
COVID-19 Monoclonal Antibody Use at a Stand Alone Children’s Hospital
et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofad500.615, Nov 2023
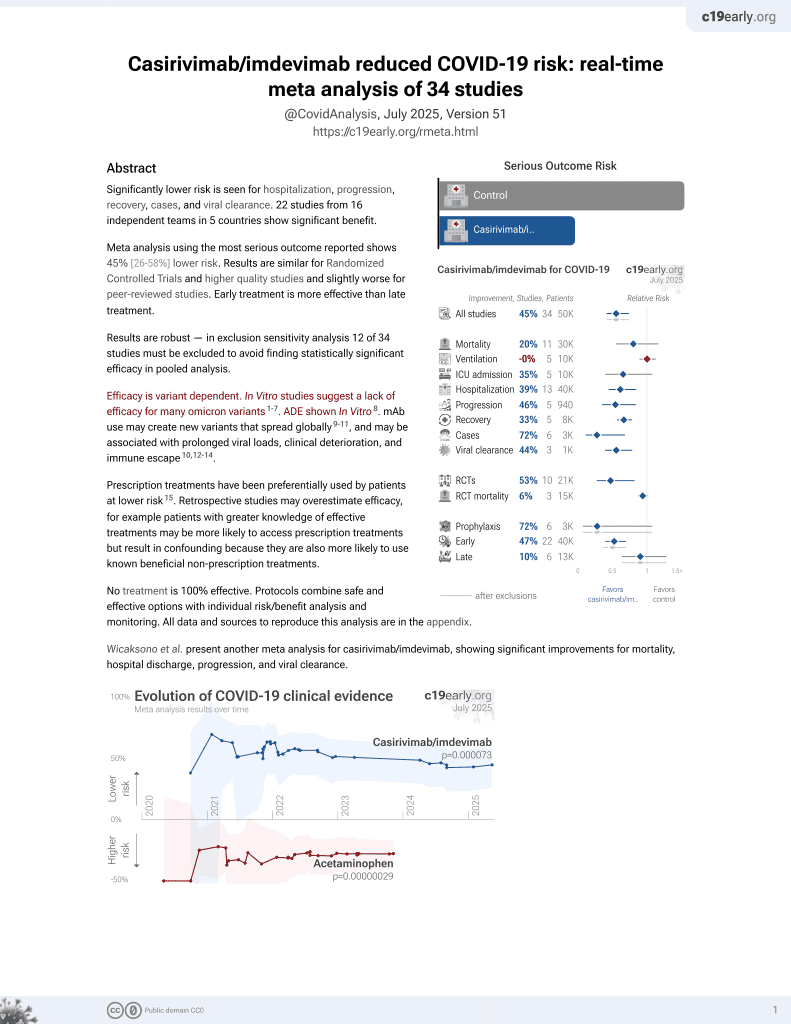
18th treatment shown to reduce risk in
March 2021, now with p = 0.000095 from 34 studies, recognized in 52 countries.
Efficacy is variant dependent.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
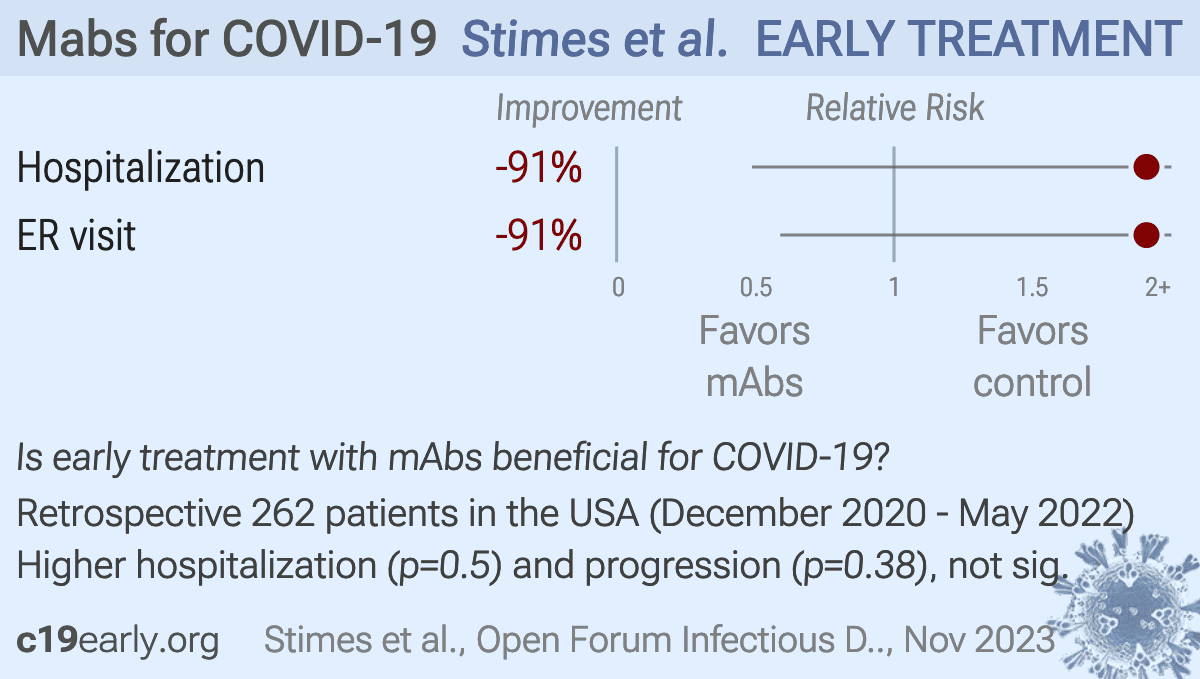
Retrospective 262 pediatric patients referred for COVID-19 monoclonal antibody treatment, 134 treated (74% receiving casirivimab/imdevimab), showing higher ER visits and hospitalization with treatment, without statistical significance. Authors do not provide results for specific treatments.
Efficacy is variant dependent. In Vitro research suggests a lack of efficacy for many omicron variants1-7.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments8.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of hospitalization, 91.0% higher, RR 1.91, p = 0.50, treatment 6 of 134 (4.5%), control 3 of 128 (2.3%).
|
|
ER visit, 91.0% higher, RR 1.91, p = 0.38, treatment 8 of 134 (6.0%), control 4 of 128 (3.1%).
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
1.
Liu et al., Striking Antibody Evasion Manifested by the Omicron Variant of SARS-CoV-2, bioRxiv, doi:10.1101/2021.12.14.472719.
2.
Sheward et al., Variable loss of antibody potency against SARS-CoV-2 B.1.1.529 (Omicron), bioRxiv, doi:10.1101/2021.12.19.473354.
3.
VanBlargan et al., An infectious SARS-CoV-2 B.1.1.529 Omicron virus escapes neutralization by several therapeutic monoclonal antibodies, bioRxiv, doi:10.1101/2021.12.15.472828.
4.
Tatham et al., Lack of Ronapreve (REGN-CoV; casirivimab and imdevimab) virological efficacy against the SARS-CoV 2 Omicron variant (B.1.1.529) in K18-hACE2 mice, bioRxiv, doi:10.1101/2022.01.23.477397.
5.
Pochtovyi et al., In Vitro Efficacy of Antivirals and Monoclonal Antibodies against SARS-CoV-2 Omicron Lineages XBB.1.9.1, XBB.1.9.3, XBB.1.5, XBB.1.16, XBB.2.4, BQ.1.1.45, CH.1.1, and CL.1, Vaccines, doi:10.3390/vaccines11101533.
6.
Haars et al., Prevalence of SARS-CoV-2 Omicron Sublineages and Spike Protein Mutations Conferring Resistance against Monoclonal Antibodies in a Swedish Cohort during 2022–2023, Microorganisms, doi:10.3390/microorganisms11102417.
Stimes et al., 27 Nov 2023, USA, peer-reviewed, 6 authors, study period 1 December, 2020 - 5 May, 2022.
{kind=link}
50 vs WA1). Evaluation of CH.1.1 and XBF by introducing variant-defining mutations into the replicon showed no change in in vitro susceptibility (< 1.8-fold change). Phenotyping of clinical isolates of BF.7, BQ.1, XBB.1.5, and CH.1.1 indicated no loss of RDV or ODV in vitro antiviral activity (< 1.3-fold change).
DOI record:
{
"DOI": "10.1093/ofid/ofad500.615",
"ISSN": [
"2328-8957"
],
"URL": "http://dx.doi.org/10.1093/ofid/ofad500.615",
"abstract": "<jats:title>Abstract</jats:title>\n <jats:sec>\n <jats:title>Background</jats:title>\n <jats:p>Texas Children’s Hospital (TCH) implemented an outpatient clinic for eligible patients to receive infusions when COVID monoclonal antibodies (mAbs) were approved for use in non-hospitalized, high-risk patients with mild to moderate COVID-19. There are limited data evaluating the use of outpatient COVID mAbs in pediatric patients. We describe the clinical characteristics and outcomes of the patients treated with COVID mAbs at TCH.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Methods</jats:title>\n <jats:p>Patients that were referred to receive COVID mAbs from 12/1/2020 to 5/5/2022 were included. Information collected included demographics, comorbidities, refusal reason, adverse events, emergency center (EC) visits or admission within 14 days after final dose, and EC visit or admission within 14 days of referral if patients did not receive COVID mAbs. Chi-square was used to determine differences between the groups.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Results</jats:title>\n <jats:p>There were 262 patients referred during the study period. The median age of all referred patients was 15.8 years (IQR 14-17.4 years). Majority of referrals were for treatment of COVID-19 infection rather than post-exposure prophylaxis (92.8% vs 7.2%). Of the 262 referrals, 134 patients received COVID mAbs (51.2%) while 128 patients were not treated. Majority of the patients received casirivimab-imdevimab (73.9%). The comorbidities of all patients are shown in Figure 1. The most common reasons for patients to not receive COVID mAbs were no drug available or not listed, and the full list of reasons are listed in Figure 2. The median time from reported symptom onset to infusion was 4 days (IQR 2-6 days). Of the 134 infused patients, 8 patients (6%) visited the EC within 14 days from infusion, and 6 (4.5%) were admitted while 4 patients (3.1%) that did not receive an antibody visited the EC resulting in 3 admissions (2.3%) (EC visits p=0.27; admissions p=0.34). There were 11 patients (8.2%) that experienced adverse events from their infusion, which led to 5 of the 8 EC visits. Comorbidities were similar across the infused and non-infused groups (p=0.16).</jats:p>\n <jats:p />\n <jats:p>Number of high-risk conditions represented by all referred, high-risk patients</jats:p>\n <jats:p />\n <jats:p>Number of patients for each reason for not receiving a COVID-19 antibody infusion</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Conclusion</jats:title>\n <jats:p>COVID mAb treatments were well tolerated among pediatric patients. Majority of patients in both groups did not require EC visit or hospitalization. More data are needed to determine the clinical efficacy of mAbs patients.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Disclosures</jats:title>\n <jats:p>Flor M. Munoz, MD, MSc, CDC respiratory virus surveillance: Grant/Research Support|Gilead: Grant/Research Support|Moderna, sanofi, aztra zeneca, Merck, GSK: Advisor/Consultant|NIH: DSMB|NIH COVID-19 vaccines in pregnancy: Grant/Research Support|Pfizer Pediatric COVID-19 vaccines: Grant/Research Support|Pfizer, Dynavax, Monderna, Meissa, NIH: DSMB Lisa Forbes Satter, MD, ADMA: Advisor/Consultant|CsL Behring: Advisor/Consultant|Grifols: Advisor/Consultant|incyte: Advisor/Consultant|Pharming: Advisor/Consultant|Takeda: Advisor/Consultant</jats:p>\n </jats:sec>",
"author": [
{
"affiliation": [
{
"name": "Texas Children's Hospital , Houston, Texas"
}
],
"family": "Stimes",
"given": "Grant T",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Texas Children's Hospital , Houston, Texas"
}
],
"family": "Rodriguez",
"given": "Brittany",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Texas Children's Hospital , Houston, Texas"
}
],
"family": "Gillispie",
"given": "Amanda",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Texas Children's Hospital , Houston, Texas"
}
],
"family": "Hilliard",
"given": "Tanya J",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Baylor College of Medicine , Houston, TX"
}
],
"family": "Munoz",
"given": "Flor M",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Baylor College of Medicine , Houston, TX"
}
],
"family": "Satter",
"given": "Lisa Forbes",
"sequence": "additional"
}
],
"container-title": "Open Forum Infectious Diseases",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T02:13:24Z",
"timestamp": 1701051204000
},
"deposited": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T02:13:25Z",
"timestamp": 1701051205000
},
"indexed": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T05:18:16Z",
"timestamp": 1701062296969
},
"is-referenced-by-count": 0,
"issue": "Supplement_2",
"issued": {
"date-parts": [
[
2023,
11,
27
]
]
},
"journal-issue": {
"issue": "Supplement_2",
"published-print": {
"date-parts": [
[
2023,
11,
27
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://creativecommons.org/licenses/by/4.0/",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T00:00:00Z",
"timestamp": 1701043200000
}
}
],
"link": [
{
"URL": "https://academic.oup.com/ofid/article-pdf/10/Supplement_2/ofad500.615/53772285/ofad500.615.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "syndication"
},
{
"URL": "https://academic.oup.com/ofid/article-pdf/10/Supplement_2/ofad500.615/53772285/ofad500.615.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "286",
"original-title": [],
"prefix": "10.1093",
"published": {
"date-parts": [
[
2023,
11,
27
]
]
},
"published-online": {
"date-parts": [
[
2023,
11,
27
]
]
},
"published-other": {
"date-parts": [
[
2023,
12
]
]
},
"published-print": {
"date-parts": [
[
2023,
11,
27
]
]
},
"publisher": "Oxford University Press (OUP)",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "https://academic.oup.com/ofid/article/doi/10.1093/ofid/ofad500.615/7448106"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Infectious Diseases",
"Oncology"
],
"subtitle": [],
"title": "546. COVID-19 Monoclonal Antibody Use at a Stand Alone Children’s Hospital",
"type": "journal-article",
"volume": "10"
}