
Treatment of Severe COVID-19 with Low-Dose Selinexor: Demonstration of Anti-Viral and Anti-Inflammatory Activities in a Randomized, International, Multicenter, Placebo-Controlled Phase 2 Clinical Trial
et al., Karyopharm Therapeutics, XPORT-CoV-1001, Oct 2020
{kind=link}
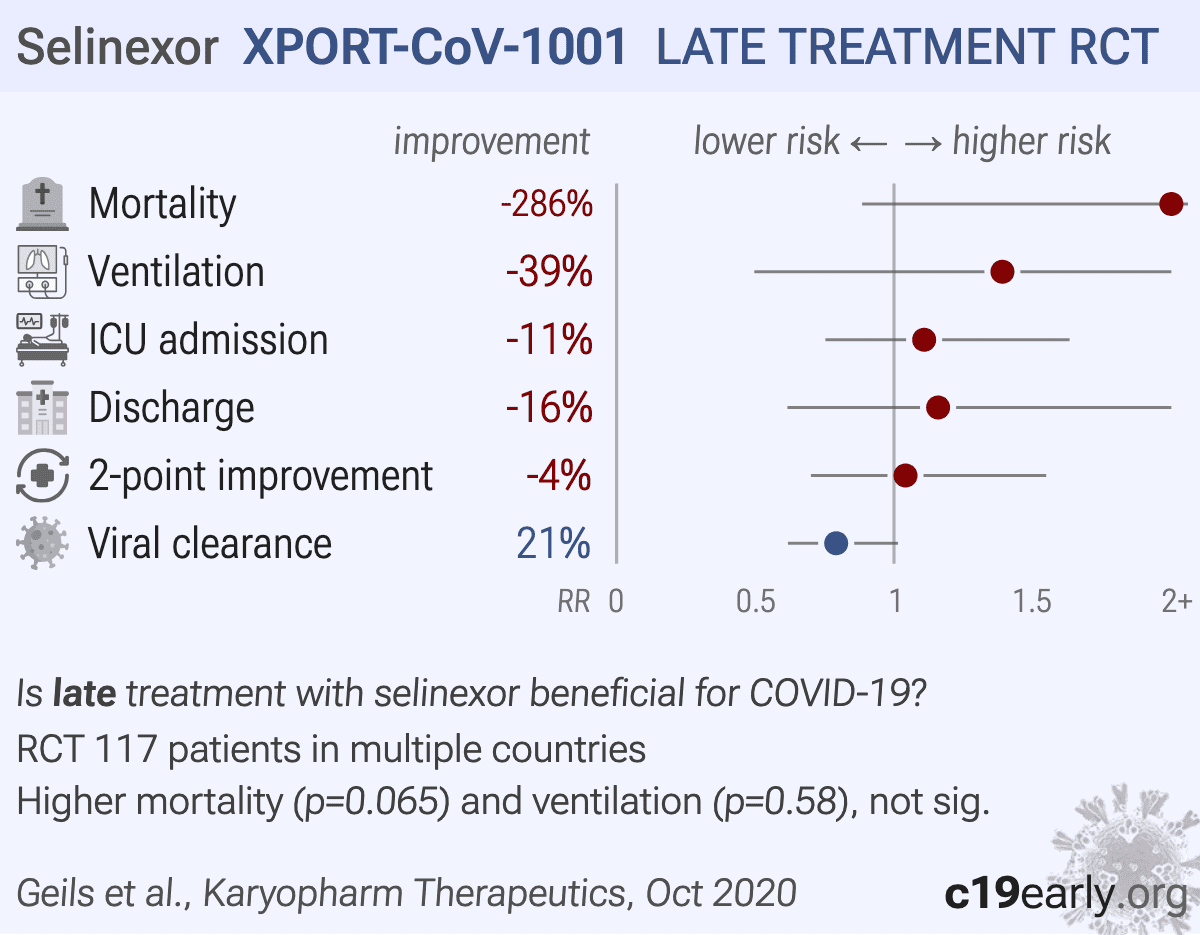
RCT 188 hospitalized patients with severe COVID-19 showing higher mortality (p=0.07) and no significant clinical improvement with oral selinexor (20mg) compared to placebo. In the intention-to-treat analysis, the study failed its primary endpoint, with day 14 clinical improvement rates being numerically lower in the treatment group (53.0%) compared to placebo (54.9%). More concerningly, day 28 mortality was nearly four times higher in the selinexor group (15.2%) versus placebo (3.9%), and mechanical ventilation requirements were also increased (13.6% vs 9.8%) . While the authors focus on a subgroup analysis of patients with low inflammatory markers (low LDH/D-dimer) showing improved discharge rates, patients with high markers experienced drastically higher mortality with treatment (33.3% vs 8.7% in placebo). The study was single-blind, introducing potential bias regarding discharge decisions, and the reliance on post-hoc subgroup analysis to claim benefit despite a failed primary endpoint and safety signals in the overall population raises concerns.
|
risk of death, 286.4% higher, RR 3.86, p = 0.07, treatment 10 of 66 (15.2%), control 2 of 51 (3.9%), day 28.
|
|
risk of mechanical ventilation, 39.1% higher, RR 1.39, p = 0.58, treatment 9 of 66 (13.6%), control 5 of 51 (9.8%).
|
|
risk of ICU admission, 10.9% higher, RR 1.11, p = 0.71, treatment 33 of 66 (50.0%), control 23 of 51 (45.1%).
|
|
risk of no hospital discharge, 15.9% higher, RR 1.16, p = 0.68, treatment 18 of 66 (27.3%), control 12 of 51 (23.5%).
|
|
risk of no 2-point improvement, 4.2% higher, RR 1.04, p = 0.85, treatment 31 of 66 (47.0%), control 23 of 51 (45.1%), day 14.
|
|
risk of no viral clearance, 20.8% lower, RR 0.79, p = 0.06, treatment 42 of 66 (63.6%), control 41 of 51 (80.4%), NNT 6.0.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Geils et al., 10 Oct 2020, Single Blind Randomized Controlled Trial, placebo-controlled, multiple countries, preprint, 35 authors, XPORT-CoV-1001 trial.
Selinexor is an oral small molecule Selective Inhibitor of Nuclear Export (SINE) that blocks the transport protein exportin-1 (XPO1). By inhibiting XPO1, selinexor prevents the nuclear export of viral ribonucleoproteins and restores the nuclear localization of host anti-inflammatory and tumor suppressor proteins, theoretically reducing viral replication and mitigating cytokine storm.
Abstract: Treatment of Severe COVID-19 with Low-Dose Selinexor:
Demonstration of Anti-Viral and Anti-Inflammatory Activities
in a Randomized, International, Multicenter,
Placebo-Controlled Phase 2 Clinical Trial
George Geils Jr., Zainab Shahid, Don Stevens, Nathan C. Bahr, Jacek Skarbinski,
Vaishali Sanchorawala, Marcelo Gareca, Ronda Oram, Miguel Marcos, Parameswaran Hari, Paul Boyce,
Enrico Lallana, John P. Haran, Guenther Koehne, Otto Yang, Catherine B. Small, Ruben Niesvizky,
Charles Brummitt, Piers Patten, Mansour Ceesay, Benjamin J. Gaborit, Ran Nir-Paz, Manish Sagar,
Michael Kauffman, Sharon Shacham, Jatin Shah, Dayana Michel, Sharon Tamir, Tami Rashal, Lingling Li,
Hong Yan, Yosef Landesman, Ralph A. Tripp, Thomas J. Walsh, Mezgebe Berhe
Disclosures – George Geils Jr.
Research Support
None
Consultant
None
Honoraria
None
Scientific Advisory Board
None
Major Stockholder
None
Speakers Bureau
Amgen, Celgene, Janssen Oncology, and Sanofi
Genzyme
©2020 Karyopharm Therapeutics Inc.
2
Exportin 1 (XPO1): Viral replication
• Exportin 1 (XPO1) mediates SARS-CoV-2 lifecycle and proinflammatory transcription
factors
• XPO1 has been identified as a “hub” host protein for SARS-CoV propagation.
• XPO1 plays a central role in inflammation through regulation of the NF-kB and COX-2
pathways
• XPO1 facilitates the nuclear export of the HMGB1, RXRα, COMMD1, PPARγ, and
GLTSCR2, all of which augment inflammatory signaling and inhibit innate immune
response to enable viral infection
©2020 Karyopharm Therapeutics Inc.
3
Selinexor (XPOVIO®️) XPO1 Inhibition: Unique Dual Mechanism
of Action with Anti-Viral and Anti-inflammatory Activities
©2020 Karyopharm Therapeutics Inc.
4
Selinexor Inhibits SARS-CoV-2 Viral
Propagation and Shedding and Induces
Nuclear Accumulation of ACE2 In Vitro
Selinexor Decreases SARS-CoV-2 Viral
Load and Severity of Rhinitis and Lung
Inflammation In Vivo
Rhinitis
©2020 Karyopharm Therapeutics Inc.
Alveolitis
5
XPORT-CoV-1001: A Phase 2 Randomized Single-Blind Study to Evaluate
the Activity and Safety of Low Dose Oral Selinexor (KPT-330) in Patients
with Severe COVID-19
~70 International Study Sites, ~8 countries
2 interim analyses (~74 randomized and ~124 randomized)
2:1 1:1
randomization
N ~ 223
Hospitalized
Patients ≥18
years old with
COVID-19
Oral Selinexor
20 mg Days 1, 3, and 5 of each week
for up to 2 weeks
If the patient is tolerating therapy well and clinically
benefitting, dosing can continue for additional 2
weeks on Days 15, 17, 19, 22, 24, 26
Oral Placebo
Days 1, 3, and 5 of each week
for up to 2 weeks
©2020 Karyopharm Therapeutics Inc.
Primary endpoints:
Day 14 Ordinal Scale Improvement (OSI) Proportion of patients with at least a 2-point improvement
in the Ordinal Scale from baseline to Day 14
Key Secondary endpoint
• Overall death rate on Day 28
• Rate of mechanical ventilation
• Time to mechanical ventilation
• Time to an improvement of 2 points using Ordinal
Scale Improvement (TTCI-2)
6
XPORT-CoV-1001: Inclusion Criteria
Eligible patients had symptoms of severe COVID-19 as demonstrated by:
At least 1 of the following:
• Fever
• Cough
• Sore throat
• Malaise
• Headache
• Muscle pain
• Shortness of breath at rest or with exertion
• Confusion
• Symptoms of severe lower respiratory
symptoms including dyspnea at rest or
respiratory distress
©2020 Karyopharm Therapeutics Inc.
Clinical signs indicative of lower
respiratory infection with COVID-19,
with at least 1 of the following:
AND
•..
Late treatment
is less effective
is less effective
