An open-label, multicentre, randomised, adaptive platform trial of the safety and efficacy of several therapies, including antiviral therapies, versus control in mild/moderate cases of COVID-19
et al., ANTICOV, ANTICOV, Mar 2024
HCQ for COVID-19
1st treatment shown to reduce risk in
March 2020, now with p < 0.00000000001 from 424 studies, used in 59 countries.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
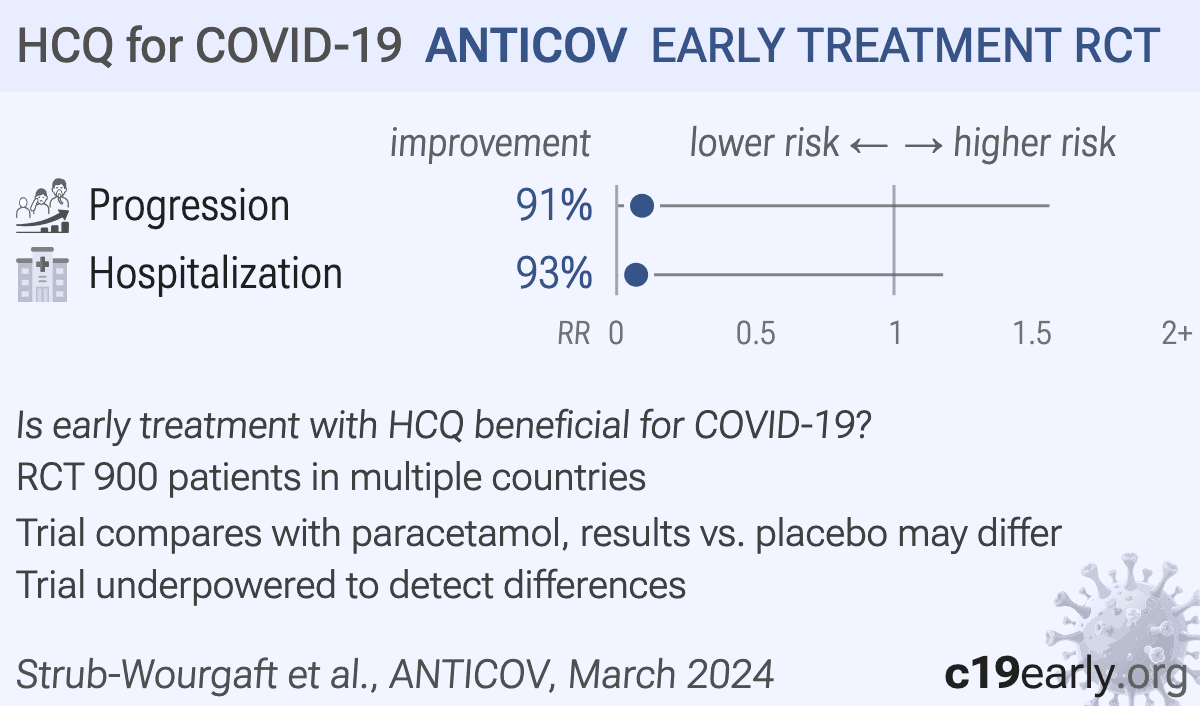
RCT 1,942 patients testing HCQ, lopinavir/ritonavir, nitazoxanide/ciclesonide, ivermectin/ASAQ, and fluoxetine/budesonide compared wirth paracetamol.
Paracetamol was used as a control group. Results with concurrent controls are only provided for nitazoxanide/ciclesonide. Other groups only have comparisons with the full control group. The full control group continues beyond the time of most arms, including patients at later times when COVID-19 risk was lower, therefore results may underestimate efficacy.
The nitazoxanide/ciclesonide concurrent controls are closer in time than the full group for ivermectin/ASAQ and fluoxetine/budesonide and may be a more appropriate comparison. The control group in this case shows worse results. We currently use the full control group results to be conservative.
Authors indicate that the data is available however it is not available as of May 2026.
This study is excluded in the after exclusion results of meta-analysis:
significant confounding by time possible.
|
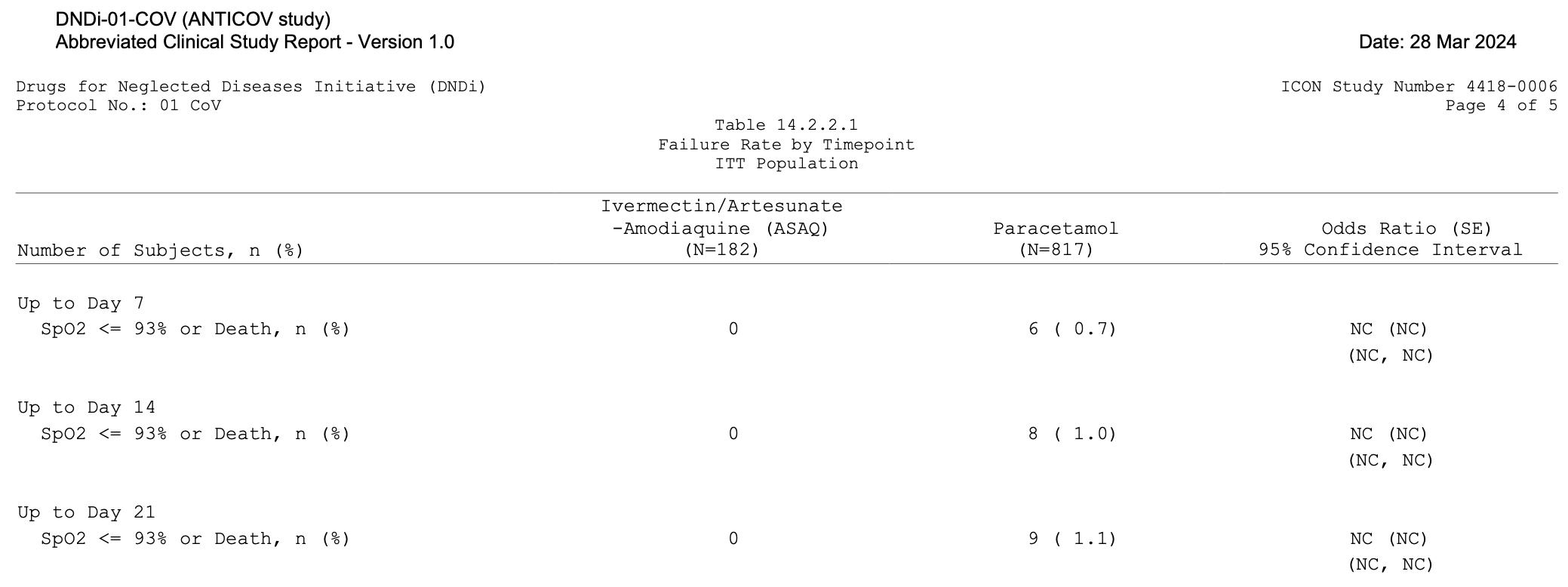
risk of progression, 90.8% lower, RR 0.09, p = 1.00, treatment 0 of 83 (0.0%), control 9 of 817 (1.1%), NNT 91, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), SpO2 ≤93 or death, day 21, Table 14.2.2.1.
|
|
risk of hospitalization, 93.0% lower, RR 0.07, p = 0.62, treatment 0 of 83 (0.0%), control 12 of 817 (1.5%), NNT 68, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), COVID-19 hospitalization, day 21, Table 14.2.2.13.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Strub-Wourgaft et al., 28 Mar 2024, Randomized Controlled Trial, multiple countries, preprint, 12 authors, average treatment delay 3.0 days, this trial compares with another treatment - results may be better when compared to placebo, ANTICOV trial.
strubwourgaft