Aspirin is associated with lower risks of severe covid-19 disease: a population-based study
et al., Heart, doi:10.1136/heartjnl-2023-BCS.211, Jun 2023
{kind=link}
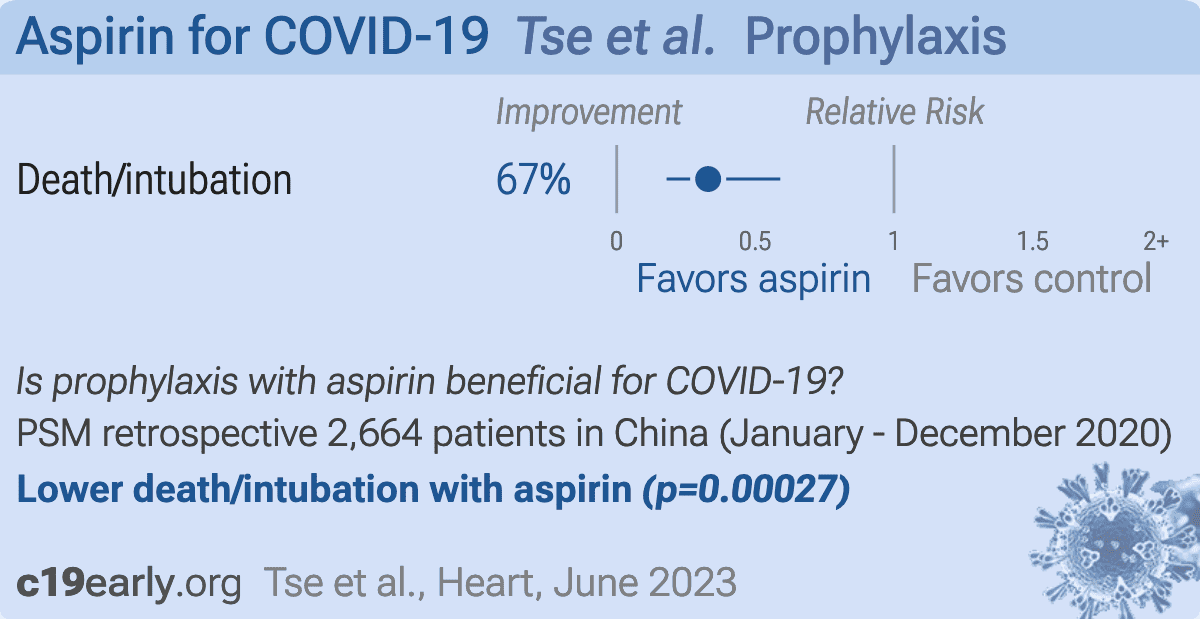
PSM retrospective 2,664 COVID-19 hospitalized patients receiving steroids/antiviral therapy in Hong Kong, showing lower risk of combined death/intubation with aspirin use.
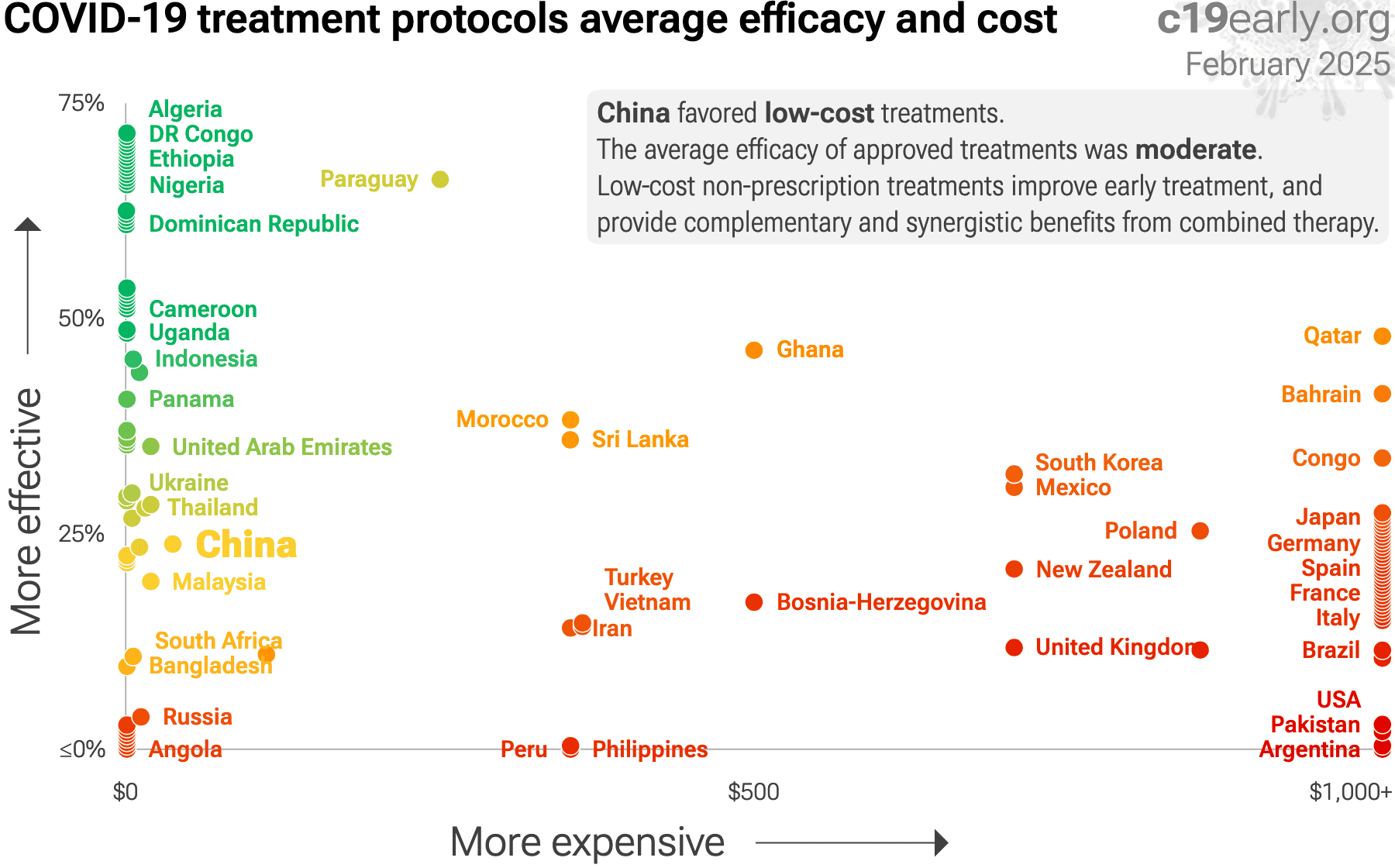
Standard of Care (SOC) for COVID-19 in the study country,
China, is poor with low average efficacy for approved treatments1.
|
risk of death/intubation, 67.0% lower, OR 0.33, p < 0.001, adjusted per study, propensity score matching, multivariable, day 30, RR approximated with OR.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Tse et al., 2 Jun 2023, retrospective, China, peer-reviewed, 12 authors, study period 1 January, 2020 - 8 December, 2020.
{kind=link}
Abstract: Abstracts
210
Emmanouela Kampouraki.
10.1136/heartjnl-2023-BCS.210
Introduction It is estimated that statin non-adherence reaches
50% in patients with hyperlipidaemia. Factors related to the
healthcare system, among others, play an important role in
statin non-adherence. We designed and tested a modified version of the MYMEDS© tool (1), called The My Experience
of Taking Statin Medicines (mySTATINmed) online questionnaire, which examined the presence of modifiable barriers to
adherence to support patients on statins. The impact of consultation experience with healthcare professionals on the display of potential or actual barriers to adherence was extracted
from the questionnaire.
Methods The mySTATINmed questionnaire explored patient
perspectives on the main modifiable factors that are likely to
be associated with statin non-adherence, including the consultation experience with healthcare professionals and the level
of information received during consultations. Information
included the mechanism of action of statins, their expected
benefit, treatment duration, expected side effects, management
of side effects and lifestyle changes needed. The quality of
consultation experience and the level of information received
during consultation were analysed in relation to the display of
potential or actual barriers to adherence. Chi-squared test was
used to compare the frequencies.
Results The mySTATINmed questionnaire was responded by
466 patients [59% males; age mean±SD (range): 65±11 (2186) years] across 29 GP Practices in Leeds. Based on
responses in four questionnaire domains (shown in Table 1),
the level of display of potential or actual barriers to adherence was scored. Based on this score, patients were then
dichotomised between adherent (54%) and non-adherent
(46%).
Overall, the mySTATINmed detected that 46% of participants displayed some level of actual or potential barriers to
statin adherence based on their responses. A greater proportion of patients in the adherent versus the non-adherent group
rated their consultation experience highly (72% v 57% respectively; p<0.001) and reported having received enough
Abstract 210 Table 1 Core mySTATINmed domains which were
included in the display of potential or actual barriers to adherence
score. Comparison of adherent/non-adherent scores per domain
Questionnaire domain and
Non-adherent
Adherent
p-value (chi-sq
score
(%)
(%)
test)
<0.001
information during consultations (56% v 43% respectively;
p=0.003). The type and level of information shared during
consultations and the quality of consultation positively correlated with adherence (Table 1).
Conclusions The mySTATINmed is a simple tool which identified the level of display of potential or actual barriers to statin adherence, which in turn can inform a better structured,
personalised statin consultation. A good consultation experience is associated with better statin adherence.
Conflict of Interest None
211
ASPIRIN IS ASSOCIATED WITH LOWER RISKS OF SEVERE
COVID-19 DISEASE: A POPULATION-BASED STUDY
1
Gary Tse, 2Qingpeng Zhang, 3Abraham Wai, 4Emma King, 5Keith Leung, 6Sharen Lee,
Carlin Chang, 3Ian Wong, 3Bernard Cheung, 8Jiandong Zhou, 9Tong Liu, 3Hok Him Pui.
1
Hong Kong Metropolitan University; 2City University of Hong Kong; 3The University of
Hong Kong; 4Cardiovascular Analytics Group; 5Aston University / The University of Hong
Kong; 6Chinese University of Hong Kong; 7Queen Mary Hospital; 8University of Oxford;
9
Second..
DOI record:
{
"DOI": "10.1136/heartjnl-2023-bcs.211",
"URL": "http://dx.doi.org/10.1136/heartjnl-2023-BCS.211",
"alternative-id": [
"10.1136/heartjnl-2023-BCS.211"
],
"author": [
{
"affiliation": [],
"family": "Tse",
"given": "Gary",
"sequence": "first"
},
{
"affiliation": [],
"family": "Zhang",
"given": "Qingpeng",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Wai",
"given": "Abraham",
"sequence": "additional"
},
{
"affiliation": [],
"family": "King",
"given": "Emma",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Leung",
"given": "Keith",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Lee",
"given": "Sharen",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Chang",
"given": "Carlin",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Wong",
"given": "Ian",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Cheung",
"given": "Bernard",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Zhou",
"given": "Jiandong",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Liu",
"given": "Tong",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Pui",
"given": "Hok Him",
"sequence": "additional"
}
],
"container-title": "Stable IHD/Prevention/Hypertension/Lipids",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"bmj.com"
]
},
"created": {
"date-parts": [
[
2023,
7,
17
]
],
"date-time": "2023-07-17T17:00:31Z",
"timestamp": 1689613231000
},
"deposited": {
"date-parts": [
[
2023,
7,
17
]
],
"date-time": "2023-07-17T17:00:33Z",
"timestamp": 1689613233000
},
"event": "British Cardiovascular Society Annual Conference, ‘Future-proofing Cardiology for the next 10 years’, 5–7 June 2023",
"indexed": {
"date-parts": [
[
2023,
7,
18
]
],
"date-time": "2023-07-18T04:24:23Z",
"timestamp": 1689654263580
},
"is-referenced-by-count": 0,
"issued": {
"date-parts": [
[
2023,
6
]
]
},
"link": [
{
"URL": "https://syndication.highwire.org/content/doi/10.1136/heartjnl-2023-BCS.211",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "239",
"original-title": [],
"prefix": "10.1136",
"published": {
"date-parts": [
[
2023,
6
]
]
},
"published-online": {
"date-parts": [
[
2023,
6,
2
]
]
},
"published-print": {
"date-parts": [
[
2023,
6
]
]
},
"publisher": "BMJ Publishing Group Ltd and British Cardiovascular Society",
"reference-count": 0,
"references-count": 0,
"relation": {},
"resource": {
"primary": {
"URL": "https://heart.bmj.com/lookup/doi/10.1136/heartjnl-2023-BCS.211"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subtitle": [],
"title": "211 Aspirin is associated with lower risks of severe covid-19 disease: a population-based study",
"type": "proceedings-article",
"update-policy": "http://dx.doi.org/10.1136/crossmarkpolicy"
}