Exercise rehabilitation associates with lower mortality and hospitalisation in cardiovascular disease patients with COVID-19
et al., European Journal of Preventive Cardiology, doi:10.1093/eurjpc/zwaa135, Jul 2021
Exercise for COVID-19
9th treatment shown to reduce risk in
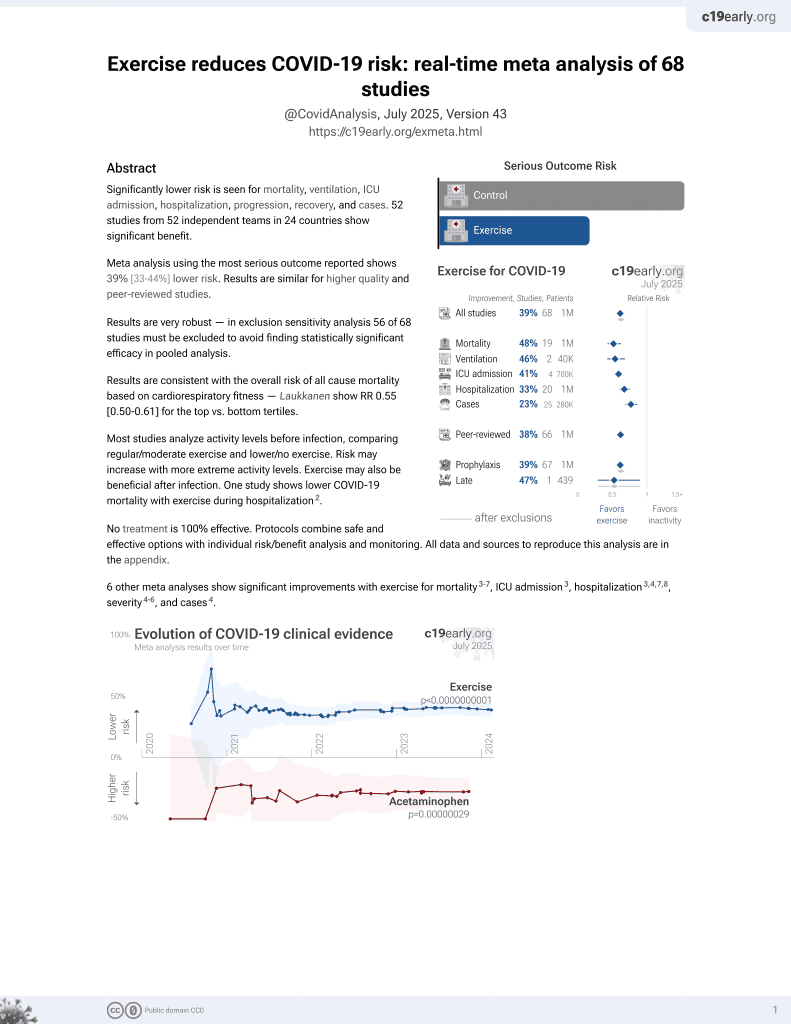
October 2020, now with p < 0.00000000001 from 68 studies.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

{kind=link}
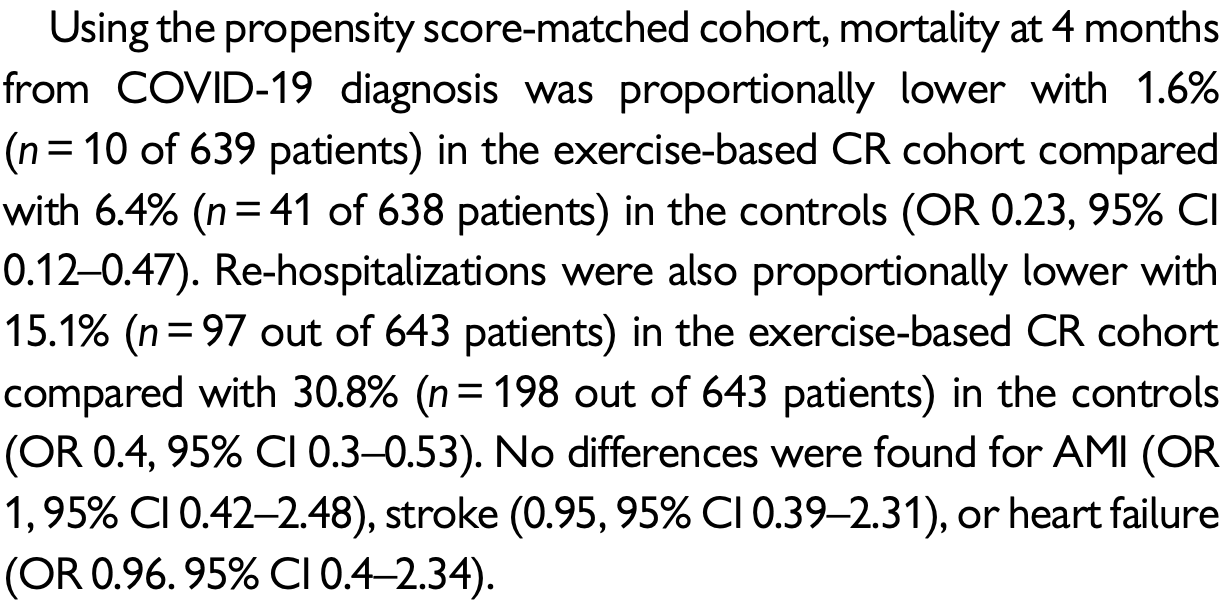
PSM retrospective 643 COVID-19 patients with cardiovascular disease undergoing exercise rehabilitation within 3 months of diagnosis, showing significantly lower re-hospitalization and mortality with exercise rehabilitation.
Standard of Care (SOC) for COVID-19 in the study country,
the USA, is very poor with very low average efficacy for approved treatments1.
Only expensive, high-profit treatments were approved for early treatment. Low-cost treatments were excluded, reducing the probability of early treatment due to access and cost barriers, and eliminating complementary and synergistic benefits seen with many low-cost treatments.
|
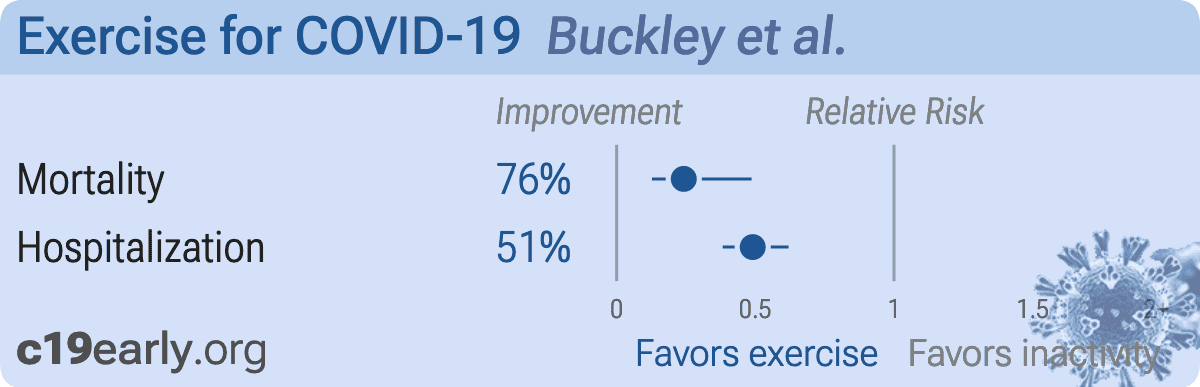
risk of death, 75.8% lower, RR 0.24, p < 0.001, high activity levels 10 of 639 (1.6%), low activity levels 41 of 638 (6.4%), NNT 21, odds ratio converted to relative risk.
|
|
risk of hospitalization, 50.9% lower, RR 0.49, p < 0.001, high activity levels 97 of 643 (15.1%), low activity levels 198 of 643 (30.8%), NNT 6.4, odds ratio converted to relative risk.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Buckley et al., 5 Jul 2021, retrospective, USA, peer-reviewed, 7 authors.
{kind=link}
Abstract: RESEARCH LETTER
European Journal of Preventive Cardiology
doi:10.1093/eurjpc/zwaa135
Exercise rehabilitation associates with lower
mortality and hospitalisation in cardiovascular
disease patients with COVID-19
Benjamin J.R. Buckley 1*, Stephanie L. Harrison1, Elnara Fazio-Eynullayeva2,
Paula Underhill3, Ian D. Jones4, Nefyn Williams5, and Gregory Y.H. Lip1,4,6
1
Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, William Henry Duncan Building, Liverpool L7 8TX, UK; 2TriNetX
Inc, Cambridge, MA, USA; 3TriNetX Inc, London, UK; 4Liverpool Centre for Cardiovascular Science, Liverpool John Moores University, Liverpool, UK; 5Department of Primary
Care and Mental Health, University of Liverpool, UK; and 6Aalborg Thrombosis Research Unit, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Received 21 October 2020; revised 9 November 2020; editorial decision 10 November 2020
The COVID-19 pandemic has caused global health, social, and economic system challenges. In an effort to try and reduce transmission
rates, most countries have varying levels of societal ‘lockdowns’ and
social restrictions in place. This creates a unique challenge for the
promotion of physical activity and exercise, which we know has profound physical and mental health benefits. Although there was initial
promise of increased population interest in physical activity and exercise at the beginning of the COVID-19 pandemic,1 recent large-scale
data from over 455 000 people has demonstrated a 27% decrease in
average daily steps within 30 days of the pandemic declaration.2
It may therefore be more important now than ever to facilitate
physical activity and exercise promotion during and post-COVID19. Despite, recent collaborative efforts developing post-COVID-19
guidelines for athletes returning to exercise,3 limited evidence is
available for the impact of exercise and cardiac rehabilitation (CR)
on clinical outcomes following-COVID-19. Secondary prevention
through comprehensive CR has been recognized as the most costeffective intervention to ensure favourable outcomes across a wide
spectrum of cardiovascular diseases.4 Given there is a high prevalence of cardiovascular disease among patients with COVID-19, and
>7% experience COVID-19 induced myocardial injury,5 CR following COVID-19 infection warrants investigation. The objective of
this study was therefore to compare mortality, hospitalization, and
cardiovascular comorbidity between patients with cardiovascular
disease and COVID-19 with and without an electronic medical
record (EMR) of CR or exercise programmes.
This retrospective observational study was conducted in October
2020 with anonymized data provided by TriNetX, a global federated
health research network with access to EMRs from participating academic medical centres, specialty physician practices, and community
hospitals, predominantly in the USA. Patients with COVID-19 were
identified via Centers for Disease Control and Prevention (CDC)
coding using ICD-10-CM codes, or specific laboratory Logical
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
..
Observation Identifiers Names and Codes.6 All patients were aged
>_18 years with COVID-19 recorded in EMRs between 20 January
2020 (date COVID-19 first confirmed in the USA)7 and 26 May 2020
(to allow 4-month follow-up). Cardiac rehabilitation was..
DOI record:
{
"DOI": "10.1093/eurjpc/zwaa135",
"ISSN": [
"2047-4873",
"2047-4881"
],
"URL": "http://dx.doi.org/10.1093/eurjpc/zwaa135",
"author": [
{
"ORCID": "http://orcid.org/0000-0002-1479-8872",
"affiliation": [
{
"name": "Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, William Henry Duncan Building, Liverpool L7 8TX, UK"
}
],
"authenticated-orcid": false,
"family": "Buckley",
"given": "Benjamin J R",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, William Henry Duncan Building, Liverpool L7 8TX, UK"
}
],
"family": "Harrison",
"given": "Stephanie L",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "TriNetX Inc, Cambridge, MA, USA"
}
],
"family": "Fazio-Eynullayeva",
"given": "Elnara",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "TriNetX Inc, London, UK"
}
],
"family": "Underhill",
"given": "Paula",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Liverpool Centre for Cardiovascular Science, Liverpool John Moores University, Liverpool, UK"
}
],
"family": "Jones",
"given": "Ian D",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Primary Care and Mental Health, University of Liverpool, UK"
}
],
"family": "Williams",
"given": "Nefyn",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, William Henry Duncan Building, Liverpool L7 8TX, UK"
},
{
"name": "Liverpool Centre for Cardiovascular Science, Liverpool John Moores University, Liverpool, UK"
},
{
"name": "Aalborg Thrombosis Research Unit, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark"
}
],
"family": "Lip",
"given": "Gregory Y H",
"sequence": "additional"
}
],
"container-title": [
"European Journal of Preventive Cardiology"
],
"content-domain": {
"crossmark-restriction": false,
"domain": []
},
"created": {
"date-parts": [
[
2021,
6,
30
]
],
"date-time": "2021-06-30T19:22:11Z",
"timestamp": 1625080931000
},
"deposited": {
"date-parts": [
[
2022,
2,
19
]
],
"date-time": "2022-02-19T21:39:53Z",
"timestamp": 1645306793000
},
"funder": [
{
"name": "TriNetX LLC"
},
{
"DOI": "10.13039/100002491",
"doi-asserted-by": "publisher",
"name": "Bristol-Myers Squibb"
}
],
"indexed": {
"date-parts": [
[
2022,
4,
4
]
],
"date-time": "2022-04-04T06:39:29Z",
"timestamp": 1649054369945
},
"is-referenced-by-count": 2,
"issn-type": [
{
"type": "print",
"value": "2047-4873"
},
{
"type": "electronic",
"value": "2047-4881"
}
],
"issue": "1",
"issued": {
"date-parts": [
[
2021,
7,
5
]
]
},
"journal-issue": {
"issue": "1",
"published-online": {
"date-parts": [
[
2021,
7,
5
]
]
},
"published-print": {
"date-parts": [
[
2022,
2,
19
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://academic.oup.com/journals/pages/open_access/funder_policies/chorus/standard_publication_model",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
7,
5
]
],
"date-time": "2021-07-05T00:00:00Z",
"timestamp": 1625443200000
}
}
],
"link": [
{
"URL": "https://academic.oup.com/eurjpc/article-pdf/29/1/e32/42560560/zwaa135.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "syndication"
},
{
"URL": "https://academic.oup.com/eurjpc/article-pdf/29/1/e32/42560560/zwaa135.pdf",
"content-type": "unspecified",
"content-version": "vor",
"intended-application": "similarity-checking"
}
],
"member": "286",
"original-title": [],
"page": "e32-e34",
"prefix": "10.1093",
"published": {
"date-parts": [
[
2021,
7,
5
]
]
},
"published-online": {
"date-parts": [
[
2021,
7,
5
]
]
},
"published-other": {
"date-parts": [
[
2022,
1,
1
]
]
},
"published-print": {
"date-parts": [
[
2022,
2,
19
]
]
},
"publisher": "Oxford University Press (OUP)",
"reference": [
{
"DOI": "10.1136/bjsports-2020-102575",
"article-title": "Is the COVID-19 lockdown nudging people to be more active: a big data analysis",
"author": "Ding",
"doi-asserted-by": "crossref",
"first-page": "1183",
"journal-title": "Br J Sports Med",
"key": "2022021921392285700_zwaa135-B1",
"volume": "54",
"year": "2020"
},
{
"DOI": "10.7326/M20-2665",
"article-title": "Worldwide effect of COVID-19 on physical activity: a descriptive study",
"author": "Tison",
"doi-asserted-by": "crossref",
"first-page": "767",
"journal-title": "Ann Intern Med",
"key": "2022021921392285700_zwaa135-B2",
"volume": "173",
"year": "2020"
},
{
"DOI": "10.1177/2047487320930596",
"article-title": "Exercise in the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) era: a question and answer session with the experts endorsed by the Section of Sports Cardiology & Exercise of the European Association of Preventive Cardiology (EAPC",
"author": "Bhatia",
"doi-asserted-by": "crossref",
"first-page": "1242",
"journal-title": "Eur J Prev Cardiol",
"key": "2022021921392285700_zwaa135-B3",
"volume": "27",
"year": "2020"
},
{
"article-title": "Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology",
"author": "Ambrosetti",
"journal-title": "Eur J Prev Cardiol",
"key": "2022021921392285700_zwaa135-B4",
"year": "2020"
},
{
"DOI": "10.1161/CIRCULATIONAHA.120.046941",
"article-title": "COVID-19 and cardiovascular disease",
"author": "Clerkin",
"doi-asserted-by": "crossref",
"first-page": "1648",
"journal-title": "Circulation",
"key": "2022021921392285700_zwaa135-B5",
"volume": "141",
"year": "2020"
},
{
"key": "2022021921392285700_zwaa135-B6"
},
{
"DOI": "10.1056/NEJMoa2001191",
"article-title": "First case of 2019 novel coronavirus in the United States",
"author": "Holshue",
"doi-asserted-by": "crossref",
"first-page": "929",
"journal-title": "N Engl J Med",
"key": "2022021921392285700_zwaa135-B7",
"volume": "382",
"year": "2020"
},
{
"DOI": "10.1186/1472-6963-11-105",
"article-title": "A comparison of comorbidities obtained from hospital administrative data and medical charts in older patients with pneumonia",
"author": "Chong",
"doi-asserted-by": "crossref",
"first-page": "105",
"journal-title": "BMC Health Serv Res",
"key": "2022021921392285700_zwaa135-B8",
"volume": "11",
"year": "2011"
},
{
"article-title": "The future is now: a call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology",
"author": "Scherrenberg",
"first-page": "doi:10.1177/",
"journal-title": "Eur J Prev Cardiol",
"key": "2022021921392285700_zwaa135-B9",
"year": "2020"
}
],
"reference-count": 9,
"references-count": 9,
"relation": {},
"resource": {
"primary": {
"URL": "https://academic.oup.com/eurjpc/article/29/1/e32/6314558"
}
},
"score": 1,
"short-container-title": [],
"short-title": [],
"source": "Crossref",
"subject": [
"Cardiology and Cardiovascular Medicine",
"Epidemiology"
],
"subtitle": [],
"title": [
"Exercise rehabilitation associates with lower mortality and hospitalisation in cardiovascular disease patients with COVID-19"
],
"type": "journal-article",
"volume": "29"
}