A randomized controlled study of convalescent plasma for individuals hospitalized with COVID-19 pneumonia
et al., Journal of Clinical Investigation, doi:10.1172/JCI155114, PennCCP2, NCT04397757, Dec 2021
{kind=link}
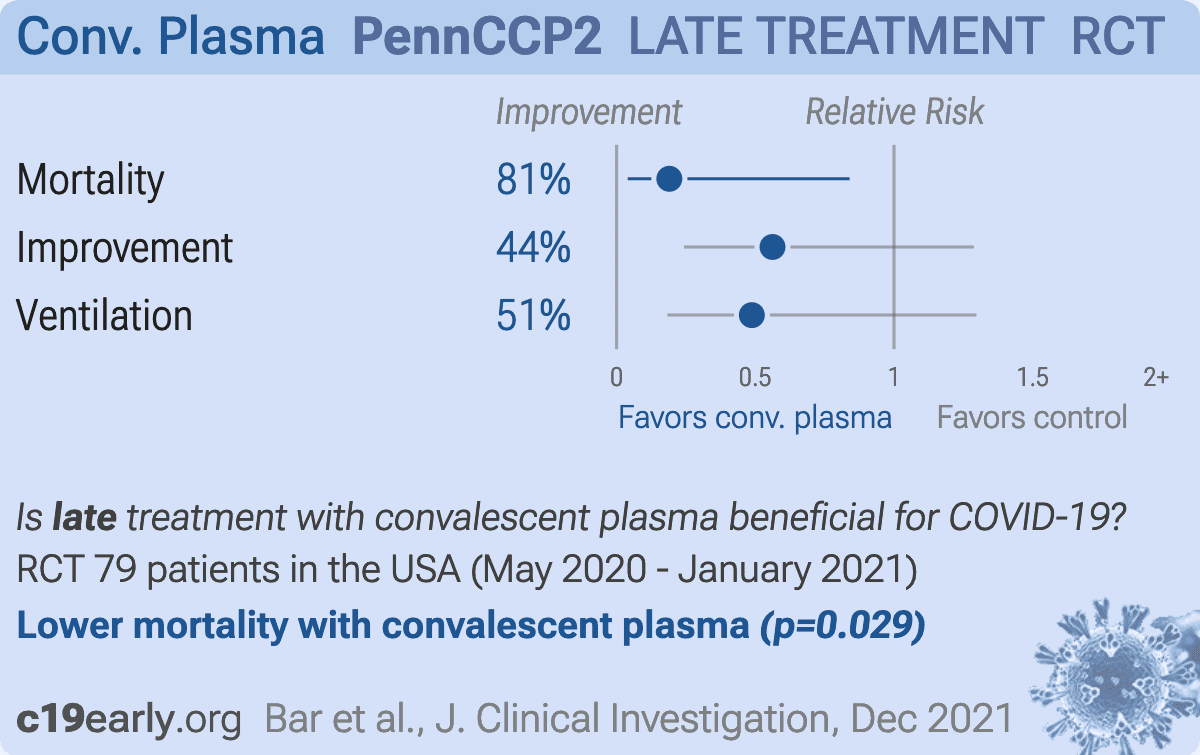
RCT 79 hospitalized patients in the USA, showing significant benefit in clinical severity score and 28-day mortality with convalescent plasma treatment.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
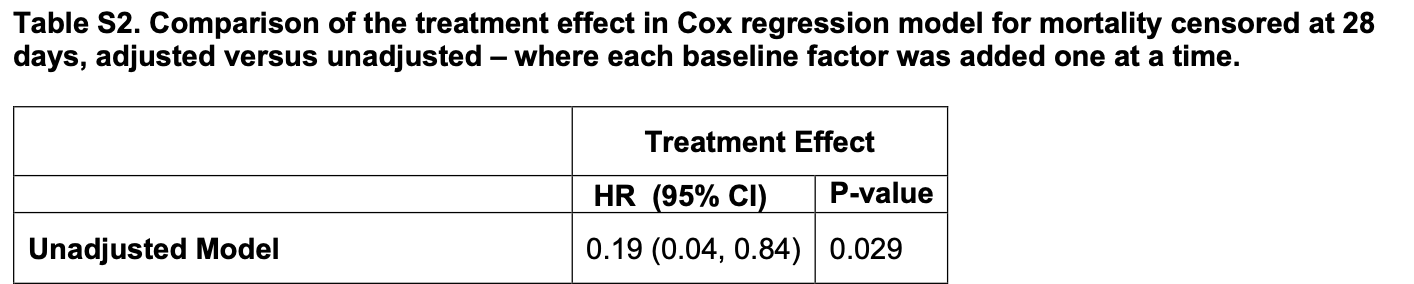
risk of death, 81.0% lower, HR 0.19, p = 0.03, treatment 40, control 39, Cox proportional hazards, day 28.
|
|
risk of no improvement, 43.8% lower, OR 0.56, p = 0.18, treatment 40, control 39, WHO8 score, day 28, RR approximated with OR.
|
|
risk of mechanical ventilation, 51.2% lower, RR 0.49, p = 0.16, treatment 5 of 40 (12.5%), control 10 of 39 (25.6%), NNT 7.6.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Bar et al., 15 Dec 2021, Randomized Controlled Trial, USA, peer-reviewed, median age 63.0, 40 authors, study period 18 May, 2020 - 8 January, 2021, trial NCT04397757 (history) (PennCCP2).
{kind=link}
The Journal of Clinical Investigation
doi:10.1172/JCI155114.
infected individuals developing severe pneumonia requiring hospitalization. Substantial morbidity and mortality remain for patients with COVID-19 who are hospitalized with pneumonia, and few efficacious therapies exist. Early in the COVID-19 pandemic, convalescent COVID-19 plasma (CCP) was recognized as a potentially promising intervention. Use of convalescent plasma in other infectious diseases (2-5) and previous coronavirus pandemics (6, 7) provided biological plausibility, and early observational studies suggested possible benefit (8-10). In the setting of limited treatments and desperate clinical need, CCP was widely used in hospitalized patients with COVID-19 in the United States via an expanded access program (EAP) or emergency use authorization (EUA; refs. 3, 11) . These mechanisms enabled access to CCP by more than 500,000 hospitalized individuals, with up to 40% of US inpatients with COVID-19 receiving CCP in the fall of 2020 ( 12 ). Observational BACKGROUND. Antibody-based strategies for COVID-19 have shown promise in prevention and treatment of early disease. COVID-19 convalescent plasma (CCP) has been widely used but results from randomized trials supporting its benefit in hospitalized patients with pneumonia are limited. Here, we assess the efficacy of CCP in severely ill, hospitalized adults with COVID-19 pneumonia.
METHODS. We performed a randomized control trial (PennCCP2), with 80 adults hospitalized with COVID-19 pneumonia, comparing up to 2 units of locally sourced CCP plus standard care versus standard care alone. The primary efficacy endpoint was comparison of a clinical severity score. Key secondary outcomes include 14-and 28-day mortality, 14-and 28-day maximum 8-point WHO ordinal score (WHO8) score, duration of supplemental oxygenation or mechanical ventilation, respiratory SARS-CoV-2 RNA, and anti-SARS-CoV-2 antibodies.
RESULTS. Eighty hospitalized adults with confirmed COVID-19 pneumonia were enrolled at median day 6 of symptoms and day 1 of hospitalization; 60% were anti-SARS-CoV-2 antibody seronegative. Participants had a median of 3 comorbidities, including risk factors for severe COVID-19 and immunosuppression. CCP treatment was safe and conferred significant benefit by clinical severity score (median [MED] and interquartile range ], P = 0.037) and 28-day mortality (n = 10, 26% vs. n = 2, 5%; P = 0.013). All other prespecified outcome measures showed weak evidence toward benefit of CCP.
CONCLUSION. Two units of locally sourced CCP administered early in hospitalization to majority seronegative participants conferred a significant benefit in clinical severity score and 28-day mortality. Results suggest CCP may benefit select populations, especially those with comorbidities who are treated early. TRIAL REGISTRATION. ClinicalTrials.gov NCT04397757.
Author contributions KJB, PAS, GHC, NA, AF, MC, JLP, MAE, IF, SEH, DLS, and PT designed the clinical trial. KJB, PAS, GHC, NA, AF, HSC, LG, JS, MA, MM, CA, GF, MD, MB, MC, JG, AW, MAM, FM, EL, AMM, HB, AP, LI, RT, RAE, FD, JLP, WRS, MAE, JB, NJM, KOD, IF, DLS, and PT conducted the clinical trial. KJB, LG, AW, MAM, FM, EL, SG, ETLP, SEH, and DLS conducted experiments. KJB, PAS, GHC, JBY, and PT analyzed data. KJB, PAS, GHC, MC, and PT wrote the manuscript.
References
Agarwal, Convalescent plasma in the management of moderate covid-19 in adults in India: open label phase II multicentre randomised controlled trial (PLACID Trial), BMJ
Anderson, Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection, Cell, doi:10.1016/j.cell.2021.02.010
Assaad, High mortality rate in cancer patients with symptoms of COVID-19 with or without detectable SARS-COV-2 on RT-PCR, Eur J Cancer, doi:10.1016/j.ejca.2020.05.028
Avendano-Sola, A multicenter randomized open-label clinical trial for convalescent plasma in patients hospitalized with COVID-19 pneumonia, J Clin Invest, doi:10.1172/JCI152740
Begin, Convalescent plasma for adults with acute COVID-19 respiratory illness (CON-COR-1): study protocol for an international, multicentre, randomized, open-label trial, Trials, doi:10.1186/s13063-021-05235-3
Briggs, Early but not late convalescent plasma is associated with better survival in moderate-to-severe COVID-19, PLoS One, doi:10.1371/journal.pone.0254453
Casadevall, Convalescent plasma use in the USA was inversely correlated with COVID-19 mortality, Elife, doi:10.7554/eLife.69866
Casadevall, The principles of antibody therapy for infectious diseases with relevance for COVID-19, mBio
Cheng, Use of convalescent plasma therapy in SARS patients in Hong Kong, Eur J Clin Microbiol Infect Dis, doi:10.1007/s10096-004-1271-9
Dodd, Endpoints for randomized controlled clinical trials for COVID-19 treatments, Clin Trials, doi:10.1177/1740774520939938
Duan, Effectiveness of convalescent plasma therapy in severe COVID-19 patients, Proc Natl Acad Sci U S A, doi:10.1073/pnas.2004168117
Evans, Desirability of outcome ranking (DOOR) and response adjusted for duration of antibiotic risk (RADAR), Clin Infect Dis, doi:10.1093/cid/civ495
Everett, SARS-CoV-2 Genomic Variation in Space and Time in Hospitalized Patients in Philadelphia, mBio
Flannery, SARS-CoV-2 seroprevalence among parturient women in Philadelphia, Sci Immunol, doi:10.1126/sciimmunol.abd5709
Gharbharan, Convalescent plasma for COVID-19. A randomized clinical trial, Nat Commun
Gharbharan, Effects of treatment of COVID-19 with convalescent plasma in 25 B-cell depleted patients
Goldfeld, Prospective individual patient data meta-analysis: Evaluating convalescent plasma for COVID-19, Stat Med, doi:10.1002/sim.9115
Harrison, Comorbidities associated with mortality in 31,461 adults with COVID-19 in the United States: A federated electronic medical record analysis, PLoS Med, doi:10.1371/journal.pmed.1003321
Joyner, Convalescent plasma antibody levels and the risk of death from Covid-19, N Engl J Med, doi:10.1056/NEJMoa2031893
Joyner, Early safety indicators of COVID-19 convalescent plasma in 5000 patients, J Clin Invest, doi:10.1172/JCI140200
Klassen, The effect of convalescent plasma therapy on mortality among patients with COVID-19: systematic review and meta-analysis, doi:10.1016/j.mayocp.2021.02.008
Korley, Early convalescent plasma for high-risk outpatients with Covid-19
Korper, Results of the CAPSID randomized trial for high-dose convalescent plasma in patients with severe COVID-19, J Clin Invest, doi:10.1172/JCI152264
Kunze, Mortality in individuals treated with COVID-19 convalescent plasma varies with the geographic provenance of donors, Nat Commun, doi:10.1038/s41467-021-25113-5
Li, Effect of convalescent plasma therapy on time to clinical improvement in patients with severe and life-threatening COVID-19: a randomized clinical trial, JAMA, doi:10.1001/jama.2020.10044
Libster, Early high-titer plasma therapy to prevent severe Covid-19 in older adults, N Engl J Med, doi:10.1056/NEJMoa2033700
O'brien, Subcutaneous REGEN-COV antibody combination in early SARS-CoV-2 infection, doi:10.1101/2021.06.14
O'donnell, A randomized double-blind controlled trial of convalescent plasma in adults with severe COVID-19, J Clin Invest
Petkova, Pooling data from individual clinical trials in the COVID-19 era, JAMA, doi:10.1001/jama.2020.13042
Pocock, The win ratio: a new approach to the analysis of composite endpoints in clinical trials based on clinical priorities, Eur Heart J
Ripoll, Convalescent plasma for infectious diseases: historical framework and use in COVID-19, Clin Microbiol Newsl, doi:10.1016/j.clinmicnews.2021.02.001
Rodionov, Potential benefit of convalescent plasma transfusions in immunocompromised patients with COVID-19, Lancet Microbe, doi:10.1016/S2666-5247(21)00030-6
Rosenthal, Risk factors associated with in-hospital mortality in a US National sample of patients With COVID-19, JAMA Netw Open, doi:10.1001/jamanetworkopen.2020.29058
Senefeld, Program and patient characteristics for the United States Expanded Access Program to COVID-19 convalescent plasma, doi:10.1101/2021.04.08.21255115
Shaw, Fay, A rank test for bivariate timeto-event outcomes when one event is a surrogate, Stat Med, doi:10.1002/sim.6950
Shen, Treatment of 5 critically ill patients with COVID-19 with convalescent plasma, JAMA, doi:10.1001/jama.2020.4783
Simonovich, A randomized trial of convalescent plasma in Covid-19 severe pneumonia, N Engl J Med, doi:10.1056/NEJMoa2031304
Soo, plasma with continuing high-dose methylprednisolone treatment in SARS patients, Clin Microbiol Infect, doi:10.1111/j.1469-0691.2004.00956.x
Sormani, SARS-CoV-2 serology after COVID-19 in multiple sclerosis: An international cohort study
Sun, A potentially effective treatment for COVID-19: A systematic review and meta-analysis of convalescent plasma therapy in treating severe infectious disease, Int J Infect Dis, doi:10.1016/j.ijid.2020.06.107
Thompson, Association of convalescent plasma therapy with survival in patients with hematologic cancers and COVID-19
Weinreich, REGN-COV2, a neutralizing antibody cocktail, doi:10.1056/NEJMoa2035002
Worldometers, None
Zeng, Effect of convalescent plasma therapy on viral shedding and survival in patients with Coronavirus Disease 2019, J Infect Dis, doi:10.1093/infdis/jiaa228
DOI record:
{
"DOI": "10.1172/jci155114",
"ISSN": [
"1558-8238"
],
"URL": "http://dx.doi.org/10.1172/JCI155114",
"alternative-id": [
"10.1172/JCI155114"
],
"author": [
{
"ORCID": "http://orcid.org/0000-0002-9773-0071",
"affiliation": [],
"authenticated-orcid": false,
"family": "Bar",
"given": "Katharine J.",
"sequence": "first"
},
{
"ORCID": "http://orcid.org/0000-0003-1883-8410",
"affiliation": [],
"authenticated-orcid": false,
"family": "Shaw",
"given": "Pamela A.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Choi",
"given": "Grace H.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Aqui",
"given": "Nicole",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-2705-803X",
"affiliation": [],
"authenticated-orcid": false,
"family": "Fesnak",
"given": "Andrew",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Yang",
"given": "Jasper B.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Soto-Calderon",
"given": "Haideliza",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-6912-2183",
"affiliation": [],
"authenticated-orcid": false,
"family": "Grajales",
"given": "Lizette",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Starr",
"given": "Julie",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Andronov",
"given": "Michelle",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-5824-9365",
"affiliation": [],
"authenticated-orcid": false,
"family": "Mastellone",
"given": "Miranda",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Amonu",
"given": "Chigozie",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Feret",
"given": "Geoff",
"sequence": "additional"
},
{
"affiliation": [],
"family": "DeMarshall",
"given": "Maureen",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Buchanan",
"given": "Marie",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Caturla",
"given": "Maria",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Gordon",
"given": "James",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Wanicur",
"given": "Alan",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Monroy",
"given": "M. Alexandra",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Mampe",
"given": "Felicity",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-5721-0787",
"affiliation": [],
"authenticated-orcid": false,
"family": "Lindemuth",
"given": "Emily",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-7853-8340",
"affiliation": [],
"authenticated-orcid": false,
"family": "Gouma",
"given": "Sigrid",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-4803-3667",
"affiliation": [],
"authenticated-orcid": false,
"family": "Mullin",
"given": "Anne M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Barilla",
"given": "Holly",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Pronina",
"given": "Anastasiya",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Irwin",
"given": "Leah",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Thomas",
"given": "Raeann",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-3327-3043",
"affiliation": [],
"authenticated-orcid": false,
"family": "Eichinger",
"given": "Risa A.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-7306-9023",
"affiliation": [],
"authenticated-orcid": false,
"family": "Demuth",
"given": "Faye",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Luning Prak",
"given": "Eline T.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-1613-7912",
"affiliation": [],
"authenticated-orcid": false,
"family": "Pascual",
"given": "Jose L.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Short",
"given": "William R.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-7554-7180",
"affiliation": [],
"authenticated-orcid": false,
"family": "Elovitz",
"given": "Michal A.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Baron",
"given": "Jillian",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-4597-5584",
"affiliation": [],
"authenticated-orcid": false,
"family": "Meyer",
"given": "Nuala J.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Degnan",
"given": "Kathleen O.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-7824-0106",
"affiliation": [],
"authenticated-orcid": false,
"family": "Frank",
"given": "Ian",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-2928-7506",
"affiliation": [],
"authenticated-orcid": false,
"family": "Hensley",
"given": "Scott E.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Siegel",
"given": "Donald L.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-5345-7942",
"affiliation": [],
"authenticated-orcid": false,
"family": "Tebas",
"given": "Pablo",
"sequence": "additional"
}
],
"container-title": "Journal of Clinical Investigation",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2021,
11,
17
]
],
"date-time": "2021-11-17T17:00:27Z",
"timestamp": 1637168427000
},
"deposited": {
"date-parts": [
[
2021,
12,
14
]
],
"date-time": "2021-12-14T19:04:53Z",
"timestamp": 1639508693000
},
"indexed": {
"date-parts": [
[
2023,
1,
14
]
],
"date-time": "2023-01-14T10:50:09Z",
"timestamp": 1673693409497
},
"is-referenced-by-count": 30,
"issue": "24",
"issued": {
"date-parts": [
[
2021,
12,
15
]
]
},
"journal-issue": {
"issue": "24",
"published-online": {
"date-parts": [
[
2021,
12,
15
]
]
},
"published-print": {
"date-parts": [
[
2021,
12,
15
]
]
}
},
"language": "en",
"link": [
{
"URL": "https://www.jci.org/articles/view/155114/files/pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "232",
"original-title": [],
"prefix": "10.1172",
"published": {
"date-parts": [
[
2021,
12,
15
]
]
},
"published-online": {
"date-parts": [
[
2021,
12,
15
]
]
},
"published-print": {
"date-parts": [
[
2021,
12,
15
]
]
},
"publisher": "American Society for Clinical Investigation",
"reference": [
{
"key": "B1",
"unstructured": "Worldometers.info. https://www.worldometers.info/coronavirus/ Updated November 1, 2021. Accessed November 1, 2021."
},
{
"DOI": "10.1128/mBio.03372-20",
"article-title": "The principles of antibody therapy for infectious diseases with relevance for COVID-19",
"author": "Casadevall",
"doi-asserted-by": "crossref",
"issue": "2",
"journal-title": "mBio",
"key": "B2",
"volume": "12",
"year": "2021"
},
{
"DOI": "10.1172/JCI140200",
"doi-asserted-by": "publisher",
"key": "B3"
},
{
"DOI": "10.1016/j.clinmicnews.2021.02.001",
"doi-asserted-by": "publisher",
"key": "B4"
},
{
"DOI": "10.1016/j.ijid.2020.06.107",
"doi-asserted-by": "publisher",
"key": "B5"
},
{
"DOI": "10.1111/j.1469-0691.2004.00956.x",
"doi-asserted-by": "publisher",
"key": "B6"
},
{
"DOI": "10.1007/s10096-004-1271-9",
"doi-asserted-by": "publisher",
"key": "B7"
},
{
"DOI": "10.1073/pnas.2004168117",
"doi-asserted-by": "publisher",
"key": "B8"
},
{
"DOI": "10.1093/infdis/jiaa228",
"doi-asserted-by": "publisher",
"key": "B9"
},
{
"DOI": "10.1001/jama.2020.4783",
"doi-asserted-by": "publisher",
"key": "B10"
},
{
"DOI": "10.1101/2021.04.08.21255115",
"doi-asserted-by": "crossref",
"key": "B11",
"unstructured": "Senefeld JW, et al. Program and patient characteristics for the United States Expanded Access Program to COVID-19 convalescent plasma [preprint]. https://doi.org/10.1101/2021.04.08.21255115 Posted on medRxiv April 10, 2021"
},
{
"DOI": "10.7554/eLife.69866",
"doi-asserted-by": "publisher",
"key": "B12"
},
{
"DOI": "10.1056/NEJMoa2031893",
"doi-asserted-by": "publisher",
"key": "B13"
},
{
"article-title": "Convalescent plasma in the management of moderate covid-19 in adults in India: open label phase II multicentre randomised controlled trial (PLACID Trial)",
"author": "Agarwal",
"journal-title": "BMJ",
"key": "B14",
"volume": "371",
"year": "2020"
},
{
"article-title": "Convalescent plasma for COVID-19. A randomized clinical trial",
"author": "Gharbharan",
"journal-title": "Nat Commun",
"key": "B15",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1172/JCI150646",
"article-title": "A randomized double-blind controlled trial of convalescent plasma in adults with severe COVID-19",
"author": "O’Donnell",
"doi-asserted-by": "crossref",
"issue": "13",
"journal-title": "J Clin Invest",
"key": "B16",
"volume": "131",
"year": "2021"
},
{
"DOI": "10.1056/NEJMoa2031304",
"doi-asserted-by": "publisher",
"key": "B17"
},
{
"DOI": "10.1016/S0140-6736(21)00897-7",
"doi-asserted-by": "publisher",
"key": "B18"
},
{
"DOI": "10.1186/s13063-021-05235-3",
"doi-asserted-by": "publisher",
"key": "B19"
},
{
"key": "B20",
"unstructured": "Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-score-news-2 Updated December 19, 2017. Accessed November 1, 2021"
},
{
"DOI": "10.1371/journal.pmed.1003321",
"doi-asserted-by": "publisher",
"key": "B21"
},
{
"DOI": "10.1001/jamanetworkopen.2020.29058",
"doi-asserted-by": "publisher",
"key": "B22"
},
{
"article-title": "SARS-CoV-2 serology after COVID-19 in multiple sclerosis: An international cohort study",
"author": "Sormani",
"journal-title": "Mult Scler",
"key": "B23"
},
{
"DOI": "10.1126/sciimmunol.abd5709",
"doi-asserted-by": "publisher",
"key": "B24"
},
{
"DOI": "10.1016/j.cell.2021.02.010",
"doi-asserted-by": "publisher",
"key": "B25"
},
{
"DOI": "10.1101/2021.06.14.21258569",
"doi-asserted-by": "crossref",
"key": "B26",
"unstructured": "O’Brien MP, et al. Subcutaneous REGEN-COV antibody combination in early SARS-CoV-2 infection [preprint]. https://doi.org/10.1101/2021.06.14.21258569 Posted on medRxiv June 14, 2021"
},
{
"DOI": "10.1056/NEJMoa2035002",
"doi-asserted-by": "publisher",
"key": "B27"
},
{
"DOI": "10.1056/NEJMoa2033700",
"doi-asserted-by": "publisher",
"key": "B28"
},
{
"DOI": "10.1038/s41467-021-25113-5",
"doi-asserted-by": "publisher",
"key": "B29"
},
{
"DOI": "10.1172/JCI152264",
"doi-asserted-by": "publisher",
"key": "B30"
},
{
"DOI": "10.1002/sim.6950",
"doi-asserted-by": "publisher",
"key": "B31"
},
{
"DOI": "10.1001/jama.2020.10044",
"doi-asserted-by": "publisher",
"key": "B32"
},
{
"article-title": "Early convalescent plasma for high-risk outpatients with Covid-19",
"author": "Korley",
"journal-title": "N Engl J Med",
"key": "B33"
},
{
"DOI": "10.1016/j.mayocp.2021.02.008",
"doi-asserted-by": "publisher",
"key": "B34"
},
{
"DOI": "10.1001/jama.2020.13042",
"doi-asserted-by": "publisher",
"key": "B35"
},
{
"DOI": "10.1371/journal.pone.0254453",
"doi-asserted-by": "publisher",
"key": "B36"
},
{
"DOI": "10.1016/j.ejca.2020.05.028",
"doi-asserted-by": "publisher",
"key": "B37"
},
{
"DOI": "10.1093/cid/civ495",
"doi-asserted-by": "publisher",
"key": "B38"
},
{
"article-title": "Effects of treatment of COVID-19 with convalescent plasma in 25 B-cell depleted patients",
"author": "Gharbharan",
"journal-title": "Clin Infect Dis",
"key": "B39"
},
{
"article-title": "Association of convalescent plasma therapy with survival in patients with hematologic cancers and COVID-19",
"author": "Thompson",
"journal-title": "JAMA Oncol",
"key": "B40"
},
{
"DOI": "10.1016/S2666-5247(21)00030-6",
"doi-asserted-by": "publisher",
"key": "B41"
},
{
"DOI": "10.1002/sim.9115",
"doi-asserted-by": "publisher",
"key": "B42"
},
{
"DOI": "10.1093/eurheartj/ehr352",
"article-title": "The win ratio: a new approach to the analysis of composite endpoints in clinical trials based on clinical priorities",
"author": "Pocock",
"doi-asserted-by": "crossref",
"first-page": "176",
"issue": "2",
"journal-title": "Eur Heart J",
"key": "B43",
"volume": "33",
"year": "2011"
},
{
"DOI": "10.1177/1740774520939938",
"doi-asserted-by": "publisher",
"key": "B44"
},
{
"DOI": "10.1172/JCI152740",
"doi-asserted-by": "publisher",
"key": "B45"
},
{
"key": "B46",
"unstructured": "World Health Organization. COVID-19 Treatment Trial Design Master Protocol Synopsis. https://www.who.int/blueprint/priority-diseases/key-action/COVID-19_Treatment_Trial_Design_Master_Protocol_synopsis_Final_18022020.pdf Updated February 18, 2020. Accessed November 1, 2021"
},
{
"DOI": "10.1128/mBio.03456-20",
"article-title": "SARS-CoV-2 Genomic Variation in Space and Time in Hospitalized Patients in Philadelphia",
"author": "Everett",
"doi-asserted-by": "crossref",
"issue": "1",
"journal-title": "mBio",
"key": "B47",
"volume": "12",
"year": "2021"
}
],
"reference-count": 47,
"references-count": 47,
"relation": {},
"resource": {
"primary": {
"URL": "https://www.jci.org/articles/view/155114"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"General Medicine"
],
"subtitle": [],
"title": "A randomized controlled study of convalescent plasma for individuals hospitalized with COVID-19 pneumonia",
"type": "journal-article",
"volume": "131"
}
Late treatment
is less effective
is less effective
