Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: a study in 48 440 adult patients
et al., British Journal of Sports Medicine, doi:10.1136/bjsports-2021-104080, Apr 2021
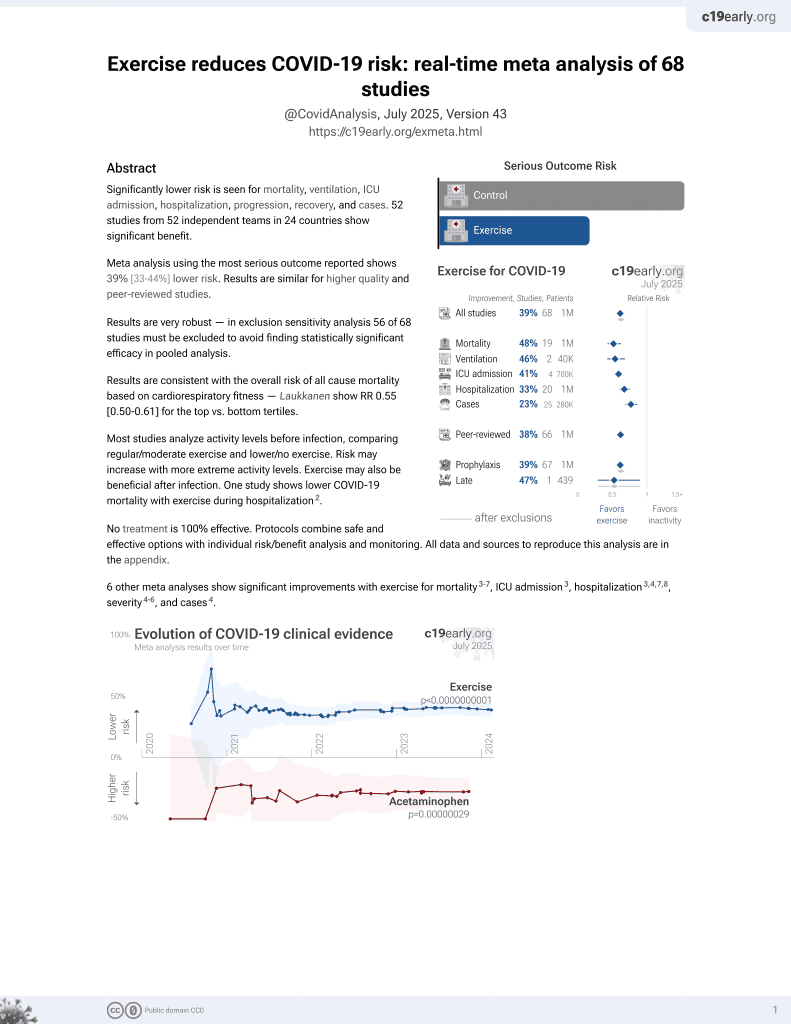
Exercise for COVID-19
9th treatment shown to reduce risk in
October 2020, now with p < 0.00000000001 from 68 studies.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
Retrospective 48,440 COVID-19 patients in the USA, showing significantly lower mortality, ICU admission, and hospitalization with exercise.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
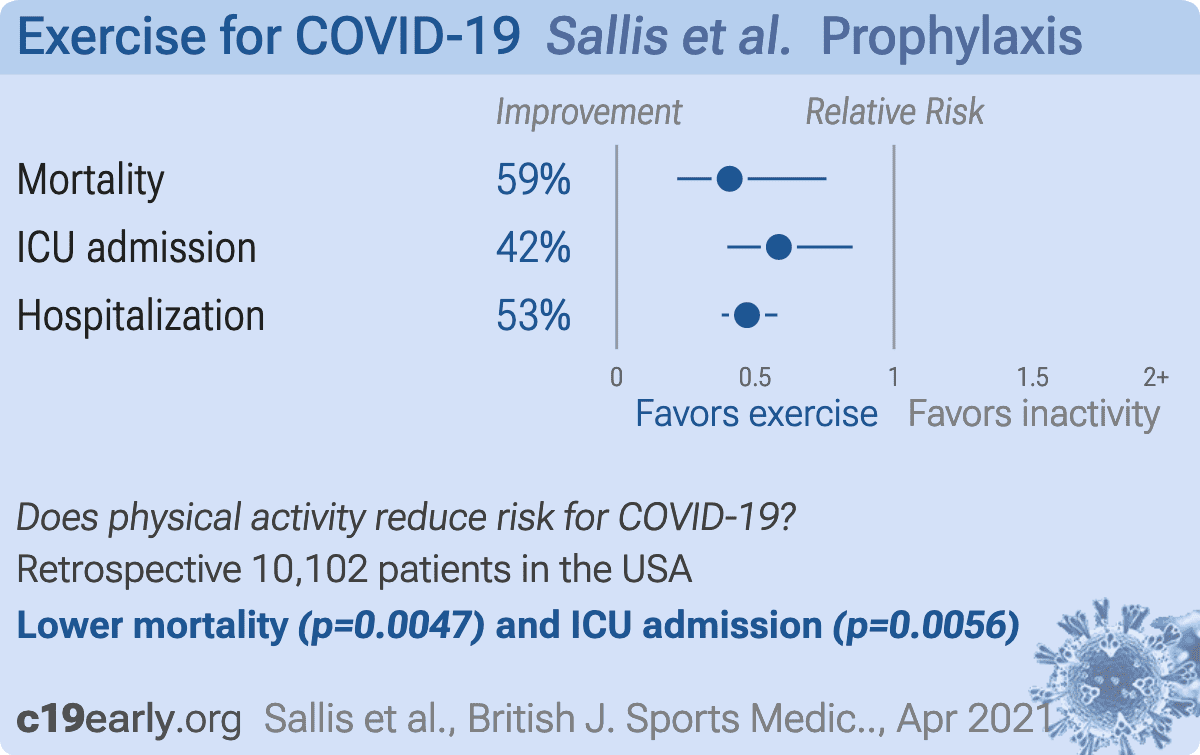
risk of death, 59.2% lower, RR 0.41, p = 0.005, high activity levels 11 of 3,118 (0.4%), low activity levels 170 of 6,984 (2.4%), adjusted per study, inverted to make RR<1 favor high activity levels, odds ratio converted to relative risk, consistently active vs. consistently inactive, multivariable.
|
|
risk of ICU admission, 41.5% lower, RR 0.58, p = 0.006, high activity levels 32 of 3,118 (1.0%), low activity levels 195 of 6,984 (2.8%), adjusted per study, inverted to make RR<1 favor high activity levels, odds ratio converted to relative risk, consistently active vs. consistently inactive, multivariable.
|
|
risk of hospitalization, 53.0% lower, RR 0.47, p < 0.001, high activity levels 99 of 3,118 (3.2%), low activity levels 732 of 6,984 (10.5%), adjusted per study, inverted to make RR<1 favor high activity levels, odds ratio converted to relative risk, consistently active vs. consistently inactive, multivariable.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Sallis et al., 13 Apr 2021, retrospective, USA, peer-reviewed, 8 authors.
{kind=link}
Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: a study in 48 440 adult patients
British Journal of Sports Medicine, doi:10.1136/bjsports-2021-104080
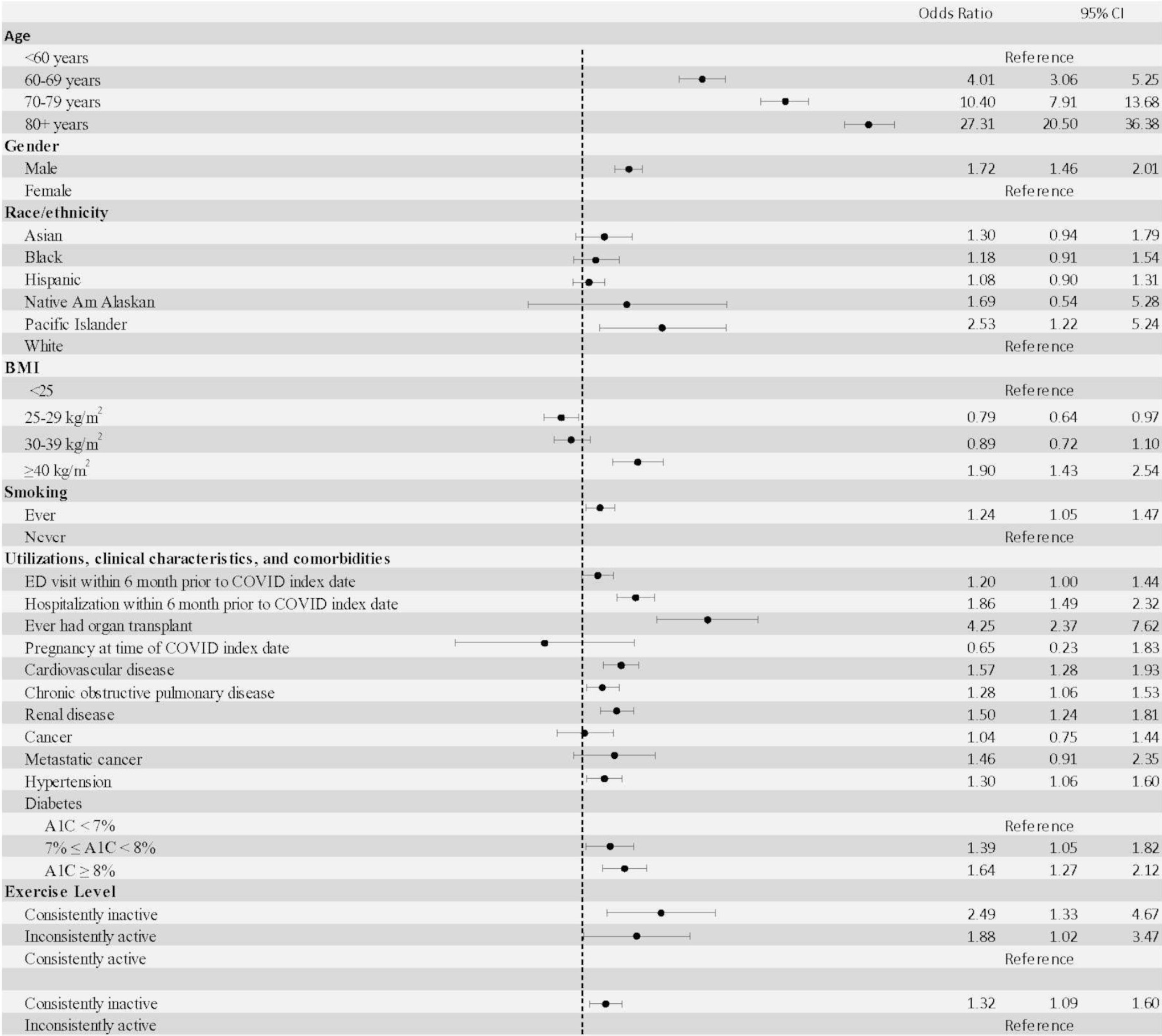
Objectives To compare hospitalisation rates, intensive care unit (ICU) admissions and mortality for patients with COVID-19 who were consistently inactive, doing some activity or consistently meeting physical activity guidelines. Methods We identified 48 440 adult patients with a COVID-19 diagnosis from 1 January 2020 to 21 October 2020, with at least three exercise vital sign measurements from 19 March 2018 to 18 March 2020. We linked each patient's self-reported physical activity category (consistently inactive=0-10 min/ week, some activity=11-149 min/week, consistently meeting guidelines=150+ min/week) to the risk of hospitalisation, ICU admission and death after COVID-19 diagnosis. We conducted multivariable logistic regression controlling for demographics and known risk factors to assess whether inactivity was associated with COVID-19 outcomes. Results Patients with COVID-19 who were consistently inactive had a greater risk of hospitalisation (OR 2.26; 95% CI 1.81 to 2.83), admission to the ICU (OR 1.73; 95% CI 1.18 to 2.55) and death (OR 2.49; 95% CI 1.33 to 4.67) due to COVID-19 than patients who were consistently meeting physical activity guidelines. Patients who were consistently inactive also had a greater risk of hospitalisation (OR 1.20; 95% CI 1.10 to 1.32), admission to the ICU (OR 1.10; 95% CI 0.93 to 1.29) and death (OR 1.32; 95% CI 1.09 to 1.60) due to COVID-19 than patients who were doing some physical activity. Conclusions Consistently meeting physical activity guidelines was strongly associated with a reduced risk for severe COVID-19 outcomes among infected adults. We recommend efforts to promote physical activity be prioritised by public health agencies and incorporated into routine medical care. This is a retrospective observational study in which PA was documented in the EHR in the 2 years preceding the March 2020 pandemic lockdown.
Competing interests SYT reports grants from Roche/Genentech during the conduct of the study.
Patient consent for publication Not required. Ethics approval This study was approved by the Kaiser Permanente Southern California Institutional Review Board. Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Summary box What are the findings? ► Patients with COVID-19 who were consistently inactive during the 2 years preceding the pandemic were more likely to be hospitalised, admitted to the intensive care unit and die than patients who were consistently meeting physical activity guidelines. ► Other than advanced age and a history of organ transplant, physical inactivity was the strongest risk factor for..
References
Ammar, Brach, Trabelsi, Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey, Nutrients, doi:10.3390/nu12061583
Buitrago-Garcia, Egli-Gany, Counotte, Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: a living systematic review and meta-analysis, PLoS Med, doi:10.1371/journal.pmed.1003346
Bull, Ss, Biddle, World Health organization 2020 guidelines on physical activity and sedentary behaviour, Br J Sports Med, doi:10.1136/bjsports-2020-102955
Burtscher, Millet, Burtscher, Low cardiorespiratory and mitochondrial fitness as risk factors in viral infections: implications for COVID-19, British Journal of sports medicine
Coleman, Ngor, Reynolds, Initial validation of an exercise "vital sign" in electronic medical records, Med Sci Sports Exerc, doi:10.1249/MSS.0b013e3182630ec1
Da Silveira, Da, Fagundes, Bizuti, Physical exercise as a tool to help the immune system against COVID-19: an integrative review of the current literature, Clin Exp Med, doi:10.1007/s10238-020-00650-3
Duncan, Avery, Seto, Perceived change in physical activity levels and mental health during COVID-19: findings among adult twin pairs, PLoS One, doi:10.1371/journal.pone.0237695
Greenland, Mansournia, Altman, Sparse data bias: a problem hiding in plain sight, BMJ, doi:10.1136/bmj.i1981
Guthold, Stevens, Riley, Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1•9 million participants, Lancet Glob Health, doi:10.1016/S2214-109X(18)30357-7
Honey-Roses, Anguelovski, Bohigas, The impact of COVID-19 on public space: a review of the emerging questions
Katzmarzyk, Friedenreich, Shiroma, Physical inactivity and noncommunicable disease burden in low-income, middle-income and high-income countries, Br J Sports Med, doi:10.1136/bjsports-2020-103640
Koebnick, Langer-Gould, Gould, Sociodemographic characteristics of members of a large, integrated health care system: comparison with us census bureau data, Perm J, doi:10.7812/TPP/12-031
Kuntz, Young, Saelens, Validity of the exercise vital sign tool to assess physical activity, Am J Prev Med
Meyer, Mcdowell, Lansing, Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 us adults, Int J Environ Res Public Health, doi:10.3390/ijerph17186469
Nieman, Wentz, The compelling link between physical activity and the body's defense system, J Sport Health Sci, doi:10.1016/j.jshs.2018.09.009
Pedersen, Saltin, Exercise as medicine -evidence for prescribing exercise as therapy in 26 different chronic diseases, Scand J Med Sci Sports, doi:10.1111/sms.12581
Piercy, Troiano, Ballard, The physical activity guidelines for Americans, JAMA, doi:10.1001/jama.2018.14854
Rogers, Waterlow, Brindle, Behavioral change towards reduced intensity physical activity is disproportionately prevalent among adults with serious health issues or Self-Perception of high risk during the UK COVID-19 Lockdown, Front Public Health, doi:10.3389/fpubh.2020.575091
Ross, Blair, Arena, Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart association, Circulation, doi:10.1161/CIR.0000000000000461
Sallis, Adlakha, Oyeyemi, An international physical activity and public health research agenda to inform coronavirus disease-2019 policies and practices, J Sport Health Sci, doi:10.1016/j.jshs.2020.05.005
Sallis, Floyd, Rodríguez, Role of built environments in physical activity, obesity, and cardiovascular disease, Circulation, doi:10.1161/CIRCULATIONAHA.110.969022
Sallis, None, Br Sports Med
Stamatakis, Bull, Putting physical activity in the 'must-do' list of the global agenda, Br J Sports Med, doi:10.1136/bjsports-2020-103509
Sturm, Cohen, Free time and physical activity among Americans 15 years or older: cross-sectional analysis of the American time use survey, Prev Chronic Dis, doi:10.5888/pcd16.190017
Young, Coleman, Ngor, Associations between physical activity and cardiometabolic risk factors assessed in a southern California health care system, 2010-2012, Prev Chronic Dis, doi:10.5888/pcd11.140196
Young, Cradock, Eyler, Creating built environments that expand active transportation and active living across the United States: a policy statement from the American heart association, Circulation, doi:10.1161/CIR.0000000000000878
Zhao, Veeranki, Magnussen, Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study, BMJ, doi:10.1136/bmj.m2031
DOI record:
{
"DOI": "10.1136/bjsports-2021-104080",
"ISSN": [
"0306-3674",
"1473-0480"
],
"URL": "http://dx.doi.org/10.1136/bjsports-2021-104080",
"abstract": "<jats:sec><jats:title>Objectives</jats:title><jats:p>To compare hospitalisation rates, intensive care unit (ICU) admissions and mortality for patients with COVID-19 who were consistently inactive, doing some activity or consistently meeting physical activity guidelines.</jats:p></jats:sec><jats:sec><jats:title>Methods</jats:title><jats:p>We identified 48 440 adult patients with a COVID-19 diagnosis from 1 January 2020 to 21 October 2020, with at least three exercise vital sign measurements from 19 March 2018 to 18 March 2020. We linked each patient’s self-reported physical activity category (consistently inactive=0–10 min/week, some activity=11–149 min/week, consistently meeting guidelines=150+ min/week) to the risk of hospitalisation, ICU admission and death after COVID-19 diagnosis. We conducted multivariable logistic regression controlling for demographics and known risk factors to assess whether inactivity was associated with COVID-19 outcomes.</jats:p></jats:sec><jats:sec><jats:title>Results</jats:title><jats:p>Patients with COVID-19 who were consistently inactive had a greater risk of hospitalisation (OR 2.26; 95% CI 1.81 to 2.83), admission to the ICU (OR 1.73; 95% CI 1.18 to 2.55) and death (OR 2.49; 95% CI 1.33 to 4.67) due to COVID-19 than patients who were consistently meeting physical activity guidelines. Patients who were consistently inactive also had a greater risk of hospitalisation (OR 1.20; 95% CI 1.10 to 1.32), admission to the ICU (OR 1.10; 95% CI 0.93 to 1.29) and death (OR 1.32; 95% CI 1.09 to 1.60) due to COVID-19 than patients who were doing some physical activity.</jats:p></jats:sec><jats:sec><jats:title>Conclusions</jats:title><jats:p>Consistently meeting physical activity guidelines was strongly associated with a reduced risk for severe COVID-19 outcomes among infected adults. We recommend efforts to promote physical activity be prioritised by public health agencies and incorporated into routine medical care.</jats:p></jats:sec>",
"alternative-id": [
"10.1136/bjsports-2021-104080"
],
"author": [
{
"ORCID": "http://orcid.org/0000-0001-7633-7345",
"affiliation": [],
"authenticated-orcid": false,
"family": "Sallis",
"given": "Robert",
"sequence": "first"
},
{
"affiliation": [],
"family": "Young",
"given": "Deborah Rohm",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Tartof",
"given": "Sara Y",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Sallis",
"given": "James F",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Sall",
"given": "Jeevan",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Li",
"given": "Qiaowu",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Smith",
"given": "Gary N",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Cohen",
"given": "Deborah A",
"sequence": "additional"
}
],
"container-title": [
"British Journal of Sports Medicine"
],
"content-domain": {
"crossmark-restriction": true,
"domain": [
"bmj.com"
]
},
"created": {
"date-parts": [
[
2021,
4,
14
]
],
"date-time": "2021-04-14T00:00:29Z",
"timestamp": 1618358429000
},
"deposited": {
"date-parts": [
[
2022,
1,
16
]
],
"date-time": "2022-01-16T16:31:06Z",
"timestamp": 1642350666000
},
"funder": [
{
"DOI": "10.13039/100005977",
"doi-asserted-by": "publisher",
"name": "Kaiser Permanente"
}
],
"indexed": {
"date-parts": [
[
2022,
3,
30
]
],
"date-time": "2022-03-30T21:13:28Z",
"timestamp": 1648674808703
},
"is-referenced-by-count": 144,
"issn-type": [
{
"type": "print",
"value": "0306-3674"
},
{
"type": "electronic",
"value": "1473-0480"
}
],
"issue": "19",
"issued": {
"date-parts": [
[
2021,
4,
13
]
]
},
"journal-issue": {
"issue": "19",
"published-online": {
"date-parts": [
[
2021,
9,
16
]
]
},
"published-print": {
"date-parts": [
[
2021,
10
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://bmj.com/coronavirus/usage",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
4,
13
]
],
"date-time": "2021-04-13T00:00:00Z",
"timestamp": 1618272000000
}
}
],
"link": [
{
"URL": "https://syndication.highwire.org/content/doi/10.1136/bjsports-2021-104080",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "239",
"original-title": [],
"page": "1099-1105",
"prefix": "10.1136",
"published": {
"date-parts": [
[
2021,
4,
13
]
]
},
"published-online": {
"date-parts": [
[
2021,
4,
13
]
]
},
"published-print": {
"date-parts": [
[
2021,
10
]
]
},
"publisher": "BMJ",
"reference": [
{
"key": "2022011608300960000_55.19.1099.1",
"unstructured": "Centers for Disease Control and Prevention . COVID-19 people of any age with underlying medical conditions. Available: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html [Accessed 20 Dec 2020]."
},
{
"key": "2022011608300960000_55.19.1099.2",
"unstructured": "Centers for Disease Control and Prevention . About chronic diseases. Available: https://www.cdc.gov/chronicdisease/about/index.htm [Accessed 20 Dec 2020]."
},
{
"DOI": "10.1001/jama.2018.14854",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.3"
},
{
"key": "2022011608300960000_55.19.1099.4",
"unstructured": "World Health Organization . World Health organization 2020 guidelines on physical activity and sedentary behavior, 2020. Available: https://bjsm.bmj.com/content/54/24/1451"
},
{
"DOI": "10.1136/bjsports-2020-102955",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.5"
},
{
"DOI": "10.1136/bjsports-2020-103509",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.6"
},
{
"DOI": "10.1016/j.jshs.2018.09.009",
"article-title": "The compelling link between physical activity and the body's defense system",
"author": "Nieman",
"doi-asserted-by": "crossref",
"first-page": "201",
"journal-title": "J Sport Health Sci",
"key": "2022011608300960000_55.19.1099.7",
"volume": "8",
"year": "2019"
},
{
"DOI": "10.1007/s10238-020-00650-3",
"article-title": "Physical exercise as a tool to help the immune system against COVID-19: an integrative review of the current literature",
"author": "da Silveira",
"doi-asserted-by": "crossref",
"first-page": "1",
"journal-title": "Clin Exp Med",
"key": "2022011608300960000_55.19.1099.8",
"volume": "21",
"year": "2021"
},
{
"DOI": "10.1136/bjsports-2020-103572",
"doi-asserted-by": "crossref",
"key": "2022011608300960000_55.19.1099.9",
"unstructured": "Burtscher J , Millet GP , Burtscher M . Low cardiorespiratory and mitochondrial fitness as risk factors in viral infections: implications for COVID-19. British Journal of sports medicine (Published Online First: 24 November 2020)."
},
{
"DOI": "10.1016/j.jshs.2020.05.005",
"article-title": "An international physical activity and public health research agenda to inform coronavirus disease-2019 policies and practices",
"author": "Sallis",
"doi-asserted-by": "crossref",
"first-page": "328",
"journal-title": "J Sport Health Sci",
"key": "2022011608300960000_55.19.1099.10",
"volume": "9",
"year": "2020"
},
{
"DOI": "10.1371/journal.pmed.1003346",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.11"
},
{
"key": "2022011608300960000_55.19.1099.12",
"unstructured": "Honey-Roses J , Anguelovski I , Bohigas J . The impact of COVID-19 on public space: a review of the emerging questions."
},
{
"DOI": "10.1016/S2214-109X(18)30357-7",
"article-title": "Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants",
"author": "Guthold",
"doi-asserted-by": "crossref",
"first-page": "e1077",
"journal-title": "Lancet Glob Health",
"key": "2022011608300960000_55.19.1099.13",
"volume": "6",
"year": "2018"
},
{
"DOI": "10.3390/nu12061583",
"article-title": "Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey",
"author": "Ammar",
"doi-asserted-by": "crossref",
"journal-title": "Nutrients",
"key": "2022011608300960000_55.19.1099.14",
"volume": "12",
"year": "2020"
},
{
"DOI": "10.1371/journal.pone.0237695",
"article-title": "Perceived change in physical activity levels and mental health during COVID-19: findings among adult twin pairs",
"author": "Duncan",
"doi-asserted-by": "crossref",
"journal-title": "PLoS One",
"key": "2022011608300960000_55.19.1099.15",
"volume": "15",
"year": "2020"
},
{
"DOI": "10.3390/ijerph17186469",
"doi-asserted-by": "crossref",
"key": "2022011608300960000_55.19.1099.16",
"unstructured": "Meyer J , McDowell C , Lansing J , et al . Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 us adults. Int J Environ Res Public Health 2020;17:6469. doi:10.3390/ijerph17186469"
},
{
"DOI": "10.7812/TPP/12-031",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.17"
},
{
"DOI": "10.1249/MSS.0b013e3182630ec1",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.18"
},
{
"DOI": "10.5888/pcd11.140196",
"article-title": "Associations between physical activity and cardiometabolic risk factors assessed in a southern California health care system, 2010-2012",
"author": "Young",
"doi-asserted-by": "crossref",
"journal-title": "Prev Chronic Dis",
"key": "2022011608300960000_55.19.1099.19",
"volume": "11",
"year": "2014"
},
{
"DOI": "10.3389/fpubh.2020.575091",
"article-title": "Behavioral change towards reduced intensity physical activity is disproportionately prevalent among adults with serious health issues or Self-Perception of high risk during the UK COVID-19 Lockdown",
"author": "Rogers",
"doi-asserted-by": "crossref",
"first-page": "575091",
"journal-title": "Front Public Health",
"key": "2022011608300960000_55.19.1099.20",
"volume": "8",
"year": "2020"
},
{
"DOI": "10.5888/pcd16.190017",
"article-title": "Free time and physical activity among Americans 15 years or older: cross-sectional analysis of the American time use survey",
"author": "Sturm",
"doi-asserted-by": "crossref",
"journal-title": "Prev Chronic Dis",
"key": "2022011608300960000_55.19.1099.21",
"volume": "16",
"year": "2019"
},
{
"DOI": "10.1161/CIRCULATIONAHA.110.969022",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.22"
},
{
"DOI": "10.1161/CIR.0000000000000878",
"article-title": "Creating built environments that expand active transportation and active living across the United States: a policy statement from the American heart association",
"author": "Young",
"doi-asserted-by": "crossref",
"first-page": "e167",
"journal-title": "Circulation",
"key": "2022011608300960000_55.19.1099.23",
"volume": "142",
"year": "2020"
},
{
"key": "2022011608300960000_55.19.1099.24",
"unstructured": "Ref Kuntz J , Young DR , Saelens BE . Validity of the exercise vital sign tool to assess physical activity. Am J Prev Med."
},
{
"DOI": "10.1111/sms.12581",
"article-title": "Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases",
"author": "Pedersen",
"doi-asserted-by": "crossref",
"first-page": "1",
"journal-title": "Scand J Med Sci Sports",
"key": "2022011608300960000_55.19.1099.25",
"volume": "25 Suppl 3",
"year": "2015"
},
{
"DOI": "10.1161/CIR.0000000000000461",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.26"
},
{
"DOI": "10.1136/bmj.m2031",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.27"
},
{
"article-title": "Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries",
"author": "Katzmarzyk",
"journal-title": "Br J Sports Med",
"key": "2022011608300960000_55.19.1099.28",
"year": "2021"
},
{
"DOI": "10.1136/bmj.i1981",
"doi-asserted-by": "publisher",
"key": "2022011608300960000_55.19.1099.29"
}
],
"reference-count": 29,
"references-count": 29,
"relation": {},
"resource": {
"primary": {
"URL": "https://bjsm.bmj.com/lookup/doi/10.1136/bjsports-2021-104080"
}
},
"score": 1,
"short-container-title": [
"Br J Sports Med"
],
"short-title": [],
"source": "Crossref",
"subject": [
"Physical Therapy, Sports Therapy and Rehabilitation",
"Orthopedics and Sports Medicine",
"General Medicine"
],
"subtitle": [],
"title": [
"Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: a study in 48 440 adult patients"
],
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1136/crossmarkpolicy",
"volume": "55"
}