Mielke",
"doi-asserted-by": "crossref",
"first-page": "481",
"journal-title": "Sports Med",
"key": "10.1016/S2214-109X(18)30357-7_bib38",
"volume": "48",
"year": "2018"
},
{
"DOI": "10.1016/j.amepre.2011.03.008",
"article-title": "Physical activity in 22 African countries: results from the World Health Organization STEPwise approach to chronic disease risk factor surveillance",
"author": "Guthold",
"doi-asserted-by": "crossref",
"first-page": "52",
"journal-title": "Am J Prev Med",
"key": "10.1016/S2214-109X(18)30357-7_bib39",
"volume": "41",
"year": "2011"
},
{
"key": "10.1016/S2214-109X(18)30357-7_bib40",
"series-title": "Promoting physical activity in the Eastern Mediterranean Region through a life-course approach",
"year": "2014"
},
{
"DOI": "10.1016/S2213-8587(16)00081-4",
"article-title": "BMI, leisure-time physical activity, and physical fitness in adults in China: results from a series of national surveys, 2000–14",
"author": "Tian",
"doi-asserted-by": "crossref",
"first-page": "487",
"journal-title": "Lancet Diabetes Endocrinol",
"key": "10.1016/S2214-109X(18)30357-7_bib41",
"volume": "4",
"year": "2016"
},
{
"article-title": "Insights from an observational assessment of park-based physical activity in Nanchang, China",
"author": "Tu",
"first-page": "930",
"journal-title": "Prev Med",
"key": "10.1016/S2214-109X(18)30357-7_bib42",
"volume": "2",
"year": "2015"
},
{
"article-title": "Physical activity assessment in the general population; validated self-report methods",
"author": "Ara",
"first-page": "211",
"issue": "suppl 3",
"journal-title": "Nutr Hosp",
"key": "10.1016/S2214-109X(18)30357-7_bib43",
"volume": "31",
"year": "2015"
},
{
"DOI": "10.1249/MSS.0000000000000661",
"article-title": "Utilization and harmonization of adult accelerometry data: review and expert consensus",
"author": "Wijndaele",
"doi-asserted-by": "crossref",
"first-page": "2129",
"journal-title": "Med Sci Sports Exerc",
"key": "10.1016/S2214-109X(18)30357-7_bib44",
"volume": "47",
"year": "2015"
}
],
"reference-count": 33,
"references-count": 33,
"relation": {},
"score": 1,
"short-container-title": [
"The Lancet Global Health"
],
"short-title": [],
"source": "Crossref",
"subject": [
"General Medicine"
],
"subtitle": [],
"title": [
"Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants"
],
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1016/elsevier_cm_policy",
"volume": "6"
}