The Minimal Effect of Zinc on the Survival of Hospitalized Patients With COVID-19
et al., Chest, doi:10.1016/j.chest.2020.06.082, Jul 2020
Zinc for COVID-19
2nd treatment shown to reduce risk in
July 2020, now with p = 0.00000012 from 41 studies, recognized in 23 countries.
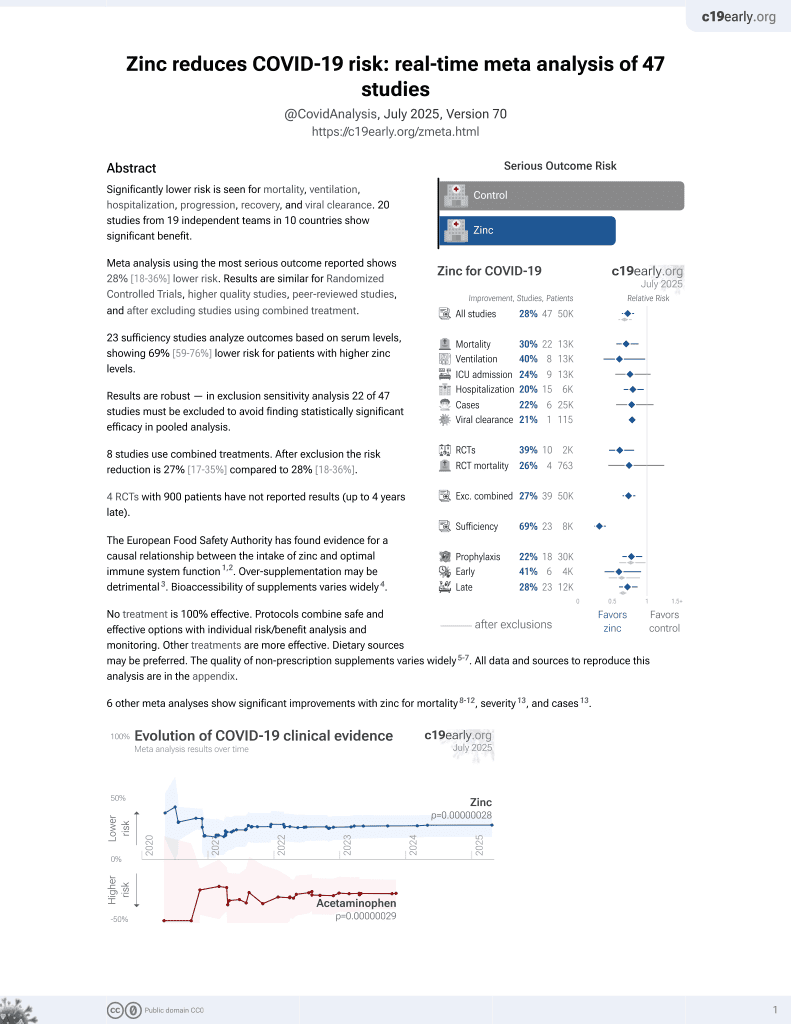
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
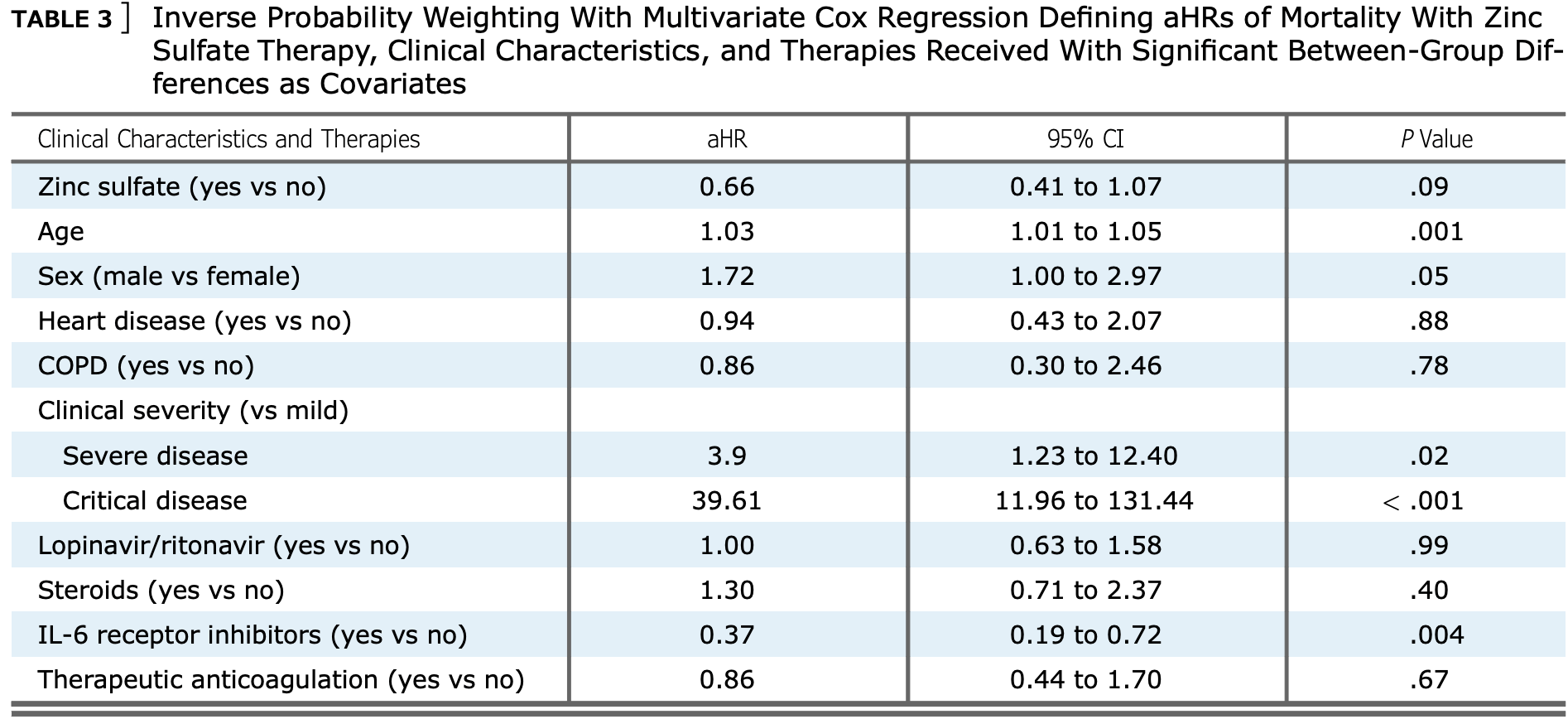
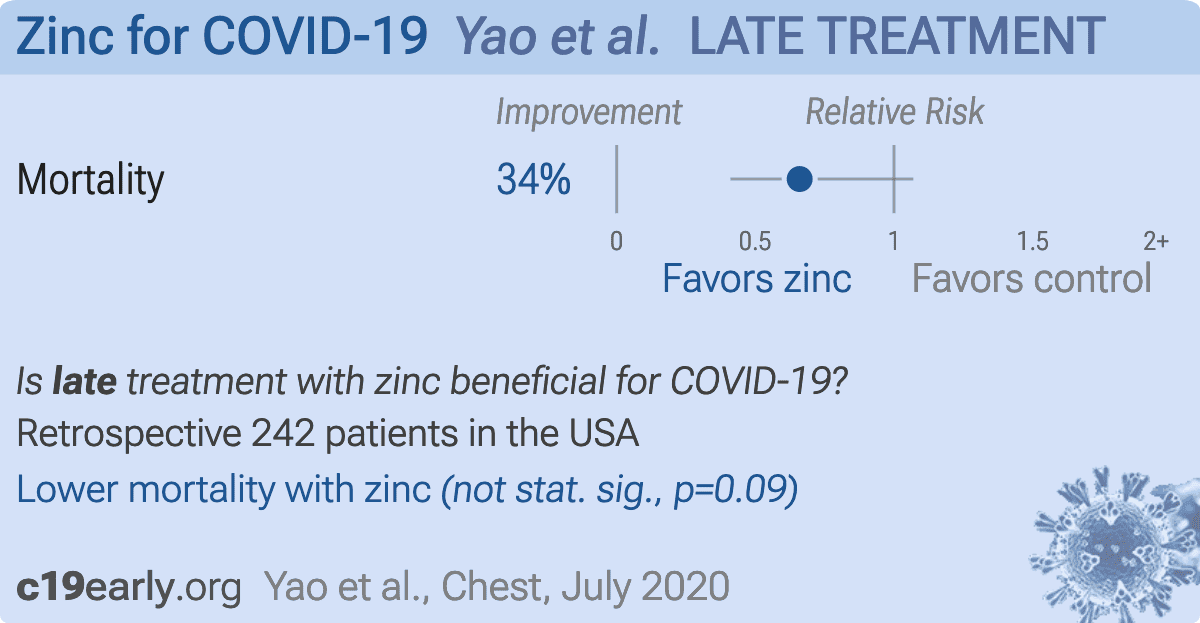
Retrospective 242 hospitalized patients in the USA showing adjusted hazard ratio for zinc treatment, aHR 0.66 [0.41-1.07].1 notes that the study would be more informative if baseline serum zinc levels were known.
Although the 34% lower mortality is not statistically significant, it is consistent with the significant 35% lower mortality [17‑49%] from meta-analysis of the 18 mortality results to date.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments2.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
This may explain in part the very high mortality seen in this study.
Results may differ in countries with improved SOC.
|
risk of death, 34.0% lower, RR 0.66, p = 0.09, treatment 73 of 196 (37.2%), control 21 of 46 (45.7%), adjusted per study, multivariate Cox regression.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Yao et al., 22 Jul 2020, retrospective, USA, peer-reviewed, 9 authors.
{kind=link}
Abstract: [
Chest Infections Research Letter
]
The Minimal Effect of Zinc on
the Survival of Hospitalized
Patients With COVID-19
An Observational Study
To the Editor:
Zinc is an investigational agent against coronavirus
disease 2019 (COVID-19) and has known preventative
and therapeutic roles in other infections.1-3 Zinc
deficiency is associated with lower survival among older
patients with pneumonia and predisposes to other viral
infections.3 Established risk factors for critical COVID-19,
including older age, diabetes mellitus, and cardiovascular
disease, are also associated with zinc deficiency.2
The antiviral and immunomodulatory effects of zinc
have made it a candidate against severe acute respiratory
Methods
In this single-institution retrospective study, we assessed the survival of
hospitalized patients with COVID-19 treated with vs without zinc
sulfate. This study was conducted in accordance with the amended
Declaration of Helsinki. This study’s protocol was approved and was
granted a waiver of informed consent by the hospital board on April
15, 2020, based on its retrospective design and the lack of identifying
information to be published, collected, or analyzed.
Data of all patients with COVID-19 (N ¼ 242) admitted at the Hoboken
University Medical Center until April 11, 2020, were retrospectively
collected on April 21, 2020. COVID-19 was confirmed in all patients
using quantitative real-time reverse transcription polymerase chain
reaction for SARS-CoV-2 RNA. Clinical severity was stratified based
on World Health Organization8 guidelines according to clinical,
radiographic, and laboratory information from the first 24 h of
admission. The primary outcome was days from admission to inhospital mortality. Data for patients who did not meet the primary
outcome were censored on April 21, 2020.
Our primary analysis explored the causal association between zinc therapy
and the survival of hospitalized patients with COVID-19. Inverse
probability weighting (IPW) and a censorship model derived an effect
estimate of zinc therapy on survival using the parameter defined as the
Results
Of 242 patients, 81.0% received zinc sulfate at a total
daily dose of 440 mg (100 mg elemental zinc). The
median age of patients who received zinc was 65 years
(interquartile range, 53-77), whereas that of the control
108 Research Letter
syndrome-coronavirus-2 (SARS-CoV-2) infection.2-4
Zinc may decrease the activity of the angiotensin
converting enzyme 2, the receptor for SARS-CoV-2.
Zinc T-cell modulation may downregulate the cytokine
storm associated with severe COVID-19.2,4 These
properties underlie the speculated efficacy of
chloroquine, a zinc ionophore, and the derivative
hydroxychloroquine, which are investigational agents
in the worldwide World Health Organization
SOLIDARITY trial.2,5,6 Furthermore, chloroquine may
increase cellular zinc uptake, suggesting therapeutic
benefit from the combination of the two agents.4
Despite zinc’s low risk of adverse effects, zinc’s role
in the management of COVID-19 must be
supported by clinical data.7 Therefore, we
investigated the role of zinc among hospitalized
patients with COVID-19.
average treatment effect on the treated (ATET). The lack of sufficient
overlap or the positive probability of assignment to each treatment level
precluded the estimation of the average treatment effect.
Multivariable logistic regression modeled the propensity to receive zinc
by assigning weights to established predictors of mortality and..
DOI record:
{
"DOI": "10.1016/j.chest.2020.06.082",
"ISSN": [
"0012-3692"
],
"URL": "http://dx.doi.org/10.1016/j.chest.2020.06.082",
"alternative-id": [
"S0012369220319619"
],
"assertion": [
{
"label": "This article is maintained by",
"name": "publisher",
"value": "Elsevier"
},
{
"label": "Article Title",
"name": "articletitle",
"value": "The Minimal Effect of Zinc on the Survival of Hospitalized Patients With COVID-19"
},
{
"label": "Journal Title",
"name": "journaltitle",
"value": "Chest"
},
{
"label": "CrossRef DOI link to publisher maintained version",
"name": "articlelink",
"value": "https://doi.org/10.1016/j.chest.2020.06.082"
},
{
"label": "Content Type",
"name": "content_type",
"value": "article"
},
{
"label": "Copyright",
"name": "copyright",
"value": "© 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved."
}
],
"author": [
{
"affiliation": [],
"family": "Yao",
"given": "Jasper Seth",
"sequence": "first"
},
{
"affiliation": [],
"family": "Paguio",
"given": "Joseph Alexander",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Dee",
"given": "Edward Christopher",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Tan",
"given": "Hanna Clementine",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Moulick",
"given": "Achintya",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Milazzo",
"given": "Carmelo",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Jurado",
"given": "Jerry",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Della Penna",
"given": "Nicolás",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Celi",
"given": "Leo Anthony",
"sequence": "additional"
}
],
"container-title": "Chest",
"container-title-short": "Chest",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"clinicalkey.fr",
"clinicalkey.jp",
"clinicalkey.com.au",
"clinicalkey.es",
"clinicalkey.com",
"journal.chestnet.org",
"elsevier.com",
"sciencedirect.com"
]
},
"created": {
"date-parts": [
[
2020,
7,
22
]
],
"date-time": "2020-07-22T15:16:06Z",
"timestamp": 1595430966000
},
"deposited": {
"date-parts": [
[
2022,
7,
12
]
],
"date-time": "2022-07-12T00:30:29Z",
"timestamp": 1657585829000
},
"indexed": {
"date-parts": [
[
2024,
3,
31
]
],
"date-time": "2024-03-31T18:57:47Z",
"timestamp": 1711911467002
},
"is-referenced-by-count": 61,
"issue": "1",
"issued": {
"date-parts": [
[
2021,
1
]
]
},
"journal-issue": {
"issue": "1",
"published-print": {
"date-parts": [
[
2021,
1
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://www.elsevier.com/tdm/userlicense/1.0/",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
1,
1
]
],
"date-time": "2021-01-01T00:00:00Z",
"timestamp": 1609459200000
}
},
{
"URL": "http://www.elsevier.com/open-access/userlicense/1.0/",
"content-version": "am",
"delay-in-days": 370,
"start": {
"date-parts": [
[
2022,
1,
6
]
],
"date-time": "2022-01-06T00:00:00Z",
"timestamp": 1641427200000
}
}
],
"link": [
{
"URL": "https://api.elsevier.com/content/article/PII:S0012369220319619?httpAccept=text/xml",
"content-type": "text/xml",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://api.elsevier.com/content/article/PII:S0012369220319619?httpAccept=text/plain",
"content-type": "text/plain",
"content-version": "vor",
"intended-application": "text-mining"
}
],
"member": "78",
"original-title": [],
"page": "108-111",
"prefix": "10.1016",
"published": {
"date-parts": [
[
2021,
1
]
]
},
"published-print": {
"date-parts": [
[
2021,
1
]
]
},
"publisher": "Elsevier BV",
"reference": [
{
"article-title": "Zinc and respiratory tract infections: perspectives for COVID-19 (review)",
"author": "Skalny",
"first-page": "17",
"issue": "1",
"journal-title": "Int J Mol Med",
"key": "10.1016/j.chest.2020.06.082_bib2",
"volume": "46",
"year": "2020"
},
{
"DOI": "10.1016/j.dsx.2020.04.015",
"article-title": "Enhancing immunity in viral infections, with special emphasis on COVID-19: a review",
"author": "Jayawardena",
"doi-asserted-by": "crossref",
"first-page": "367",
"issue": "4",
"journal-title": "Diabetes Metab Syndr Clin Res Rev",
"key": "10.1016/j.chest.2020.06.082_bib3",
"volume": "14",
"year": "2020"
},
{
"DOI": "10.1007/s12011-020-02194-9",
"doi-asserted-by": "crossref",
"key": "10.1016/j.chest.2020.06.082_bib4",
"unstructured": "Rahman MT, Idid SZ. Can Zn be a critical element in COVID-19 treatment [published online ahead of print May 26, 2020]? Biol Trace Elem Res. https://doi.org/10.1007/s12011-020-02194-9"
},
{
"article-title": "Zinc: An essential micronutrient",
"author": "Saper",
"first-page": "768",
"issue": "9",
"journal-title": "Am Fam Physician",
"key": "10.1016/j.chest.2020.06.082_bib7",
"volume": "79",
"year": "2009"
},
{
"author": "Diaz",
"key": "10.1016/j.chest.2020.06.082_bib8"
},
{
"DOI": "10.1001/jama.2020.6775",
"article-title": "Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area",
"author": "Richardson",
"doi-asserted-by": "crossref",
"first-page": "2052",
"issue": "20",
"journal-title": "JAMA",
"key": "10.1016/j.chest.2020.06.082_bib9",
"volume": "323",
"year": "2020"
},
{
"DOI": "10.1513/AnnalsATS.201808-564PS",
"article-title": "Control of confounding and reporting of results in causal inference studies",
"author": "Lederer",
"doi-asserted-by": "crossref",
"first-page": "22",
"issue": "1",
"journal-title": "Ann Am Thorac Soc",
"key": "10.1016/j.chest.2020.06.082_bib10",
"volume": "16",
"year": "2019"
}
],
"reference-count": 7,
"references-count": 7,
"relation": {},
"resource": {
"primary": {
"URL": "https://linkinghub.elsevier.com/retrieve/pii/S0012369220319619"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"Cardiology and Cardiovascular Medicine",
"Critical Care and Intensive Care Medicine",
"Pulmonary and Respiratory Medicine"
],
"subtitle": [],
"title": "The Minimal Effect of Zinc on the Survival of Hospitalized Patients With COVID-19",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1016/elsevier_cm_policy",
"volume": "159"
}
Late treatment
is less effective
is less effective
