Treatments Associated with Lower Mortality among Critically Ill COVID-19 Patients: A Retrospective Cohort Study
et al., Anesthesiology, doi:10.1097/ALN.0000000000003999, Oct 2021
{kind=link}
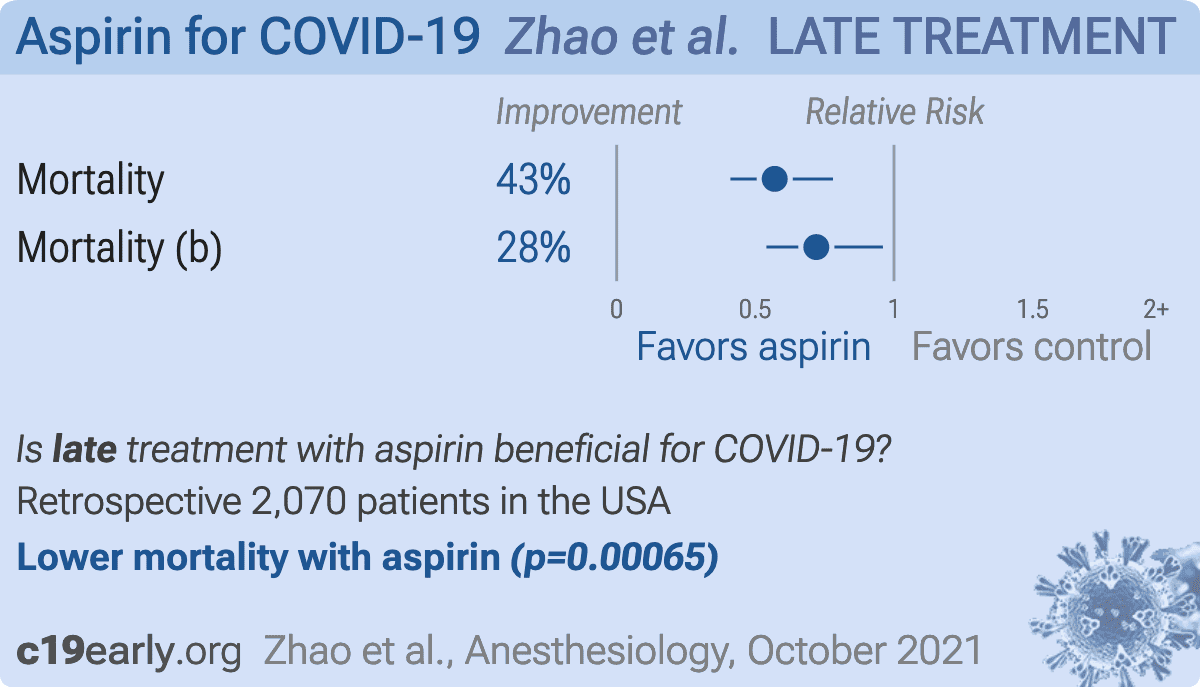
Retrospective 2,070 hospitalized patients in the USA, showing lower mortality with aspirin treatment.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
This may explain in part the very high mortality seen in this study.
Results may differ in countries with improved SOC.
|
risk of death, 43.0% lower, HR 0.57, p < 0.001, treatment 121 of 473 (25.6%), control 140 of 473 (29.6%), adjusted per study, PSM.
|
|
risk of death, 28.0% lower, HR 0.72, p = 0.03, treatment 473, control 1,597, adjusted per study, multivariable.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Zhao et al., 1 Oct 2021, retrospective, USA, peer-reviewed, 6 authors.
{kind=link}
Treatments Associated with Lower Mortality among Critically Ill COVID-19 Patients: A Retrospective Cohort Study
Anesthesiology, doi:10.1097/aln.0000000000003999
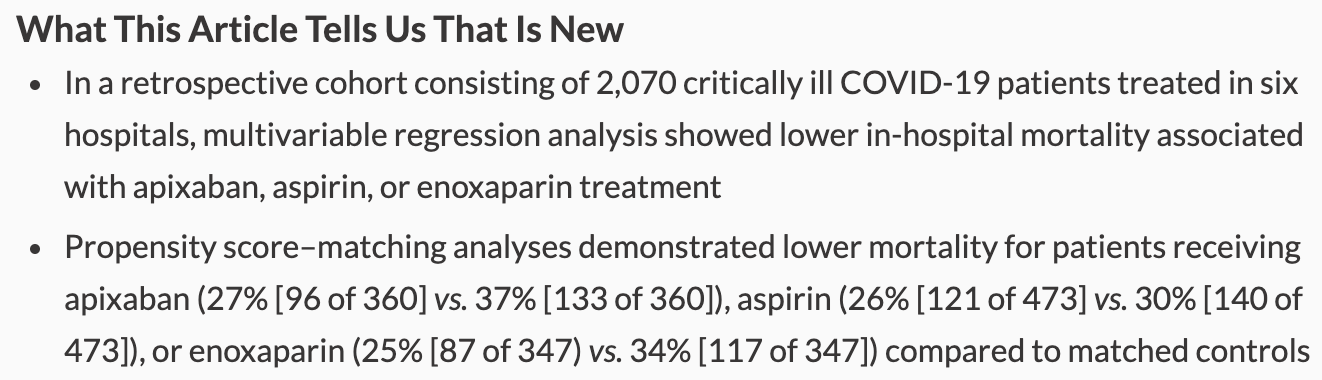
What We Already Know about This Topic • While the treatment of critically ill COVID-19 patients has improved, mortality rates remain high What This Article Tells Us That Is New • In a retrospective cohort consisting of 2,070 critically ill COVID-19 patients treated in six hospitals, multivariable regression analysis showed lower in-hospital mortality associated with apixaban, aspirin, or enoxaparin treatment • Propensity score-matching analyses demonstrated lower mortality for patients receiving apixaban (27% [96 of 360] vs. 37% [133 of 360]), aspirin (26% [121 of 473] vs. 30% [140 of 473]), or enoxaparin (25% [87 of 347) vs. 34% [117 of 347]) compared to matched controls A Particular challenge of COVID-19 treatment is the high mortality, especially among critically ill patients. Although the mortality rate was estimated to be ~50% among critically ill COVID-19 patients in the early stage of the pandemic, 1 a study performed at a later stage of the pandemic showed a downward trend of mortality rates from ~44% to ~19%. 2 Effective treatments might be one factor responsible for this decline. Continuous efforts in discovering effective treatments are needed and have been ongoing as evidenced by the recent trials exploring the effectiveness of therapeutic versus prophylactic anticoagulation in hospitalized and critically ill patients. [3] [4] [5] With the passing of the COVID-19 pandemic's first anniversary and the surge of the Delta variant, a look back at the data accumulated over 1 yr provides an opportunity to identify potentially effective treatments. Such an approach could corroborate established treatments or generate hypotheses for future investigations. This retrospective cohort study hypothesized that certain treatments would be associated with lower mortality in patients
References
Aghajani, Moradi, Amini, Tehrani, Pourheidar et al., Decreased in-hospital mortality associated with aspirin administration in hospitalized patients due to severe COVID-19, J Med Virol
Anesi, Jablonski, Harhay, Atkins, Bajaj et al., Characteristics, outcomes, and trends of patients with cOVID-19-related critical illness at a learning health system in the United States, Ann Intern Med
Beigel, Tomashek, Dodd, Mehta, Zingman et al., None
Billett, Reyes-Gil, Szymanski, Ikemura, Stahl et al., Anticoagulation in COVID-19: Effect of enoxaparin, heparin, and apixaban on mortality, Thromb Haemost
Bloch, Shoham, Casadevall, Sachais, Shaz et al., Deployment of convalescent plasma for the prevention and treatment of COVID-19, J Clin Invest
Chow, Khanna, Kethireddy, Yamane, Levine et al., Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019, Anesth Analg
Connors, Levy, COVID-19 and its implications for thrombosis and anticoagulation, Blood
Du, Kao, Zhou, He, Zhao et al., Cleavage of spike protein of SARS coronavirus by protease factor Xa is associated with viral infectivity, Biochem Biophys Res Commun
Freedberg, Conigliaro, Wang, Tracey, Callahan et al., Famotidine Research Group: Famotidine use is associated with improved clinical outcomes in hospitalized COVID-19 patients: A propensity score matched retrospective cohort study, Gastroenterology
Goligher, Bradbury, Mcverry, Lawler, Berger et al., Therapeutic anticoagulation with heparin in critically ill patients with COVID-19, N Engl J Med
Grasselli, Greco, Zanella, Albano, Antonelli et al., None
Horby, Lim, Emberson, Mafham, Bell et al., Dexamethasone in hospitalized patients with Covid-19, N Engl J Med
Horby, Mafham, Linsell, Bell, Staplin et al., Effect of hydroxychloroquine in hospitalized patients with Covid-19, N Engl J Med
Lawler, Goligher, Berger, Neal, Mcverry et al., Therapeutic anticoagulation with heparin in noncritically ill patients with COVID-19, N Engl J Med
Lin, Wei, The robust inference for the Cox proportional hazards model, J Am Stat Assoc
Lombardy, Network, Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy, JAMA Intern Med
Lopes, De, Silva, Furtado, Macedo et al., ACTION Coalition COVID-19 Brazil IV Investigators: Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): An open-label, multicentre, randomised, controlled trial, Lancet
Martha, Pranata, Lim, Wibowo, Akbar, Active prescription of low-dose aspirin during or prior to hospitalization and mortality in COVID-19: A systematic review and meta-analysis of adjusted effect estimates, Int J Infect Dis
Mcmichael, Currie, Clark, Pogosjans, Kay et al., Public Health-Seattle and King County, EvergreenHealth, and CDC COVID-19 Investigation Team: Epidemiology of Covid-19 in a long-term care facility in King County, Washington, N Engl J Med
Meizlish, Goshua, Liu, Fine, Amin et al., Intermediate-dose anticoagulation, aspirin, and in-hospital mortality in COVID-19: A propensity score-matched analysis, Am J Hematol
Minno, Ambrosino, Calcaterra, Minno, COVID-19 and venous thromboembolism: A meta-analysis of literature studies, Semin Thromb Hemost
Nadkarni, Bagiella, Chang, Moreno, Pujadas et al., Anticoagulation, bleeding, mortality, and pathology in hospitalized patients with COVID-19, J Am Coll Cardiol
Osborne, Veigulis, Arreola, Mahajan, Röösli et al., Association of mortality and aspirin prescription for COVID-19 patients at the Veterans Health Administration, PLoS One
Porfidia, Valeriani, Pola, Porreca, Rutjes et al., Venous thromboembolism in patients with COVID-19: Systematic review and meta-analysis, Thromb Res
Ra, Potential therapeutic roles for direct factor Xa inhibitors in coronavirus infections, Am J Cardiovasc Drugs
Testa, Prandoni, Paoletti, Morandini, Tala et al., Direct oral anticoagulant plasma levels' striking increase in severe COVID-19 respiratory syndrome patients treated with antiviral agents: The Cremona experience, J Thromb Haemost
Thachil, Juffermans, Ranucci, Connors, Warkentin et al., ISTH DIC subcommittee communication on anticoagulation in COVID-19, J Thromb Haemost
Wang, Zhang, Du, Du, Zhao et al., Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial, Lancet
Wenzler, Engineer, Yaqoob, Benken, Safety and efficacy of apixaban for therapeutic anticoagulation in critically ill ICU patients with severe COVID-19 respiratory disease, TH Open
Zhang, Shen, Le, Pan, Kong et al., Incidence of venous thromboembolism in hospitalized coronavirus disease 2019 patients: A systematic review and meta-analysis, Front Cardiovasc Med
DOI record:
{
"DOI": "10.1097/aln.0000000000003999",
"ISSN": [
"0003-3022",
"1528-1175"
],
"URL": "http://dx.doi.org/10.1097/ALN.0000000000003999",
"abstract": "<jats:sec>\n <jats:title>Background</jats:title>\n <jats:p>Mortality in critically ill COVID-19 patients remains high. Although randomized controlled trials must continue to definitively evaluate treatments, further hypothesis-generating efforts to identify candidate treatments are required. This study’s hypothesis was that certain treatments are associated with lower COVID-19 mortality.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Methods</jats:title>\n <jats:p>This was a 1-yr retrospective cohort study involving all COVID-19 patients admitted to intensive care units in six hospitals affiliated with Yale New Haven Health System from February 13, 2020, to March 4, 2021. The exposures were any COVID-19–related pharmacologic and organ support treatments. The outcome was in-hospital mortality.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Results</jats:title>\n <jats:p>This study analyzed 2,070 patients after excluding 23 patients who died within 24 h after intensive care unit admission and 3 patients who remained hospitalized on the last day of data censoring. The in-hospital mortality was 29% (593 of 2,070). Of 23 treatments analyzed, apixaban (hazard ratio, 0.42; 95% CI, 0.363 to 0.48; corrected CI, 0.336 to 0.52) and aspirin (hazard ratio, 0.72; 95% CI, 0.60 to 0.87; corrected CI, 0.54 to 0.96) were associated with lower mortality based on the multivariable analysis with multiple testing correction. Propensity score–matching analysis showed an association between apixaban treatment and lower mortality (with vs. without apixaban, 27% [96 of 360] vs. 37% [133 of 360]; hazard ratio, 0.48; 95% CI, 0.337 to 0.69) and an association between aspirin treatment and lower mortality (with vs. without aspirin, 26% [121 of 473] vs. 30% [140 of 473]; hazard ratio, 0.57; 95% CI, 0.41 to 0.78). Enoxaparin showed similar associations based on the multivariable analysis (hazard ratio, 0.82; 95% CI, 0.69 to 0.97; corrected CI, 0.61 to 1.05) and propensity score–matching analysis (with vs. without enoxaparin, 25% [87 of 347] vs. 34% [117 of 347]; hazard ratio, 0.53; 95% CI, 0.367 to 0.77).</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Conclusions</jats:title>\n <jats:p>Consistent with the known hypercoagulability in severe COVID-19, the use of apixaban, enoxaparin, or aspirin was independently associated with lower mortality in critically ill COVID-19 patients.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Editor’s Perspective</jats:title>\n <jats:sec>\n <jats:title>What We Already Know about This Topic</jats:title>\n </jats:sec>\n <jats:sec>\n <jats:title>What This Article Tells Us That Is New</jats:title>\n </jats:sec>\n </jats:sec>",
"author": [
{
"affiliation": [
{
"name": "Department of Anesthesiology, Yale University School of Medicine, New Haven, Connecticut"
}
],
"family": "Zhao",
"given": "Xu",
"sequence": "first"
},
{
"affiliation": [
{
"name": "the Department of Medicine, Division of Physical Medicine and Rehabilitation, McGill University Health Center, Montreal, Quebec, Canada"
}
],
"family": "Gao",
"given": "Chan",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "the Department of Biostatistics, Yale University School of Public Health, New Haven, Connecticut"
}
],
"family": "Dai",
"given": "Feng",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Anesthesiology, Yale University School of Medicine, New Haven, Connecticut"
}
],
"family": "Treggiari",
"given": "Miriam M.",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Anesthesiology, Yale University School of Medicine, New Haven, Connecticut"
}
],
"family": "Deshpande",
"given": "Ranjit",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-5168-5084",
"affiliation": [
{
"name": "Department of Anesthesiology, Yale University School of Medicine, New Haven, Connecticut"
}
],
"authenticated-orcid": true,
"family": "Meng",
"given": "Lingzhong",
"sequence": "additional"
}
],
"container-title": "Anesthesiology",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T20:30:01Z",
"timestamp": 1633120201000
},
"deposited": {
"date-parts": [
[
2021,
12,
8
]
],
"date-time": "2021-12-08T22:30:58Z",
"timestamp": 1639002658000
},
"indexed": {
"date-parts": [
[
2022,
10,
5
]
],
"date-time": "2022-10-05T07:59:29Z",
"timestamp": 1664956769618
},
"is-referenced-by-count": 3,
"issue": "6",
"issued": {
"date-parts": [
[
2021,
10,
1
]
]
},
"journal-issue": {
"issue": "6",
"published-online": {
"date-parts": [
[
2021,
10,
1
]
]
},
"published-print": {
"date-parts": [
[
2021,
12,
1
]
]
}
},
"language": "en",
"link": [
{
"URL": "https://pubs.asahq.org/anesthesiology/article-pdf/135/6/1076/527622/20211200.0-00025.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "syndication"
},
{
"URL": "https://pubs.asahq.org/anesthesiology/article-pdf/135/6/1076/527622/20211200.0-00025.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "276",
"original-title": [],
"page": "1076-1090",
"prefix": "10.1097",
"published": {
"date-parts": [
[
2021,
10,
1
]
]
},
"published-online": {
"date-parts": [
[
2021,
10,
1
]
]
},
"published-print": {
"date-parts": [
[
2021,
12,
1
]
]
},
"publisher": "Ovid Technologies (Wolters Kluwer Health)",
"reference": [
{
"DOI": "10.1001/jamainternmed.2020.3539",
"article-title": "Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy.",
"author": "Grasselli",
"doi-asserted-by": "crossref",
"first-page": "1345",
"journal-title": "JAMA Intern Med",
"key": "2021120822165406200_R1",
"volume": "180",
"year": "2020"
},
{
"DOI": "10.7326/M20-5327",
"article-title": "Characteristics, outcomes, and trends of patients with cOVID-19–related critical illness at a learning health system in the United States.",
"author": "Anesi",
"doi-asserted-by": "crossref",
"first-page": "613",
"journal-title": "Ann Intern Med",
"key": "2021120822165406200_R2",
"volume": "174",
"year": "2021"
},
{
"DOI": "10.1056/NEJMoa2105911",
"article-title": "Therapeutic anticoagulation with heparin in noncritically ill patients with COVID-19.",
"author": "Lawler",
"doi-asserted-by": "crossref",
"first-page": "790",
"journal-title": "N Engl J Med",
"key": "2021120822165406200_R3",
"volume": "385",
"year": "2021"
},
{
"DOI": "10.1056/NEJMoa2103417",
"article-title": "Therapeutic anticoagulation with heparin in critically ill patients with COVID-19.",
"author": "Goligher",
"doi-asserted-by": "crossref",
"first-page": "777",
"journal-title": "N Engl J Med",
"key": "2021120822165406200_R4",
"volume": "385",
"year": "2021"
},
{
"DOI": "10.1016/S0140-6736(21)01203-4",
"article-title": "Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): An open-label, multicentre, randomised, controlled trial.",
"author": "Lopes",
"doi-asserted-by": "crossref",
"first-page": "2253",
"journal-title": "Lancet",
"key": "2021120822165406200_R5",
"volume": "397",
"year": "2021"
},
{
"DOI": "10.1080/01621459.1989.10478874",
"article-title": "The robust inference for the Cox proportional hazards model.",
"author": "Lin",
"doi-asserted-by": "crossref",
"first-page": "1074",
"journal-title": "J Am Stat Assoc",
"key": "2021120822165406200_R6",
"volume": "84",
"year": "1989"
},
{
"DOI": "10.1016/S0140-6736(20)31022-9",
"article-title": "Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial.",
"author": "Wang",
"doi-asserted-by": "crossref",
"first-page": "1569",
"journal-title": "Lancet",
"key": "2021120822165406200_R7",
"volume": "395",
"year": "2020"
},
{
"DOI": "10.1056/NEJMoa2007764",
"article-title": "Remdesivir for the treatment of COVID-19: Final report.",
"author": "Beigel",
"doi-asserted-by": "crossref",
"first-page": "1813",
"journal-title": "N Engl J Med",
"key": "2021120822165406200_R8",
"volume": "383",
"year": "2020"
},
{
"DOI": "10.1056/NEJMoa2021436",
"article-title": "Dexamethasone in hospitalized patients with Covid-19.",
"author": "Horby",
"doi-asserted-by": "crossref",
"first-page": "693",
"journal-title": "N Engl J Med",
"key": "2021120822165406200_R9",
"volume": "384",
"year": "2021"
},
{
"DOI": "10.1056/NEJMoa2022926",
"article-title": "Effect of hydroxychloroquine in hospitalized patients with Covid-19.",
"author": "Horby",
"doi-asserted-by": "crossref",
"first-page": "2030",
"journal-title": "N Engl J Med",
"key": "2021120822165406200_R10",
"volume": "383",
"year": "2020"
},
{
"DOI": "10.1172/JCI138745",
"article-title": "Deployment of convalescent plasma for the prevention and treatment of COVID-19.",
"author": "Bloch",
"doi-asserted-by": "crossref",
"first-page": "2757",
"journal-title": "J Clin Invest",
"key": "2021120822165406200_R11",
"volume": "130",
"year": "2020"
},
{
"DOI": "10.1053/j.gastro.2020.05.053",
"article-title": "Famotidine use is associated with improved clinical outcomes in hospitalized COVID-19 patients: A propensity score matched retrospective cohort study.",
"author": "Freedberg",
"doi-asserted-by": "crossref",
"first-page": "1129",
"journal-title": "Gastroenterology",
"key": "2021120822165406200_R12",
"volume": "159",
"year": "2020"
},
{
"DOI": "10.1016/j.thromres.2020.08.020",
"article-title": "Venous thromboembolism in patients with COVID-19: Systematic review and meta-analysis.",
"author": "Porfidia",
"doi-asserted-by": "crossref",
"first-page": "67",
"journal-title": "Thromb Res",
"key": "2021120822165406200_R13",
"volume": "196",
"year": "2020"
},
{
"DOI": "10.3389/fcvm.2020.00151",
"article-title": "Incidence of venous thromboembolism in hospitalized coronavirus disease 2019 patients: A systematic review and meta-analysis.",
"author": "Zhang",
"doi-asserted-by": "crossref",
"first-page": "151",
"journal-title": "Front Cardiovasc Med",
"key": "2021120822165406200_R14",
"volume": "7",
"year": "2020"
},
{
"DOI": "10.1055/s-0040-1715456",
"article-title": "COVID-19 and venous thromboembolism: A meta-analysis of literature studies.",
"author": "Di Minno",
"doi-asserted-by": "crossref",
"first-page": "763",
"journal-title": "Semin Thromb Hemost",
"key": "2021120822165406200_R15",
"volume": "46",
"year": "2020"
},
{
"DOI": "10.1056/NEJMoa2005412",
"article-title": "Epidemiology of Covid-19 in a long-term care facility in King County, Washington.",
"author": "McMichael",
"doi-asserted-by": "crossref",
"first-page": "2005",
"journal-title": "N Engl J Med",
"key": "2021120822165406200_R16",
"volume": "382",
"year": "2020"
},
{
"DOI": "10.1182/blood.2020006000",
"article-title": "COVID-19 and its implications for thrombosis and anticoagulation.",
"author": "Connors",
"doi-asserted-by": "crossref",
"first-page": "2033",
"journal-title": "Blood",
"key": "2021120822165406200_R17",
"volume": "135",
"year": "2020"
},
{
"DOI": "10.1111/jth.15004",
"article-title": "ISTH DIC subcommittee communication on anticoagulation in COVID-19.",
"author": "Thachil",
"doi-asserted-by": "crossref",
"first-page": "2138",
"journal-title": "J Thromb Haemost",
"key": "2021120822165406200_R18",
"volume": "18",
"year": "2020"
},
{
"DOI": "10.1016/j.jacc.2020.08.041",
"article-title": "Anticoagulation, bleeding, mortality, and pathology in hospitalized patients with COVID-19.",
"author": "Nadkarni",
"doi-asserted-by": "crossref",
"first-page": "1815",
"journal-title": "J Am Coll Cardiol",
"key": "2021120822165406200_R19",
"volume": "76",
"year": "2020"
},
{
"DOI": "10.1055/s-0040-1720978",
"article-title": "Anticoagulation in COVID-19: Effect of enoxaparin, heparin, and apixaban on mortality.",
"author": "Billett",
"doi-asserted-by": "crossref",
"first-page": "1691",
"journal-title": "Thromb Haemost",
"key": "2021120822165406200_R20",
"volume": "120",
"year": "2020"
},
{
"DOI": "10.1055/s-0040-1720962",
"article-title": "Safety and efficacy of apixaban for therapeutic anticoagulation in critically ill ICU patients with severe COVID-19 respiratory disease.",
"author": "Wenzler",
"doi-asserted-by": "crossref",
"first-page": "e376",
"journal-title": "TH Open",
"key": "2021120822165406200_R21",
"volume": "4",
"year": "2020"
},
{
"DOI": "10.1007/s40256-020-00438-6",
"article-title": "Potential therapeutic roles for direct factor Xa inhibitors in coronavirus infections.",
"author": "Al-Horani",
"doi-asserted-by": "crossref",
"first-page": "525",
"journal-title": "Am J Cardiovasc Drugs",
"key": "2021120822165406200_R22",
"volume": "20",
"year": "2020"
},
{
"DOI": "10.1016/j.bbrc.2007.05.092",
"article-title": "Cleavage of spike protein of SARS coronavirus by protease factor Xa is associated with viral infectivity.",
"author": "Du",
"doi-asserted-by": "crossref",
"first-page": "174",
"journal-title": "Biochem Biophys Res Commun",
"key": "2021120822165406200_R23",
"volume": "359",
"year": "2007"
},
{
"DOI": "10.1111/jth.14871",
"article-title": "Direct oral anticoagulant plasma levels’ striking increase in severe COVID-19 respiratory syndrome patients treated with antiviral agents: The Cremona experience.",
"author": "Testa",
"doi-asserted-by": "crossref",
"first-page": "1320",
"journal-title": "J Thromb Haemost",
"key": "2021120822165406200_R24",
"volume": "18",
"year": "2020"
},
{
"DOI": "10.1213/ANE.0000000000005292",
"article-title": "Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019.",
"author": "Chow",
"doi-asserted-by": "crossref",
"first-page": "930",
"journal-title": "Anesth Analg",
"key": "2021120822165406200_R25",
"volume": "132",
"year": "2021"
},
{
"DOI": "10.1002/jmv.27053",
"article-title": "Decreased in-hospital mortality associated with aspirin administration in hospitalized patients due to severe COVID-19.",
"author": "Haji Aghajani",
"doi-asserted-by": "crossref",
"first-page": "5390",
"journal-title": "J Med Virol",
"key": "2021120822165406200_R26",
"volume": "93",
"year": "2021"
},
{
"DOI": "10.1371/journal.pone.0246825",
"article-title": "Association of mortality and aspirin prescription for COVID-19 patients at the Veterans Health Administration.",
"author": "Osborne",
"doi-asserted-by": "crossref",
"first-page": "e0246825",
"journal-title": "PLoS One",
"key": "2021120822165406200_R27",
"volume": "16",
"year": "2021"
},
{
"DOI": "10.1002/ajh.26102",
"article-title": "Intermediate-dose anticoagulation, aspirin, and in-hospital mortality in COVID-19: A propensity score–matched analysis.",
"author": "Meizlish",
"doi-asserted-by": "crossref",
"first-page": "471",
"journal-title": "Am J Hematol",
"key": "2021120822165406200_R28",
"volume": "96",
"year": "2021"
},
{
"DOI": "10.1016/j.ijid.2021.05.016",
"article-title": "Active prescription of low-dose aspirin during or prior to hospitalization and mortality in COVID-19: A systematic review and meta-analysis of adjusted effect estimates.",
"author": "Martha",
"doi-asserted-by": "crossref",
"first-page": "6",
"journal-title": "Int J Infect Dis",
"key": "2021120822165406200_R29",
"volume": "108",
"year": "2021"
}
],
"reference-count": 29,
"references-count": 29,
"relation": {},
"resource": {
"primary": {
"URL": "https://pubs.asahq.org/anesthesiology/article/135/6/1076/117698/Treatments-Associated-with-Lower-Mortality-among"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Anesthesiology and Pain Medicine"
],
"subtitle": [],
"title": "Treatments Associated with Lower Mortality among Critically Ill COVID-19 Patients: A Retrospective Cohort Study",
"type": "journal-article",
"volume": "135"
}
Late treatment
is less effective
is less effective
