
Casirivimab/imdevimab reduced COVID-19 risk: real-time meta-analysis of 34 studies (Version 51)
, May 2026
18th treatment shown to reduce risk in
March 2021, now with p = 0.000095 from 34 studies, recognized in 52 countries.
Efficacy is variant dependent.
No treatment is 100% effective. Protocols
combine treatments.
6,600+ studies for
220+ treatments. c19early.org
|

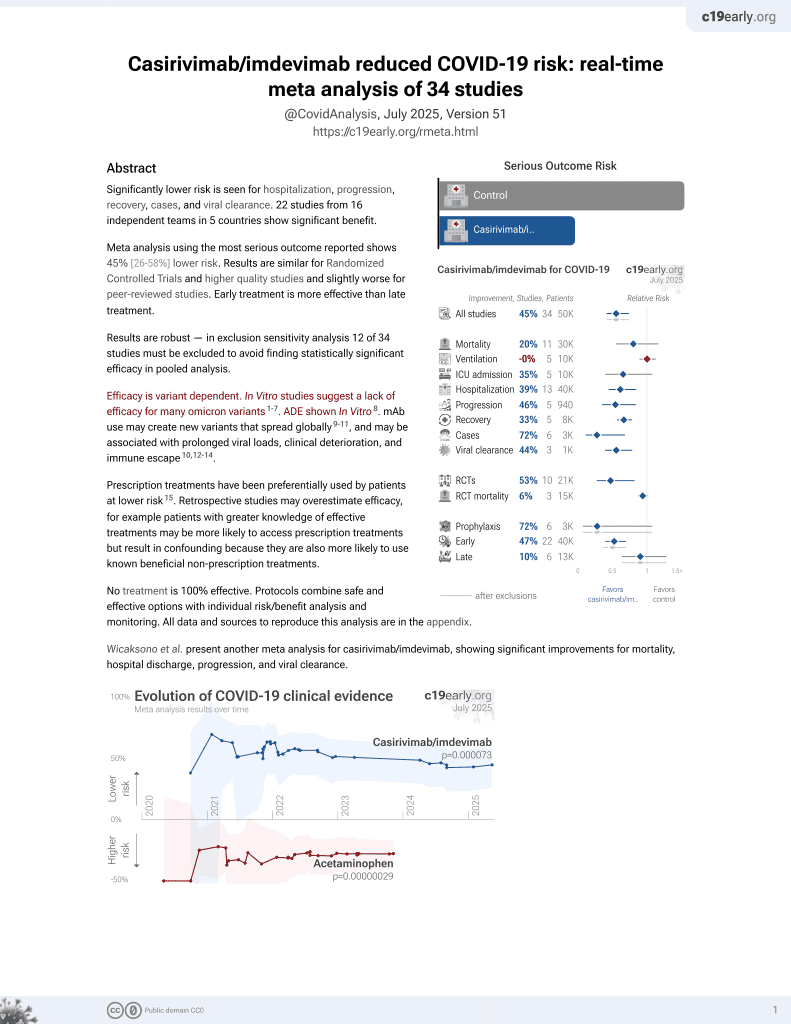
Significantly lower risk is seen for hospitalization, progression, recovery, cases, and viral clearance. 22 studies from 16 independent teams in 5 countries show significant benefit.
Meta-analysis using the most serious outcome reported shows 45% [26‑59%] lower risk. Results are similar for Randomized Controlled Trials and higher quality studies and slightly worse for peer-reviewed studies. Early treatment is more effective than late treatment.
Results are robust—in worst case exclusion sensitivity analysis 11 of 34 studies must be excluded before statistical significance is lost. Emergent results for meta-regression of efficacy vs. treatment delay (p = 0.00000019) that match biological mechanisms confirm efficacy.
Control Casirivimab/i..
Efficacy is variant dependent. In Vitro studies suggest a lack of efficacy for many omicron variants1-7. ADE shown In Vitro8. mAb use may create new variants that spread globally9-11, and may be associated with increased risk of autoimmune disease12, prolonged viral loads, clinical deterioration, and immune escape10,13-17.
Prescription treatments have been preferentially used by patients at lower risk18. Retrospective studies may overestimate efficacy, for example patients with greater knowledge of effective treatments may be more likely to access prescription treatments but result in confounding because they are also more likely to use known beneficial non-prescription treatments.
No treatment is 100% effective. Protocols combine safe and effective options with individual risk/benefit analysis and monitoring. All data and sources to reproduce this analysis are in the appendix.
Wicaksono et al. present another meta-analysis for casirivimab/imdevimab, showing significant improvements for mortality, hospital discharge, progression, and viral clearance.
{kind=link}
Covid Analysis et al., May 2026, preprint, 1 author.