Prognostic factors at admission on patients with cancer and COVID-19: Analysis of HOPE registry data
et al., Medicina Clínica, doi:10.1016/j.medcle.2021.02.010, Oct 2021
{kind=link}
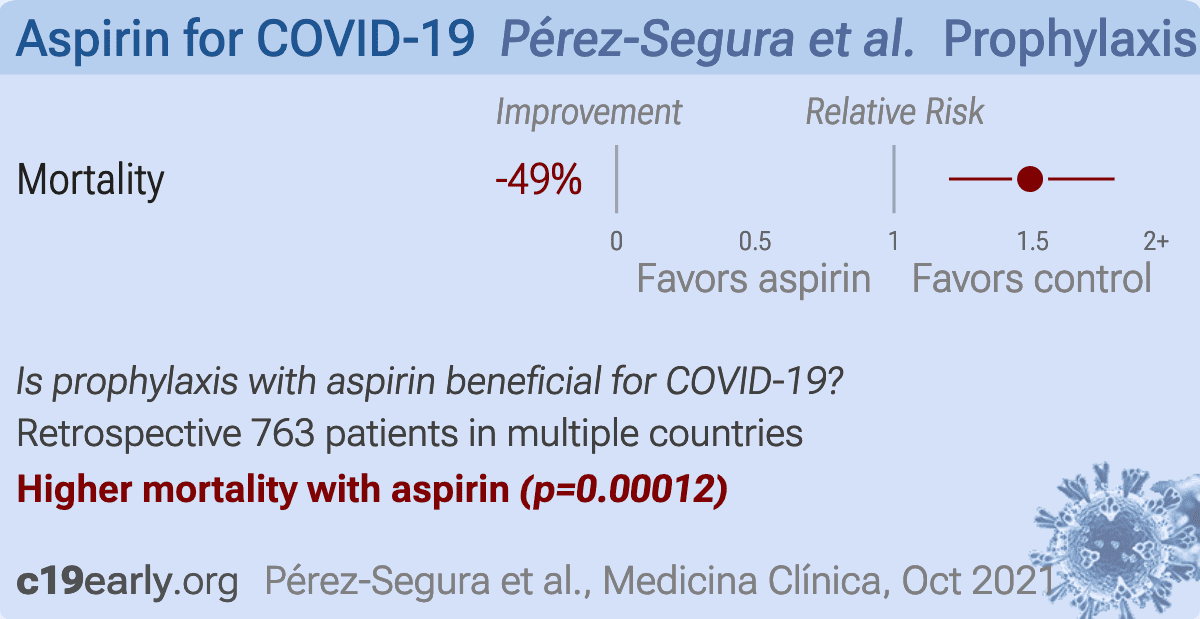
Retrospective 770 COVID-19 patients with cancer, showing increased mortality with aspirin use in unadjusted results.
|
risk of death, 49.1% higher, RR 1.49, p < 0.001, treatment 66 of 155 (42.6%), control 183 of 608 (30.1%), odds ratio converted to relative risk.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |
{kind=link}
Pérez-Segura et al., 4 Oct 2021, retrospective, multiple countries, peer-reviewed, 23 authors.
Prognostic factors at admission on patients with cancer and COVID-19: Analysis of HOPE registry data
Medicina Clínica, doi:10.1016/j.medcli.2021.02.021
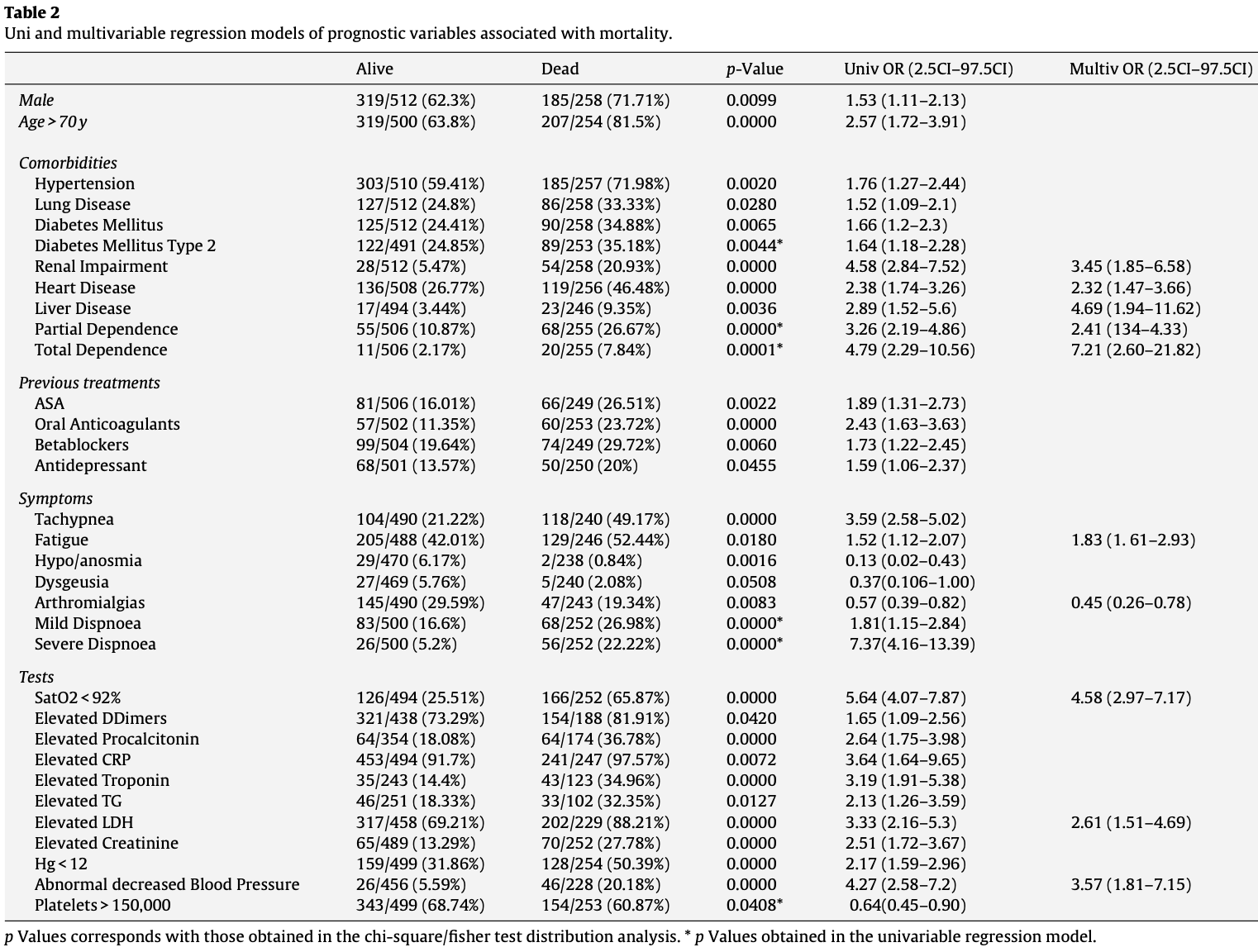
Background: Previous works seem to agree in the higher mortality of cancer patients with COVID-19. Identifying potential prognostic factors upon admission could help identify patients with a poor prognosis. Methods: We aimed to explore the characteristics and evolution of COVID-19 cancer patients admitted to hospital in a multicenter international registry (HOPE COVID-19). Our primary objective is to define those characteristics that allow us to identify cancer patients with a worse prognosis (mortality within 30 days after the diagnosis of COVID-19). Results: 5838 patients have been collected in this registry, of whom 770 had cancer among their antecedents. In hospital mortality reached 258 patients (33.51%). The median was 75 years (65-82). Regarding the distribution by sex, 34.55% of the patients (266/770) were women. The distribution by type of cancer: genitourinary 238/745 (31.95%), digestive 124/745 (16.54%), hematologic 95/745 (12.75%). In multivariate regression analysis, factors that are independently associated with mortality at admis-
identification of factors predicting a worse prognosis, such as those presented here, can help us to better manage this process and try to reduce mortality from COVID-19 in the cancer patient.
Conflict of interests The authors declare that they have no conflict of interest.
References
Alqahtani, Oyelade, Aldhahir, Alghamdi, Almehmadi et al., Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis, PLOS ONE, doi:10.1371/journal.pone.0233147
Blimark, Holmberg, Mellqvist, Landgren, Björkholm et al., Multiple mieloma and infections: a population-based study on 9253 multiple mieloma patients, Haematologica
Cdc, COVID-19 Response Team. Severe outcomes among patients with coronavirus disease 2019 (COVID-19) -United States, MMWR Morb Mortal Wkly Rep
Dai, Liu, Liu, Zhou, Li et al., Patients with cancer appear more vulnerable to SARS-Co-2: a multicenter study during the COVID-19 outbreak, Cancer Discov, doi:10.1158/2159-8290.CD-20-0422
Guan, Ni, Hu, Liang, Ou et al., Clinical characteristics of coronavirus disease 2019 in China, N Engl J Med
Kuderer, Choueiri, Shah, Shyr, Rubinstein et al., Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study, Lancet, doi:10.1016/S0140-6736(20)31187-9
Liang, Guan, Chen, Li, Xu, Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China, Lancet Oncol
Mehta, Goel, Kabarriti, Cole, Goldfinger et al., Case fatality rate of cancer patients with Covid-19 in a New York hospital system, Cancer Disc, doi:10.1158/2159-8290.CD-20-0516
Miyashita, Mikami, Chopra, Yamada, Chernyavsky et al., Do patients with cancer have a poorer prognosis of COVID-19? An experience in New York City, Ann Oncol, doi:10.1016/j.annonc.2020.04.006
Who, WHO Director-General's opening remarks at the media briefing con COVID-19
DOI record:
{
"DOI": "10.1016/j.medcle.2021.02.010",
"ISSN": [
"2387-0206"
],
"URL": "http://dx.doi.org/10.1016/j.medcle.2021.02.010",
"alternative-id": [
"S238702062100485X"
],
"assertion": [
{
"label": "This article is maintained by",
"name": "publisher",
"value": "Elsevier"
},
{
"label": "Article Title",
"name": "articletitle",
"value": "Prognostic factors at admission on patients with cancer and COVID-19: Analysis of HOPE registry data"
},
{
"label": "Journal Title",
"name": "journaltitle",
"value": "Medicina Clínica (English Edition)"
},
{
"label": "CrossRef DOI link to publisher maintained version",
"name": "articlelink",
"value": "https://doi.org/10.1016/j.medcle.2021.02.010"
},
{
"label": "Content Type",
"name": "content_type",
"value": "article"
},
{
"label": "Copyright",
"name": "copyright",
"value": "© 2021 Elsevier España, S.L.U. All rights reserved."
}
],
"author": [
{
"ORCID": "http://orcid.org/0000-0001-5049-7199",
"affiliation": [],
"authenticated-orcid": false,
"family": "Pérez-Segura",
"given": "Pedro",
"sequence": "first"
},
{
"affiliation": [],
"family": "Paz-Cabezas",
"given": "M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Núñez-Gil",
"given": "I.J.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Arroyo-Espliguero",
"given": "R.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-7684-868X",
"affiliation": [],
"authenticated-orcid": false,
"family": "Maroun Eid",
"given": "C.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-3777-2050",
"affiliation": [],
"authenticated-orcid": false,
"family": "Romero",
"given": "R.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Fernández Rozas",
"given": "I.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-6911-7480",
"affiliation": [],
"authenticated-orcid": false,
"family": "Uribarri",
"given": "A.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Becerra-Muñoz",
"given": "V.M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "García Aguado",
"given": "M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Huang",
"given": "J.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Rondano",
"given": "E.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Cerrato",
"given": "E.",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-1063-9898",
"affiliation": [],
"authenticated-orcid": false,
"family": "Rodríguez",
"given": "E. Alfonso",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Ortega-Armas",
"given": "M.E.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Raposeiras Roubin",
"given": "S.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Pepe",
"given": "M.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Feltes",
"given": "G.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Gonzalez",
"given": "A.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Cortese",
"given": "B.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Buzón",
"given": "L.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "El-Battrawy",
"given": "I.",
"sequence": "additional"
},
{
"affiliation": [],
"family": "Estrada",
"given": "V.",
"sequence": "additional"
}
],
"container-title": "Medicina Clínica (English Edition)",
"container-title-short": "Medicina Clínica (English Edition)",
"content-domain": {
"crossmark-restriction": true,
"domain": [
"elsevier.es",
"elsevier.com",
"sciencedirect.com"
]
},
"created": {
"date-parts": [
[
2021,
10,
4
]
],
"date-time": "2021-10-04T23:37:22Z",
"timestamp": 1633390642000
},
"deposited": {
"date-parts": [
[
2023,
5,
23
]
],
"date-time": "2023-05-23T04:13:20Z",
"timestamp": 1684815200000
},
"indexed": {
"date-parts": [
[
2023,
8,
1
]
],
"date-time": "2023-08-01T08:31:28Z",
"timestamp": 1690878688849
},
"is-referenced-by-count": 2,
"issue": "7",
"issued": {
"date-parts": [
[
2021,
10
]
]
},
"journal-issue": {
"issue": "7",
"published-print": {
"date-parts": [
[
2021,
10
]
]
}
},
"language": "en",
"license": [
{
"URL": "https://www.elsevier.com/tdm/userlicense/1.0/",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T00:00:00Z",
"timestamp": 1633046400000
}
},
{
"URL": "https://doi.org/10.15223/policy-017",
"content-version": "stm-asf",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T00:00:00Z",
"timestamp": 1633046400000
}
},
{
"URL": "https://doi.org/10.15223/policy-037",
"content-version": "stm-asf",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T00:00:00Z",
"timestamp": 1633046400000
}
},
{
"URL": "https://doi.org/10.15223/policy-012",
"content-version": "stm-asf",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T00:00:00Z",
"timestamp": 1633046400000
}
},
{
"URL": "https://doi.org/10.15223/policy-029",
"content-version": "stm-asf",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T00:00:00Z",
"timestamp": 1633046400000
}
},
{
"URL": "https://doi.org/10.15223/policy-004",
"content-version": "stm-asf",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2021,
10,
1
]
],
"date-time": "2021-10-01T00:00:00Z",
"timestamp": 1633046400000
}
}
],
"link": [
{
"URL": "https://api.elsevier.com/content/article/PII:S238702062100485X?httpAccept=text/xml",
"content-type": "text/xml",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://api.elsevier.com/content/article/PII:S238702062100485X?httpAccept=text/plain",
"content-type": "text/plain",
"content-version": "vor",
"intended-application": "text-mining"
}
],
"member": "78",
"original-title": [],
"page": "318-324",
"prefix": "10.1016",
"published": {
"date-parts": [
[
2021,
10
]
]
},
"published-print": {
"date-parts": [
[
2021,
10
]
]
},
"publisher": "Elsevier BV",
"reference": [
{
"author": "WHO",
"key": "10.1016/j.medcle.2021.02.010_bib0055",
"series-title": "WHO Director-General's opening remarks at the media briefing con COVID-19",
"year": "2020"
},
{
"DOI": "10.1016/S1470-2045(20)30096-6",
"article-title": "Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China",
"author": "Liang",
"doi-asserted-by": "crossref",
"first-page": "335",
"journal-title": "Lancet Oncol",
"key": "10.1016/j.medcle.2021.02.010_bib0060",
"volume": "21",
"year": "2020"
},
{
"DOI": "10.1158/2159-8290.CD-20-0422",
"article-title": "Patients with cancer appear more vulnerable to SARS-Co-2: a multicenter study during the COVID-19 outbreak",
"author": "Dai",
"doi-asserted-by": "crossref",
"journal-title": "Cancer Discov",
"key": "10.1016/j.medcle.2021.02.010_bib0065",
"year": "2020"
},
{
"DOI": "10.1016/j.annonc.2020.04.006",
"article-title": "Do patients with cancer have a poorer prognosis of COVID-19? An experience in New York City",
"author": "Miyashita",
"doi-asserted-by": "crossref",
"journal-title": "Ann Oncol",
"key": "10.1016/j.medcle.2021.02.010_bib0070",
"year": "2020"
},
{
"DOI": "10.3324/haematol.2014.107714",
"article-title": "Multiple mieloma and infections: a population-based study on 9253 multiple mieloma patients",
"author": "Blimark",
"doi-asserted-by": "crossref",
"first-page": "107",
"journal-title": "Haematologica",
"key": "10.1016/j.medcle.2021.02.010_bib0075",
"volume": "100",
"year": "2015"
},
{
"DOI": "10.15585/mmwr.mm6912e2",
"article-title": "COVID-19 Response Team. Severe outcomes among patients with coronavirus disease 2019 (COVID-19) – United States, February 12–March 16, 2020",
"author": "CDC",
"doi-asserted-by": "crossref",
"first-page": "343",
"journal-title": "MMWR Morb Mortal Wkly Rep",
"key": "10.1016/j.medcle.2021.02.010_bib0080",
"volume": "69",
"year": "2020"
},
{
"DOI": "10.1056/NEJMoa2002032",
"article-title": "Clinical characteristics of coronavirus disease 2019 in China",
"author": "Guan",
"doi-asserted-by": "crossref",
"first-page": "1708",
"journal-title": "N Engl J Med",
"key": "10.1016/j.medcle.2021.02.010_bib0085",
"volume": "382",
"year": "2020"
},
{
"DOI": "10.1158/2159-8290.CD-20-0516",
"article-title": "Case fatality rate of cancer patients with Covid-19 in a New York hospital system",
"author": "Mehta",
"doi-asserted-by": "crossref",
"journal-title": "Cancer Disc",
"key": "10.1016/j.medcle.2021.02.010_bib0090",
"year": "2020"
},
{
"DOI": "10.1016/S0140-6736(20)31187-9",
"article-title": "Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study",
"author": "Kuderer",
"doi-asserted-by": "crossref",
"journal-title": "Lancet",
"key": "10.1016/j.medcle.2021.02.010_bib0095",
"year": "2020"
},
{
"DOI": "10.1371/journal.pone.0233147",
"article-title": "Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis",
"author": "Alqahtani",
"doi-asserted-by": "crossref",
"journal-title": "PLOS ONE",
"key": "10.1016/j.medcle.2021.02.010_bib0100",
"volume": "15",
"year": "2020"
}
],
"reference-count": 10,
"references-count": 10,
"relation": {},
"resource": {
"primary": {
"URL": "https://linkinghub.elsevier.com/retrieve/pii/S238702062100485X"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"General Medicine"
],
"subtitle": [],
"title": "Prognostic factors at admission on patients with cancer and COVID-19: Analysis of HOPE registry data",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.1016/elsevier_cm_policy",
"volume": "157"
}