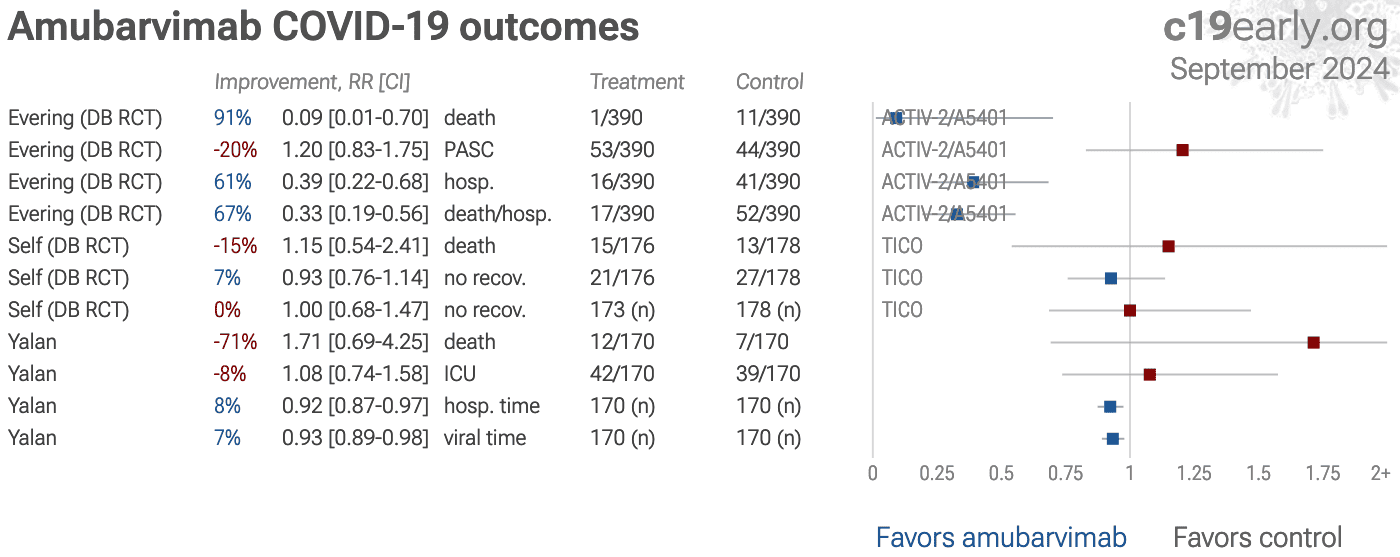
4 amubarvimab COVID-19 controlled studies, 2 RCTs
Supplementary Data — Amubarvimab/romlusevimab for COVID-19: real-time meta-analysis of 4 studies
0
0.25
0.5
0.75
1
1.25
1.5
1.75
2+ ACTIV-2/A5401 Evering (DB RCT) 91% 0.09 [0.01-0.70] death 1/390 11/390 Improvement, RR [CI] Treatment Control ACTIV-2/A5401 Evering (DB RCT) -20% 1.20 [0.83-1.75] PASC 53/390 44/390 ACTIV-2/A5401 Evering (DB RCT) 61% 0.39 [0.22-0.68] hosp. 16/390 41/390 ACTIV-2/A5401 Evering (DB RCT) 67% 0.33 [0.19-0.56] death/hosp. 17/390 52/390 ACTIV-3/TICO Self (DB RCT) -15% 1.15 [0.54-2.41] death 15/176 13/178 ACTIV-3/TICO Self (DB RCT) 7% 0.93 [0.76-1.14] no recov. 21/176 27/178 ACTIV-3/TICO Self (DB RCT) 0% 1.00 [0.68-1.47] no recov. 173 (n) 178 (n) Yalan -71% 1.71 [0.69-4.25] death 12/170 7/170 Yalan -8% 1.08 [0.74-1.58] ICU 42/170 39/170 Yalan 8% 0.92 [0.87-0.97] hosp. time 170 (n) 170 (n) Yalan 7% 0.93 [0.89-0.98] viral time 170 (n) 170 (n) Qu (ICU) 46% 0.54 [0.29-1.04] death 47 (n) 47 (n) ICU patients Qu (ICU) 4% 0.96 [0.57-1.64] viral+ 47 (n) 47 (n) ICU patients Amubarvimab COVID-19 outcomes c19 early .org July 2026 Favors amubarvimab Favors control
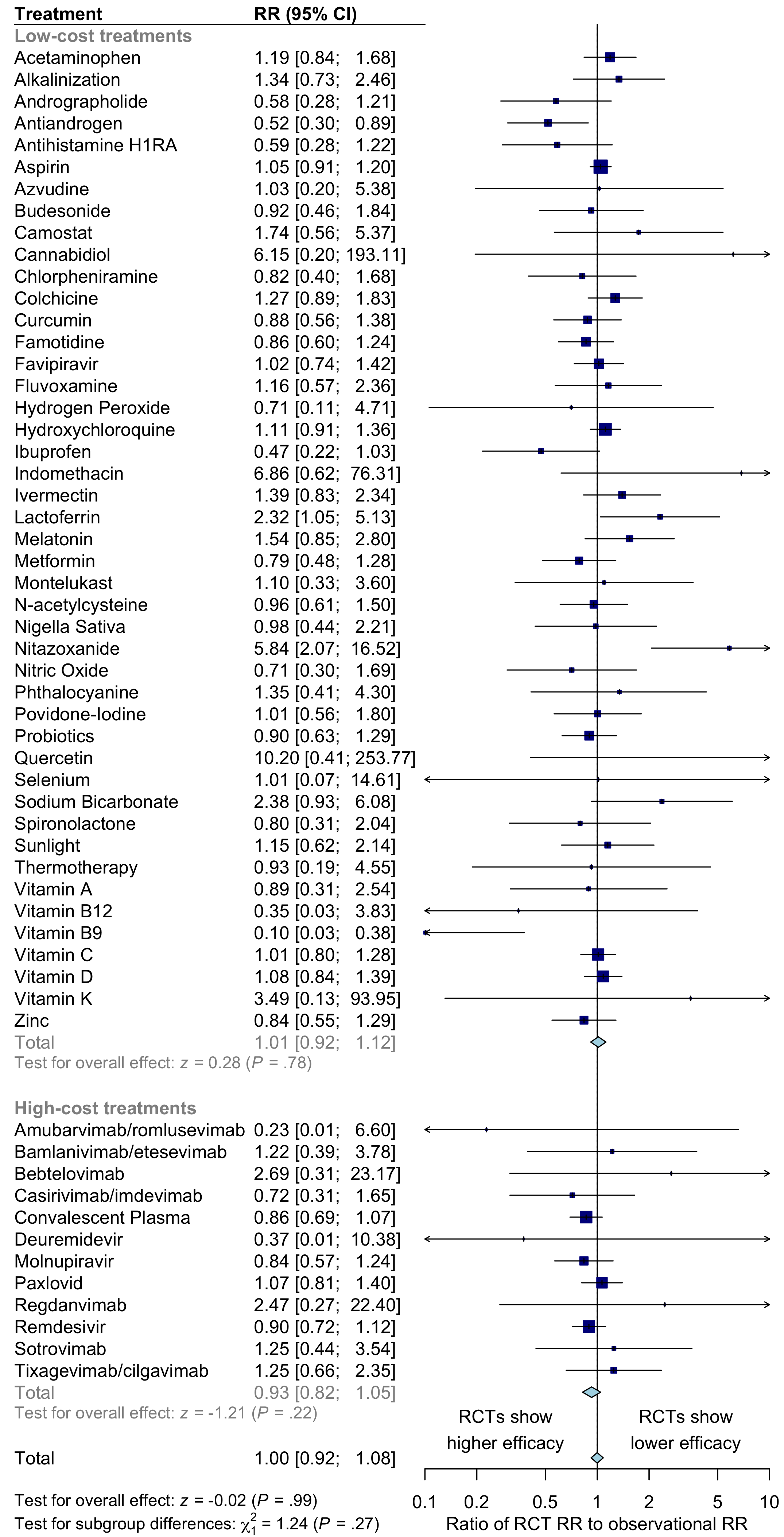
Fig. S2. Comparison of results for RCTs versus observational studies.
For COVID-19 treatments, there is no significant difference between the results of RCTs and observational studies. Observational studies do not systematically over or underestimate efficacy. For high-cost treatments, there is a non-significant trend towards RCTs showing greater efficacy.
Please send us corrections, updates, or comments.
c19early involves the extraction of 200,000+ datapoints from
thousands of papers.
Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation.
IMA and
WCH
provide treatment protocols.
Submit
{kind=link}
{kind=link}