Mortality Risk Among Patients With COVID-19 Prescribed Selective Serotonin Reuptake Inhibitor Antidepressants
et al., JAMA Network Open, doi:10.1001/jamanetworkopen.2021.33090, Nov 2021
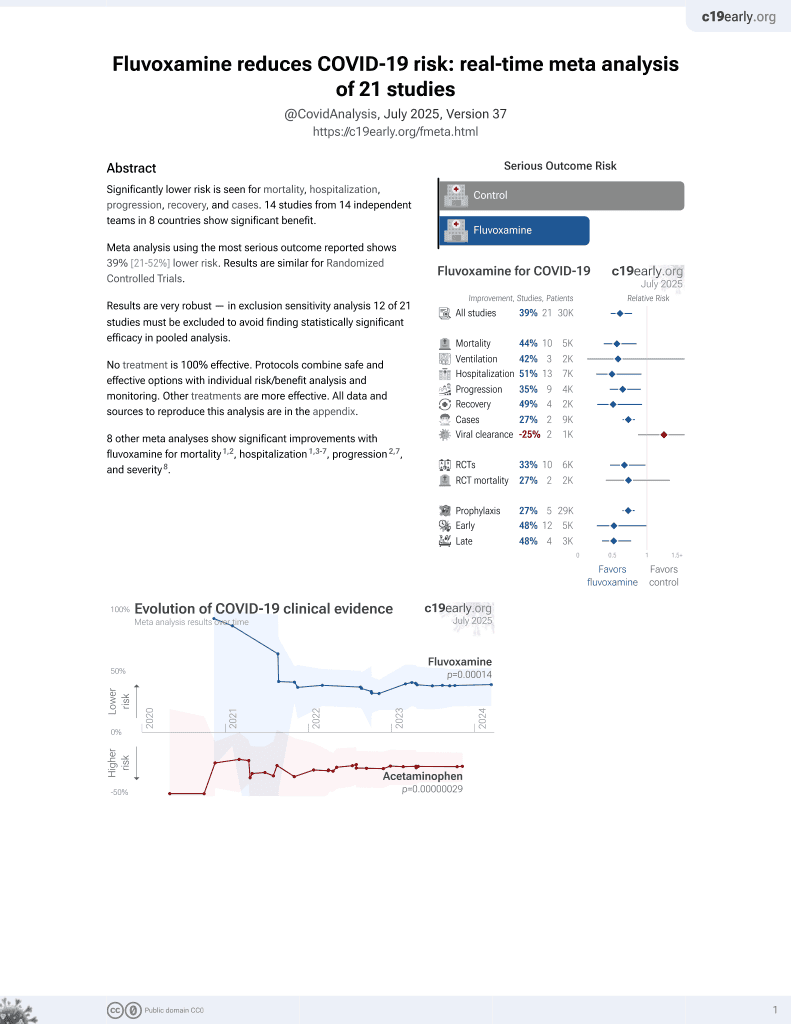
30th treatment shown to reduce risk in
November 2021, now with p = 0.00014 from 21 studies, recognized in 2 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
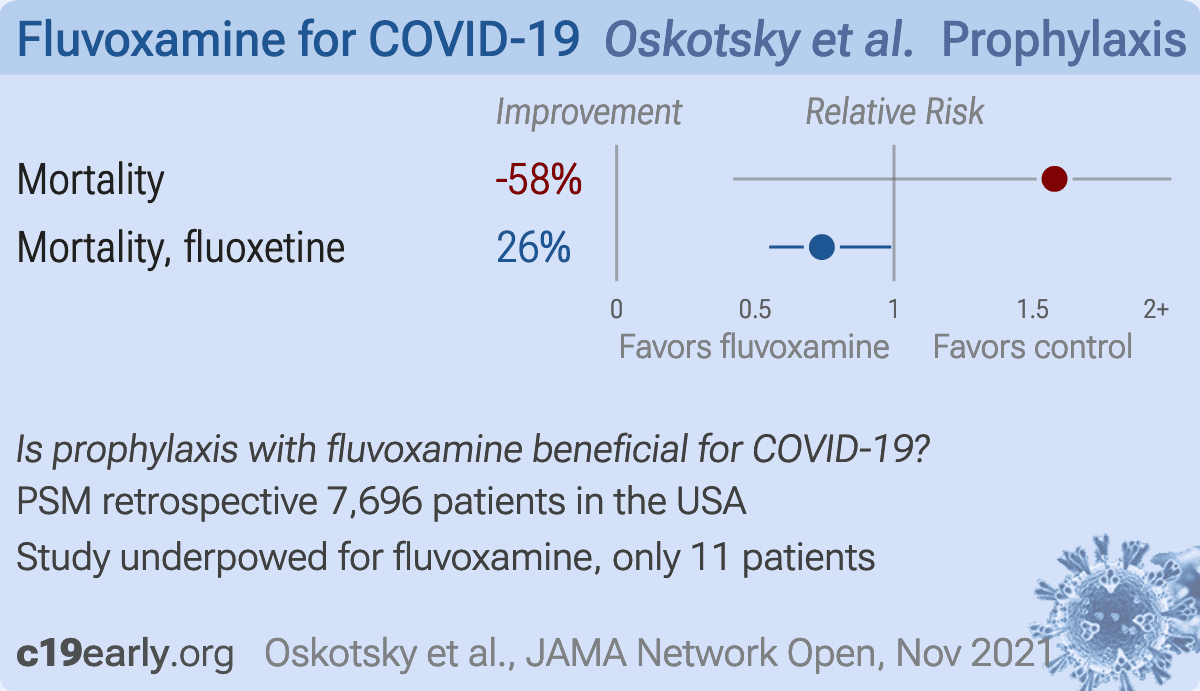
Retrospective database analysis of 83,584 patients in the USA, showing lower mortality with existing fluoxetine use in PSM analysis. There were 11 fluvoxamine patients, showing non-statistically significant higher mortality.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of death, 57.9% higher, RR 1.58, p = 0.62, treatment 2 of 11 (18.2%), control 19 of 165 (11.5%), fluvoxamine.
|
|
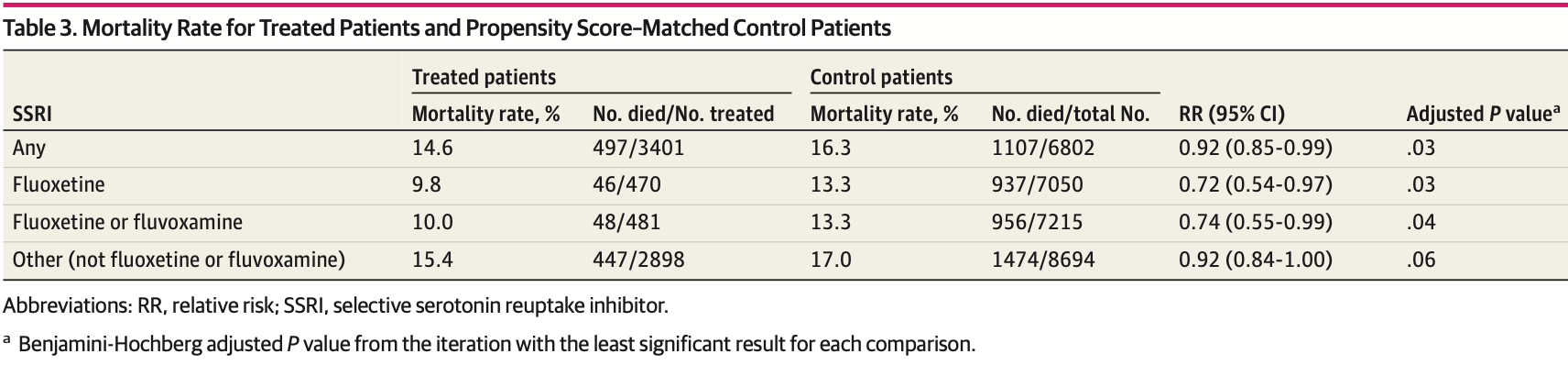
risk of death, 26.0% lower, RR 0.74, p = 0.04, treatment 48 of 481 (10.0%), control 956 of 7,215 (13.3%), NNT 31, fluoxetine.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Oskotsky et al., 15 Nov 2021, retrospective, propensity score matching, USA, peer-reviewed, 8 authors.
{kind=link}
Mortality Risk Among Patients With COVID-19 Prescribed Selective Serotonin Reuptake Inhibitor Antidepressants
JAMA Network Open, doi:10.1001/jamanetworkopen.2021.33090
IMPORTANCE Antidepressant use may be associated with reduced levels of several proinflammatory cytokines suggested to be involved with the development of severe COVID-19. An association between the use of selective serotonin reuptake inhibitors (SSRIs)-specifically fluoxetine hydrochloride and fluvoxamine maleate-with decreased mortality among patients with COVID-19 has been reported in recent studies; however, these studies had limited power due to their small size.
OBJECTIVE To investigate the association of SSRIs with outcomes in patients with COVID-19 by analyzing electronic health records (EHRs). DESIGN, SETTING, AND PARTICIPANTS This retrospective cohort study used propensity score matching by demographic characteristics, comorbidities, and medication indication to compare SSRItreated patients with matched control patients not treated with SSRIs within a large EHR database representing a diverse population of 83 584 patients diagnosed with COVID-19 from January to September 2020 and with a duration of follow-up of as long as 8 months in 87 health care centers across the US. EXPOSURES Selective serotonin reuptake inhibitors and specifically (1) fluoxetine, (2) fluoxetine or fluvoxamine, and (3) other SSRIs (ie, not fluoxetine or fluvoxamine). MAIN OUTCOMES AND MEASURES Death. RESULTS A total of 3401 adult patients with COVID-19 prescribed SSRIs (2033 women [59.8%]; mean [SD] age, 63.8 [18.1] years) were identified, with 470 receiving fluoxetine only (280 women [59.6%]; mean [SD] age, 58.5 [18.1] years), 481 receiving fluoxetine or fluvoxamine (285 women [59.3%]; mean [SD] age, 58.7 [18.0] years), and 2898 receiving other SSRIs (1733 women [59.8%]; mean [SD] age, 64.7 [18.0] years) within a defined time frame. When compared with matched untreated control patients, relative risk (RR) of mortality was reduced among patients prescribed any SSRI (497 of 3401 [14.6%] vs 1130 of 6802 [16.6%]; RR, 0.92 [95% CI, 0.85-0.99]; adjusted P = .03); fluoxetine (46 of 470 [9.8%] vs 937 of 7050 [13.3%]; RR, 0.72 [95% CI, 0.54-0.97]; adjusted P = .03); and fluoxetine or fluvoxamine (48 of 481 [10.0%] vs 956 of 7215 [13.3%]; RR, 0.74 [95% CI, 0.55-0.99]; adjusted P = .04). The association between receiving any SSRI that is not fluoxetine or fluvoxamine and risk of death was not statistically significant (447 of 2898 [15.4%] vs 1474 of 8694 [17.0%]; RR, 0.92 [95% CI, 0.84-1.00]; adjusted P = .06). CONCLUSIONS AND RELEVANCE These results support evidence that SSRIs may be associated with reduced severity of COVID-19 reflected in the reduced RR of mortality. Further research and randomized clinical trials are needed to elucidate the effect of SSRIs generally, or more specifically of fluoxetine and fluvoxamine, on the severity of COVID-19 outcomes.
ARTICLE INFORMATION Accepted for Publication
References
Ahern, 5-HT and the immune system, Curr Opin Pharmacol, doi:10.1016/j.coph.2011.02.004
Austin, Small, The use of bootstrapping when using propensity-score matching without replacement: a simulation study, Stat Med, doi:10.1002/sim.6276
Carpinteiro, Edwards, Hoffmann, Pharmacological inhibition of acid sphingomyelinase prevents uptake of SARS-CoV-2 by epithelial cells, Cell Rep Med, doi:10.1016/j.xcrm.2020.100142
Carpinteiro, Gripp, Hoffmann, Inhibition of acid sphingomyelinase by ambroxol prevents SARS-CoV-2 entry into epithelial cells, J Biol Chem, doi:10.1016/j.jbc.2021.100701
Creeden, Imami, Eby, Fluoxetine as an anti-inflammatory therapy in SARS-CoV-2 infection, Biomed Pharmacother, doi:10.1016/j.biopha.2021.111437
Dechaumes, Nekoua, Belouzard, Fluoxetine can inhibit SARS-CoV-2 in vitro, Microorganisms
Diez-Quevedo, Iglesias-González, Giralt-López, Mental disorders, psychopharmacological treatments, and mortality in 2150 COVID-19 Spanish inpatients, Acta Psychiatr Scand, doi:10.1111/acps.13304
Furukawa, Cipriani, Cowen, Leucht, Egger et al., Optimal dose of selective serotonin reuptake inhibitors, venlafaxine, and mirtazapine in major depression: a systematic review and dose-response metaanalysis, Lancet Psychiatry, doi:10.1016/S2215-0366(19)30217-2
Günster, Busse, Spoden, 6-Month follow up of 8679 hospitalized COVID-19 patients in Germany: a nationwide cohort study. medRxiv, doi:10.1101/2021.04.24.21256029
Hamed, Mgm, Hagag, The possible immunoregulatory and anti-inflammatory effects of selective serotonin reuptake inhibitors in coronavirus disease patients, Med Hypotheses, doi:10.1016/j.mehy.2020.110140
Hannestad, Dellagioia, Bloch, The effect of antidepressant medication treatment on serum levels of inflammatory cytokines: a meta-analysis, Neuropsychopharmacology, doi:10.1038/npp.2011.132
Hayasaka, Purgato, Magni, Dose equivalents of antidepressants: evidence-based recommendations from randomized controlled trials, J Affect Disord, doi:10.1016/j.jad.2015.03.021
Hoertel, Sánchez-Rico, Gulbins, Association between psychotropic medications functionally inhibiting acid sphingomyelinase and reduced risk of intubation or death among individuals with mental disorder and severe COVID-19: an observational study. medRxiv, doi:10.1101/2021.02.18.21251997
Hoertel, Sánchez-Rico, Gulbins, Entrepôt de Données de Santé" AP-HP Consortium. Association between FIASMAs and reduced risk of intubation or death in individuals hospitalized for severe COVID-19: an observational multicenter study, Clin Pharmacol Ther. Published online, doi:10.1002/cpt.2317
Hoertel, Sánchez-Rico, Vernet, Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: results from an observational study, Mol Psychiatry, doi:10.1038/s41380-021-01021-4
Ishima, Fujita, Hashimoto, Interaction of new antidepressants with sigma-1 receptor chaperones and their potentiation of neurite outgrowth in PC12 cells, Eur J Pharmacol, doi:10.1016/j.ejphar.2014.01.064
Kristiansen, Hansen, Inhibition of HIV replication by neuroleptic agents and their potential use in HIV infected patients with AIDS related dementia, Int J Antimicrob Agents, doi:10.1016/S0924-8579(99)00157-0
Köhler, Freitas, Stubbs, Peripheral alterations in cytokine and chemokine levels after antidepressant drug treatment for major depressive disorder: systematic review and meta-analysis, Mol Neurobiol, doi:10.1007/s12035-017-0632-1
Lenze, Mattar, Zorumski, Fluvoxamine vs placebo and clinical deterioration in outpatients with symptomatic COVID-19: a randomized clinical trial, JAMA, doi:https://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2020.22760&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamanetworkopen.2021.33090
Luo, Kataoka, Ostinelli, Cipriani, Furukawa, National prescription patterns of antidepressants in the treatment of adults with major depression in the US between 1996 and 2015: a population representative survey based analysis, Front Psychiatry, doi:10.3389/fpsyt.2020.00035
Marín-Corral, Rodríguez-Morató, Gomez-Gomez, Metabolic signatures associated with severity in hospitalized COVID-19 patients, Int J Mol Sci, doi:10.3390/ijms22094794
Pashaei, Drug repurposing of selective serotonin reuptake inhibitors: could these drugs help fight COVID-19 and save lives?, J Clin Neurosci, doi:10.1016/j.jocn.2021.03.010
Pirraglia, Stafford, Singer, Trends in prescribing of selective serotonin reuptake inhibitors and other newer antidepressant agents in adult primary care, Prim Care Companion J Clin Psychiatry, doi:10.4088/PCC.v05n0402
Ravindran, Stein, The pharmacologic treatment of anxiety disorders: a review of progress, J Clin Psychiatry, doi:10.4088/JCP.10r06218blu
Sacre, Medghalchi, Gregory, Brennan, Williams, Fluoxetine and citalopram exhibit potent antiinflammatory activity in human and murine models of rheumatoid arthritis and inhibit toll-like receptors, Arthritis Rheum, doi:10.1002/art.27304
Seftel, Boulware, Prospective cohort of fluvoxamine for early treatment of coronavirus disease 19, Open Forum Infect Dis, doi:10.1093/ofid/ofab050
Słuzewska, Rybakowski, Laciak, Mackiewicz, Sobieska et al., Interleukin-6 serum levels in depressed patients before and after treatment with fluoxetine, Ann N Y Acad Sci, doi:10.1111/j.1749-6632.1995.tb32372.x
Taquet, Luciano, Geddes, Harrison, Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA, Lancet Psychiatry, doi:10.1016/S2215-0366(20)30462-4
Vj, Illescas-Montes, Puerta-Puerta, Ruiz, Melguizo-Rodríguez, SARS-CoV-2 infection: the role of cytokines in COVID-19 disease, Cytokine Growth Factor Rev, doi:10.1016/j.cytogfr.2020.06.001
Von Elm, Altman, Egger, Pocock, Gøtzsche et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies, Lancet, doi:10.1016/S0140-6736(07)61602-X
Wang, Xu, Volkow, Increased risk of COVID-19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States, World Psychiatry, doi:10.1002/wps.20806
Zimniak, Kirschner, Hilpert, The serotonin reuptake inhibitor fluoxetine inhibits SARS-CoV-2 in human lung tissue, Sci Rep, doi:10.1038/s41598-021-85049-0
Zuo, Quinn, Kye, Cooper, Damoiseaux et al., Propensity Scores (PS) and Standardized Mean Differences (SMD) of Covariates for Comparison of Fluoxetine-Treated Patients and Matched Control Patients eFigure 3. Propensity Scores (PS) and Standardized Mean Differences (SMD) of Covariates for Comparison of Fluoxetine-or Fluvoxamine-Treated Patients and Matched Control Patients eFigure 4. Propensity Scores (PS) and Standardized Mean Differences (SMD) of Covariates for Comparison of Other (Not Fluoxetine or Fluvoxamine) SSRI-Treated Patients and Matched Control Patients eTable 1. Standardized Mean Differences (SMD) of Covariates Between SSRI-Treated and Control Groups Before and After Matching eTable 2. Standardized Mean Differences (SMD) of Covariates Between Fluoxetine-Treated and Control Groups Before and After Matching eTable 3. Standardized Mean Differences (SMD) of Covariates Between Fluoxetine-or Fluvoxamine-Treated and Control Groups Before and After Matching eTable 4. Standardized Mean Differences (SMD) of Covariates Between Other (Not Fluoxetine or Fluvoxamine) SSRI-Treated and Control Groups Before and After Matching eTable 5. Propensity Score (PS) Matching by Demographics, Encounter Type at the Time of the First Recorded COVID-19 Diagnosis, COVID-19 Comorbidities, and Prescription Indications for SSRI-Exposed Patients and Unexposed Control Patients eTable 6. Propensity Score (PS) Matching by Demographics, Encounter Type at the Time of the First Recorded COVID-19 Diagnosis, COVID-19 Comorbidities, and Prescription Indications for Fluoxetine-Exposed Patients and Unexposed Control Patients eTable 7. Propensity Score (PS) Matching by Demographics, Encounter Type at the Time of the First Recorded COVID-19 Diagnosis, COVID-19 Comorbidities, and Prescription Indications for Fluoxetine-or Fluvoxamine-Exposed Patients and Unexposed Control Patients eTable 8. Propensity Score (PS) Matching by Demographics, Encounter Type at the Time of the First Recorded COVID-19 Diagnosis, COVID-19 Comorbidities, and Prescription Indications for Other (Not Fluoxetine or Fluvoxamine) SSRI-Exposed Patients and Unexposed Control Patients, doi:10.1128/AAC.00983-12
DOI record:
{
"DOI": "10.1001/jamanetworkopen.2021.33090",
"ISSN": [
"2574-3805"
],
"URL": "http://dx.doi.org/10.1001/jamanetworkopen.2021.33090",
"author": [
{
"affiliation": [
{
"name": "Department of Pediatrics, University of California, San Francisco"
},
{
"name": "Bakar Computational Health Sciences Institute, University of California, San Francisco"
}
],
"family": "Oskotsky",
"given": "Tomiko",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, Stanford University School of Medicine, Stanford, California"
}
],
"family": "Marić",
"given": "Ivana",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, University of California, San Francisco"
},
{
"name": "Bakar Computational Health Sciences Institute, University of California, San Francisco"
},
{
"name": "Graduate Program in Bioengineering, University of California, San Francisco"
}
],
"family": "Tang",
"given": "Alice",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, University of California, San Francisco"
},
{
"name": "Bakar Computational Health Sciences Institute, University of California, San Francisco"
}
],
"family": "Oskotsky",
"given": "Boris",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, Stanford University School of Medicine, Stanford, California"
}
],
"family": "Wong",
"given": "Ronald J.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, Stanford University School of Medicine, Stanford, California"
},
{
"name": "Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, California"
},
{
"name": "Department of Biomedical Data Science, Stanford University School of Medicine, Stanford, California"
}
],
"family": "Aghaeepour",
"given": "Nima",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, University of California, San Francisco"
},
{
"name": "Bakar Computational Health Sciences Institute, University of California, San Francisco"
}
],
"family": "Sirota",
"given": "Marina",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Pediatrics, Stanford University School of Medicine, Stanford, California"
},
{
"name": "Center for Academic Medicine, Stanford University School of Medicine, Stanford, California"
}
],
"family": "Stevenson",
"given": "David K.",
"sequence": "additional"
}
],
"container-title": [
"JAMA Network Open"
],
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2021,
11,
15
]
],
"date-time": "2021-11-15T16:35:47Z",
"timestamp": 1636994147000
},
"deposited": {
"date-parts": [
[
2021,
11,
15
]
],
"date-time": "2021-11-15T16:35:57Z",
"timestamp": 1636994157000
},
"indexed": {
"date-parts": [
[
2021,
11,
16
]
],
"date-time": "2021-11-16T10:40:04Z",
"timestamp": 1637059204295
},
"is-referenced-by-count": 0,
"issn-type": [
{
"type": "electronic",
"value": "2574-3805"
}
],
"issue": "11",
"issued": {
"date-parts": [
[
2021,
11,
15
]
]
},
"journal-issue": {
"issue": "11",
"published-print": {
"date-parts": [
[
2021,
11,
1
]
]
}
},
"language": "en",
"link": [
{
"URL": "https://jamanetwork.com/journals/jamanetworkopen/articlepdf/2786136/oskotsky_2021_oi_210938_1636051230.14579.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "10",
"original-title": [],
"page": "e2133090",
"prefix": "10.1001",
"published": {
"date-parts": [
[
2021,
11,
15
]
]
},
"published-online": {
"date-parts": [
[
2021,
11,
15
]
]
},
"publisher": "American Medical Association (AMA)",
"reference": [
{
"DOI": "10.1001/jama.2020.22760",
"article-title": "Fluvoxamine vs placebo and clinical deterioration in outpatients with symptomatic COVID-19: a randomized clinical trial.",
"author": "Lenze",
"doi-asserted-by": "publisher",
"first-page": "2292",
"issue": "22",
"journal-title": "JAMA",
"key": "zoi210938r2",
"volume": "324",
"year": "2020"
},
{
"DOI": "10.1093/ofid/ofab050",
"article-title": "Prospective cohort of fluvoxamine for early treatment of coronavirus disease 19.",
"author": "Seftel",
"doi-asserted-by": "publisher",
"first-page": "b050",
"issue": "2",
"journal-title": "Open Forum Infect Dis",
"key": "zoi210938r3",
"volume": "8",
"year": "2021"
},
{
"DOI": "10.3390/microorganisms9020339",
"article-title": "Fluoxetine can inhibit SARS-CoV-2 in vitro.",
"author": "Dechaumes",
"doi-asserted-by": "publisher",
"first-page": "339",
"issue": "2",
"journal-title": "Microorganisms",
"key": "zoi210938r4",
"volume": "9",
"year": "2021"
},
{
"DOI": "10.1038/s41598-021-85049-0",
"article-title": "The serotonin reuptake inhibitor fluoxetine inhibits SARS-CoV-2 in human lung tissue.",
"author": "Zimniak",
"doi-asserted-by": "publisher",
"first-page": "5890",
"issue": "1",
"journal-title": "Sci Rep",
"key": "zoi210938r5",
"volume": "11",
"year": "2021"
},
{
"DOI": "10.1016/j.biopha.2021.111437",
"article-title": "Fluoxetine as an anti-inflammatory therapy in SARS-CoV-2 infection.",
"author": "Creeden",
"doi-asserted-by": "crossref",
"journal-title": "Biomed Pharmacother",
"key": "zoi210938r6",
"volume": "138",
"year": "2021"
},
{
"DOI": "10.1016/j.cytogfr.2020.06.001",
"article-title": "SARS-CoV-2 infection: the role of cytokines in COVID-19 disease.",
"author": "Costela-Ruiz",
"doi-asserted-by": "publisher",
"first-page": "62",
"journal-title": "Cytokine Growth Factor Rev",
"key": "zoi210938r7",
"volume": "54",
"year": "2020"
},
{
"DOI": "10.4088/PCC.v05n0402",
"article-title": "Trends in prescribing of selective serotonin reuptake inhibitors and other newer antidepressant agents in adult primary care.",
"author": "Pirraglia",
"doi-asserted-by": "publisher",
"first-page": "153",
"issue": "4",
"journal-title": "Prim Care Companion J Clin Psychiatry",
"key": "zoi210938r8",
"volume": "5",
"year": "2003"
},
{
"DOI": "10.3389/fpsyt.2020.00035",
"article-title": "National prescription patterns of antidepressants in the treatment of adults with major depression in the US between 1996 and 2015: a population representative survey based analysis.",
"author": "Luo",
"doi-asserted-by": "publisher",
"first-page": "35",
"journal-title": "Front Psychiatry",
"key": "zoi210938r9",
"volume": "11",
"year": "2020"
},
{
"DOI": "10.4088/JCP.10r06218blu",
"article-title": "The pharmacologic treatment of anxiety disorders: a review of progress.",
"author": "Ravindran",
"doi-asserted-by": "publisher",
"first-page": "839",
"issue": "7",
"journal-title": "J Clin Psychiatry",
"key": "zoi210938r10",
"volume": "71",
"year": "2010"
},
{
"DOI": "10.1038/npp.2011.132",
"article-title": "The effect of antidepressant medication treatment on serum levels of inflammatory cytokines: a meta-analysis.",
"author": "Hannestad",
"doi-asserted-by": "publisher",
"first-page": "2452",
"issue": "12",
"journal-title": "Neuropsychopharmacology",
"key": "zoi210938r11",
"volume": "36",
"year": "2011"
},
{
"DOI": "10.1002/art.27304",
"article-title": "Fluoxetine and citalopram exhibit potent antiinflammatory activity in human and murine models of rheumatoid arthritis and inhibit toll-like receptors.",
"author": "Sacre",
"doi-asserted-by": "publisher",
"first-page": "683",
"issue": "3",
"journal-title": "Arthritis Rheum",
"key": "zoi210938r12",
"volume": "62",
"year": "2010"
},
{
"article-title": "Pharmacological inhibition of acid sphingomyelinase prevents uptake of SARS-CoV-2 by epithelial cells.",
"author": "Carpinteiro",
"issue": "8",
"journal-title": "Cell Rep Med",
"key": "zoi210938r13",
"volume": "1",
"year": "2020"
},
{
"DOI": "10.1016/j.jbc.2021.100701",
"article-title": "Inhibition of acid sphingomyelinase by ambroxol prevents SARS-CoV-2 entry into epithelial cells.",
"author": "Carpinteiro",
"doi-asserted-by": "crossref",
"journal-title": "J Biol Chem",
"key": "zoi210938r14",
"volume": "296",
"year": "2021"
},
{
"DOI": "10.3390/ijms22094794",
"article-title": "Metabolic signatures associated with severity in hospitalized COVID-19 patients.",
"author": "Marín-Corral",
"doi-asserted-by": "publisher",
"first-page": "4794",
"issue": "9",
"journal-title": "Int J Mol Sci",
"key": "zoi210938r15",
"volume": "22",
"year": "2021"
},
{
"article-title": "Association between FIASMAs and reduced risk of intubation or death in individuals hospitalized for severe COVID-19: an observational multicenter study.",
"author": "Hoertel",
"journal-title": "Clin Pharmacol Ther",
"key": "zoi210938r16"
},
{
"DOI": "10.1016/S2215-0366(20)30462-4",
"article-title": "Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62?354 COVID-19 cases in the USA.",
"author": "Taquet",
"doi-asserted-by": "publisher",
"first-page": "130",
"issue": "2",
"journal-title": "Lancet Psychiatry",
"key": "zoi210938r19",
"volume": "8",
"year": "2021"
},
{
"DOI": "10.1111/acps.v143.6",
"article-title": "Mental disorders, psychopharmacological treatments, and mortality in 2150 COVID-19 Spanish inpatients.",
"author": "Diez-Quevedo",
"doi-asserted-by": "publisher",
"first-page": "526",
"issue": "6",
"journal-title": "Acta Psychiatr Scand",
"key": "zoi210938r20",
"volume": "143",
"year": "2021"
},
{
"DOI": "10.1016/S0140-6736(07)61602-X",
"article-title": "The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.",
"author": "von Elm",
"doi-asserted-by": "publisher",
"first-page": "1453",
"issue": "9596",
"journal-title": "Lancet",
"key": "zoi210938r22",
"volume": "370",
"year": "2007"
},
{
"DOI": "10.1002/sim.v33.24",
"article-title": "The use of bootstrapping when using propensity-score matching without replacement: a simulation study.",
"author": "Austin",
"doi-asserted-by": "publisher",
"first-page": "4306",
"issue": "24",
"journal-title": "Stat Med",
"key": "zoi210938r24",
"volume": "33",
"year": "2014"
},
{
"DOI": "10.1016/j.jad.2015.03.021",
"article-title": "Dose equivalents of antidepressants: evidence-based recommendations from randomized controlled trials.",
"author": "Hayasaka",
"doi-asserted-by": "publisher",
"first-page": "179",
"journal-title": "J Affect Disord",
"key": "zoi210938r25",
"volume": "180",
"year": "2015"
},
{
"DOI": "10.1016/S2215-0366(19)30217-2",
"article-title": "Optimal dose of selective serotonin reuptake inhibitors, venlafaxine, and mirtazapine in major depression: a systematic review and dose-response meta-analysis.",
"author": "Furukawa",
"doi-asserted-by": "publisher",
"first-page": "601",
"issue": "7",
"journal-title": "Lancet Psychiatry",
"key": "zoi210938r26",
"volume": "6",
"year": "2019"
},
{
"DOI": "10.1016/j.mehy.2020.110140",
"article-title": "The possible immunoregulatory and anti-inflammatory effects of selective serotonin reuptake inhibitors in coronavirus disease patients.",
"author": "Hamed",
"doi-asserted-by": "crossref",
"journal-title": "Med Hypotheses",
"key": "zoi210938r28",
"volume": "144",
"year": "2020"
},
{
"DOI": "10.1016/j.jocn.2021.03.010",
"article-title": "Drug repurposing of selective serotonin reuptake inhibitors: could these drugs help fight COVID-19 and save lives?",
"author": "Pashaei",
"doi-asserted-by": "crossref",
"first-page": "163",
"issue": "0",
"journal-title": "J Clin Neurosci",
"key": "zoi210938r29",
"volume": "88",
"year": "2021"
},
{
"DOI": "10.1016/j.coph.2011.02.004",
"article-title": "5-HT and the immune system.",
"author": "Ahern",
"doi-asserted-by": "publisher",
"first-page": "29",
"issue": "1",
"journal-title": "Curr Opin Pharmacol",
"key": "zoi210938r30",
"volume": "11",
"year": "2011"
},
{
"article-title": "Peripheral alterations in cytokine and chemokine levels after antidepressant drug treatment for major depressive disorder: systematic review and meta-analysis.",
"author": "Köhler",
"first-page": "4195",
"issue": "5",
"journal-title": "Mol Neurobiol",
"key": "zoi210938r31",
"volume": "55",
"year": "2018"
},
{
"DOI": "10.1111/j.1749-6632.1995.tb32372.x",
"article-title": "Interleukin-6 serum levels in depressed patients before and after treatment with fluoxetine.",
"author": "Sluzewska",
"doi-asserted-by": "publisher",
"first-page": "474",
"issue": "1",
"journal-title": "Ann N Y Acad Sci",
"key": "zoi210938r32",
"volume": "762",
"year": "1995"
},
{
"DOI": "10.1016/j.ejphar.2014.01.064",
"article-title": "Interaction of new antidepressants with sigma-1 receptor chaperones and their potentiation of neurite outgrowth in PC12 cells.",
"author": "Ishima",
"doi-asserted-by": "publisher",
"first-page": "167",
"journal-title": "Eur J Pharmacol",
"key": "zoi210938r33",
"volume": "727",
"year": "2014"
},
{
"DOI": "10.1016/S0924-8579(99)00157-0",
"article-title": "Inhibition of HIV replication by neuroleptic agents and their potential use in HIV infected patients with AIDS related dementia.",
"author": "Kristiansen",
"doi-asserted-by": "publisher",
"first-page": "209",
"issue": "3",
"journal-title": "Int J Antimicrob Agents",
"key": "zoi210938r34",
"volume": "14",
"year": "2000"
},
{
"DOI": "10.1128/AAC.00983-12",
"article-title": "Fluoxetine is a potent inhibitor of coxsackievirus replication.",
"author": "Zuo",
"doi-asserted-by": "publisher",
"first-page": "4838",
"issue": "9",
"journal-title": "Antimicrob Agents Chemother",
"key": "zoi210938r35",
"volume": "56",
"year": "2012"
},
{
"DOI": "10.1038/s41380-021-01021-4",
"article-title": "Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: results from an observational study.",
"author": "Hoertel",
"doi-asserted-by": "crossref",
"key": "zoi210938r1",
"volume-title": "Mol Psychiatry"
},
{
"DOI": "10.1101/2021.02.18.21251997",
"doi-asserted-by": "crossref",
"key": "zoi210938r17",
"unstructured": "Hoertel? N, Sánchez-Rico? M, Gulbins? E, . Association between psychotropic medications functionally inhibiting acid sphingomyelinase and reduced risk of intubation or death among individuals with mental disorder and severe COVID-19: an observational study.? medRxiv. Preprint posted online February 20, 2021. doi:10.1101/2021.02.18.21251997"
},
{
"DOI": "10.1002/wps.20806",
"doi-asserted-by": "crossref",
"key": "zoi210938r18",
"unstructured": "Wang QQ, Xu R, Volkow ND. Increased risk of COVID-19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry. Published online October 7, 2020. Accessed September 3, 2021. https://onlinelibrary.wiley.com/doi/full/10.1002/wps.20806"
},
{
"DOI": "10.1101/2021.04.24.21256029",
"doi-asserted-by": "crossref",
"key": "zoi210938r21",
"unstructured": "Günster? C, Busse? R, Spoden? M, . 6-Month follow up of 8679 hospitalized COVID-19 patients in Germany: a nationwide cohort study.? medRxiv. Preprint posted online April 24, 2012. doi:10.1101/2021.04.24.21256029"
},
{
"key": "zoi210938r23",
"unstructured": "ICD-10 Version:2019. Updated April 16, 2020. Accessed August 9, 2021. https://icd.who.int/browse10/2019/en#/U07.1"
},
{
"key": "zoi210938r27",
"unstructured": "CDC/National Center for Health Statistics. Antidepressant use among adults: United States, 2015-2018. September 8, 2020. Accessed September 3, 2021. https://www.cdc.gov/nchs/products/databriefs/db377.htm"
}
],
"reference-count": 35,
"references-count": 35,
"relation": {},
"score": 1,
"short-container-title": [
"JAMA Netw Open"
],
"short-title": [],
"source": "Crossref",
"subject": [
"General Medicine"
],
"subtitle": [],
"title": [
"Mortality Risk Among Patients With COVID-19 Prescribed Selective Serotonin Reuptake Inhibitor Antidepressants"
],
"type": "journal-article",
"volume": "4"
}