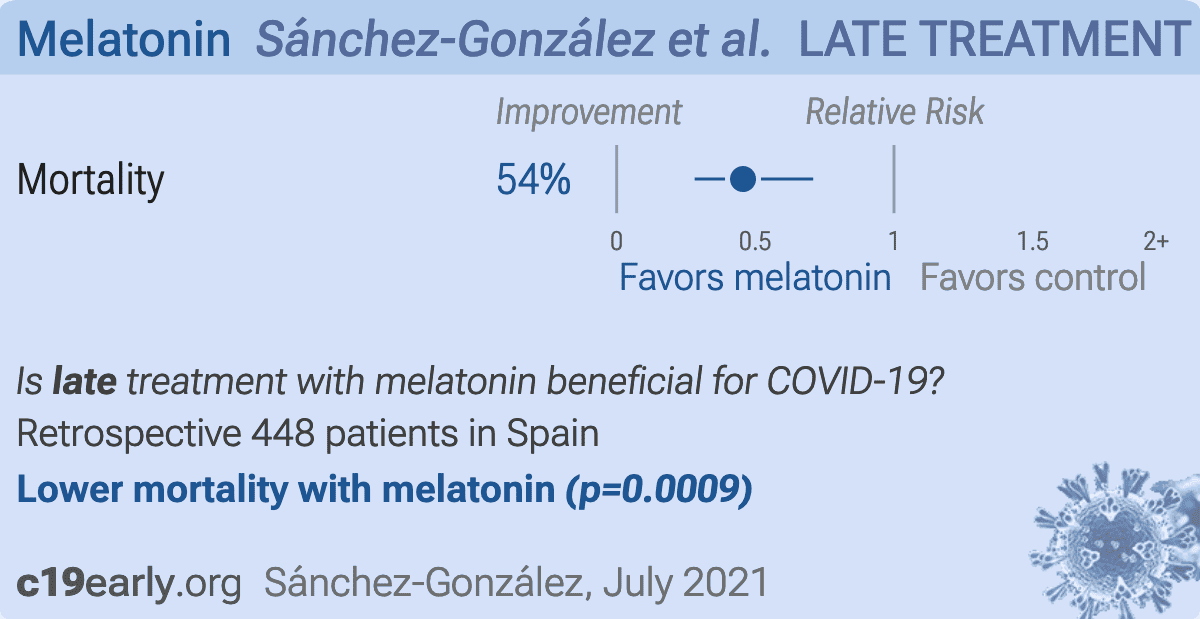
What if melatonin could help COVID-19 severe patients?
, Journal of Clinical Sleep Medicine, doi:10.5664/jcsm.9554, Jul 2021
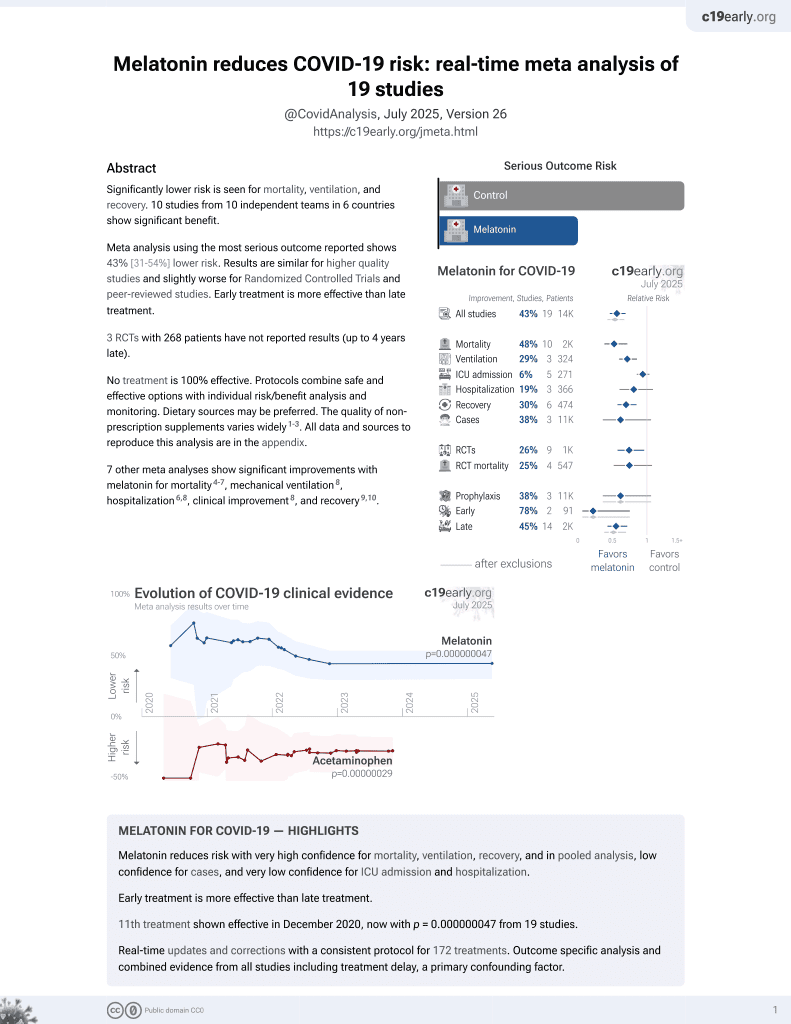
Melatonin for COVID-19
25th treatment shown to reduce risk in
May 2021, now with p = 0.000000015 from 18 studies.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
Retrospective 2,463 hospitalized patients in Spain, 265 treated with melatonin, showing lower mortality with treatment in PSM analysis, however these results are subject to immortal time bias. Authors excluded from the sample patients that died during the first 72 hours of admission without taking melatonin, and patients that started on melatonin in the last 7 days of their admittance, having completed 75% of their stay.
This study is excluded in the after exclusion results of meta-analysis:
immortal-time bias may significantly affect results.
|
risk of death, 54.4% lower, RR 0.46, p < 0.001, treatment 24 of 224 (10.7%), control 53 of 224 (23.7%), NNT 7.7, odds ratio converted to relative risk, PSM.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Sánchez-González et al., 20 Jul 2021, retrospective, Spain, peer-reviewed, 4 authors.
{kind=link}
Abstract: https://doi.org/10.5664/jcsm.9554
LETTERS TO THE EDITOR
What if melatonin could help patients with severe COVID-19?
Miguel Angel
Sanchez-Gonzalez, MD, PhD1,2; Ignacio Mahıllo-Fernandez, PhD3; Felipe Villar-Alvarez,
MD, PhD4; Lucıa Llanos, MD, PhD5
Psychiatry Department, Fundacion Jimenez Dıaz University Hospital, Health Research Institute (IIS-FJD, UAM), Madrid, Spain; 2Department of Anatomy, Histology, and
Neuroscience, School of Medicine, Universidad Autonoma de Madrid, Madrid, Spain; 3Biostatistics Unit, Fundacion Jimenez Dıaz University Hospital, Health Research Institute
(IIS-FJD, UAM), Madrid, Spain; 4Pulmonology Department, Fundacion Jimenez Dıaz University Hospital, Health Research Institute (IIS-FJD, UAM), CIBERES, Universidad
Autonoma de Madrid, Madrid, Spain; 5Clinical Research Unit, Fundacion Jimenez Dıaz University Hospital, Health Research Institute (IIS-FJD, UAM), Madrid, Spain
1
Copyright 2022 American Academy of Sleep Medicine. All rights reserved.
In March 2020, a protocol recommending the prescription of melatonin, among other sleep- and biorhythms-promoting measures, to
hospitalized patients with coronavirus disease 2019 (COVID-19)
with sleep problems or delirium was sent from the consultationliaison psychiatrist to the medical staff of the Fundaci
on Jimenez
Dıaz University Hospital (FJDUH) in Madrid, Spain. Several
authors have suggested a potential benefit of melatonin use in
COVID-19.1–4 In addition to its circadian function, melatonin is
thought to have several health-promoting properties, including
immune response modulation and anti-inflammatory and antioxidant properties.5 We here report a retrospective analysis showing
an association of melatonin with survival in a sample of 2,463
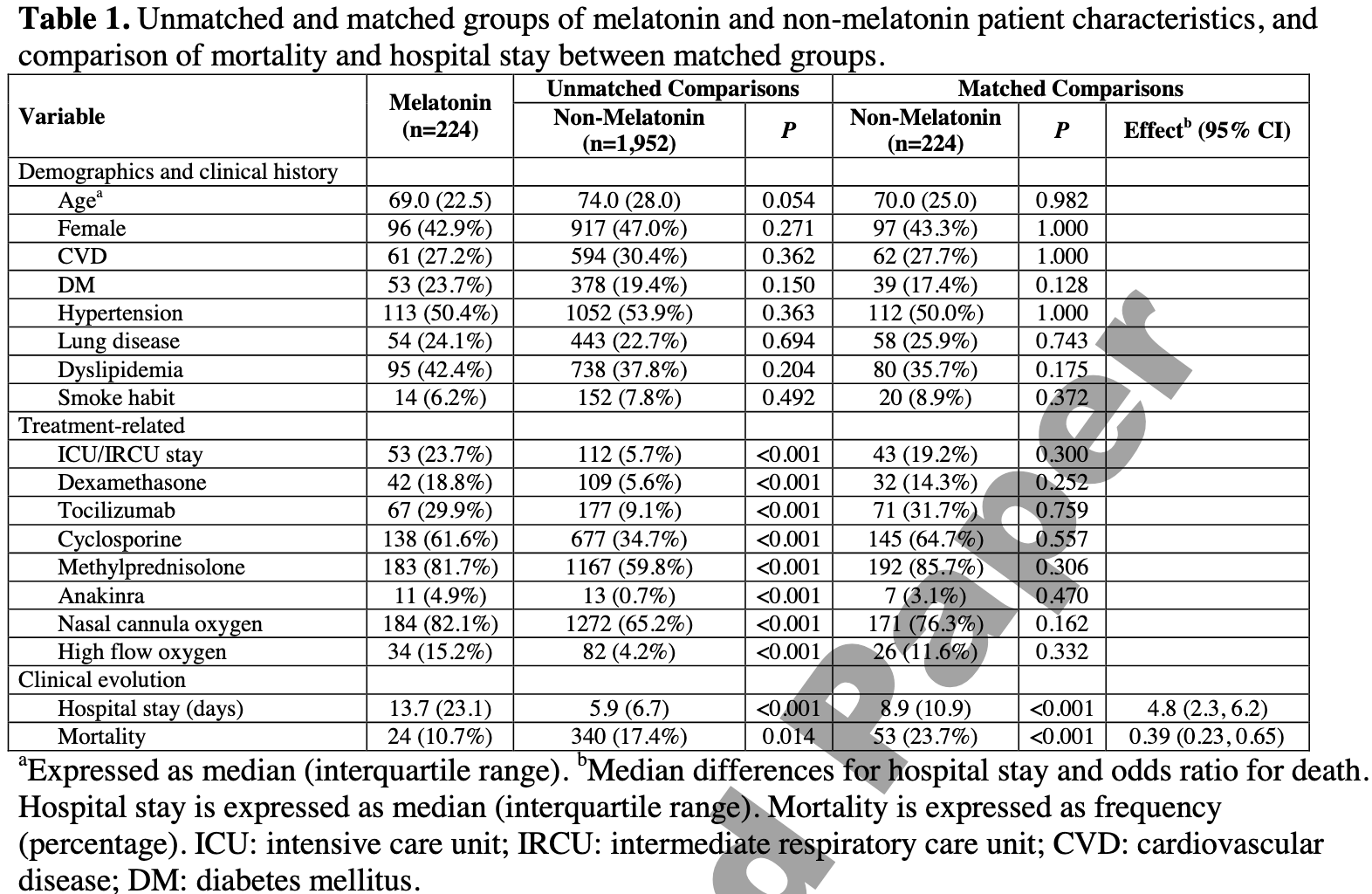
Table 1—Unmatched and matched groups of melatonin and non-melatonin patient characteristics, and comparison of mortality and
hospital stay between matched groups.
Variable
Demographics and clinical history
Agea
Female
CVD
DM
Hypertension
Lung disease
Dyslipidemia
Smoking habit
Treatment-related
ICU/IRCU stay
Dexamethasone
Tocilizumab
Cyclosporine
Methylprednisolone
Anakinra
Nasal cannula oxygen
High-flow oxygen
Clinical evolution
Hospital stay, d
Mortality
Melatonin
(n = 224)
Unmatched Comparisons
Matched Comparisons
Non-Melatonin
(n = 1,952)
P Value
Non-Melatonin
(n = 224)
P Value
Effectb (95% CI)
69.0 (22.5)
96 (42.9%)
61 (27.2%)
53 (23.7%)
113 (50.4%)
54 (24.1%)
95 (42.4%)
14 (6.2%)
74.0 (28.0)
917 (47.0%)
594 (30.4%)
378 (19.4%)
1,052 (53.9%)
443 (22.7%)
738 (37.8%)
152 (7.8%)
.054
.271
.362
.150
.363
.694
.204
.492
70.0 (25.0)
97 (43.3%)
62 (27.7%)
39 (17.4%)
112 (50.0%)
58 (25.9%)
80 (35.7%)
20 (8.9%)
.982
> .99
> .99
.128
> .99
.743
.175
.372
—
—
—
—
—
—
—
—
53 (23.7%)
42 (18.8%)
67 (29.9%)
138 (61.6%)
183 (81.7%)
11 (4.9%)
184 (82.1%)
34 (15.2%)
112 (5.7%)
109 (5.6%)
177 (9.1%)
677 (34.7%)
1,167 (59.8%)
13 (0.7%)
1,272 (65.2%)
82 (4.2%)
<.001
<.001
<.001
<.001
<.001
<.001
<.001
<.001
43 (19.2%)
32 (14.3%)
71 (31.7%)
145 (64.7%)
192 (85.7%)
7 (3.1%)
171 (76.3%)
26 (11.6%)
.300
.252
.759
.557
.306
.470
.162
.332
—
—
—
—
—
—
—
—
13.7 (23.1)
24 (10.7%)
5.9 (6.7)
340 (17.4%)
<.001
.014
8.9 (10.9)
53 (23.7%)
<.001
<.001
4.8 (2.3–6.2)
0.39 (0.23–0.65)
a
Expressed as median (interquartile range). bMedian differences for hospital stay and odds ratio..
DOI record:
{
"DOI": "10.5664/jcsm.9554",
"ISSN": [
"1550-9389",
"1550-9397"
],
"URL": "http://dx.doi.org/10.5664/jcsm.9554",
"alternative-id": [
"10.5664/jcsm.9554"
],
"author": [
{
"affiliation": [
{
"name": "Psychiatry Department, Fundación Jiménez Díaz University Hospital, Health Research Institute (IIS-FJD, UAM), Madrid, Spain;"
},
{
"name": "Department of Anatomy, Histology, and Neuroscience, School of Medicine, Universidad Autónoma de Madrid, Madrid, Spain;"
}
],
"family": "Sánchez-González",
"given": "Miguel Ángel",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Biostatistics Unit, Fundación Jiménez Díaz University Hospital, Health Research Institute (IIS-FJD, UAM), Madrid, Spain;"
}
],
"family": "Mahíllo-Fernández",
"given": "Ignacio",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Pulmonology Department, Fundación Jiménez Díaz University Hospital, Health Research Institute (IIS-FJD, UAM), CIBERES, Universidad Autónoma de Madrid, Madrid, Spain;"
}
],
"family": "Villar-Álvarez",
"given": "Felipe",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Clinical Research Unit, Fundación Jiménez Díaz University Hospital, Health Research Institute (IIS-FJD, UAM), Madrid, Spain"
}
],
"family": "Llanos",
"given": "Lucía",
"sequence": "additional"
}
],
"container-title": "Journal of Clinical Sleep Medicine",
"container-title-short": "Journal of Clinical Sleep Medicine",
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2021,
7,
20
]
],
"date-time": "2021-07-20T15:42:27Z",
"timestamp": 1626795747000
},
"deposited": {
"date-parts": [
[
2025,
12,
1
]
],
"date-time": "2025-12-01T12:32:37Z",
"timestamp": 1764592357000
},
"indexed": {
"date-parts": [
[
2025,
12,
1
]
],
"date-time": "2025-12-01T12:42:53Z",
"timestamp": 1764592973841,
"version": "3.46.0"
},
"is-referenced-by-count": 2,
"issue": "1",
"issued": {
"date-parts": [
[
2022,
1
]
]
},
"journal-issue": {
"issue": "1",
"published-print": {
"date-parts": [
[
2022,
1
]
]
}
},
"language": "en",
"member": "297",
"original-title": [],
"page": "335-336",
"prefix": "10.1007",
"published": {
"date-parts": [
[
2022,
1
]
]
},
"published-print": {
"date-parts": [
[
2022,
1
]
]
},
"publisher": "Springer Science and Business Media LLC",
"reference": [
{
"DOI": "10.1016/j.lfs.2020.117583",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_2_2"
},
{
"DOI": "10.1016/j.virusres.2020.198108",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_3_2"
},
{
"DOI": "10.1080/08830185.2020.1756284",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_4_2"
},
{
"DOI": "10.1371/journal.pone.0240149",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_5_2"
},
{
"DOI": "10.2174/1570159X14666161228122115",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_6_2"
},
{
"article-title": "Melatonin is significantly associated with survival of intubated COVID-19 patients",
"author": "Ramlall V",
"journal-title": "medRxiv.",
"key": "e_1_3_2_7_2",
"unstructured": "Ramlall V, Zucker J, Tatonetti N. Melatonin is significantly associated with survival of intubated COVID-19 patients. medRxiv. Preprint posted online October 18, 2020."
},
{
"DOI": "10.1016/j.ijid.2020.11.003",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_8_2"
},
{
"DOI": "10.1016/j.lfs.2020.117902",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_9_2"
},
{
"DOI": "10.1016/j.jcrc.2017.03.002",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_10_2"
},
{
"DOI": "10.1097/CCM.0000000000004697",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_11_2"
},
{
"DOI": "10.1111/jpi.12683",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_12_2"
},
{
"DOI": "10.1186/s13063-020-04737-w",
"doi-asserted-by": "publisher",
"key": "e_1_3_2_13_2"
}
],
"reference-count": 12,
"references-count": 12,
"relation": {},
"resource": {
"primary": {
"URL": "http://jcsm.aasm.org/doi/10.5664/jcsm.9554"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [],
"subtitle": [],
"title": "What if melatonin could help patients with severe COVID-19?",
"type": "journal-article",
"volume": "18"
}
Late treatment
is less effective
is less effective
