Mega doses of retinol: A possible immunomodulation in Covid-19 illness in resource-limited settings
et al., Reviews in Medical Virology, doi:10.1002/rmv.2204, Dec 2020
Vitamin A for COVID-19
49th treatment shown to reduce risk in
May 2023, now with p = 0.004 from 14 studies.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

Review of the potential benefits of vitamin A for COVID-19, including the effect of vitamin A on ACE2 expression in the respiratory tract, potentially improving the generation of protective immune responses to vaccines, and dosage and safety analysis.
{kind=link}
1.
Younes, S., The influence of micronutrients on olfactory dysfunction associated with COVID-19 and long COVID, Next Research, doi:10.1016/j.nexres.2026.101727.
2.
Al-Khrasani et al., Do vitamins halt the COVID-19-evoked pro-inflammatory cytokines involved in the development of neuropathic pain?, Biomedicine & Pharmacotherapy, doi:10.1016/j.biopha.2025.118346.
3.
Sanduzzi Zamparelli et al., Immune-Boosting and Antiviral Effects of Antioxidants in COVID-19 Pneumonia: A Therapeutic Perspective, Life, doi:10.3390/life15010113.
4.
DiGuilio et al., Micronutrient Improvement of Epithelial Barrier Function in Various Disease States: A Case for Adjuvant Therapy, International Journal of Molecular Sciences, doi:10.3390/ijms23062995.
5.
Stephensen et al., Vitamin A in resistance to and recovery from infection: relevance to SARS-CoV2, British Journal of Nutrition, doi:10.1017/S0007114521000246.
Midha et al., 31 Dec 2020, peer-reviewed, 4 authors.
Mega doses of retinol: A possible immunomodulation in Covid‐19 illness in resource‐limited settings
Reviews in Medical Virology, doi:10.1002/rmv.2204
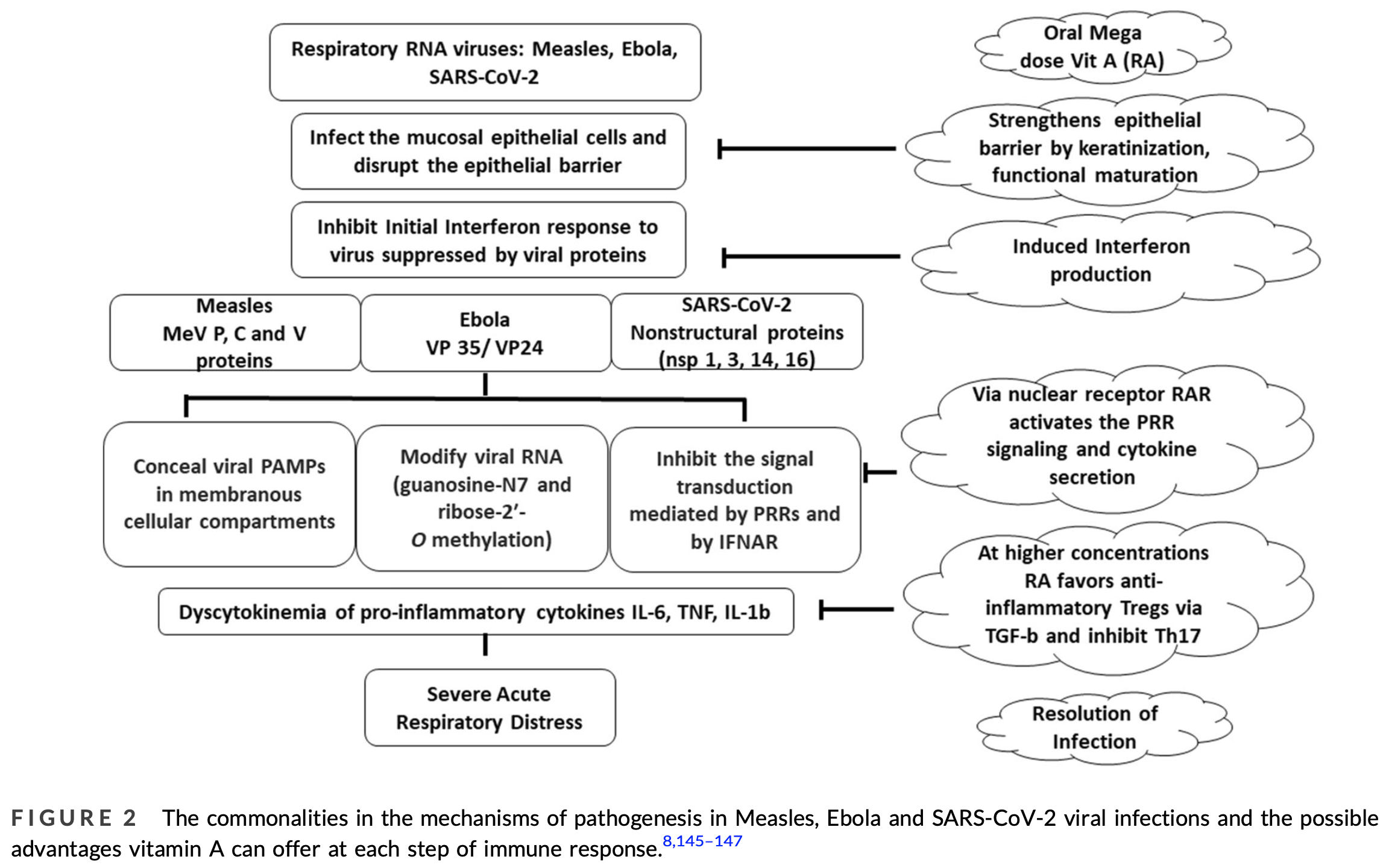
Of all the nutrients, vitamin A has been the most extensively evaluated for its impact on immunity. There are three main forms of vitamin A, retinol, retinal and retinoic acid (RA) with the latter being most biologically active and all-trans-RA (ATRA) its main derivative. Vitamin A is a key regulator of the functions of various innate and adaptive immune cells and promotes immune-homeostasis. Importantly, it augments the interferon-based innate immune response to RNA viruses decreasing RNA virus replication. Several clinical trials report decreased mortality in measles and Ebola with vitamin A supplementation. During the Covid-19 pandemic interventions such as convalescent plasma, antivirals, monoclonal antibodies and immunomodulator drugs have been tried but most of them are difficult to implement in resource-limited settings. The current review explores the possibility of mega dose vitamin A as an affordable adjunct therapy for Covid-19 illness with minimal reversible side effects. Insight is provided into the effect of vitamin A on ACE-2 expression in the respiratory tract and its association with the prognosis of Covid-19 patients. Vitamin A supplementation may aid the generation of protective immune response to Covid-19 vaccines. An overview of the dosage and safety profile of vitamin A is presented along with recommended doses for prophylactic/therapeutic use in randomised controlled trials in Covid-19 patients.
CONFLICT OF INTEREST All the authors declare that there is no conflict of interest.
AUTHOR CONTRIBUTIONS Ish K. Midha conceived the idea for the review and prepared the draft. Nilesh Kumar and Amit Kumar contributed to the draft with respect to role of vitamin A in recognition of RNA viruses and impact of Vitamin A on ACE-2 and prognosis of Covid-19 patients respectively. Taruna Madan contributed to the draft for immunemodulatory role of vitamin A and preparation of the figures.
References
Ahmad, Haskell, Raqib, Stephensen, Markers of innate immune function are associated with vitamin a stores in men, J Nutr
Allen, Britton, Leonardi-Bee, Association between antioxidant vitamins and asthma outcome measures: systematic review and meta-analysis, Thorax
Aluisio, Perera, Yam, Vitamin A supplementation was associated with reduced mortality in patients with Ebola virus disease during the West African outbreak, J Nutr
Amanna, Balancing the efficacy and safety of vaccines in the elderly, Open Longev Sci
Andersen, Rambaut, Lipkin, Holmes, Garry, The proximal origin of SARS-CoV-2, Nat Med
Arnhold, Nau, Meyer, Rothkoetter, Lampen, Porcine intestinal metabolism of excess vitamin A differs following vitamin A supplementation and liver consumption, J Nutr
Baena, Campoy, Bayes, Blanca, Fernandez et al., Vitamin A, retinol binding protein and lipids in type 1 diabetes mellitus, Eur J Clin Nutr
Balmer, Blomhoff, Gene expression regulation by retinoic acid, J Lipid Res
Barclay, Foster, Sommer, Vitamin A supplements and mortality related to measles: a randomised clinical trial, Br Med J
Basu, Tze, Leichter, Serum vitamin A and retinol-binding protein in patients with insulin-dependent diabetes mellitus, Am J Clin Nutr
Behm, Blumberg, Bush, Personalized Nutrition and the COVID-19 Era: Prepared by the Personalized Nutrition &COVID-19 Task Force of the American Nutrition Association
Benn, Combining vitamin A and vaccines: convenience or conflict?, Dan Med J
Bichon, Aubry, Benarous, Case report: ribavirin and vitamin A in a severe case of measles, Medicine
Biesalski, Stofft, Wellner, Niederauer, Bässler, Vitamin A and ciliated cells. I. Respiratory epithelia, Z Ernahrungswiss
Bixler, Goff, The role of cytokines and chemokines in filovirus infection, Viruses
Bowman, Goonewardene, Pasatiempo, Ross, Taylor, Vitamin A deficiency decreases natural killer cell activity and interferon production in rats, J Nutr
Bozkurt, Kovacs, Harrington, HFSA/ACC/AHA Statement Addresses Concerns Re: Using RAAS Antagonists in COVID-19, American College of Cardiology
Brown, Esterhazy, Sarde, Retinoic acid is essential for Th1 cell lineage stability and prevents transition to a Th17 cell program, Immunity
Buonaguro, Ascierto, Morse, Covid-19: time for a paradigm change, Rev Med Virol
Butler, Havens, Day, Measles severity and serum retinol (vitamin A) concentration among children in the United States, Pediatrics
Böcher, Wallasch, Höhler, Galle, All-trans retinoic acid for treatment of chronic hepatitis C, Liver Int
Caldeira, Alarcão, Vaz-Carneiro, Costa, Risk of pneumonia associated with use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers: systematic review and metaanalysis, BMJ
Channappanavar, Fehr, Vijay, Dysregulated type I interferon and inflammatory monocyte-macrophage responses cause lethal pneumonia in SARS-CoV-infected mice, Cell Host Microbe
Channappanavar, Fehr, Zheng, IFN-I response timing relative to virus replication determines MERS coronavirus infection outcomes, J Clin Invest
Chen, Esplin, Garrett, Welner, Webb et al., Retinoids accelerate B lineage lymphoid differentiation, J Immunol
Chen, Liu, Liu, Zhonghuajie he he hu
Chen, Ross, Retinoic acid promotes mouse splenic B cell surface IgG expression and maturation stimulated by CD40 and IL-4, Cell Immunol
Cheung, Poon, Ng, Cytokine responses in severe acute respiratory syndrome coronavirus-infected macrophages in vitro: possible relevance to pathogenesis, J Virol
Chousterman, Swirski, Weber, Cytokine storm and sepsis disease pathogenesis, Seminars Immunopathol
Chu, Chan, Wang, Comparative replication and immune activation profiles of SARS-CoV-2 and SARS-CoV in human lungs: an ex vivo study with implications for the pathogenesis of COVID-19, Clin Infect Dis, doi:10.1093/cid/ciaa410
Coombes, Siddiqui, Arancibia-Cárcamo, A functionally specialized population of mucosal CD103+ DCs induces Foxp3+ regulatory T cells via a TGF-beta and retinoic aciddependent mechanism, J Exp Med
Coutsoudis, Broughton, Coovadia, Vitamin A supplementation reduces measles morbidity in young African children: a randomized, placebo-controlled, double-blind trial, Am J Clin Nutr
Coutsoudis, Kiepiela, Coovadia, Broughton, Vitamin A supplementation enhances specific IgG antibody levels and total lymphocyte numbers while improving morbidity in measles, Pediatr Infect Dis J
Cárdenas, Loo, Gale, Ebola virus VP35 protein binds double-stranded RNA and inhibits alpha/beta interferon production induced by RIG-I signaling, J Virol
Davidson, Maini, Wack, Disease-promoting effects of type I interferons in viral, bacterial, and coinfections, J Interferon Cytokine Res
Desimone, Position Statement of the ESC Council on Hypertension on ACE-Inhibitors and Angiotensin Receptor Blockers
Diaz, Hypothesis: angiotensin-converting enzyme inhibitors and angiotensin receptor blockers may increase the risk of severe COVID-19, J Travel Med
Dollimore, Cutts, Binka, Ross, Morris et al., Measles incidence, case fatality, and delayed mortality in children with or without vitamin A supplementation in rural Ghana, Am J Epidemiol
Elkazzaz, Haydara, Abdelaal, Assessment the Activity Value of 13-cis-Retinoic Acid (Isotretinoin) in the Treatment of COVID-19
Ellison, Intensive vitamin therapy in measles, Br Med J
Ema Advises, Continued Use of Medicines for Hypertension
Fujii, Miyahara, Taniguchi, Effect of a retinoid X receptor partial agonist on airway inflammation and hyperresponsiveness in a murine model of asthma, Respir Res
Furuse, Suzuki, Oshitani, Origin of measles virus: divergence from rinderpest virus between the 11th and 12th centuries, Virol J
García-Sastre, Biron, Type 1 interferons and the virus-host relationship: a lesson in detente, Science
Geissmann, Revy, Brousse, Retinoids regulate survival and antigen presentation by immature dendritic cells, J Exp Med
Gheblawi, Wang, Viveiros, Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the reninangiotensin system: celebrating the 20th anniversary of the discovery of ACE 2, Circ Res
Goverse, Labao-Almeida, Ferreira, Vitamin A controls the presence of RORγ+ innate lymphoid cells and lymphoid tissue in the small intestine, J Immunol
Green, Mellanby, Vitamin A as an anti-infective agent, Br Med J
Griffin, The immune response in measles: virus control, clearance and protective immunity, Viruses
Gundra, Girgis, Gonzalez, Vitamin A mediates conversion of monocyte-derived macrophages into tissue-resident macrophages during alternative activation, Nat Immunol
Hall, Grainger, Spencer, Belkaid, The role of retinoic acid in tolerance and immunity, Immunity
Ho, Hofs, Elisia, All trans retinoic acid, transforming growth factor β and prostaglandin E2 in mouse plasma synergize with basophil-secreted interleukin-4 to M2 polarize murine macrophages, PLoS One
Hoffmann, Kleine-Weber, Schroeder, SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor, Cell, doi:10.1016/j.cell.2020.02.052e8
Huang, Wang, Li, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China, Lancet
Hughes, ACE inhibitors protective against severe COVID-19
Hussey, Klein, A randomized, controlled trial of vitamin A in children with severe measles, N Engl J Med
Imai, Kuba, Penninger, The discovery of angiotensin-converting enzyme 2 and its role in acute lung injury in mice, Exp Physiol
Indrevaer, Moskaug, Paur, IRF4 is a critical gene in retinoic acid-mediated plasma cell formation and is deregulated in common variable immunodeficiency-derived B cells, J Immunol
Inua, Duggan, West, Post-measles corneal ulceration in children in northern Nigeria: the role of vitamin A, malnutrition and measles, Ann Trop Paediatr
Jee, Hoet, Azevedo, Effects of dietary vitamin A content on antibody responses of feedlot calves inoculated intramuscularly with an inactivated bovine coronavirus vaccine, Am J Vet Res
Jia, Pulmonary angiotensin-converting enzyme 2 (ACE2) and inflammatory lung disease, Shock
Johansen, Dewald, Shoemaker, A screen of approved drugs and molecular probes identifies therapeutics with anti-Ebola virus activity, Sci Transl Med
Kang, Chung, Kim, Kang, Choe et al., Retinoidmediated inhibition of interleukin-12 production in mouse macrophages suppresses Th1 cytokine profile in CD4(+) T cells, Br J Pharmacol
Karanth, Marupudi, Gupta, Rau, Fatal measles presenting as acute respiratory distress syndrome in an immunocompetent adult, Case Rep
Karrer, Morf, Schöpp, Zurkenntnis des vitamins-A ausfischtranen, Helv Chim Acta
Kawaguchi, Zhong, Kassai, Ter-Stepanian, Sun, Vitamin A transport mechanism of the multitransmembrane cell-surface receptor STRA6, Membranes
Kawasaki, Hosoya, Katayose, Suzuki, The efficacy of oral vitamin A supplementation for measles and respiratory syncytial virus (RSV) infection. Kansenshogakuzasshi, J Jpn Assoc Infect Dis
Kesel, Huang, Murray, Retinazone inhibits certain blood-borne human viruses including Ebola virus Zaire, Antivir Chem Chemother
Kheirouri, Alizadeh, Decreased serum and mucosa immunoglobulin A levels in vitamin Aand zinc-deficient mice, Centr Eur J Immunol
Kim, Taparowsky, Kim, Retinoicacid differentially regulates the migration of innate lymphoid cell subsets to the gut, Immunity
Kligman, Mills, Leyden, Gross, Allen et al., Oral vitamin A in acne vulgaris Preliminary report, Int J Dermatol
Konjevic, Mirjacic-Martinovic, Vuletic, Babovic, In vitro increased natural killer cell activity of metastatic melanoma patients MIDHA ET AL. with interferon-α alone as opposed to its combination with 13-cis retinoic acid is associated with modulation of NKG2D and CD161 activating receptor expression, J BUON
Lau, Lau, Chan, Delayed induction of proinflammatory cytokines and suppression of innate antiviral response by the novel Middle East respiratory syndrome coronavirus: implications for pathogenesis and treatment, J Gen Virol
Law, Cheung, Ng, Chemokine up-regulation in sars-coronavirus-infected, monocyte-derived human dendritic cells, Blood
Lee, Hu, Chen, Huang, Hsueh, Are children less susceptible to COVID-19?, J Microbiol Immunol Infect
Lee, Ko, New perspectives regarding the antiviral effect of vitamin A on norovirus using modulation of gut microbiota, Gut Microb
Li, He, Wang, All-trans retinoic acid negatively regulates cytotoxic activities of nature killer cell line 92, Biochem Biophys Res Commun
Li, Hu, Su, Dai, Hypokalemia and Clinical Implications in Patients with Coronavirus Disease, doi:10.1101/2020.02.27.20028530v1
Li, Zhao, Liu, Zhang, Liu et al., Clinical report of serious complications associated with measles pneumonia in children hospitalized at Shengjing hospital, China, J Infect Dev Ctries
Loganathan, Schleicher, Malik, Rare driver mutations in head and neck squamous cell carcinomas converge on NOTCH signaling, Science, doi:10.1126/science.aax0902
Long, Tang, Shi, Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections, Nat Med
Lopes, Macedo, De, Silva, Continuing versus suspending angiotensin-converting enzyme inhibitors and angiotensin receptor blockers: impact on adverse outcomes in hospitalized patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)--The BRACE CORONA Trial, Am Heart J
Ma, Chen, Ross, Retinoic acid and polyriboinosinic: polyribocytidylic acid stimulate robust anti-tetanus antibody production while differentially regulating type 1/type 2 cytokines and lymphocyte populations, J Immunol
Ma, Ross, The anti-tetanus immune response of neonatal mice is augmented by retinoic acid combined with polyriboinosinic: polyribocytidylic acid, Proc Natl Acad Sci
Maciaszek, Coniglio, Talmage, Viglianti, Retinoidinduced repression of human immunodeficiency virus type 1 core promoter activity inhibits virus replication, J Virol
Manicassamy, Ravindran, Deng, Toll-like receptor 2-dependent induction of vitamin A-metabolizing enzymes in dendritic cells promotes T regulatory responses and inhibits autoimmunity, Nat Med
Markowitz, Nzilambi, Driskell, Vitamin A levels and mortality among hospitalized measles patients, Kinshasa, Zaire, J Trop Pediatr
Marquez, Cardoso, Vitamin A-retinoid signaling in pulmonary development and disease, Mol Cell Pediatr
Mccollum, Davis, The essential factors in the diet during growth, J Biol Chem
Mccullough, Clewes, Thurnham, The effect of vitamin A on epithelial integrity, Proc Nutr Soc
Mcgill, Kelly, Guerra-Maupome, Vitamin A deficiency impairs the immune response to intranasal vaccination and RSV infection in neonatal calves, Sci Rep
Mehta, Mcqueen, Tucker, Pandita, Aggarwal, Inhibition by all-trans-retinoic acid of tumor necrosis factor and nitric oxide production by peritoneal macrophages, J Leukoc Biol
Mellanby, On diet and disease. With special reference to the teeth, lungs, and pre-natal feeding, Br Med J
Midha, Kumar, Kumar, Madan, Mega doses of retinol: A possible immunomodulation in Covid-19 illness in resource-limited settings, Rev Med Virol
Mora, Iwata, Von Andrian, Vitamin effects on the immune system: vitamins A and D take centre stage, Nat Rev Immunol
Na, Kang, Chung, Retinoids inhibit interleukin-12 production in macrophages through physical associations of retinoid X receptor and NFκB, J Biol Chem
Nicholls, Peiris, Good ACE, bad ACE do battle in lung injury, SARS, Nat Med
Ogaro, Orinda, Onyango, Black, Effect of vitamin A on diarrhoeal and respiratory complications of measles. TGM, Trop Geogr Med)
Olivares, Hertrampf, Capurro, Wegner, Prevalence of anemia in elderly subjects living at home: role of micronutrient deficiency and inflammation, Eur J Clin Nutr
Oliveira, Teixeira, Sato, Impact of retinoic acid on immune cells and inflammatory diseases, Mediat Inflamm, doi:10.1155/2018/3067126
Olson, Shah, Vitamin, toxicity
Olson, Vitamin A
Ortacersoy, Tanriover, Ocal, Ozisik, Inkaya et al., Severe measles pneumonia in adults with respiratory failure: role of ribavirin and high-dose vitamin A, Clin Respir J
Pal, Bhansali, COVID-19, diabetes mellitus and ACE 2: the conundrum, Diabetes Res Clin Pract
Paranjpe, Newton, Pyott, Nutritional disorders in Cornea
Patel, Verma, COVID-19 and angiotensin-converting enzyme inhibitors and angiotensin receptor blockers: what is the evidence?, J Am Med Assoc
Penkert, Jones, Häcker, Partridge, Hurwitz, Vitamin A differentially regulates cytokine expression in respiratory epithelial and macrophage cell lines, Cytokine
Penniston, Tanumihardjo, The acute and chronic toxic effects of vitamin A, Am J Clin Nutr
Reddy, Bhaskaram, Raghuramulu, Relationship between measles, malnutrition, and blindness: a prospective study in Indian children, Am J Clin Nutr
Rockx, Baas, Zornetzer, Early upregulation of acute respiratory distress syndrome-associated cytokines promotes lethal disease in an aged-mouse model of severe acute respiratory syndrome coronavirus infection, J Virol
Rosales, Kjolhede, A single 210-µmol oral dose of retinol does not enhance the immune response in children with measles, J Nutr
Rosales, Kjolhede, Goodman, Efficacy of a single oral dose of 200,000 IU of oil-soluble vitamin A in measles-associated morbidity, Am J Epidemiol
Rosales, Ritter, Zolfaghari, Smith, Ross, Effects of acute inflammation on plasma retinol, retinol-binding protein, and its mRNA in the liver and kidneys of vitamin A-sufficient rats, J. Lipid Res
Rudraraju, Jones, Surman, Sealy, Thomas et al., Respiratory tract epithelial cells express retinaldehyde dehydrogenase ALDH1A and enhance IgA production by stimulated B cells in the presence of vitamin A, PLoS One, doi:10.1371/journal.pone.0086554
Ruiter, Patil, Shreffler, Vitamins A and D have antagonistic effects on expression of effector cytokines and gut-homing integrin in human innate lymphoid cells, Clin Exp Allergy
Rupp, Schwartz, Bechard, Measles pneumonia: treatment of a near-fatal case with corticosteroids and vitamin A, Chest
Sakamoto, Koya, Tsukioka, The effects of all-trans retinoic acid on the induction of oral tolerance in a murine model of bronchial asthma, Int Arch Allergy Immunol
Schuster, Kenyon, Stephensen, Vitamin A deficiency decreases and high dietary vitamin A increases disease severity in the mouse model of asthma, J Immunol
Scrimshaw, Taylor, Gordon, Interactions of nutrition and infection. Geneva: World Health Organization, Monogr Ser World Health Organ
Semba, Semba, The Vitamin A Story -Lifting the Shadow of the Death, World Rev Nutr Diet
Semba, Vitamin A and immunity to viral, bacterial and protozoan infections, Proc Nutr Soc
Semba, Vitamin A as "anti-infective" therapy, 1920-1940, J Nutr
Shaw, Goldstein, Montgomery, Age-dependent dysregulation of innate immunity, Nature Rev Immunol
Sheldon, Netherlands faces measles epidemic, Br Med J
Shin, Mukherjee, Grewe, Papain-like protease regulates SARS-CoV-2 viral spread and innate immunity, Nature, doi:10.1038/s41586-020-2601-5
Shrestha, Kim, Yun, Retinoic acid induces hypersegmentation and enhances cytotoxicity of neutrophils against cancer cells, Immunol Lett
Shrivastava, Shrivastava, Ramasamy, Measles in India: challenges & recent developments, Infect Ecol Epidemiol
Siddiqui, Powrie, CD103+ GALT DCs promote Foxp3+ regulatory T cells, Mucosal Immunol
Smits, Lang, Van Den, Brand, Exacerbated innate host response to SARS-CoV in aged non-human primates, PLoS Pathog
Soderlund, Fex, Nilsson-Ehle, Concentrations of retinoids in early pregnancy and in newborns and their mothers, Am J Clin Nutr
Soroosh, Doherty, Duan, Lung-resident tissue macrophages generate Foxp3+ regulatory T cells and promote airway tolerance, J Exp Med
Soye, Trottier, Lenardo, In vitro inhibition of mumps virus by retinoids, Virol J
Stephensen, Borowsky, Lloyd, Disruption of Rxra gene in thymocytes and T lymphocytes modestly alters lymphocyte frequencies, proliferation, survival and T helper type 1/type 2 balance, Immunology
Stock, Booth, Cerundolo, Prostaglandin E2 suppresses the differentiation of retinoic acid-producing dendritic cells in mice and humans, J Exp Med
Surman, Jones, Sealy, Rudraraju, Hurwitz, Oral retinyl palmitate or retinoic acid corrects mucosal IgA responses toward an intranasal influenza virus vaccine in vitamin A deficient mice, Vaccine
Suzuki, Maruya, Kawamoto, The sensing of environmental stimuli by follicular dendritic cells promotes immunoglobulin A generation in the gut, Immunity
Tagarro, Epalza, Santos, Screening and severity of coronavirus disease 2019 (COVID-19) in children in Madrid, Spain, JAMA Pediatr
Thoms, Buschauer, Ameismeier, Structural basis for translational shutdown and immune evasion by the Nsp1 protein of SARS-CoV-2, Science, doi:10.1126/science.abc8665
Thorlund, Dron, Park, Hsu, Forrest et al., A real-time dashboard of clinical trials for COVID-19, Lancet Digital Health
Tikellis, Thomas, Angiotensin-converting enzyme 2 (ACE 2) is a key modulator of the renin angiotensin system in health and disease, Int J Pept
Trottier, Chabot, Mann, Retinoids inhibit measles virus in vitro via nuclear retinoid receptor signaling pathways, Antivir Res
Turpin, Vargo, Meltzer, Enhanced HIV-1 replication in retinoid-treated monocytes: retinoid effects mediated through mechanisms related to cell differentiation and to a direct transcriptional action on viral gene expression, J Immunol
Uematsu, Fujimoto, Jang, Regulation of humoral and cellular gut immunity by lamina propria dendritic cells expressing Toll-like receptor 5, Nat Immunol
Van De Pavert, Ferreira, Domingues, Maternal retinoids control type 3 innate lymphoid cells and set the offspring immunity, Nature
Van Der Loo, Labugger, Aebischer, Age-related changes of vitamin A status, J Cardiovasc Pharmacol
Varghese, Tsolaki, Yasmin, Host-pathogen interaction in COVID-19: pathogenesis, potential therapeutics and vaccination strategies, Immunobiology
Villamor, Fawzi, Effects of vitamin A supplementation on immune responses and correlation with clinical outcomes, Clin Microbiol Rev
Wang, Allen, Ballow, Retinoic acid enhances the production of IL-10 while reducing the synthesis of IL-12 and TNF-α from LPSstimulated monocytes/macrophages, J Clin Immunol
Wang, Ballow, The effects of retinoic acid on in vitro immunoglobulin synthesis by cord blood and adult peripheral blood mononuclear cells, Cell Immunol
Wilkinson, Trial of inhaled anti-viral (SNG001) for SARS-CoV-2 (COVID-19) infection
Wu, Zhang, Liu, Zhong, Xia, All-trans retinoic acid attenuates airway inflammation by inhibiting Th2 and Th17 response in experimental allergic asthma, BMC Immunol
Xiao, Korn, Retinoic acid increases Foxp3+ regulatory T cells and inhibits development of Th17 cells by enhancing TGF-beta-driven Smad3 signaling and inhibiting IL-6 and IL-23 receptor expression, J Immunol
Yang, Mao, Wan, Vitamin A for treating measles in children, Cochrane Database Syst Rev
Yang, Yang, Du, Retinoic acid promotes the endogenous repair of lung stem/progenitor cells in combined with simvastatin after acute lung injury: a stereological analysis, Resp Res
Yokota, Takeuchi, Maeda, GM-CSF and IL-4 synergistically trigger dendritic cells to acquire retinoic acid-producing capacity, Int Immunol
Zhang, Zhu, Cai, Association of inpatient use of angiotensin converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID-19, Circ Res
Zhong, Huang, Yang, Upregulation of angiotensinconverting enzyme 2 by all-trans retinoic acid in spontaneously hypertensive rats, Hypertension
Zhou, Ou, Rong, Drummen, Effect of all-trans retinoic acid treatment on prohibitin and renin-angiotensin-aldosterone system expression in hypoxia-induced renal tubular epithelial cell injury, J Renin Angiotensin Aldosterone Syst
DOI record:
{
"DOI": "10.1002/rmv.2204",
"ISSN": [
"1052-9276",
"1099-1654"
],
"URL": "http://dx.doi.org/10.1002/rmv.2204",
"abstract": "<jats:title>Summary</jats:title><jats:p>Of all the nutrients, vitamin A has been the most extensively evaluated for its impact on immunity. There are three main forms of vitamin A, retinol, retinal and retinoic acid (RA) with the latter being most biologically active and all‐trans‐RA (ATRA) its main derivative. Vitamin A is a key regulator of the functions of various innate and adaptive immune cells and promotes immune‐homeostasis. Importantly, it augments the interferon‐based innate immune response to RNA viruses decreasing RNA virus replication. Several clinical trials report decreased mortality in measles and Ebola with vitamin A supplementation.During the Covid‐19 pandemic interventions such as convalescent plasma, antivirals, monoclonal antibodies and immunomodulator drugs have been tried but most of them are difficult to implement in resource‐limited settings. The current review explores the possibility of mega dose vitamin A as an affordable adjunct therapy for Covid‐19 illness with minimal reversible side effects. Insight is provided into the effect of vitamin A on ACE‐2 expression in the respiratory tract and its association with the prognosis of Covid‐19 patients. Vitamin A supplementation may aid the generation of protective immune response to Covid‐19 vaccines. An overview of the dosage and safety profile of vitamin A is presented along with recommended doses for prophylactic/therapeutic use in randomised controlled trials in Covid‐19 patients.</jats:p>",
"alternative-id": [
"10.1002/rmv.2204"
],
"assertion": [
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Received",
"name": "received",
"order": 0,
"value": "2020-10-16"
},
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Accepted",
"name": "accepted",
"order": 1,
"value": "2020-12-01"
},
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Published",
"name": "published",
"order": 2,
"value": "2020-12-31"
}
],
"author": [
{
"ORCID": "http://orcid.org/0000-0003-3363-7297",
"affiliation": [
{
"name": "Pentamed Hospital New Delhi India"
}
],
"authenticated-orcid": false,
"family": "Midha",
"given": "Ish K.",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Saint Vincent Hospital Worcester Massachusetts USA"
}
],
"family": "Kumar",
"given": "Nilesh",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Dwight D. Eisenhower VA Medical Center Leavenworth Kansas USA"
}
],
"family": "Kumar",
"given": "Amit",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Innate Immunity ICMR‐National Institute for Research in Reproductive Health Mumbai India"
}
],
"family": "Madan",
"given": "Taruna",
"sequence": "additional"
}
],
"container-title": "Reviews in Medical Virology",
"container-title-short": "Reviews in Medical Virology",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"onlinelibrary.wiley.com"
]
},
"created": {
"date-parts": [
[
2020,
12,
31
]
],
"date-time": "2020-12-31T22:33:27Z",
"timestamp": 1609454007000
},
"deposited": {
"date-parts": [
[
2023,
8,
29
]
],
"date-time": "2023-08-29T17:28:38Z",
"timestamp": 1693330118000
},
"indexed": {
"date-parts": [
[
2024,
5,
7
]
],
"date-time": "2024-05-07T19:36:10Z",
"timestamp": 1715110570312
},
"is-referenced-by-count": 19,
"issue": "5",
"issued": {
"date-parts": [
[
2020,
12,
31
]
]
},
"journal-issue": {
"issue": "5",
"published-print": {
"date-parts": [
[
2021,
9
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://onlinelibrary.wiley.com/termsAndConditions#vor",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2020,
12,
31
]
],
"date-time": "2020-12-31T00:00:00Z",
"timestamp": 1609372800000
}
}
],
"link": [
{
"URL": "https://onlinelibrary.wiley.com/doi/pdf/10.1002/rmv.2204",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://onlinelibrary.wiley.com/doi/full-xml/10.1002/rmv.2204",
"content-type": "application/xml",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://onlinelibrary.wiley.com/doi/pdf/10.1002/rmv.2204",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "311",
"original-title": [],
"page": "1-14",
"prefix": "10.1002",
"published": {
"date-parts": [
[
2020,
12,
31
]
]
},
"published-online": {
"date-parts": [
[
2020,
12,
31
]
]
},
"published-print": {
"date-parts": [
[
2021,
9
]
]
},
"publisher": "Wiley",
"reference": [
{
"key": "e_1_2_12_2_1",
"unstructured": "Rolling updates on coronavirus disease (COVID‐19).https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen. Updated June 03 2020; Cited June 06 2020."
},
{
"key": "e_1_2_12_3_1",
"volume-title": "Preparedness and Response Plan for Novel Infectious Disease of Public Health Significance",
"year": "2020"
},
{
"key": "e_1_2_12_4_1",
"unstructured": "Coronavirus.https://www.who.int/health-topics/coronavirus#tab=tab_1. Cited June 06 2020."
},
{
"DOI": "10.1016/j.jmii.2020.02.011",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_5_1"
},
{
"article-title": "Screening and severity of coronavirus disease 2019 (COVID‐19) in children in Madrid, Spain",
"author": "Tagarro A",
"first-page": "e201346",
"journal-title": "JAMA Pediatr",
"key": "e_1_2_12_6_1",
"year": "2020"
},
{
"key": "e_1_2_12_7_1",
"unstructured": "R&D Blueprint and COVID‐19.https://www.who.int/teams/blueprint/Covid-19. Cited June 06 2020."
},
{
"DOI": "10.1016/S2589-7500(20)30086-8",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_8_1"
},
{
"DOI": "10.1016/j.chom.2016.01.007",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_9_1"
},
{
"DOI": "10.1089/jir.2014.0227",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_10_1"
},
{
"DOI": "10.1038/nri3547",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_11_1"
},
{
"DOI": "10.1182/blood-2004-10-4166",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_12_1"
},
{
"DOI": "10.1128/JVI.79.12.7819-7826.2005",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_13_1"
},
{
"DOI": "10.1099/vir.0.055533-0",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_14_1"
},
{
"article-title": "Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia",
"author": "Chen L",
"first-page": "E005",
"journal-title": "Zhonghuajie he he hu xi za zhi",
"key": "e_1_2_12_15_1",
"volume": "43",
"year": "2020"
},
{
"DOI": "10.1002/rmv.2134",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_16_1"
},
{
"DOI": "10.1016/j.imbio.2020.152008",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_17_1"
},
{
"DOI": "10.1007/s00281-017-0639-8",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_18_1"
},
{
"DOI": "10.1126/science.1125676",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_19_1"
},
{
"DOI": "10.1172/JCI126363",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_20_1"
},
{
"DOI": "10.1038/s41586-020-2601-5",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_21_1"
},
{
"article-title": "Structural basis for translational shutdown and immune evasion by the Nsp1 protein of SARS‐CoV‐2",
"author": "Thoms M",
"journal-title": "Science",
"key": "e_1_2_12_22_1",
"volume": "80",
"year": "2020"
},
{
"DOI": "10.1093/cid/ciaa410",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_23_1"
},
{
"DOI": "10.1371/journal.ppat.1000756",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_24_1"
},
{
"DOI": "10.1128/JVI.00127-09",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_25_1"
},
{
"DOI": "10.1016/S0140-6736(20)30183-5",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_26_1"
},
{
"key": "e_1_2_12_27_1",
"unstructured": "WHO welcomes preliminary results about dexamethasone use in treating critically ill COVID‐19 patients.https://www.who.int/news/item/16-06-2020-who-welcomes-preliminary-results-about-dexamethasone-use-in-treating-critically-ill-covid-19-patients. Updated June 16 2020; Cited November 29 2020."
},
{
"key": "e_1_2_12_28_1",
"unstructured": "WilkinsonT.Trial of inhaled anti‐viral (SNG001) for SARS‐CoV‐2 (COVID‐19) infection.https://clinicaltrials.gov/ct2/show/NCT04385095. Updated August 27 2020; Cited November 29 2020."
},
{
"DOI": "10.1136/bmj.2.3537.691",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_29_1"
},
{
"DOI": "10.1038/nri2378",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_30_1"
},
{
"DOI": "10.3390/membranes5030425",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_31_1"
},
{
"DOI": "10.1093/ajcn/81.3.633",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_32_1"
},
{
"article-title": "Impact of retinoic acid on immune cells and inflammatory diseases",
"author": "Oliveira LD",
"first-page": "3067126",
"journal-title": "Mediat Inflamm",
"key": "e_1_2_12_33_1",
"year": "2018"
},
{
"DOI": "10.1194/jlr.R100015-JLR200",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_34_1"
},
{
"DOI": "10.1016/j.immuni.2011.07.002",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_35_1"
},
{
"DOI": "10.1084/jem.20101967",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_36_1"
},
{
"DOI": "10.1038/nm.1925",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_37_1"
},
{
"DOI": "10.1093/intimm/dxp003",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_38_1"
},
{
"DOI": "10.1084/jem.20030390",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_39_1"
},
{
"DOI": "10.1016/j.immuni.2010.07.003",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_40_1"
},
{
"DOI": "10.1002/jlb.55.3.336",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_41_1"
},
{
"DOI": "10.1074/jbc.274.12.7674",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_42_1"
},
{
"DOI": "10.1038/sj.bjp.0703345",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_43_1"
},
{
"DOI": "10.1007/s10875-006-9068-5",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_44_1"
},
{
"DOI": "10.1371/journal.pone.0168072",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_45_1"
},
{
"DOI": "10.1038/ni.3734",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_46_1"
},
{
"DOI": "10.1016/j.imlet.2017.01.001",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_47_1"
},
{
"DOI": "10.1038/nature13158",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_48_1"
},
{
"DOI": "10.4049/jimmunol.1501106",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_49_1"
},
{
"DOI": "10.1016/j.immuni.2015.06.009",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_50_1"
},
{
"DOI": "10.1111/cea.12568",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_51_1"
},
{
"DOI": "10.1016/j.bbrc.2006.10.132",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_52_1"
},
{
"article-title": "In vitro increased natural killer cell activity of metastatic melanoma patients with interferon‐α alone as opposed to its combination with 13‐cis retinoic acid is associated with modulation of NKG2D and CD161 activating receptor expression",
"author": "Konjevic G",
"first-page": "761",
"issue": "4",
"journal-title": "J BUON",
"key": "e_1_2_12_53_1",
"volume": "17",
"year": "2012"
},
{
"DOI": "10.3945/jn.108.100198",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_54_1"
},
{
"DOI": "10.5114/ceji.2014.43716",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_55_1"
},
{
"DOI": "10.4049/jimmunol.180.1.138",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_56_1"
},
{
"DOI": "10.1016/j.cellimm.2007.11.001",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_57_1"
},
{
"DOI": "10.4049/jimmunol.1500250",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_58_1"
},
{
"DOI": "10.1006/cimm.1993.1113",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_59_1"
},
{
"DOI": "10.1038/mi.2008.43",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_60_1"
},
{
"DOI": "10.1111/j.1365-2567.2007.02595.x",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_61_1"
},
{
"DOI": "10.1016/j.immuni.2015.02.003",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_62_1"
},
{
"DOI": "10.1084/jem.20070590",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_63_1"
},
{
"DOI": "10.1038/ni.1622",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_64_1"
},
{
"DOI": "10.4049/jimmunol.181.4.2277",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_65_1"
},
{
"DOI": "10.4049/jimmunol.180.3.1834",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_66_1"
},
{
"DOI": "10.1186/s12931-017-0507-z",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_67_1"
},
{
"DOI": "10.1186/s40348-016-0054-6",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_68_1"
},
{
"DOI": "10.1136/thx.2008.101469",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_69_1"
},
{
"DOI": "10.1159/000437326",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_70_1"
},
{
"DOI": "10.1186/1471-2172-14-28",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_71_1"
},
{
"DOI": "10.1084/jem.20121849",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_72_1"
},
{
"DOI": "10.1016/j.cyto.2016.11.015",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_73_1"
},
{
"DOI": "10.1017/S0029665199000403",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_74_1"
},
{
"DOI": "10.1007/BF02020741",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_75_1"
},
{
"DOI": "10.1002/hlca.19310140511",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_76_1"
},
{
"DOI": "10.1136/bmj.1.3403.515",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_77_1"
},
{
"DOI": "10.1136/bmj.2.3745.708",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_78_1"
},
{
"DOI": "10.1093/jn/129.4.783",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_79_1"
},
{
"article-title": "Interactions of nutrition and infection. Geneva: World Health Organization",
"author": "Scrimshaw NS",
"first-page": "3",
"journal-title": "Monogr Ser World Health Organ",
"key": "e_1_2_12_80_1",
"volume": "57",
"year": "1968"
},
{
"article-title": "The essential factors in the diet during growth",
"author": "McCollum EV",
"first-page": "23",
"journal-title": "J Biol Chem",
"key": "e_1_2_12_81_1",
"volume": "15",
"year": "1915"
},
{
"DOI": "10.1128/CMR.18.3.446-464.2005",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_82_1"
},
{
"DOI": "10.1017/S0029665199000944",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_83_1"
},
{
"DOI": "10.1128/JVI.02199-05",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_84_1"
},
{
"DOI": "10.1080/19490976.2017.1353842",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_85_1"
},
{
"DOI": "10.1186/1743-422X-10-337",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_86_1"
},
{
"DOI": "10.1126/scitranslmed.aaa5597",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_87_1"
},
{
"DOI": "10.3851/IMP2568",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_88_1"
},
{
"DOI": "10.1016/j.antiviral.2008.04.003",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_89_1"
},
{
"DOI": "10.4049/jimmunol.148.8.2539",
"article-title": "Enhanced HIV‐1 replication in retinoid‐treated monocytes: retinoid effects mediated through mechanisms related to cell differentiation and to a direct transcriptional action on viral gene expression",
"author": "Turpin JA",
"doi-asserted-by": "crossref",
"first-page": "2539",
"journal-title": "J Immunol",
"key": "e_1_2_12_90_1",
"volume": "148",
"year": "1992"
},
{
"DOI": "10.1128/JVI.72.7.5862-5869.1998",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_91_1"
},
{
"DOI": "10.1111/j.1478-3231.2007.01666.x",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_92_1"
},
{
"article-title": "Measles in India: challenges & recent developments",
"author": "Shrivastava SR",
"first-page": "27784",
"issue": "1",
"journal-title": "Infect Ecol Epidemiol",
"key": "e_1_2_12_93_1",
"volume": "5",
"year": "2015"
},
{
"DOI": "10.1136/bmj.320.7227.76",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_94_1"
},
{
"DOI": "10.1093/ajcn/54.5.890",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_95_1"
},
{
"DOI": "10.1080/02724936.1983.11748292",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_96_1"
},
{
"DOI": "10.1093/tropej/35.3.109",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_97_1"
},
{
"DOI": "10.1093/ajcn/44.6.924",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_98_1"
},
{
"DOI": "10.1542/peds.91.6.1176",
"article-title": "Measles severity and serum retinol (vitamin A) concentration among children in the United States",
"author": "Butler JC",
"doi-asserted-by": "crossref",
"first-page": "1176",
"issue": "6",
"journal-title": "Pediatrics",
"key": "e_1_2_12_99_1",
"volume": "91",
"year": "1993"
},
{
"article-title": "Vitamin A for treating measles in children",
"author": "Yang HM",
"first-page": "CD001479",
"issue": "4",
"journal-title": "Cochrane Database Syst Rev",
"key": "e_1_2_12_100_1",
"year": "2005"
},
{
"DOI": "10.1136/bmj.294.6567.294",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_101_1"
},
{
"DOI": "10.1056/NEJM199007193230304",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_102_1"
},
{
"article-title": "Effect of vitamin A on diarrhoeal and respiratory complications of measles",
"author": "Ogaro FO",
"first-page": "283",
"issue": "6",
"journal-title": "TGM (Trop Geogr Med)",
"key": "e_1_2_12_103_1",
"volume": "45",
"year": "1993"
},
{
"DOI": "10.1093/oxfordjournals.aje.a008761",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_104_1"
},
{
"DOI": "10.1093/oxfordjournals.aje.a009330",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_105_1"
},
{
"DOI": "10.11150/kansenshogakuzasshi1970.73.104",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_106_1"
},
{
"DOI": "10.1097/00006454-199203000-00006",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_107_1"
},
{
"DOI": "10.1093/jn/124.9.1604",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_108_1"
},
{
"DOI": "10.1378/chest.103.5.1625",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_109_1"
},
{
"DOI": "10.1111/crj.12269",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_110_1"
},
{
"article-title": "Fatal measles presenting as acute respiratory distress syndrome in an immunocompetent adult",
"author": "Karanth SS",
"journal-title": "Case Rep",
"key": "e_1_2_12_111_1",
"volume": "2014",
"year": "2014"
},
{
"DOI": "10.1097/MD.0000000000009154",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_112_1"
},
{
"DOI": "10.3855/jidc.6534",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_113_1"
},
{
"DOI": "10.1093/jn/nxz142",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_114_1"
},
{
"DOI": "10.1155/2012/256294",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_115_1"
},
{
"DOI": "10.1016/j.cell.2020.02.052",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_116_1"
},
{
"DOI": "10.1126/science.aax0902",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_117_1"
},
{
"DOI": "10.1016/j.ahj.2020.05.002",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_118_1"
},
{
"DOI": "10.1161/01.HYP.0000146400.57221.74",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_119_1"
},
{
"DOI": "10.1177/1470320314542727",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_120_1"
},
{
"key": "e_1_2_12_121_1",
"unstructured": "BehmVY BlumbergJ BushC. Personalized Nutrition and the COVID‐19 Era: Prepared by the Personalized Nutrition &COVID‐19 Task Force of the American Nutrition Associationhttps://theana.org/COVID-19. Updated Jul 10 2020; Cited September 2 2020."
},
{
"DOI": "10.1161/CIRCRESAHA.120.317015",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_122_1"
},
{
"DOI": "10.1016/j.diabres.2020.108132",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_123_1"
},
{
"key": "e_1_2_12_124_1",
"unstructured": "LiX HuC SuF DaiJ. Hypokalemia and Clinical Implications in Patients with Coronavirus Disease 2019 (COVID‐19).https://www.medrxiv.org/content/10.1101/2020.02.27.20028530v1. Updated February 29 2020; Cited June 7 2020."
},
{
"DOI": "10.1113/expphysiol.2007.040048",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_125_1"
},
{
"DOI": "10.1097/SHK.0000000000000633",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_126_1"
},
{
"key": "e_1_2_12_127_1",
"unstructured": "COVID‐19 and the Use of Angiotensin‐Converting Enzyme Inhibitors and Receptor Blockers.https://www.who.int/news-room/commentaries/detail/covid-19-and-the-use-of-angiotensin-converting-enzyme-inhibitors-and-receptor-blockers. Updated May 07 2020; Cited November 29 2020."
},
{
"DOI": "10.1093/jtm/taaa041",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_128_1"
},
{
"DOI": "10.1038/nm0805-821",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_129_1"
},
{
"article-title": "COVID‐19 and angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers: what is the evidence?",
"author": "Patel AB",
"first-page": "1769",
"issue": "18",
"journal-title": "J Am Med Assoc",
"key": "e_1_2_12_130_1",
"volume": "323",
"year": "2020"
},
{
"DOI": "10.1136/bmj.e4260",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_131_1"
},
{
"DOI": "10.1161/CIRCRESAHA.120.317134",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_132_1"
},
{
"key": "e_1_2_12_133_1",
"unstructured": "HughesS. ACE inhibitors protective against severe COVID‐19?https://www.medscape.com/viewarticle/930841. Updated May 20 2020; Cited June 7 2020."
},
{
"author": "Giovanni deSimone",
"key": "e_1_2_12_134_1",
"volume-title": "Position Statement of the ESC Council on Hypertension on ACE‐Inhibitors and Angiotensin Receptor Blockers\". European Society of Cardiology (ESC)",
"year": "2020"
},
{
"key": "e_1_2_12_135_1",
"volume-title": "EMA Advises Continued Use of Medicines for Hypertension, Heart or Kidney Disease during COVID‐19 Pandemic",
"year": "2020"
},
{
"author": "Bozkurt B",
"key": "e_1_2_12_136_1",
"volume-title": "HFSA/ACC/AHA Statement Addresses Concerns Re: Using RAAS Antagonists in COVID‐19"
},
{
"DOI": "10.1097/00005344-200401000-00005",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_137_1"
},
{
"DOI": "10.1038/sj.ejcn.1601099",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_138_1"
},
{
"DOI": "10.1093/ajcn/50.2.329",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_139_1"
},
{
"DOI": "10.1038/sj.ejcn.1601279",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_140_1"
},
{
"DOI": "10.1186/1743-422X-7-52",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_141_1"
},
{
"key": "e_1_2_12_142_1",
"unstructured": "History of Ebola Virus Disease.https://www.cdc.gov/vhf/ebola/history/summaries.html. Updated September 18 2018; Cited July 03 2020."
},
{
"DOI": "10.1038/s41591-020-0820-9",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_143_1"
},
{
"DOI": "10.2174/1876326X01206010064",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_144_1"
},
{
"author": "American Academy of Pediatrics",
"first-page": "386",
"key": "e_1_2_12_145_1",
"volume-title": "Red Book: 2015 Report of the Committee on Infectious Diseases",
"year": "2015"
},
{
"DOI": "10.1093/jn/120.10.1264",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_146_1"
},
{
"DOI": "10.3390/v8100282",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_147_1"
},
{
"DOI": "10.3390/v7102892",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_148_1"
},
{
"DOI": "10.1016/S0022-2275(20)42007-3",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_149_1"
},
{
"DOI": "10.1093/jn/132.2.197",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_150_1"
},
{
"DOI": "10.1186/s12931-015-0300-9",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_151_1"
},
{
"key": "e_1_2_12_152_1",
"unstructured": "Recommended Dietary Allowance.https://archive.fssai.gov.in/dam/jcr:651fb6ae-d530-4162-be1a-8bf38c3743c7/Note_Dietary_Allowance_27_02_2019.pdf. Updated February 27 2019; Cited July 21 2020."
},
{
"author": "Paranjpe DR",
"first-page": "721",
"key": "e_1_2_12_153_1",
"volume-title": "Nutritional disorders in Cornea",
"year": "2011"
},
{
"DOI": "10.1111/j.1365-4362.1981.tb04338.x",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_154_1"
},
{
"DOI": "10.1093/ajcn/83.2.191",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_155_1"
},
{
"author": "World Health Organization",
"key": "e_1_2_12_156_1",
"volume-title": "Using national immunization days to deliver vitamin A. EPI Update",
"year": "1993"
},
{
"author": "Olson JA",
"first-page": "109",
"key": "e_1_2_12_157_1",
"volume-title": "Present knowledge in nutrition",
"year": "2001"
},
{
"key": "e_1_2_12_158_1",
"unstructured": "Vitamin A Supplementation in Infants and Children 6–59 Months of Age.https://www.who.int/elena/titles/vitamina_children/en/. Updated February 11 2019; Cited July 12 2020."
},
{
"author": "Olson JM",
"key": "e_1_2_12_159_1",
"volume-title": "Vitamin A toxicity"
},
{
"author": "ELkazzaz M",
"key": "e_1_2_12_160_1",
"volume-title": "Assessment the Activity Value of 13‐cis‐Retinoic Acid (Isotretinoin) in the Treatment of COVID‐19"
},
{
"author": "Semba RD",
"first-page": "132",
"key": "e_1_2_12_161_1",
"volume-title": "The Vitamin A Story – Lifting the Shadow of the Death. World Rev Nutr Diet. Basel, Karger",
"year": "2012"
},
{
"DOI": "10.1038/s41591-020-0965-6",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_162_1"
},
{
"DOI": "10.1371/journal.pone.0086554",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_163_1"
},
{
"article-title": "Combining vitamin A and vaccines: convenience or conflict?",
"author": "Benn CS",
"first-page": "B4378",
"issue": "1",
"journal-title": "Dan Med J",
"key": "e_1_2_12_164_1",
"volume": "59",
"year": "2012"
},
{
"DOI": "10.2460/ajvr.74.10.1353",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_165_1"
},
{
"DOI": "10.1038/s41598-019-51684-x",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_166_1"
},
{
"DOI": "10.1016/j.vaccine.2014.03.025",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_167_1"
},
{
"DOI": "10.4049/jimmunol.174.12.7961",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_168_1"
},
{
"DOI": "10.1073/pnas.0506438102",
"doi-asserted-by": "publisher",
"key": "e_1_2_12_169_1"
}
],
"reference-count": 168,
"references-count": 168,
"relation": {},
"resource": {
"primary": {
"URL": "https://onlinelibrary.wiley.com/doi/10.1002/rmv.2204"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [],
"subtitle": [],
"title": "Mega doses of retinol: A possible immunomodulation in Covid‐19 illness in resource‐limited settings",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1002/crossmark_policy",
"volume": "31"
}