No association of low-dose aspirin with severe COVID-19 in France: A cohort of 31.1 million people without cardiovascular disease
et al., Research and Practice in Thrombosis and Haemostasis, doi:10.1002/rth2.12743, Jun 2022
{kind=link}
Retrospective 31 million people without cardiovascular disease in France, showing no significant difference in hospitalization or combined intubation/death with low dose aspirin prophylaxis.
|
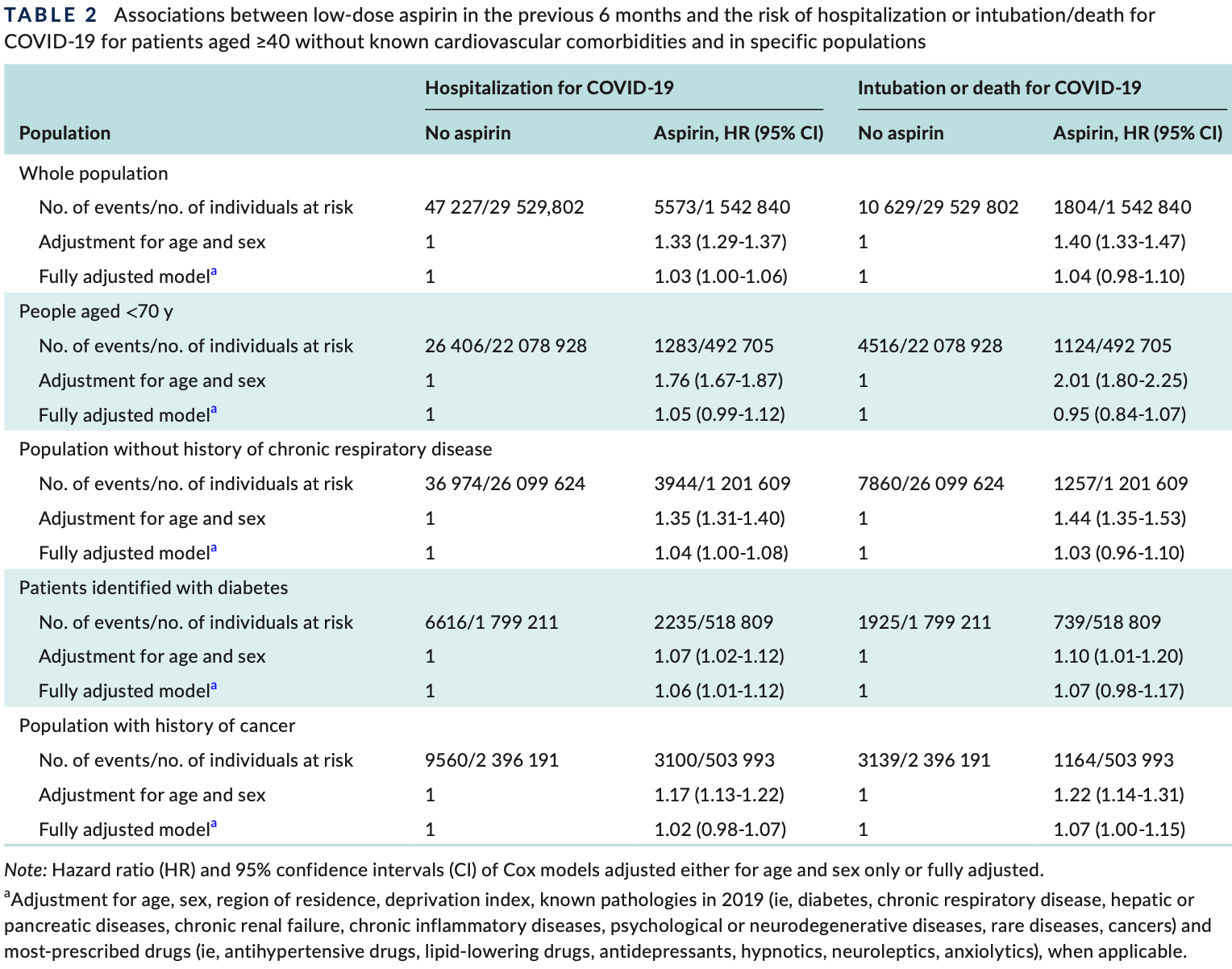
risk of death/intubation, 4.0% higher, HR 1.04, p = 0.18, Cox proportional hazards.
|
|
risk of hospitalization, 3.0% higher, HR 1.03, p = 0.046, Cox proportional hazards.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Botton et al., 17 Jun 2022, retrospective, France, peer-reviewed, 7 authors.
Contact: jeremie.botton@ansm.sante.fr.
{kind=link}
No association of low‐dose aspirin with severe COVID‐19 in France: A cohort of 31.1 million people without cardiovascular disease
Research and Practice in Thrombosis and Haemostasis, doi:10.1002/rth2.12743
Background: Aspirin at low doses has been reported to be a potential drug candidate to treat or prevent severe coronavirus disease 2019 (COVID-19).
Objectives: We aimed to explore whether low-dose aspirin used for primary cardiovascular prevention was associated with a lower risk of severe COVID-19. Method: A large cohort of patients without known cardiovascular comorbidities was constructed from the entire French population registered in national health care databases. In total, 31.1 million patients aged ≥40 years, including 1.5 million reimbursed for low-dose aspirin at least at three time points during the 6 months before the epidemic, were followed until hospitalization with a COVID-19 diagnosis or intubation/ death for hospitalized patients. Results: Cox models adjusted for age and sex showed a positive association between low-dose aspirin and the risk of hospitalization (hazard ratio [HR], 1.33; 95% confidence interval (CI), 1.29-1.37]) or death/intubation (HR, 1.40 [95% CI, 1.33-1.47]). In fully adjusted models, associations were close to null (HR, 1.03 [95% CI, 1.00-1.06] and 1.04 [95% CI, 0.98-1.10], respectively).
Conclusion: There was no evidence for an effect of low-dose aspirin for primary cardiovascular prevention in reducing severe COVID-19.
AUTH O R CO NTR I B UTI O N S JB and LS contributed equally to this work, performing the analyses and preparing the first draft. JD and OSL suggested this study and provided the hypotheses. RDS, AW, and MZ supervised the work, especially the design of the study and the statistical analyses. All the authors read the manuscript, made comments, suggested modifications, and approved the final version.
R EL ATI O N S H I P D I SCLOS U R E The authors declare no conflicts of interest.
O RCI D
Jérémie Botton https://orcid.
References
Abani, Abbas, Abbas, Aspirin in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial, Lancet, doi:10.1016/S0140-6736(21)01825-0
Aly, Ibrahim, Should aspirin be used for prophylaxis of COVID-19-induced coagulopathy?, Med Hypotheses
Arnett, Blumenthal, Albert, ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, Circulation, doi:10.1161/CIR.0000000000000677
Botton, Semenzato, Dupouy, No association of low-dose aspirin with severe COVID-19 in France: A cohort of 31.1 million people without cardiovascular disease, Res Pract Thromb Haemost
Chow, Khanna, Kethireddy, Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019, Anesth Analg
Chow, Rahnavard, Gomberg-Maitland, Association of early aspirin use with in-hospital mortality in patients with moderate COVID-19, JAMA Netw Open
Franklin, Lin, Gatto, Rassen, Glynn et al., Real-world evidence for assessing pharmaceutical treatments in the context of COVID-19, Clin Pharmacol Ther, doi:10.1002/cpt.2185
Griffith, Morris, Tudball, Collider bias undermines our understanding of COVID-19 disease risk and severity, Nat Commun, doi:10.1038/s41467-020-19478-2
Kow, Ramachandram, Hasan, Use of aspirin for primary prevention in patients with diabetes during the COVID-19 pandemic, Irish J Med Sci, doi:10.1007/s11845-021-02787-w
Liu, Huang, Li, Effect of low-dose aspirin on mortality and viral duration of the hospitalized adults with COVID-19, Medicine
Merzon, Green, Vinker, The use of aspirin for primary prevention of cardiovascular disease is associated with a lower likelihood of COVID-19 infection, FEBS J, doi:10.1111/febs.15784
Osborne, Veigulis, Arreola, Mahajan, Röösli et al., Association of mortality and aspirin prescription for COVID-19 patients at the Veterans Health Administration, PLoS One, doi:10.1371/journal.pone.0246825
Rachas, Gastaldi-Ménager, Denis, Prevalences and healthcare expenditures related to 58 health conditions from 2012 to 2017 in France: diseases and healthcare expenditure mapping, a national population-based study, doi:10.1101/2020.09.21.20198853
Russo, Maio, Attena, Clinical impact of pre-admission antithrombotic therapy in hospitalized patients with COVID-19: a multicenter observational study, Pharmacol Res, doi:10.1016/j.phrs.2020.104965
Salah, Mehta, Meta-analysis of the effect of aspirin on mortality in COVID-19, Am J Cardiol, doi:10.1016/j.amjcard.2020.12.073
Semenzato, Botton, Drouin, Hypertension antihypertensive drugs and COVID-19 risk a cohort study of 2 million hypertensive patients, Hypertension, doi:10.1161/HYPERTENSIONAHA.120.16314
Siegel, Aspirin use for primary cardiovascular prevention during the covid-19 pandemic, Am J Med, doi:10.1016/j.amjmed.2020.11.008
Wang, Ao, Nasr, Qi, Effect of antiplatelet treatments on patients with COVID-19 infection: a systematic review and meta-analysis, Am J Emerg Med, doi:10.1016/j.ajem.2021.01.016
DOI record:
{
"DOI": "10.1002/rth2.12743",
"ISSN": [
"2475-0379",
"2475-0379"
],
"URL": "http://dx.doi.org/10.1002/rth2.12743",
"alternative-id": [
"10.1002/rth2.12743"
],
"assertion": [
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Received",
"name": "received",
"order": 0,
"value": "2021-07-04"
},
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Accepted",
"name": "accepted",
"order": 1,
"value": "2022-04-20"
},
{
"group": {
"label": "Publication History",
"name": "publication_history"
},
"label": "Published",
"name": "published",
"order": 2,
"value": "2022-06-17"
}
],
"author": [
{
"ORCID": "http://orcid.org/0000-0002-4814-6370",
"affiliation": [
{
"name": "EPI‐PHARE Scientific Interest Group in Epidemiology of Health Products French National Agency for the Safety of Medicines and Health Products French National Health Insurance Saint‐Denis France"
}
],
"authenticated-orcid": false,
"family": "Botton",
"given": "Jérémie",
"sequence": "first"
},
{
"ORCID": "http://orcid.org/0000-0002-8305-3487",
"affiliation": [
{
"name": "EPI‐PHARE Scientific Interest Group in Epidemiology of Health Products French National Agency for the Safety of Medicines and Health Products French National Health Insurance Saint‐Denis France"
}
],
"authenticated-orcid": false,
"family": "Semenzato",
"given": "Laura",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-7801-286X",
"affiliation": [
{
"name": "MSPU de Pins Justaret University Paul Sabatier Toulouse III UMR 1295 Inserm Univ. Paul Sabatier F‐31000 Toulouse France"
}
],
"authenticated-orcid": false,
"family": "Dupouy",
"given": "Julie",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-7646-3667",
"affiliation": [
{
"name": "EPI‐PHARE Scientific Interest Group in Epidemiology of Health Products French National Agency for the Safety of Medicines and Health Products French National Health Insurance Saint‐Denis France"
}
],
"authenticated-orcid": false,
"family": "Dray‐Spira",
"given": "Rosemary",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-8687-9092",
"affiliation": [
{
"name": "EPI‐PHARE Scientific Interest Group in Epidemiology of Health Products French National Agency for the Safety of Medicines and Health Products French National Health Insurance Saint‐Denis France"
}
],
"authenticated-orcid": false,
"family": "Weill",
"given": "Alain",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-3731-3476",
"affiliation": [
{
"name": "University Paris‐Saclay UVSQ Univ. Paris‐Sud Inserm Primary Care and Prevention CESP Villejuif France"
}
],
"authenticated-orcid": false,
"family": "Saint‐Lary",
"given": "Olivier",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-8393-4217",
"affiliation": [
{
"name": "EPI‐PHARE Scientific Interest Group in Epidemiology of Health Products French National Agency for the Safety of Medicines and Health Products French National Health Insurance Saint‐Denis France"
},
{
"name": "University Paris‐Saclay UVSQ Univ. Paris‐Sud Inserm Primary Care and Prevention CESP Villejuif France"
}
],
"authenticated-orcid": false,
"family": "Zureik",
"given": "Mahmoud",
"sequence": "additional"
}
],
"container-title": "Research and Practice in Thrombosis and Haemostasis",
"container-title-short": "Res Pract Thromb Haemost",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"onlinelibrary.wiley.com"
]
},
"created": {
"date-parts": [
[
2022,
6,
17
]
],
"date-time": "2022-06-17T08:13:00Z",
"timestamp": 1655453580000
},
"deposited": {
"date-parts": [
[
2022,
6,
27
]
],
"date-time": "2022-06-27T10:30:50Z",
"timestamp": 1656325850000
},
"indexed": {
"date-parts": [
[
2022,
6,
27
]
],
"date-time": "2022-06-27T11:15:19Z",
"timestamp": 1656328519695
},
"is-referenced-by-count": 0,
"issue": "4",
"issued": {
"date-parts": [
[
2022,
5
]
]
},
"journal-issue": {
"issue": "4",
"published-print": {
"date-parts": [
[
2022,
5
]
]
}
},
"language": "en",
"license": [
{
"URL": "http://creativecommons.org/licenses/by-nc-nd/4.0/",
"content-version": "vor",
"delay-in-days": 47,
"start": {
"date-parts": [
[
2022,
6,
17
]
],
"date-time": "2022-06-17T00:00:00Z",
"timestamp": 1655424000000
}
},
{
"URL": "http://doi.wiley.com/10.1002/tdm_license_1.1",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2022,
5,
1
]
],
"date-time": "2022-05-01T00:00:00Z",
"timestamp": 1651363200000
}
}
],
"link": [
{
"URL": "https://onlinelibrary.wiley.com/doi/pdf/10.1002/rth2.12743",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://onlinelibrary.wiley.com/doi/full-xml/10.1002/rth2.12743",
"content-type": "application/xml",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://onlinelibrary.wiley.com/doi/pdf/10.1002/rth2.12743",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "311",
"original-title": [],
"prefix": "10.1002",
"published": {
"date-parts": [
[
2022,
5
]
]
},
"published-online": {
"date-parts": [
[
2022,
6,
17
]
]
},
"published-print": {
"date-parts": [
[
2022,
5
]
]
},
"publisher": "Wiley",
"reference": [
{
"DOI": "10.1016/j.mehy.2020.109975",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_2_1"
},
{
"DOI": "10.1213/ANE.0000000000005292",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_3_1"
},
{
"DOI": "10.1016/j.phrs.2020.104965",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_4_1"
},
{
"DOI": "10.1016/j.amjmed.2020.11.008",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_5_1"
},
{
"DOI": "10.1016/S0140‐6736(21)01825‐0",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_6_1"
},
{
"DOI": "10.1111/febs.15784",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_7_1"
},
{
"DOI": "10.1097/MD.0000000000024544",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_8_1"
},
{
"DOI": "10.1371/journal.pone.0246825",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_9_1"
},
{
"DOI": "10.1001/jamanetworkopen.2022.3890",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_10_1"
},
{
"DOI": "10.1016/j.amjcard.2020.12.073",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_11_1"
},
{
"DOI": "10.1016/j.ajem.2021.01.016",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_12_1"
},
{
"DOI": "10.1161/HYPERTENSIONAHA.120.16314",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_13_1"
},
{
"DOI": "10.1101/2020.09.21.20198853",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_14_1"
},
{
"DOI": "10.1161/CIR.0000000000000677",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_15_1"
},
{
"DOI": "10.1007/s11845‐021‐02787‐w",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_16_1"
},
{
"DOI": "10.1002/cpt.2185",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_17_1"
},
{
"DOI": "10.1038/s41467‐020‐19478‐2",
"doi-asserted-by": "publisher",
"key": "e_1_2_7_18_1"
}
],
"reference-count": 17,
"references-count": 17,
"relation": {},
"resource": {
"primary": {
"URL": "https://onlinelibrary.wiley.com/doi/10.1002/rth2.12743"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Hematology"
],
"subtitle": [],
"title": "No association of low‐dose aspirin with severe COVID‐19 in France: A cohort of 31.1 million people without cardiovascular disease",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1002/crossmark_policy",
"volume": "6"
}