Hemorrhagic Fever with Renal Syndrome: Treatment with Recombinant Interferon
et al., Journal of Infectious Diseases, doi:10.1093/infdis/155.5.1047, May 1987
{kind=link}
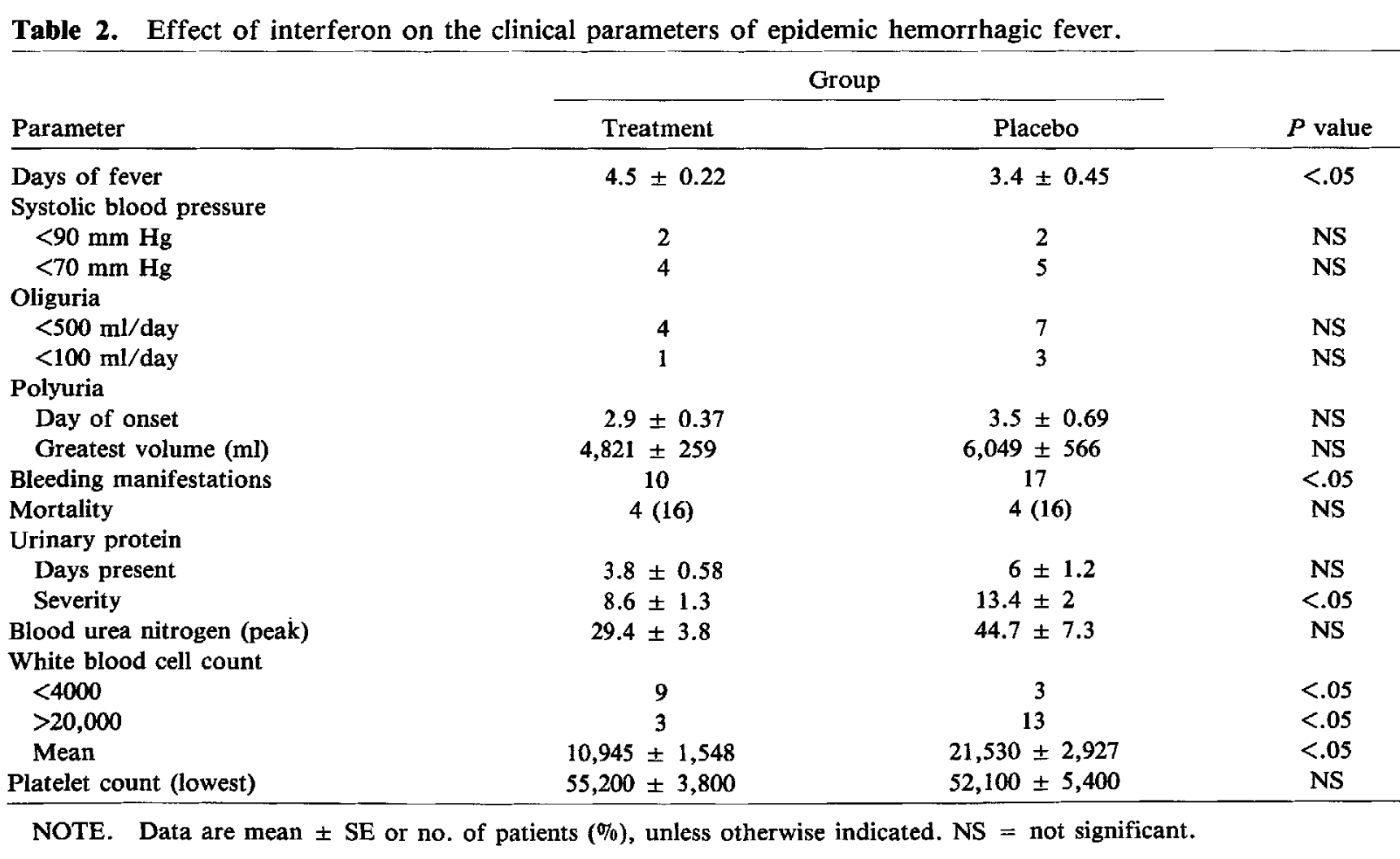
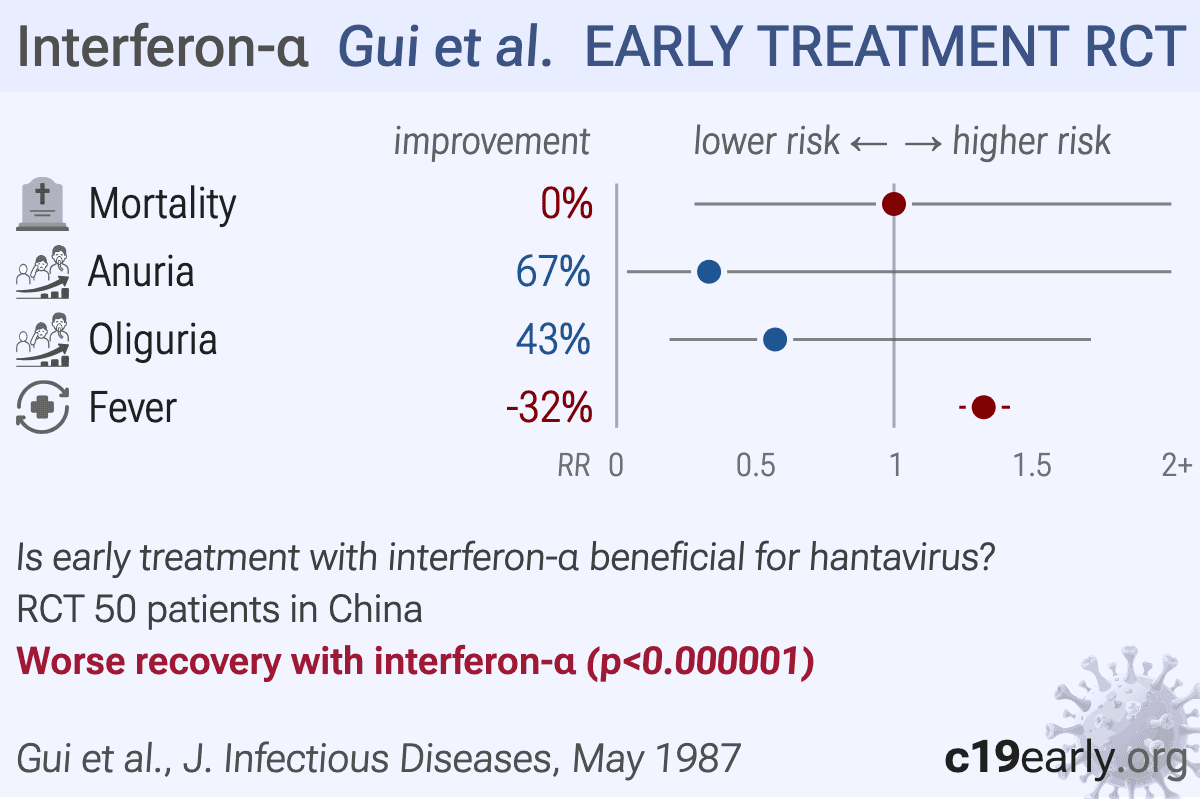
RCT 50 hospitalized patients with hemorrhagic fever with renal syndrome (HFRS) showing no significant benefit with recombinant alpha-2 interferon treatment. Mortality was identical in both groups (16% each, 4 deaths per group). The interferon group showed significantly fewer serious bleeding manifestations (10 vs. 17 patients) and less severe proteinuria, but no significant differences in hypotension, oliguria, polyuria, uremia, or thrombocytopenia. Authors hypothesize that the lack of significant therapeutic effect may be because all patients already had high antibody levels on admission, suggesting that treatment may have been too late. They suggest earlier treatment or different dosing might show greater effectiveness.
|
risk of death, no change, RR 1.00, p = 1.00, treatment 4 of 25 (16.0%), control 4 of 25 (16.0%).
|
|
anuria, 66.7% lower, RR 0.33, p = 0.61, treatment 1 of 25 (4.0%), control 3 of 25 (12.0%), NNT 13.
|
|
oliguria, 42.9% lower, RR 0.57, p = 0.50, treatment 4 of 25 (16.0%), control 7 of 25 (28.0%), NNT 8.3.
|
|
fever, 32.4% higher, RR 1.32, p < 0.001, treatment mean 4.5 (±0.22) n=25, control mean 3.4 (±0.45) n=25.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Gui et al., 1 May 1987, Randomized Controlled Trial, placebo-controlled, China, peer-reviewed, 6 authors, HFRS, Hantann.
Interferon-α (IFNa) is a recombinant type I interferon cytokine with antiviral and immunomodulatory activity, administered subcutaneously, intramuscularly, or by nebulization, that induces interferon-stimulated genes to inhibit viral replication and modulate the host innate immune response.
Abstract: 8. Kaul TN, Welliver RC, Ogra PL. Comparison of fluorescent antibody, neutralizing-antibody, and complement enhanced neutralizing-antibody assays for detection of se rum antibody to respiratory syncytial virus. J Clin Microbiol 1981;13:957-62
9. Powers CN, Peavy DL, Knight V.Selectiveinhibition of func tionallymphocyte subpopulations by ribavirin. Antimicrob Agents Chemother 1982;22:108-14
10. Connor JD, Hintz M, Van Dyke R, McCormick JB, Mcin tosh K. Ribavirin pharmacokinetics in children and adults during therapeutic trials. In: Smith RA, Knight V, Smith JAD, eds. Clinical applications of ribavirin. Orlando, Fla: Academic Press 1984:107-23
12. McIntosh K, McQuillin J, Gardner PS. Cell-free and cell bound antibody in nasal secretions from infants with re spiratory syncytial virus infections. Infect Immun 1979;23:276-81
13. Kaul TN, WelliverRC, Wong Dr, Udwadia RA, Riddlesberger K, Ogra PL. Secretory antibody response to respiratory syncytial virus infection. Am J Dis Child 1981;135:1013-6
14. Hemming VG,Prince GA, Horswood RL, London WT, Mur phy BR, Walsh EE, Fischer GW, Weisman LE, Baron PA, Chanock RM. Studies of passive immunotherapy for in fections of respiratory syncytial virus in the respiratory tract of a primate model. J Infect Dis 1985;152:1083-7
11. McIntosh K, Masters HB, Orr I, Chao RK, Barkin RM. The immunologic response to infection with respiratory syn cytial virus in infants. J Infect Dis 1978;138:24-32
15. Henderson FW, Collier A, Clyde WA Jr, Denny RW. Respiratory-syncytial-virus infections, reinfections and im munity. A prospective, longitudinal study in children. N Engl J Med 1979;300:530-4
THE JOURNAL OF INFECTIOUS DISEASES · VOL. 155, NO.5. MAY 1987 © 1987 by The University of Chicago. All rights reserved. 0022-1899/87/5505-0030$01.00
Hemorrhagic Fever with Renal Syndrome: Treatment with Recombinant a Interferon
Epidemic hemorrhagic fever with renal syndrome (HFRS) [1], also called Far Eastern hemorrhagic fever and Korean hemorrhagic fever, is caused by a member ofthe bunyavi rus group called Hantaan virus [2]. This virus (or related viruses) has been found in rodents in many parts of the world, including the United States, areas of the Eurasian landmass, and most provinces in China. The frequency ofinfection and morbidity varies geographically.In Hubei Province, where morbidity rates are the highest in China [3], the disease is primarily rural and occurs in the fall and winter months. Patients complain of headache, back ache, orbital pain, nausea, and vomiting. The febrilephase lasts two to 15 days. During or shortly after this phase, patients typically develop hypotension, oliguria, uremia, and polyuria, and they typically have a late recovery. Leu kocytosis, lymphocytosis, and atypical lymphocytosismay be noted. The mortality rate in Hubei is t'\JllOJo [4].
The antiviral properties of interferon have been known since its discovery in 1957 [5]. Its broad antiviral spectrum and relative lack of toxicity make it an attractive antiviral agent. Since 1980 [6], adequate amounts ofinterferon have
Received for publication 18 August 1986, and in revised form 15 October 1986.
Wethank Schering Plough Corporation for supplying the in terferon and supporting the study, Drs. George French and John W.Huggins for providing the methods and materials for the IgG and IgM antibody tests, and Dr. Nina Singh for reviewing the paper.
Please address requests for reprints to Dr. Monto Ho, A427 Crabtree Hall,..
DOI record:
{
"DOI": "10.1093/infdis/155.5.1047",
"ISSN": [
"0022-1899",
"1537-6613"
],
"URL": "http://dx.doi.org/10.1093/infdis/155.5.1047",
"author": [
{
"affiliation": [],
"family": "Gui",
"given": "X.-E.",
"sequence": "first"
},
{
"affiliation": [],
"family": "Ho",
"given": "M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Cohen",
"given": "M. S.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Wang",
"given": "Q.-L.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Huang",
"given": "H.-P.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Xie",
"given": "Q.-X.",
"sequence": "additional"
}
],
"container-title": "Journal of Infectious Diseases",
"container-title-short": "Journal of Infectious Diseases",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2011,
3,
18
]
],
"date-time": "2011-03-18T17:57:06Z",
"timestamp": 1300471026000
},
"deposited": {
"date-parts": [
[
2017,
8,
23
]
],
"date-time": "2017-08-23T16:42:05Z",
"timestamp": 1503506525000
},
"indexed": {
"date-parts": [
[
2025,
9,
24
]
],
"date-time": "2025-09-24T08:57:22Z",
"timestamp": 1758704242996
},
"is-referenced-by-count": 14,
"issue": "5",
"issued": {
"date-parts": [
[
1987,
5,
1
]
]
},
"journal-issue": {
"issue": "5",
"published-print": {
"date-parts": [
[
1987,
5,
1
]
]
}
},
"language": "en",
"link": [
{
"URL": "http://academic.oup.com/jid/article-pdf/155/5/1047/2377806/155-5-1047.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "286",
"original-title": [],
"page": "1047-1051",
"prefix": "10.1093",
"published": {
"date-parts": [
[
1987,
5,
1
]
]
},
"published-print": {
"date-parts": [
[
1987,
5,
1
]
]
},
"publisher": "Oxford University Press (OUP)",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "https://academic.oup.com/jid/article-lookup/doi/10.1093/infdis/155.5.1047"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [],
"subtitle": [],
"title": "Hemorrhagic Fever with Renal Syndrome: Treatment with Recombinant Interferon",
"type": "journal-article",
"volume": "155"
}