
Real-world Effectiveness of Sotrovimab for COVID-19: Evidence from United States (US) Administrative Claims Data
et al., Open Forum Infectious Diseases, doi:10.1093/ofid/ofad500.579, Nov 2023
Sotrovimab for COVID-19
45th treatment shown to reduce risk in
August 2022, now with p = 0.00048 from 29 studies, recognized in 42 countries.
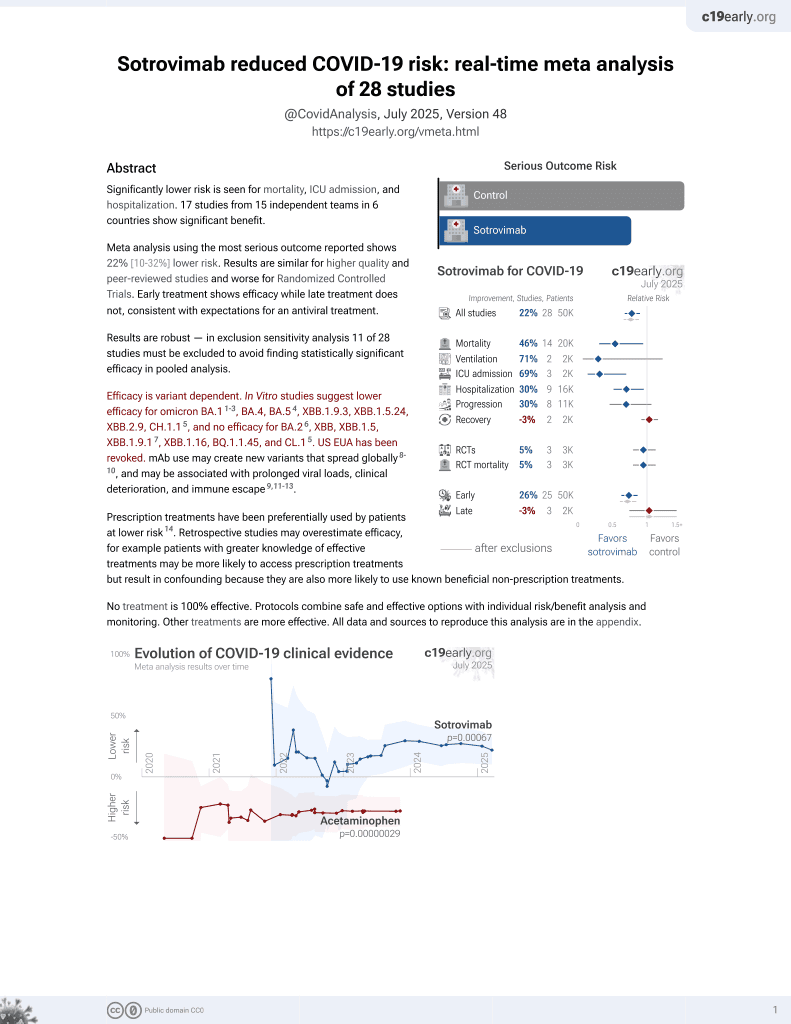
Efficacy is variant dependent.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
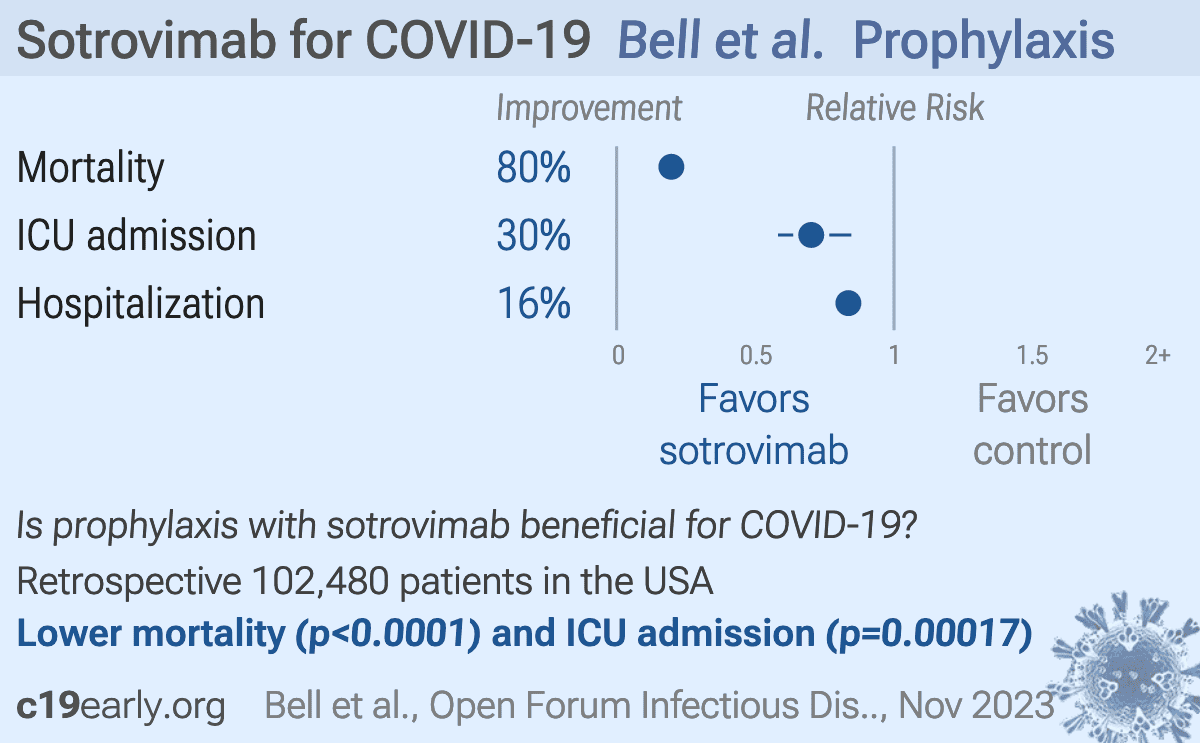
Retrospective 34,160 COVID-19 patients in the USA treated with sotrovimab matched to 68,320 untreated patients from May 2021-April 2022, during periods when Delta and early Omicron were predominant. Sotrovimab-treated patients had significantly lower rates of hospitalization, mortality, ICU admission, and need for respiratory support compared to matched untreated patients.
Authors exclude patients using antivirals in the control group but not the treatment group.
Confounding by treatment propensity. This study analyzes a population
where only a fraction of eligible patients received the treatment. Patients
receiving treatment may be more likely to follow other recommendations, more
likely to receive additional care, and more likely to use additional
treatments that are not tracked in the data (e.g., nasal/oral hygiene1,2, vitamin D3, etc.) — either because the physician
recommending sotrovimab also recommended them, or
because the patient seeking out sotrovimab is more
likely to be familiar with the efficacy of additional treatments and more
likely to take the time to use them.
Therefore, these kind of studies may
overestimate efficacy.
Efficacy is variant dependent. In Vitro studies predict lower efficacy for BA.14-6, BA.4, BA.57, XBB.1.9.3, XBB.1.5.24, XBB.2.9, CH.1.18, and no efficacy for BA.29, XBB, XBB.1.5, ХВВ.1.9.110, XBB.1.16, BQ.1.1.45, and CL.18. US EUA has been revoked.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments11.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
risk of death, 80.3% lower, RR 0.20, p < 0.001, treatment 52 of 34,160 (0.2%), control 527 of 68,320 (0.8%), NNT 162.
|
|
risk of ICU admission, 29.8% lower, RR 0.70, p < 0.001, treatment 147 of 34,160 (0.4%), control 419 of 68,320 (0.6%), NNT 547.
|
|
risk of hospitalization, 16.4% lower, RR 0.84, p < 0.001, treatment 1,350 of 34,160 (4.0%), control 3,231 of 68,320 (4.7%), NNT 129.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
4.
Liu et al., Striking Antibody Evasion Manifested by the Omicron Variant of SARS-CoV-2, bioRxiv, doi:10.1101/2021.12.14.472719.
5.
Sheward et al., Variable loss of antibody potency against SARS-CoV-2 B.1.1.529 (Omicron), bioRxiv, doi:10.1101/2021.12.19.473354.
6.
VanBlargan et al., An infectious SARS-CoV-2 B.1.1.529 Omicron virus escapes neutralization by several therapeutic monoclonal antibodies, bioRxiv, doi:10.1101/2021.12.15.472828.
7.
Haars et al., Prevalence of SARS-CoV-2 Omicron Sublineages and Spike Protein Mutations Conferring Resistance against Monoclonal Antibodies in a Swedish Cohort during 2022–2023, Microorganisms, doi:10.3390/microorganisms11102417.
8.
Pochtovyi et al., In Vitro Efficacy of Antivirals and Monoclonal Antibodies against SARS-CoV-2 Omicron Lineages XBB.1.9.1, XBB.1.9.3, XBB.1.5, XBB.1.16, XBB.2.4, BQ.1.1.45, CH.1.1, and CL.1, Vaccines, doi:10.3390/vaccines11101533.
9.
Zhou et al., SARS-CoV-2 Omicron BA.2 Variant Evades Neutralization by Therapeutic Monoclonal Antibodies, bioRxiv, doi:10.1101/2022.02.15.480166.
Bell et al., 27 Nov 2023, retrospective, USA, peer-reviewed, 6 authors.
{kind=link}
Real-world Effectiveness of Sotrovimab for COVID-19: Evidence from United States (US) Administrative Claims Data
Background. This study compared outcomes among COVID-19 patients (pts) treated with the monoclonal antibody (mAb) sotrovimab matched to untreated pts. Methods. Administrative claims (Komodo Health) were used to identify pts (≥ 12 years) diagnosed with COVID-19 (ICD-10: U0.7.1) in an ambulatory setting in the US (26 May 2021-5 April 2022). The sotrovimab cohort included pts meeting sotrovimab's Emergency Use Authorization (EUA) criteria and receiving sotrovimab ≤ 10 days from diagnosis (index date = day of infusion). The untreated cohort included pts with no evidence of early/prophylaxis mAb or antiviral treatments (index date imputed based on the time distribution between diagnosis and sotrovimab infusion for their matched counterpart from the sotrovimab cohort). Pts were required to be continuously enrolled for ≥ 12 months pre-index and ≥ 29 days post-index (excluding death). Exact matching and propensity-score matching (EM/PSM) methods were used to construct 1:2 matched cohorts of sotrovimab-treated and untreated patients (EM; age [≤ 5 years], diagnosis date [≤ 14 days], state: PSM; gender, payor, region,
DOI record:
{
"DOI": "10.1093/ofid/ofad500.579",
"ISSN": [
"2328-8957"
],
"URL": "http://dx.doi.org/10.1093/ofid/ofad500.579",
"abstract": "<jats:title>Abstract</jats:title>\n <jats:sec>\n <jats:title>Background</jats:title>\n <jats:p>This study compared outcomes among COVID-19 patients (pts) treated with the monoclonal antibody (mAb) sotrovimab matched to untreated pts.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Methods</jats:title>\n <jats:p>Administrative claims (Komodo Health) were used to identify pts (≥ 12 years) diagnosed with COVID-19 (ICD-10: U0.7.1) in an ambulatory setting in the US (26 May 2021–5 April 2022). The sotrovimab cohort included pts meeting sotrovimab’s Emergency Use Authorization (EUA) criteria and receiving sotrovimab ≤ 10 days from diagnosis (index date = day of infusion). The untreated cohort included pts with no evidence of early/prophylaxis mAb or antiviral treatments (index date imputed based on the time distribution between diagnosis and sotrovimab infusion for their matched counterpart from the sotrovimab cohort). Pts were required to be continuously enrolled for ≥ 12 months pre-index and ≥ 29 days post-index (excluding death). Exact matching and propensity-score matching (EM/PSM) methods were used to construct 1:2 matched cohorts of sotrovimab-treated and untreated patients (EM; age [≤ 5 years], diagnosis date [≤ 14 days], state: PSM; gender, payor, region, Quan-Charlson score, EUA criteria, index date, baseline healthcare utilization). Outcomes evaluated in the 29-day post-index period were all-cause hospitalization, all-cause hospitalization and/or mortality, all-cause mortality, intensive care unit (ICU) admission, and maximum level of respiratory support.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Results</jats:title>\n <jats:p>A total of 34,160 sotrovimab pts were matched to 68,320 untreated pts (characteristics well balanced: 54 years of age, approximately 40% male, 42% had commercial payor, and approximately 50% indexed in January 2022). The 29-day hospitalization and/or mortality rates were 4.0% (n=1,380 / 34,160) and 5.2% (n=3,566 / 68,320) in the sotrovimab and untreated cohorts, respectively (p &lt; 0.0001). Patients in the sotrovimab cohort had statistically significantly lower rates of all-cause hospitalization, all-cause mortality, ICU admission, and respiratory support as compared with patients in the untreated cohort (Table).</jats:p>\n <jats:p>*Obtained from conditional logistic regression models (binary outcomes). All models adjusted for malignancy. ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Conclusion</jats:title>\n <jats:p>Sotrovimab demonstrated effectiveness in preventing severe outcomes (hospitalization, mortality and respiratory support) as compared with untreated pts during the period in which Delta and early Omicron variants were predominant.</jats:p>\n </jats:sec>\n <jats:sec>\n <jats:title>Disclosures</jats:title>\n <jats:p>Christopher F. Bell, MS, GSK: Employee|GSK: Stocks/Bonds Tasneem Lokhandwala, PhD, GSK: Funding to conduct study|Vir Biotechnology, Inc: Funding to conduct study Daniel C. Gibbons, PhD, GSK: Employee|GSK: Stocks/Bonds Myriam Drysdale, PhD, GSK: Employee|GSK: Stocks/Bonds Jane Wang, MS, GSK: Funding to conduct study|Vir Biotechnology, Inc: Funding to conduct study Emily Lloyd, MSc, GSK: Employee|GSK: Stocks/Bonds</jats:p>\n </jats:sec>",
"author": [
{
"affiliation": [
{
"name": "GlaxoSmithKline , Durham, North Carolina"
}
],
"family": "Bell",
"given": "Christopher F",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Xcenda LLC , Carrollton, Texas"
}
],
"family": "Lokhandwala",
"given": "Tasneem",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "GlaxoSmithKline plc. , Brentford, Middlesex , UK, Brentford, England, United Kingdom"
}
],
"family": "Gibbons",
"given": "Daniel C",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "GSK , Brentford, Middlesex, England , United Kingdom"
}
],
"family": "Drysdale",
"given": "Myriam",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Xcenda LLC , Carrollton, Texas"
}
],
"family": "Wang",
"given": "Jane",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "GSK , Brentford, Middlesex, England , United Kingdom"
}
],
"family": "Lloyd",
"given": "Emily",
"sequence": "additional"
}
],
"container-title": "Open Forum Infectious Diseases",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T02:22:24Z",
"timestamp": 1701051744000
},
"deposited": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T02:22:25Z",
"timestamp": 1701051745000
},
"indexed": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T05:16:36Z",
"timestamp": 1701062196607
},
"is-referenced-by-count": 0,
"issue": "Supplement_2",
"issued": {
"date-parts": [
[
2023,
11,
27
]
]
},
"journal-issue": {
"issue": "Supplement_2",
"published-print": {
"date-parts": [
[
2023,
11,
27
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://creativecommons.org/licenses/by/4.0/",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2023,
11,
27
]
],
"date-time": "2023-11-27T00:00:00Z",
"timestamp": 1701043200000
}
}
],
"link": [
{
"URL": "https://academic.oup.com/ofid/article-pdf/10/Supplement_2/ofad500.579/53777417/ofad500.579.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "syndication"
},
{
"URL": "https://academic.oup.com/ofid/article-pdf/10/Supplement_2/ofad500.579/53777417/ofad500.579.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "286",
"original-title": [],
"prefix": "10.1093",
"published": {
"date-parts": [
[
2023,
11,
27
]
]
},
"published-online": {
"date-parts": [
[
2023,
11,
27
]
]
},
"published-other": {
"date-parts": [
[
2023,
12
]
]
},
"published-print": {
"date-parts": [
[
2023,
11,
27
]
]
},
"publisher": "Oxford University Press (OUP)",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "https://academic.oup.com/ofid/article/doi/10.1093/ofid/ofad500.579/7448428"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Infectious Diseases",
"Oncology"
],
"subtitle": [],
"title": "510. Real-world Effectiveness of Sotrovimab for COVID-19: Evidence from United States (US) Administrative Claims Data",
"type": "journal-article",
"volume": "10"
}